
Abstract
Mesothelioma is a fatal disease that has historically been associated with exposure to airborne asbestos. Because occupational asbestos exposures dropped dramatically in the late 1960s and early 1970s, far fewer cases of mesothelioma today are due to these fibers but, instead, are usually a result of the aging process or genetic predisposition. In May of 2022, a Morbidity and Mortality Weekly Report (MMWR) was issued by the Centers for Disease Control and Prevention (CDC) regarding malignant mesothelioma incidence in women from 1999 to 2020. While this MMWR alerted citizens to the continued presence of the disease, after reading this article one might have thought that the CDC was suggesting that the disease was increasing in women due to asbestos exposures (which it is not). In the present analysis, we investigate several factors related to the interpretation of epidemiological data for mesothelioma, including the role of asbestos as a risk factor over time. The authors conducted a review of the scientific community’s understanding of mesothelioma incidence and asbestos exposures amongst women, as well as an investigation of the methods and references in the MMWR article. Although various articles have recently discussed the incidence of both peritoneal and pleural mesothelioma in women, it is fortunate that the age-adjusted rates for mesothelioma have remained flat (neither increased nor decreased significantly) in women for the past 50 years. Incredibly few women in the U. S. have had appreciable cumulative exposures to any type of asbestos (chrysotile, amosite, or crocidolite) in the workplace or from the ambient environment, especially since about 1965–1970. In this paper, we highlight six factors that should be considered when evaluating the incidence of mesothelioma amongst American women in the current era. Without sufficient consideration of these factors, improper conclusions have been drawn over the past several years.
Introduction
The Morbidity and Mortality Weekly Report (MMWR) is a weekly series published by the Centers for Disease Control and Prevention (CDC) and is available in the public domain. On the CDC’s website, the MMWR is considered “the voice of the CDC” and reflects the stance of its parent organization (Shaw et al., 2011; Centers for Disease Control and Prevention (CDC), 2022a). On May 13, 2022, there was a published report in the MMWR titled “Malignant Mesothelioma Mortality in Women – United States, 1999-2020” (Mazurek et al., 2022). The authors of this MMWR relied upon the National Vital Statistic System’s Multiple Cause of Death (MCD) records to analyze trends for this disease in women.
According to the CDC’s National Vital Statistics Reports, life expectancy for females in the United States has increased 0.5 years from 1999 (79.4 for females and 73.9 for males; 76.7 overall) to 2020 (79.9 for females and 74.2 for males; 77.0 overall) (Anderson and DeTurk, 2002; Arias and Xu, 2022).
The MMWR reported that the MCD records showed an increased incidence of 25% in malignant mesothelioma mortalities in women between 1999 and 2020 (Mazurek et al., 2022), and this statement was placed in headlines in the popular press (American Industrial Hygiene Association (AIHA), 2022). While this statement is correct, the more important observation was that the age-adjusted death rate for women remained flat throughout this time period (fluctuating between 4.12 and 4.99 per 1 million from 1999 to 2020) (Mazurek et al., 2022), which suggests that the net increase in mesotheliomas amongst women was due to longer life-spans and not associated with exposures to asbestos.
Mesothelioma (certainly pleural mesothelioma) has long been considered a hallmark disease of asbestos exposure in men, but this is not the case in women (Ilgren and Wagner, 1991; Pavlisko and Sporn, 2014; Price, 2022; Price and Ware, 2009; Wagner et al., 1960). The exposure-response relationship for asbestos and mesothelioma is believed to be consistent across genders. However, due to historic occupational trends, few women have been exposed to significant cumulative airborne concentrations (doses) of any fiber type of asbestos. As a result, mesothelioma occurrences among women do not correlate with asbestos consumption in the United States, in contrast to the correlation observed with men (Moolgavkar et al., 2023).
Relevant to understanding the risk associated with various exposures, there are drastic differences in the potency and the ability of asbestos fibers to cause disease based on the chemical composition and dimension of the fibers (Darnton, 2023; Garabrant and Pastula, 2018; Hodgson and Darnton, 2000; Korchevskiy et al., 2019; Stanton et al., 1977; Wagner et al., 1960; Yarborough, 2006).
In order to address the underlying topics relevant to the MMWR article by Mazurek et al., a non-systematic review on the scientific community’s state-of-the-art understanding of mesothelioma incidence and asbestos exposures amongst women in the United States, as well as a critical investigation of the methods and references in the MMWR, was conducted. For purposes of our review, online tools (PubMed, Scopus, and Google Scholar) were queried for various combinations of terms including “mesothelioma,” “women,” “asbestos,” “take-home exposures”, “para-occupational exposure,” “background rates of mesothelioma,” and “background rates of asbestos exposure,” with results current through April 2024. The references cited in various published papers were examined to identify additional publications of merit. Studies of non-United States populations of women were excluded. We discuss almost 200 informative resources in this paper.
We concluded that the MMWR should have provided a more thorough discussion of the many factors that need to be considered when assessing trends in the incidence of mesothelioma. In this paper, we address (1) shortcomings in the national database regarding anatomical location and occupational classification deaths, (2) the importance of asbestos fiber type, (3) the historical trends of women’s occupational exposures to asbestos in the United States, (4) the likelihood that take-home and para-occupational exposures have caused mesothelioma in women, (5) the potential for various exposures to asbestos in the post-OSHA era (after 1970), and (6) the risk factors of mesothelioma when asbestos exposure is absent.
Background
According to the CDC, most MMWR articles are not peer-reviewed in the way typical submissions to health-related journals are evaluated for quality (Shaw et al., 2011). They undergo a streamlined “multi-level clearance” within the CDC, which has allowed them to publish on relevant epidemiology and public health issues “as quickly as possible” with a “short rapid report” format (Shaw et al., 2011). This journal, generally intended for health professionals, serves an important purpose for informing both the health professional and the public. It focuses on alerting them to time-sensitive issues such as food and water safety, environmental mishaps and diseases, and the spread of viruses/diseases (including Covid).
As a trade-off, sometimes, these articles have been shown to have shortcomings with respect to the accuracy of the content (Renner, 2009; Leoning, 2010; Centers for Disease Control and Prevention (CDC), 2010b; Centers for Disease Control and Prevention (CDC), 2010a).
Asbestos is one of the most extensively studied hazards in the fields of toxicology, occupational health, and environmental science. The idea that asbestos exposures amongst American women in the 2020s is a time-sensitive issue that needed to be communicated to health profesionals and the public “as quickly as possible” seems unsubstantiated. In our view, a proper peer review of the article by Mazurek et al. (2022) may have led to more well-informed conclusions by the readers.
Shortcomings in database recordkeeping
Types of databases
The CDC’s Multiple Cause of Death (MCD) record is a database that contains the national mortality data from 1999 to 2020. ICD-10 codes are used to select between 113 different causes of death (which can be used to calculate crude death rates and age-adjusted death rates), and place of residence, age, race, ethnicity, and gender are also recorded for each entry (Centers for Disease Control and Prevention (CDC), 2022b). The ICD code was established in 1999, and screening and reporting for mesothelioma has likely increased and improved thereafter. While the MCD does not record occupation, information from the MCD can be combined with industrial and occupational data for analysis. Combined databases like these have been used in a number of papers with respect to mesothelioma (Bang et al., 2006; Mazurek et al., 2017, 2022). Unfortunately, at least for mesothelioma, those records are limited for characterizing incidence rates (as explained in the next two sections).
An additional database that can be used to analyze mesothelioma incidence from 1975 to 2018 is the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program (SEER). While the SEER database uses the ICD style coding, it also uses a list of registries that encompasses the entire SEER database and measures the incidence of diseases via patient demographics, primary tumor site, tumor morphology, stage at diagnosis, treatment, and vital status (National Institute of Health (NIH), n.d).
Neither database considers whether diagnoses of mesothelioma were accompanied by causation assessments from pathologists or pulmonologists. Most mesotheliomas do not have causation assessments, nor should these assessments be considered reliable if they are not confirmed by pathology via lung-tissue analysis (as done in Roggli et al., 2023). In many cases, the absence of a national epidemiological surveillance system can lead to significant and hasty judgments regarding the inclusion or exclusion of asbestos as the cause of the mesothelioma. The recent analysis by distinguished pathologist, Dr. Victor Roggli, indicates that roughly 35% of mesotheliomas in men that were considered “asbestos-induced” in these causation assessments were inaccurate as lung-tissue analysis revealed that there were fewer asbestos fibers in the lung tissue of these individuals compared to background rates (Roggli et al., 2023).
Shortcomings with occupational record keeping
One of the challenges with recordkeeping is the determination of a person’s occupational history with their stated cause of death. An inherent problem with this approach is defining a singular occupation for a person’s lifetime and which occupation, if any, could have contributed to an individual’s cause of death.
The CDC’s National Center for Health Statistics and the National Institute for Occupational Safety and Health (NIOSH) collaborated to create a database in 2020 on industry and occupation (I&O) data as applicable to mortality vital statistics (Steege et al., 2020). This database used the “usual occupation” from the 2012 census coding scheme to define the occupation that a person worked for most of their life (Steege et al., 2020). This approach, as was done in the MMWR, does not account for an occupation where someone could have been exposed to a hazardous chemical for a significant portion of their life. This presents an opportunity for exposure misclassification.
For example, a young man could have been in the Navy for 4 years and was exposed to asbestos, then worked 4 years in a textile mill where he was exposed to cotton dust, but from ages 34–65, he worked as bus driver. His primary occupation would be listed as a bus driver.
At this time, this approach to coding occupations may very well be the best way to correlate between occupational history and disease incidence, but it clearly can be misleading for some persons. Neither the MCD nor SEER databases, by themselves, track occupation for either men or women.
Shortcomings with anatomical locations of mesothelioma
It is important to understand anatomical sites such as pleural (originating in the lining outside of the lungs), peritoneal (abdominal cavity), and pericardial (heart) mesotheliomas, which are distinct diseases with different dose-response relationships, pathology, and survival rates.
Number of deaths and age-adjusted death rates for malignant mesothelioma in women above the age of 25 years organized by mesothelioma anatomical location (Mazurek et al., 2022).
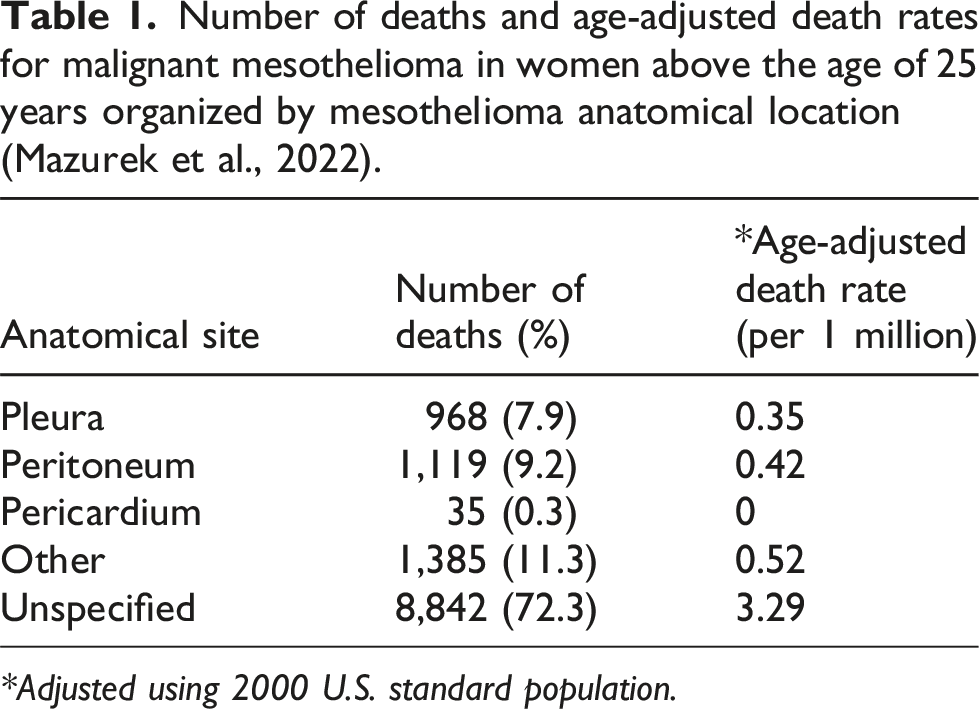
*Adjusted using 2000 U. S. standard population.
There are a number of papers that use the SEER database which provide a stronger analysis regarding the anatomical location of mesotheliomas (Moolgavkar et al., 2009; Price, 2022; Price and Ware, 2004, 2009). Unlike the MCD, the SEER database does not include anatomical locations that are labeled unspecified.
Pleural mesothelioma
Historically, it is estimated that approximately 80% of total mesotheliomas in men and approximately 60% in women are pleural mesotheliomas (McDonald and McDonald, 1980; Pavlisko and Sporn, 2014). Pleural mesothelioma in men is clearly correlated, when considering latency, with asbestos consumption in the United States from approximately the mid-1930s to the early 1970s (Price and Ware, 2009).
Since pleural mesothelioma make up the majority of cases, Price and Ware (2009) stated that “… the pattern over time of pleural mesothelioma was indistinguishable from the pattern for total mesothelioma defined as the sum of pleural and peritoneal cases.” Asbestos consumption peaked in the mid-1950s until 1972, when it rapidly declined in use over the years following (Price, 2022). There is strong evidence that the latency period of pleural mesothelioma due to asbestos exposure is 30 to 40 years (Pavlisko and Sporn, 2014). Based on the consumption trends, it makes sense that the age-adjusted incidence of pleural mesothelioma peaked in the 1990s (see Figure 1). Despite the massive increase in the use of asbestos between 1930 and 1970, there was no associated increase in the incidence of pleural mesotheliomas in women (see Figure 1).
Roggli et al. (2023) reported “…that asbestos fiber content of lung tissue [in those who developed mesothelioma] has steadily decreased over the past four decades, with a concomitant increase in the relative proportion of cases that are not asbestos related.” Specifically, “[a] decreasing percentage of [pleural mesothelioma] cases with an elevated lung asbestos content [in comparison to 20 subjects with no known exposure to asbestos and normal lungs at autopsy] was once again observed: 91.8% of cases in the 1980s, 93.1% in the 1990s, 84.6% in the 2000s, and 65.1% in the 2010s.” For all mesothelioma cases [not just pleural mesotheliomas] in the 2010s, Roggli et al. (2023) found that 54% had “elevated” fibers in their lungs compared to the reference population. Cases were considered “elevated” if at least one of five possible parameters exceeded the reference population: total asbestos bodies (by EM or LM), commercial amphibole fibers (amosite and crocidolite), non-commercial amphibole fibers (tremolite, actinolite, and anthophyllite), or chrysotile fibers. Observed and expected SEER data regarding age-adjusted incidence of pleural and peritoneal mesothelioma from 1915 to 1995 as well as the relevant exposures from 1973 to 2012 (recreated from Mezei et al., 2017). When considering a 30–40-year latency period, there is a strong association between asbestos use and pleural mesothelioma amongst men. Commercial asbestos use in the U.S. did not have a significant effect on peritoneal mesotheliomas for either men or women as the age-adjusted peritoneal mesothelioma rates are generally flat.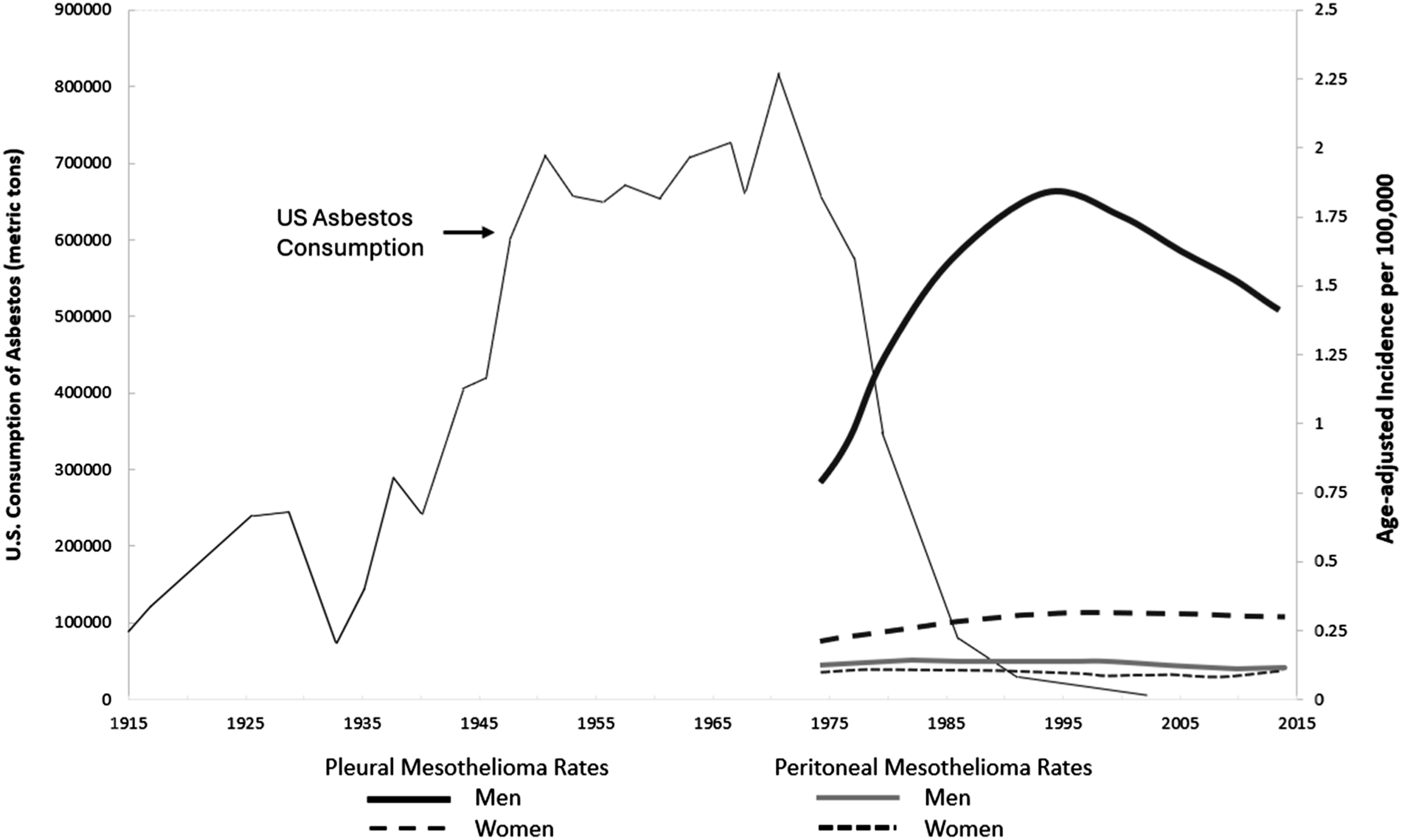
“Elevated” fibers in the lungs, as it is defined, can still be well below a dose of asbestos that would have any measurable impact on a person’s likelihood of developing mesothelioma. Roggli et al. noted, “Furthermore, women and peritoneal cases accounted for an increasing percentage [of mesothelioma cases] in the last two decades, and these groups are associated with a substantially lower number of cases with elevated tissue asbestos content” (Roggli et al., 2023).
Peritoneal mesothelioma
Historically, high cumulative airborne exposures of amphibole asbestos (i.e., 20 or more f/cc-years), only conceivable in the pre-OSHA era, have been associated with an increased incidence of peritoneal mesothelioma (Browne and Smither, 1983; Darnton, 2023; Selikoff et al., 1979).
Even for men, the incidence of peritoneal mesothelioma in the U.S. has been infrequently associated with occupational exposure to asbestos that occurred in the post-OSHA era (Moolgavkar et al., 2023; Price, 2022). From approximately 1940 to 1975, insulators who had high amosite asbestos exposures (estimated time-weighted average (TWA) exposures of 4 to 12 f/cc or cumulative exposures of 160 to 480 f/cc-years) had an increased incidence of peritoneal mesothelioma (Selikoff et al., 1965, 1979). With incredibly few exceptions (Cowan et al., 2015), it is unlikely workers (both men and women) in the United States have been exposed to enough amosite asbestos to have caused peritoneal mesothelioma since the mid-1970s due to regulatory and litigation pressures.
When accounting for latency, mesotheliomas as a result of exposures prior to 1973 would have been apparent by 2018 at the latest (assuming up to a 45-year latency). Moolgavkar et al. (2017) stated “Using combined data from the National Program for Cancer Registries (NPCR) and SEER, Henley et al. (2013) confirmed that between 2003 and 2008, female pleural mesothelioma rates were flat, whereas male rates continued to decline [and flatten out in the mid-2010s]. Trends in some European countries also [similar to those in the U.S.] indicate that a large fraction of peritoneal mesotheliomas is unrelated to asbestos exposure, with flat age-adjusted rates in both men and women (e.g., Burdorf et al., 2007; Hemminki and Li, 2003).”
If asbestos-related, peritoneal mesothelioma are associated with cumulative exposure levels much higher than those associated with pleural mesothelioma (Beckett et al., 2023; Darnton, 2023; Goswami et al., 2013; Pierce et al., 2016; Roggli et al., 1992). In short, it is highly improbable that peritoneal mesotheliomas that have been observed since the mid-2010s were caused by amphibole (or chrysotile) asbestos (for men/women).
Misdiagnosis is yet another possible confounder when interpreting MCD and SEER data. It is noteworthy that “[m]alignant mesothelioma must be distinguished from benign, reactive mesothelial proliferations on the one hand and on the other from various primary and secondary malignancies involving the serosal membranes” (Pavlisko and Sporn, 2014). As noted by Dr. Roggli, a distinguished pathologist, “Peritoneal carcinomatosis is commonly due to another primary malignancy and may readily be confused with peritoneal mesothelioma. Such a distinction is critical in determining whether a peritoneal malignancy might be asbestos related” (Personal communications with Roggli). Almost always, a careful histological examination with immunohistochemical analysis can discriminate between peritoneal mesotheliomas and another cancer, for instance, ovarian cancer.
Importance of fiber type and dimension
It is unfortunate that for the past 100 years, the term asbestos has been used without adequate precision of mineral type. It has brought about numerous misunderstandings in the scientific, medical and legal communities, as well as the public. Asbestos represents six distinctly different fibrous minerals. Chrysotile is the only serpentine asbestos fiber, while there are five forms of amphibole asbestos: amosite, crocidolite, asbestiform actinolite, asbestiform anthophyllite, and asbestiform tremolite (Gunter, 2010; Virta, 2002). Each is chemically distinct and has a different potency with respect to the risk for mesothelioma (Beckett et al., 2023; Darnton, 2023; Korchevskiy et al., 2019). Historically, approximately 95% of asbestos used in the world, and the related exposures, has been to chrysotile asbestos (Budavari, 1989: 893). It follows that if there was an opportunity for occupational asbestos exposure for women in the U.S., it would have primarily been to chrysotile and prior to the 1980s (Hein et al., 2007; Loomis et al., 2009; McDonald et al., 1984). Amongst the amphiboles, amosite and crocidolite were used commercially. Specific to women, one of the known exceptions in which amphibole exposure occurred are the women who worked in certain respirator manufacturing facilities during the years surrounding World War II (WWII) (Acheson et al., 1982; Schipske, 2008) or the use/manufacture of crocidolite containing Kent cigarette filters from 1952–1956 (Longo et al., 1995).
In addition to mineral type, fiber dimension has long been recognized as a determinant in the potency of asbestos (King et al., 1946). Specifically, it has been known since the early 1970s that long, thin fibers present a greater risk of disease than shorter fibers (Agency for Toxic Substances and Disease Registry (ATSDR), 2002; Eastern Research Group Inc., 2003a; Eastern Research Group Inc., 2003b; Lippmann, 1988; Stanton, 1973; Stanton et al., 1977). An 11 member ATSDR panel in 2002 “agreed that there is a strong weight of evidence that asbestos and short vitreous fibers shorter than 5 µm are unlikely to cause cancer in humans” based on “findings from epidemiologic studies, laboratory animal studies, and in vitro genotoxicity studies, combined with the lung’s ability to clear short fibers” (Eastern Research Group Inc., 2003b). Asbestos fibers are currently defined by OSHA as particles greater than 5 microns in length with a length to width (aspect) ratio of at least 3:1. In terms of aspect ratios, Korchevskiy et al. (2019) reported that chrysotile (Quebec) had a median aspect ratio of 7.09 (although chrysotile used in the textile industry could be much longer), while amosite (Transvaal) and crocidolite (South Africa, Bolivia, and Australia) were reported to have median aspect ratios of 8.59 (with a standard deviation of 2.4) and between 9.99 and 12.6 (depending on the region), respectively (Korchevskiy et al., 2019).
The difference in potency between fiber types for causing mesothelioma is dramatic. Numerous researchers have suggested that the relative potency for malignant mesothelioma between crocidolite, amosite, and chrysotile (the commercial forms) is approximately 500:100:1, respectively (Berman and Crump, 2003, 2008b; Darnton, 2023; Garabrant and Pastula, 2018; Hodgson and Darnton, 2000; Korchevskiy et al., 2019). Asbestiform anthophyllite appears to have roughly the same potency as amosite, while Libby amphiboles, actinolite, and tremolite appear to have less than half the potency of amosite (Garabrant and Pastula, 2018; Korchevskiy et al., 2019). Thus, when discussing exposures to asbestos fibers, it is important to identify the specific fiber type. Exposure to an equal airborne concentration of chrysotile, amosite, and crocidolite would have significantly different risks of developing mesothelioma.
Consistent with these analyses on fiber type potency, Yarborough (2006) concluded that “[e]pidemiological studies investigating mesothelioma risk from exposures of cohort members to chrysotile asbestos fibers not known to be contaminated with amphiboles do not justify a conclusion of causality at this time.” Berman and Crump (2008a, 2003) supported the widely held belief that pure chrysotile may be non-potent for mesothelioma based on the epidemiology data. Darnton (2023) recently published a meta-analysis that included the most up to date occupational epidemiology data. This data is not inconsistent with the theory that pure chrysotile asbestos fibers may have near zero potency for mesothelioma.
There continues to be a growing body of evidence that chrysotile does not pose a mesothelioma hazard except, perhaps, at doses greater than those that cause asbestosis (which occurs at a minimum of 25–100 f/cc-years). A “best estimate” no-observed-adverse-effect-level (NOAEL) for typical cohorts with chrysotile exposure has been estimated to be between 250 and 379 fibers/cc-year (f/cc-year) (Beckett et al., 2023). This estimate is based on an epidemiological analysis of 16 cohorts that were exposed to mainly chrysotile asbestos (less than 10% amphibole) (Beckett et al., 2023). Exposures of this magnitude were likely only feasible for persons who worked in an asbestos brake factory in the 1930s through 1950s (Berry, 1994: 540), or in an asbestos mine (McDonald et al., 1980: 16), raw asbestos processing factory (Darnton, 2023), or as an insulator in a shipyard (Selikoff et al., 1979), all in the pre-OSHA era. NOAELs for amosite and crocidolite appear in the ranges of 2–5 f/cc-years and 0.6–1 f/cc-years, respectively (Beckett et al., 2023). This is, of course, relevant in understanding why asbestos has generally not been a substantial cause of mesothelioma in women in the U.S. at any time.
The historical trends of women’s occupational exposures to asbestos in the United States
Asbestos exposure due to unrecognized sources has recently been suggested by some published papers to be the primary reason for the increasing incidence in mesothelioma among women (Baur et al., 2023; Kanarek and Liegel, 2020; Kanarek and Mandich, 2016; Mazurek et al., 2022); however, this conclusion does not fit historical trends and historical occupational exposures. For example, nearly all mesotheliomas due to asbestos occurred because of workplace exposure from the 1930s to 1970s, and these occupations were nearly always limited to men. Women in the United States have generally not been occupationally exposed to asbestos, aside from some exceptions including surrounding WWII production efforts (Acheson et al., 1982; Schipske, 2008).
This lack of historical exposure is the reason that age-adjusted mesothelioma death rates for women have been flat since the data were originally recorded in 1975 (Price, 2022; Price and Ware, 2009). Price estimates that, based on the data in Lane (1951), “10% of women born between 1900 and 1924 worked in high asbestos exposure jobs during WWII; subsequently, 0.1% of women born between 1925 and 1959 worked in high asbestos exposure jobs” (Price, 2022). In 2023, women born between 1900 and 1924 would be between 99 and 123 years old; well beyond the current lifespan published by National Center for Health Statistics (NCHS) (2023). If women were exposed to appreciable concentrations of airborne amphiboles in the factories supplying goods for WWII (1939–1945), and if they did develop mesothelioma, the number of cases was not sufficient to alter the age-adjusted incidence rate in American women shown in the SEER database (Moolgavkar et al., 2009; Price, 2022; Price and Ware, 2009).
The possibility of at-risk occupations
The MMWR by Mazurek et al. (2022) noted that “Among 21 industry groups, the three with the most deaths were health care and social assistance (89, 15.7%); education services (64; 11.3%) and manufacturing (50; 8.8%).” The authors noted that “The three occupations with the highest numbers of mesothelioma deaths were homemakers (129; 22.8%); elementary and middle school teachers (32; 5.6%); and registered nurses (28; 4.9%)” (Mazurek et al., 2022: 646). These percentages do not account for the number of women performing these occupations and, as such, are not informative as presented.
The suggestion that these occupations are at elevated risk of mesothelioma, (Gao et al., 2023; Moline et al., 2023) is inconsistent with the epidemiology and the exposure data (discussed below). Any suggestion that these occupations present an asbestos health hazard is, based on the evidence, unsubstantiated.
Because suspected asbestos exposures have been lacking, the occupations predominated by women have not received much study, but when they have, there has been no increased risk of mesothelioma amongst teachers (Stellman and Stellman, 1981; Rolland et al., 2010: 1212), finished goods textile workers (Hein et al., 2007: 620; Agudo et al., 2000: 163), and nurses (Stellman and Stellman, 1981; Rolland et al., 2010: 1213). Teschke et al. (1997) performed a large epidemiology study of mesothelioma (peritoneal and pleural) among many occupations. They reported odds ratios (OR) and confidence intervals (CI) for health care workers, teachers and librarians, office clerks and secretaries, and housekeepers (Teschke et al., 1997). These occupations had no statistically increased risk of pleural mesothelioma when compared to background. Based on numerous epidemiology studies, women in the occupations for which Mazurek et al. (2022) expressed concern and the need for more research, have shown no increased risk of peritoneal nor pleural mesothelioma when corrected for age (Agudo et al., 2000; Rolland et al., 2010; Teschke et al., 1997; Teta et al., 1983).
The lack of exposure to asbestos by women has been discussed in the literature for several decades. For example, Stellman (1994) did not list asbestos as an occupational hazard for women in any of the common occupations that they studied. Although that observation was made more than 25 years ago, there is no reason to believe that exposures have increased since then. Even for men, there has been little opportunity to be exposed to either chrysotile or amphiboles since the 1980s (Cowan et al., 2015; Moolgavkar et al., 2023; Price, 2022; Williams et al., 2007b). In the late 1980s, the federal government banned asbestos in products. This ban was later overturned in court; however, the national effort to remove asbestos from commercial products had already taken effect. There have been very little new uses of asbestos in the United States since that time. For those women involved in remediation or abatement work to remove old asbestos-containing materials, PPE and other measures prevent exposure (Paustenbach et al., 2023; U. S. Environmental Protection Agency (EPA), 2011).
The EPA has expressed concern about chrysotile-containing brakes in automobiles, but asbestos-free products were substituted in vehicles during the 1980s and asbestos was no longer used in virtually all passenger vehicles and light trucks by 2000 (U.S. Environmental Protection Agency (EPA), 2020; Paustenbach et al., 2021; Paustenbach et al., 2004). Exposures of mechanics to asbestos have been shown to be quite low, a mean of 0.05 f/cc of chrysotile during a brake job, even during the era when asbestos was in brakes (Paustenbach et al., 2003). Although the epidemiology does not support they were ever at risk (Paustenbach et al., 2004; Garabrant et al., 2016) generally speaking, women were not vehicle mechanics over the past 60 years.
Some published papers highlight the fact that “Although asbestos is no longer mined in the United States, as of early 2022 it is still imported and used” (Kanarek and Mandich, 2016). This observation, without quantification and an understanding of the products, is irrelevant from a human health standpoint. There has been almost no use of asbestos in the U.S. over the past 40 years, with two exceptions; the chlor-alkali industry’s use of raw chrysotile and the rare use of crocidolite gaskets in chemical production (Paustenbach et al., 2021; U.S. Environmental Protection Agency (EPA), 2020). These rare instances of industrial uses persist due to a lack of suitable and safe alternatives to asbestos for this purpose. In the chlor-alkali industry, employee medical monitoring as well as asbestos exposures have been carefully monitored (per OSHA requirements) and are low as a result of engineering controls, PPE, and access restrictions (American Chemistry Council (ACC), 2022; U.S. Environmental Protection Agency (EPA), 2020).
The available information indicates there are ample data to support conclusions regarding women and their associated mesothelioma incidence or risk. The rates of mesothelioma in women have been tracked for many years, and four studies have discussed the trend using SEER data (Moolgavkar et al., 2009; Price, 2022; Price and Ware, 2004, 2009). Based on our review, the epidemiology literature does not support claims that mesothelioma in women is related to exposure to asbestos, except for the few historical instances that have been mentioned previously (FDA, 2019; FDA, 2021; FDA, 2022a; FDA, 2022b; Lewis et al., 2023; Miller et al., 2022; Miller et al., 2024; Pierce et al., 2017).
The potential for various unidentified exposures to asbestos in the post-OSHA era
The MMWR and some other reports (Baur et al., 2023; Kanarek and Mandich, 2016; Mazurek et al., 2022) have raised concerns that there may be some unidentified low-level exposures to asbestos, of which scientists are not aware, which may be of concern to women. Shortly after the mesothelioma hazard of asbestos became known (Selikoff et al., 1965), a series of OSHA regulatory initiatives were put in place starting in 1971 (Martonik et al., 2001). There was a widespread decline in workplace airborne concentrations of asbestos over time as a result of the increasing awareness (Cowan et al., 2015). In our review of the epidemiology and the historic airborne concentrations across a number of industries (Cowan et al., 2015; Williams et al., 2007a, 2007b), there is almost no evidence of continued exposure to concerning airborne concentrations of asbestos (those that would increase the risk of disease) since these controls were implemented in the United States.
Mazurek et al.’s MMWR stated that women might be exposed to asbestos today in “… work settings as a consequence of disturbance of previously installed friable asbestos-containing materials during maintenance or renovation, or the resuspension of settled fibers into the air caused by dusting, sweeping, or cleaning” (Mazurek et al., 2022: 647). As discussed previously, there are no occupations common amongst women in which plausible cumulative exposures to amphiboles or even chrysotile (above background) would likely occur over the past five decades (the post-OSHA era). Not long after the promulgation of OSHA, nearly all the friable asbestos-containing materials were no longer sold and not many encapsulated products were sold after about 1985 (e.g., gaskets, brakes, bakelite items, floor tiles). Large companies generally issued directives to staff and purchasing departments that no asbestos-containing materials or products were to be purchased after 1975 (Paustenbach et al., 2021).
Laws are in place, and have been for half a century, which require awareness of the presence of friable asbestos in nearly every environment (Occupational Safety and Health Administration (OSHA), 1972b). In modern settings in the United States, suspected asbestos-containing insulation is required to either be removed or the insulation is kept intact under many coats of sealant (U. S. Environmental Protection Agency (EPA), 1985). Commercial buildings, especially offices, began removing friable or damaged asbestos-containing materials in the early 1980s using certified asbestos abatement firms. Intact or non-friable asbestos-containing products are generally considered safe and have been historically exempt from federal asbestos labeling requirements (Occupational Safety and Health Administration (OSHA), 1995; Selikoff, 1970; U.S. Environmental Protection Agency (EPA), 1990; Mowat et al., 2005). Many buildings, especially schools and hospitals, chose not to remove materials because the hazard associated with wrapped and painted asbestos-insulated pipes was de minimis.
Hundreds of buildings were sampled in the 1980s and very low or non-detectable airborne concentrations of asbestos were reported (Lee et al., 1992).
For the past four decades, there have been mandated procedures in place to minimize or eliminate exposure to asbestos in insulation or historical products during removal (e.g., PPE, negative pressure plastic containment areas, wetting of materials, removal of materials in sealed bags, asbestos monitoring devices) (EPA). The EPA’s Asbestos Hazard Emergency Response Act of 1986 was the first of these mandates. Clearance samples of the air and the surfaces are always collected to ensure that there is a de minimis amount of residual fibers before the area is re-occupied. Concern that fibers are still distributed in some workplaces or offices due to remediation activities is almost never warranted (based on what is known about fiber settling and resuspension, discussed in the section below). In our experience, which collectively involves hundreds of evaluations, the number of unknown exposures in the indoor environment for at least the past four decades is expected to be zero or almost certainly below the limit of detection of the analyses under normal circumstances (Paustenbach et al., 2021).
Fiber resuspension (occupationally and non-occupationally)
Relevant to both occupational and non-occupational exposures, the resuspension of trace quantities of asbestos fibers from floors is often one of the suggested routes of plausible exposure. There have been studies performed to evaluate that hazard. The exposures have been shown not to be a hazard in nearly all situations (Corn and Stein, 1965). Aside from some anecdotal claims, the literature indicates that resuspended asbestos fibers (5 microns or greater in length), if initially on the floor of a building, are rarely a hazard of concern (Kelman et al., 1994; U.S. Environmental Protection Agency (EPA), 2003a; U.S. Environmental Protection Agency (EPA), 2003b; U.S. Environmental Protection Agency (EPA), 2005).
A 2009 EPA report concluded that resuspended fibers due to walking decreased substantially as carpet pile height decreased. They reported that previous studies revealed that “No measurable dusts were observed from dusts on bare flooring… Low pile, indoor-outdoor carpeting also provided essentially immeasurable air concentration levels.” The 2009 EPA study, which including walking and vacuuming on medium-pile carpeting, revealed K-factors (the ratio of resuspended particles, although not necessarily respirable fibers, compared to surface loading) ranging from 0.01–0.0001, depending on particle factors (U.S. Environmental Protection Agency (EPA), 2009). In other testing of the resuspension of particulate matter from medium-pile carpet during walking or jogging under various humidity (20%, 40%, 80%), HVAC, and carpet conditions, Rosati et al. (2008) found that “walking on ‘real-world’ carpet did not result in the measurable (above real-world background) resuspension of particles smaller than 0.7 μm [diameter].” For particulate matter greater than 0.7 μm, the authors surmised that electrostatic force was the primary adhesion mechanism for new, unsoiled carpet, which increasing relative humidity would neutralize, but increasing relative humidity decreased the resuspension of particulate matter from older carpet due to capillary adhesion force and greater contact area (Rosati et al., 2008).
The general understanding, based on both theory and field measurements, is that fibers that are biologically significant bind tenaciously to flat surfaces (Corn and Stein, 1965: 332). This is because of van der Waals forces, electrostatic forces, and surface tension, which make it nearly impossible to resuspend them (Esmen, 1996: 379). For particles between 5 and 30 microns in length, at a 3:1 aspect ratio, the diameters would range from at most 1.6 to 10 microns in diameter. Corn and Stein (1965) reported that particles less than 0.5 microns and 5 microns in diameter are generally not removed by an air stream with a velocity of 335 mph and 200 mph, respectively. Similarly, Hinds (1999) reported that for particles less than 10 microns in diameter the adhesive force (van der Waals forces, electrostatic force, and surface tension) on the particles adheres them tightly together such that they cannot be easily dislodged or removed by “common forces” (Hinds, 1999: 144). Hinds and Zhu (2022) published the third edition of Aerosol Technology: Properties, Behavior, and Measurement of Airborne Particles, in which they cite research conducted by Corn and Stein (1965) and have mathematically shown that air velocities up to 200 miles per hour will not dislodge particles up to 10 microns in size from a surface. Thus, the concerns about the resuspension of fibers in offices or homes in the post-1960 era are usually without merit.
When airborne, the weight of evidence from multiple studies indicates that under typical conditions it takes approximately 20–80 min for 99% of airborne fibers to settle and be cleared from the air (Sahmel et al., 2015). Before assessing the particle physics, for resuspension to occur, the fibers need to be present in the first place.
The likelihood of take-home and para-occupational exposures
It has been suggested that take-home or para-occupational asbestos exposure over the past 45 years might explain some cases of mesothelioma among women in the U.S. since 2010. However, as Roggli et al. (2023) and others have noted, since the likelihood of spontaneous mesotheliomas increases logarithmically after age 55, it is impossible to determine whether any of the mesotheliomas alleged to be due to take-home exposure in the last 10–15 years are spontaneous or due to low-level exposures to amphiboles. For example, a 25-year-old woman in 1970 would be 65 years old in 2010 and nearly 80 years old today.
In the pre-OSHA era, particularly in the 1930s to 1960s, some workers (insulation workers, miners, asbestos product manufacturers, shipyard workers) went home with significant amounts of amosite on their clothing which presented a hazard to a spouse or family member who laundered this clothing (Gross, 1997; Metro-North Commuter Railroad Co v. Buckley, 1997). During this era, it is noteworthy that the review by Donovan et al. (2012) reported a small percentage of the mesotheliomas associated with household exposure were peritoneal (19 vs 259 pleural mesotheliomas). Post-1972, the OSHA regulation required change rooms and two clothes lockers to prevent the contamination of street clothes for occupations in which some fraction of the airborne samples collected exceeded the PEL for regulated chemicals (Occupational Safety and Health Administration (OSHA), 1972a). With the massive amount of attention asbestos had gained through the years, employers who continued to use asbestos-containing materials, especially given the threat of injury and litigation, tended to be diligent in following regulations specific to asbestos.
These regulations were especially effective in industries with labor unions (Paustenbach et al., 2023; Weil, 1991, 1992). Change rooms, employer laundering of contaminated clothing, abatement of asbestos building materials, additional workplace controls, and a decreased use of asbestos, is why it has generally been more than 45 years since high-risk occupations (asbestos product manufacturing, insulators, shipyard workers, and miners) brought home clothing covered with asbestos to be laundered (Donovan et al., 2012; Goswami et al., 2013). If heavily contaminated clothing was laundered by a spouse in the 1945–1975 era, for the plausible cumulative exposures of the launderer to pose a mesothelioma hazard, the fibers would need to be amphiboles. Take-home exposure to chrysotile has generally been believed to pose no mesothelioma hazard (Donovan et al., 2012; Goswami et al., 2013; Wagner et al., 1960) as the plausible doses (Ferracini and Sahmel, 2024; Sahmel et al., 2014) would not be sufficient to cause disease given the low potency of the fibers (Beckett et al., 2023; Darnton, 2023).
In the United States, Vianna and Polan (1978) reported a 10-fold increase in the relative risk of mesothelioma among women in the 1930 to 1950 era with a husband or father in the asbestos industry. This paper is often referenced, but more recent study periods do not support that such an elevated risk persists beyond this time period (Ferracini and Sahmel, 2024). The simulation study by Sahmel et al. reported that the inhaled dose while handling contaminated clothing was usually less than 1% of the airborne concentration of the activities through which the clothing was originally exposed (Sahmel et al., 2014). Furthermore, the duration was much shorter for handling contaminated clothing prior to placing the items in the washing machine (2–5 min) compared to the typical occupational exposures (4–8 h/day). It has been reported that the cumulative lifetime exposure through handling chrysotile-contaminated clothing was comparable to lifetime chrysotile exposure to ambient air (Sahmel et al., 2014). A recent review by Ferracini and Sahmel (2024) indicated that the potential ratios of take-home exposure were in the range of approximately 0.2%–6.5%, depending on the study.
For a hazard from laundering a spouse’s clothes to be appreciative, the spouse would have needed to be exposed to extraordinarily high concentrations of amphiboles and the worker would not have blown any dust off of their clothing with a high pressure air hose at the end of the work day (which was commonplace when asbestos was relevant in industry) (Abelmann et al., 2017; Colinet et al., 2007; Pollock et al., 2006). Based on the weight of evidence, take-home exposure to amphiboles has not occurred in any appreciable manner for almost 50 years and is certainly not a concern today in the United States.
Non-occupational use of talcum powder
Some have raised a concern regarding mesothelioma due to trace amounts of tremolite in cosmetic talcum powder, but (as summarized in Ierardi et al. (2024)) the vast amount of bulk sample data indicate that, if tremolite was detected, it was non-asbestiform and the concentrations in cosmetic talc powder were at trace amounts (Food and Drug Administration (FDA), 2019, Food and Drug Administration (FDA), 2021, Food and Drug Administration (FDA), 2022a, Food and Drug Administration (FDA), 2022b; Kennedy, 1979; Miller et al., 2022, 2024; Pierce et al., 2017). Also, the epidemiology data do not support a relationship between cosmetic talcum powder end users and mesothelioma (Lewis et al., 2023). Ierardi et al. (2024) concluded that “The current weight of evidence suggests that relatively pure talc, which is used in cosmetics, as well as other consumer products, does not pose a carcinogenic health risk upon inhalation.”
The risk factors for mesothelioma when asbestos exposure is absent
In their MMWR, Mazurek et al. (2022) suggested that, even in 2022, the mesotheliomas that are observed in most persons are due to exposure to asbestos. This belief is often repeated in some published papers (Baur et al., 2023) and news articles (American Industrial Hygiene Association (AIHA), 2022). While it may have been historically accurate for males exposed in the pre-OSHA era, the statement that “Malignant mesothelioma … is almost always caused by asbestos or other asbestiform fibers” (Baur et al., 2023) is out-of-date; certainly when referring to mesotheliomas in 2023 and beyond. When considering the time periods in which significant amphibole exposures occurred and the latency of asbestos-induced mesotheliomas, it is unsurprising the number of asbestos-induced mesotheliomas has plummeted over the last decade (Price, 2022).
Price (2022) examined age-adjusted mesothelioma rates (for men and women) in comparison to mesothelioma use in the United States. Although the absolute number of mesotheliomas is higher for women compared to 20 years ago, and it will continue to climb due to increasing population size and life expectancy, the age-adjusted incidence for women has remained flat since the 1970s (and this would likely would be the case for the decades prior) because, by and large, they have not been exposed to asbestos. However, it should be acknowledged that the incidence of mesothelioma in men has strongly correlated to the consumption of asbestos plus latency (Figure 1). When one accounts for the 30–40 years latency for asbestos to cause mesothelioma, Figure 1 supports Price’s conclusions that an estimated 75% of the current mesotheliomas in men are non-asbestos related (personal communications with Bert Price, 2022) and that by 2040, virtually all mesotheliomas will be non-asbestos related (Price 2022). This is consistent with the work of (Tomasetti et al., 2015, 2017; Tomasetti and Vogelstein, 2015) indicating that about 67% of all cancer risk (not just mesotheliomas) is due to random mutations.
The importance of age on the onset of mesothelioma
By definition, cancer is a disease of the genome, meaning it arises from mutations in the genetic material within cells. The vast majority, if not all, of the malignant mesothelioma cases in the populations of women are unknown in origin or are primarily due to age and an accumulation (and lack of repair) of spontaneous genetic mutations (Moolgavkar et al., 2017: 58). As the MMWR authors stated, “Increases in total number, but not age-adjusted death rates, suggest that changes in underlying annual age distributions of the population over time are contributing to the observed increases in total mesothelioma deaths in women” (Mazurek et al., 2022: 647).
Carbone et al. (2023) has noted that “the risk of developing most cancers, including mesothelioma, increases with old age because of the inevitable accumulation of genetic damage in our cells. Therefore, the older the population, the higher the incidence of cancer, including mesothelioma” (Carbone et al., 2023: 695). This is due to impaired DNA repair mechanisms for replication errors resulting in an accumulation of spontaneous mutations (Garraway and Lander, 2013; Stratton et al., 2009; Tomasetti et al., 2017; Vogelstein et al., 2013). According to Tomasetti et al., 2017, “Recent evidence from mouse models supports the notion that the number of normal cell divisions [which corresponds with age] dictates cancer risk in many organs (Zhu et al., 2016).” To illustrate the importance of age on the development of mesothelioma, it has been shown that “Every doubling of age increases the risk of pleural mesothelioma approximately 30-fold and that of peritoneal mesothelioma approximately eightfold” (Moolgavkar et al., 2017: 46).
Number of deaths and age-adjusted death rates for malignant mesothelioma in women in the United States above the age of 25 years organized by 10-year age increments (Mazurek et al., 2022).
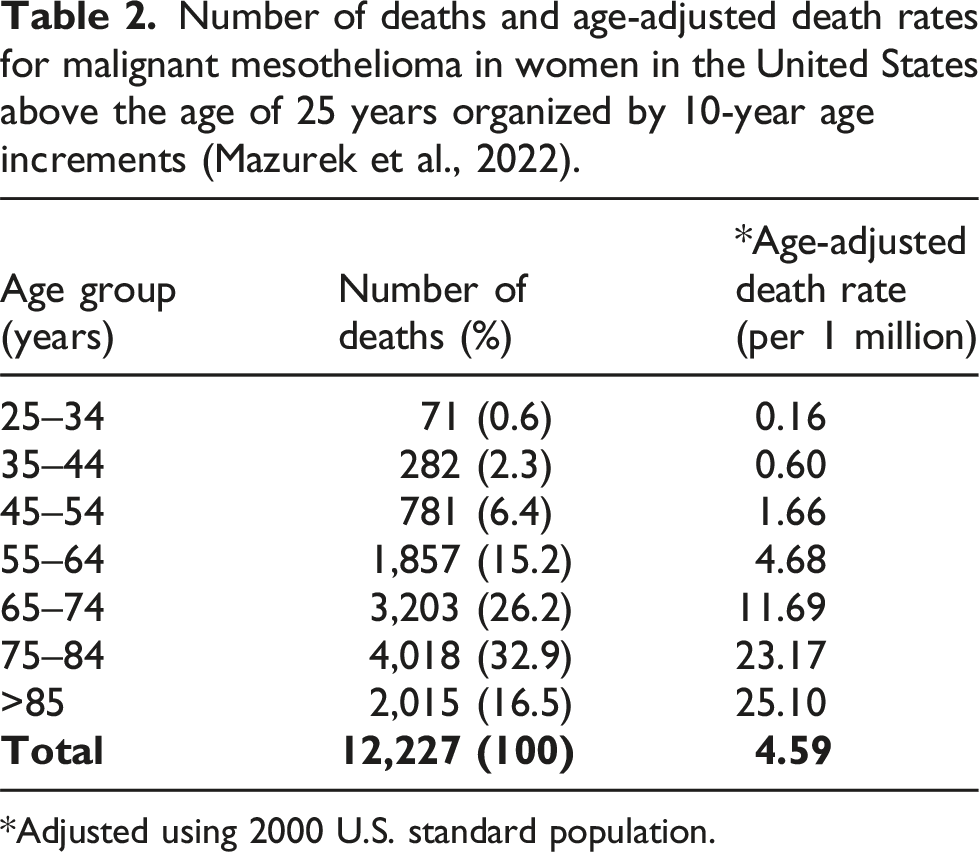
*Adjusted using 2000 U.S. standard population.
Similar to the MMWR data, the most recent World Cancer Report shows that cancers have been increasing as a percentage of all deaths (Wild et al., 2020: 568); primarily because we have made advances with respect to preventing cardiovascular disease through medication and the decreasing percentage of smokers. In short, progress made in eradicating, curing, or preventing many diseases in the nineteenth and early twentieth century has allowed persons to live much longer, and thus, the absolute number of all cancers is increasing.
Other alternative explanations for background incidence of mesothelioma
Medical treatment for cancer and other ailments using radiation therapy is a cause of secondary cancers, with mesothelioma being among them (Attanoos et al., 2018). In large measure, the high radiation doses that caused secondary cancers ended by 1990–2000, but the impact of some of these treatments are just now being observed (Cavazza et al., 1996; Sekine et al., 2021; Teta et al., 2007). It is noteworthy that one would rarely know if it was the treatment or old age that caused a particular mesothelioma in those populations.
Unlike radiation, which directly affects DNA, chronic inflammation has been found to be a necessary precursor in the pathogenesis of some cancers and is generally considered the mode of action by which asbestos causes mesothelioma (Cox, 2019; Mossman, 2018; International Agency for Research on Cancer (IARC), 2012; Thompson and Shukla, 2017; Cox et al., 2020). The inflammatory response involves the release of reactive oxygen species and immune cells, which can damage the DNA of normal cells, increasing the risk of mutations and, therefore, cancer (Singh et al., 2019). With this understanding, many experts believe that chronic irritation of or around the peritoneum, such as intra-abdominal shunt catheters (Mujahed et al., 2021), Crohn’s disease (Attanoos et al., 2018; Butnor et al., 2017), and endometriosis (Butnor et al., 2018; Malpica et al., 2022), increases the risk of peritoneal mesothelioma. All of the diseases associated with repeated irritation or cytotoxicity are believed to have a threshold dose (Weisburger and Williams, 1989; Klaunig and Kamendulis, 2007: 347; Klaunig and Wang, 2019: 450).
Although exposures are likely rare in the United States, erionite and other non-asbestos mineral fibers have gained attention in recent years as they are expected to contribute to the risk of developing mesothelioma via a similar mechanism to amphibole asbestos (Carbone et al., 2012; Stevens et al., 2024).
Genetic Susceptability
It has been known that genetic susceptibility can play a large role in the development of both pleural and peritoneal mesothelioma. This has been discussed at length over the past 10 years by Carbone et al. (2013, 2019, 2020), Testa and Berns (2020), and others. Having genetic mutations in DNA repair can mean that a person has a greater probability of developing mesothelioma following even low-level exposure to an amphibole asbestos fiber, or the mesothelioma (both pleural and peritoneal) can develop without any exposure to asbestos. For example, it is now known that persons develop mesothelioma simply due to inadequate DNA repair due to mutations of these specific germlines, including young children (without asbestos exposures) (Argani et al., 2021; Brenner et al., 1981; Moran et al., 2008; Wolff-Bar et al., 2015; Mijalovsky et al., 2018; Silberstein et al., 1983; Nishioka et al., 1988; Lin-Chu et al., 1989).
While research advances occur regularly, it is currently understood that genetic mutations that affect the BRCA1-associated protein 1 (BAP1) is the one most commonly associated with mesothelioma (Carbone et al., 2013, 2019, 2020). Napolitano et al. (2016) found that germline BAP1 heterozygosity increased mesothelioma incidence by way of the peritoneal inflammatory response when exposed to low-dose asbestos fibers. Badhai et al. suggests additional mutations (Nf2 and Cdkn2ab, which are also frequently observed in human mesotheliomas), in combination with BAP1, led to the rapid onset of mesothelioma in 100% of mice and BAP1 deletion alone caused mesotheliomas in 1 out of 20 mutant mice (5%) in the absence of asbestos exposure (Badhai et al., 2020).
In small sample groups, Testa et al. (2011) and Bott et al. (2011) found between 22%–23% of mesotheliomas in humans had a BAP1 mutation (Bott et al., 2011; Testa et al., 2011). For mesotheliomas the authors defined as sporadic, 8% (2 out of 26), in the Testa et al. study had BAP1 mutations (Testa et al., 2011). A later study by Panou et al. determined that 26% of mesotheliomas with no known asbestos exposure had some form of germline mutations. Of these germline mutations found, 25% (6.5% of the total) were in the BAP1 gene (Panou et al., 2018). A more recent study by Carbone et al. reports that 84.3% of BAP1 deletion carriers (295/350 carriers) (all ages) developed some form of cancer and 29.6% of them developed mesothelioma specifically (an even amount of pleural and peritoneal mesotheliomas) (Carbone et al., 2020).
Currently, the available human data leans toward the notion that germline mutations (BAP1 and others) may induce mesothelioma independent of asbestos exposure (Attanoos et al., 2018). Patients diagnosed with mesothelioma are rarely tested for germline mutations (personal experience of the authors and personal communications with Dr. Victor Roggli and Dr. Steven Smith, 2024). It is apparent that this testing could lead to an improved understanding of the role of genetic susceptibility and mesothelioma.
Discussion and conclusion
Like others who have raised awareness of the hazards of asbestos, we recognize that asbestos has historically had a catastrophic effect on the health of mostly male workers, dating back almost 100 years. Fortunately, the opportunity to experience cumulative exposures in the United States which might cause these diseases generally ended by the mid-1970s and, surely, not much later than 1980. The virtual elimination of all sales of all forms of asbestos in the United States was a remarkable achievement. The controls implemented after 1972 (when the OSHA asbestos regulation was promulgated) have likely prevented thousands of persons from developing asbestos-related diseases over the past 50 years. A virtual ban on imports in the United States was formally announced early in 2024 (U.S. Environmental Protection Agency (EPA), 2024).
The primary reason, if not the sole reason, for the increased incidence of mesothelioma deaths in the United States, especially in women, in the post-OSHA era is increased longevity. The incidence of mesothelioma in women, when corrected for age, suggests that the historical exposure for women to asbestos fibers has typically been, from a large-scale health perspective, virtually the same as background exposure since the 1930s (when considering latency) (Price, 2022). The number of women, if any, that developed mesothelioma as a result of significant amphibole exposures in the factories supplying goods for WWII (1939–1945) or other exceptional circumstances was not sufficient to alter the national age-adjusted incidence rate in women in the SEER database (Moolgavkar et al., 2009; Price, 2022; Price and Ware, 2009).
As noted above, Price and Ware (2009) reported that “The absence of a time trend in age-adjusted female mesothelioma incidence [as seen by the flat rate in Figure 1] suggests that most female cases may not be a consequence of asbestos exposure and the female rate may be an estimate of the risk of background.” That was reinforced in a paper by Price (2022), where he noted that a significant number of the current mesotheliomas in men (Price estimates 75%) are non-asbestos related and that by 2040, virtually all mesotheliomas will be non-asbestos related. This conclusion, when considering a 30–40-year lag from the time of exposure until the disease presents, coincides with government regulations promulgated by OSHA in 1972; soon thereafter, amphiboles were phased out of manufacturing and commercial products, and the restrictions on occupational exposure tightened markedly. By 2040, persons who were potentially first exposed in the early 1970s at age 20 would be around 80 to 90 years old.
As scientists, it is important that we correct misunderstandings that have crept into the scientific and lay literature because we run the risk of misleading policymakers to spend resources where there is a good chance of no resulting improvement in the overall public well-being. As Kabak, a researcher at the Albert Einstein Medical school, has warned: “The distortion of information about health risks has consequences and costs … Clearly, resources devoted to a poorly-substantiated threat cannot be devoted to less sensational lines of work, which may prove to be more valuable. Another cost entails the needless anxiety about problems that were miniscule or non-existent … The amplification of hazards diverts attention from real and consequential dangers” (Kabat, 2008)
There are many things to consider when assessing epidemiology data. The topics addressed in this paper; (1) shortcomings in the national databases, (2) fiber type, (3) historical exposures amongst women, (4) the likelihood of take-home and para-occupational exposures, (5) the potential for modern exposures, and (6) alternative risk factors (including genetic susceptability), if not properly considered, can lead to misleading conclusions. This illustrates why it is important to thoroughly consider the relevant variables when conducting these analyses and interpreting the data. This analysis should bring some clarity to erroneous claims that mesotheliomas in women are increasing, allegedly due to asbestos from some unknown source.
Footnotes
Author Contributions
All authors completed the requirements for authorship according to the “Uniform Requirements for Manuscripts Submitted to Biomedical Journals,” developed by the ICMJE. All listed authors had an important role in the literature review, writing, and revisions to the paper that led to the final version, approved of said final version, and agreed to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors work within Paustenbach and Associates, which is a consulting firm headquartered in Jackson, Wyoming. The firm specializes in conducting risk assessment of occupational and environmental hazards, as well as contaminated foods, sediments and soils, ambient air, radiological sites, and consumer products. This paper was funded internally by Paustenbach and Associates. Its development was not requested by any entity or law firm. No lawyer had input into the text and no lawyer has read this document prior to submission.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not required for this paper. There were no experimental procedures performed on humans or animals.
Data availability statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.