
Abstract
Daylight saving time (DST) is a source of circadian disruption impinging on millions of people every year. Our aim was to assess modifications, if any, in the number, type, and outcome of Accident & Emergency (A&E) visits/return visits over the DST months. The study included 366,527 visits and 84,380 return visits to the A&E of Padova hospital (Northern Italy) over 3 periods between the years 2007 and 2016: period 1 (2 weeks prior to DST to 19 weeks after), period 2 (2 weeks prior to the return to “winter time” to 4 weeks after), and period 3 (5 consecutive non-DST weeks). For each A&E visit/return visit, information was obtained on triage severity code, main medical complaint, and outcome. Data were aggregated by day, cumulated over the years, and analyzed by generalized Poisson models. Generalized additive models for Poisson data were then used to include photoperiod as an additional covariate. An increase in A&E visits and return visits (mostly white codes, resulting in discharges) was observed a few weeks after the enforcement of DST and was significant over most weeks of period 1 (increase of ≈30 [2.8%] visits and ≈25 [10%] return visits per week per year). After the return to winter time, a decrease in absolute number of return visits was observed (mostly white codes, resulting in discharges), which was significant at weeks 3 and 4 of period 2 (decrease of ≅25 [10%] return visits per week per year). When photoperiod was taken into account, changes in A&E visits (and related white codes/discharges) were no longer significant, while changes in return visits (and related white codes/discharges) were still significant. In conclusion, changes in A&E visits/return visits were observed in relation to both DST and photoperiod, which are worthy of further study and could lead to modifications in A&E organization/staffing.
Keywords
The human circadian system encompasses a master clock in the suprachiasmatic nuclei of the brain and peripheral, ancillary time-keepers in virtually every organ of the body (Takahashi, 2017). Light is the main synchronizer of the circadian timing system, but nonphotic stimuli such as food (Mistlberger and Antle, 2011), physical activity (Buxton et al., 1997), and social cues (Honma et al., 1995) also play a role.
In recent years, evidence has emerged that desynchrony between our endogenous circadian clock and the natural environment, for instance, in relation to frequent intercontinental travels or shift work (Cho, 2001, Vosko et al., 2010), has serious medical consequences. These include shorter and more disturbed sleep but also an increased risk of cardiovascular disease (Vetter et al., 2016, Hoevenaar-Blom et al., 2011), metabolic dysfunction (Kim et al., 2015), and an increased incidence of certain types of cancer (Hansen, 2017; Bonde et al., 2012). A source of desynchrony impinging on millions of people every year is the enforcement of daylight saving time (DST; Kantermann et al., 2007; Lahti et al., 2006). Evidence has started to emerge that DST has profound social and medical consequences, including changes in the frequency of road traffic accidents (Lahti et al., 2010; Robb and Barnes, 2018), work performance (Burgess et al., 2013), school performance (Medina et al., 2015), and even changes in the incidence (Janszky and Ljung 2008) and timing (Sipilä et al., 2016) of myocardial infarction, especially in high-risk populations (Kirchberger et al., 2015; Janszky et al., 2012).
The aim of the present study was to assess modifications, if any, in the number, type, and outcomes of Accident & Emergency (A&E) visits and return visits (i.e., within 96 h of the first visit) in relation to the enforcement of DST, taking into account of photoperiod.
Patients and Methods
The study included 366,527 visits and 84,380 return visits (either voluntary or scheduled by the doctor, within 96 h of the first visit) to the A&E Department of Padova University teaching hospital, in Northern Italy, over 3 periods of cumulated, consecutive years (2007-2016):
Period 1: From 2 weeks prior to the enforcement of DST to 19 weeks after (n = 22 weeks). This was selected with a view to detect any changes occurring after the switch and their duration over the subsequent months.
Period 2: From 2 weeks prior to the return to what we will refer to as “winter time” (i.e., non-DST public time, which is the same within a given time zone) to 4 weeks after (n = 7 weeks). This was selected with a view to detect any changes in relation to the return to winter time.
Period 3: Five consecutive weeks starting from the second week in January (i.e., excluding the festivities), used as non-DST reference.
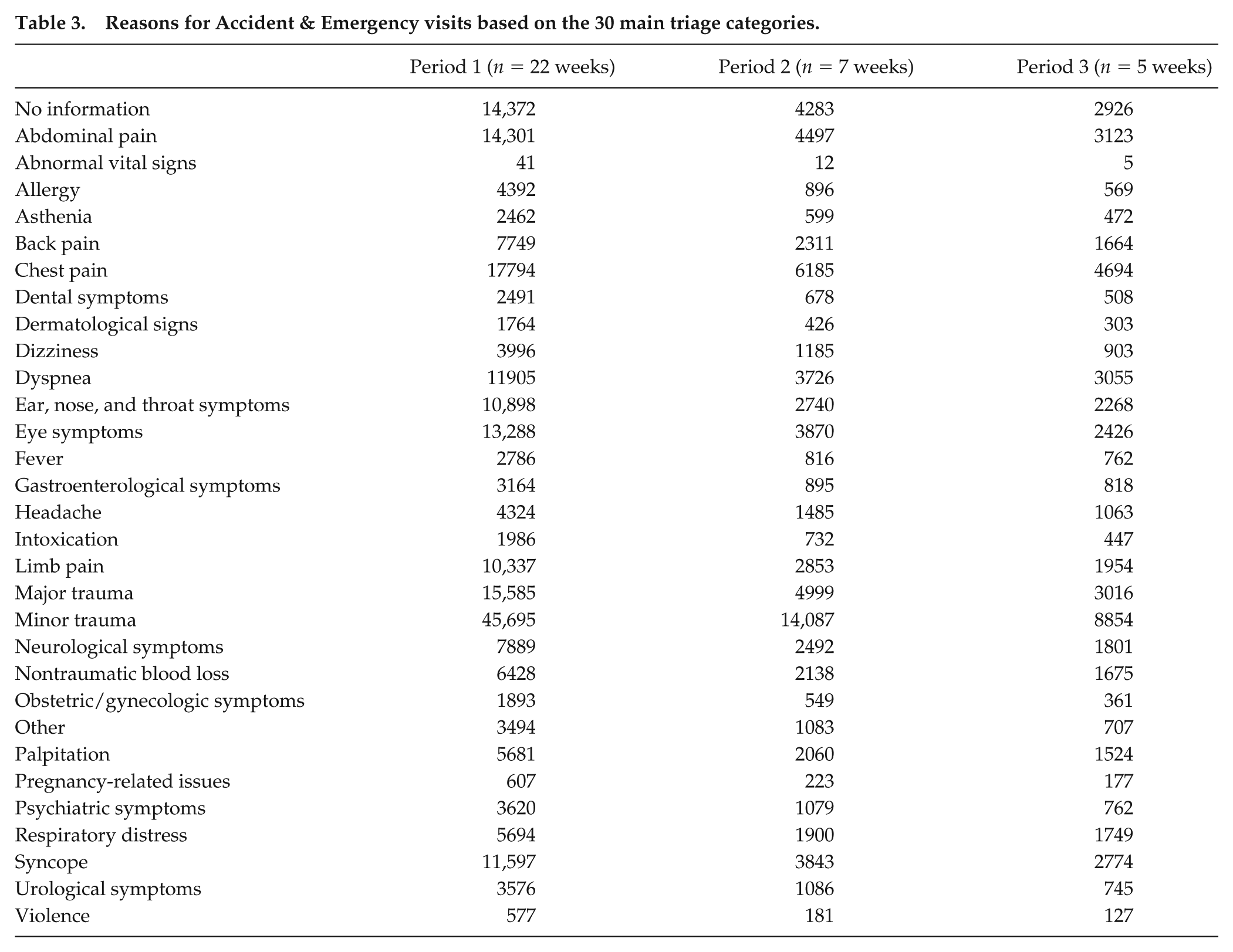
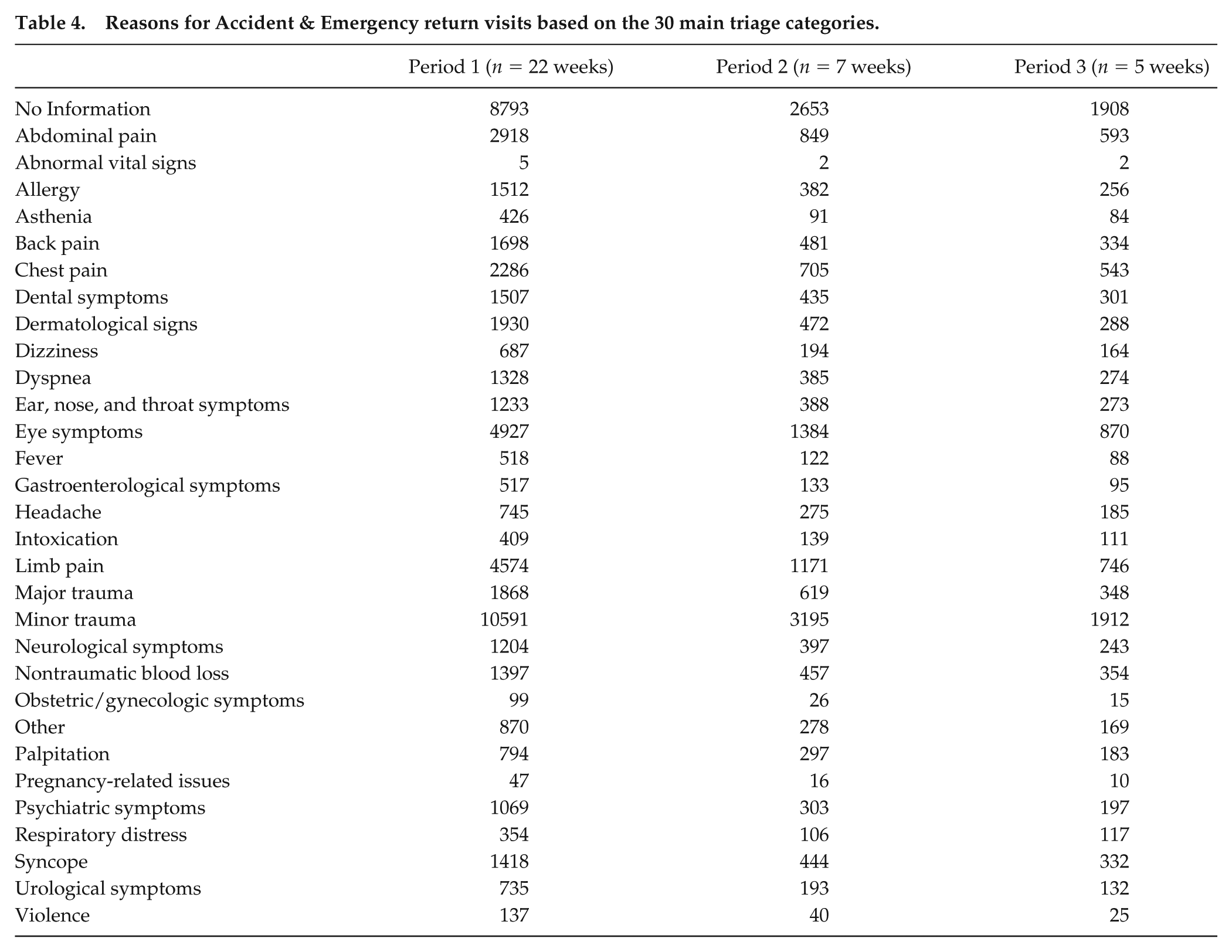
The relevant permission for retrospective data analyses was obtained from the Padova University Hospital Ethics Committee, and the following information was gathered for each patient/access via the QlikView Accident and Emergency software: triage color code assigned by the nursing staff upon arrival (white, no priority of risk/suffering; green, state of severe pain; yellow, risk of death or serious disability; red, acute alterations of vital functions). Where available, more specific summary, medical information was also obtained and categorized based on the main patient complaint, according to 30 main medical categories, as in use in the A&E Department of Padova University Hospital. Finally, outcome categories were obtained for each patient/access: discharged, does not answer/come back from referral, admitted, and deceased. The above information is summarized in Tables 1 and 3 for first visits and Tables 2 and 4 for return visits, by period.
Demographic characteristics, triage code severity, and outcomes of Accident & Emergency visits.
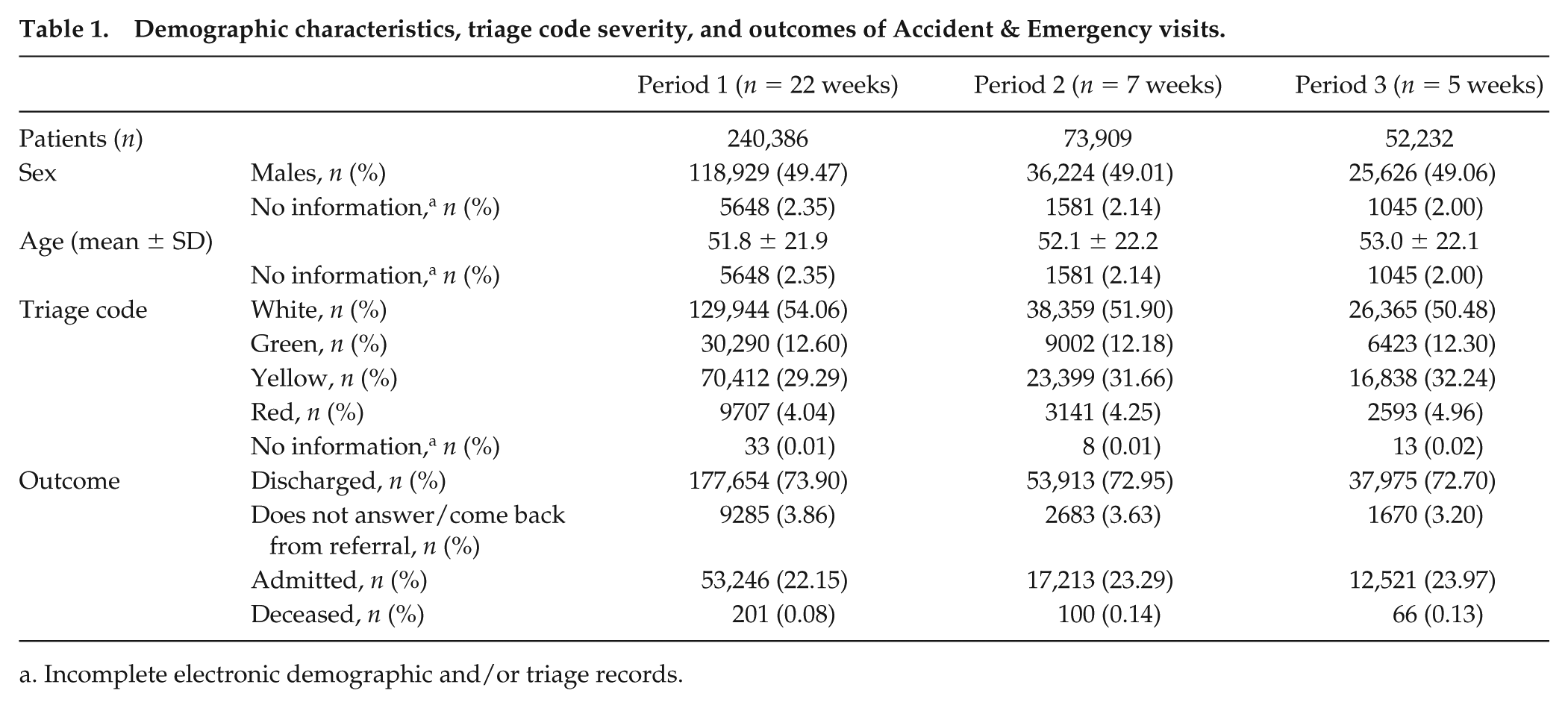
Incomplete electronic demographic and/or triage records.
Demographic characteristics, triage code severity, and outcomes of Accident & Emergency return visits.
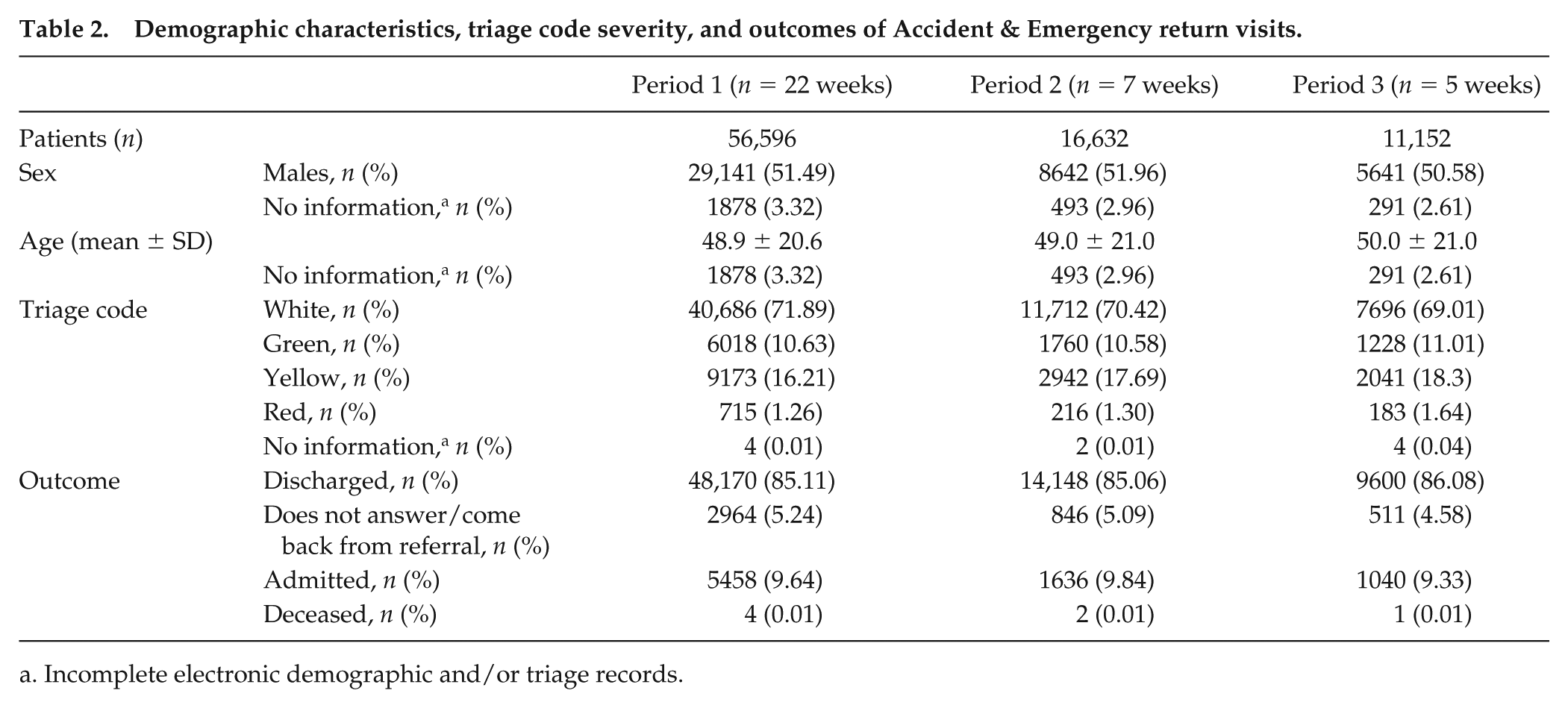
Incomplete electronic demographic and/or triage records.
Reasons for Accident & Emergency visits based on the 30 main triage categories.
Reasons for Accident & Emergency return visits based on the 30 main triage categories.
Visits and return visits were aggregated by day (with reference to DST) and cumulated over the years, according to triage color codes and outcomes. The variable week was set with reference to DST (week 0 = the week before the enforcement of DST within period 1 and the week before the return to winter time within period 2). Data counts were analyzed using generalized Poisson models and generalized additive models. Specifically, 3 Poisson models (Jones et al., 2013) were estimated using the total number of visits/return visits, the number of white color codes (among visits and return visits), and the number of discharged patients (among visits and return visits) as dependent variables, and the variable week as a covariate. Then, a second set of analyses was conducted using generalized additive models for Poisson data, to include photoperiod (i.e., day length) as an additional covariate specified nonparametrically as spline functions. Weekly photoperiods were obtained as the average of the daily difference between sunrise and sunset, based on United States Naval Observatory Department data (United States Naval Observatory [USNO] Astronomy Application Department. Rise, Set, and Twilight Definitions, http://aa.usno.navy.mil/faq/docs/RST_defs.php) for the years 2010 (periods 1 and 2) and 2011 (period 3): period 1, minimum photoperiod = 11.47 h, maximum = 15.68 h; period 2, minimum photoperiod = 9.10 h, maximum = 11.23 h; period 3, minimum photoperiod = 8.97 h, maximum = 10.28 h. The Wald test was used to test the significance of the coefficient of the covariate week, with week 0 as a reference. Analyses were confined to the most common triage code (white) and outcome (discharged) because the small number of frequencies of color codes other than white and outcomes other than discharges did not guarantee sufficient statistical power to adequately estimate the model coefficients. Similarly, the detected changes in relation to DST- versus non DST-enforced months were not large enough to allow for subanalyses, for example, in relation to sex and age. In addition, it is important to point out that differences in sex and age are expected in relation to severity codes and outcomes, as both sex and age are part of the triage code assignment (for example, chest pain receives a different code depending on age <45 or >45, because the likelihood of the pain being of cardiac origin changes with age) and impact on outcomes, with older patients being more likely to be admitted and to die. For purposes of data presentation, counts were aggregated using their sum within any given week. Data analyses were performed using the R software (https://www.r-project.org).
Results
Visits
The features and outcomes of A&E visits are presented in Tables 1 and 3. More than 50% of visits were triaged as white codes, and more than 70% of them resulted in discharges (Table 1).
An overall increase in the total number of A&E visits (approximately 30 [≅2.8%] extra cases per week per year) was observed over the DST-enforced months, which was statistically significant at weeks 4, 6, 7, and 9 to 12 compared with week 0 of period 1 (p < 0.01 for weeks 4 and 11 and p < 0.05 for weeks 6, 7, 9, 10, and 12; Fig. 1A). This was largely due to an increase in white codes (Fig. 1B). The number of white codes was significantly higher in weeks 4 to 18 compared with week 0 of period 1 (p < 0.01 for week 7 and p < 0.05 for weeks 4-6 and 8-18; Fig. 1B). Similar fluctuations were observed in discharges from A&E (Fig. 1C). The number of discharges was significantly higher in weeks 4, 6 to 13, and 15 to 18 compared with week 0 (i.e., the week before DST enforcement) of period 1 (p < 0.01 for weeks 13 and 18 and p < 0.05 for weeks 4, 6-12, and 15-17; Fig. 1C).
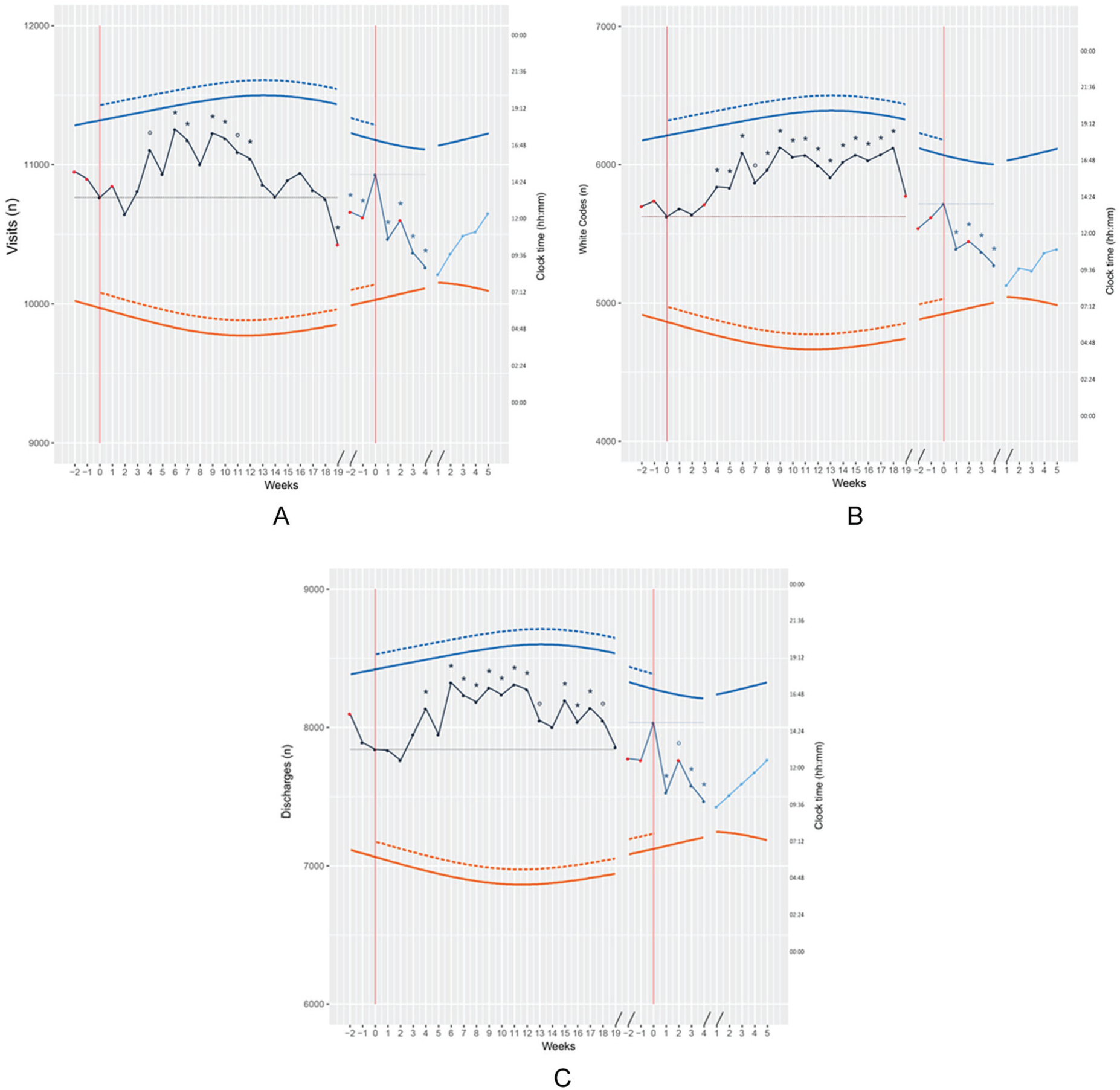
Total number of patients (left y-axis) attending Accident & Emergency (A&E) (A), being qualified as white triage codes (B) and being discharged from A&E (C) over periods 1 (black), 2 (dark blue), and 3 (light blue), by week (full circles). The two red lines/0 weeks mark the reference weeks prior to the enforcement of daylight saving time (DST; first 0, to the left of the x-axis) and prior to the return to winter time (second 0, to the right of the x-axis); consecutive, non DST reference weeks of period 3 are numbered progressively.
A more irregular pattern was observed after the return to winter time, with significantly lower absolute number of visits both before and after the switch to DST (p < 0.05; Fig. 1A). White codes and discharges were significantly lower on weeks 1 to 4 after the switch as compared with week 0 of period 2 (white codes: p < 0.05; Fig. 1B; discharges: p < 0.01 for week 2 and p < 0.05 for weeks 1, 3, and 4; Fig. 1C).
Once analyses were repeated, including photoperiod as a covariate, most of the changes detected in absolute number of visits, white codes, and discharges were no longer significant (Fig. 1A-C). Absolute numbers of visits, white codes, and discharges seemed to parallel photoperiod lengthening also in non DST reference period 3.
Return Visits
The features and outcomes of A&E return visits are presented in Tables 2 and 4. More than 70% of return visits were triaged as white codes, and more than 85% of them resulted in discharges (Table 2). A high discharge rate is expected for return visits, a proportion of which are scheduled by the doctor for review purposes or completion of investigations.
An overall, consistent increase in the total number of A&E return visits (approximately 25 [≅10%] extra cases per week per year) was observed after the enforcement of DST, which was significant at weeks 3, 5 to 15, and 17 compared with week 0 of period 1 (p < 0.01 for week 7 and p < 0.05 for weeks 3, 5, 6, 8 to 15, and 17; Fig. 2A). As in the case of first visits, this was largely due to an increase in white codes (Fig. 2B). The number of white codes was significantly higher in weeks 3, 5 to 6, 8 to 15, and 17 compared with week 0 of period 1 (p < 0.05; Fig. 2B). Similar fluctuations were observed in discharges from A&E (Fig. 2C). The number of discharges was significantly higher in weeks 3, 5 to 15, and 17 compared with week 0 (i.e., the week before DST enforcement) of period 1 (p < 0.05; Fig. 2C).
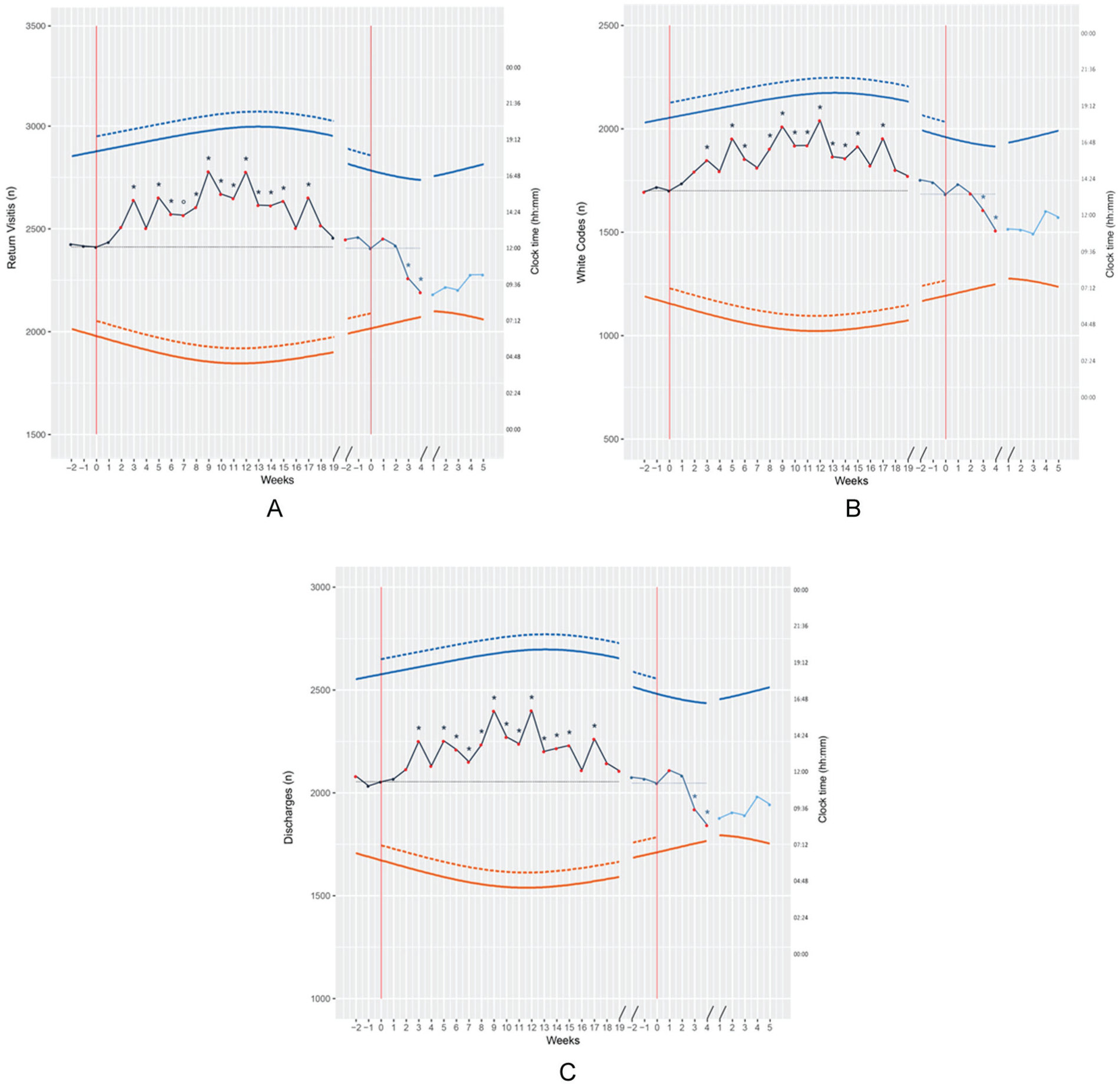
Total number of patients (left y-axis) reattending Accident & Emergency (A&E) (A), being qualified as white triage codes (B) and being discharged from A&E (C) over periods 1 (black), 2 (dark blue), and 3 (light blue), by week (full circles). The 2 red lines/0 weeks mark the reference weeks prior to the enforcement of daylight saving time (DST; first 0, to the left of the x-axis) and prior to the return to winter time (second 0, to the right of the x-axis); consecutive, non DST reference weeks of period 3 are numbered progressively.
After return to winter time, a decrease in the absolute number of return visits (approximately 25 [≅10%] cases less per week per year), white codes, and discharges was observed, which was significant at weeks 3 and 4 after the switch, as compared with week 0 of period 2 (p < 0.05; Fig. 2A-C).
Once analyses were repeated adding photoperiod as a covariate, virtually all the increases detected over the DST months in absolute number of visits (weeks 2-18), white codes (weeks 2-19), and discharges (weeks 2-19) remained significant (p < 0.05; Fig. 2A-C, full red dots on the plots). The same applied to the observed decreases in the absolute number of return visits (weeks 3-4), white codes (weeks 2-4), and discharges (weeks 3-4) after the return to winter time (p < 0.05; Fig. 2A-C).
Discussion
After the enforcement of DST, significant increases were observed in the total number of visits/return visits, the number of white (least severe) codes, and the number of discharges from A&E. In addition, the total number of return visits, and among them white codes and discharges, decreased after the return to winter time. When photoperiod was taken into account, most of the observed changes in A&E visits (and related white codes/discharges) were no longer significant. In contrast, they remained significant for return visits (and related white codes/discharges). Thus, both the enforcement of DST and photoperiod seemed to contribute to A&E access over the year.
It has been convincingly demonstrated that our circadian clock is predominantly entrained by the sun (and sun time) rather than by public time (Roenneberg et al., 2007; Hadlow et al., 2014). Mid-light (mid-dark) phases and midday (midnight) coincide in Greenwich and in any other place the longitude of which is a multiple of 15°, eastward or westward. In Padova, midday and midnight (non DST public time) occur approximately 13 min earlier compared with the respective sun time. This means that after the enforcement of DST, the difference between Padova sun time (which is key to daily synchronization of the endogenous circadian clock) and Padova DST public time (which we read on our watches) is of approximately 73 min. Such difference, which affects the population to a variable extent depending on both chronotype and photoperiod, may explain some of the observations presented in this study (Roenneberg et al., 2007; Hadlow et al., 2014). The effect may be further enhanced by the lengthening of the photoperiod over the summer months (Juda et al., 2013), despite differences in entrainment across seasons being limited in the modern artificial light-dark cycle (Wright et al., 2013; Stothard et al., 2017). The role of photoperiod may relate to the fact that longer daylight hours may favor a decision to access A&E (which may be logistically easier in the daylight) even for minor issues that tend to be triaged as white and to result in discharges. For example, an elderly patient may be more inclined to use public transport/their car to access A&E in the late afternoon and evening hours for a minor medical complaint, when there is still light outside. Future studies may address this hypothesis directly by studying A&E visits by time of the day. In our series, the enforcement of DST seemed to play a more relevant role in determining A&E return visits (and related white codes/discharges). However, it should also be pointed out that part of the differences between first and return visits after adjustment for photoperiod may relate to the fact that there was considerable variability in first visits over the DST months, while the behavior of return visits was more stable, possibly favoring the detection of statistically significant differences after adjustment for photoperiod.
While the available literature is neither broad nor conclusive, there is evidence that DST may have effects not unlike those of chronic, daily jet-lag east (Roenneberg et al., 2007; Hadlow et al., 2014), which leads to sleep deprivation (Tonetti et al., 2013) and to reported discomfort (Alencar et al., 2017). Cumulative sleep deprivation may explain the 3 to 4 weeks of lag observed in our study between the switch to DST and the change in absolute number of A&E return visits, white codes, and discharges. This is in line with the published observation that several weeks are needed for activity to adjust/re-entrain after the enforcement of DST (Kantermann et al., 2007). From a mechanistic point of view, sleep deprivation and general discomfort may determine an actual increase in the incidence of minor medical issues, leading to A&E return visits qualified as white codes and largely resulting in discharges. Alternatively, they may determine lower tolerance to minor medical conditions, leading to an increase in A&E return visits for white codes, which would not otherwise take place and which lead, in turn, to an increase in the number of discharges. Similar mechanisms could affect nurses’ and doctors’ decisions as well as patients’ attitudes, although this seems less likely to play a major role because A&E working shifts are highly irregular (Peters et al., 2015; Vetter et al., 2015). In addition, nurses’ and doctors’ decisions may affect only triage, outcomes, and prescribed return visits but not the absolute number of spontaneous return visits.
The study has a number of limitations. First, we did not acquire data for all weeks of the year, which would have completed the picture and provided useful information. However, all seasons were covered, and the issue was at least partly addressed by the inclusion of photoperiod within the model. Second, we had no control group with no exposure to DST, which could also help to distinguish between seasonal versus DST-related changes. While this group would have been useful, it may not be easily identified, as countries that do not adopt DST tend to have health systems that are not strictly comparable with the Italian one, with different A&E access patterns and A&E management strategies. Finally, power did not allow for analysis by day, which would have helped define the more acute effects of DST. An interesting study on this issue has been recently published and documents higher rates of road accidents on days 1 and 2 after the switch to DST (Robb and Barnes, 2018). This and other studies (Fan et al., 2016; Burke et al., 2015; Lim et al., 2016; Schuld et al., 2013) suggest that a whole host of mechanisms contribute to A&E access across the year. However, the overall, consistent increase in visits and return visits observed in our series over the spring/summer months, with such tight relationships with both the enforcement of DST/return to winter time and the changes in photoperiod, seems unlikely to be fully explained by completely different mechanisms. The findings are interesting also in terms of their potential health-economics implications. Cost analysis is beyond the aims and means of the present study but may be planned if similar studies are performed in the future, especially on a larger, multicenter, international scale. Such data would add to the debate on whether the enforcement of DST has health consequences and health costs that may outweigh its economic advantages.
Footnotes
Acknowledgements
This work was partly funded by a grant from the Italian Ministry of Health to Sara Montagnese (GR-2009-1604309) and by a National Research Council of Italy grant (EPIGEN Progetto Bandiera Epigenomica, subproject 4) to Rodolfo Costa. Giovanni Frighetto and Matteo Turco were also partly funded by a grant from the Italian Ministry of Health to Sara Montagnese (GR-2009-1604309).
Conflict of Interest Statement
The authors have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.