
Abstract
Understanding the biological rhythms that influence young adult health is vital because the combination of biological changes and a circadian phase delay lead to young adults being at high risk of circadian misalignment. We have previously established a self-rating of biological rhythm disorder for adolescents (SBRDA). However, we did not externally validate the SBRDA against objective measures of biological rhythms such as dim light melatonin onset (DLMO)—the gold standard of the endogenous circadian phase. The purpose of this study was to verify the effectiveness of SBRDA in identifying individuals with biological rhythm disorders. Our participants were 42 (47.2%) boys and 47 (52.8%) girls with an average age of 18.5 ± 1.2 years. Saliva samples were collected from 4 h before bed time to 2 h after sleep every 60 min in a dim-light (<50 lx) laboratory environment. Biological rhythm parameters were assessed using questionnaires, including SBRDA, MEQ, and MCTQ. The mean DLMO time (h) was 22.2 ± 1.9. The DLMO correlated significantly with the SBRDA score (r = 0.33, p < 0.001), MEQ score (r = -0.24, p < 0.05), and MSFsc (r = 0.26, p < 0.05). ROC curve analysis showed that SBRDA was of diagnostic value for biological rhythm disorder (p < 0.05). Our observations demonstrate that SBRDA, which is consistent with MEQ and MCTQ, can be used to reflect endogenous circadian rhythm disorders in young adults. Exposure to dim light may activate melatonin secretion and lead to an earlier peak in young adults with biological rhythm disorder.
Biological rhythms are defined by biological changes repeated in a certain time sequence, such as the sleep/wake cycle, secretion of hormones, and regular food intake (Guan and Lazar, 2021). The physiological processes in the human brain and body are regulated by an endogenous circadian rhythm system that oscillates at approximately 24 h (Logan and McClung, 2019). If the endogenous circadian rhythm system fails to adapt to environmental changes, the ability to regulate internal homeostasis may become impaired. Biological rhythm disorders are implicated in a variety of adverse health outcomes, including mental disorders (Spanagel, 2018; Delorme et al., 2020). Based on a synthesis of the human circadian rhythm literature, varied approaches to the operationalization and analysis of circadian rhythms have been applied. These include objective measures of laboratory testing, such as dim light melatonin onset (DLMO), core body temperature, and sleep timing estimated via actimetry. The human endogenous circadian phase is regulated by a biological clock. According to the commonly accepted understanding of the biological clock, the most reliable and accurate measure of endogenous circadian homeostasis in humans is nocturnal DLMO (Pandi-Perumal et al., 2007; Lewy et al., 1999). Melatonin in saliva, blood, and urine samples can be used to detect DLMO. However, this laboratory testing technique still has limitations that demand the collection of blood or saliva samples at intervals of an hour or half an hour under dim light conditions. It is generally accepted that DLMO typically occurs 2 to 3 h before sleep onset and that melatonin can only be detected in dim light (Burgess and Eastman, 2005; Sletten et al., 2010). Therefore, this technique requires invasive, expensive testing, and it is time-consuming and laborious. The application of DLMO to large sample epidemiological investigations is limited, especially in healthy young adults. Young adulthood is a sensitive and dynamic maturational period that is a cornerstone for future health (Sawyer et al., 2012). Understanding the biological rhythms that influence young adult health is vital because the combination of biological changes and circadian phase delay puts young adults at high risk of circadian misalignment (Sivertsen et al., 2021).
Human circadian rhythms can also be evaluated by subjective measures of questionnaires, such as the Morningness-Eveningness Questionnaire (MEQ) and Munich ChronoType Questionnaire (MCTQ). Internationally recognized and widely used self-report questionnaires (such as the MEQ and MCTQ) have been designed to assess circadian rhythm. Horne and Ostberg were pioneers who compiled the MEQ to assess circadian function, which consists of 19 items divided into subscales for the optimal time of physical and mental phenotypes, habitual wake-up and sleep time, and subjective alertness after getting up and before sleep (Horne and Ostberg, 1976). The MEQ was reduced to 5 items in 1991. The reduced MEQ, which was constructed with 5 items from the full MEQ, exhibited high reliability and was the broadest tool used to describe circadian rhythm (Adan and Almirall, 1991). The MCTQ assessed circadian rhythm with 14 questions integrating sleep and wake time on weekdays and weekends, emphasizing the regularity of people’s work schedules (Roenneberg et al., 2007, 2003). Giglio et al. (2009) compiled biological rhythm interviews for assessment in neuropsychiatry (BRIAN) with four subscales for social rhythms, eating patterns, sleep, and activities. However, there are limitations to their application in healthy young adult populations. Moreover, the time efficiency of the abovementioned biological rhythm assessment questionnaire still needs to be explored with the rapid development of information and communication technology in the current society, which has led to digital media use being embedded in our lives. In fact, a substantial body of study has demonstrated the impact of digital media use on biological rhythm. For instance, a clinical trial with a representative sample of 1,508 American adults revealed that the use of electronic devices with light-emitting screens was associated with negative sleep, circadian timing, and next-morning alertness, and suppressed the phase shift of the biological clock (Chang et al., 2015). Similarly, another study showed that digital media use negatively affected biological regulation (Green et al., 2017).
To address the gap in the lack of assessment of digital media use in self-report questionnaires of biological rhythm and on the basis of literature reviews, we compiled a Self-Rating of Biological Rhythm Disorder for Adolescents (SBRDA). The generally accepted view is that one of the most apparent outputs of the biological rhythm is the sleep-wake cycle (Green et al., 2017). Erratic eating patterns are an important factor affecting biological rhythms (Melkani and Panda, 2017). Thus, the SBRDA contains four dimensions: digital media use, diet, sleep, and activities. We focused specifically on young adults because it is a time in development when the endogenous circadian phase begins to flourish and therefore composes a sensitive period where the misaligning of these processes may restrain an individual’s ability to recover homeostasis and ultimately lead to negative biological outcomes. Our previous studies have evaluated the reliability and construct validity of the SBRDA in 1,152 college students and 8,082 middle school students, and the results show that the SBRDA meets the evaluation standard of psychometrics (Xie et al., 2021). In addition, our previous study also found that SBRDA was significantly associated with depressive symptoms. We have published an article based on this result (Xie, 2021), which shows that after adjusting for confounding factors, the biological rhythm disorder score could predict depressive symptoms after 6 months in adolescents. The odds ratio (OR) value (95% confidence interval [CI]) of the association between the high biological rhythm score group and depressive symptoms was 3.76 (2.30-6.09), p < 0.001. The OR value (95% CI) of the association between the middle group and depressive symptoms was 2.24 (1.42-3.54), p < 0.05. However, we did not externally validate the SBRDA against objective measures of biological rhythm such as DLMO.
Hence, the first purpose of this study is to further validating the compliance and accuracy of SBRDA and DLMO. Second, we compared the differences between the SBRDA, MEQ, and MCTQ questionnaires in healthy Chinese young adults. Finally, we hypothesize that the SBRDA can be widely used in the preliminary screening of biological rhythm disorder among healthy young adults.
Methods
Participants
A total of 120 college students for the current study were recruited from Anhui Medical University in Hefei, Anhui Province, between October 2021 and February 2022. After evaluating eligibility for participation, 16 (13.3%) were excluded for meeting the exclusion criteria and 7 (5.8%) dropped out during the experiment. The inclusion criteria including young adults under the age of 25. The exclusion criteria were a history of mental illness, shift work or sleep disorder, and inability to complete the assessment of questionnaire and unwillingness to participate in the investigation (Figure 1). Ninety-seven college students were registered and all provided saliva samples in a laboratory setting for melatonin assays. Eight college students were excluded because DLMO was undetected during the sampling period. Ultimately, 89 valid data points were analyzed, including 42 (47.2%) boys and 47 (52.8%) girls, with an average age of 18.5 ± 1.2 years. This study was approved by the Ethics Committee of Anhui Medical University (No.20200965). All young adults and their parents were informed of the procedures and provided written consent.
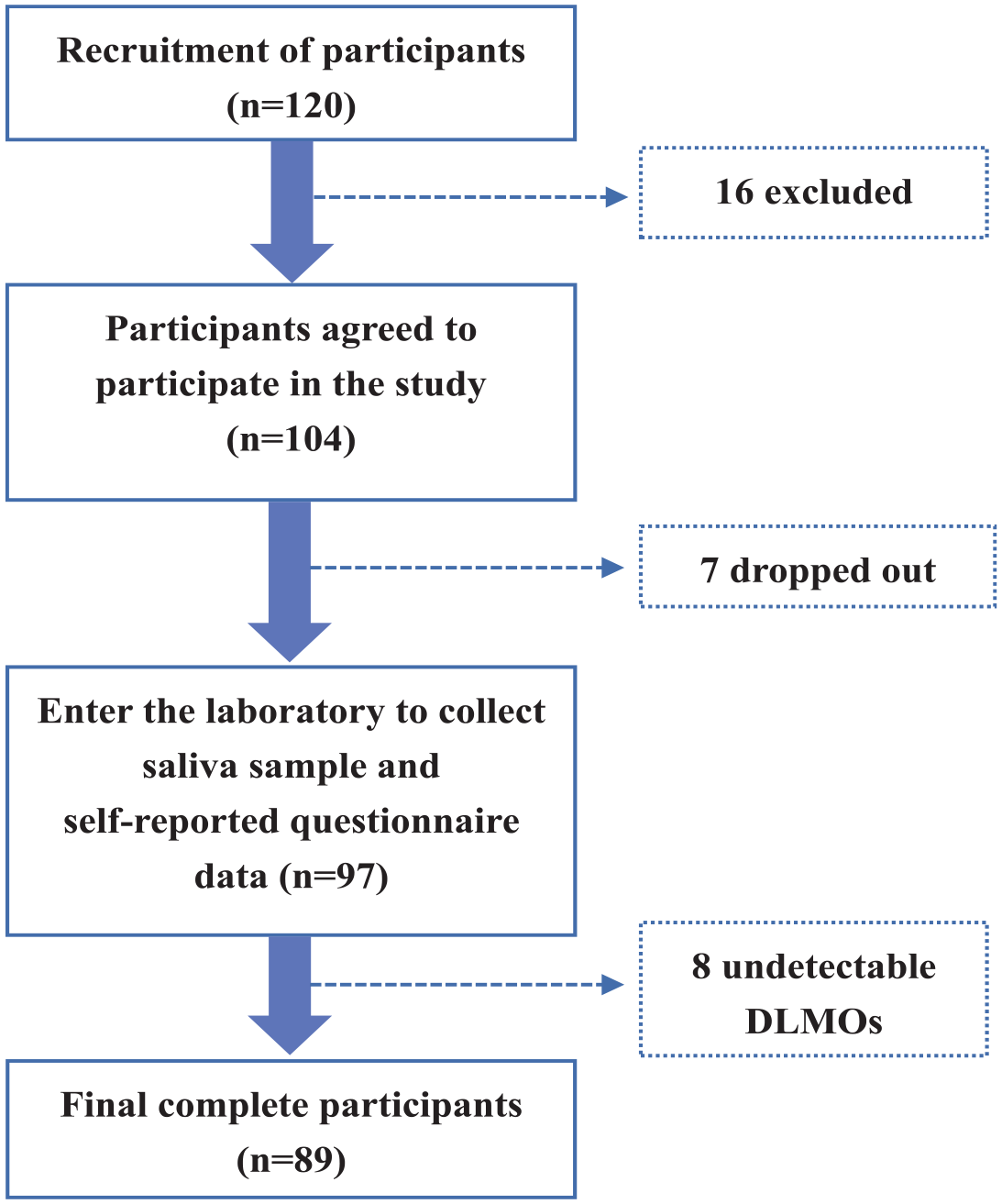
Study flowchart. Abbreviations: DLMO = Dim light melatonin onset.
Materials and Procedure
Sociodemographic Data
In the present study, sociodemographic data for each participant were collected, including sex (boys or girls), age, self-reported height and weight, and body mass index (BMI).
Dim Light Melatonin Onset (DLMO)
Sampling and testing for DLMO was scheduled for workdays between October 2021 and February 2022. Taking into account the influence of season, the sampling of all subjects was completed in October, and the work of saliva sample testing lasted until February 2022. All participants were required to fill in a sleep diary (including sleep time, average wake-up time, bed time, midpoint of sleep, and sleep duration) of their habitual sleep-wake pattern for the previous 7 days. Participants were invited into the laboratory 5 h in advance for one evening based on their self-reported bed time in their sleep diaries. Saliva samples were collected from 4 h before bed time to 2 h after sleep every 60 min by chewing on a cotton swab in a dim-light (<50 lx) laboratory environment, and all participants refrained from caffeine. Saliva samples were obtained from participants under supervision of our research team. A total of 7 samples were collected from each participant. Samples were immediately stored at -80 °C and later assayed for melatonin by a commercially available melatonin enzyme-linked immunosorbent assay (ELISA) kit (IBL-International, Hamburg, Germany). We used linear interpolation to calculate DLMO, which means the time at which melatonin levels crossed the 4 pg/mL threshold in saliva (Smits et al., 2003).
Biological Rhythm Disorder
Biological rhythm was assessed using the SBRDA (Xie et al., 2021). The SBRDA consists of 29 items, reflecting four dimensions: sleep, digital media use, diet, and activities. In SBRDA, items 4, 5, 6, 7, 8, and 9 constitute the sleep dimension, the diet dimension includes items 14, 15, 16, 17, 18, 19, 20, and 21, the activity dimension includes items 1, 2, 3, 10, 11, 12, and 13, and the media use dimension includes items 22, 23, 24, 25, 26, 27, 28, and 29. Each of the four dimensions is calculated based on the score of the sum of the items it contains. Participants were required to fill in their true biological rhythm status during the past 30 days. Each item was rated on a five-point Likert-type scale, spanning from 1 = “completely inconsistent,” 2 = “basically inconsistent,” 3 = “somewhat consistent,” 4 = “basically consistent,” to 5 = “completely consistent.” The composite SBRDA score ranged from 29 to 145, corresponding to the levels from none to extreme; the higher the score on the questionnaire, the greater the degree of biological rhythm disorder. The Cronbach’s α coefficient of the SBRDA was 0.950.
MEQ
In this study, the reduced Morning and Evening Questionnaire (MEQ) was used to identify the circadian rhythm among young adults to compare the difference with SBRDA. The total score of the MEQ is 4-25 points, according to which the subjects can be divided into evening type (4-11 points), neutral type (12-17 points), and morning type (18-25 points). The Cronbach’s α coefficient of the MEQ was 0.68 (Danielsson et al., 2019).
MCTQ
The ultrashort Munich Chronotype Questionnaire (MCTQ) contains 6 items that ask about sleep and activity schedules, such as “When do you usually go to bed?” “How long does it take you to fall asleep?,” and “What time do you get up?.” Through the integration of sleep and wake time information on workdays and work-free days, the individual’s “feel best rhythm” during sleep and activity time is compared with the habits of others, and the individual’s sleep-wake time is evaluated with high precision. The individual’s circadian rhythm of MCTQ is calculated as the midsleep on free days corrected for differences between sleep duration on free days and sleep duration on work days (MSFsc) (Ghotbi et al., 2020). We used MCTQ to compare the concordance of SBRDA.
Statistical Analysis
All statistical analyses in this study were conducted by SPSS version 23.0 (SPSS, Chicago, IL, USA) and diagrams were generated by GraphPad Prism version 8 (GraphPad software, Inc., CA, USA). The Kolmogorov-Smirnov test was used to evaluate the normal distribution of the SBRDA, DLMO, MEQ, and MSFsc. Categorical variables were presented as frequencies (%), and continuous variables were presented as the means ± standard deviations. Multipoint salivary melatonin concentrations were presented as the mean ± standard deviation and the 25th percentile, 50th percentile, and 75th percentile. We used Pearson pairwise bivariate correlation analyses to evaluate relationships between SBRDA, DLMO, MEQ, and MSFsc. We conducted a chi-square test to compare the gender differences among different sociodemographic variables. We used one-way analysis of variance (ANOVA) to compare differences between groups. A receiver operating characteristic (ROC) curve was used to analyze the discrimination proprieties of the SBRDA for biological rhythm disorder by Medcalc version 18.11.3. Statistical significance was set at p < 0.05 (two-tailed).
Results
Characteristics of Participants
Of the 89 young adults, the mean age and standard deviation were 18.5 ± 1.2 years, and 42 (47.2%) were boys. The average BMI and standard deviation were 21.5 ± 3.9 kg/m2. The demographic and DLMO questionnaire-derived biological rhythm parameters of the participants are shown in Table 1. The distributions of the SBRDA score, MEQ score, DLMO and MSFsc are shown in Figure 2.
Descriptive statistics of demographics, DLMO and questionnaire-derived biological rhythm parameters.
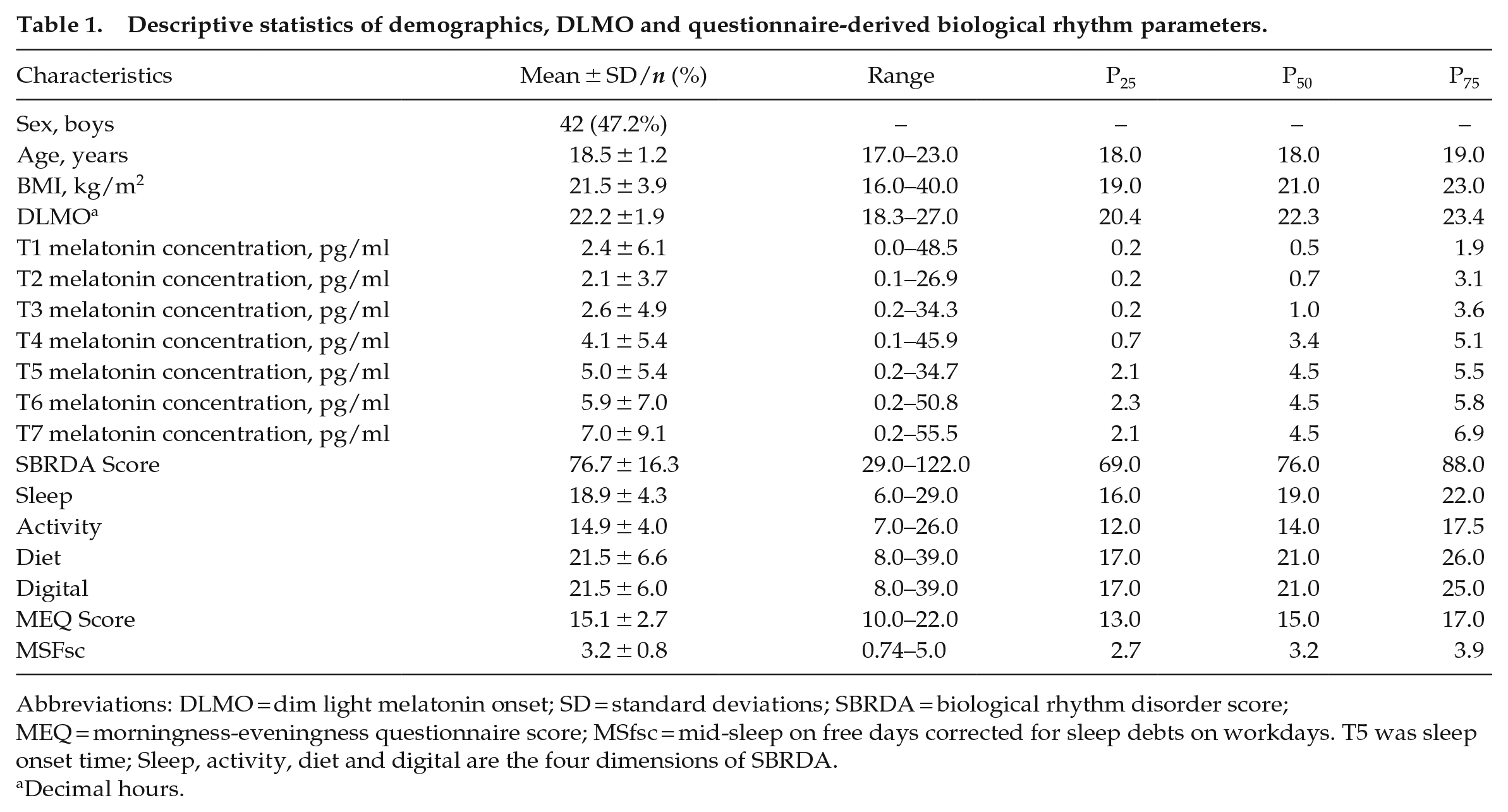
Abbreviations: DLMO = dim light melatonin onset; SD = standard deviations; SBRDA = biological rhythm disorder score; MEQ = morningness-eveningness questionnaire score; MSfsc = mid-sleep on free days corrected for sleep debts on workdays. T5 was sleep onset time; Sleep, activity, diet and digital are the four dimensions of SBRDA.
Decimal hours.
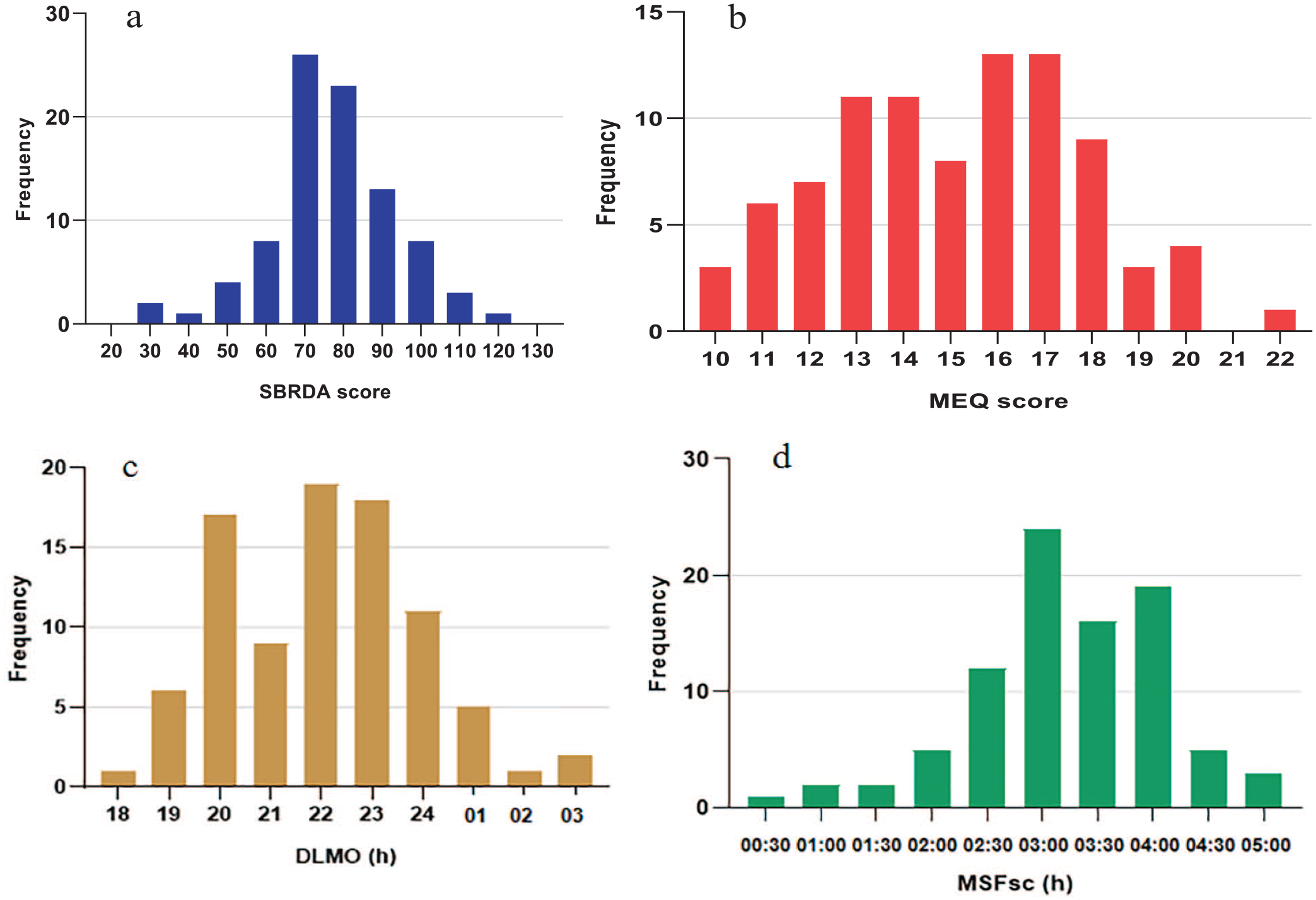
The distributions of SBRDA score, MEQ score, DLMO and MSFsc in whole sample. The X-axis in Figure 2a shows the SBRDA scores of 89 participants; In Figure 2b, the X-axis represents the MEQ score; The X-axis of Figure 2c represents DLMO, 18 is at 6 pm, 19 is at 7 pm, 01 is at 1 am, 02 is at 2 am and 03 is at 3 am; The X-axis of Figure 2d shows the MSFsc time, and the Y-axis of all figures shows the frequency distribution. Abbreviations: SBRDA = self-rating of biological rhythm disorder for adolescents; MEQ = Morningness-Eveningness Questionnaire; DLMO = dim light melatonin onset; MSFsc = mid-sleep on free days corrected for sleep debts on workdays.
Dim Light Melatonin Onset Profiles and Questionnaire-Derived Biological Rhythm Parameters
The mean DLMO time (h) was 22.2 ± 1.9 (Table 1). In this study, we found that DLMO time was later in the boy participants than in the girl participants (22.5 ± 2.0 h vs 21.9 ± 1.9 h), but there was no significant difference (p > 0.05). The SBRDA score and the four dimensions are described in Table 1. To verify the self-rating of biological rhythm disorder, two different assessment methods for chronotype were used in this study, MEQ, and the phase of entrainment of MCTQ (the time of MSFsc). No significant gender difference was found for questionnaire-derived biological rhythm parameters. The distribution of multipoint salivary melatonin concentrations is shown in Table 1. The mean melatonin concentration at the first time point (T1) was 2.4 pg/ml, the mean melatonin concentration at the second time point (T2) was 2.1 pg/ml, the mean melatonin concentration at T3 was 2.6 pg/ml, the mean melatonin concentration at T4 was 4.1 pg/ml, and the mean melatonin concentration at T5 was 5.0 pg/ml. The average melatonin concentration was 5.9 pg/ml at T6 and 7.0 pg/ml at T7.
Multipoints Salivary Melatonin Concentration
Table S2, Table S3, and Table S4 show the secretion trend of the average concentration of melatonin in saliva at 7 time points of young adults in different groups of SBRDA, MEQ, and MSFsc. At 7 time points, the overall concentration of melatonin in the saliva of SBRDA Group Q1 and MSFsc Group Q1 was significantly higher than that of SBRDA Group Q3 and MSFsc Group Q3 (p < 0.05). However, there was no significant difference in the other SBRDA groups and MSFsc groups. In SBRDA Group Q4, the salivary melatonin concentration of young adults at the first time point was the lowest, followed by Group Q3, and the highest in Groups Q2 and Q1. With the dim light environment, the salivary melatonin activation secretion of young adults in Group Q4 rapidly reached the threshold of 4 pg/mL. The salivary concentration trend in the MSFsc Group Q4 was consistent with that in the SBRDA Group Q4. There was no significant difference among the four MEQ groups.
Associations Between SBRDA, DLMO and Other Biological Rhythm Parameters
Pearson’s correlation coefficients and p values for SBRDA, DLMO, and other biological rhythm parameters are shown in the heatmap (Figure 3) and Table S1 in the supplemental material. DLMO moderately and positively correlated with SBRDA score (coefficients range, 0.28~0.33). The MEQ score moderately and negatively correlated with DLMO and SBRDA (coefficients range, -0.33 ~-0.21). Specifically, the DLMO correlated significantly with the SBRDA score (r = 0.33, p < 0.001), MEQ score (r = -0.24, p < 0.05), and MSFsc (r = 0.26, p < 0.05).
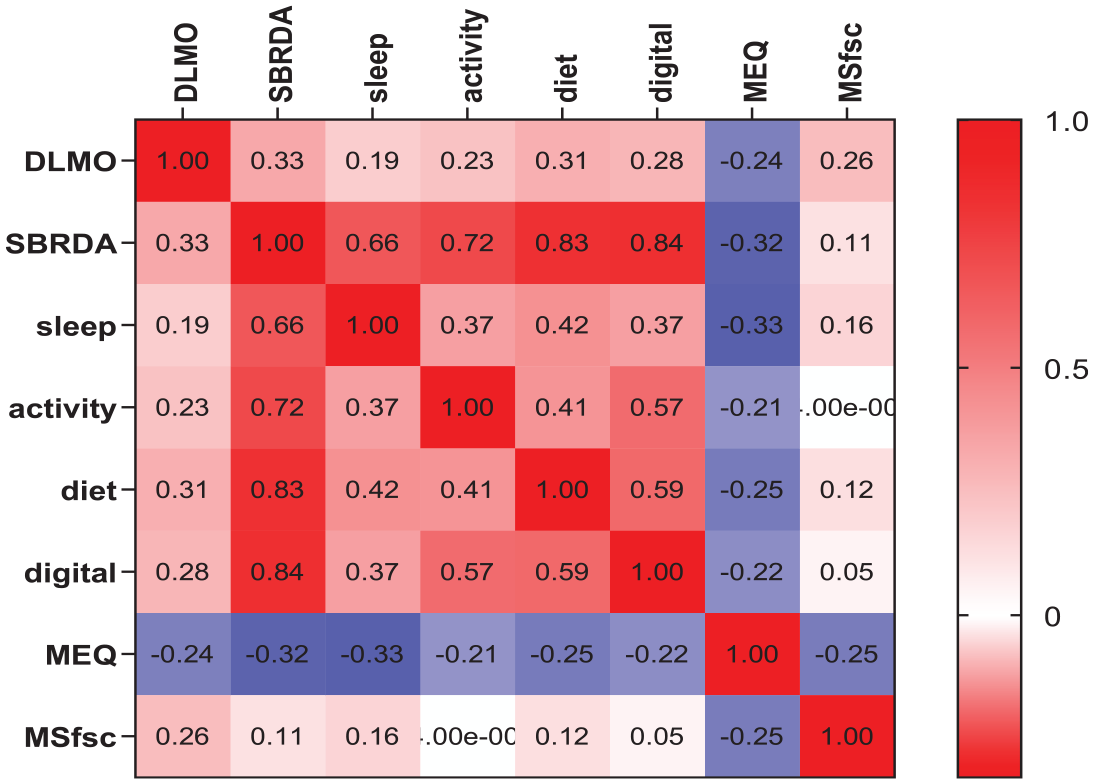
Heatmap analysis of the correlation between DLMO and biological rhythm parameters. The values in the figure represent the correlation coefficients. Abbreviations: DLMO = Dim light melatonin onset; SBRDA = biological rhythm disorder score; sleep, activity, diet and digital are the four dimensions of SBRDA; MEQ = morningness-eveningness questionnaire score; MSfsc = mid-sleep on free days corrected for sleep debts on workdays.
Discrimination Validity
This study examined differences in DLMO and MEQ scores between differing SBRDA-group quartiles. Young adults were classified into the following SBRDA quartiles in Table 2 and Figure 4. Visualization of the density distributions of the data using violin plots (Figure 4) indicated the difference in DLMO and MEQ scores in the SBRDA quartile group. The results of this study showed that DLMO in the Q4 group was significantly later than that in the Q1 group and Q2 group (p < 0.05). The results also showed that the MEQ of the Q4 group was significantly lower than that of the Q1 group and Q3 group (p < 0.05). Violin plots showed that both SBRDA and MSFsc had discriminative validity.
DLMO in the SBRDA, MEQ, and MSFsc quartile groups.
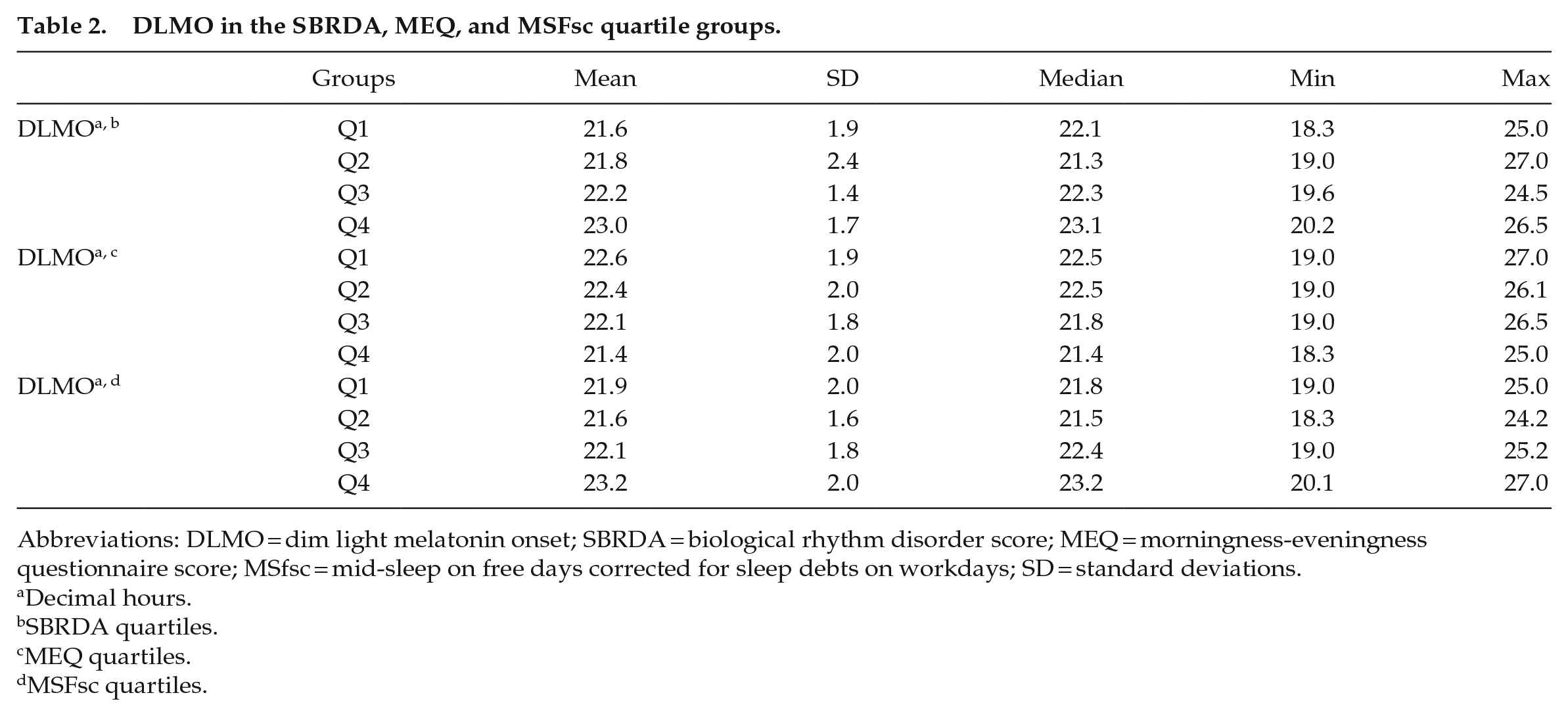
Abbreviations: DLMO = dim light melatonin onset; SBRDA = biological rhythm disorder score; MEQ = morningness-eveningness questionnaire score; MSfsc = mid-sleep on free days corrected for sleep debts on workdays; SD = standard deviations.
Decimal hours.
SBRDA quartiles.
MEQ quartiles.
MSFsc quartiles.
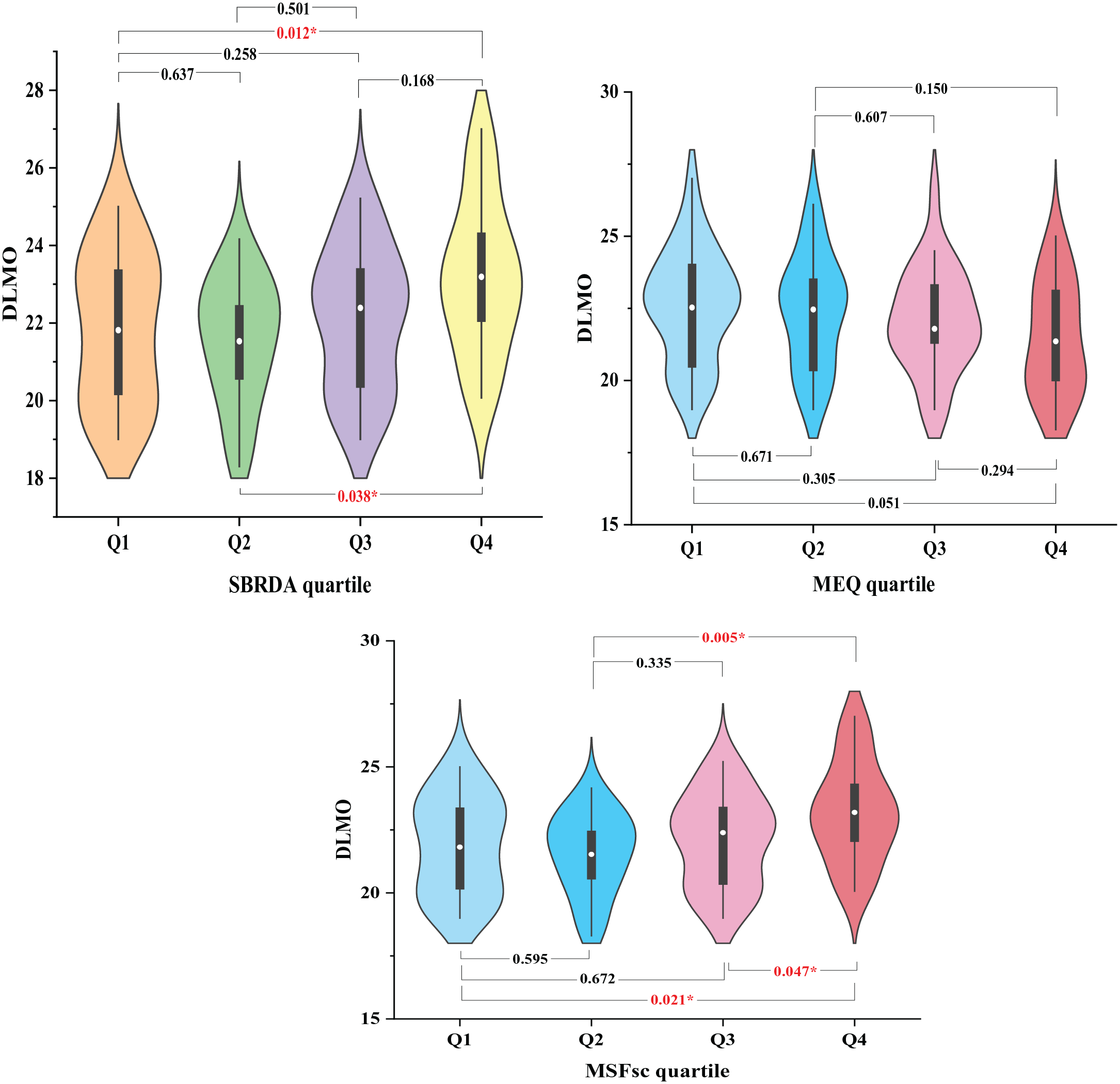
Violin plots of DLMO distribution differences in SBRDA, MEQ, and MSFsc quartile groups. Abbreviations: DLMO = dim light melatonin onset; SBRDA = self-rating of biological rhythm disorder for adolescents; MEQ = Morningness-Eveningness Questionnaire; MSFsc = mid-sleep on free days corrected for sleep debts on workdays.
ROC Curves
ROC curves were used to assess the diagnostic performance and accuracy in hypothetical clinical settings by the area under the curve (AUC). With ROC analysis, the closer AUC is to 1, the more likely the SBRDA will accurately distinguish biological rhythm disorder from normal. ROC curve analysis showed that SBRDA was of diagnostic value for biological rhythm disorder (Figure 5). Analysis of the sensitivity and specificity data of SBRDA showed that the sensitivity was 62.2%, and the specificity was 61.4%. The AUC was 0.64, ranging from 0.54 to 0.74 (Table S5).
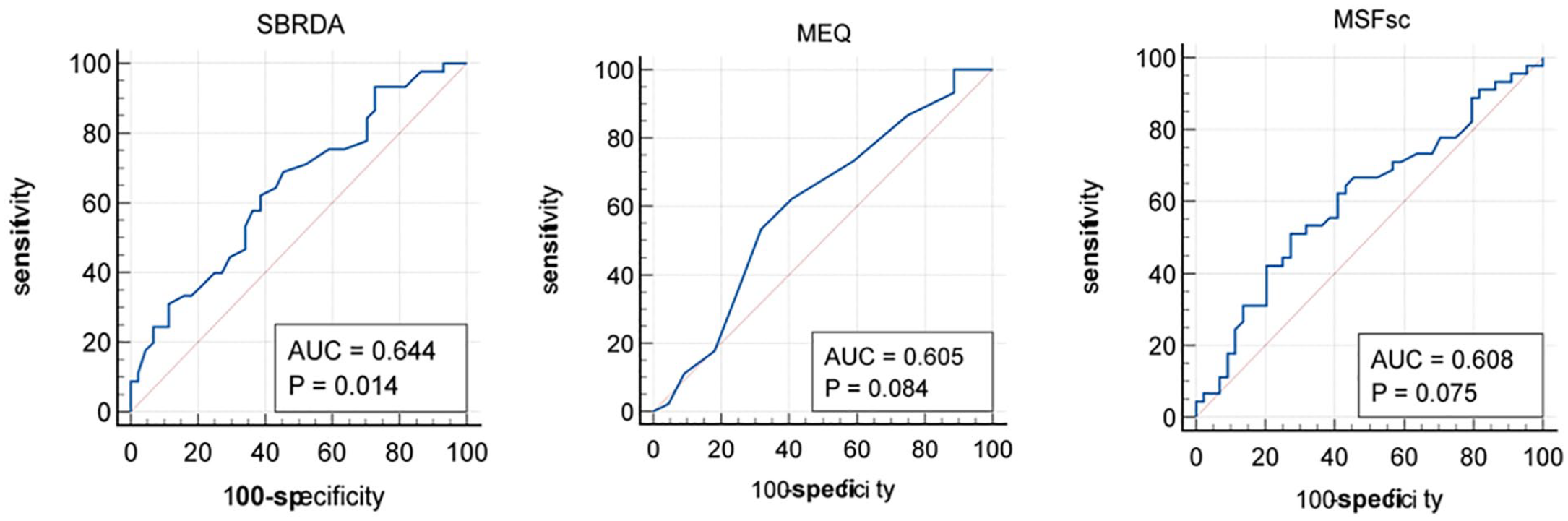
ROC curves for biological rhythm disorders using SBRDA, MEQ, and MSFsc. Abbreviations: ROC = Receiver operating characteristic; SBRDA = self-rating of biological rhythm disorder for adolescents; MEQ = Morningness-Eveningness Questionnaire; MSFsc = mid-sleep on free days corrected for sleep debts on workdays.
Discussion
In this laboratory study of 89 Chinese young adults, the compliance of SBRDA and DLMO was basically consistent, and similar results were obtained with MEQ and MCTQ. DLMO moderately and positively correlated with SBRDA total score (r = 0.33, p < 0.001). The DLMO correlated significantly with the MEQ score (r = -0.24, p < 0.05), and MSFsc (r = 0.26, p < 0.05). Specifically, the results indicated an association between SBRDA and DLMO among healthy young adults, although the correlation was weak. These results suggest that SBRDA, like MSFsc/MEQ, can also reflect the endogenous circadian rhythm of healthy Chinese young adults. Currently, some studies to date have compared the correlation between DLMO with MEQ and MCTQ in special individuals, such as older adults, patients with delayed sleep phase disorder (DSPD), or rural populations, but few studies extend to young adults. For instance, Kitamura et al. reported that MSFsc derived from the MCTQ (r = 0.542, p < 0.001) associated more highly with the DLMO than MEQ score (r = -0.402, p < 0.055) in Japanese adults (Kitamura et al., 2014). However, Kantermann et al. found that the MEQ score (r = -0.70, p < 0.001) was more highly correlated with DLMO than MSFsc (r = 0.68, p < 0.001) in 36 healthy controls and 24 patients with DSPD, and age ranged between 18 and 62 years (Kantermann et al., 2015). A study investigating the circadian phase of healthy rural adults showed that DLMO significantly correlated with MEQ score (r =-0.30, p = 0.02) but not MSFsc (r = 0.25, p = 0.13) (Ruiz et al., 2020). According to the ROC analysis, compared with MEQ and MCTQ, a slightly higher resolution was found for the SBRDA. The total AUC was 0.64. As a result of the ROC analysis and subsequently setting the SBRDA score at 75 points, we were able to distinguish biological rhythm disorder from healthy young adults with high sensitivity and specificity. A recent Japanese study assessing delayed sleep-wake phase disorder (DSWPD) patients reported that the BRIAN cut-off for the presence of DSWPD was 40 points, and the AUC of the ROC was 0.84 (Kanda et al., 2021). One significant reason for this discrepancy is the difference in the target population and assessment questionnaire between these two studies. Our study targeted healthy young adults, while the other study targeted DSWPD.
Our study is broadly consistent with previous studies but is the first to extend analysis to healthy Chinese young adults and is also the first to compare the SBRDA with the DLMO, MEQ, and MCTQ. As described in our introduction, young adults are more susceptible to circadian rhythm disorder than other individuals, since young adults are a time in development when the endogenous circadian phase begins to flourish, and then circadian output from the suprachiasmatic nucleus (SCN) of the hypothalamus in the central biological clock will exhibit age-related declines (Nakamura et al., 2016). In addition, increasingly pervasive digital media use was linked to later bedtime among young adults by inducing circadian phase delays (Orzech et al., 2016). A clinical trial of 12 young adults revealed that digital media use was associated with short sleep timing (Chang et al., 2015). Thus, young adults were a more sensitive group of the population considering the increase in circadian rhythm disorder (Logan et al., 2018). In the present study, we verified an effective tool for assessing biological rhythm disorder in young adults. According to the currently known factors affecting biological rhythms, we determined the dimensions of SBRDA, including digital media use, diet, sleep, and activities. Moreover, we compared the consistency of SBRDA with DLMO, the gold standard marker for circadian phase. SBRDA is a slightly better representative of the central endogenous circadian phase than MCTQ and MEQ in healthy Chinese young adults.
A particularly important finding was that young adults with an SBRDA diagnosis of biological rhythm disorder of the highest quartile had the lowest initial secretion concentration of melatonin, which was rapidly activated and peaked when exposed to dim light. However, although our results indicate that young adults in the highest quartile of SBRDA have a faster rate of nocturnal melatonin secretion than those in the other three groups, exposure to darkness during the evening has not been reported to stimulate melatonin production. Further study is therefore warranted to explore the effect of biological rhythm disorder on the pattern and mechanism of nocturnal melatonin secretion in young adults.
For the previous study, we conducted only internal evaluation of SBRDA (Xie et al., 2021). The strengths of the present study include that this study externally validates the SBRDA against an objective measure (melatonin secretion) of biological rhythm, further demonstrating the effectiveness of SBRDA. In addition, we used the ROC to estimate the discrimination proprieties of the SBRDA for biological rhythm disorder, which was thought to be applicable in clinical settings. Despite the above strengths, the present study has several limitations. First, although we already collect saliva in the dim light (<50 lx) to detect DLMO, recent research (Phillips et al., 2019) also suggests that some people might show sensitivity to light levels lower than 50 lx. A one-day measurement of DLMO may not represent the all-year endogenous circadian phase of participants. Both activity and eating may affect biological rhythm, but we did not record detailed data on activity and eating of participants during DLMO collection. Therefore, more stringent experimental conditions and designs are needed to further clarify the authenticity of DLMO. Second, although SBRDA, MEQ and MCTQ can all evaluate biological rhythms, they still have certain differences. For example, MEQ and MCTQ tend to reflect chronotypes, while SBRDA tends to reflect individual daily life rhythms. Finally, the SBRDA has only been validated in healthy young adults. Further studies are needed to clarify the effectiveness in a wider population.
The current study was conducted in a laboratory study of healthy young adults and objectively measured multipoint individual-level melatonin secretion, indicating that SBRDA can be used to identify biological rhythm disorders in apparently healthy young adults. In addition, compared with MEQ and MCTQ, SBRDA is more suitable for the evaluation of biological rhythm disorders in healthy young adults in China.
Supplemental Material
sj-docx-1-jbr-10.1177_07487304221141939 – Supplemental material for Validation of the Self-Rating of Biological Rhythm Disorder for Adolescents (SBRDA) Scale by Dim Light Melatonin Onset in Healthy Young Adults
Supplemental material, sj-docx-1-jbr-10.1177_07487304221141939 for Validation of the Self-Rating of Biological Rhythm Disorder for Adolescents (SBRDA) Scale by Dim Light Melatonin Onset in Healthy Young Adults by Yang Xie, Xiaoyan Wu, Xingyue Mou, Meng Wang, Shuman Tao, Yuhui Wan and Fangbiao Tao in Journal of Biological Rhythms
Footnotes
Acknowledgements
We would like to appreciate our co-operators for assistance in data collection and all staff and participants. This work was supported by the National Natural Science Foundation of China (Grant number: 82073578)
Author Contributions
Conceptualization, Formal analysis, Y.X. (Yang Xie), M.X. (Xingyue Mou), M.W. (Meng Wang); Writingoriginal draft, Y.X., Y.W. (Yuhui Wan), F.T. (Fangbiao Tao); Investigation, Y.X., X.W. (Xiaoyan Wu), Y.W., S.T. (Shuman Tao), F.T.; Methodology, Y.X., Y.W.,; Supervision, F.T.; Funding acquisition, Writing-review and editing, F.T.; All authors checked interpreted results and approved the final version.
Conflict of Interest Statement
The author(s) have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Statement
Both the design and data collection were approved and reviewed by the Ethics Committee of Anhui Medical University (No.20200965). All participants signed informed consent for inclusion before the administration of the survey.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.