
Abstract
Deficits in cognitive functioning associated with shift work are particularly relevant to occupational performance; however, few studies have examined how cognitive functioning is associated with specific components of shift work. This observational study examined how circadian phase, nocturnal sleepiness, and daytime insomnia in a sample of shift workers (N = 30) were associated with cognitive flexibility during the night shift. Cognitive flexibility was measured using a computerized task-switching paradigm, which produces 2 indexes of flexibility: switch cost and set inhibition. Switch cost represents the additional cognitive effort required in switching to a different task and can impact performance when multitasking is involved. Set inhibition is the efficiency in returning to previously completed tasks and represents the degree of cognitive perseveration, which can lead to reduced accuracy. Circadian phase was measured via melatonin assays, nocturnal sleepiness was assessed using the Multiple Sleep Latency Test, and daytime insomnia was assessed using the Insomnia Severity Index. Results indicated that those with an earlier circadian phase, insomnia, and sleepiness exhibited reduced cognitive flexibility; however, specific components of cognitive flexibility were differentially associated with circadian phase, insomnia, and sleepiness. Individuals with an earlier circadian phase (thus more misaligned to the night shift) exhibited larger switch costs, which was also associated with reduced task efficiency. Shift workers with more daytime insomnia demonstrated difficulties with cognitive inhibition, whereas nocturnal sleepiness was associated with difficulties in reactivating previous tasks. Deficits in set inhibition were also related to reduced accuracy and increased perseverative errors. Together, this study indicates that task performance deficits in shift work are complex and are variably impacted by different mechanisms. Future research may examine phenotypic differences in shift work and the associated consequences. Results also suggest that fatigue risk management strategies may benefit from increased scope and specificity in assessment of sleep, sleepiness, and circadian rhythms in shift workers.
Keywords
As the work force becomes more globalized, so does the demand for a 24-h work force. An estimated 1 in 5 workers worldwide are engaged in night shift work (McMenamin, 2007; US Bureau of Labor Statistics, 2014), which often include safety-sensitive operations such as law enforcement, transportation, and health care. Because humans are typically diurnal, the night shift schedule requires workers to operate against their endogenous circadian rhythms (i.e. working during the biological night when sleep is physiologically anticipated). Although some shift workers spontaneously demonstrate complete circadian adjustment to their nocturnal work schedule, the majority of night shift workers show incomplete circadian adjustment (Folkard, 2008) and therefore experience adverse consequences to health, performance, and safety.
Among the numerous consequences of circadian misalignment in shift work, deficits in cognitive functioning are particularly relevant to occupational performance. Compromised cognitive functioning not only reduces productivity but also increases risk for injuries or fatalities in safety-sensitive operations. Despite the importance of undiminished cognitive functioning in the 24-h workplace, the range of deficits associated with circadian misalignment in shift work has not been completely delineated.
Existing research has focused on vigilance as measured by the psychomotor vigilance task, with results showing increased attentional lapses and slowed reaction time during the biological night (Horowitz et al., 2003; Graw et al., 2004; Van Dongen and Dinges, 2005). These studies often utilize a simulated shift work paradigm using day workers, which presents some limitations. While it effectively induces circadian misalignment in day workers, a simulated shift work paradigm may be limited in its generalizability to actual night shift workers due to self-selection, attrition, and so forth. Furthermore, the circadian misalignment produced in simulated shift work paradigms is acute, and the effects of circadian misalignment over time have not yet been examined. As fixed night shift workers are engaged in night work for long periods, it is unknown whether shift workers have the opportunity to habituate, develop compensatory mechanisms, or accumulate deficits over time.
There is evidence that components of cognitive functioning other than vigilance and cognitive speed (e.g., selective attention, visual search) may also be impacted by circadian misalignment and its associated symptoms (Horowitz et al., 2003; Santhi et al., 2007, 2008). One recent study indicated that the neurobiological process of directing and orienting attention may be adversely impacted in shift workers who are unadjusted to the nocturnal work schedule (Gumenyuk et al., 2014). This study examined cognitive function via event-related potentials during an attention reorientation task in a sample of fixed night shift workers with and without symptoms of nocturnal sleepiness and daytime insomnia. Results revealed that symptomatic night shift workers, who also demonstrated increased circadian misalignment, exhibited slowed reaction times and decreased neuronal activity in trials with distractors relative to asymptomatic night shift workers. This suggests that sleepiness, insomnia, and circadian misalignment in night shift workers may be associated with specific patterns of impaired task performance as a consequence of deficits in maintaining focus and flexibly shifting attention.
Among the various components of executive functioning, cognitive flexibility is particularly relevant to occupational performance and shift work. Occupational settings often require workers to monitor the environment for various stimuli and information, each of which may require a different response. For example, nurses on the night shift may need to respond to different diagnostic or therapeutic information in addition to the patients’ emotional, behavioral, and physiological states in order to provide appropriate care. Such flexibility not only increases patient satisfaction but also enhances the effectiveness of health care interventions (Leach, 2005).
Cognitive flexibility also enables effective adaptation to a dynamic environment. This is critical to workers engaged in safety-sensitive operations such as emergency responders, security personnel, or chemical plant operators, all of whom routinely work in shifts to maintain 24-h operations. The environment in safety-sensitive operations can be prone to abrupt changes and therefore requires not only sustained vigilance but also the ability to flexibly switch attention from one task to another in an accurate and effective manner. Efficiency and flexibility of performance is critical in these contexts because delayed responses can dramatically impact outcome (e.g., fatalities, severity of injuries, etc.).
Cognitive flexibility may also be particularly relevant to the night shift because of a reduction in personnel relative to the work demand. Both state- and nationwide surveys of hospital staffing (Sochalski, 2001; Cavouras and Suby, 2003) have indicated that night shift nurses had higher average patient loads than day shift nurses. For example, the nurse-to-patient ratio on a medical-surgical unit was 1:6 for day shift nurses, with 23% reporting larger than average patient loads (7-12 per shift). This is contrasted with a 1:7 ratio for night shift nurses, with 34% (11% more than the day shift) reporting larger than average patient loads (8-12 per shift). The same trend was reported for nurses on critical care units (Cavouras and Suby, 2003). In addition, the percentage of care hours have also been shown to be higher in night versus day nurses (de Cordova et al., 2014). The larger work load for night shift workers likely translates to increased multitasking and therefore greater demand for cognitive flexibility.
The lack of cognitive flexibility that accompanies fatigue can have devastating results in the workplace, as was observed at the BP America Refinery in Texas City, Texas, where explosions and fires killed 15 people and injured another 180 in March 2005. Although this disaster occurred during daytime hours and was consequential to multiple problems, the US Chemical Safety Board concluded that a lack of cognitive flexibility was a contributing cause. Sleepiness and fatigue among the chemical operations personnel (several of whom had been working 12-h shifts for 29 or more consecutive days) likely contributed to cognitive fixation on the symptoms rather than the underlying cause of the problem (US Chemical Safety Board, 2007).
Cognitive flexibility is commonly measured using a task-switching paradigm (Mayr and Keele, 2000; Whitmer and Banich, 2007), which produces 2 indexes: switch cost and set inhibition. The switch cost represents the additional cognitive effort required in switching to a different task compared to repeating the same task. Larger switch costs indicate less cognitive flexibility because more effort is required to switch tasks. Set inhibition represents performance when returning to prior tasks compared to switching to a different task. Set inhibition may lead to deficits in performance in 2 opposing ways: (1) prior tasks may be inadequately suppressed, or (2) prior tasks may take additional effort to reactivate. When prior tasks are inadequately suppressed, they continue to occupy working memory, thereby increasing cognitive load and decreasing performance on new tasks (e.g., increased errors). Conversely, inefficient reactivation of prior tasks can also be problematic when that task is repeated during the work flow.
The present study aimed to further delineate cognitive deficits (beyond overall accuracy and reaction time) that are associated with circadian phase, nocturnal sleepiness, and daytime insomnia in fixed night shift workers. This study specifically examined cognitive flexibility using a task-switching paradigm. To increase ecological validity, the task was modified for identification of relevant social information using facial stimuli instead of geometric shapes (e.g., Cheng et al., 2015). Given evidence of the adverse effects of circadian misalignment on cognitive functioning, we hypothesized that an early circadian phase would be associated with (1) less cognitive flexibility, as indexed by larger switch costs, and (2) set inhibition scores that indicate either difficulties with cognitive suppression (negative set-inhibition scores) or cognitive reactivation (positive set-inhibition scores). Finally, we also explored the impact of switch cost and set inhibition on general performance outcomes (type of errors, overall accuracy, and task efficiency).
Materials and Methods
Participants
Participants were recruited as part of a larger observational study examining the association between shift work and cardiometabolic risk, and we thus targeted shift workers without a history of heart disease or diabetes. Recruitment was conducted primarily through flyers distributed in the community and a health system–wide newsletter, which sampled across 6 major hospitals serving the greater Detroit metropolitan area. A total of 125 prospective participants completed an initial Internet-based prescreening survey, and 40 eligible participants were invited for an in-person interview. During the interview, participants provided information about their shift work and sleep schedules and completed the Structured Clinical Interview for DSM Disorders, conducted by a doctoral-level clinical psychologist. The final sample (N = 30) included 22 women and 8 men with a mean age of 38.8 ± 10.27 years (range, 24-57). All procedures were approved by the Henry Ford Health System institutional review board, and all participants provided informed consent prior to study participation.
Study inclusion required working a fixed night shift work schedule, which was operationalized as starting between 1800 and 0300 h, with shifts lasting between 6 and 12 h. Inclusion of 1800 in the start time was targeted for individuals working 12-h shifts (e.g., 1800 to 0600), and schedules that were better characterized as the afternoon/evening shift (i.e., second shift) were excluded. In addition, work shifts must have occurred at least 3 nights per week for a minimum of 1 year. Participants must have reported habitual time in bed between 6 and 9 h to preclude inadequate sleep opportunity as a confounding variable. Study exclusion was based on a medical history of diabetes, hypertension, central nervous system disorders, liver conditions, sleep disorders, or a current body mass index ≥35. Use of substances that may interfere with any outcome measures in the larger study (sleepiness, circadian phase, blood pressure, cortisol, glucose tolerance) also resulted in study exclusion; these included dependence on alcohol use (≥4 beverages per day), heavy tobacco use (≥10 cigarettes per day), recreational drug use, oral contraceptive use, medications impacting central nervous system functioning, and caffeine use in excess of 5 to 6 servings (approximately 600 mg) per day.
Procedures
Participants were instructed to arrive at the laboratory at 0730 following a night shift, and they completed symptom questionnaires (see below) prior to an 8-h in-laboratory sleep opportunity between 0830 and 1630. Lights-on (lux < 10) was strictly enforced at 1630. Upon awakening, participants remained in the laboratory for 24 h, with hourly saliva samples assayed for melatonin (see the circadian phase section below). The larger protocol assessed for alertness, cardiovascular functioning, and glucose tolerance throughout the 24 h. Cognitive flexibility was measured at 0500 (11.5 h following wake time), which also corresponds to the latter portion of most night shifts.
Questionnaires
Insomnia symptoms were assessed using the Insomnia Severity Index (ISI) (Bastien et al., 2001). Because shift workers intermittently engage in both daytime and nighttime sleep, insomnia during both daytime and nighttime was assessed separately (Gumenyuk et al., 2015). Self-report nocturnal sleepiness was assessed using the Epworth Sleepiness Scale (ESS) (Johns, 1991), with instructions modified for nocturnal sleepiness (Gumenyuk et al., 2015).
Objective Sleepiness
In addition to the ESS, objective nocturnal sleepiness was also assessed using the standard Multiple Sleep Latency Test (MSLT) (Carskadon et al., 1986). Electrode integrity was checked by visual inspection via biocalibration before each nap. A total of 5 naps were included. Naps started at 2300 and were repeated every 2 h, with the last nap occurring at 0700. The MSLT was terminated upon 4 epochs (2 min) of stage 2 sleep.
Circadian Phase
The daily rhythm of melatonin secretion is a reliable marker for circadian phase (Lewy and Sack, 1989) and was assessed via dim light melatonin onset (DLMO) based on hourly salivary samples for a total period of 24 h consecutively. Samples were collected in a private and sound-attenuated room under constant dim light (<10 lux). During saliva collection, all participants were asked to remain seated in a comfortable chair until adequate collection of saliva was verified. No food or drinks were allowed 10 min prior to saliva sample collection, and food items that may interfere with melatonin assays, such as banana and mustard, were precluded from participants. Between hourly samples, subjects were allowed to partake in approved activities, such as reading or listening to music. Use of electronics was permitted if backlit screens were maintained at ≤10 lux (based on angle of gaze). DLMO was determined using a relative threshold based on 25% of the maximum melatonin concentration, defined as an average of the 5 highest consecutive melatonin values. Linear interpolation was used to estimate the time at which melatonin concentration surpassed the threshold.
Saliva samples were collected using a Salivette tube (Sarstedt AG & Co.) with a cotton insert. Participants were instructed to place the cotton insert in their mouth by the salivary glands underneath the tongue with the goal of saturating the cotton insert with saliva. Duration of salivary collection started at 2 min but was increased if the sample produced did not meet the minimum amount for analysis. Each sample was weighed to ensure a minimum of 0.5 g of saliva before it was centrifuged and frozen. Samples were submitted to SolidPhase Inc. to be radioimmunoassayed for melatonin.
Cognitive Flexibility
Participants completed a computerized task-switching paradigm, which was adapted from previous studies (Cheng et al., 2015). The task was completed at 0500, which corresponds to the latter portion of the shift for most night shifts. In this task, participants were presented with faces serially. Prior to stimulus onset, participants were provided with a cue that instructed them to identify either the sex (male or female), race (black or white), or emotional expression (happy or neutral) of the facial stimulus. Participants pressed either the “d” key if the stimulus was male, white, or happy or the “k” key if the stimulus was female, black, or neutral (see Figure 1). Practice trials were provided until the participants felt acclimated to the paradigm. All incorrect trials were indicated with the word “incorrect” on the screen following the response. Participants completed 4 blocks of 42 trials with 10-sec breaks between each trial.
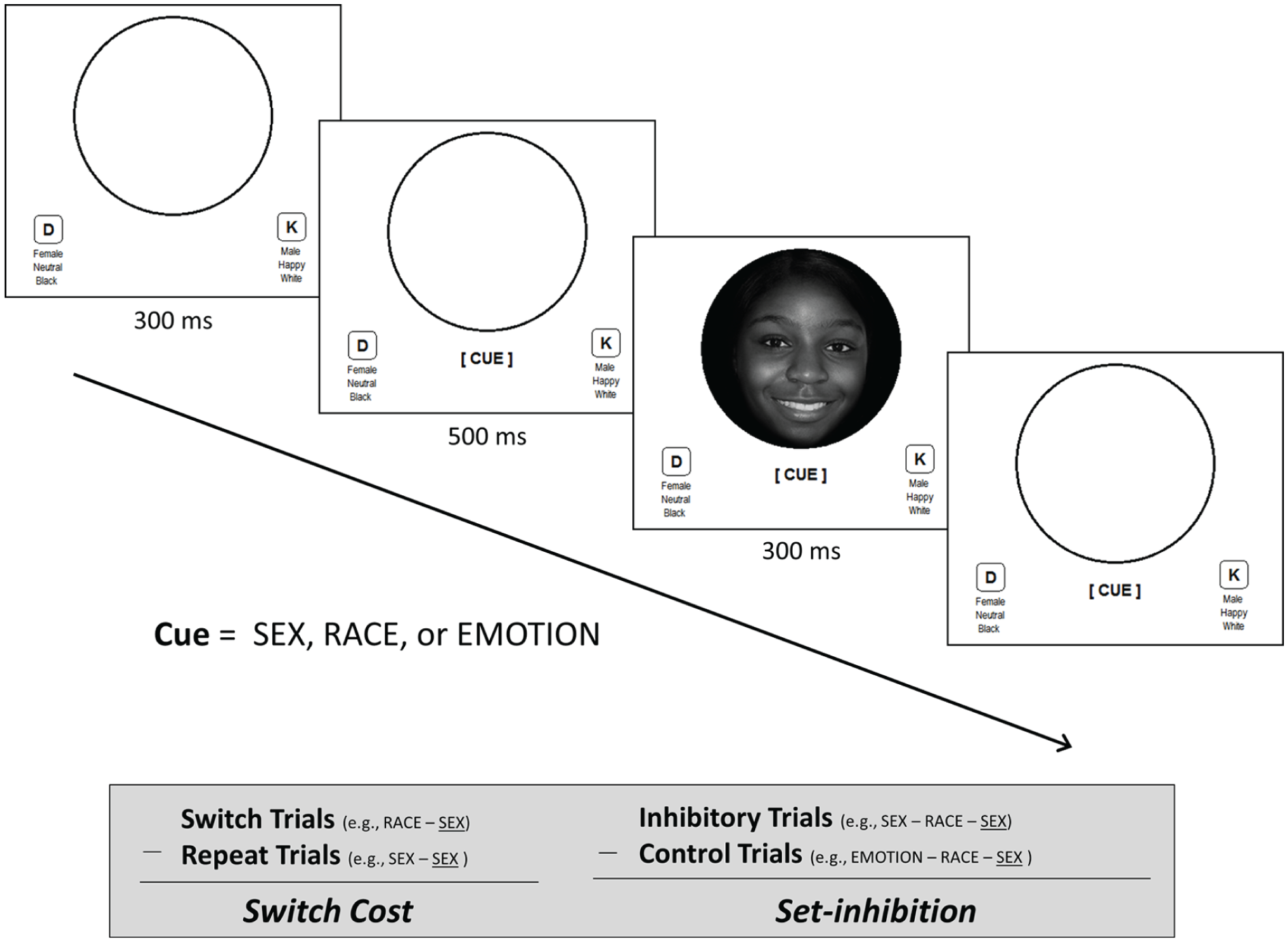
Schematic of the task-switching paradigm.
Switch Cost
The efficiency of switching from one task to a different task can be described by a switch cost. When the same task is performed in succession (i.e., repeat trials), reaction time between the 2 tasks should be comparable. However, when the task changes (i.e., switch trials), reaction time to the new task should be longer than the old task due to the effort required in replacing the old task rule with the new task rule. The switch cost is calculated by subtracting the reaction time of the repeat trials from the switch trials, and the resulting value represents the magnitude of the additional cognitive effort required to switch to a different task (above and beyond overall reaction time).
Set Inhibition
Cognitive flexibility is also influenced by how efficiently one can return to previous tasks when they are repeated in the work flow. Inadequate suppression of previous tasks may impact performance on the new task due to increased cognitive load. In contrast, inefficient reactivation of previous tasks can also be problematic for task performance. Both types of deficits are measured by a set-inhibition score. For a series of 3 tasks, 2 trials of the same task separated by one trial of a different task (e.g., sex/race/sex) were categorized as inhibitory trials, whereas 3 trials of disparate tasks (e.g., emotion/race/sex) were categorized as control trials. The set-inhibition score was calculated by subtracting the average reaction time on control trials from inhibitory trials. The resulting value represents the type and degree of deficits in returning to previous trials (above and beyond baseline switch costs). Ideally, performance on inhibitory trials should be comparable to control trials (set-inhibition score of zero) to maximize fluidity between tasks. Positive scores indicate faster performance on inhibitory trials than switch trials, suggesting difficulties with cognitive suppression of previous tasks rules. Negative scores suggest that additional cognitive effort was required to reactivate the previous task (Mayr and Keele, 2000).
Task Performance
In addition to switch cost and set inhibition, general measures of task performance were also examined in order to delineate the relationship with cognitive flexibility. Accuracy and efficiency were included as common measures of performance.
Accuracy was operationalized as the percentage of correct trials among all 168 trials. Given the expectation that reduced cognitive flexibility might lead to deficits in reorienting to a new task, errors were categorized as either perseverative or nonperseverative. Perseverative errors were operationalized as the number of erroneous responses that would have been accurate for the previous task (e.g., continuing to engage in race identification when the task has shifted from race to sex identification). Task efficiency was defined as time to task completion, which was operationalized as an aggregate of reaction time across all 168 trials.
Statistical Analyses
Exploratory analyses were conducted using linear regression in order to examine how switch cost and set inhibition were associated with more general indicators of task performance, including speed and accuracy. The first hypothesis was tested using multiple linear regression with switch cost as the dependent variable, and MSLT (sleepiness), raw ISI scores (insomnia), and DLMO (circadian phase) as independent variables entered simultaneously in the model.
Based on evidence demonstrating the nonlinearity of set inhibition (see the set inhibition and task performance section below), we considered 3 different models (absolute value transformation, linear, and logistic) for describing the relationship between set inhibition and circadian phase, sleepiness, and insomnia. The fit (based on McFadden’s R2) of the logit model (R2 = 0.37) surpassed the fit of either a linear model (R2 = 0.31) or a model using an absolute value transformation (R2 = 0.26). As such, a logistic regression was conducted using negative (cognitive suppression) or positive (cognitive reactivation) scores as the binary outcome variable and nocturnal MSLT, daytime ISI, and circadian phase as predictors.
Results
Sample Characteristics
A total of 30 fixed night shift workers (22 women) participated, with a mean age of 38.8 ± 10.3 years (range, 24-57). Participants worked an average of 3.9 shifts a week (range, 3-7) and have been on the night shift for an average of 6.6 ± 5.6 years (range, 1-24 years). Shift start times ranged from 1800 to 2400, and shift end times ranged from 0500 to 0800. Shift duration ranged from 8 to 12 h and lasted an average of 10.7 h (see Table 1 for summary statistics of demographic and experimental variables). Participants slept for an average of 6.93 ± 0.98 h in the laboratory prior to the experimental procedures. Average DLMO was at 2242 h, with skewness (−0.15) and excess kurtosis (−0.17) values falling within the range of normal distribution. Earlier DLMO (and thus increased circadian misalignment) was associated with a significant increase in excessive nocturnal sleepiness (r = −0.38, p < 0.05) and daytime insomnia (r = −0.36, p = 0.05). Age, sex, or number of years on the night shift were not significantly associated with primary outcome variables (switch costs, set-inhibition scores) or predictors (DLMO, sleepiness, insomnia), and were tested in initial models as covariates but were ultimately excluded in the final models due to nonsignificance.
Demographic and experimental variables.
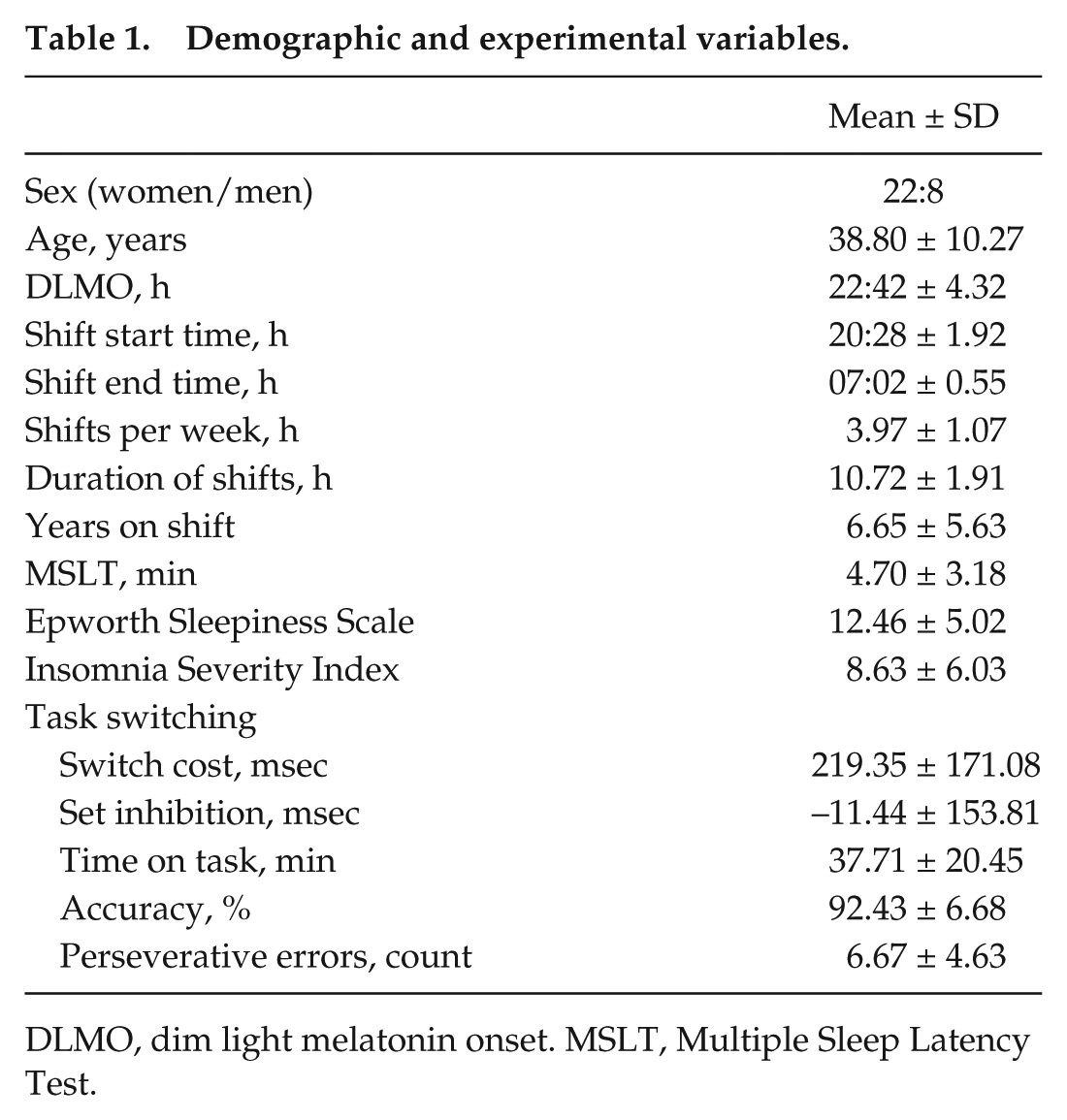
DLMO, dim light melatonin onset. MSLT, Multiple Sleep Latency Test.
Switch costs and set-inhibition scores across the sample were examined to ensure that the measures of cognitive flexibility were detected in this task. The average switch cost (switch trials minus repeat trials = 219.35 ± 171.08 msec) differed significantly from zero, t(29) = 7.02 (p < 0.001), demonstrating the effectiveness of this method for measuring switch costs. Set inhibition was examined as a bidimensional factor, with negative scores (n = 14) measuring efficiency in cognitive suppression, and positive scores (n = 16) measuring efficiency of cognitive reactivation. Mean positive set-inhibition scores (mean 102.01 ± 93.50 msec) differed significantly from zero (p < 0.001), as did the mean negative set-inhibition scores (mean −141.01 ± 93.50 msec, p < 0.001).
Examination of the relationship between cognitive flexibility and mean reaction time demonstrated that these were independent constructs. While switch costs correlated with mean reaction time at a low to moderate strength (r = 0.31), this did not reach statistical significance (p = 0.09). Set-inhibition scores showed no relationship with mean reaction time (r = −0.06). Overall, these findings indicate that the measures of cognitive flexibility in this study provide additional information beyond overall reaction time.
Switch Cost and Task Performance
No significant relationships were detected between switch cost and accuracy, either for perseverative or nonperseverative errors. Switch cost alone was a marginally significant predictor of time to task completion (β = 0.32, p = 0.08) and was significant when accuracy was entered into the model in order to account for the speed/accuracy tradeoff (β = 0.38, p < 0.05). Based on model prediction, time to task completion doubled from 28 to 56 min at a switch cost of 556 msec, which fell within the range of switch costs detected in this sample (max = 577 msec).
Set Inhibition and Task Performance
Because of the bidimensional aspect of set inhibition, examination of set inhibition and task performance included set inhibition as both a linear and quadratic predictor in order to describe any nonlinear relationships. Results indicated that set-inhibition scores deviating from zero (i.e., in both positive and negative directions) were significantly associated with reduced accuracy (β = −0.38, p < 0.05). This effect was strongest for perseverative errors (β = 0.45, p < 0.05), while the relationship between set inhibition and nonperseverative errors was only trending toward significance (β = 0.33, p = 0.08). Set inhibition was also not significantly associated with time to task completion, and no significant linear relationships were detected.
Cognitive Flexibility, Circadian Phase, Insomnia, and Sleepiness
Switch Cost
As predicted, results indicated that circadian phase was a unique predictor of switch cost above and beyond symptoms of sleepiness and insomnia. Specifically, earlier DLMO was associated with significantly larger switch costs (β = −0.66, p < 0.01; see Figure 2), with the β coefficient indicating a large effect size. The unstandardized beta coefficient indicated that a 1-h advance in DLMO resulted in an increase of 15.89 msec in switch cost. Nocturnal MSLT also appeared to be significantly associated with switch cost, although in the opposite direction as expected (greater alertness associated with greater switch costs); upon further inspection, this was designated a suppressor effect because it met all criteria of classical suppression (Pandey and Elliott, 2010). Neither MSLT nor ISI was independently correlated with switch cost, whereas DLMO was (r = −0.40, p < 0.05). Furthermore, a post hoc analysis replacing the MSLT with the ESS in the model also revealed a significant effect of circadian phase (β = −0.52, p < 0.05) and no significant effect of nocturnal sleepiness or daytime insomnia. Taken together, the effect of MSLT was treated as spurious and the interpretation relied on the model with the ESS as a measure of sleepiness instead.
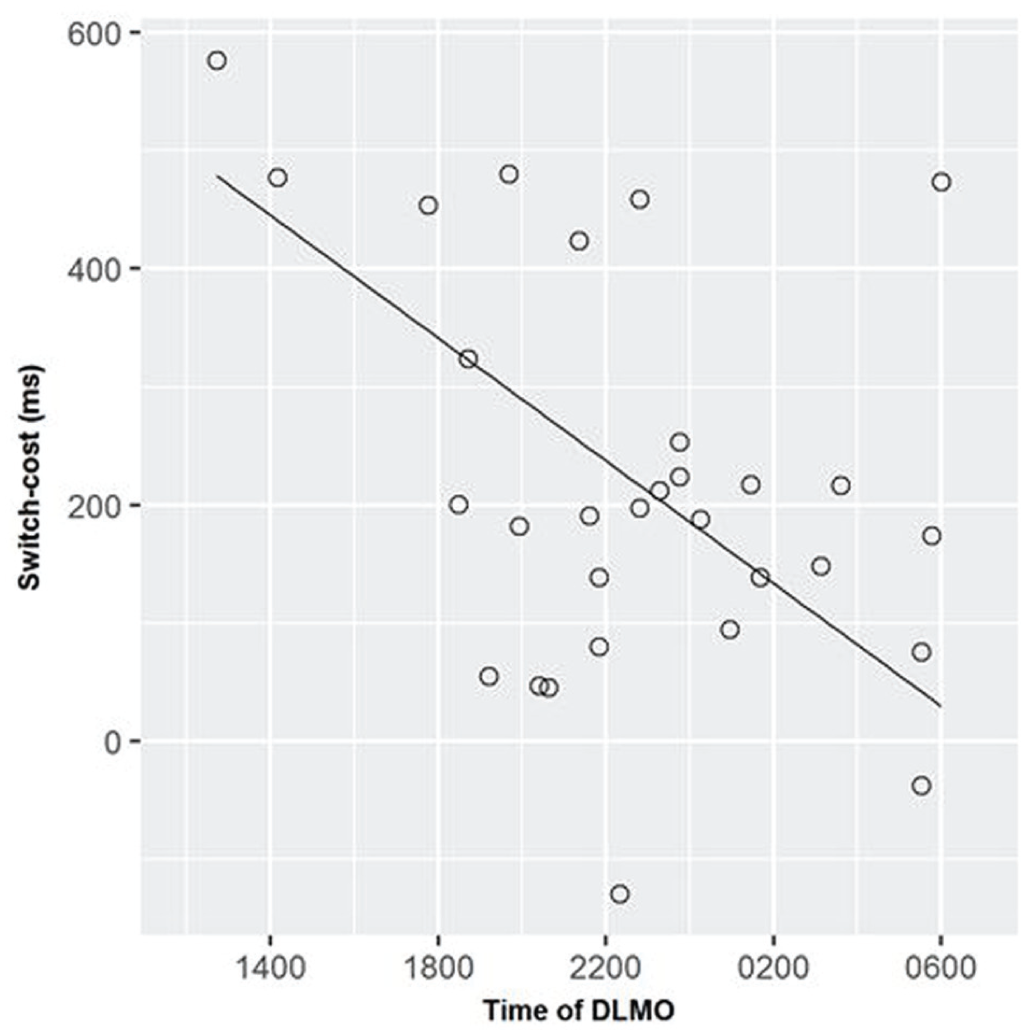
Circadian phase as a predictor of switch cost (task performance at 0500).
Set Inhibition
Based on the likelihood ratio test on the logistic regression model, both nocturnal MSLT and daytime ISI scores were significant predictors of the type of set-inhibition deficit, whereas circadian phase was not a significant predictor. Increasing daytime ISI was associated with higher odds of exhibiting deficits related to reduced cognitive suppression (adjusted odds, 3.45; 95% confidence interval [95% CI]. 1.21, 13.07; p < 0.05). Alternatively, increasing nocturnal sleepiness was associated with higher odds of exhibiting deficits related to inefficient cognitive reactivation (adjusted odds, 4.67; 95% CI, 1.33, 17.62; p < 0.01). Post hoc analysis replacing the MSLT with the ESS revealed the same results. Furthermore, both ISI and MSLT were independent predictors of the type of set-inhibition deficit, whereas circadian phase was not.
Discussion
This study aimed to extend our knowledge of neurobehavioral processes that are sensitive to circadian phase, sleepiness, and insomnia. This study provides novel evidence that shift workers who are maladjusted to the night shift schedule experience deficits in cognitive flexibility in addition to well-documented deficits in sustained attention and processing speed. Furthermore, results also suggest that specific domains of cognitive flexibility are differentially associated with circadian phase in relation to the work schedule versus symptoms of nocturnal sleepiness and daytime insomnia, which have implications for improving occupational performance and safety.
Switch Cost
Results pertaining to switch costs indicate that the ability to flexibly orient to a new task is more strongly associated with the circadian phase versus sleepiness and insomnia symptoms. This is consistent with prior research showing that overall cognitive functioning is sensitive to variations in circadian rhythms, including sustained attention as measured by the psychomotor vigilance test (Horowitz et al., 2003; Valdez et al., 2010) and selective attention as measured by the Stroop and Simon tasks (Bratzke et al., 2012). The results suggest that circadian phase might be a stronger candidate mechanism than symptoms of sleepiness or insomnia in explaining larger switch costs in shift workers. A likely explanation might be a downregulation of biological resources allocated toward cognitive performance during the biological night when sleep is physiologically anticipated. Efficient neuronal activity is metabolically expensive and therefore only diverted when needed (Harris et al., 2012).
While this study did not include day workers as a comparison group, the switch cost found in this sample was considerably larger than switch costs found in previous task-switching experiments in the general population. Prior studies in healthy adults have found switch costs of 123 msec (Cheng et al., 2015), 100 msec (Whitmer and Banich, 2007), and 127 msec (Mayr and Keele, 2000). In contrast, the switch cost found in this sample of night shift workers was 219 msec; however, results also indicated that those with the most delayed circadian phase (DLMO around 6 AM), and were therefore most adjusted to the night shift, had an average switch cost of 103 msec, which is comparable to results found in the general population. Taken together, these data suggest that maladjusted night shift workers may demonstrate reduced cognitive flexibility relative to the general population, particularly in the latter portion of a typical night shift, replication of these results should be conducted in a controlled experimental study. Future research may also examine whether cognitive flexibility can be improved by delaying the circadian phase to better match the night shift schedule. Given evidence that the cognitive deficits associated with shift work increase with exposure to shift work and can persist for years following the conclusion of shift work (Marquié et al., 2015), early detection and intervention of vulnerable individuals may significantly impact the health and longevity of shift workers.
The increased switch costs found in this study might have important implications for occupational performance. Results demonstrated that higher switch costs led to reduced task efficiency, as evidenced by increased duration of task completion. A switch cost of approximately half a second resulted in a 2-fold increase in time to task completion. This has implications for multitasking because evidence suggests that multitasking may actually manifest as serial and rapid task switches, particularly if the task requires the same domains of functioning (Fischer and Plessow, 2015). The reduction in cognitive flexibility could reduce worker efficiency below that of day shift workers, particularly if the workload-to-personnel ratio on the night shift is higher (Sochalski, 2001; Cavouras and Suby, 2003; de Cordova et al., 2014).
In addition to the cumulative effect of switch costs, there are also circumstances in which milliseconds of time are crucial to task performance. For example, police officers often rely on visually identified information for use-of-force decisions (e.g., discharging a firearm at a suspect), and increased switch costs would delay reaction times and elevate risk for otherwise preventable injuries and fatalities. Similarly, highway driving is also sensitive to millisecond delays; a half-second delay in switching from tuning the radio to watching the road might amount to a loss of 52 feet (15.9 meters) in braking distance when traveling at 70 miles per hour (31.3 meters per second), which accounts for approximately 20% of the recommended braking distance.
Set Inhibition
Results pertaining to set inhibition indicate that the ability to flexibly return to a previously performed task is not associated with the circadian phase and is instead differentially associated with symptoms of sleepiness and insomnia. This is consistent with evidence that inhibitory control might not be primarily impacted by circadian rhythms (Bratzke et al., 2012). Convergent evidence examining working memory capacity (measured by the n-back task) also shows minimal variation by circadian phase (Lo et al., 2012), which is relevant to the current findings because set inhibition involves suppression and reactivation of prior tasks in working memory.
Findings from this study show that task performance deteriorates with larger negative or positive set-inhibition scores. Individuals with larger negative set-inhibition scores return to a previously inhibited task faster than switching to a new task, suggesting that the previous task was inadequately inhibited and therefore continued to occupy working memory resources. Greater symptoms of insomnia were associated with a negative set-inhibition score, which is consistent with research demonstrating deficient inhibition in insomnia (Bastien et al., 2001; Gumenyuk et al., 2014). This can lead to increased propensity for cognitive intrusion and perseveration, which has been implicated in the etiology of insomnia (Drake et al., 2014; Pillai et al., 2014a, 2014b). Finally, prior research using the task-switching paradigm has also indicated that lower set-inhibition scores were associated with increased rumination because of the increased difficulty in inhibiting the repetitive and cyclical thoughts (Whitmer and Banich, 2007). In contrast, sleepiness was associated with an increased likelihood of a positive set-inhibition score, which indicates that more effort is required when returning to a previous task compared to switching to a different task. This may be related to an increased appetitive drive toward novelty that has been associated with sleepiness (Anderson and Horne, 2006; Gumenyuk et al., 2010), which could interfere with reorienting attention back to prior tasks.
Reduced cognitive flexibility in returning to prior tasks also has implications for occupational performance. Results indicated that deficits in set inhibition were associated with reduced accuracy, specifically with greater occurrences of perseverative errors. This reduction in productivity can be expensive and therefore can have a significant economic impact. Furthermore, deficits in set inhibition may also interfere with learning and enacting novel tasks due to perseveration on the old task. With the perpetual development and adoption of new technology, there might be an increased demand for workers to learn and implement new protocols, thereby increasing the impact of such deficits.
Results from this study may also have implications for fatigue risk management systems to reduce accidents, such as the consensus standard that was developed subsequent to the 2005 BP Texas City refinery incident (American National Standards Institute and American Petroleum Institute, 2010). Whereas such standards include sleep and circadian disruption broadly under “fatigue” as a major risk factor, this study suggests that sleepiness, sleep disturbance, and circadian phase may independently confer differential risks to cognitive and occupational performance. As such, improvements to these standards may consider the differentiation of fatigue from the circadian phase, sleepiness, insomnia, or a combined estimate of all 3, in both assessment and intervention strategies.
Limitations and Future Directions
While the observational design of this study prevents definitive conclusions of causality, future research may examine whether aligning the circadian phase with the work schedule and/or reducing sleep-wake symptoms in shift workers may result in improvements in specific aspects of cognitive flexibility. Evidence derived from simulated night shift protocols suggests that shifting the circadian phase using bright light leads to reduced attentional impairment (Santhi et al., 2008; Smith and Eastman, 2008), but this has yet to be demonstrated in a sample of fixed night shift workers. While cognitive flexibility has important implications for occupational performance, future research should directly examine the relationship between switch costs, set inhibition, and on-the-job performance. In addition, future research might modify task design to better match specific tasks in occupational settings involving shift work and examine improvements in real-world outcomes following a reduction in circadian misalignment. Results from this study might also be used to examine how tasks during night shift work can be redesigned to reduce the impact of circadian misalignment on cognitive flexibility and therefore work productivity. For example, the number of task switches could be minimized to reduce the impact of increased switch costs and deficits in set inhibition. However, this may not always be feasible or pragmatic. Finally, future research might also examine these issues among rotating shift workers.
Conclusion
This study aimed to extend our knowledge of neurobehavioral processes that are sensitive to specific components of shift work, including circadian phase, sleepiness, and insomnia. Specifically, cognitive flexibility was measured via a task-switching paradigm in a sample of fixed night shift workers, and its relationships with circadian misalignment, nocturnal sleepiness, and reported daytime insomnia were examined. Results revealed that specific components of cognitive flexibility were differentially associated with circadian misalignment versus symptoms of sleepiness and insomnia. Whereas set switching was specifically associated with circadian misalignment, set inhibition was associated with symptoms of sleepiness and insomnia. Furthermore, both components of cognitive flexibility differentially impacted aspects of task performance; whereas deficits in set switching reduced task efficiency, deficits in set inhibition reduced accuracy with increased perseverative errors. These results have implications for occupational performance, and future research might explore whether correcting circadian misalignment might rescue cognitive flexibility, or if tasks on the night shift might be altered to reduce the impact of reduced cognitive flexibility.
Footnotes
Acknowledgements
This study was funded by Teva Pharmaceuticals Industries. The authors thank the technical staff of Henry Ford Hospital Sleep Center for invaluable assistance in the completion of the present study, and Paul Bork and John Dizor at The Dow Chemical Company for their valuable feedback on the manuscript.
Conflict of Interest Statement
The author(s) have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.