
Abstract
Background:
Chin implantation is a commonly performed facial plastic surgery procedure. There are 2 approaches to this procedure: submental and transoral. There is no consensus as to which is the best and safest approach.
Objective:
The objective of this review is to ascertain the risks and benefits of using an intraoral versus submental approach for chin implantation.
Methods:
A systematic review of all articles published in MEDLINE, Embase, Cochrane Library, and Google Scholar was performed from 1966 to 2020.
Results:
A total of 1410 articles were reviewed and 38 were chosen for the review based on predetermined selection criteria. Total complication rates in the transoral group ranged from 0% to 14.7%, whereas total complication rates in the submental group ranged from 0% to 15%. No clear difference in the rates of any specific complication was found between the 2 groups.
Conclusion:
There is no demonstrated difference in complication rates between the 2 approaches to chin implantation. Individual patient assessment and surgeon preference remain the most important determinants of surgical approach.
Introduction
Facial harmony and balanced proportions of facial features are the hallmarks of beauty. The appearance of any face is a composite of its anatomic elements—teeth, bone, and soft tissues—and their relationship to one another. 1 The chin is a prominent feature that has a large role in overall facial balance.
The casual observer usually does not recognize an under-projected or over-projected chin as contributing to facial disproportion. 2 Since a person’s view of themselves is usually in a mirror (anterior-posterior dimension), discrepancies of chin projection are often not recognized by the patient themselves. As such, surgical correction of minor deformities of the chin is infrequently requested. However, it is well known that improvement of chin projection to ideal aesthetic proportions can significantly improve one’s appearance. The facial plastic surgeon must therefore be able to accurately recognize, diagnose, and treat deformities of the chin to optimize facial proportions. 3
Augmentation of the chin can be achieved via osseous genioplasty, or placement of various chin implants. Each procedure has its own unique indications, advantages, and disadvantages. The use of a chin implant for augmentation is a simple and reliable method for correction of a mild to moderate horizontal chin deficiency. Generally, significant vertical chin discrepancies (excess or deficiency) or transverse asymmetries of the chin are addressed via osseous genioplasty. Osseous genioplasty allows advancement or retrusion in the anterior-posterior direction, as well as lengthening or shortening in the vertical dimension and also provides a method to correct transverse chin asymmetries. 3
For chin implantation, many varieties of alloplastic implant materials have been described in the literature which commonly include: Silastic (solid silicone; Michigan Medical Corporation, Santa Barbara, California), Mersilene mesh (polyester fiber mesh; Ethicon, Somerville, New Jersey), Supramid (polymide nylon mesh; Ethicon, Somerville, New Jersey), Proplast (polytef; Novamed, Chicago, Illinois), Medpor (porous polyethylene; Porex Surgical Inc, College Park, Georgia), and Gore-Tex (polytetrafluoroethylene; W.L. Gore & Associates Inc, Flagstaff, Arizona). 4
With regard to chin implant technique, either of 2 incisions is used: external (via submental incision) or intraoral (via an incision in the gingivobuccal sulcus). 4 The intraoral technique can be performed through either a vertical or a horizontal incision. The choice of incision site is often determined by surgeon preference and comfort with technique. External submental incisions are also used for chin implants if another procedure (such as submentoplasty) is being done at the same time.
Asymmetry, malposition, infection, extrusion, mental nerve dysfunction, and chin ptosis are the most commonly cited complications of chin implants.5,6 It is often anecdotally noted that the intraoral approach has higher rates of all of these complications.4,5,7,8 Malposition and ptosis are attributed to the presumable disruption of the attachments of the mentalis muscle via the intraoral approach. The disadvantage of the submental approach is usually cited to be a visible scar and the potential for poor scarring. However, these assertions have never been studied in any trials or through meta-analysis or systematic review of literature.
The objective of this review is to ascertain the risks and benefits of using an intraoral versus submental approach for chin implantation. The results of a consecutive case series of 89 consecutive patients who underwent a chin implant procedure via the submental approach at UC Davis Medical Center over a 10-year period (January 2002-December 2011) have been added to the analysis.
Methods
Search Strategy
A comprehensive search methodology was used to assist in locating both published and unpublished studies. Two experienced librarians completed the search. MEDLINE, Embase, Cochrane Library, and Google Scholar were searched from 1966 to 2020. The search strategies employed database-specific subject headings and keywords for “chin,” “implant,” “prosthesis,” “genioplasty,” “mentoplasty,” “chin,” “augment,” “reconstruct,” and “humans.”
Study Selection Strategy
Studies included were from any country, in English or French, and were research articles. Only full-text articles were included. The study designs included were randomized and nonrandomized trials, observational studies including prospective and retrospective, and case series. Studies were included if they involved patients undergoing chin implantation using alloplastic materials using either transoral or submental approach for implant insertion. Selected studies were those providing data on patient demographics and rates of postoperative complications as outcomes.
Studies were excluded if their population included pediatric patients, animal studies, or virtual 3D participants only. Interventions involving chin augmentation other than chin implant, for example sliding genioplasty, were not included. Studies that did not report on rates of complications were not included. Studies designed as a single case report, letter to the editor, or expert opinion were not included. Non-English or non-French studies were not included.
Data Extraction Strategy
Qualitative and quantitative data necessary for analysis were obtained from each study. One reviewer extracted the data using an excel template which was then carefully reviewed by a second reviewer. Where conflicting results were obtained, this was resolved with discussion among the 2 reviewers. Information on study author, date, location, design, patient demographics, approach to implantation, material of implant, type of fixation, follow-up periods, type and rates of complications, and use of perioperative antibiotics was extracted and entered into an excel template.
Outcome Measures
The primary outcome measure was total complication rate. The secondary outcome measures were specific complication rates including infection, seroma, implant extrusion, wound dehiscence, hypoesthesia, misposition of implant, and number of revisions.
Ethics Approval
Ethics approval was not required as the data in this review were collected and synthesized from previously conducted trials. All data are anonymous. There are no other ethical considerations. There are no conflicts of interest for any authors.
Results
Study Selection
The initial search strategy found 1410 articles. Based on title and abstract review, 1293 articles were eliminated, and the remaining 117 were read in full by both reviewers. A further 79 articles were eliminated because they did not contain the necessary information for this systematic review. In total, 38 articles were included. See Figure 1 for search strategy results. 9
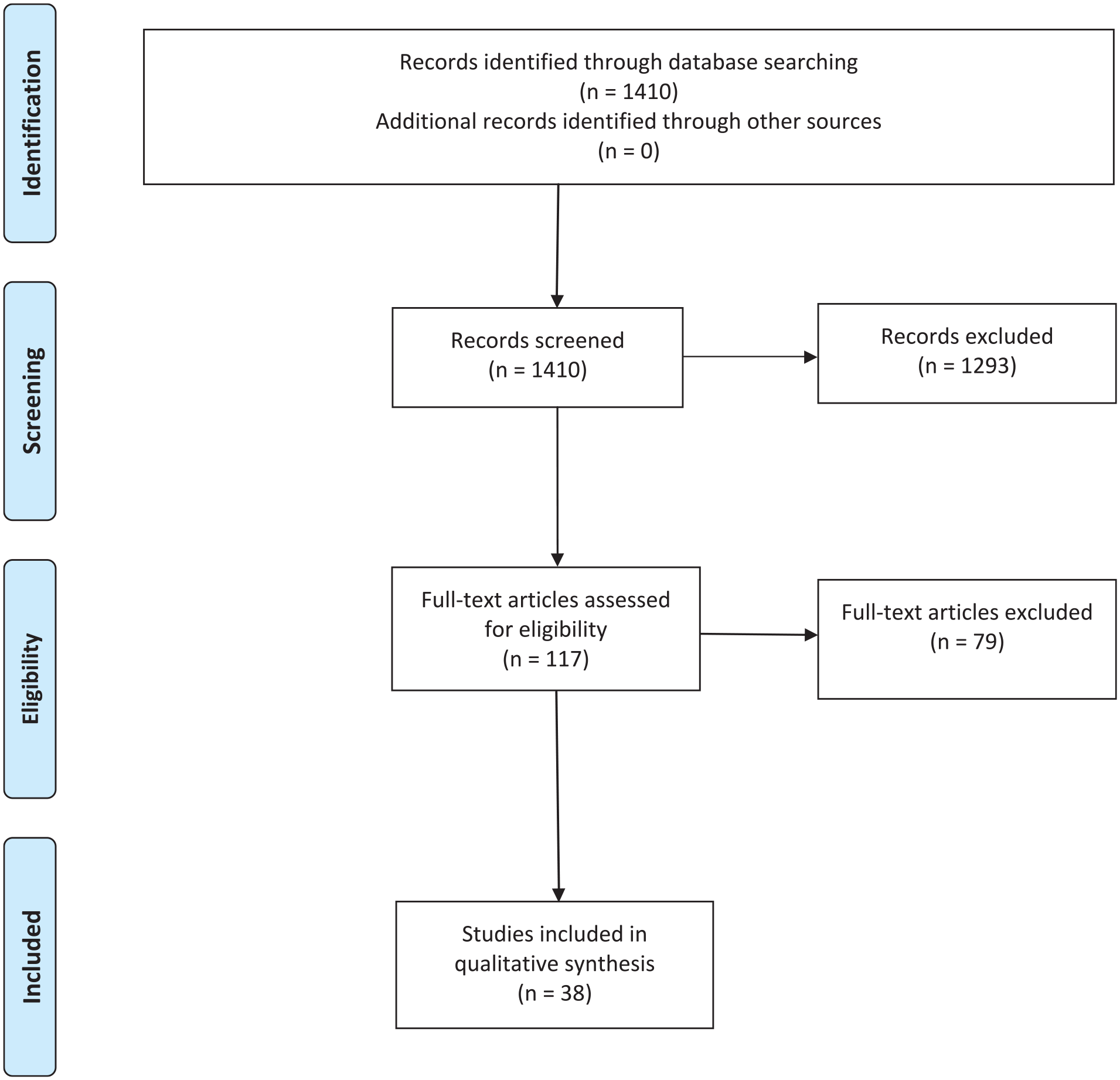
PRISMA diagram.
Study Characteristics
There were no randomized controlled trials available for review. There were 2 prospective cohort studies. All other studies were either retrospective reviews, consecutive case series, or unspecified.
Study Results
In 20 of the studies, the transoral approach was used.10-29 In 15 studies, plus our center’s data set, the submental approach was used.7,30-43 In 3 studies, their experience with both transoral and submental approaches was described.4,44,45 The results are described in Tables 1 to 3.
Studies Using Transoral Approach.
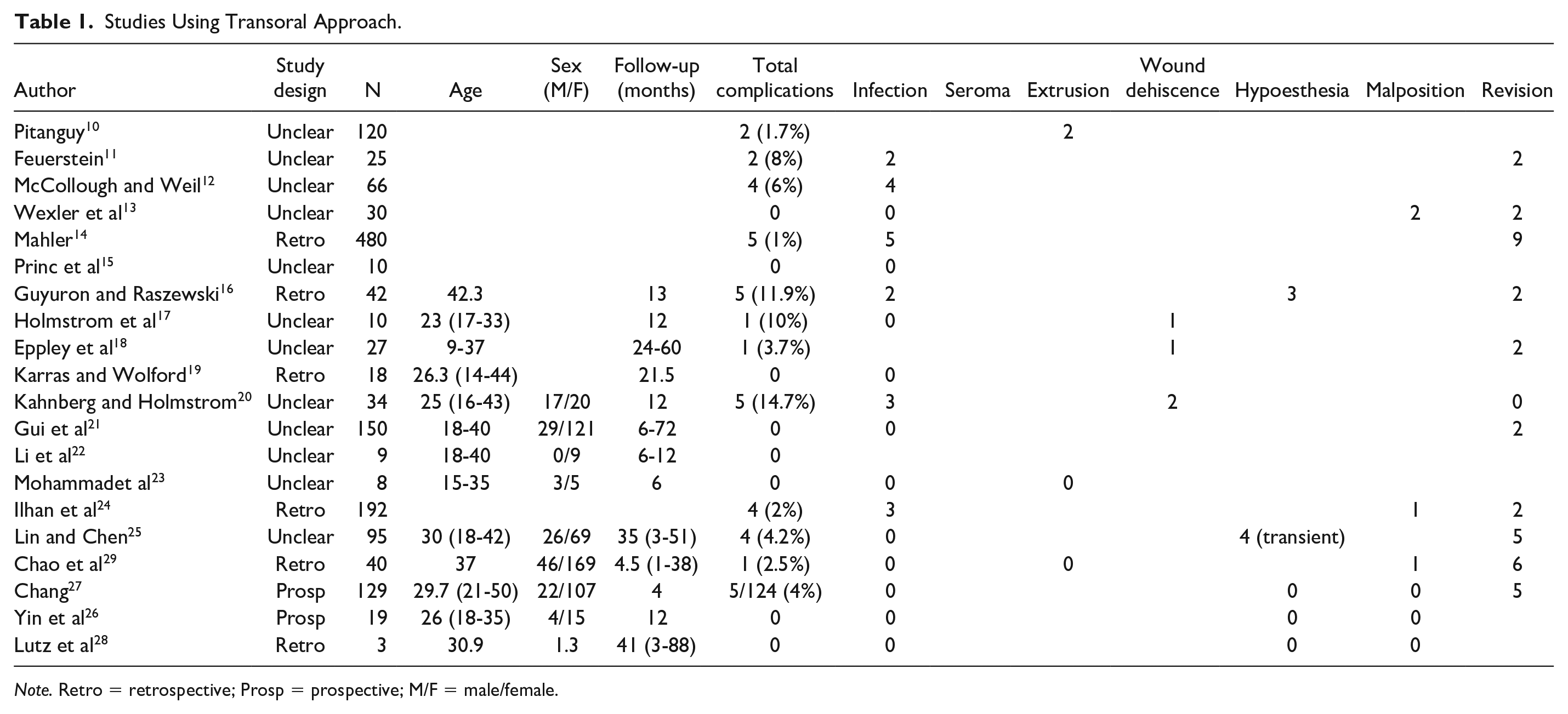
Note. Retro = retrospective; Prosp = prospective; M/F = male/female.
Studies Using Submental Approach.
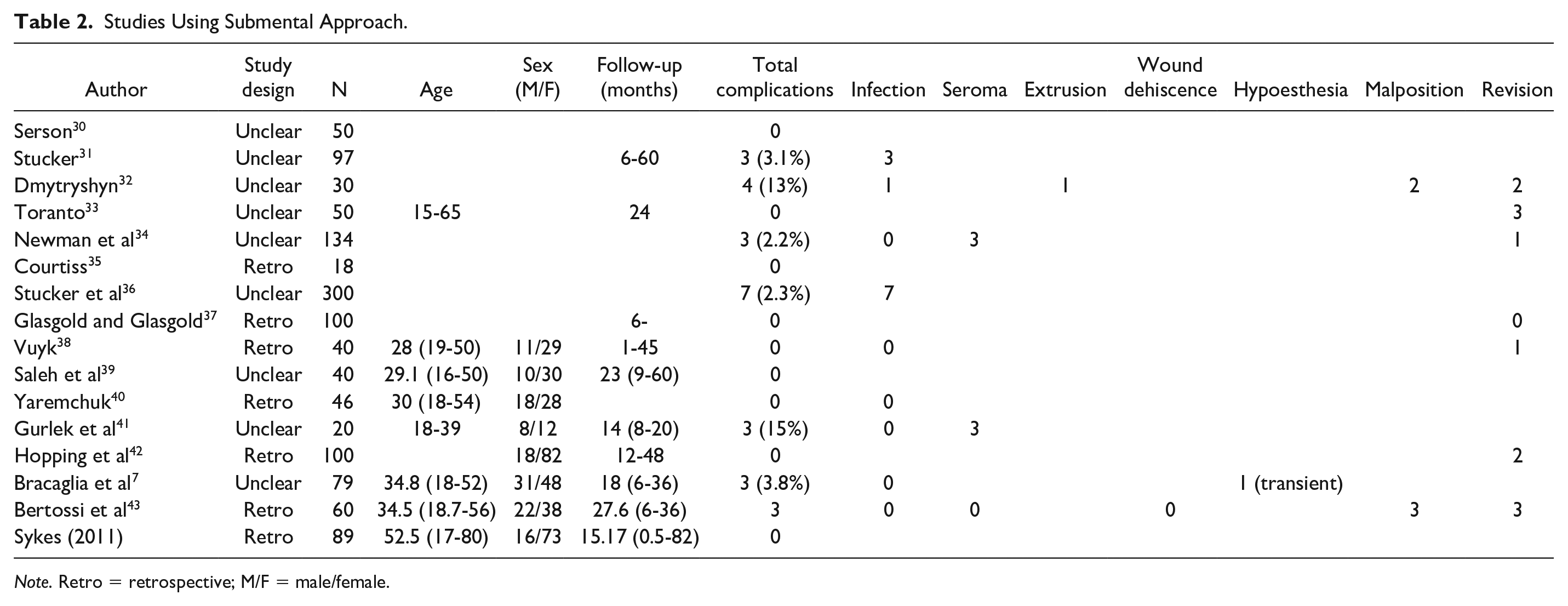
Note. Retro = retrospective; M/F = male/female.
Studies With Both Transoral and Submental Approach.
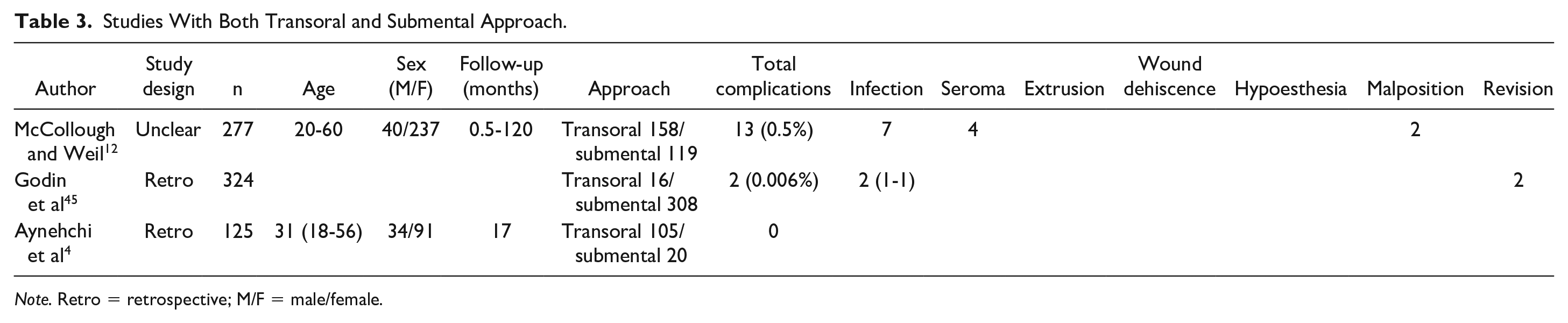
Note. Retro = retrospective; M/F = male/female.
Materials used for the implants primarily included silicone, Medpor, and hard tissue replacement polymer. Materials used more rarely included Gore-Tex, hard acrylic, Mersilene mesh, prolene mesh, Marlex, and diced polyethylene. If described, methods of fixation most often included suture fixation or the use of titanium screws.
Total complication rates in the transoral group ranged from 0% to 14.7%. Total complication rates in the submental group ranged from 0% to 15% (Table 4). The reported rates of total complications, infection, seroma, extrusion, wound dehiscence, hypoesthesia, implant malposition, and revision are shown in Tables 1–3.
Summary of Complication Rates by Surgical Approach.

Discussion
Chin implantation is a procedure with a longstanding history of great results and patient satisfaction which continues to be a very commonly performed procedure. Its utility on its own or as a compliment to other facial surgery procedures such as rhinoplasty, rhytidectomy, or submentoplasty makes it a great procedure for enhancement of facial harmony.
In this study, we conducted a thorough scientific systematic review of current available literature from 1966 to 2020. From direct analysis of the articles meeting our inclusion criteria, we have found that no clear evidence exists to indicate that the intraoral approach to chin implants is inferior or superior to the submental (external) approach. Both approaches have been shown to produce reliable results with low complication rates.
The literature does not seem to suggest higher rates of any of the usual complications attributed to each approach to chin implants in one group or the other. Namely, this review of the published data on the transoral approach does not show higher rates of asymmetry, malposition, infection, extrusion, mental nerve dysfunction, or chin ptosis when compared with the submental approach.
Although there has not yet been a systematic review published on the approaches to chin implantation, there has been one comparing the type of implant material used. A systematic review performed in 2018 by Rojas et al 46 compared silicone and Medpore implants in facial augmentation. This study included all locations (malar, chin, mandible, nose, ears, temporal fossa, frontocranial, and orbit) and compared associated complications for silicone versus Medpore implants. The average total complication rate in chin augmentation was 1% with silicone implants and 3.3% with Medpore implants. 46 The study by Rojas et al did not compare approach to implantation and did not report on complication rates for transoral versus transcutaneous approaches.
Unfortunately, we have no randomized prospective studies examining outcomes in chin implantation. As such, a systematic review of the literature will provide us with the most evidence-based approach to recommendation for surgical approach.
In this systematic review, we have found that both techniques remain valid and safe approaches to chin implantation. This is consistent with the general consensus of the surgical community. Individual analysis of each patient remains the best method of approach to that particular patient’s procedure. For example, when chin implants are done along with submentoplasty, an open approach is most often appropriate. In the setting of patients with a history of poor skin scarring including keloid or hypertrophic scars, the intraoral approach would be most appropriate. Surgeon preference and comfort with approach to the procedure will remain one of the most common reasons for the choice of one approach to another. There are many factors that can affect surgeon preference. The individual surgeon’s experience and comfort level with either surgical approach may reflect initial by approach taught during training. The surgeon’s level of tolerance for external scarring, or perceived risk of infection rate, may play a role. Other factors that may contribute but were not accounted for in this study include the status of the patient’s oral hygiene, smoking, and medical comorbidities like diabetes mellitus. A randomized controlled trial comparing approaches would be the gold standard.
Conclusion
In summary, this systematic review found that both submental and transoral approaches to chin implantation remain valid and safe approaches. This systematic review provides clinical equipoise for performance of a randomized controlled trial to directly compare the external to the intraoral approach to chin implantation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.