
Abstract
The objective of this study was to characterize the associations between light exposure in the free-living environment and multiple dimensions of sleep health of typically developing adolescents. Fifty-six (29 girls, 27 boys) typically developing adolescents (mean age = 13.59, SD = 0.89, range = 12-17 years) participated. For six consecutive nights, sleep was assessed in the home environment using actigraphy. During the same period, participants were asked to fill out a daily sleep log and a daily light exposure log, and to complete questionnaires regarding their alertness and subjective sleep satisfaction. Longer self-reported exposure to daylight in the morning was associated with longer objectively measured sleep duration. Longer self-reported exposures to electronic devices in the evening were associated with later objectively measured sleep onset and offset times, shorter sleep duration, and greater day-to-day sleep variability. Longer morning exposure to outdoor light was associated with a longer sleep duration. Self-reported light exposure was not associated with sleep satisfaction, alertness/sleepiness, or sleep efficiency. Among the covariates, circadian preference accounted for the highest percentage of variance. Adolescents’ sleep health is associated with the self-reported duration of exposure to daylight in the morning and to electronic devices in the evening.
Good sleep health, which is characterized by subjective satisfaction, appropriate timing, adequate duration, high efficiency, and sustained alertness during waking hours (Buysse, 2014), exerts key positive effects on adolescents’ physical health (Simon et al., 2021), mental health (Dong et al., 2019; Fuligni et al., 2018), and daytime functioning (Dong et al., 2019; Fuligni et al., 2018). Healthy sleep is achieved and maintained in daily life through an ongoing interaction between a homeostatic process that regulates sleep duration and depth, and a circadian process that uses environmental time-givers to align sleep timing and alertness with the 24-h day-night cycle (Allada et al., 1998; Blau and Young, 1999; Czeisler et al., 1986; Ebadi and Govitrapong, 1986; R. Y. Moore, 1999). Sleep health among typically developing adolescents is generally poor (Crowley et al., 2018). Since poor sleep health influences adolescents’ cognition, mental health, and physical health, it is important to identify, characterize, and seek to optimize real-world factors that are associated with adolescents’ sleep health.
Typically developing adolescents in the free-living environment are exposed to light daily. Light is an environmental cue that is used by the circadian timing system to shape the sleep-wake cycle (Dautovich et al., 2019; Mistlberger and Skene, 2005; R. Y. Moore and Silver, 1998). Light exposure that is poorly timed and/or insufficient in its amount or duration can result in circadian rhythms that are desynchronized from the light-dark cycle (Gronfier et al., 2007; Middleton et al., 2002). This, in turn, shapes other aspects of sleep health, such as sleep duration, daytime alertness, and sleep satisfaction. Light exposure may be particularly disruptive to adolescents’ sleep health due to an increased sensitivity of their circadian system in response to light in general (Crowley et al., 2015; Crowley et al., 2018) and to short wavelength light in particular (Crowley et al., 2015; Nagare et al., 2019). Moreover, due to the slowed accumulation of homeostatic sleep pressure in adolescents (Jenni et al., 2005), they are able to tolerate longer waking episodes, which increases their exposure to light during times when the circadian system is most sensitive to light (Crowley and Eastman, 2017). Such exposure and adolescents’ delayed sleep are likely bidirectionally associated such that delayed sleep contributes to shorter exposure to daytime light or longer and poorly timed exposure to artificial light which further delays adolescents’ circadian clock (Skeldon et al., 2017).
A small number of studies have examined the associations between light exposure in the free-living environment and adolescents’ sleep health. Studies examining the associations between exposure to light-emitting electronic devices at night and the sleep health of typically developing adolescents have yielded mixed findings. Some reported that such exposure was associated with shorter (Baiden et al., 2019; Bartel et al., 2019; Mireku et al., 2019; Perrault et al., 2019; Stine et al., 2021) or delayed (Bartel et al., 2019; Mireku et al., 2019; Perrault et al., 2019) sleep, while some (Belmon et al., 2021; da Costa et al., 2021; Gumport et al., 2021) found no such association (for a review, see Gruber and Gauthier-Gagné, 2022). Other studies found that longer exposure to sunlight during the day was associated with a longer sleep duration (Baradaran Mahdavi et al., 2020; Zheng et al., 2019), higher levels of artificial light at night were associated with a later weeknight bedtime, and lower levels of artificial light at night were associated with a longer weeknight sleep duration (Paksarian et al., 2020). These studies were useful, as they highlighted the importance of assessing the associations between sleep health and adolescents’ exposure to light. However, their contribution was limited because they did not record simultaneous exposure to electronic devices and other sources of artificial light at night (Weaver et al., 2010), and did not integrate data from adolescents’ light exposure during the day and night (Yang et al., 2010). Daytime exposure to bright light could decrease the magnitude of the circadian response to light exposure in the evening of the same day (Chang et al., 2011; Hébert et al., 2002; Rufiange et al., 2007). In addition, none of the previous studies examined the associations between such light exposure and the multiple dimensions comprising sleep health.
The objective of this study was to characterize the associations between light exposure in the free-living environment on school and weekend days and the multiple dimensions of sleep health of typically developing adolescents. It was hypothesized that: (1) longer exposure to daylight in the morning would be associated with earlier sleep onset and offset timing, longer sleep duration, higher levels of sleep efficiency, smaller day-to-day sleep variability, lower daytime sleepiness, and higher subjective sleep satisfaction; and (2) longer and later exposure to artificial indoor light and to electronic devices in the evening would be associated with later sleep onset and offset times, shorter sleep duration, lower sleep efficiency, greater day-to-day sleep variability, higher daytime sleepiness, and lower subjective sleep satisfaction.
Materials and Methods
Participants
Fifty-six (29 girls, 27 boys) typically developing adolescents (mean age = 13.59, SD = 0.89, range = 12-15 years) participated in the study (4 in wintertime, 52 during springtime). Participants were excluded from the study if they had any psychiatric illness, medical condition, or medication that might interfere with sleep. Demographic characteristics of the sample are presented in Table 1.
Demographic characteristics of the sample.
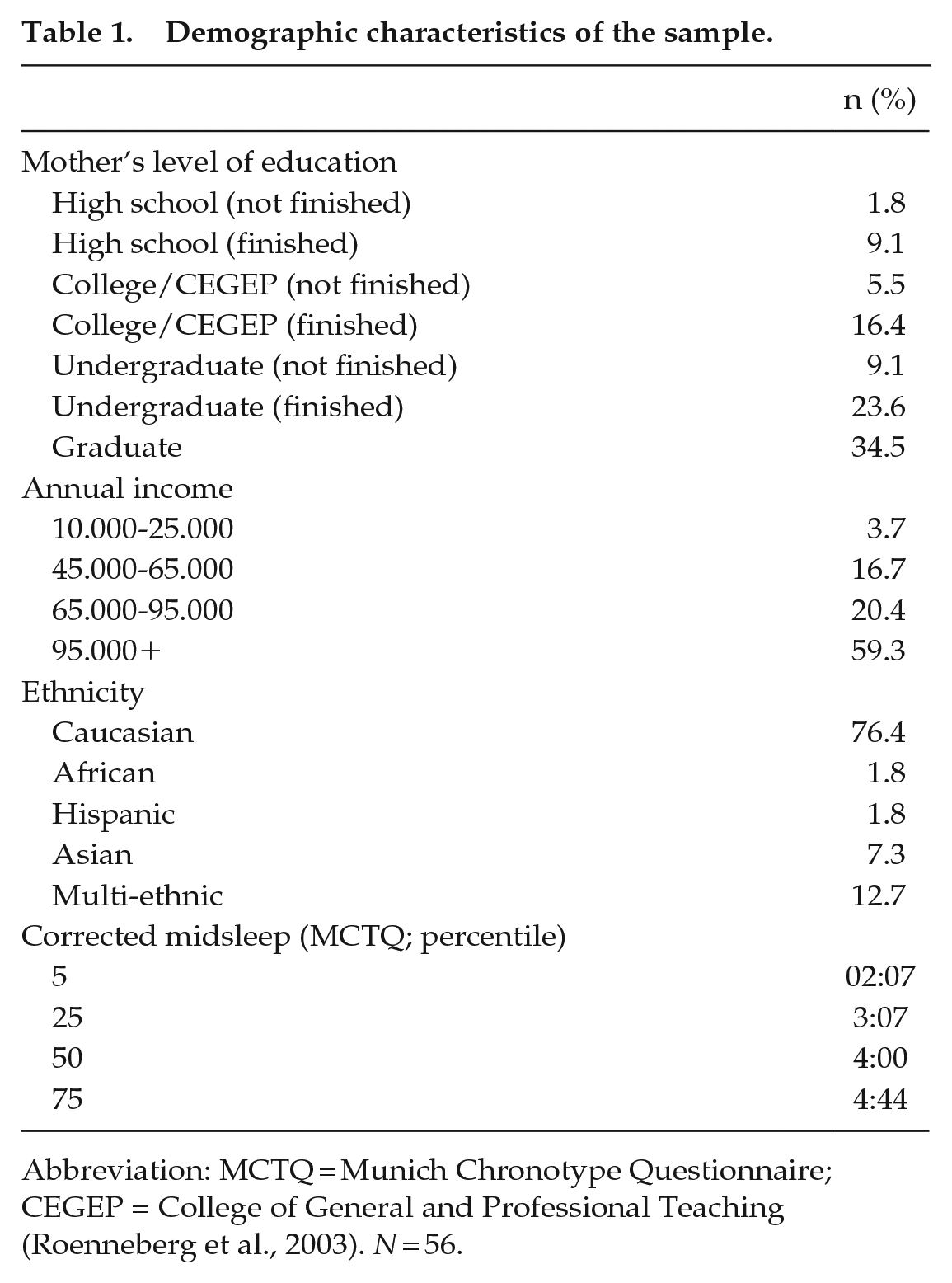
Abbreviation: MCTQ = Munich Chronotype Questionnaire; CEGEP = College of General and Professional Teaching (Roenneberg et al., 2003). N = 56.
Procedure
Each participant’s eligibility was determined through detailed health-related questionnaires completed by the parents. Eligible participants were each given a wristwatch-like actigraph device (Actiwatch 64, Mini-Mitter, Bend, OR, USA) and were instructed to wear it on their nondominant wrist at bedtime for six consecutive nights spanning four school nights and two weekend nights during a typical school week. During the same period, participants were also asked to fill out an electronic daily sleep log with information regarding their bedtimes, time attempted to sleep, final awakening time, and a daily light exposure log. Participants were also asked to complete questionnaires regarding their typical alertness during daytime situations in recent times and regarding their sleep satisfaction in the past month. To reduce recall bias or missing data, the information was collected twice a day, once in the morning at 0800 h and once in the evening at 2000 h. The log administered in the morning asked participants to report on the sleep and light exposure of the previous evening. The log administered in the evening asked participants to report on their light exposure throughout the day. Personalized reminders were sent to encourage participants to complete their log. Parents were asked to provide demographic information. Each participant and their parent gave written assent and consent, respectively, to participate in the study. The study was approved by the Research Ethics Boards of Douglas Mental Health University Institute (Montreal, Canada, approval number: IUSMD-09-12) and the Riverside School Board (Quebec, Canada).
Measures
Sleep Health
Sleep health was operationalized based on a current definition (Buysse, 2014). Sleep regularity, timing, duration, and efficiency were measured using actigraphy, and sleep satisfaction and alertness were measured using validated self-reports (Buysse et al., 1989; Janssen et al., 2017).
Actigraphy
A wristwatch-like device called an actigraph (AW-64 series, Mini-Mitter, Sunriver, OR, USA) was used to evaluate sleep by measuring movement. One-min epochs were used to record actigraphic sleep data. Actigraphy has been shown to be a reliable method for evaluating sleep in adolescents (Acebo et al., 1999; Sadeh et al., 1995). The Actiware Sleep 6.1 software (Mini-Mitter, Sunriver, OR, USA) was used to score sleep. This software package applies a sleep-scoring algorithm that was previously validated and found to display a high degree of correspondence with polysomnographic data (Quante et al., 2018). The actigraphic data were analyzed in 1-min epochs. The total number of activity events was computed for each epoch; if the threshold sensitivity value of the mean score during the active period was exceeded, the epoch was considered to be waking in nature. Otherwise, the epoch was considered to be in sleep. Time attempted to sleep and final awakening time (provided by sleep logs) were considered when determining rest intervals to score actigraphic data. Sleep onset and sleep end (offset) were calculated by the software. The utilized measures included (1) sleep regularity, which was the intra-individual variability of sleep onset, sleep offset, and sleep duration; (2) sleep timing, which was the sleep start and sleep end times; (3) sleep efficiency, which was the percentage of time attempted to sleep spent sleeping; and (4) sleep duration, which was the sum of epochs between sleep onset and sleep offset that were scored as “sleep” according to the Actiware algorithm.
Alertness/Sleepiness
The ability to maintain wakefulness or to fall asleep during daytime situations was measured using the Epworth Sleepiness Scale for Children and Adolescents (ESS-CHAD; Janssen et al. (2017)). Respondents rated their usual chances of dozing off or falling asleep as they engaged in eight daily activities in recent times. Each item is rated on a 4-point Likert-type scale (0-3). The sum of the eight situational sleep propensities provides a measure of daytime sleepiness. A score >10 indicates excessive daytime sleepiness. The internal consistency of the ESS-CHAD was reported to be satisfactory among pediatric populations 12 to 18 years old, ranging between 0.70 and 0.75 (Anderson et al., 2009; M. Moore et al., 2009).
Sleep Satisfaction/Quality
Subjective assessment of “good” or “poor” sleep was obtained using the Overall Sleep Quality component of the Pittsburgh Sleep Quality Index (PSQI; Buysse et al., 1989). This is a single item that asks participants to select the answer that represents their overall sleep quality during the past month from four options ranging between 0 (very good) to 3 (very bad). The scale has adequate psychometric properties for use with community-based adolescents (Raniti et al., 2018).
Light
Light exposure was assessed using a light log. Participants were asked to report for each hour their indoor light exposure (lights-on, only a small light on, lights-off, not inside), outdoor light exposure (yes, no), and electronic device use (yes, no) during each day of the study. Outdoor light exposure data were recoded as 1 for hours reported as being outside and 0 for hours reported as not being outside. Indoor bright light exposure was recoded as 1 for hours reported to have “lights-on” and 0 for hours reported to have “lights-off” or “only a small light on.” This distinction has ecological validity within natural environments, as individuals are able to discern whether they are being exposed to low or bright light (Thieden et al., 2006). Electronic device data were recoded as 1 for each hour in which any device was used and 0 if no device was reported as being used. Weekday (Monday-Friday) and weekend (Saturday-Sunday) means were calculated. The indices utilized in this study included weekday and weekend means of (1) duration of exposure to morning outdoor light between 0600 h and 1400 h; (2) duration of exposure to bright indoor light between 1800 h and 0000 h; and (3) duration of exposure to electronic device(s) between 1800 h and 0000 h. These time blocks were chosen based on average sleep onset times in the current sample given the proximity of light exposure to the sleep period has the potential to shift its timing: Light exposure in the beginning of the night can delay the sleep period, whereas light exposure at the end of the night or in early morning can advance the sleep period (Minors et al., 1991).
Covariates
Chronotype
The Munich Chronotype Questionnaire (MCTQ; Roenneberg et al., 2003) was used to assess participants’ diurnal preferences to control for the potential confounding effect of inter-individual variation in midsleep on the association between light exposure and sleep health. The MCTQ calculates the participants’ chronotype, which is defined as the midpoint time between sleep onset and offset on free days, corrected for oversleep on free relative to scheduled days. The scale has been validated against objective and subjective measures of sleep and circadian rhythm and has been found to be a reliable behavioral marker for circadian phase (Terman et al., 2001).
Demographic and Health Information
Demographic information regarding each participant’s age, gender, ethnicity, health, and socioeconomic status (SES) was collected through a detailed background questionnaire.
Data analysis: Descriptive statistics were computed for the demographic characteristics, sleep health, and weekly light exposure of the sample. In addition, analyses were conducted to determine the percentage of adolescents receiving sleep of insufficient (<8 h), recommended (8-10 h), or long (≥ 10 h) sleep duration and the percentage exhibiting the recommended (>85%) or less than recommended (<85%) sleep efficiency (Hirshkowitz et al., 2015; Paruthi et al., 2016).
Principal components analyses (employing Varimax rotation) were used to reduce the number of variables and aggregate sleep regularity and sleep timing measures into reliable indices. The interpretation and labeling of each component were based on loadings of 0.6 or higher.
Because age, gender, SES, season, and chronotype (Blair et al., 2012; Buckhalt et al., 2007; Sadeh et al., 2000) have been shown to affect sleep health (Blair et al., 2012), we examined their association with the sleep health indices to determine which covariates should be adjusted for in our regression analyses. The objective was to choose the fewest pre-specified factors that could be related to the dependent variables of interest.
To identify potential gender differences in sleep health measures, multiple analysis of variance (MANOVA) was used, with child gender and sleep dimensions as the dependent variables.
To identify potential differences in weekdays and weekend light exposure, paired t tests were used comparing each participant’s weekdays and weekend mean exposure to daylight, bright light in the evening, and electronic device use in the evening.
To determine the potential associations between season and sleep dimensions, an additional analysis of variance (ANOVA) was run with season of data collection as the between-subjects factor and sleep dimensions as the dependent variables. Spearman rank correlations were used to examine potential associations between SES or midsleep time and sleep health dimensions.
To test whether light exposure in the free-living environment accounted for any unique variance in adolescents’ sleep health after we removed the contributions of control variables, separate hierarchical multiple regression analyses were performed on each sleep health measure. Each regression took the same form, with demographic characteristics (age, gender, circadian preference) entered in the first step and weekday or weekend light exposure (mean durations of bright morning outdoor light exposure, bright evening indoor light exposure, and evening electronic device exposure) added in the second step.
All assumptions of regressions were confirmed prior to analyses. Normality of the residuals was confirmed using the Shapiro-Wilk test (p > 0.05). Collinearity was found to be within acceptable limits, with all variance inflation factor (VIF) values < 2.
All analyses were performed using SPSS Version 24.0 for Windows, and a p value of < 0.05 was considered to indicate statistical significance.
Results
Sample Characteristics
Table 1 shows participants’ demographic data. Table 2 provides descriptive statistics for sleep regularity, satisfaction, alertness, timing and duration, and patterns of weekday and weekend light exposure in the free-living environment.
Sample characteristics.
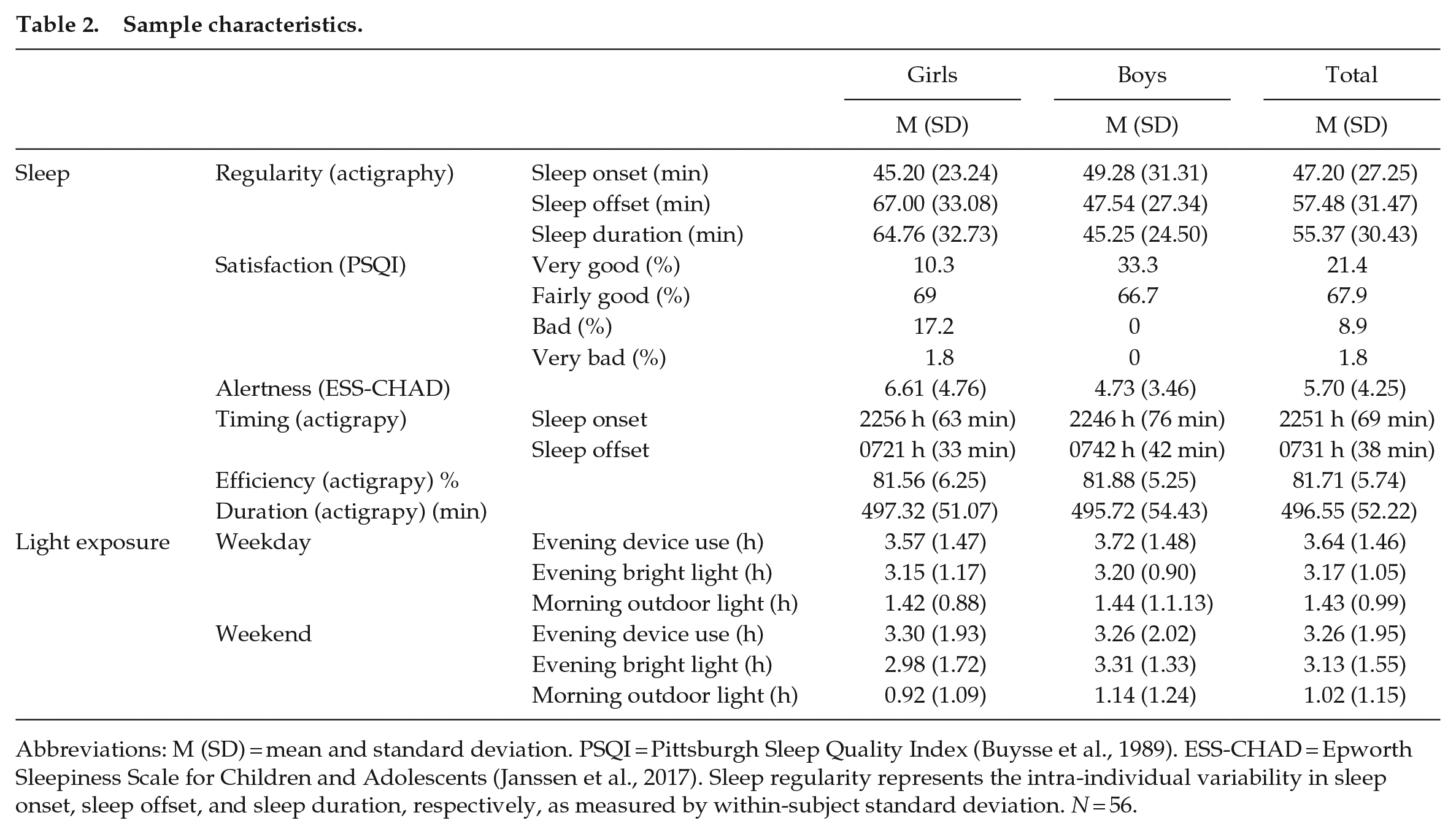
Abbreviations: M (SD) = mean and standard deviation. PSQI = Pittsburgh Sleep Quality Index (Buysse et al., 1989). ESS-CHAD = Epworth Sleepiness Scale for Children and Adolescents (Janssen et al., 2017). Sleep regularity represents the intra-individual variability in sleep onset, sleep offset, and sleep duration, respectively, as measured by within-subject standard deviation. N = 56.
Actigraphic recordings indicated that, on average, the participants slept 496.55 min (SD = 52.22 min) per night. The mean reported bedtime was 2251 h (SD = 69 min) and the mean reported rising time was 0731 h (SD = 38 min). Of the participants, 30.4% obtained less than the recommended amount of sleep, whereas the sleep duration of 69.6% of the participants was within the recommended 8 to 10 h. No participant had sleep duration longer than > 10 h. The mean sleep efficiency score was 81.71% (SD = 5.74%). Of the participants, 71.4% had a sleep efficiency below the recommended level, while 28.6% had a sleep efficiency at or above the recommended 85% level (Ohayon et al., 2017). The average variations in adolescents’ weekly sleep onset, offset, and sleep duration were 47.20 min (SD = 27.25 min), 57.48 min (SD = 31.47 min), and 55.37 min (SD = 30.43 min), respectively. Of the participants, 89.3% indicated their sleep was very good or fairly good and 10.7% indicated it was bad or very bad. The average alertness score measured by the ESS-CHAD was within the normal range (M = 5.70, SD = 4.25).
Across the entire week, adolescents reported an average of 77.56 min of daily exposure to outdoor light (SD = 62.47), 189.71 (SD = 72.39) min of daily exposure to bright light in the evening, and 221.52 min (SD = 91.20) of device use in the evening.
Self-reported evening device use on weekdays (M = 3.64, SD = 1.46) was significantly greater compared with weekend days (M = 3.26, SD = 1.95), t(59) = 2.08, p < 0.04. Self-reported duration of exposure to morning outdoor light was also significantly longer on week days (M = 1.43, SD = 0.99) compared with weekend days (M = 1.02 SD = 1.15), t(53) = 2.06 p < 0.04. There was no significant difference between self-reported exposure to bright light in the evening on week days (M = 3.17, SD = 1.05) compared with the weekend days (M = 3.13 SD = 1.55), t(59) = 0.67 p > 0.05.
Four participants were removed from the analysis because outdoor light data were not provided, M (SD) age = 13.75 (0.5); three male, one female. A linear interpolation method was applied to infer missing values. The demographic features did not differ between youth with complete (n = 52) versus partially imputed (n = 4) data.
Factor Analyses
Regularity
Principal components analysis using Varimax rotation produced a one-factor solution for the actigraphy-measured day-to-day variability in sleep onset, sleep offset, and sleep duration (Table 2). The factor accounted for 56.76% of the variance. It was weighted by all three regularity measures and was therefore termed “regularity.”
Timing
Principal components analysis using Varimax rotation produced a one-factor solution for the weekly averages of actigraphy measures for sleep onset and sleep offset (Table 2). The factor accounted for 74.80% of the variance. It was weighted by sleep onset and sleep offset and was therefore termed “timing.”
Analyses of Potential Confounding Variables
Gender
MANOVA revealed that girls had higher PSQI sleep quality scores than boys (girls: M = 1.14, SD = 0.65; boys: M = 0.65, SD = 0.48; F1,52 = 9.68, p = 0.03) and woke up earlier (girls: M = 7.21, SD = 33; boys: M = 7.42, SD = 42; F1,56 = 4.25, p = 0.04).
Season
No significant difference was found in the sleep health measures between adolescents who participated in the study during winter or spring.
Chronotype
Spearman correlations revealed that there were significant associations between adolescents’ chronotype and their sleep regularity and sleep duration (r = 0.40, p = 0.00; r = –0.31, p = 0.02, respectively).
Age
Spearman correlations revealed that there were significant associations between adolescents’ age and sleep start time (r = 0.27, p = 0.05).
SES
No significant association was found between the sleep measures and the annual income ranges of participants’ families or their mothers’ level of education.
Based on the above findings, we adjusted for gender, age, and chronotype in our regression analyses.
Tables 3 and 4 show the results of hierarchical multiple linear regression analyses performed using each of the sleep health dimensions as the dependent variable for the week and weekend.
Hierarchical regression of covariates and self-reported light exposure during the weekdays.
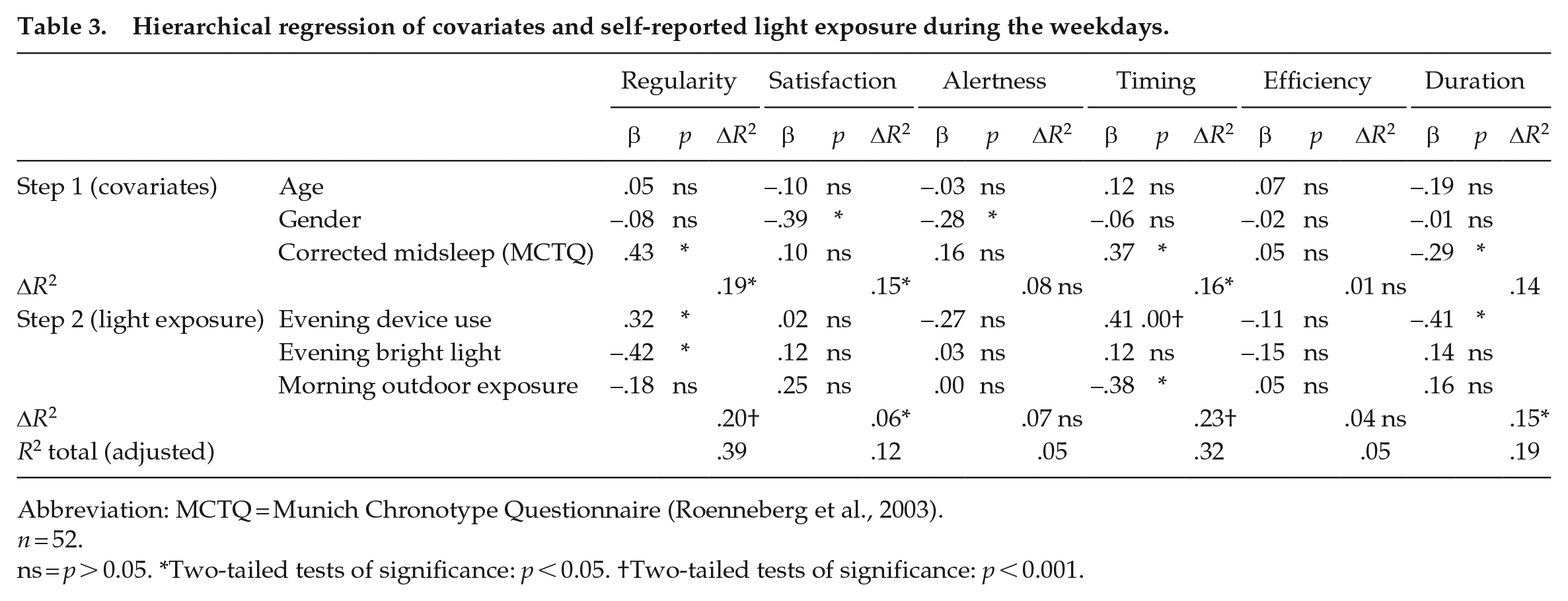
Abbreviation: MCTQ = Munich Chronotype Questionnaire (Roenneberg et al., 2003).
n = 52.
ns = p > 0.05. *Two-tailed tests of significance: p < 0.05. †Two-tailed tests of significance: p < 0.001.
Hierarchical regression of covariates and self-reported light exposure during the weekend.
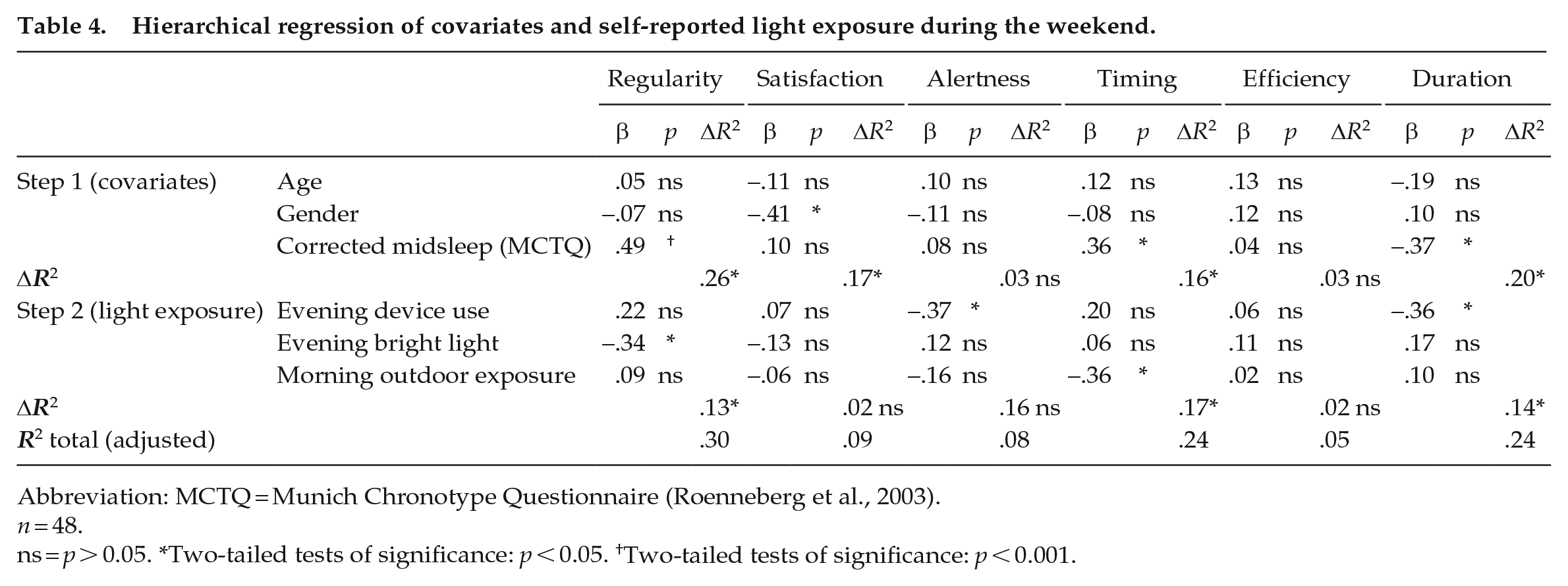
Abbreviation: MCTQ = Munich Chronotype Questionnaire (Roenneberg et al., 2003).
n = 48.
ns = p > 0.05. *Two-tailed tests of significance: p < 0.05. †Two-tailed tests of significance: p < 0.001.
Sleep Regularity
Sleep regularity and weekday light exposure: Step 1 was significant (F3,46 = 3.63, p < 0.02) and control variables explained a significant proportion of the variance. Having a later diurnal preference was associated with lower sleep regularity (higher night-to-night variability of sleep). Step 2 was significant (F6,43 = 4.59, p < 0.00). Longer evening device use and longer exposure to bright light in the evening were associated with lower sleep regularity (higher night-to-night variability of sleep; Figures 1 and 2, respectively). Sleep regularity and weekend light exposure: Step 1 was significant (F3,44 = 5.10, p < 0.00) and control variables explained a significant proportion of the variance. Having a later diurnal preference was associated with lower sleep regularity (higher night-to-night variability of sleep). Step 2 was significant (F6,41 = 4.37, p < 0.00). Longer exposure to bright light in the evening was associated with lower sleep regularity (higher night-to-night variability of sleep; Figure 3).
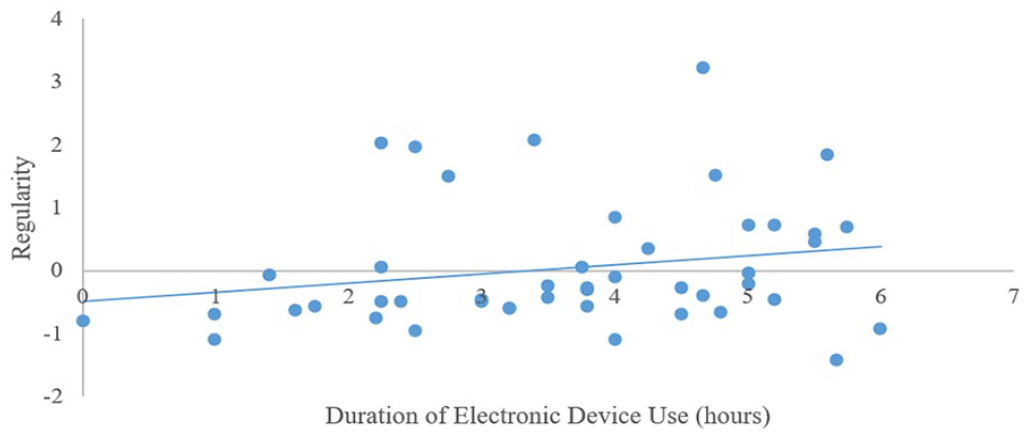
Associations between self-reported weekday electronic device use in the evening and objectively measured sleep regularity in typically developing adolescents.
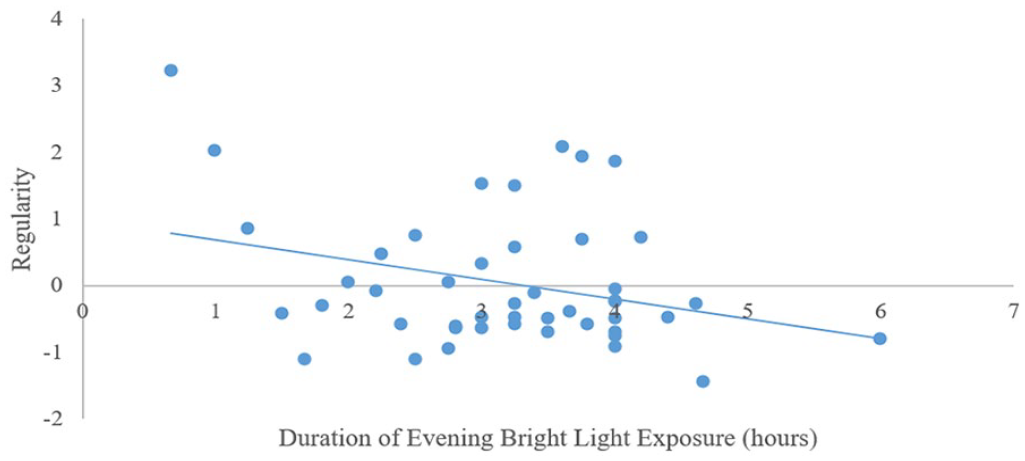
Associations between self-reported weekday bright light exposure in the evening and objectively measured sleep regularity in typically developing adolescents.
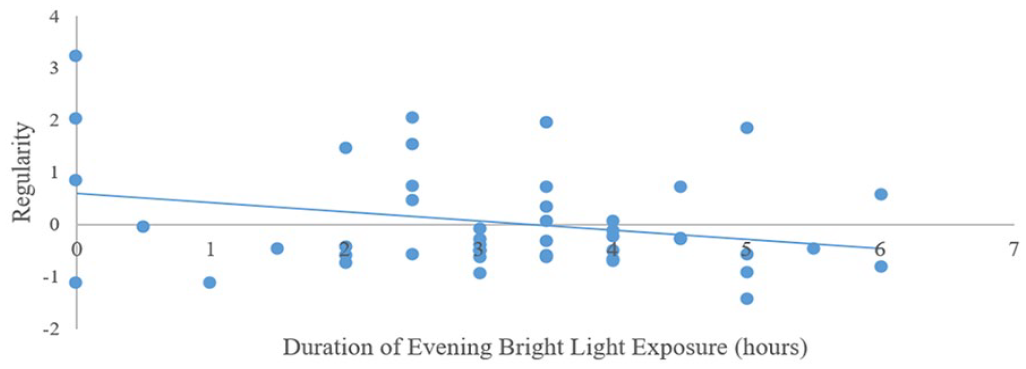
Associations between self-reported weekend bright light exposure in the evening and objectively measured sleep regularity in typically developing adolescents.
Sleep Satisfaction
Sleep satisfaction and weekday light exposure: Step 1 was significant (F3,53 = 3.10, p < 0.03). Being female was associated with significantly lower sleep satisfaction. Step 2 was significant (F6,50 = 2.25, p < 0.05) but none of the independent variables were significantly associated with sleep satisfaction. Sleep satisfaction and weekend light exposure: Step 1 was significant (F3,50 = 3.45, p < 0.02). Being female was associated with significantly lower sleep satisfaction. Step 2 was not significant (F6,47 = 1.87, p < 0.05).
Alertness/Sleepiness
Alertness/sleepiness and weekday light exposure: None of the regression steps were significant (Step 1: F3,53 = 1.58, p > 0.05; Step 2: F6,50 = 1.53, p > 0.05). Alertness/sleepiness and weekend light exposure: None of the regression steps were significant (Step 1: F3,50 = 0.55, p > 0.05; Step 2: F6,47 = 1.80, p > 0.05).
Sleep Timing
Sleep timing and weekday light exposure: Step 1 was significant (F3,53 = 3.42, p < 0.02). Having a later diurnal preference was associated with a later bedtime. Step 2 was significant (F6,50 = 5.37, p < 0.001). Longer evening device use was associated with a later bedtime (Figure 4) whereas longer duration of exposure to morning outdoor light was associated with earlier bedtime (Figure 5). Sleep timing and weekend light exposure: Step 1 was significant (F3,50 = 3.06, p < 0.04). Having a later diurnal preference was associated with a later bedtime. Step 2 was significant (F6,47 = 3.76, p < 0.00). Longer duration of exposure to morning outdoor light was associated with earlier bedtime (Figure 6).
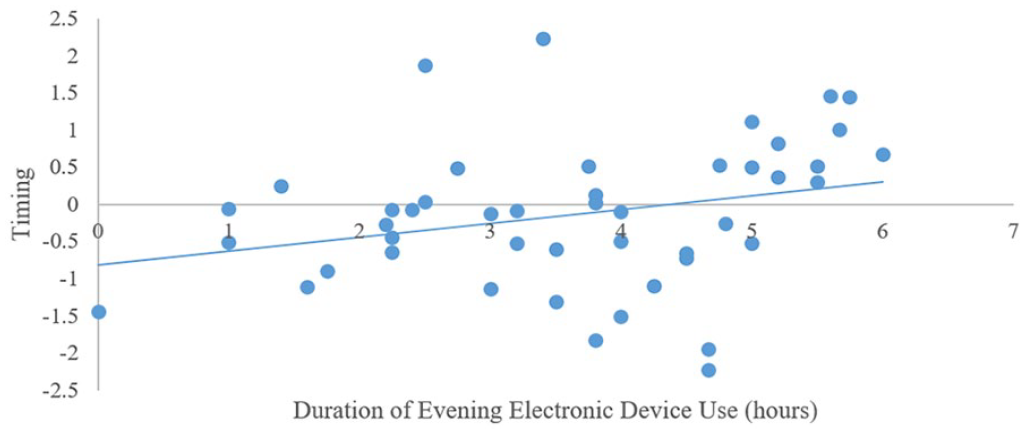
Associations between self-reported weekday electronic device use in the evening and objectively measured sleep timing in typically developing adolescents.
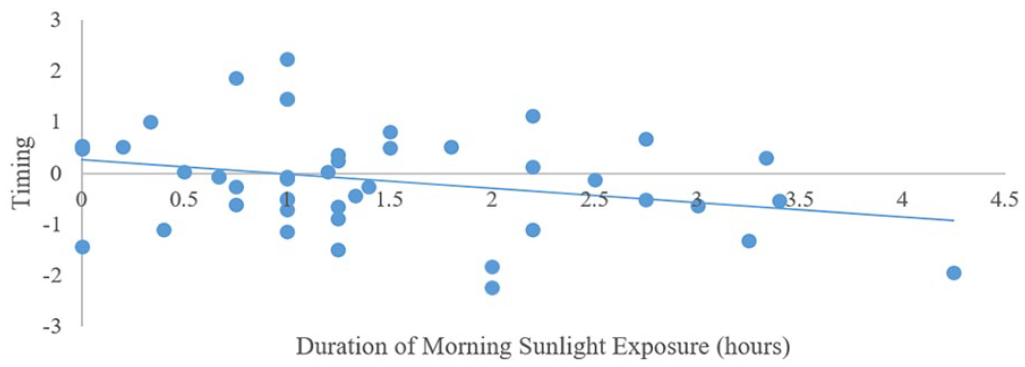
Associations between self-reported weekday sunlight exposure in the morning and objectively measured sleep timing in typically developing adolescents.
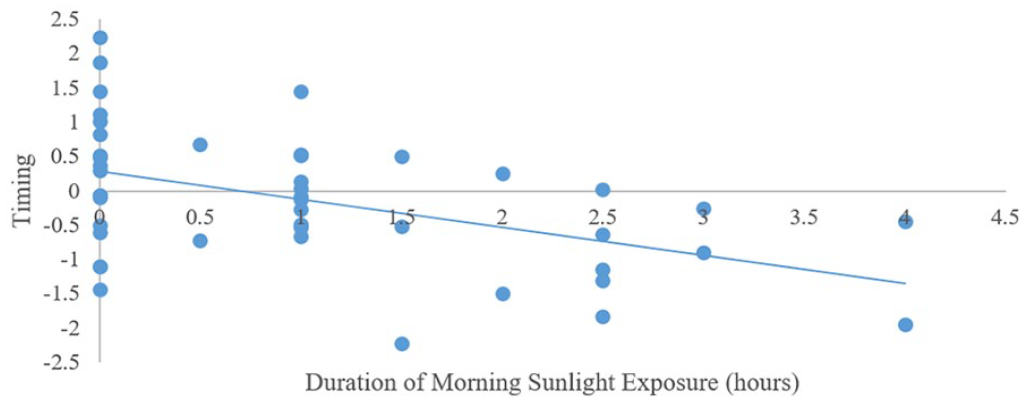
Associations between self-reported weekend day sunlight exposure in the morning and objectively measured sleep timing in typically developing adolescents.
Sleep Efficiency
Sleep efficiency and weekday light exposure: None of the regression steps were significant (Step 1: F3,48 = 0.15, p > 0.05; Step 2: F6,45 = 0.36, p > 0.05) and none of the variables accounted for a significant amount of the variance. Sleep efficiency and weekend light exposure: None of the regression steps were significant (Step 1: F3,45 = 0.48, p > 0.05; Step 2: F6,42 = 0.36, p > 0.05) and none of the variables accounted for a significant amount of the variance.
Sleep Duration
Sleep duration and weekday light exposure: Step 1 was not significant (F3,48 = 2.56, p > 0.05). Step 2 was significant (F6,45 = 3.05, p < 0.01). Longer evening device use was associated with a shorter sleep duration (Figure 7). Sleep duration and weekend light exposure: Step 1 was significant (F3,45 = 3.76, p < 0.02). Later diurnal preference was associated with shortened sleep duration. Step 2 was significant (F6,42 = 3.58, p < 0.01). Longer evening device use was associated with a shorter sleep duration (Figure 8).
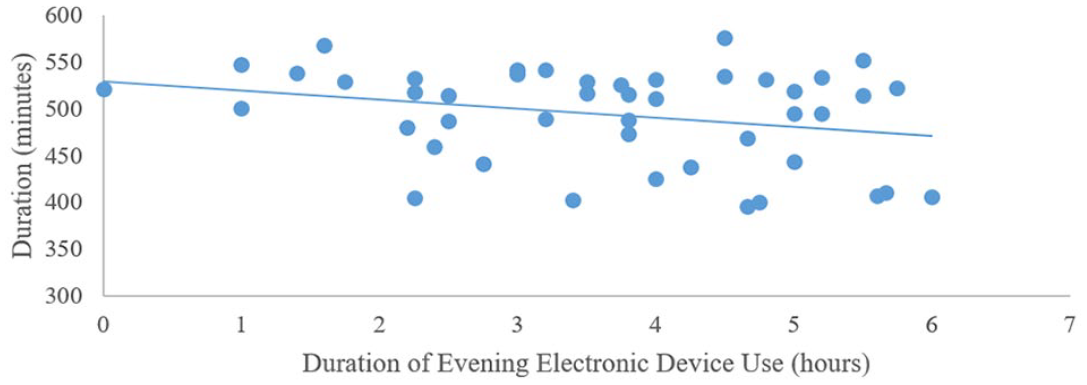
Associations between self-reported weekday electronic device use in the evening and objectively measured sleep duration in typically developing adolescents.
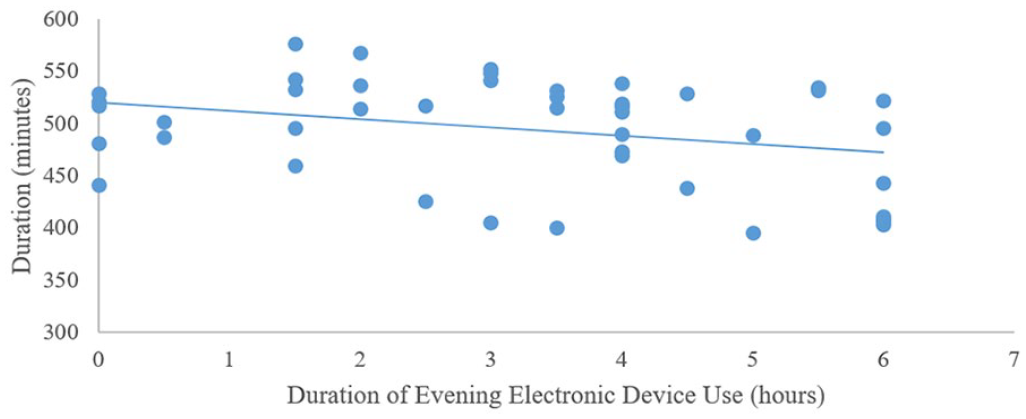
Associations between self-reported weekend day electronic device use in the evening and objectively measured sleep duration in typically developing adolescents.
Discussion
The present study assessed the relationship between self-reported light exposure in the free-living environment and sleep health among typically developing adolescents. The main hypotheses were partially confirmed, in that (1) longer exposure to daylight in the morning on weekdays or weekend days was associated with longer sleep duration; and (2) longer and later exposure to electronic devices in the evening on weekdays were associated with later sleep onset and offset times, shorter sleep duration, and greater day-to-day sleep variability. Longer and later exposure to electronic devices in the evening on the weekend was associated with shorter sleep duration. After we controlled for demographic and individual variables, both weekdays and weekend light exposure were found to account for a substantial proportion of the variance in sleep regularity, timing, and duration (weekdays: 39%, 32%, and 19%, respectively; weekend: 30%, 24%, 24%, respectively).
The duration of device use in the evening was associated with lower sleep regularity (higher intra-individual sleep variability), poorer sleep timing, and shorter sleep duration. Morning exposure to outdoor light during the week was associated with earlier sleep timing. Light exposure was not associated with sleep satisfaction, alertness/sleepiness, or sleep efficiency. Among the covariates, circadian preference accounted for the highest percentage of the variance.
This study extends previous investigations into adolescents’ light exposure in two ways: First, we provide a detailed characterization of daily exposure to outdoor light, bright light in the evening, and device use over consecutive week and weekend days and nights in the free-living environment. Notably, light exposure was logged at times in which light is likely to have the strongest association with the regulation of sleep. Second, we document the associations between light exposure in the free-living environment and each dimension of sleep health.
We found that longer exposure to electronic devices at night is associated with higher levels of variability in sleep timing and sleep duration. This is consistent with the results of previous studies showing associations between electronic device use before bedtime and unhealthy sleep (for a review, see Silva et al., 2022). Irregular sleep-wake schedules may allow for irregular light-dark schedules and vice versa (Phillips et al., 2017; Skeldon et al., 2017). Information about the day-to-day variability in sleep and light exposure is necessary to better understand this relationship in adolescents. The current study measured average light exposure duration across days, rather than day-to-day variability. Thus, it remains unclear whether sleep variability is associated with intra-individual variability light exposure and whether sleep and light regularity are bidirectionally related in adolescents. Future studies should address these gaps to clarify the relationships between variability in sleep and light exposure patterns in typically developing adolescents.
We currently lack a clear understanding of how much variability in sleep timing or duration can be tolerated without negative consequences or the extent to which variable exposure to light may contribute to such consequences. Additional studies examining the associations between sleep regularity, electronic device use, and light exposure are needed to determine the acceptable ranges of night-to-night and day-to-day variability in the sleep and light exposure of an individual.
Our finding of associations between technology use in the evening and shorter sleep and later sleep are consistent with those of previous studies documenting associations between technology use duration and sleep duration. For example, excessive screen time (>3 h/day; Baiden et al., 2019), time spent on portable electronic devices/TV/video games (Komrij et al., 2021; Twenge et al., 2019), and total screen time after 2100 h (Perrault et al., 2019) were associated with a shorter sleep duration. A longer duration of technology use has also been associated with a later bedtime (e.g., Perrault et al., 2019). The present study extends these earlier reports by providing detailed information that was obtained twice daily, in the first and last parts of the day compared with those of the earlier studies that used using retrospective self-reports and could have suffered from a recall bias.
Adolescents’ device use in the evening was longer on weekdays compared with the weekend which could be potentially explained by device use time spent on homework. Future studies would benefit from gathering information related to the purpose of adolescents’ use of electronic devices so that they can distinguish between screen exposure related to schoolwork and other purposes such as gaming or social media.
Studies that used parental reports of screen use in the final hour before bed (Belmon et al., 2021) or ecological momentary assessment of screen use (Gumport et al., 2021) did not find significant associations with adolescents’ sleep duration or bedtime. The findings of the present study, combined with those of earlier studies that used the cumulative duration of technology exposure up to the participants’ bedtime as the key independent variable, suggest that this discrepancy could reflect the omission of electronic device exposure later than 2100 h at night or the failure to document the cumulative duration of electronic device exposure in the evening. Future studies using ecological momentary assessment would benefit from extending and delaying the times of day in which they gather information related to adolescents’ use of electronic devices at night and from measuring the duration of exposure to technology and integrating it to their analysis. Given the delayed schedules of adolescents, such information gathering could potentially be conducted by methods that avoid requiring an interviewer to call participants very late at night. Moreover, when the interviewer uses a direct question, such as “At the moment the phone rang, what were you doing?” (Gumport et al., 2021), some adolescents might feel uncomfortable “admitting” they were using technology. This could bias the results. The methods described herein could be a means to overcome such challenges as while maintaining participants’ responsivity and acquiring complete data sets in 93% of the participants.
Our finding that electronic device exposure at night is associated with a later bedtime is consistent with a recent systematic review (Tähkämö et al., 2019) and findings from a recent study conducted in adolescents with strong evening tendencies (Gasperetti et al., 2021). In these individuals, a later time of last exposure to more than 10 lux was associated with a later bedtime, a later time of sleep onset, and shorter objective and subjective total sleep times.
Light exposure patterns were not significantly associated with adolescents’ daytime alertness/sleepiness.
Light exposure patterns were not significantly associated with sleep efficiency or sleep satisfaction. The sample includes typically developing adolescents with healthy sleep, hence a relatively restricted range of variability in sleep quality and in sleep efficiency which might have limited the study’s ability to capture associations between sleep quality or sleep efficiency and light exposure.
Future research is needed to further investigate these associations and help us better understand how light exposure in the free-living environment may be related to these aspects of sleep health.
Practical Implications
The sleep health of a large proportion of the participants was poor in several domains, including sleep timing, efficiency, and duration. Light exposure was related to sleep timing and duration.
Recent mathematical models quantifying the associations between lighting in the built environment and circadian timing demonstrated that increasing daytime illuminance will narrow the distribution of sleep timing and circadian phase (Papatsimpa et al., 2021). Future sleep health promotion efforts should consider including strategies aimed at increasing daytime illuminance and reducing nighttime illuminance exposure among typically developing adolescents as a strategy to advance their bedtime and extend their sleep duration.
Limitations and Future Directions
The cross-sectional design of this study limits our ability to determine causality. It is possible that adolescents are awake and therefore use electronic devices, that they are awake because they use electronic devices, or that there is a bi-directional process wherein an individual is awake due to evening tendencies, leading to a late exposure to devices that affects their circadian processes (e.g., dim light melatonin onset [DLMO]). Future experimental studies are needed to examine causality and further clarify the impact of light exposure during the day and night, and electronic device use on sleep health.
Another limitation of the study is that it relies on subjective reports of light exposure in the free-living environment rather than light logging devices. As such, there is no objective measure of light timing, intensity, or wavelength. Whereas it would have been ideal to include objective measure to capture adolescents’ light exposure in the real world, the wearable light sensors that currently exist on the market do not contain all information required to estimate the non-visual impact of a light (Webler et al., 2019), and are unreliable in estimating light intensity, with some devices overestimating photopic illuminance by 18% to 152% (Markvart et al., 2015), and spectrum, with several device models having spectral mismatches between 3.3% and 303% across photopic and α-opic sensitivity curves (Price et al., 2017). These limitations are significant given adolescents’ increased sensitivity to light of low intensity (Crowley et al., 2015) and short wavelength (Nagare et al., 2019) such that small measurement errors may exceed levels that can have significant effects on adolescents’ physiology. Furthermore, devices that have been used in a laboratory environment would have significantly limited the value of the data as they would interfere with the ecological validity of the study and with natural sleep and would create significant inconveniences for adolescents. Future studies may be able to use devices that are currently being tested and developed to document objectively adolescents’ daily light exposure in the real world while overcoming methodological barriers.
The study is descriptive and cannot explain the mechanism underlying the observed associations.
Future studies should examine potential mechanisms, such as how the timing of light exposure in the evening, at night, and in the morning affects DLMO and sleep health among adolescents.
In summary, given the lack of data on the type of light to which adolescents are exposed as a result of their daily activities and the environment in which they live, this study fills an important knowledge gap and could inform future research aiming at objective characterization of the interplay between sleep and light exposure in typically developing adolescents.