
Abstract
The present study aimed to determine the prevalence of musculoskeletal pain, unfavorable working conditions, and assessment of occupational injuries among sawmill workers. The Nordic Musculoskeletal Questionnaire, measurement of handgrip strength, working environment, and occupational injuries were assessed among 135 sawmill workers participating in the study. The data showed that sawmill workers complained of discomfort (pain) felt primarily in the low back region of the body followed by the shoulders, hands, knees, upper back, and wrist. This study indicated that sawmill workers had less handgrip strength due to more intense manual work than control subjects. Based on the results of this study, it was concluded that sawmill workers were highly affected due to working in an awkward posture with manual material handling for an extended period of time and that these factors may lead to work-related musculoskeletal disorders as well as occupational injuries. Proper training, a proper work-rest schedule, and modifications of some working procedures may reduce injuries and work-related musculoskeletal pain.
Keywords
Introduction
The sawmill industry is one of the oldest and essential industries in West Bengal, India. Sawmill workers generally perform rigorous hand-intensive jobs for a sustained period of time. They are forced to carry various loads during work, and they may suffer from work-related musculoskeletal disorders (WMSDs) and other occupational health problems (Das, 2020a). Sawmill workers must perform several types of physical task in sawmills with a manual material handling (MMH) and working in a constrained and awkward posture for long durations, which may lead to work-related musculoskeletal disorders (Qutubuddin et al., 2012).
The sawmill industry involves cutting logs into lumber in different shapes according to the orders, and recently in the modern sawmill, motorized saws are generally used to cut logs into different shapes (Sharma et al., 2021). It is common for sawmill workers to be exposed to physical and ergonomics hazards, which can cause a variety of diseases. Due to ergonomic risk factors from handling heavy loads and repetitive movements, and working in an awkward posture for prolonged periods of time, sawmill workers suffer a high rate of acute and chronic injuries.
Sawmill workers generally perform rigorous hand-intensive jobs for a sustained period. As a result, they are forced to carry various amounts of load during their work day, which may cause them to suffer from WMSD. The sawmill industry is known to have a high level of MMH, with tasks often involving high loads/forces, awkward postures, and repetitive movements, some of the critical risk factors for musculoskeletal disorders (MSD) (Tappin et al., 2003).
Manual material handling is an important causative factor for the development of work-related musculoskeletal disorders among sawmills workers. Using hands or body force to lift, lower, push, pull, carry, or move a load is considered MMH. Work in MMH is physically demanding and has a high risk of work-related injuries and WMSDs. MMH tasks can be found in most workplaces and may contribute to WMSDs. Globally, WMSDs are a major occupational health problem (Ayub and Shah, 2018).
Work-related musculoskeletal disorders are known to be of multifactorial etiology. These disorders are due to excessive, long-term unilateral stress on muscles, tendons, joints, and nerves. They are associated with the specific workload in the sawmill industry with its adverse static positions, high demands on hand movements, work with vibrating tools, and unsupported elevated arms. WMSDs can be caused by heavy physical work, static work postures, frequent bending, twisting, lifting, pushing, pulling, repetitive work, vibration, and psychological and psychosocial stress (Ajayeoba, 2019). In the sawmill industry, the workers repetitively perform heavy manual tasks for a prolonged period, leading to severe physical stress.
Occupational injuries resulting from such incidences include being caught in or struck by machinery, falling from a height, heavy lifting or repetitive movements, and twisting or reaching, while working to increase productivity. Besides, the hazards inherent in this profession are the unfavorable weather conditions and noise pollution that injure human health (Michael and Wiedenbeck, 2004). Due to the high level of manual handling involved in sawmilling operations, the workers are exposed to higher levels of risk and a high physical workload. Excessive physical workload, noise, and heat stress have been identified as factors resulting in adverse health effects among sawmill workers.
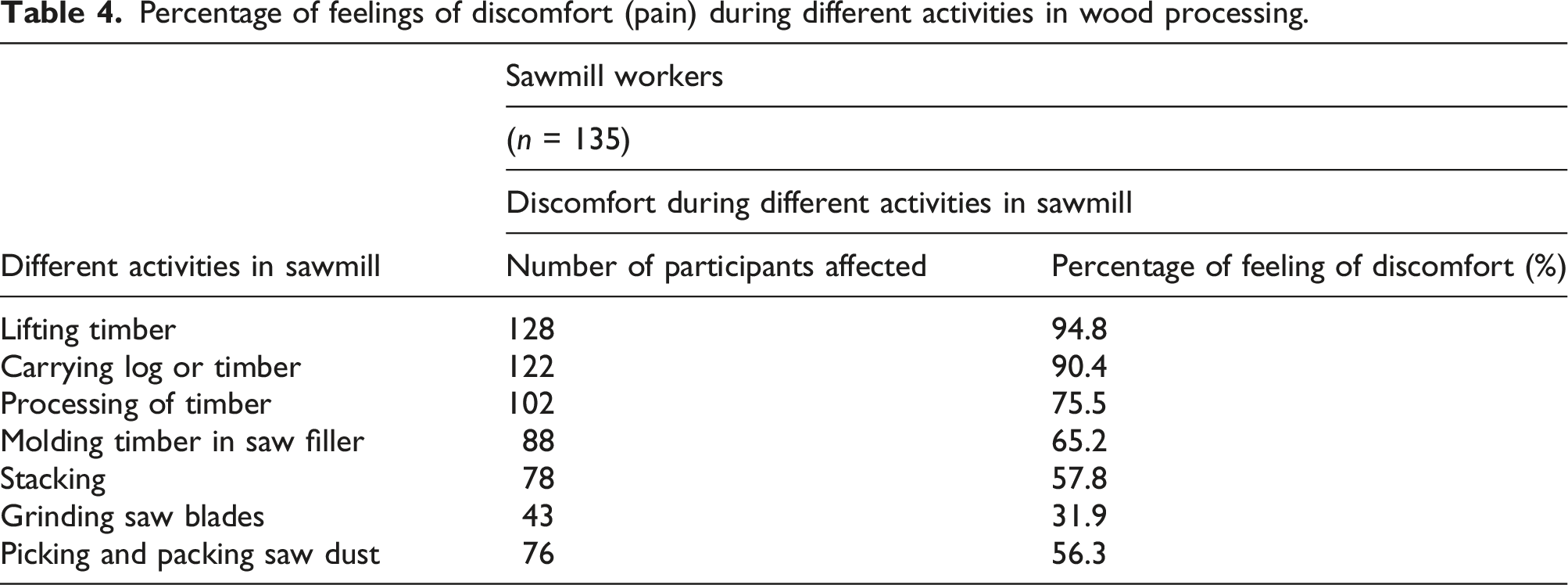
Sawmill workers perform several types of strenuous activities. Among this i) carrying log or timber, ii) lifting timber, iii) processing of timber, iv) molding timber in saw filler, v) stacking (loading and unloading the timber), vii) grinding saw blades, and viii) picking and packing sawdust. During this process, sawmill workers have to face many problems during their work. Adverse environmental and physical conditions affect the sawmill workers' health condition. The sawmill workers also performed several types of activities in which they suffered from hearing loss. Boateng and Amedofu (2004) also reported noise-induced hearing loss (NIHL) among local sawmill workers.
The main aim of the present investigation was (i) to determine the prevalence of WMSDs among the sawmill workers and compare them to control workers, (ii) to analyze thermal stress, (iii) to identify unfavorable working conditions among the sawmill workers, and (iv) to analyze the occupational injuries.
Methods
Selection of working sites
This cross-sectional study was conducted on 135 sawmill workers from 21 sawmills working in a selected sawmill unit of Bhadrakali in Hooghly district, which was situated on the side of the Hooghly River; 130 control group subjects were also selected who were engaged in office work like making and serving tea, carrying files, and cleaning floors, involving a minimum amount of hand-intensive work. This sawmill unit was randomly selected from the surrounding area. No subjects worked for less than 6 months in the sawmill.
Measurement of physical parameters
The height and weight of the sawmill workers were measured by an anthropometer and weighing machine, respectively. In addition, all subjects' body mass index (BMI) (Cole, 2000) was also computed. Before conducting the survey, consent was obtained from sawmill owners and each subject. Furthermore, written permission for the project was obtained from the Institutional Human Ethical Clearance Committee over the Indian Council of Medical Research Guidelines.
Questionnaire study
A detailed Nordic musculoskeletal disorder questionnaire (Dickinson et al., 1992) was developed and applied to both the sawmill workers and the controls. The Nordic Questionnaire was modified to acquire detailed information about the discomfort feeling among the sawmill workers and control subjects. The modified questionnaire was translated into the local language, Bengali and Hindi, which helped all subjects to understand the study. In the modified questionnaire, both subjects were asked about the types of discomfort, such as pain, tingling, numbness, stiffness, or swelling. Both groups also completed a questionnaire based on the modified Nordic musculoskeletal disorder questionnaire. The subjects were asked about the details of pain felt, where it was felt at a maximum during work, after work, and after 7 days, and 12 months. The questionnaire consisted of several objective questions, with multiple choice answers identifying the participant's viewpoints, the pattern of work, duration of work, and discomfort levels in different body parts as well as the details suffering from the different health hazards.
Assessment of working environment
The working environment of the sawmill workers was assessed as follows. First, the wet bulb globe temperature (WBGT) index was calculated (Das, 2018). Then, the mean globe temperature and wet and dry bulb temperatures were recorded. The formula for calculating the WBGT index for indoor conditions is WBGT (indoor) = 0.7 (NWB) + 0.3 (GT), where NWB is the natural wet bulb temperature, and GT is the globe temperature. Relative humidity was also estimated from a psychometric chart developed by Weksler Instrument (USA) (Tayyari and Smith, 1997). A sound level meter manufactured by Lutron Electronics Enterprise (Taiwan) was used; it was kept 4 m from the source of sound and 1 m above the ground to record the noise level generated during different activities in sawmilling. A Lux meter (Lutron) was used to assess the other areas' illumination levels in two worksites (indoor and outdoor).
Injury data collection
To obtain the epidemiological information on all types of injury-related events for a period of 12 months, all selected sawmills were visited every week during the study period. The investigators visited every selected sawmill to collect injury data of the sawmill workers through the survey.
Interviews were performed by the development of the questionnaire, which was developed in English, then translated into local language (Bengali and Hindi). The translated questionnaire was pretested by sawmill office staff. Direct personal interviews were conducted by questioning to the sawmill workers in a local language on the following topics: (1) type of injuries, (2) body parts injured, and (3) injuries occurred due to which activities in sawmill.
Incident rate
Incident rate was calculated by the formula per 1000 workers as days active: I = E/T, where E = event or incidence, T = time/days active (Das, 2014, 2020c).
Statistical analysis
The mean and standard deviation of age, stature, weight, and BMI of the sawmill workers and the control group of subjects were calculated. The Student's t-test was used to determine whether there was any significant difference between the physical parameters of the two groups of workers. A two-tail Chi-square test of independence was applied to determine whether or not the test item had any significant association with discomfort. The computed χ2 was compared with the critical χ2 values for the chosen significance level (p<.05). Statistical analysis was performed using the statistical package Primer of Biostatistics (Primer of Biostatistics 5.0.msi, Msi version 1.20.1827.0, Primer for Windows, McGraw-Hill).
Results
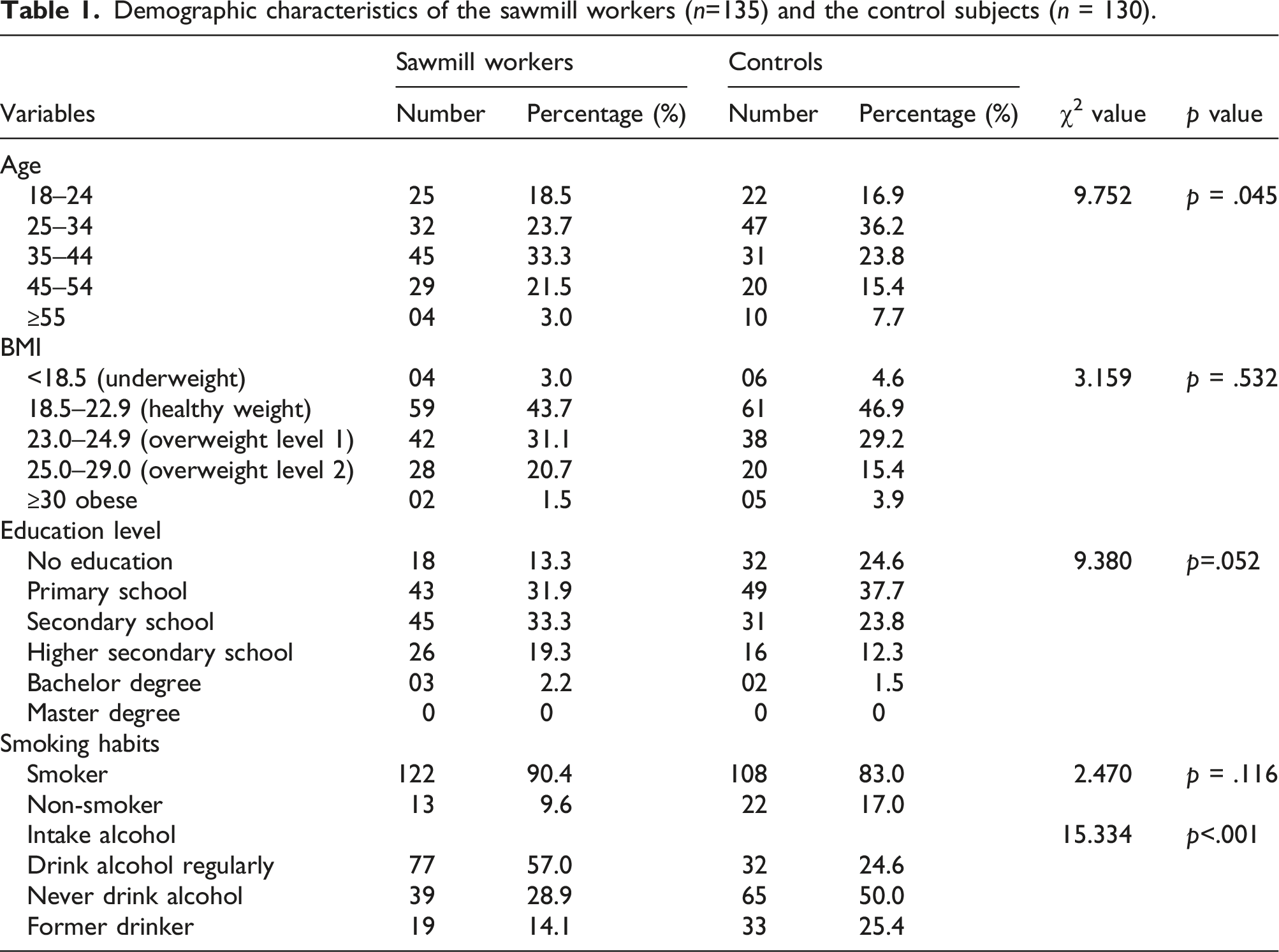
Demographic characteristics of the sawmill workers (n=135) and the control subjects (n = 130).
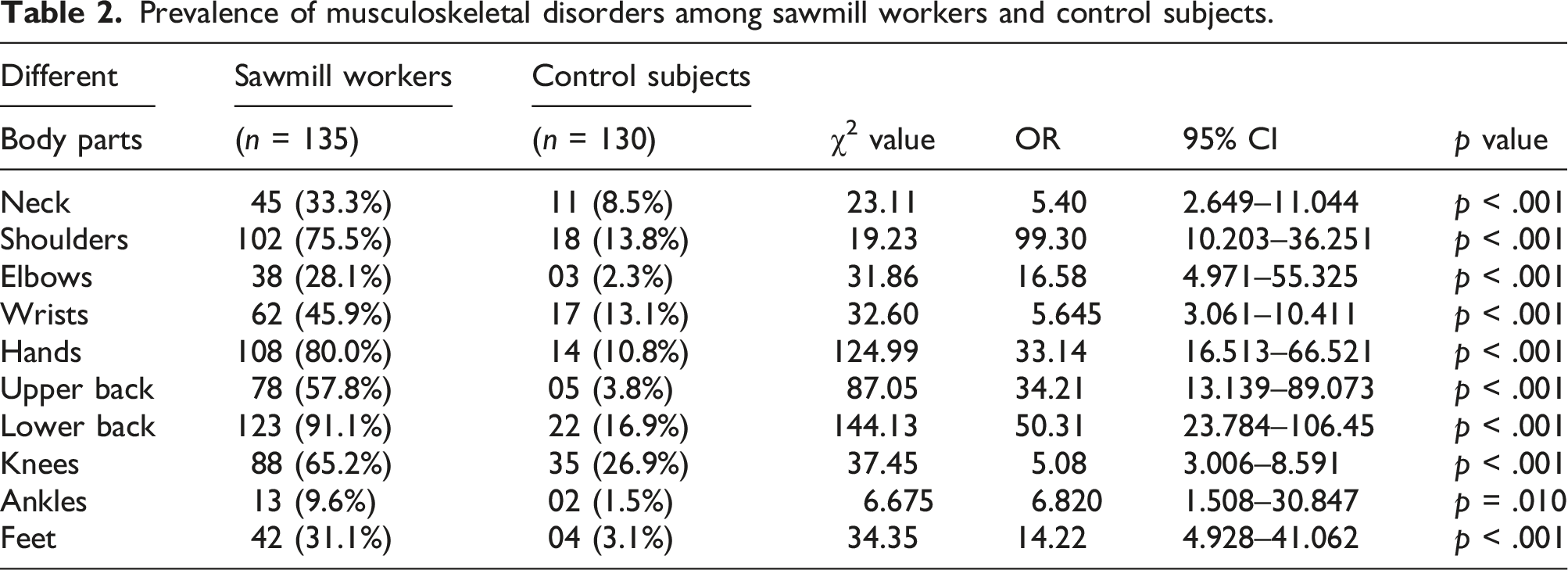
Prevalence of musculoskeletal disorders among sawmill workers and control subjects.
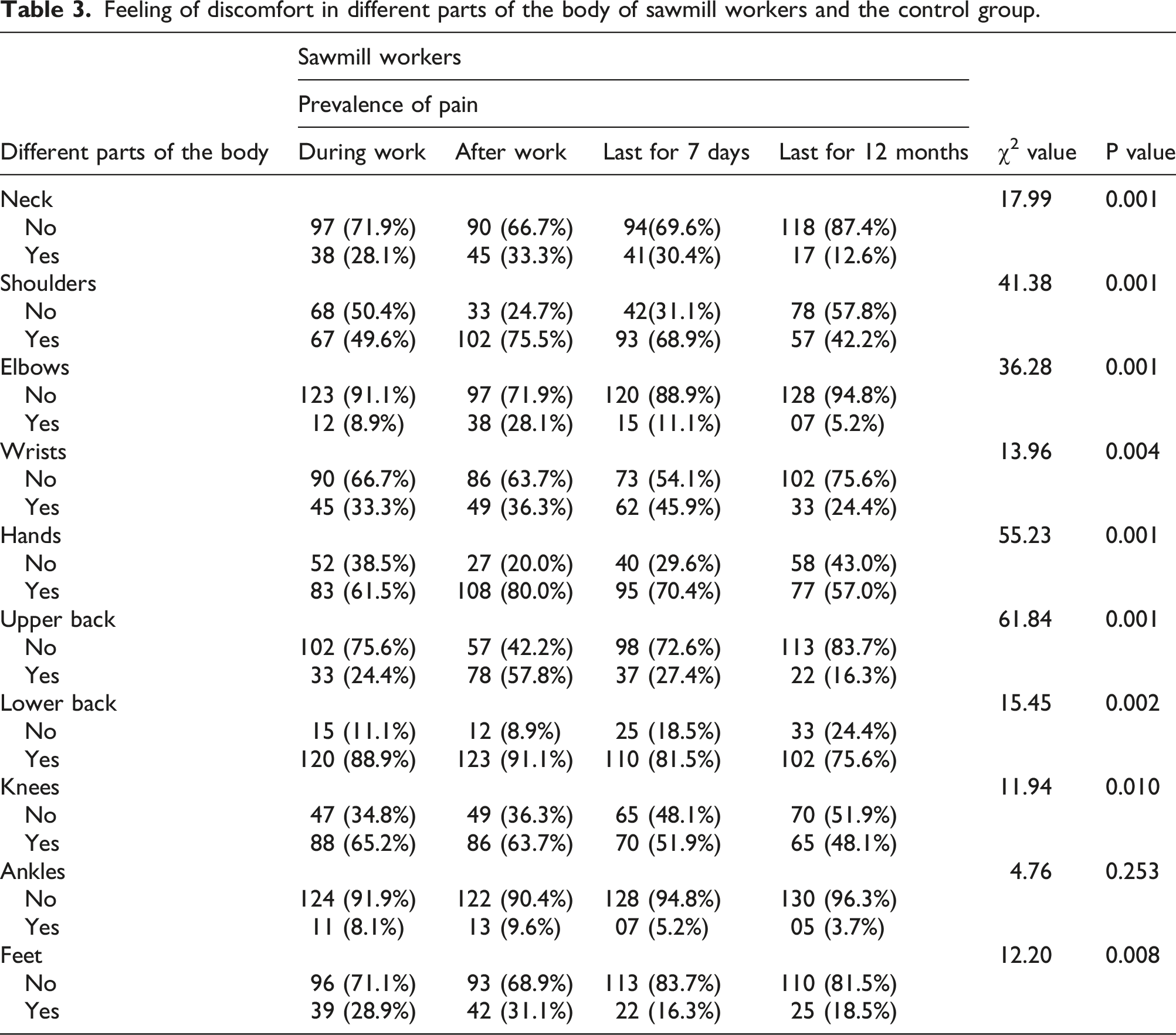
Feeling of discomfort in different parts of the body of sawmill workers and the control group.
Percentage of feelings of discomfort (pain) during different activities in wood processing.
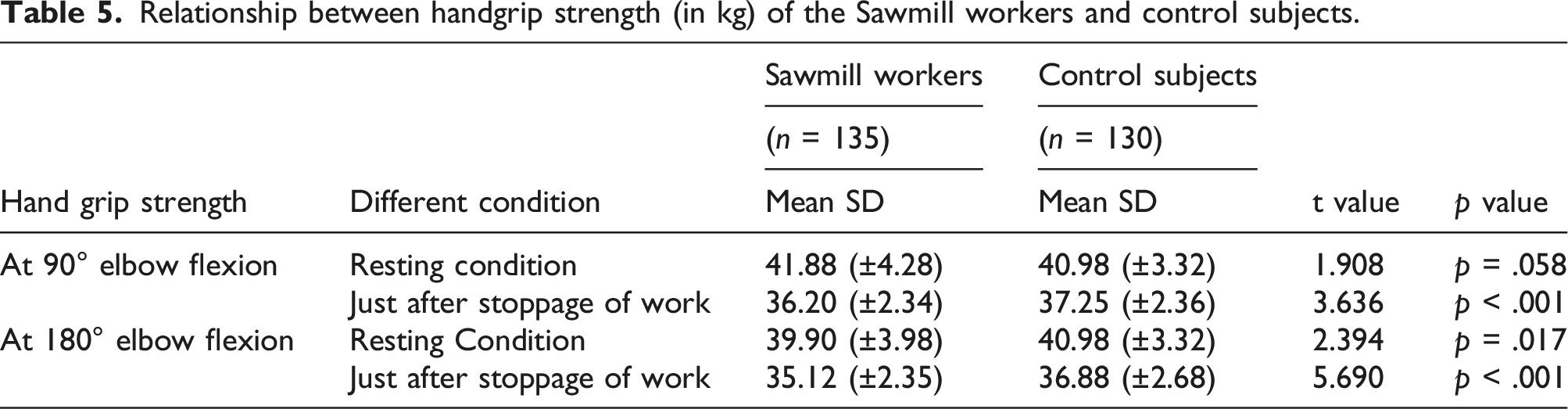
Relationship between handgrip strength (in kg) of the Sawmill workers and control subjects.
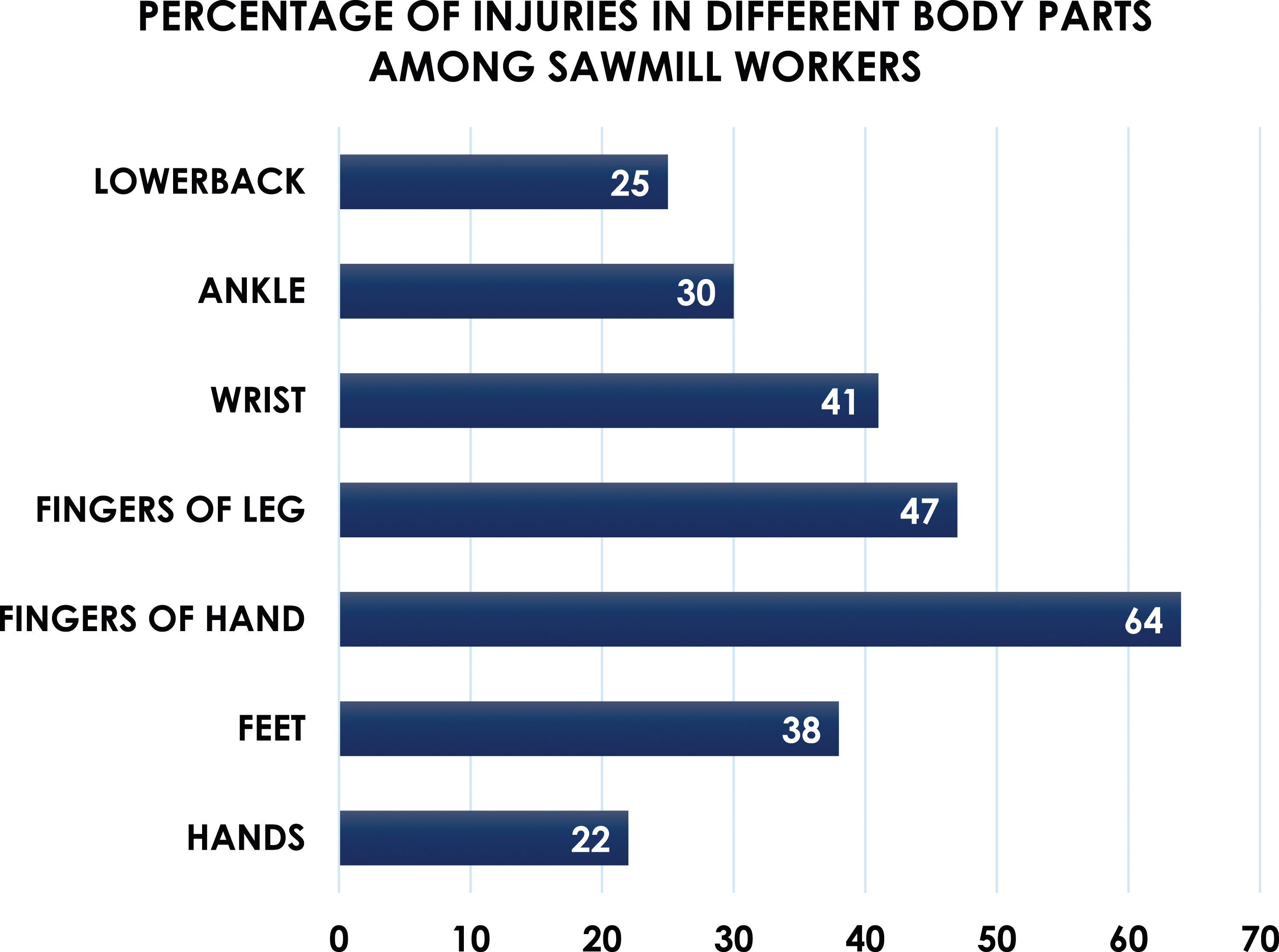
Incident rate of injuries occur among sawmill workers.

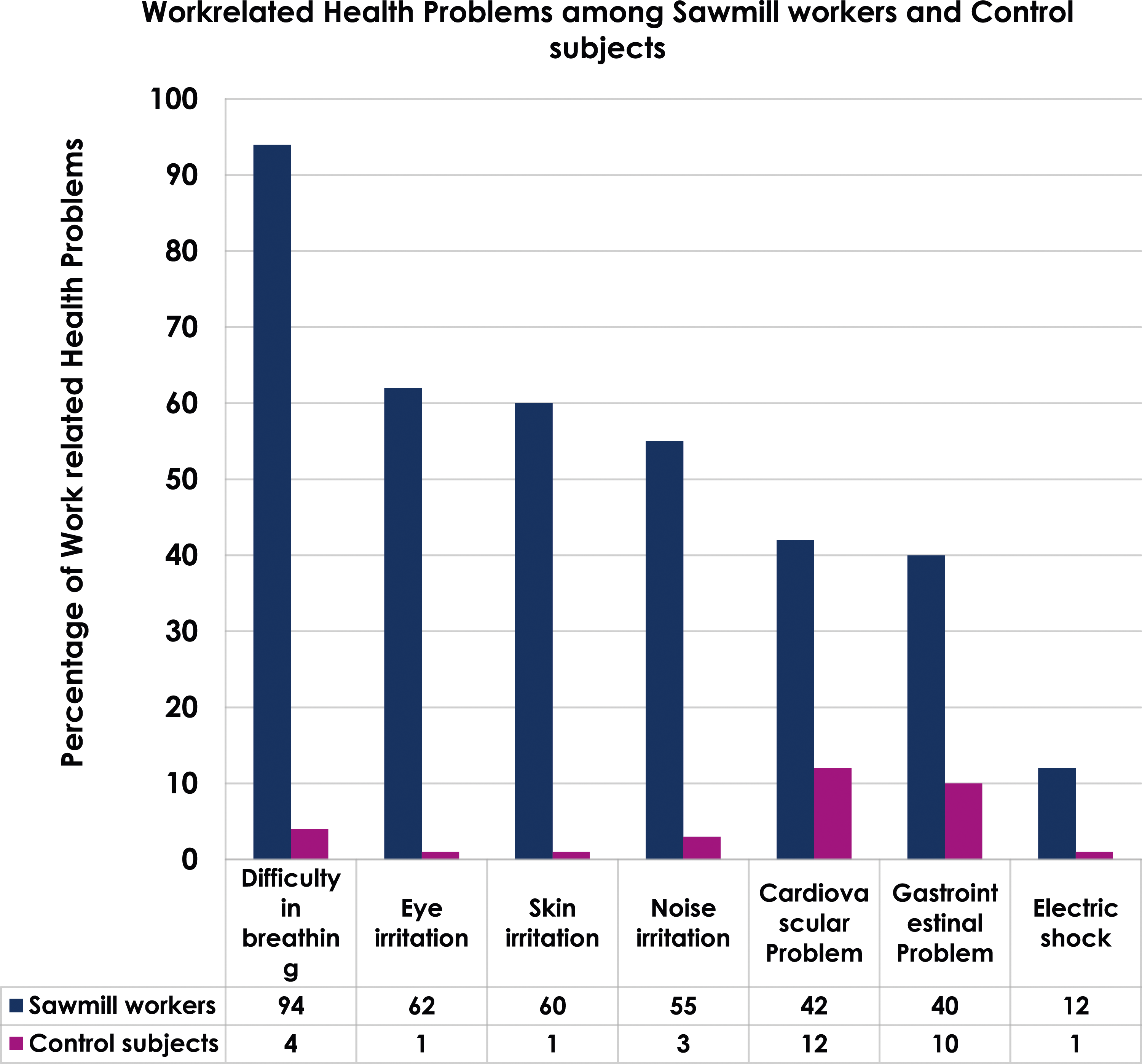
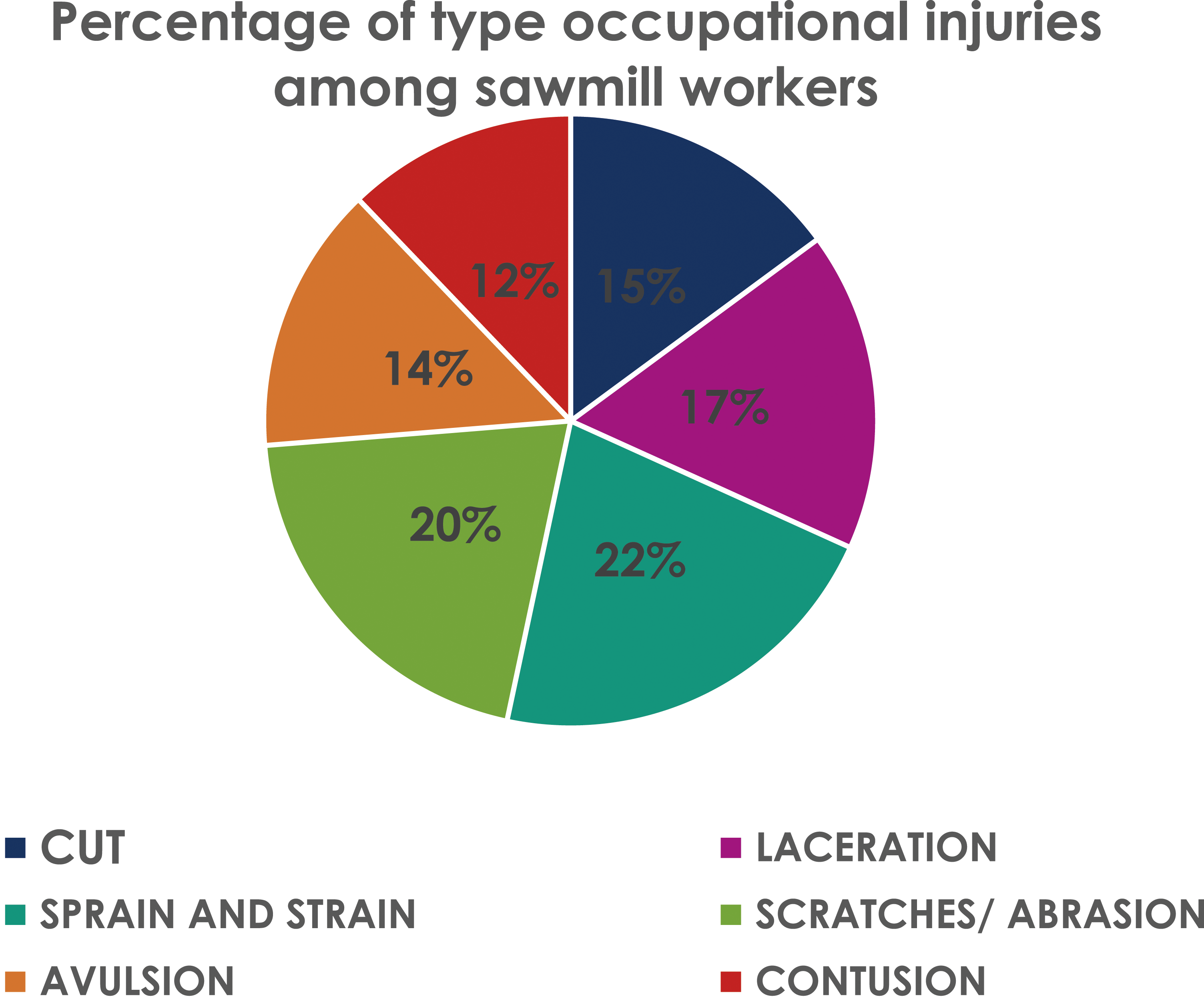
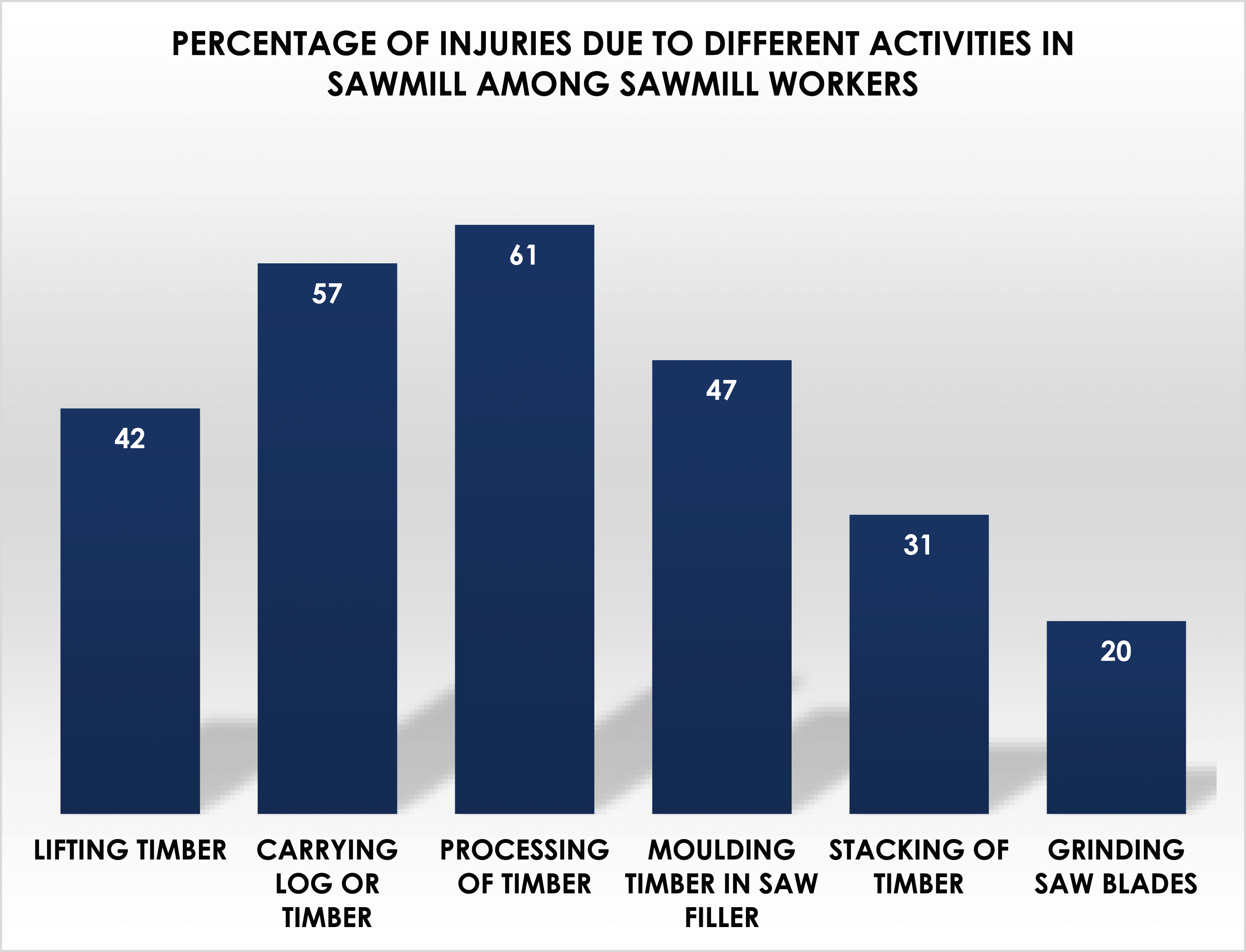
Figure 1 represents the different types of discomfort among experimental and control subjects. The results of the study showed that pain is predominant among discomfort feelings, followed by tingling, numbness, and stiffness. Questionnaire studies (Figure 2) showed that apart from discomfort feeling, most of the sawmill workers suffered from difficulties in breathing (94%), eye irritation (62%), skin irritation (60%), noise irritation (55%), cardiovascular problem (42%), gastrointestinal problem (40%), and electric shock (12%). In Figure 3, the percentage of type of occupational injuries among sawmill workers is shown, where sprain and strain are the main types of injury followed by scratches and abrasions, laceration, avulsion, cuts, and contusions. Figure 4 mainly shows the percentage of injuries in different body parts among sawmill workers. The results mainly showed that fingers and feet are the main affected parts of the body, followed by wrist, lower back, and hands. The results of the study (Figure 5) summarizes the percentage of injuries due to different activities among sawmill workers. These results showed that most of the injuries occurred during processing of timber followed by carrying logs or timber, molding timber in the saw filler, and lifting timber. Types of discomfort feelings among sawmill workers and control subjects. Comparative study of work-related health problems among sawmills workers and control subjects. Percentage of type of occupational injuries among sawmill workers. Percentage of injuries in different body parts among sawmill workers. Percentage of injuries due to different activities in sawmill among sawmill workers.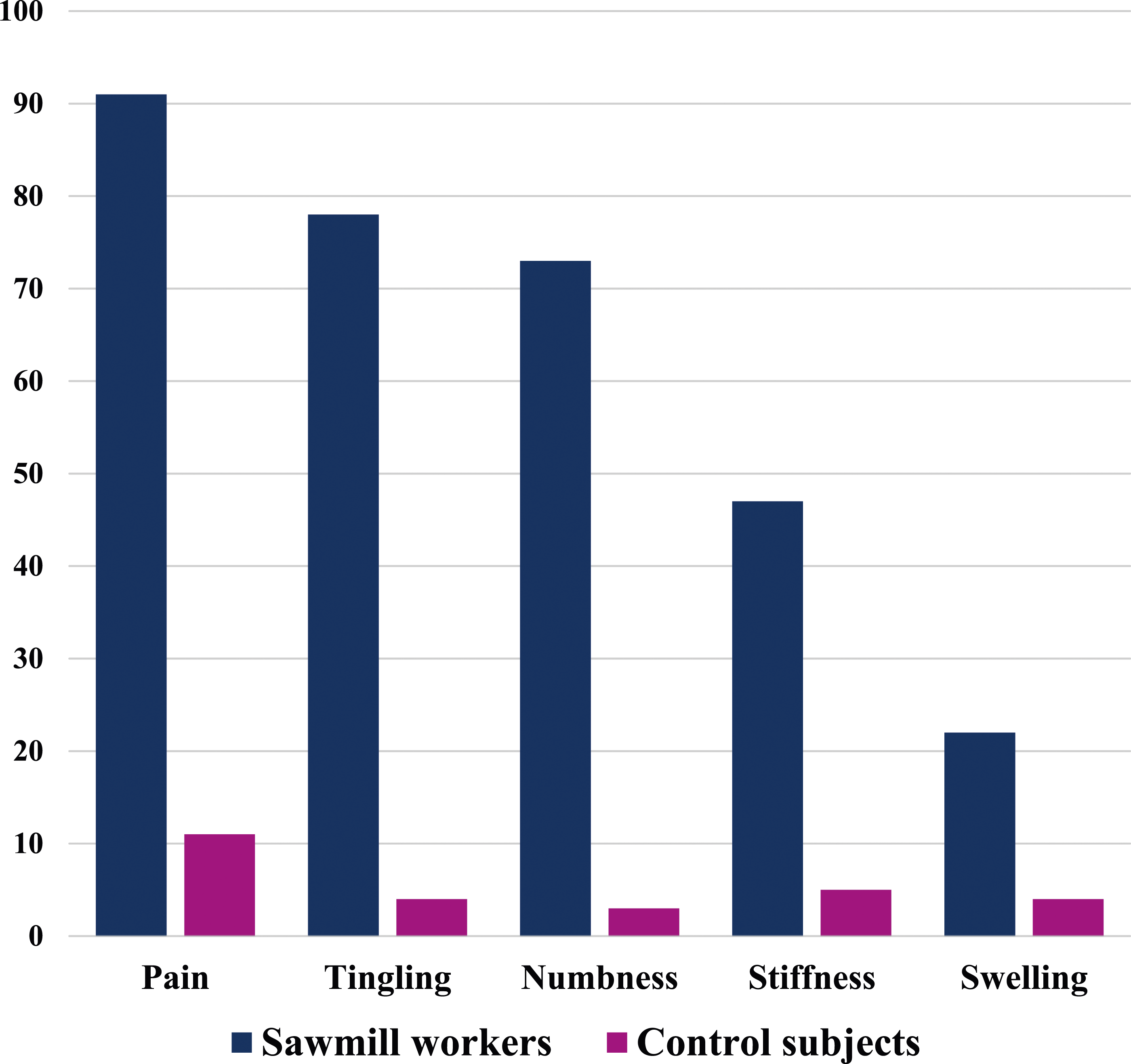
Discussion
The prevalence of occupational health hazards has been reported to be high among the people of India (Gangopadhyay et al., 2010). In the present study, sawmill workers and the control group had no significant differences regarding age, height, weight, or BMI. The survey also revealed that the sawmill workers (experimental group) were engaged in rigorous hand-intensive jobs for many years. In contrast, the control group was not involved in such work. From the investigation, it can be concluded that the sawmill workers were heavy workers and most often worked in awkward postures; they had various musculoskeletal disorders that affected primarily the low back region.
Pushing, pulling, and carrying are the most common human activities in several occupations involving manual material handling. During sawmill activities, workers perform several kinds of manual material handling that may be causative factors for musculoskeletal disorders among them. The present study dealt with manual material handling in which workers had to lift and carry heavy loads (logs), which may be causative factors of musculoskeletal disorders. From the statistical analysis, it is evident that there was a significant association between positive and negative responses to discomfort feeling among the sawmill workers and comparison groups. This suggests that the sawmill workers engaged in hand-intensive activities, had to perform strenuous tasks repeatedly throughout the day, and suffered the most. In contrast, the control group performed comparatively less strenuous activity and suffered less.
From the observation of the working conditions of the experimental group, it is evident that sawmill workers work in unfavorable conditions; they must lift and carry heavy loads (logs). This may cause discomfort in different parts, especially in the body's lower back, hands, shoulder, knees, upper back, wrist, and neck. Goldsheyder et al. (2002) mainly supported this result. According to them, mason tenders experienced a high prevalence of lower back pain due to carrying heavy loads in their profession. Das (2020b) found similar results in the case of railway track maintainers. Like sawmill workers, track maintainers also have to carry heavy loads (concrete sleepers) in their profession. Also, they have severe musculoskeletal disorders in different body parts, especially the low back, shoulder, hands, and knees.
Work-related musculoskeletal disorders has been associated with lifting heavy objects in an awkward posture (Das, 2020c). Severe flexion or lateral twist and bending mainly are significantly related to lower back pain (Das, 2015). Posture and the location and weight of a load affect the moment of the force applied in the lumbar region, affecting muscle loading and compressive forces on the internal vertebral disc (Callaghan and Mcgill, 2001). Thus, lower back problems appear to be associated with postures that require back flexion, carrying and lifting heavy loads, and exposure to whole-body vibration (Das, 2021, 2022). Even nowadays, many physically heavy work phases and a combination of several stress factors, including poor work postures and activities requiring the use of force, are common among sawmill workers. The National Institute of Occupational Safety and Health (NIOSH, 2018), in a review of work related to MSDs, found strong evidence that low back disorders are related to forceful lifting and the weight of load lifted (Garg, 1989).
Handgrip strength of both groups was measured at 90° and 180° elbow flexion during rest and after work. Handgrip strength was significantly different between the sawmill workers and the control group after work conditions. If sawmill workers are constantly engaged in hand-intensive jobs, they may be affected by discomfort (pain) in the upper extremities and significant changes in the handgrip strength. This result corroborates with the work of Gangopadhyay et al. (2007) and Das et al. (2012). They also suggested that the handgrip strength of the experimental subjects was less than control subjects just after work conditions at 90° and 180° elbow flexion. The handgrip strength was measured primarily to correlate with back, neck, and shoulder pain. Chandra et al. (2011) stated that handgrip measurements of the sawmill workers revealed that the decreased handgrip strength might be related to increased loading at the proximal end, muscles at the cervical spine, and shoulder joints may have to exert greater forces to control the arm movements. Our study also observed a significant difference in handgrip strength between the sawmill workers and the comparison group.
The sawmill workers adopting awkward postures at work leads to MSDs because they remain in such postures for prolonged periods. In addition, the amount and quality of forward-bent work postures influence the compressive forces on the vertebral discs and the erector spine, stating that lower back pain and other musculoskeletal conditions are a significant problem for sawmill workers.
From the observation of the working conditions of the unorganized sector, it was evident that the experimental subjects (sawmill workers) had to work in a congested and poorly illuminated (13.28 lux) work area because most of the working areas were inside and fully covered with asbestos and tin to protect the logs or timber from rainwater, where the illumination level was insufficient. Not only that, but the noise level while cutting the lumber in the working area was also very high (104 dB(A)), which could affect the sawmill workers. It is also evident from the results that the experimental group subjects suffered from high noise during the processing and molding of timber, which seriously affected their health. Noise-induced hearing impairment is hardly a public health concern in many developing countries like India. However, occupational noise remains a severe industrial disease (Sataloff and Sataloff, 1987). Noise is a risk factor for sleep disturbance, cardiovascular dysfunction, speech interference, and mental health distortion, including hearing impairment and balance disorder. Repeated or prolonged exposure to noise levels greater than 80 dB hearing impairment may occur (Satterfield, 2001).
The results of the study showed that the type of occupational injuries prevalent in sawmill workers. Sprain and strain are the main types of injury followed by scratches and abrasion, laceration, avulsion, cut, and contusion. The study results showed a high percentage of injuries in hands and feet, followed by wrist, and lower back. Das (2020b) reported similar types of findings in railway track maintainers. They stated that due to manual material handling, the workers were more prone occupational injuries. Their study also found that most of the injuries occurred during processing of timber followed by carrying log or timber, molding timber in the saw filler, and lifting timber. Similar findings were reported by Chandra et al. (2011). They also concluded that sawmill workers performed rigorous types of work in the sawmills. Due to constant manual material handling and working in an awkward posture, musculoskeletal pain and injuries occurred among them.
Limitations of the study
This study did however have some limitations, for example, the study was conducted only on 135 sawmill workers from 21 sawmills in the same area of Bhadrakali, Kotrung, and its surrounding area of West Bengal, India. This study did not reflect the EMG analysis during the different activities, where the muscle fatigue of the sawmill workers could be assessed. Nevertheless, it reflects the problem of work-related upper-limb disorders among the sawmill workers compared with control subjects. Future studies will include goniometry analysis to understand the relationship between joint angles and different posture on MSD in sawmill activities.
Conclusion
The conclusions reached from the investigation are as follows: (1) This study showed that sawmill workers had work-related musculoskeletal disorders (WMSDs), especially in the upper extremities and lower back of the body, due to working in an awkward posture for an extended period and manual material handling (MMH). (2) This study indicated that sawmill workers had less handgrip strength due to performing more intense hands than control subjects. (3) The present investigation showed that sawmill workers had to work in unfavorable working conditions. The average value of the indoor WBGT index of the worksites was 34.5°C, with a relative humidity of 76%. The intermediate noise level was 98 dB(A) during timber or log cutting. Moreover, the heavy log dust emitted could affect sawmillers. The study also concluded that the sawmillers had to work sometimes at night in poor illumination conditions (M 13.28 lux). (4) The prevalence rate of injuries (15.2%) among sawmill workers occured at a substantially higher rate compared with other types of workers in different unorganized sectors.
Preventive measures
(1) The possible ergonomics interventions are identified to increase the value of this investigation. (2) Proper training, knowledge, and education (operator training) should be provided for the sawmill workers for the betterment of their health and to avoid accidents. (3) Manual material handling (MMH) should be avoided, which is the most important factor for musculoskeletal disorders (MSD) among sawmill workers. (4) Sawmill workers should rotate their jobs. (5) The sawmill workers should change their posture frequently to avoid discomfort. (6) Recommendations include changing the work schedule by increasing the short rest break in their work to avoid excessive physical stress. (7) Different types of stretching exercises should be practiced during the breaks. (8) For molding or processing logs or timbers, safety glasses, nose masks, and helmets should be worn. (9) In the case of a high thermal load caused by environmental stress and physical labor, fluid replacement can be essential to preventing dehydration.
Ethical statement
Ethical approval
Necessary Ethical clearance was granted by the Institutional Human Ethical Clearance Committee over the Indian Council of Medical Research Guidelines.
Footnotes
Acknowledgments
The author is thankful for the grant provided by the University Grant Commission, India, for partial funding of the study. Author express their sincere gratitude to all the sawmill workers and sawmill owners who rendered immense cooperation during the completion of this study.
Author contributions
BD in his research project designed the study, collected data, conducted data analysis, and wrote the manuscript and critical revision of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University Grants Commission (UGC Reference No. F. PSW-147/11-12 (ERO)).