
Abstract
Objective:
To evaluate the effect of facial attractiveness on treatment recommendations for non-melanoma skin cancer of the head and neck.
Methods:
We conducted a cross-sectional survey of Canadian surgeons and radiation oncologists to assess the effect of facial attractiveness on treatment choices for non-melanoma head and neck skin cancers. Participants rated preference of surgery or radiotherapy (RT) for digitally altered images with lesions at 5 facial subsites. The primary outcome was the association between attractiveness and treatment choice; the secondary outcome was the influence of lesion location. Associations between attractiveness and treatment choice were analyzed with Spearman’s correlation, and site-specific differences were descriptively evaluated.
Results:
One hundred and eight respondents (17.8% response rate) completed the survey. Surgery was favored across all anatomical subsites. Facial attractiveness was not significantly associated with treatment recommendations at any subsite. At the nasal tip, there was a trend toward recommending surgery for more attractive patients (ρ = 0.13, P = .08). Independent of attractiveness, lesion location appeared to influence treatment recommendations, with the nasal tip more often considered for RT than other subsites.
Conclusions:
Facial attractiveness did not influence treatment recommendations for non-melanoma head and neck skin cancers. Surgery was preferred across anatomic subsites, but respondents often considered for RT for treating nasal tip non-melanoma skin cancers.
Keywords
Introduction
The influence of cognitive heuristics and bias in clinical decision-making (CDM) remains understudied in medicine and surgery. Physical attractiveness stereotype (PAS) is the tendency to attribute positive characteristics to more attractive faces, but no research has investigated its role in CDM. 1 Studies have shown that higher patient attractiveness decreases the likelihood of a missed clinical diagnosis and that physicians rated pain more severely in less attractive patients.2,3 In their early stages, non-melanoma head and neck skin cancers generally herald favorable outcomes and may be guideline concordantly managed via surgical excision or directed external beam radiotherapy (RT).4-6 Surgical excision typically involves removing the cancer under local anesthesia with a clinically appropriate surgical margin; this surgical defect may be repaired primarily or via the transposition of local or distant tissue. Alternatively, RT utilizes successive doses of radiation to an affected area over a defined period. While this remains controversial, RT is anecdotally associated with relatively better cosmesis than its surgical counterpart, especially in cosmetically sensitive areas or locations that require technically challenging reconstruction.7,8 Since both approaches often confer relatively similar clinical outcomes for disease control, physician discretion plays a key role in treatment decisions. Understanding how non-clinical factors like physical attractiveness influence these choices is important for identifying bias and promoting equitable care. We tested whether the PAS affects clinician’s recommendation between surgery and RT in patients with non-melanoma skin cancers of the head and neck.
Methods
Study Design
We conducted a cross-sectional online survey to assess the effect of facial attractiveness on clinician decision-making in non-melanoma skin cancer of the head and neck. Ethics approval was obtained from the Hamilton Integrated Research Ethics Board (2023-14615-GRA). This study was performed in accordance with Checklist for Reporting Results of Internet E-Surveys (CHERRIES) guidelines. 9
Survey Design and Distribution
This online survey consisted of 4 sections: (1) demographics and experience, including years in practice and subspecialty training; (2) treatment practices and general preferences for surgery or RT; (3) image-based judgments, where respondents reviewed randomized faces stratified by attractiveness, ethnicity, gender, and lesion site; and (4) a general open-comment/debriefing section (Supplementary Appendix A). Online invitations were sent to Canadian otolaryngologists, radiation oncologists, and plastic surgeons via professional society email lists (ie, Canadian Society of Otolaryngology–Head and Neck Surgery and Canadian Association of Radiation Oncologists) as a closed survey. Participation was voluntary and anonymous, with electronic informed consent collected before survey initiation. Licensed, retired, and resident otolaryngologists, plastic surgeons, and radiation oncologists in active clinical practice in Canada were eligible to participate. All survey respondents were presented with an equal number of photo stimuli with varied skin tones and ethnicities from validated databases of facial stimuli. All survey answers were included in analysis as per consent form.
Survey Stimuli and Materials
Facial stimuli were selected from 2 validated databases of faces with validated normative attractiveness ratings for each face: the Chicago Face Database 10 and the FACES database, 11 and limited to individuals aged 30+ and rated in the upper or lower quartiles of facial attractiveness (ie, Likert scale range: 0-2.5 or 4-7). Both repositories provide facial images with written informed consent for publication and research use, as confirmed by their release agreements. As such, no additional consent regarding the release of these images was required for this study. Anonymization is not possible due to the nature of this study. We then used Adobe Photoshop (Adobe Inc, San Jose, California), to digitally add non-melanoma (ie, basal cell carcinoma) lesions to 5 facial subsites: forehead, left cheek, right cheek, nasal tip, and lip. An example is available in the supplement (Supplementary Figure 1). A separate cohort of undergraduate psychology students revalidated the images after lesions were applied for perceived attractiveness to ensure consistency (data not shown). All included faces were stratified by attractiveness and ethnicity and randomly sampled to ensure equal distribution across image categories. Each participant viewed five lesion sites across eight total faces. For each case, participants rated likelihood to choose surgery and RT on a continuous (0-100) scale. Image order was fully randomized to minimize order effects. IP addresses were collected to ensure unique survey participants. Participants completed the questionnaire in the predetermined sequence and were unable to review answered questions. There were no time constraints for survey completion.
Outcomes
The primary outcome was the association between facial attractiveness and treatment recommendation (surgery vs RT). The secondary outcome was the influence of lesion subsite (facial location) on treatment recommendation.
Statistical Analysis
We used descriptive statistics to summarize demographics of survey respondents. Associations between stimuli attractiveness and treatment choice were assessed using Spearman’s rank correlation. Since all survey respondents were presented with an equal number of varied skin tones in the photo stimuli, we did not perform statistical adjustment for skin tone and ethnicity. Analyses were conducted in Stata 16 (StataCorp, College Station, TX) and R 4.5.1 (R Foundation for Statistical Computing, Vienna, Austria), with an alpha value of 0.05.
Results
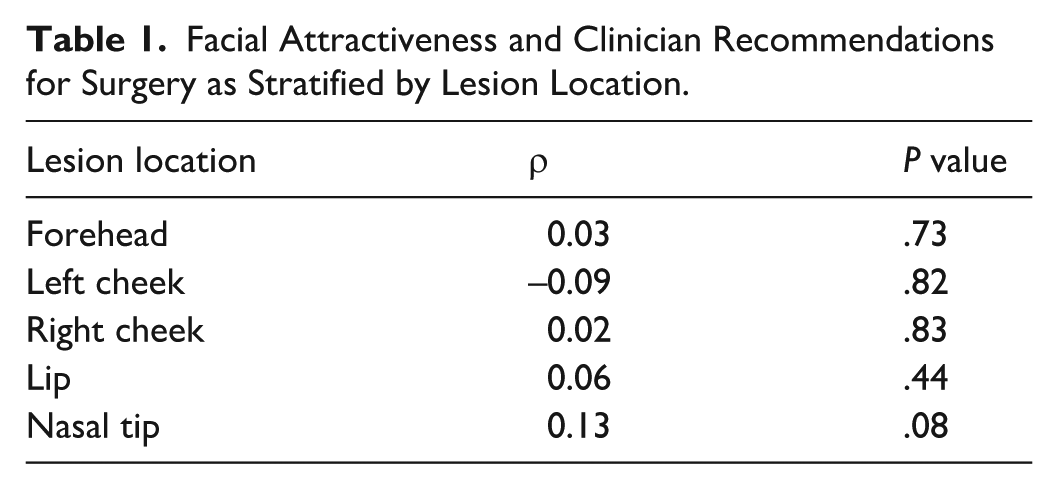
A total of 108 participants completed the survey, yielding a response rate of 17.8%. The majority were faculty otolaryngologist—head and neck surgeons practicing in Canada (90.7%, n = 98). Among respondents, 41.7% (n = 45) reported working primarily in academic settings, while 38.9% (n = 42) worked primarily in community settings (Supplementary Table 1). The remaining participants 19.4% did not specify their practice environment (n = 21). Across survey respondents, 21.5% (n = 23) had 0 to 4 years of surgical experience, while 19.6% (n = 21) had over 20 years of surgical experience (Supplementary Table 2). Spearman’s correlation coefficients showed no statistically significant association between facial attractiveness scores and the likelihood of recommending surgery for lesions across all sites (forehead [ρ = 0.03, P = .73], left cheek [ρ = −0.09, P = .82], right cheek [ρ = 0.02, P = .83], or lip [ρ = 0.06, P = .44]). For the nasal tip, the estimate was positive but not statistically significant (ρ = 0.13, P = .08) (Table 1).
Facial Attractiveness and Clinician Recommendations for Surgery as Stratified by Lesion Location.
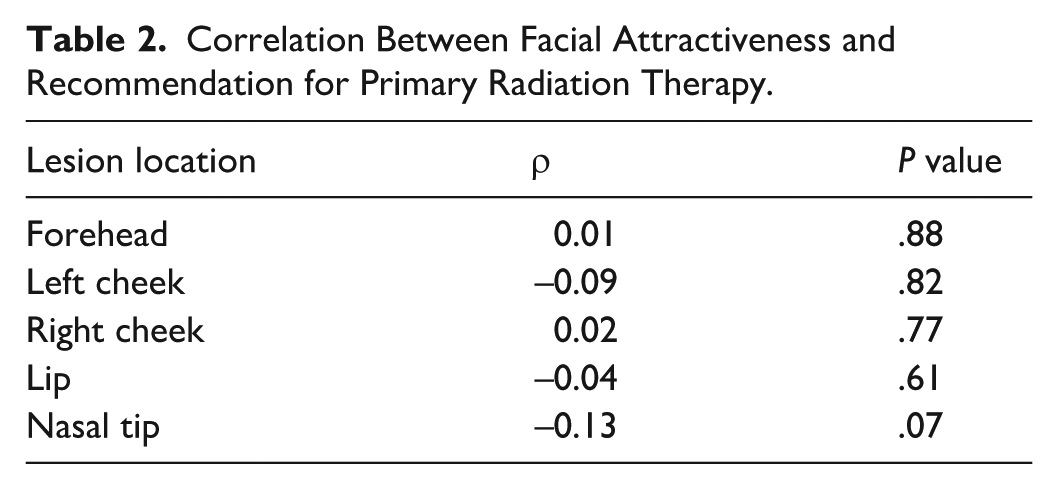
Similarly, no statistically significant association between facial attractiveness and the likelihood of recommending RT for lesions at the forehead (ρ = 0.01, P = .88), left cheek (ρ = −0.09, P = .82), right cheek (ρ = 0.02, P = .77), or lip (ρ = −0.04, P = .61) was observed. For the nasal tip, the estimate was negative but not statistically significant (ρ = −0.13, P = .07) (Table 2).
Correlation Between Facial Attractiveness and Recommendation for Primary Radiation Therapy.
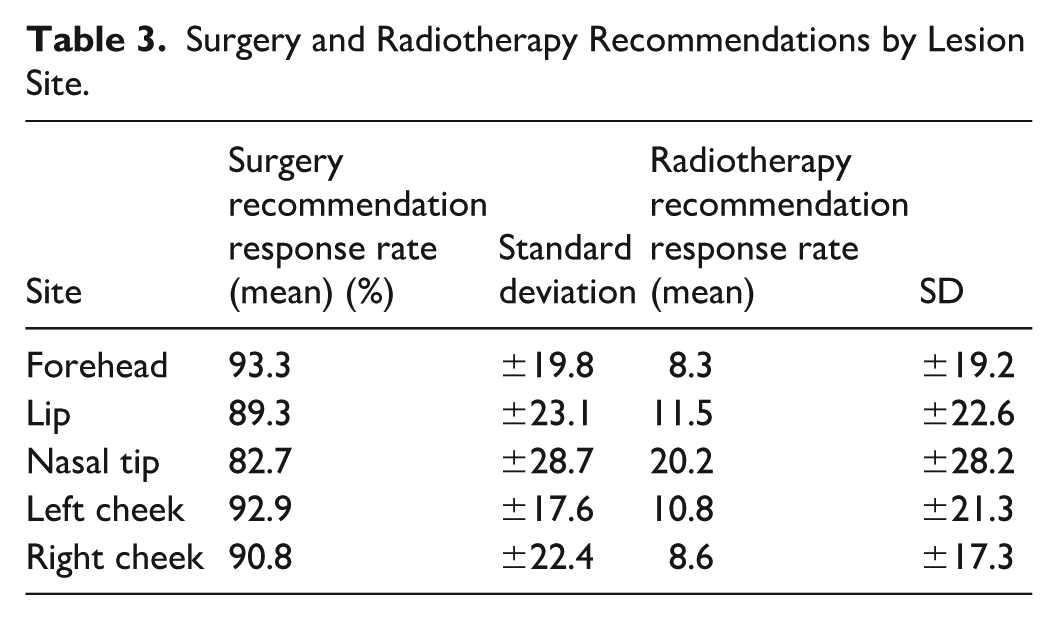
Across subsites, survey respondents demonstrated a significantly greater likelihood for recommending surgery over RT (Figure 1). The nasal tip, however, was the site least likely to receive a surgical recommendation, with a mean response rate of 82.7% (SD = 28.7) (Table 3). The forehead was the most likely location for surgical excision to be recommended with a mean of 93.3% (SD = 19.8). The nasal tip was more likely to be managed with RT than any other site with a mean response rate of 20.2% (SD = 28.2) (Table 3). The forehead had the lowest likelihood of RT being recommended with a mean response rate of 8.3% (SD = 19.2) (Table 3).
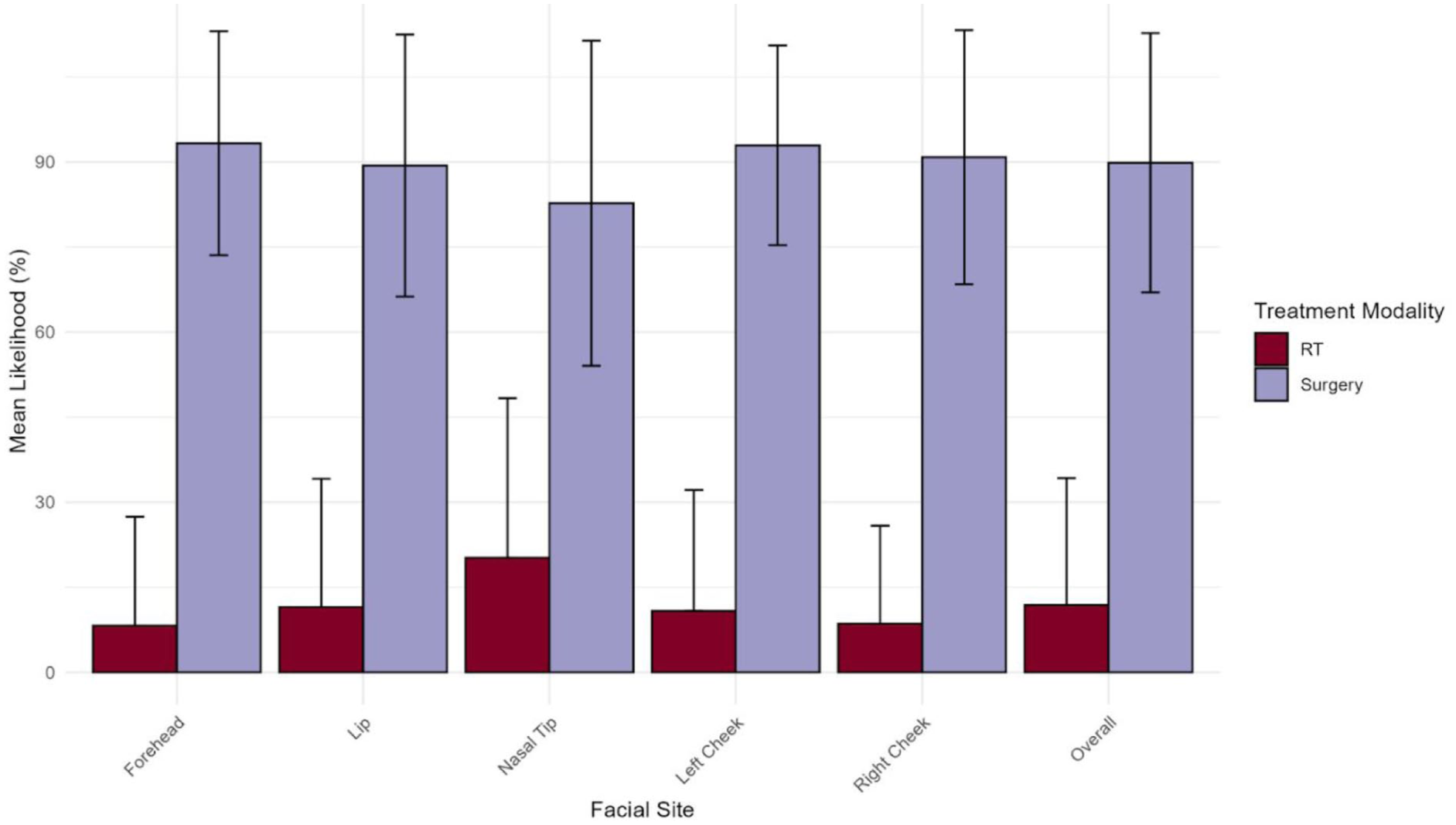
Mean likelihoods to recommend primary surgery and primary radiation therapy by facial site.
Surgery and Radiotherapy Recommendations by Lesion Site.
Discussion
To the best of our knowledge, this is the first evaluation of the impact of patient attractiveness on CDM when treating non-melanoma head and neck skin cancer. We found no significant association between patient facial attractiveness and physician recommendation for primary surgical excision or RT when treating non-melanoma head and neck skin cancer. Surveyed physicians were more likely to recommend surgery over RT independent of lesion site. Finally, clinicians may be more likely to recommend RT for non-melanoma skin cancers located on the nasal tip.
We were unable to establish an association between facial attractiveness and CDM in non-melanoma head and neck skin cancer, but the influence of PAS on healthcare decisions has been reported and necessitates further investigation.2,3,12 While our survey did evaluate for operator-specific factors, such as surgeon experience, there are many institution- and resource-specific factors that can also impact the decision to recommend surgery for RT for head and neck skin cancers.13,14 Clinician recommendations are also guided by patient comorbidities and fitness, in addition to aesthetic challenges with achieving negative surgical margins. 15 Clinician biases may further influence treatment decision-making, but further research of clinician heuristics and bias when evaluating patients required additional investigations.
Surgery was recommended over RT by survey respondents for all lesions independent of facial subsites. Most survey respondents, however, were otolaryngologist—head and neck surgeons, and it has been documented that specialists are more likely to recommend treatment modalities within their own fields. 16 Despite these findings, survey respondents were likelier to recommend primary RT for nasal tip lesions, which may reflect the well-documented aesthetic and technical challenges and fellowship-specific training needed to resect and reconstruct this facial subsite.17,18
There was a trend toward recommending primary surgery rather than RT for nasal tip lesions located on facial stimuli with higher facial attractiveness scores. Several factors may explain this trend. Surgery could be assumed to provide superior long term cosmetic outcomes in highly visible subsites, and reconstructive series support the importance of technical expertise in these regions.19,20 Many patients with nasal cancers requiring complex treatment techniques also present first to tertiary surgical centers, where operative management is the default and fellowship-trained reconstructive surgeons are readily available. 21 Finally, surgery may be considered more predictable than RT, with clinicians seeking to avoid late radiation changes, such as atrophy, telangiectasia, or dyschromia on cartilaginous subsites, reinforcing its role as the standard primary modality for facial non-melanoma skin cancers.22,23
Limitations
Survey response rate was low (17.8%) and primarily composed of otolaryngologists, with few responses from plastic surgeons and radiation oncologists, potentially biasing results toward surgical preferences. This specialty distribution reflects practice patterns in Canada, but future research could aim to better evaluate CDM amongst dermatologists, radiation oncologists, and plastic surgeons. In addition, the use of digitally altered images may not fully replicate real-world lesion presentations, and respondents may have deduced that our survey was focused on attractiveness despite our attempts at respondent deception and blinding. Finally, we did not stratify our statistical analysis based on photo stimuli skin tone and ethnicity due, in part, to the low response rate, but future studies should examine the impact of these factors on clinician decision-making in skin cancer management. 24
Conclusion
Facial attractiveness did not influence treatment recommendations for non-melanoma head and neck skin cancers. Surgery was preferred across subsites, with the nasal tip noted as a location where RT was more often considered than other subsites, likely reflecting reconstructive complexity rather than physical attractiveness bias.
Summary Statement
In this survey of Canadian clinicians, facial attractiveness did not affect management decisions for non-melanoma head and neck skin cancers, with surgery favored across subsites and the nasal tip uniquely showing a trend toward more frequent RT consideration.
Supplemental Material
sj-docx-1-acs-10.1177_07488068251405688 – Supplemental material for Physical Attractiveness and Clinical Decision-Making in Non-Melanoma Head and Neck Skin Cancer: A Cross-Sectional Survey Study
Supplemental material, sj-docx-1-acs-10.1177_07488068251405688 for Physical Attractiveness and Clinical Decision-Making in Non-Melanoma Head and Neck Skin Cancer: A Cross-Sectional Survey Study by Kieran Chalmers, Phillip Staibano, Nick Sahlollbey, Anna Krasotkina, Naiqi Xiao and Michael K. Gupta in The American Journal of Cosmetic Surgery
Supplemental Material
sj-docx-2-acs-10.1177_07488068251405688 – Supplemental material for Physical Attractiveness and Clinical Decision-Making in Non-Melanoma Head and Neck Skin Cancer: A Cross-Sectional Survey Study
Supplemental material, sj-docx-2-acs-10.1177_07488068251405688 for Physical Attractiveness and Clinical Decision-Making in Non-Melanoma Head and Neck Skin Cancer: A Cross-Sectional Survey Study by Kieran Chalmers, Phillip Staibano, Nick Sahlollbey, Anna Krasotkina, Naiqi Xiao and Michael K. Gupta in The American Journal of Cosmetic Surgery
Supplemental Material
sj-docx-3-acs-10.1177_07488068251405688 – Supplemental material for Physical Attractiveness and Clinical Decision-Making in Non-Melanoma Head and Neck Skin Cancer: A Cross-Sectional Survey Study
Supplemental material, sj-docx-3-acs-10.1177_07488068251405688 for Physical Attractiveness and Clinical Decision-Making in Non-Melanoma Head and Neck Skin Cancer: A Cross-Sectional Survey Study by Kieran Chalmers, Phillip Staibano, Nick Sahlollbey, Anna Krasotkina, Naiqi Xiao and Michael K. Gupta in The American Journal of Cosmetic Surgery
Supplemental Material
sj-docx-4-acs-10.1177_07488068251405688 – Supplemental material for Physical Attractiveness and Clinical Decision-Making in Non-Melanoma Head and Neck Skin Cancer: A Cross-Sectional Survey Study
Supplemental material, sj-docx-4-acs-10.1177_07488068251405688 for Physical Attractiveness and Clinical Decision-Making in Non-Melanoma Head and Neck Skin Cancer: A Cross-Sectional Survey Study by Kieran Chalmers, Phillip Staibano, Nick Sahlollbey, Anna Krasotkina, Naiqi Xiao and Michael K. Gupta in The American Journal of Cosmetic Surgery
Footnotes
Acknowledgements
None.
Ethical Considerations
Ethical approval for this study was obtained from the Hamilton Integrated Research Ethics Board (2023-14615-GRA) for the survey of physician participants. Written informed consent was obtained from all survey participants. Facial stimuli were obtained from the publicly available Chicago Face Database and the FACES database (Max Planck Institute), which both provide facial images with written informed consent for research and publication use.10,11 As such, no additional consent was required for the use of these images, and anonymization/blinding was not performed given the study’s focus on facial attractiveness.
Author Contributions
KC contributed to data analysis, writing, and editing; PS contributed to data analysis, study design, data collection, writing, and editing; NS contributed to study design, data collection, and editing; AK contributed to study design and data collection; NX contributed to study design and data collection; and MG contributed to study design, data collection, data analysis, writing, and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed Consent
Written consent was obtained from all of those participating in the study survey. No consent was necessary for the faces used in the construction of the survey as these are accessed through publicly available databases.
Supplemental Material
Supplemental material for this article is available online.