
Abstract
The literature remains sparse and inconclusive about the impact of shift and night work on mortality, and still more on specific causes of death. The objectives were to explore the prospective associations between exposure to shift and night work and all-cause and cause-specific mortality. The study was based on a large national representative French prospective cohort of 1,511,456 employees followed up from 1976 to 2002. Exposure to shift and night work relied on a job-exposure matrix, and 3 time-varying measures (current, cumulative, and recency-weighted cumulative exposure) were constructed. Mortality and causes of death were provided by the national registry, and all-cause, cardiovascular, cancer and preventable mortality, and suicide were studied. Cox proportional hazards models were performed to study the associations between shift and night work and mortality. During follow-up, 22,105 deaths occurred for all-cause mortality. In the study of mortality until the end of last job during follow-up, shift and/or night work were associated with all-cause, cardiovascular, cancer and preventable mortality, and suicide (except night without shift work with cancer mortality and suicide) among men. Shift work (especially shift without night work) was associated with all-cause, cancer and preventable mortality among women. The results were similar for current, cumulative, and recency-weighted cumulative exposure. Associations were found for more detailed causes of death: cerebrovascular diseases for both genders, ischemic heart diseases, respiratory cancers, smoking-related mortality, and external causes of death among men, and breast cancer among women. In the study of mortality until the end of follow-up, some additional associations were found among women between night work and all-cause and preventable mortality, and suicide, suggesting long-term or delayed exposure effects. The study may, however, be underpowered to detect all the exposure-outcome associations, especially among women. More research and prevention are needed to reduce mortality among shift and night workers.
Keywords
Shift and night work, designed to provide services throughout the day and night, address technological constraints, and increase productivity and flexibility, are complex to define given the variability and heterogeneity of the involved working hours arrangements, leading the International Agency for Research on Cancer (IARC, 2020) to consider the combination of shift and night work as the most harmful condition for circadian rhythms. Shift and night work have been found as risk factors for chronic diseases. The systematic review of systematic reviews by Rivera et al. (2020) showed significant associations of shift work with cardiovascular diseases in general but also ischemic heart disease/myocardial infarction, ischemic stroke, and cardiovascular risk factors such as hypertension, diabetes, obesity, and metabolic syndrome. Associations were also found between shift work and various cancers, breast, prostate, and colorectal cancer. High risk estimates, though non-significant, were observed for depression and occupational injuries. Other literature reviews showed that night shift work was associated with increased risk of various morbidity outcomes, such as cancer or ischemic stroke (Brown et al., 2009; Pahwa et al., 2018). Reviews shed light on the mechanisms by which shift and night work may lead to chronic diseases. Kecklund and Axelsson (2016) proposed a theoretical model of mechanisms and pathways involving behavioral (circadian disruption, disturbed sleep, altered diet, and other behaviors), physiological (neuroendocrine, cardiometabolic and cellular stress, and altered immune functioning), and psychological mechanisms (cognitive impairments). The paper by Puttonen et al. (2010) aimed to review the specific mechanisms between shift work, circadian stress, and cardiovascular and metabolic diseases and underlined the most plausible behavioral (weight gain, smoking), biological/physiological (activation of the autonomic nervous system, inflammation, changed lipid and glucose metabolism), and psychosocial mechanisms (low control on working hours, work-life imbalance, and poor recovery). Thus, the literature has brought evidence for the effects of shift and night work on morbidity outcomes and biological plausibility for their effects on morbidity and mortality outcomes.
However, the impact of shift and night work is less known on all-cause and cause-specific mortality. Five literature reviews with meta-analysis were performed on this topic, but evidence remains low for all-cause, cardiovascular and cancer mortality (Li et al., 2016; Lin et al., 2015; Taouk et al., 2020; Vyas et al., 2012; Wang et al., 2018). Three reviews (Lin et al., 2015; Taouk et al., 2020; Vyas et al., 2012) showed a non-significant association between shift and/or night work and all-cause mortality. Reviews produced contradictory results for cardiovascular and cancer mortality (Li et al., 2016; Lin et al., 2015; Taouk et al., 2020; Vyas et al., 2012; Wang et al., 2018). All in all, the literature remains sparse, with a low number of primary studies and a low statistical power to detect significant associations with mortality. Furthermore, these studies suffered from a number of limitations, including lack of representative national samples and of cumulative measures of exposure.
The objectives of the study were to explore the prospective associations of shift and night work (including cumulative exposure) with all-cause and cause-specific mortality in a large national representative sample of the French working population. Cardiovascular, cancer and preventable mortality (i.e., mortality related to high-risk behaviors), and suicide were studied, because previous studies provided evidence for increased risk for morbidity outcomes associated with these exposures. Furthermore, our study was designed to overcome the limitations of previous studies, as it relied on a large prospective nationally representative cohort and had complete data on both exposures and outcome over an entire long follow-up.
Our assumptions were the following:
Both shift work and night work are expected to be associated with mortality.
Both shift work and night work are expected to be associated with the studied causes of death.
The most harmful exposure is expected to be night with shift work.
The time lag between exposure and outcome is expected to differ according to the studied mortality outcome, as it may be hours for injury and decades for cancer, for example. Consequently, there may be differences in the results according to the studied outcome for the study of cumulative exposure as well as for the study of long-term or delayed effects after the end of exposure.
Methods
This study used the data from the STRESSJEM project, whose protocol was published previously (Niedhammer et al., 2019). The STRESSJEM project was designed to study the associations between occupational exposures, including psychosocial work exposures, exposures related to working hours/time, measured using job-exposure matrices (JEM), and mortality. Previous studies using these data focused on the psychosocial work exposures from the job strain model in association with all-cause and cause-specific mortality (Niedhammer et al., 2020a, 2020b, 2020c; Niedhammer et al., 2021). Other studies are in progress to examine other exposures.
Briefly, the STRESSJEM project was based on a large national representative prospective cohort using 3 sources of data: (1) the DADS-INSEE (Déclaration Annuelle des Données Sociales-Institut National de la Statistique et des Etudes Economiques) panel, that is, a random (1/24th) sample of the French national working population of 1,511,456 employees with data for job history over the 1976-2002 period, that is, data for all jobs held within this period, with dates of start and end of job, occupation, economic activity of the company, and company size of each job; (2) the SUMER (SUrveillance Médicale des Expositions aux Risques professionnels) survey data on the assessment of occupational exposures in the French national working population of employees and a job-exposure matrix (JEM) constructed using these data and imputed to the DADS-INSEE panel; and (3) mortality data from the INSERM-CépiDc (Institut National de la Santé Et de la Recherche Médicale-Centre d’épidémiologie et de recherche sur les causes médicales de Décès) French national registry linked to the DADS-INSEE panel through the COSMOP (COhorte de Surveillance de la MOrtalité selon l’activité Professionnelle) program set up by Santé publique France.
The assessment of exposure to shift and night work was performed using a JEM. The method was similar to the method used to construct the JEM for the job strain model exposures in a previous publication (Niedhammer et al., 2018). To construct the JEM, we used the individual measures of exposure to shift and night work collected by occupational physicians in the SUMER survey (49,984 employees). Shift work was defined by exposure to any shift system. Night work was defined by any working period including the interval between midnight to 5:00 a.m. (definition by the European Union and International Labour Organization [ILO]) more than 52 nights a year. We performed a segmentation method (Classification and Regression Tree [CART]) and cross-validation using the individual data of exposure and 3 job title variables, occupation, economic activity of the company, and company size, available in the SUMER survey data. This method allowed the identification of groups, that were homogeneous for the exposure considered and provided JEM exposures, that can be interpreted as the probability of exposure within a homogeneous group defined by one or more categories of occupation, economic activity, and/or company size. Extensive information on the CART methodology may be found elsewhere (Niedhammer et al., 2018). More detailed information about the construction and study of validity of the JEM for shift and night work can be found in the Supplementary Material. The validity of the JEM exposures to shift and night work was found to be satisfactory in the SUMER data, except the JEM measure for night work among women, for which the validity was lower. The 3 job title variables were then used to impute the JEM exposures in the DADS-INSEE panel.
Three time-varying measures of JEM exposures (assessing the probability of exposure) were used for shift and night work for the 1976-2002 period: (1) current exposure, that is, the probability of exposure for any day i within the study period; (2) cumulative exposure, that is, a mean daily probability of exposure until day i, taking all past exposures into account; and (3) recency-weighted cumulative exposure, that is, a mean daily probability of exposure within the 5 last years until day i, with higher weight for more recent exposure. The 2 cumulative measures of JEM exposure allowed us to use all data available even if the follow-up duration was not the same from an employee to another. The 3 measures of JEM exposure were then dichotomized at the value corresponding to the observed prevalence of exposure using individual data in the French national working population of employees in the SUMER survey. This choice was justified by the need to obtain consistent exposure prevalences and reduce misclassification. The threshold to dichotomize the probability of exposure was 0.42 for shift work and 0.255 for night work. Shift and night work were studied as 2 separate exposures and also as a combined exposure.
All-cause and cause-specific mortality were studied as outcomes. The causes of death were coded according to the International Classification of Diseases (ICD). The codes for cardiovascular and cancer mortality, and suicide were I00-I99, C00-C99, and X60-X84, respectively, in ICD-10 and the corresponding ICD-9 and ICD-8 codes. Preventable mortality was defined according to the Organisation for Economic Co-operation and Development and Eurostat (OECD/Eurostat, 2019) and included death causes related to health behaviors (smoking, alcohol use, physical inactivity, nutrition) and high-risk behaviors involved in external causes of death (accidents and injuries).
Cox proportional hazards models were performed to study the associations between the 3 time-varying exposures to shift and night work and the outcomes of mortality. The assumption of proportionality was checked by graphical analysis and no violation of proportionality was observed. Age (continuous variable in days) was the time scale. Covariates included calendar time and 4 occupational variables related to physical, biomechanical, chemical, and biological exposures. Physical exposure was defined by noise, thermic constraints, and radiations, and biomechanical exposure by manual materials handling, postural and articular constraints, repetitions of the same movement or series of movements at high speed, hand-arm or whole-body vibrations, and driving of specialized machinery, car, lorry, bus, and so on. Chemical and biological exposures were defined by any exposure to chemical or biological agents. These exposures were collected by occupational physicians in the SUMER survey (Niedhammer et al., 2008) and imputed through a JEM using the same methodology seen above. Models with delayed entry were used: people entered the cohort on 1 January 1976 if they were working or when they started working. First, we studied mortality until the end of last job. Follow-up ended at death date, or at the end date of last job, or at the end of follow-up (31 December 2002) if still working at this time, whichever came first. Right-censoring was used in the case of death for other causes than the studied cause of death. We used Akaike’s information criterion (AIC) to compare the models with the 3 different time-varying exposures (current, cumulative, and recency-weighted cumulative) to identify the model with the best relative quality. Second, we studied mortality until the end of follow-up, that is, including mortality that may have occurred after the end of last job. Sensitivity analyses included (1) using continuous variables of JEM exposure (i.e., continuous probability of exposure) instead of binary exposures, (2) imputing the lowest level of exposure instead of the highest level in case of multiple jobholder (3% of the sample had more than one job at the same time), and (3) adjusting for occupation. Gender-stratified analyses were performed, following best practices (Niedhammer et al., 2000), as gender differences were expected in all used variables (exposures, outcomes, and covariates). All analyses were performed using SAS and R softwares.
Results
The study sample included 1,496,332 people, as 15,214 people had totally missing values for their whole job history (i.e., 1%) and were excluded because the absence of data on job history made the use of JEM impossible. The mean age was 28 and 27 years for men and women, respectively, at entry into the cohort. The study sample was followed up for a mean duration of 17 years. The prevalence of exposure to shift and night work is presented in Supplementary Table S4. Men were more likely to be exposed to shift and night work than women. During follow-up, 22,105 deaths occurred for all-cause mortality. Tables 1 to 3 show the number of deaths according to gender and causes of death. More details about specific causes of death among exposed and non-exposed groups can be found in Supplementary Tables S5 and S6.
Combination of shift and night work and mortality among men and women in the STRESSJEM project (with follow-up until the end of last job).
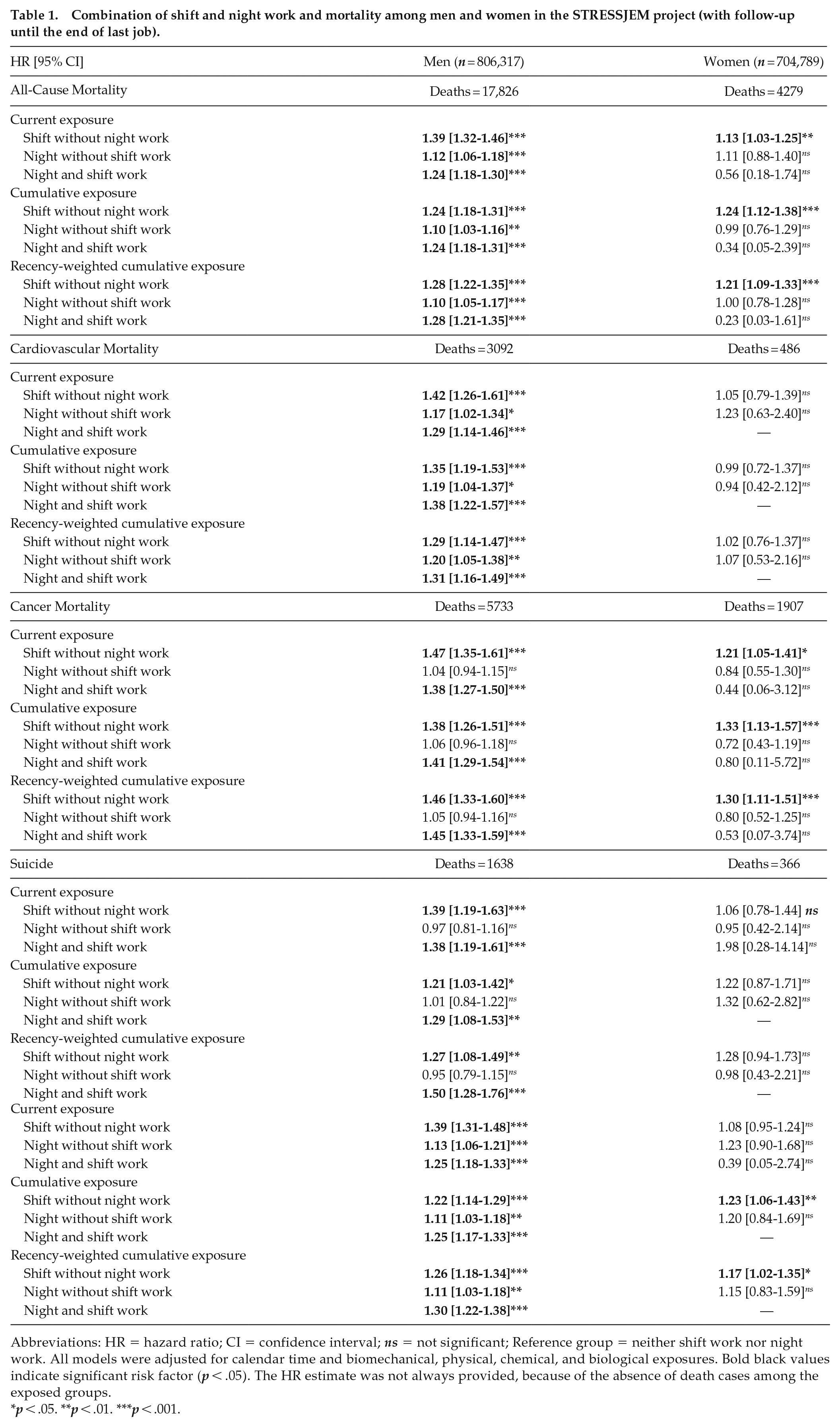
Abbreviations: HR = hazard ratio; CI = confidence interval; ns = not significant; Reference group = neither shift work nor night work. All models were adjusted for calendar time and biomechanical, physical, chemical, and biological exposures. Bold black values indicate significant risk factor (p < .05). The HR estimate was not always provided, because of the absence of death cases among the exposed groups.
p < .05. **p < .01. ***p < .001.
Current exposure to the combination of shift and night work and the most frequent detailed causes of death in the STRESSJEM project (with follow-up until the end of last job).
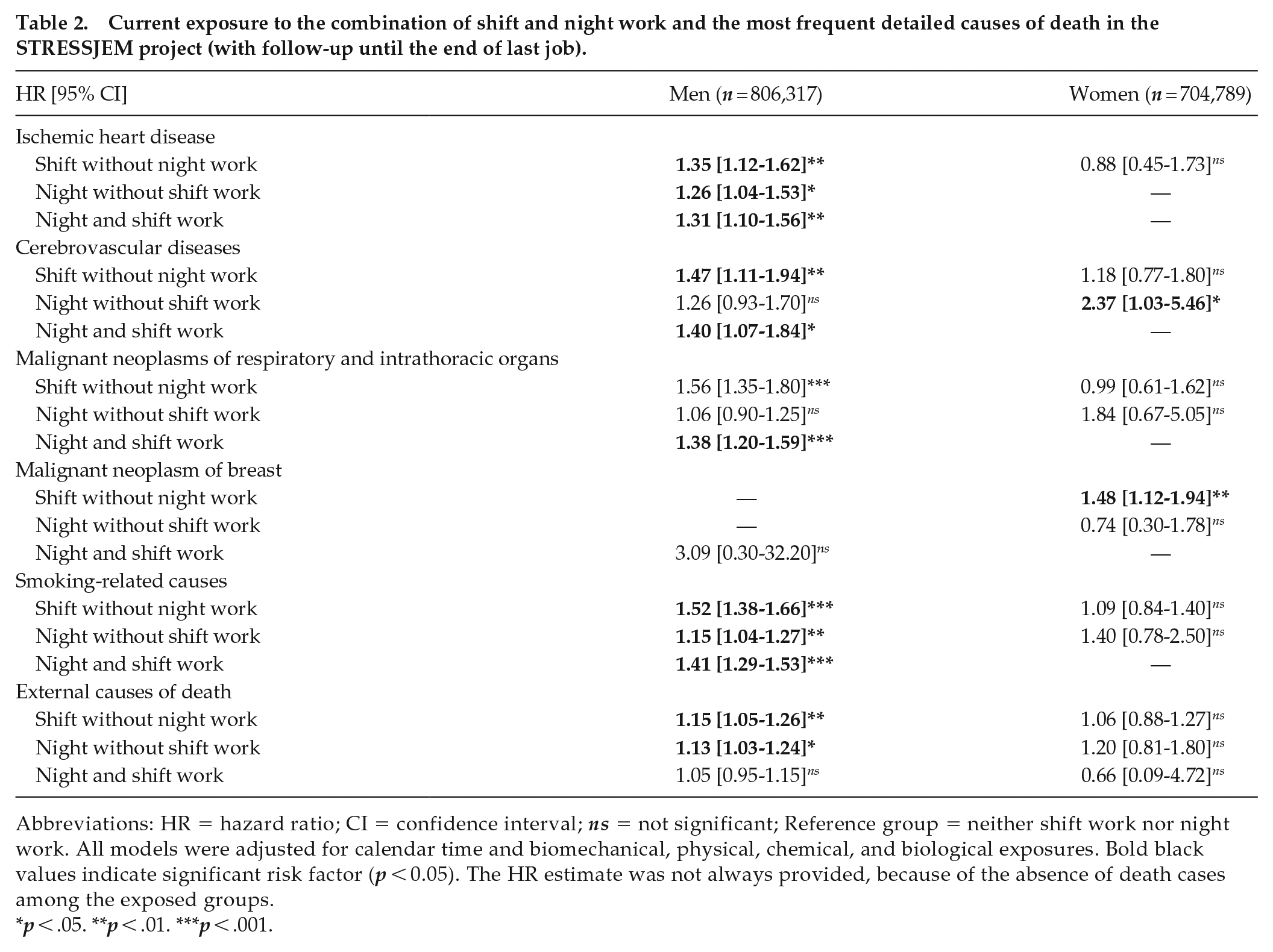
Abbreviations: HR = hazard ratio; CI = confidence interval; ns = not significant; Reference group = neither shift work nor night work. All models were adjusted for calendar time and biomechanical, physical, chemical, and biological exposures. Bold black values indicate significant risk factor (p < 0.05). The HR estimate was not always provided, because of the absence of death cases among the exposed groups.
p < .05. **p < .01. ***p < .001.
Combination of shift and night work and mortality among men and women in the STRESSJEM project (with follow-up until 31 December 2002, that is, including follow-up after the end of last job).
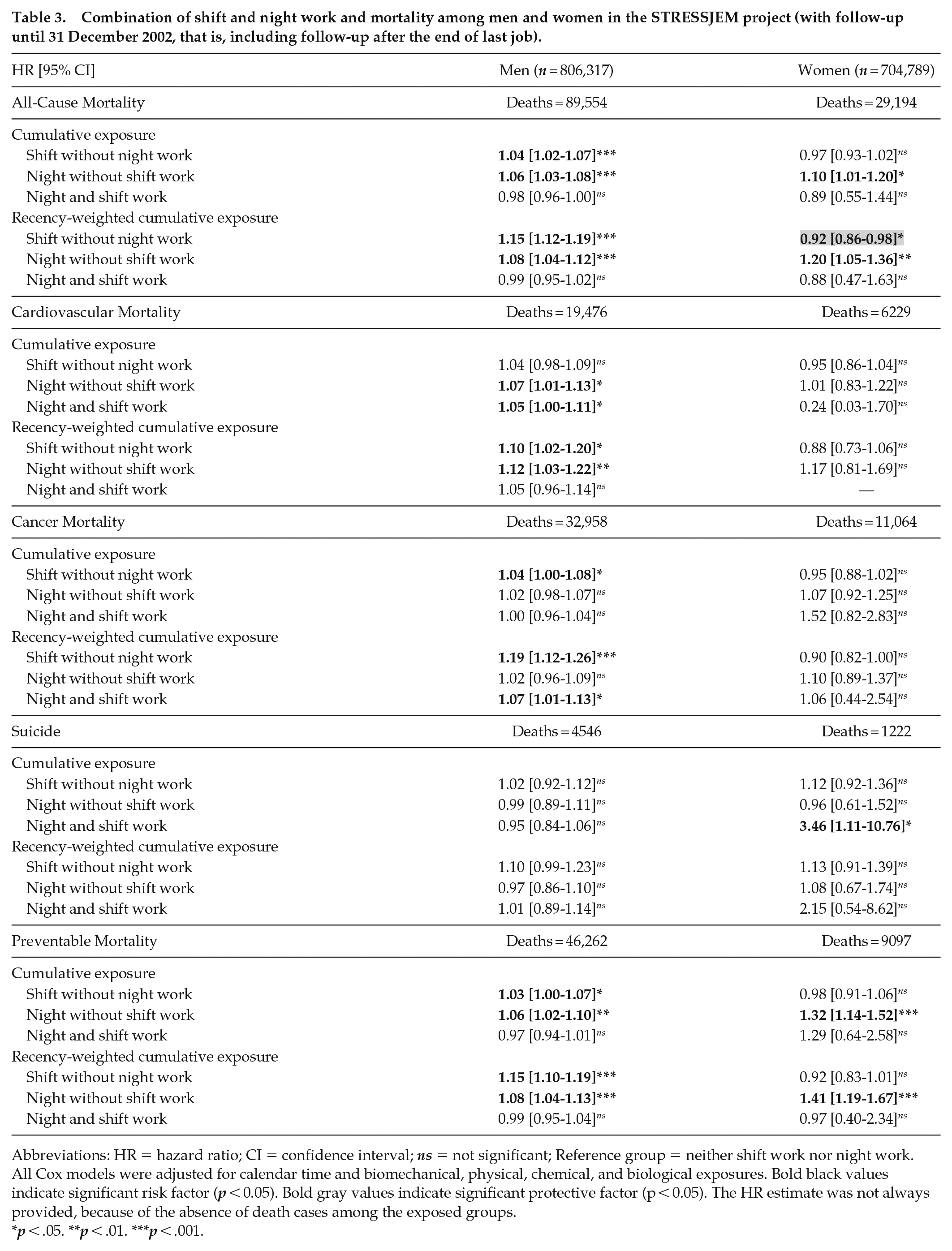
Abbreviations: HR = hazard ratio; CI = confidence interval; ns = not significant; Reference group = neither shift work nor night work. All Cox models were adjusted for calendar time and biomechanical, physical, chemical, and biological exposures. Bold black values indicate significant risk factor (p < 0.05). Bold gray values indicate significant protective factor (p < 0.05). The HR estimate was not always provided, because of the absence of death cases among the exposed groups.
p < .05. **p < .01. ***p < .001.
In the study of mortality until the end of last job, shift and night work were associated with all mortality outcomes among men (except night work with suicide), and shift work was associated with all-cause, cancer and preventable mortality among women (Supplementary Table S7). The 3 models with the different exposure measures (current, cumulative, and recency-weighted cumulative) were considered to have similar relative quality, as the AIC values for the 3 models were close. The 3 combinations of shift and night work were significantly associated with all mortality outcomes among men (except night without shift work with cancer mortality and suicide), whereas shift without night work predicted all-cause, cancer and preventable mortality among women (Table 1). Table 2 and Supplementary Table S8 provided additional results on more detailed causes of death, showing that significant associations were found between shift and/or night work and ischemic heart disease, cerebrovascular diseases, malignant neoplasms of respiratory and intrathoracic organs, smoking-related causes, and external causes of death among men. Among women, shift or night work was significantly associated with cerebrovascular diseases and malignant neoplasm of breast.
The study of mortality until the end of follow-up (i.e., including follow-up after the end of last job) provided less significant associations suggesting that past exposures may have a reduced impact on mortality after the end of last job (Table 3 and Supplementary Table S9). Nevertheless, among women, 3 additional significant associations were found between night work (more precisely night without shift work) and all-cause and preventable mortality, and between night with shift work and suicide, suggesting potential long-term or delayed exposure effects.
The sensitivity analyses provided similar results: (1) when we used continuous variables of JEM exposure (i.e., continuous probability of exposure) instead of binary exposures, (2) when we imputed the lowest level of exposure instead of the highest level in case of multiple jobholder, and (3) when we adjusted for occupation.
Discussion
Our study showed that shift and/or night work among men and women were predictive of all-cause and cause-specific mortality. These results were found for current, cumulative, and recency-weighted cumulative exposure. The associations were significant for almost all studied cause-specific mortality outcomes among men, and for cancer and preventable mortality and suicide among women. Differences in the effects and reversibility of these effects were found according to gender and the studied causes of death. However, the study may have been underpowered to detect all exposure-outcome associations.
Our assumptions were verified only partially. Shift and/or night work were found to be associated with mortality, but there were gender differences that may be explained by a lack of statistical power in the study of night work among women. Associations between these exposures and various causes of death were found, with gender differences, as the analysis among women was limited due to low numbers of cases, especially for some causes of death. The assumption related to the most harmful exposure was not verified, as night with shift work was not more strongly associated with mortality than night or shift work alone. As the relative quality of the models was the same for the model with current exposure and the 2 models with cumulative exposures in the study of all mortality outcomes, it was not possible to conclude about the potential effect of cumulative exposure. However, the study of mortality until the end of follow-up (i.e., including follow-up after the end of last job) led to less significant associations than the study of mortality until the end of last job, suggesting that past exposures may have a lower impact on mortality than more recent exposures, or in other words, there might be a reversibility of the effects after the end of exposure. Nevertheless, among women, significant associations were observed between night work and all-cause and preventable mortality, and suicide, suggesting long-term or delayed exposure effects. It may thus be assumed that the effects and reversibility of these effects may differ according to gender and the studied cause of death.
The comparison with the literature may be difficult given the lack of studies on this topic. Contrary to 3 reviews (Lin et al., 2015; Taouk et al., 2020; Vyas et al., 2012), some primary studies found that shift (Akerstedt et al., 2004) or night work (Akerstedt et al., 2020; Natti et al., 2012) was associated with all-cause mortality. Three reviews reported significant associations between shift work or night-shift work and cardiovascular mortality (Li et al., 2016; Lin et al., 2015; Wang et al., 2018), whereas 2 others (Taouk et al., 2020; Vyas et al., 2012) did not. Two studies (Akerstedt et al., 2020; Natti et al., 2012) showed an association between night work and cancer mortality, and another (Akerstedt et al., 2002) showed an association between non-daytime work and occupational fatal accident. However, comparison with the literature may be difficult as various parameters may differ from one study to another. In particular, differences in population and exposure definition and assessment may make the comparison between studies challenging.
Our study included a number of strengths. We used a large national representative prospective cohort among both men and women, with full information about exposure and outcome over long follow-up. There were no response, participation, selection or attrition bias (as the study relied on routine data), and no reporting bias for both exposure (assessed through a JEM) and outcome (provided by the national registry). The JEM was constructed using independent data from the present cohort but from the same country (France) and for men and women separately, which appears fundamental given gender differences at the workplace (Niedhammer et al., 2000). We had full detailed information about job history over follow-up which made possible the construction of 3 different time-varying measures of exposure (including cumulative measures) contrary to previous studies that commonly explored a baseline or one exposure measure only. This means that we were able to take changes and duration of exposure into account. We adjusted for other occupational exposures that served as proxies of social position and also reduced confounding due to these exposures. Sensitivity analyses were done and confirmed the results.
There were, however, some limitations. There was a lack of precision in the definition of shift and night work. Indeed, intensity for night work (number of nights a year) and past exposures (in the measurement of cumulative exposures) for both shift and night work were studied, but no information was available about permanent/rotating shift, direction of shift rotation, number of consecutive nights/shifts, and start and end time of nights/shifts. Furthermore, we studied night work with a threshold of 52 nights a year; consequently, we did not study any exposure to night work but rather a regular exposure to night work (at least once a week). This definition was, however, less restrictive than the definition used by the French Ministry of Labour that defined regular night work by 2 nights a week. Contrary to our expectations, the combination of night with shift work was not the strongest predictor of mortality. The effects of the 3 combinations of shift and night work had similar effects on mortality outcomes among men, and shift without night work (with follow-up until the end of last job) and night without shift work (including follow-up after the end of last job) were the main predictors among women. This does not mean that night with shift work had no effect on mortality among women, but rather that our analyses were unable to detect significant effects (except in association with suicide). As underlined by others (Alderson, 2004; Altman and Bland, 1995), “absence of evidence is not evidence of absence.” This may be explained by the low prevalence of exposure to night work and the low number of death cases (especially for some causes of death) among the exposed women, leading to low statistical power. A healthy worker effect may have occurred for the analysis of current exposure but seems less likely for the analysis of the 2 cumulative measures, as past exposures were taken into account. Nevertheless, there may be selection effects to enter and stay in jobs exposed to shift or night work (including self-selection), leading healthier workers with greater tolerance being more likely to be exposed. Such selection effects have been observed in France (Niedhammer et al., 1994) and elsewhere (Conway et al., 2008), and are likely to contribute to underestimated associations with health outcomes. Shift without night work, although not the most expected exposure associated with mortality, may play a role on health outcomes through circadian disruption. Its impact might also be mediated via sleep disorders and need for recovery (Harma et al., 2019) and might increase, in the long term, the risk of mortality, as sleep disorders were found to be associated with various morbidity and mortality outcomes (Cappuccio et al., 2010; Uehli et al., 2014). This exposure is also likely to be a psychosocial stressor, through work-family conflict, for example (Wöhrmann et al., 2020), and have health effects through psychosocial stress mechanisms. Previous reviews provided information on the plausible mechanisms that may explain the effects of shift work on health outcomes (Kecklund and Axelsson, 2016; Puttonen et al., 2010). The number of covariates was limited as the data were from routine sources. Consequently, a residual confounding bias remained likely, due to unaccounted confounders at or outside the workplace, which may have overestimated the observed associations. Nevertheless, our models took other occupational exposures into account, reducing confounding due to these exposures. As exposure was assessed through a JEM leading exposure assessment being performed at group level (job title) and not at individual level, our results may be affected by the absence of within-group variance, imprecision, non-differential misclassification, and bias toward the null hypothesis. Thus, the use of JEM exposure is known to produce underestimated exposure-outcome associations compared with individual exposure, in the case of significant association between individual exposure and outcome. All these limitations related to JEM were underlined in a commentary by Peters and Hall (2021) recently. The lack of significant associations for night work (especially night with shift work) among women may also be explained by a lower validity of the JEM for this exposure among women, leading to further imprecision, misclassification, and bias toward the null hypothesis. The choice made to dichotomize the probability of exposure implied that all employees belonging to groups with a probability of exposure higher than the retained threshold were classified as exposed. Other authors faced a similar issue and used various thresholds to dichotomize. No threshold can be considered as optimal as low values lead to increase misclassification among the exposed and high values lead to increase misclassification among the non-exposed. It may be underlined that our results were found to be similar in the sensibility analysis using the continuous probability of exposure instead of the binary exposure, and thus providing results that did not depend on the choice of threshold. As we found significant exposure-outcome associations in our study, we may consider that the JEM was efficient to detect some mortality effects but probably not all effects, as the use of JEM leads to underpowered studies (Peters and Hall, 2021). Among the previous studies using JEMs for shift or night work, most of them did not find significant associations with various health outcomes (Fernandez et al., 2014; Harris et al., 2020; Schwartzbaum et al., 2007; Talibov et al., 2018; Walasa et al., 2018) and only 2 reported significant associations (Fernandez et al., 2021; Hansen, 2001). JEM remains an alternative exposure assessment method in large population-based samples for which no individual exposure data are available (but job title) but cannot replace individual exposure measures. Job history data with rare missing values were treated using mid-censoring, that is, the periods of time with missing data were not considered in the analyses. We had no complete information about the whole job history but only information about the 1976-2002 period, making the assessment of life course exposures impossible. It would be difficult to assess the global effect of all these limitations on the results, as some may lead to overestimate and others to underestimate the results.
Our results suggested that shift and/or night work among men and women may be risk factors for all-cause and cause-specific mortality. More research on the effects of these exposures on mortality is needed, particularly using individual and cumulative assessment of exposure and long follow-up. As our study was certainly underpowered to study the effects of these exposures among women, more research is also needed on this point. Preventive measures should be developed to limit the effects of shift and night work on mortality.
Supplemental Material
sj-pdf-1-jbr-10.1177_07487304221092103 – Supplemental material for Shift and Night Work and All-Cause and Cause-Specific Mortality: Prospective Results From the STRESSJEM Study
Supplemental material, sj-pdf-1-jbr-10.1177_07487304221092103 for Shift and Night Work and All-Cause and Cause-Specific Mortality: Prospective Results From the STRESSJEM Study by Isabelle Niedhammer, Thomas Coutrot, Béatrice Geoffroy-Perez and Jean-François Chastang in Journal of Biological Rhythms
Footnotes
Acknowledgements
The authors thank the members of the DARES (Direction de l’Animation de la Recherche, des Etudes et des Statistiques; French Ministry of Labour), all the occupational physicians and “médecins inspecteurs régionaux du travail,” and all the employees who participated to the SUMER (SUrveillance Médicale des Expositions aux Risques professionnels) survey. The authors thank Catherine Buisson, Laurence Chérié-Challine, and Pascal Empereur-Bissonnet at Santé publique France (Direction Santé Travail) for the access to the COSMOP (COhorte de Surveillance de la MOrtalité selon l’activité Professionnelle) data. The authors also thank all people and public institutions who contributed directly or indirectly to the final COSMOP database, especially INSEE (Institut National de la Statistique et des Etudes Economiques) and INSERM-CépiDc (Institut National de la Santé Et de la Recherche Médicale-Centre d’épidémiologie et de recherche sur les causes médicales de Décès). This study was supported by the French National Research Program for Environmental and Occupational Health of ANSES (Agence nationale de sécurité sanitaire de l’alimentation, de l’environnement et du travail), France (Grant Number: EST-2016/1/49).
Conflict of Interest Statement
The author(s) have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Commission Nationale de l’Informatique et des Libertés (no 762430 V1 and no 04-1274) and Conseil National de l’Information Statistique (no 2009X705TV).
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.