
Abstract
Physical activity (PA), including active travel (AT), is related to healthy adolescent development and wellbeing, however, behavior rates are low. Simultaneously, adolescent screen use, and engagement in social media platforms (SMP) is very high. The aim of this mixed methods study was to explore the relationship between peer engagement and SMP and adolescent AT and PA. We employed an exploratory sequential design that included integration of results of qualitative interviews with 25 adolescent-parent dyads and quantitative data from a cross-sectional survey in a representative sample of Hebrew-speaking adolescents in secondary schools across Israel (n = 2,911). Reflexive thematic analysis was employed for the qualitative study; constructs identified served as the basis for development of a quantitative data collection instrument. Correlation and linear regression analyses were conducted to investigate associations between key quantitative analysis variables. The integrated analysis primarily identified convergence between datasets expressed in narrative weaving and joint displays. We found that AT with peers is a social activity; AT and PA are an opportunity for peer-to-peer communication without screens; and SMP are utilized to promote AT and PA. Interventions that emphasize these key constructs as well as use of SMP may increase adolescent AT and PA behaviors.
Physical Activity, Active Travel, and Adolescent Wellbeing
During the transitional period from childhood to adulthood, adolescents develop physically, psychologically, and socially. Adolescence is also a key phase of identity formation. As youth experience further independence and autonomy, their interactions with their peers, communities, and schools increase, contributing to identity development (Erikson, 1968). Participation in consistent physical activity (PA) is related to adolescent health and wellbeing as well as prevention of chronic disease in the future (Alberga et al., 2012; Biddle et al., 2019; Janssen & LeBlanc, 2010; Poitras et al., 2016). At this stage in life, adoption of healthy behaviors is critical; acquiring positive habits and potentially long-term lifestyle choices (Craigie et al., 2011). In spite of the contribution of this key health behavior to adolescent wellbeing, global levels of PA are low; in a review of data from 146 countries, 81% of students age 11 to 17 years did not meet recommended PA levels (Guthold et al., 2020). During and subsequent to the COVID-19 pandemic, further reductions in PA and increase in sedentary activities have been reported for adolescents in many countries worldwide (Aubert et al., 2022; Kharel et al., 2022). Moreover, adolescents around the world spent more time online; including higher use of social media platforms (SMP) (Marciano et al., 2022). There have been concerns that the short and long-term repercussions of COVID-19 will further impact and accelerate a lack of PA and sedentary behaviors, which are in turn related to increased chronic disease (Hall et al., 2021).
Active travel (AT), transport modes based on human effort including walking and cycling, is a method to incorporate PA in daily life and activities. Rates of AT are considered a core PA indicator for children and adolescents as well as adults (Aubert et al., 2022; International Society for Physical Activity and Health, 2020). Research in a number of countries points to an association between increased AT and lower BMI or obesity rates (Bassett et al., 2008; Dons et al., 2018; Flint et al., 2014). Individual benefits of AT for adolescents also include increased overall PA activity and physical fitness (Henriques-Neto et al., 2020; Ikeda et al., 2022; Larouche et al., 2014; Stewart et al., 2017). At the community level, increased AT can support urban health and sustainability as well as social connections (Brand et al., 2021; Giles-Corti et al., 2016; OECD, 2017). Shift from motorized transport to AT supports policy efforts worldwide on behalf of the 2030 Sustainable Development Goals (SDGs) (World Health Organization, 2018).
Research on adolescent AT has primarily focused on active school travel (AST). In an analysis of child and adolescent AT across 47 countries (of which 87% percent reported only AST) the average prevalence was 47% to 53% (González et al., 2020). Previous research in Israel found that 61.9% of adolescents reported regular use of AST; of which 39.3% reported 20 min or more of daily AST (Levi et al., 2022). Many countries report a significant decline in child and adolescent AST over the last decades (Ikeda et al., 2018).
A number of psychosocial factors are related to higher rates of PA and AT. Parent and peer behaviors and support have been found to be related to PA participation among adolescents; of note is the effect of friends and social networks in promoting higher levels of PA participation (Li & Moosbrugger, 2021; Martins et al., 2014; Rhodes et al., 2020; Sallis et al., 2000). Perceptions related to social support from peers and parents were also associated with higher rates of AT among adolescents (Ikeda et al., 2018; Wang et al., 2017). Similarly, adolescents that view AT in context with social interactions, in particular with peers, report increased AT mobility (Panter et al., 2008). Traveling with friends was reported as a factor to increase AST, following implementation of several initiatives within the framework of an intervention program (Hinckson, 2016).
Adolescent Use of Social Media and Technology
During adolescence, a critical stage of identity development, there is a strong influence of sociocultural factors on identity formation; development of a positive identity and a coherent sense of self in relation to the world during adolescence contributes to continued positive development and life experience (Erikson, 1968). Social identity theory recognizes that adolescent identity development occurs in context with the social groups to which they belong; individuals define their own identities with regard to their social groups, and these identifications work to protect and bolster self-identity (Tajfel et al., 1979). Adoption of similar behaviors and interests serves as the basis to enhance social identification within the group. Social identification leads to positive views of an in-group and a desire to be recognized as part of the chosen group (Reynolds et al., 2000). Social media participation has been identified as a means for supporting community formation and increased belongingness among young adolescents as well as affording opportunities for identity development (Allen et al., 2014; Quinn & Oldmeadow, 2013).
Adolescents are actively engaged in social media, technology, and screen use. George and Odgers emphasize that it is not a question of whether adolescents are using these mediums, but rather “how, why and with what effects” (George & Odgers, 2016). In the U.S. most adolescents have access to digital and technology devices, daily internet use is as high as 97%, and 46% of teens say they are online almost constantly (Vogels et al., 2022). Similar findings are reported in Israel; smartphone use is common by age 10, and more than 90% of adolescents report that they are engaged in a variety of social media platforms (SMP); most popular include Instagram, WhatsApp, YouTube and TikTok (Bezeq, 2022).
Research on the association between adolescent use of social media and technology and their health and wellbeing varies with findings that point to positive, neutral, and negative consequences of these behaviors. Peer interactions and relationships are necessary for healthy adolescent development; as adolescent engagement with SMP has increased, research has shown that adolescent friendships within SMP exhibit similar characteristics to offline relationships with peers (Yau & Reich, 2018). There is also evidence that points to the benefits of digital technology for social relationships (Kardefelt-Winther, 2017; Stoilova et al., 2021). Furthermore, a meta-analyses review of cohort and longitudinal studies pointed to a lack of evidence for strong connections between time spent on technology and SMP and poor mental health (Odgers & Jensen, 2020). A systematic review of literature reviews points to an association between higher levels of screentime with poor health measures and outcomes, including adiposity, unhealthy diet, depression, and poor quality of life. However, the authors point to moderate or low quality of some of the studies; limited data on mobile screen use; and insufficient attention to the types of content accessed or context of behaviors (Stiglic & Viner, 2019).
In view of the common use of SMP and technology among children and adolescents, a recent review of digital technology interventions to promote health in these age groups, points to positive potential for digital platforms to promote healthy nutrition and reduced sedentary behaviors (Oh et al., 2022). There is also evidence that adolescents utilize their SMP to access health-related information; in an online survey with adolescents at 10 schools in the UK, 53% reported that they actively look for health-related material and 46% reported that they had changed their behavior because of information they had seen on SMP (Goodyear et al., 2019).
Engagement in AT and PA are important contributors to adolescent development, health, and wellbeing; however, rates of these behaviors are low. Simultaneously, social media, technology and screen use are extremely prevalent, and previous research has demonstrated both positive and negative aspects of these behaviors related to adolescent health. Given that adolescents are actively engaged in SMP for various aspects of their day-to-day life, it is likely that these media could be used to promote AT and PA. Meanwhile, peer engagement during AT and PA may offer a unique space for peer interactions and simultaneously serve as an impetus for engagement in these healthy behaviors.
These facets of individual and peer behaviors may be considered within the different levels of influence recognized in the social ecological model, which serves as a theory-based framework for understanding the multifaceted social influences and interconnected environmental dynamics that both shape individuals and determine behaviors (Sallis et al., 2015). The social ecological approach assumes that health promotion and change in health behavior, including PA and AT behaviors, is dependent on a multilevel approach that targets interpersonal, organizational, community, and public policy, as these are all different factors that may either support and maintain healthy behaviors or stimulate positive change in individual and societal public health (Giles-Corti et al., 2016; McLeroy et al., 1988; Sallis et al., 2015). The context of social media is recognized as having a direct influence on health behaviors forming part of the adolescent daily psychosocial experience; peer interactions and SMP also influence behaviors at the interpersonal and community levels (McHale et al., 2009; Vaterlaus et al., 2015). A multi-level ecological approach to evaluate and inform efforts to promote healthy adolescent behaviors, including individual characteristics and behaviors and interaction with peers and SMP may provide a comprehensive framework for understanding multiple and interacting determinants of AT and PA health behaviors.
Therefore, the aim of the current research was to explore the relationship between peer engagement and SMP to adolescent AT and PA utilizing a mixed method design to allow for stronger overall analysis and interpretation. We hypothesized that positive norms, attitudes, and habits are associated with higher rates of adolescent AT and PA; higher screen use is associated with lower rates of adolescent AT and PA behaviors; and exposure to AT and PA on SMP affect AT and PA behaviors.
Method
Study Design
We employed a mixed methods study, based on an exploratory sequential design that included integration of the qualitative and quantitative phases of the study (Figure 1). Phase 1 was based on in-depth semi-structured interviews with adolescent-parent dyads; while Phase 2 entailed a cross-sectional survey. The two phases of the study did not overlap.
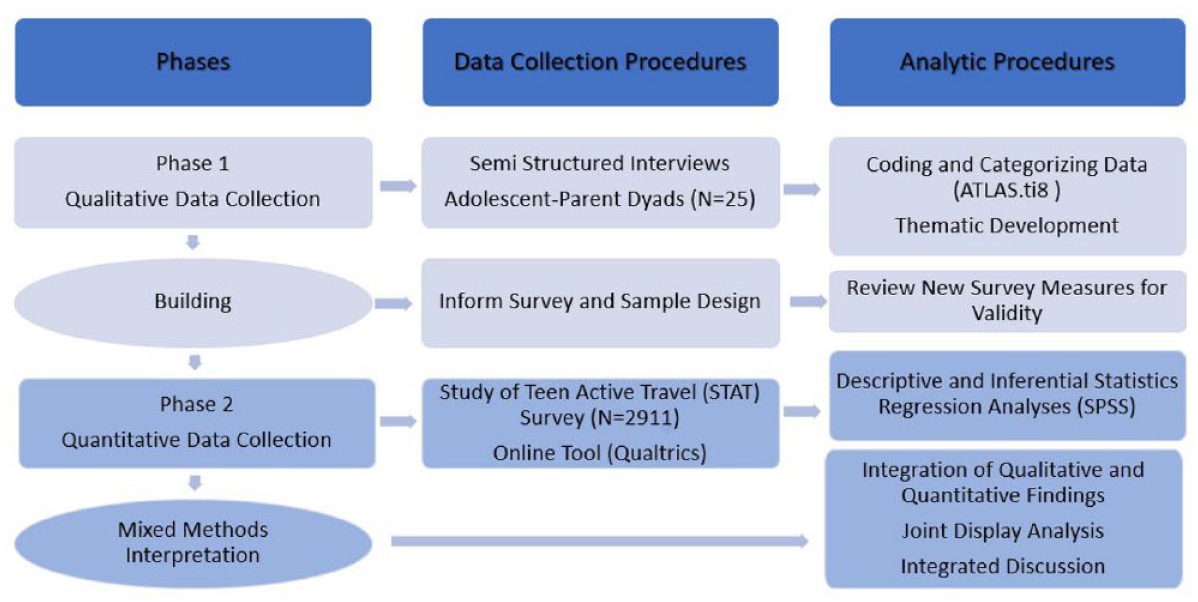
Exploratory sequential design process.
The methods of data collection and analysis were linked, based on the building approach; results from Phase 1 informed Phase 2. Specifically, several qualitative themes, codes, and categories we explored in Phase 1 served as the basis for the development of quantitative items and variables that were then included in data collection instrument, Study of Teen Active Travel (STAT) used in Phase 2. The qualitative data collection offered more detailed description of the adolescent experience, while quantitative data collection then allowed for more general and representative findings across the target population (Harrison et al., 2020). Integration of the qualitative and quantitative data analysis is based on weaving narrative, joint display, and an integrated discussion.
Phase 1 and Phase 2 of the study were approved by the University Ethics Committee —Institutional Review Board governing the use of Human Participants in Research (No. 087/20); Phase 2 was also approved by the Ministry of Education, Office of Chief Scientist (No. 11594).
Phase 1 Qualitative Interviews with Adolescent-Parent Dyads
We conducted semi-structured Zoom interviews with 25 adolescent-parent dyads in communities across Israel during early stages of the COVID-19 pandemic, March-June 2020. Detailed methods have been described previously (Levi & Baron-Epel, 2022).
Sampling and Recruitment
Purposive sampling was conducted to identify a variety of Hebrew-speaking households, with both an adolescent age 13 up to 17 years and parent in residence. A prepared recruitment message for participation in interviews on adolescent travel behavior was sent via WhatsApp. Potential participants were informed about the research purpose and letters of consent were sent in advance to both the parent and adolescent.
Interviews
A semi-structured interview format was used for both the adolescent and parent, with open-ended questions to elicit information on factors that encourage or prevent use of AT modes; probing questions further investigate effects of family, peers, social norms, and environment (Levi & Baron-Epel, 2022). As the study progressed, analysis of interviews identified additional topics for integration in the guide, to obtain wider and significant information in subsequent interviews, and to attempt to ensure theoretical saturation of the topic (Hennink et al., 2017).
Qualitative Analysis
The analysis was based on both a deductive approach based on categories in the interview guide and an inductive approach developing new categories and themes throughout the analysis process (Gioia et al., 2013). A review of all interview scripts served as the basis for a preliminary structure of codes and categories. This was followed by axial coding to identify relationships and patterns, and for theme development. A reflexive thematic analysis process was used, with multiple returns to the data set and detailed review, analysis and development of the themes (Braun & Clarke, 2021). Qualitative analysis was conducted using ATLAS.ti8 software.
Credibility of the data was established via data triangulation by conducting interviews with both adolescents and parents as well as investigator triangulation utilizing a two-person research team for coding and analysis (Korstjens & Moser, 2018). To facilitate transferability and strengthen dependability, the research process, the participants, analysis and the results have been described in detail in the current manuscript and previously (Levi & Baron-Epel, 2022). Finally, a reflective approach including recording insights immediately, utilizing a structured coding scheme, and following up with multiple returns to the dataset was utilized to enhance confirmability.
Integration of Data Collection Method
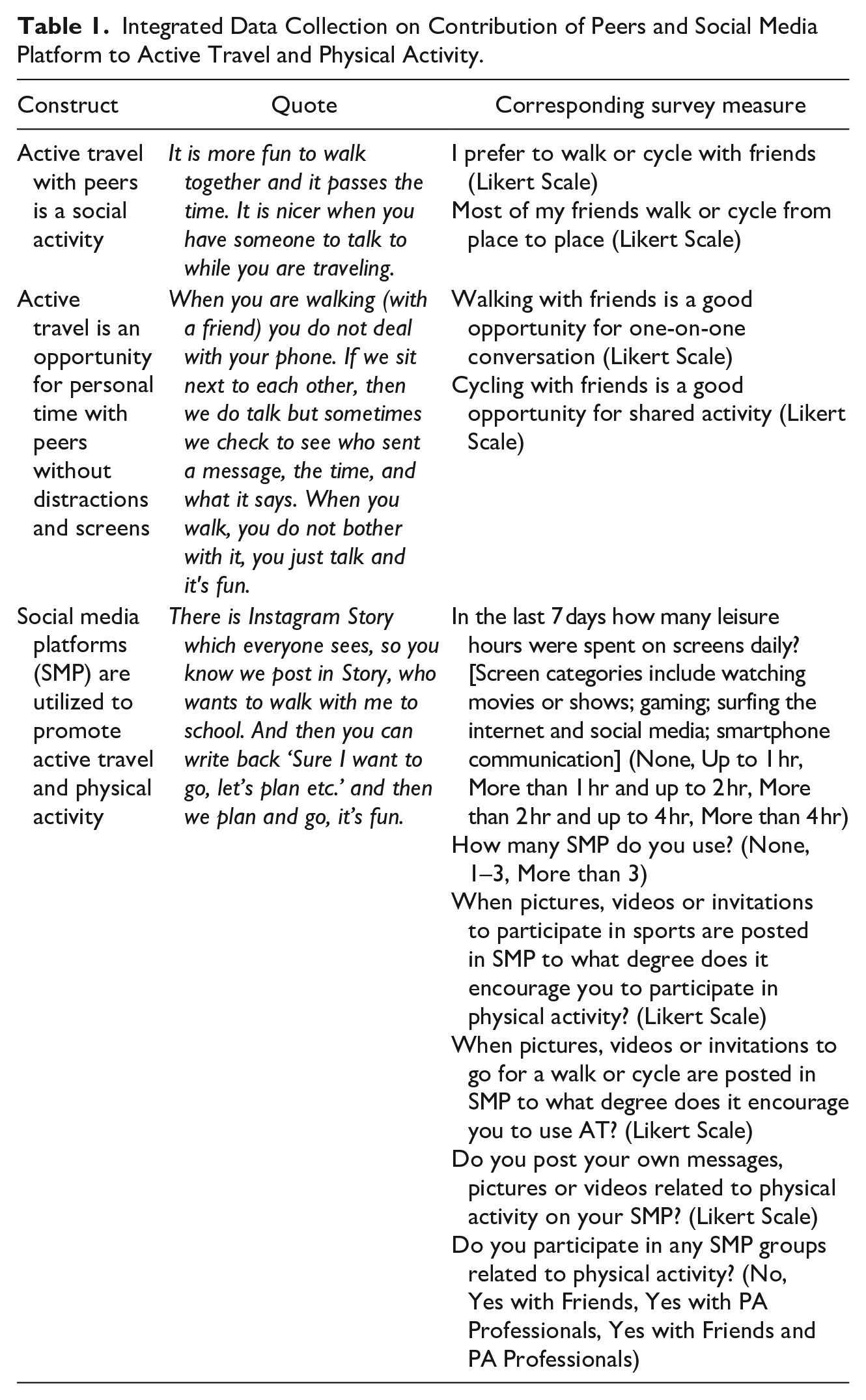
The data collection methods were linked based on the building approach; analysis of the in-depth interviews with adolescents and parents revealed several themes, categories, and codes that informed development of the quantitative data collection approach. An important theme that influenced the building of the quantitative data collection instrument relates to the contribution of peers and social media platforms (SMP) to adolescent AT and PA. These include a number of key constructs: AT with peers is a social activity; AT and PA are an opportunity for personal time with peers without distractions and screens; SMP are utilized to promote AT and PA. Several innovative questions related to the impact of peers and social media on AT and PA were introduced based on these findings (see Table 1).
Integrated Data Collection on Contribution of Peers and Social Media Platform to Active Travel and Physical Activity.
Phase 2 Study of Teen Active Travel
In the second phase of the study, we conducted a cross-sectional survey at secondary education schools across Israel during more advanced stages of the COVID-19 pandemic. The Study of Teen Active Travel (STAT) survey focused on motivations for active travel among adolescents that were not previously explored in Israel including both active school travel (AST) and active leisure travel (ALT).
Instrument Development
The STAT survey is a self-completed, anonymous questionnaire on active travel, physical activity, and sedentary behavior. Results from the qualitative data collection phase informed the development of the STAT survey instrument. Selected sections of the survey are based on previous applicable data collection tools, based on themes explored in the qualitative study. These questions include measures of attitudes, social norms, and perceived behavioral control based on the Theory of Planned Behavior (TPB) model, self-reported behaviors of AT, PA and screen use, and perceptions regarding the environment (Bird et al., 2018; Harel-Fisch et al., 2020; Saint-Maurice et al., 2017).
A subset of the questions, including the addition of a measure of AT as an opportunity for peer-to-peer communication and questions on exposure to and promotion of PA and AT on SMP, was developed building on innovative findings from Phase 1, as detailed in the section on Mixed Methods Integration. The new survey questions were developed by the research team following a review of related literature and in consultation with subject matter experts to verify content validity. The survey measurements were then evaluated to understand how respondents interpret the survey and understand the meaning of the survey questions. We conducted cognitive testing of the entire survey with a focus on the new measurements with two adolescents via Zoom, followed by a pre-test of the digital survey with five additional adolescents, prior to finalizing the survey measurements. In an analysis of reliability, we found that the subscale for attitudes including addition of peer-to-peer communication consisted of 13 items (α = .78) while the subscale on exposure to and promotion of PA and AT on SMP consisted of 3 items (α = .66).
Sampling and Recruitment
Schools served as the primary sampling unit. In order to ensure a representative sample of the Hebrew speaking population of adolescents across the country, schools were randomly selected from the Israel Ministry of Education list of all schools in the general Jewish population. Based on population density data from the Central Bureau of Statistics and categories defined by the OECD, the primary sampling units were stratified, based on urbanicity: (1) high >5,000 pop/km2; (2) medium 5,000 to 2,000 pop/km2; (3) low <2,000 pop/km2. Schools were distributed around the country by geographic region and the probability of selection was proportional to the population size of the schools in each region. For each sample school, two classrooms were randomly sampled in grades 7 to 11. All students who were present in sampled classrooms were included. Sample weights were calculated. The final sample included for analysis was 2,911 students 13 to 17 years old in 16 schools.
Data Collection
Following initial consent from the school principal, a letter was sent to both the parents and the adolescents in selected homerooms a week before the survey, to provide information and request consent. Parents and students were notified prior to the scheduled data collection that they could refuse to participate, and it would not have any negative ramifications. Students were informed again orally on the survey day and in writing at the start of the survey that they are not required to participate and may stop at any time.
The STAT survey was programmed on Qualtrics software to allow for electronic data collection via cellphone or computers in the classroom. On-site visits on data collection days were conducted by the research team at 14 schools, while 2 schools opted to conduct data collection independently utilizing the link and written instructions. The data collection period was October 2021-March 2022, with interruptions for short periods due to acute waves of the COVID-19 pandemic.
Key Variables
Quantitative analysis of survey data to investigate the key constructs related to the association of peers and SMP with AT and PA included the following variables:
Dependent Variables
Active travel and physical activity are the dependent variables of interest in the study. Active travel is based on measures of active school travel (AST) and active leisure travel (ALT), as well as a cumulative measure for all active travel (AAT). Physical activity (PA) is based on two key measures, days of recommended physical activity (DRPA) and leisure time physical activity (LTPA).
Active School Travel (AST)
The measure is based on the Health Behavior of School Age Children Study (HBSC) in Israel (Harel-Fisch et al., 2020; Inchley et al., 2018) questions “In the last 7 days how many days did you walk/cycle/e-cycle to school?” and “In the last 7 days how many days did you walk/ cycle /e-cycle from school?”. We asked for each mode separately and created a cumulative variable for AST.
Active Leisure Travel (ALT)
The measure is based on the questions “In the last 7 days how many days did you walk/cycle/e-cycle at least 10 min—for example to a friend, afternoon activity, or shopping?” (Saint-Maurice et al., 2017). We asked for each mode separately and created a cumulative variable for ALT.
All Active Travel (AAT)
We created a composite measure the different purposes of AT that includes AST and ALT.
Days of Recommended Physical Activity (DRPA)
The measure is based on the international physical activity questionnaire (IPAQ) used in HBSC (Inchley et al., 2018; Tesler et al., 2019). This measure corresponds with the WHO recommendation of an average of 60 min a day of moderate-vigorous intensity PA (MVPA) for children and youth: ‘In the last 7 days how many days did you participate in 60 min of cumulative moderate to vigorous physical activity?’
Leisure Time Physical Activity (LTPA)
We included a LTPA measure based on the Godin Leisure-Time Exercise Questionnaire (Zelener & Schneider, 2016). This measure records LTPA habits, via self-report of weekly frequencies of different levels of activities, as follows: “During a typical 7-Day period (a week), how many times on the average do you do the following kinds of exercise for more than 15 min during your free time”; with separate lines for strenuous, moderate, and light activities. The LTPA score is calculated into three categories active, moderately active, and insufficiently active or sedentary.
Independent Variables
The predictor variables of interest are the survey measures, related to the effects of peers, screen time and SMP on AT and PA, that were developed based on the qualitative study (see Table 1). These include rates of AT and PA behaviors with peers, peer norms, screen and SMP use, effects of SMP on AT and PA participation, and active SMP participation related to PA.
Covariates
Possible confounders that affect rates of AT and PA have been documented in previous literature on these health behaviors (Bauman et al., 2012; Giles-Corti & Donovan, 2003; Ikeda et al., 2018). Confounders included in this analysis are gender, grade, self-reported health, adiposity (using BMI category), socioeconomic level (based on urban Census data), vehicle ownership, and level of urbanicity.
Quantitative Analysis
To ensure a high-quality dataset for analysis, data-cleaning efforts identified questionnaires with high rates of missing information; N = 793 did not complete any or most of the survey. In addition, N = 93 were identified as anomalous data or incorrectly filled questionnaires. The final sample for analysis N = 2911 adolescents (76.7% response rate). Descriptive analyses were performed as the first step. Correlation analyses using Spearman’s test were conducted to examine associations between variables and comparisons of key variables between groups. This was followed by linear regressions which were generated by SPSS complex sample procedures (CSGLM), which take into account that the data are from a stratified cluster sample. The linear regression analyses were conducted to investigate the important predictors that are associated with the key analysis variables (e.g., AT and PA behaviors). We used a backward regression technique to eliminate non-significant predictor variables. The analyses used SPSS version 27.0 (IBM SPSS Statistics). Statistical significance was set at 0.05 unless otherwise indicated; the significance testing took into account that this is a stratified cluster sample with varying case weights.
Mixed Methods Integration
Integration took place at several key stages: design, methods, analysis and interpretation (Fetters et al., 2013). As introduced in the study design description, we utilized an exploratory sequential design process in which the findings from the qualitative phase helped to develop the quantitative phase of the study.
Integration of Analysis
Data from the qualitative and quantitative phases of the study were initially analyzed separately. This was followed by narrative weaving to integrate results from the two phases of the study for each of the key constructs related to the association between adolescent AT and PA to activities with peers and SMP (Fetters et al., 2013). In the analysis procedure we assess the fit of the data integration; is there confirmation/ convergence, expansion, or discordance between the datasets (Bazeley, 2015; Creswell, 2015; Fetters et al., 2013). Confirmation occurs in cases where results from Phases 1 and 2 converged, the findings confirm the results of the other; expansion was determined when the results address different aspects of the same finding or expand insights but are not fully complementary; and discordance points to results in the different phases that are in contradiction (Fetters et al., 2013). The findings are presented in joint displays that highlight the contribution of the integrative approach to meta-inferences based on the interpretation of both datasets (Guetterman et al., 2021).
Results
Participants in both phases of the study include adolescents 13 to 17 years old from communities across the country (see Table 2). The qualitative phase had a higher percentage of females, older teens, participants from cities, and members of households with reported income above average. The quantitative phase had a more even distribution of male and female participants and levels of urbanicity; however, there were a higher percent of younger adolescents and adolescents who reported average or above average household income. Reports of PA are similar in both phases, however reports for AT are higher in the quantitative phase. Constructs related to the association of peers, screens and SMP with adolescent AT and PA are presented; quantitative results are integrated in the discussion of each of the associated concepts.
Characteristics of Adolescent Participants in Phase 1 and Phase 2.
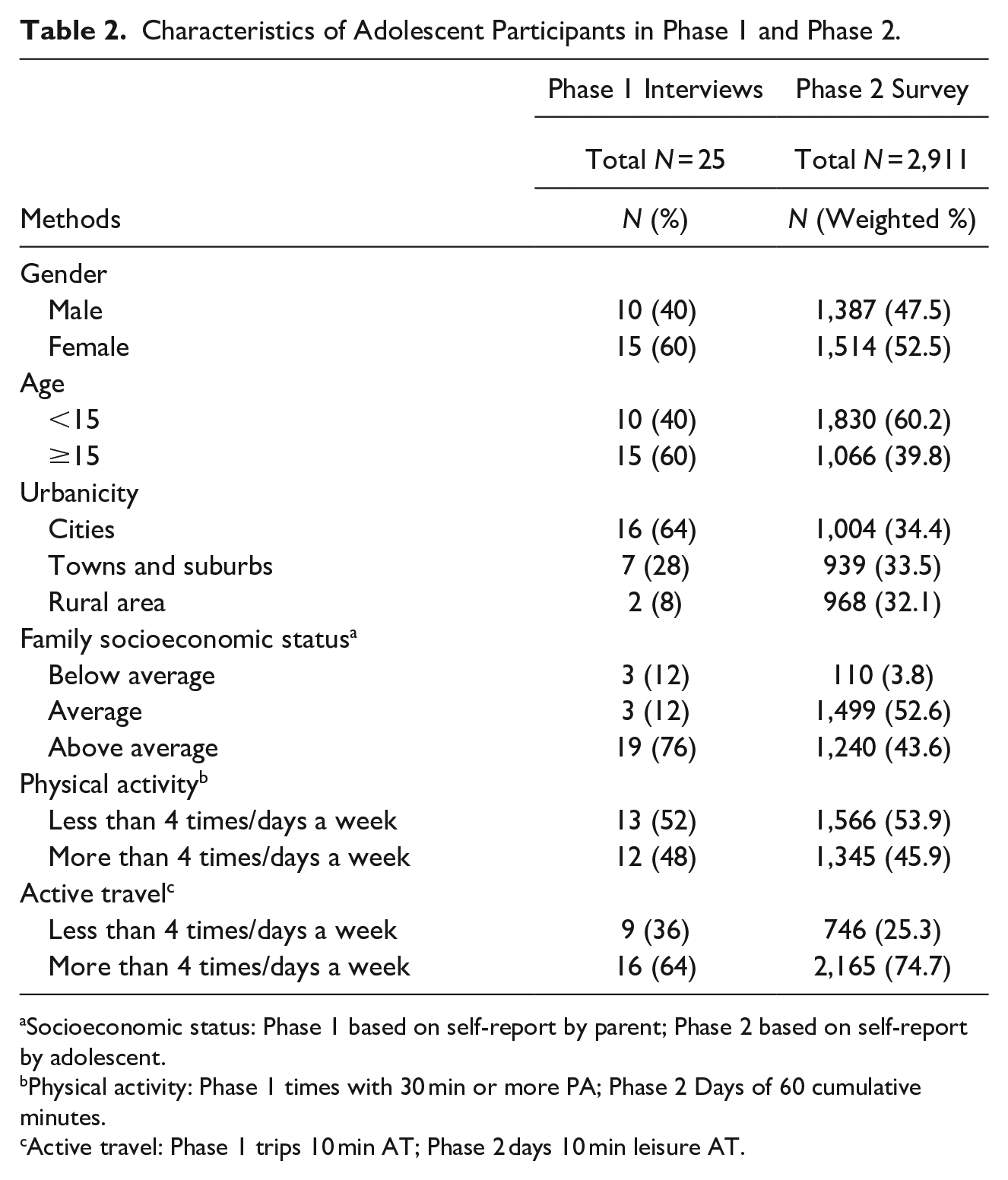
Socioeconomic status: Phase 1 based on self-report by parent; Phase 2 based on self-report by adolescent.
Physical activity: Phase 1 times with 30 min or more PA; Phase 2 Days of 60 cumulative minutes.
Active travel: Phase 1 trips 10 min AT; Phase 2 days 10 min leisure AT.
Active Travel with Peers is a Social Activity
Adolescents point to AT and PA as a social activity with their peers (N = 22). Moreover, time with peers is a facilitator for these health behaviors; as one adolescent indicated “With friends I don’t have trouble walking anywhere!” Adolescents indicated that a trip with peers tends to feel like it is of shorter duration, for example one adolescent shared, “We usually connect transport to a destination, but when you walk with friends it is different. It is not about a particular destination it can also be a trip without a particular goal or purpose.” Use of AT with peers was also voiced as a solution to safety issues such as trips at night (N = 9), “I will only walk if I have someone to walk with. For example, I have a friend who lives relatively close, so if we are out until late then we will walk together.”
It is also interesting to note that some adolescents (N = 5) indicated that while not all their friends are interested in sports, AT together is viewed positively, “Not everyone likes to play soccer, but they definitely don’t have a problem going for a walk, and talking with friends while walking. . .. Even if it’s just to walk to the park a few minutes from home to spend time together with a friend, you don't have to like sports for that.” Most of the adolescents indicated that walking is a frequent activity (N = 24). Several mentioned that cycling is less common, in particular among the adolescent girls (N = 8).
The results of the quantitative data collection confirmed these findings. Most adolescents indicate that they agree or strongly agree that they prefer to walk with friends (81%, see Table 3) while more than half prefer to cycle with friends (56%). Using Spearman’s test, we found a statistically significant correlation between ALT walking and preference for walking with friends (r = .129, p < .001); likewise for ALT cycling and preference for cycling with friends (r = .251, p < .001).
Joint Display: Active Travel With Peers is a Social Activity, Walking..
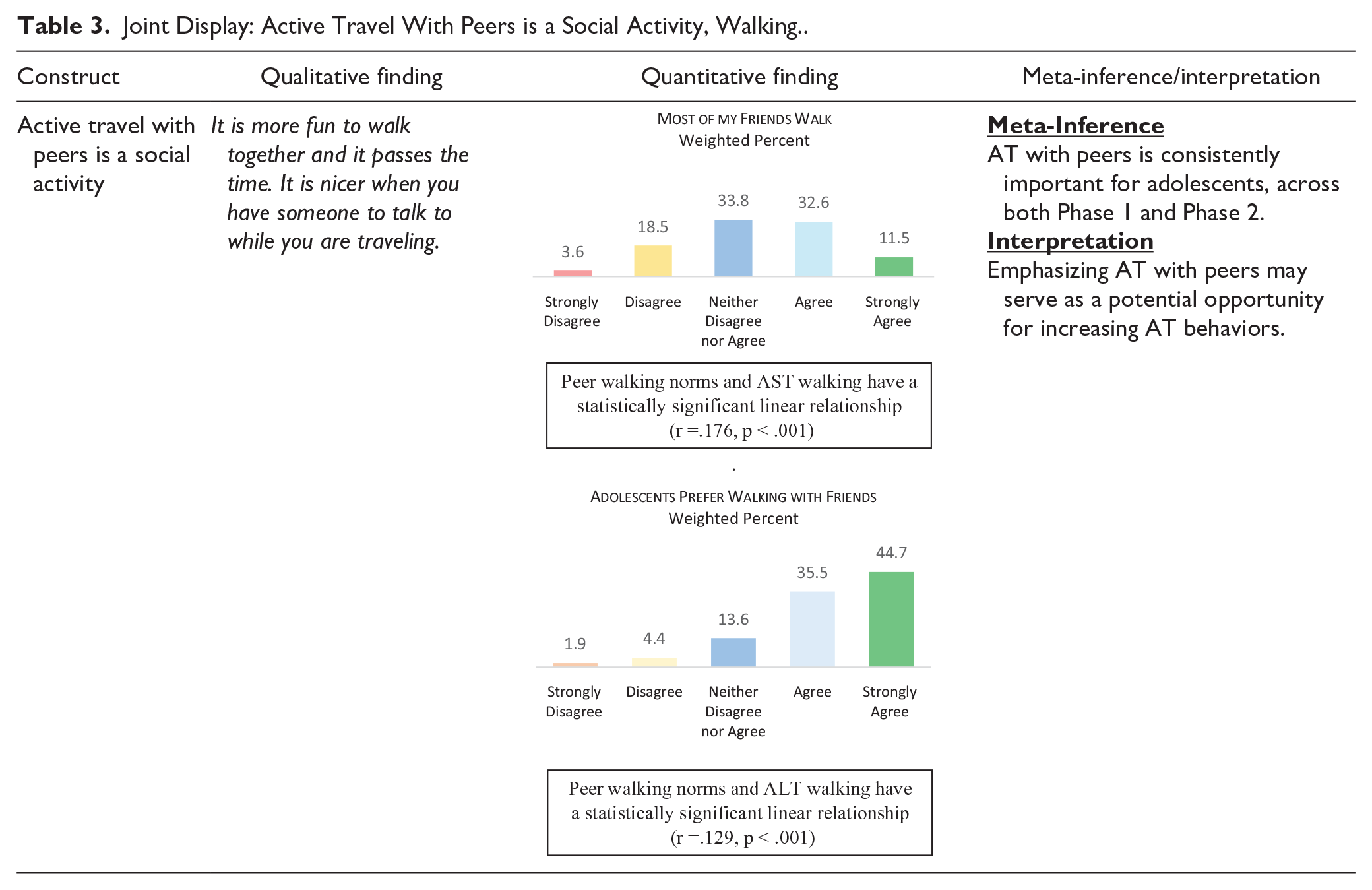
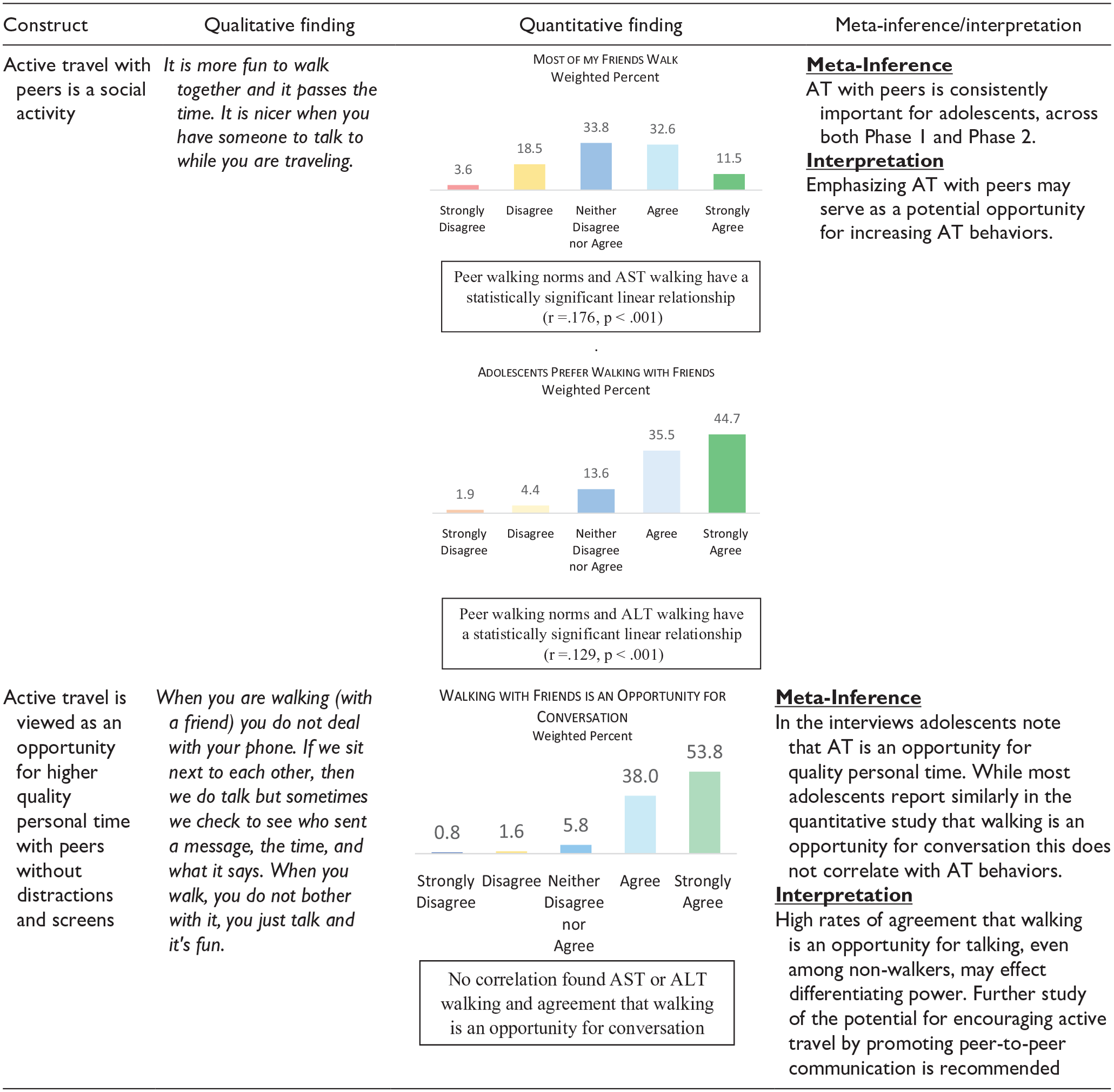
Fewer adolescents report that most of their friends walk or cycle (44.1% and 19.2%, respectively). Nevertheless, peer walking norms and AST walking have a statistically significant correlation (r = .176, p < .001). Similarly, we found a positive correlation between adolescents who indicated that most friends cycle and both AST cycling (r = .206, p < .001) and ALT cycling (r = .326, p < .001).
Active Travel and Physical Activity are an Opportunity for Personal Time with Peers without Distractions and Screens
Adolescents spoke about a high level of screen time and social media use among their peer group (N = 5); this assertion was confirmed in the quantitative study. In a detailed question on screen time, based on multiple screen types, we found that 64.1% were heavy screen users reporting at least 4 hr of cumulative screen time, 33.4% reported 2 to 4 hr of daily use, and only 2.5% reported 2 hr or less of daily use. We found that there are negative correlations between screen time and several AT and PA measures, including AAT cycling (r = −.200, p < .001); DRPA (r = −.187, p < .001) and LTPA (r = −.164, p < .001). Adolescents also reported high rates of SMP engagement: 54.8% use more than three SMP, 42.6% use one to three SMP and only 2.5% do not use SMP.
In light of these findings, it is interesting to note that several adolescents described AT and PA as an opportunity for higher quality personal time, without distractions (N = 7). As one adolescent shared, “We are a screen generation, we don’t like to go out as much. Friends are more likely to visit at home. I recommend that everyone go out especially in cool weather, it is more fun and healthier. Walking is a good time to talk, it is more fun to talk while you are walking. My friends and I often will take a walk around the school campus, because it is fun to talk [while walking].” In fact, promotion of AT and PA with peers was highlighted as a method to increase these healthy behaviors.
In Phase 1 the importance of the peer group was also highlighted in relation to adolescent AT and PA during the COVID-19 pandemic (N = 8). This type of activity was viewed as an outlet for peer-to-peer activity and communication. One adolescent shared, “I'm a lazy person. I really have no energy. But yes, during the Corona it seems to have grown on me, I take an hour and set up with a friend [for AT or PA]. So, it turns out that every day I made an appointment with a friend and we do [AT or PA] together.”
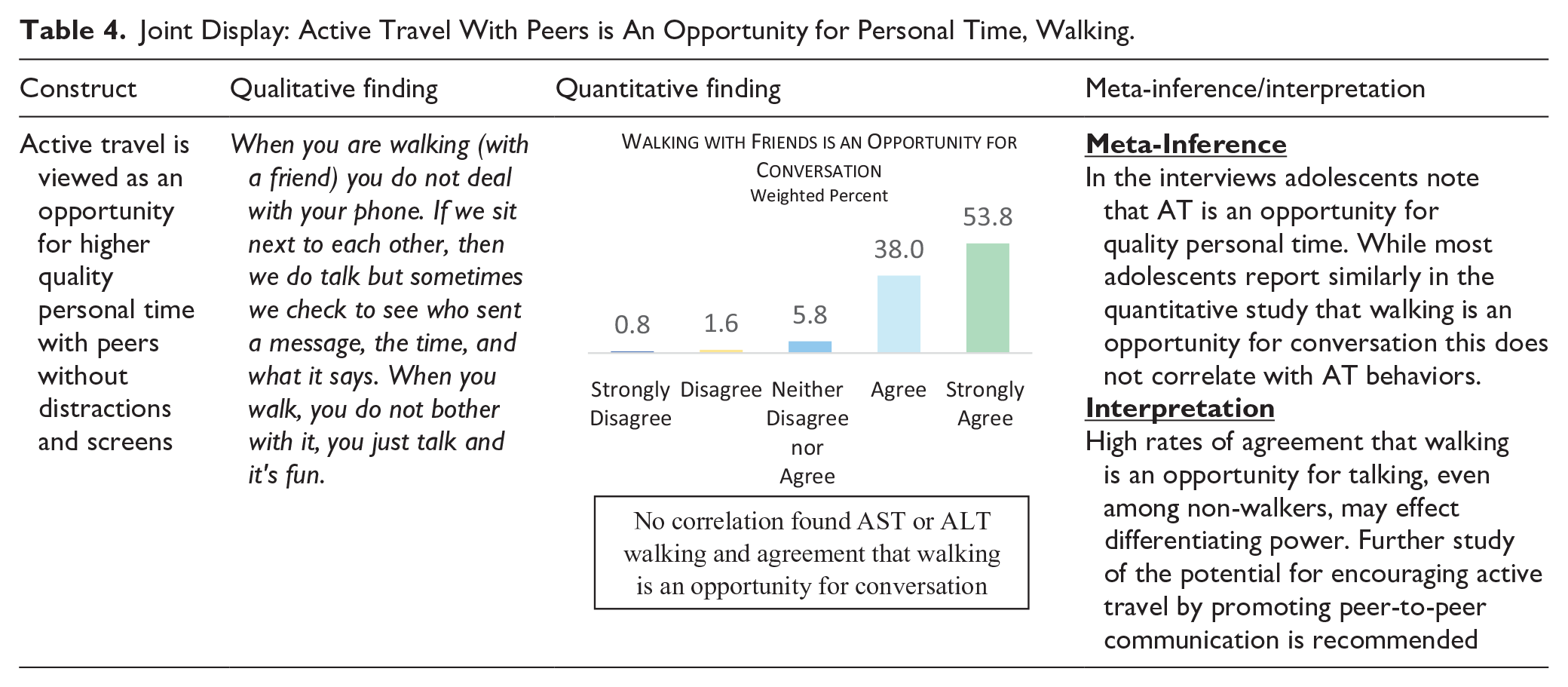
In Phase 2, we targeted the relationship between AT and peer-to-peer communication. Findings diverged to some extent. Most adolescents agree or strongly agree that walking with friends as an opportunity for one-on-one conversation (91.8%, see Table 4); however, there was no positive correlation between AST or ALT walking and agreement that walking is an opportunity for conversation. For cycling, fewer adolescents reported cycling as an opportunity for shared activity (44.1%); nevertheless, there were statistically significant correlations between adolescents who indicated that cycling is an opportunity for shared activity with AST cycling (r = .089, p < .05) and with ALT cycling (r = .177, p < .000).
Joint Display: Active Travel With Peers is An Opportunity for Personal Time, Walking.
Social Media Platforms are Utilized to Promote Active Travel and Physical Activity
Several adolescents spoke to dependence on screens and SMP among their peers. Conversely, many adolescents pointed to their SMP as a method to promote AT and PA (N = 10). They provided a variety of examples related to sharing messages on AT and PA. One participant described group discussions on SMP to encourage use of AT, “Yes, we plan to meet, and if someone doesn’t have a way to get there, we write in the [WhatsApp] group, ‘Just get up and walk.’ It’s not so far that you can’t walk there, so we walk.” Adolescents’ use of SMP to increase AT and PA was also promoted, due to the common use of the platforms and in light of the fact that adolescents indicate that they are inclined to accept invitations from a peer to use AT or do PA together. One adolescent shared, “I have friends who plan to do sports together [via SMP].”
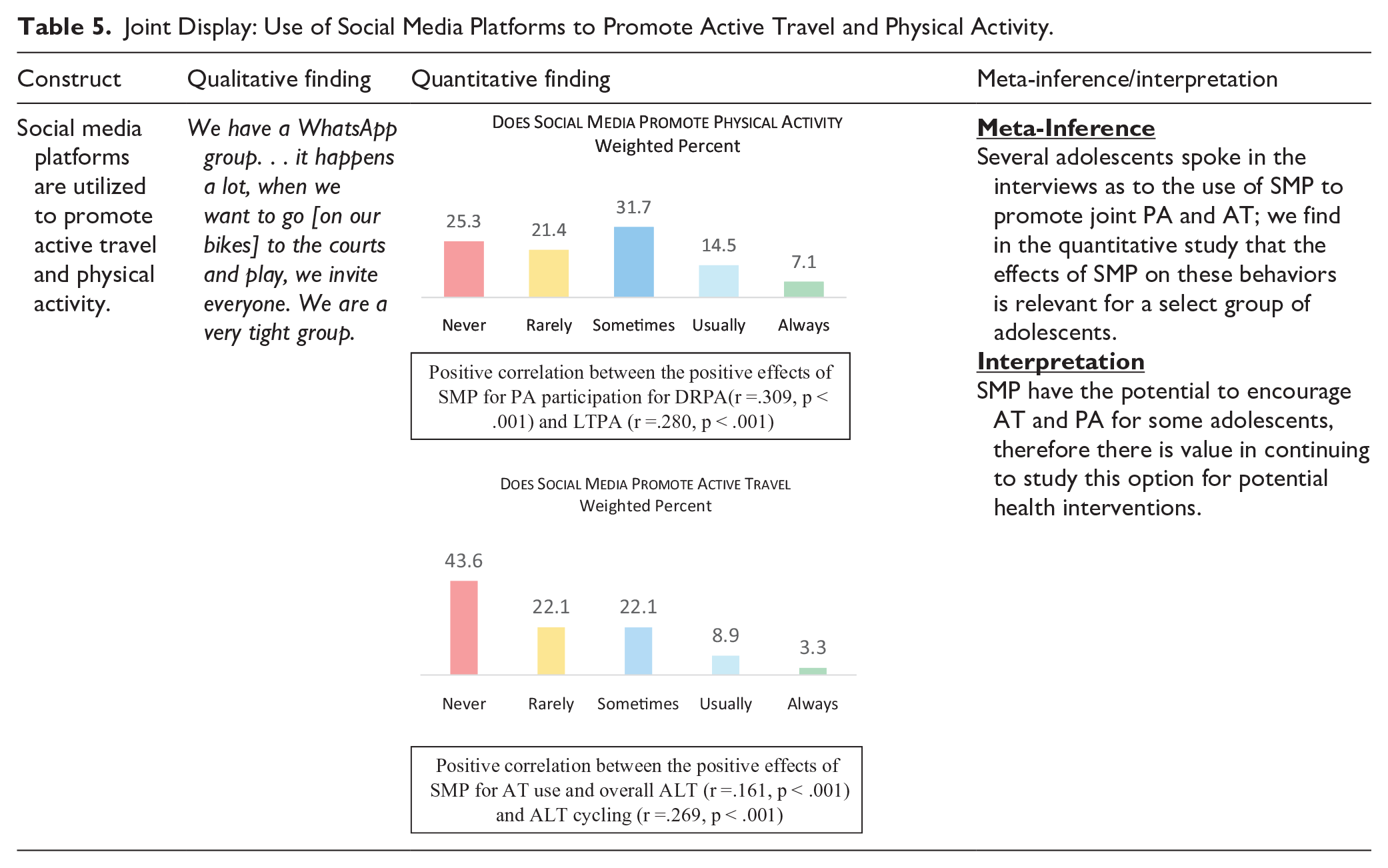
The findings in Phase 2 are mostly consistent with Phase 1. Related to the effects of social media on PA participation, we found that 21.5% of adolescents indicated that pictures, videos or invitations to participate in PA usually or always encourage them to participate in PA (see Table 5). We found a positive correlation between the positive effects of SMP for PA participation and PA measures, including DRPA and LTPA (r = .309, p < .001 and r = .280, p < .001, respectively). Similarly, we found positive correlations between other pairs of related measures, such as: (1) participation in PA groups with SMP and DRPA (r = .321, p < .001); and (2) sharing invitations/messaging about PA with SMP and DRPA (r = .238, p < .001). We included a similar question on AT; here, only 12.2% of adolescents reported that the SMP encourage them to use AT. Nevertheless, there was a positive correlation between reporting that SMP encouraged AT and actual overall ALT (r = .161, p < .001) as well as, specifically, ALT cycling (r = .269, p < .001).
Joint Display: Use of Social Media Platforms to Promote Active Travel and Physical Activity.
Relationship of Different Peer and Social Media Constructs to Adolescent Active Travel and Physical Activity
We conducted backwards linear regression analyses to further analyze the relationship between peer related activities and SMP to key adolescent AT and PA measures and interpret the findings in light of both phases of the study (see Table 6). We included the variables related to joint AT with peers, screen use, and measures related to SMP use to promote AT and PA. In addition, we controlled for the different covariates. Finally, we included the AAT measures in the regression analyses of DRPA and LTPA. As stated above, the significance testing took into account that this is a stratified cluster sample with varying case weights.
Backwards Linear Regression Models for Active Travel and Physical Activity Variables.
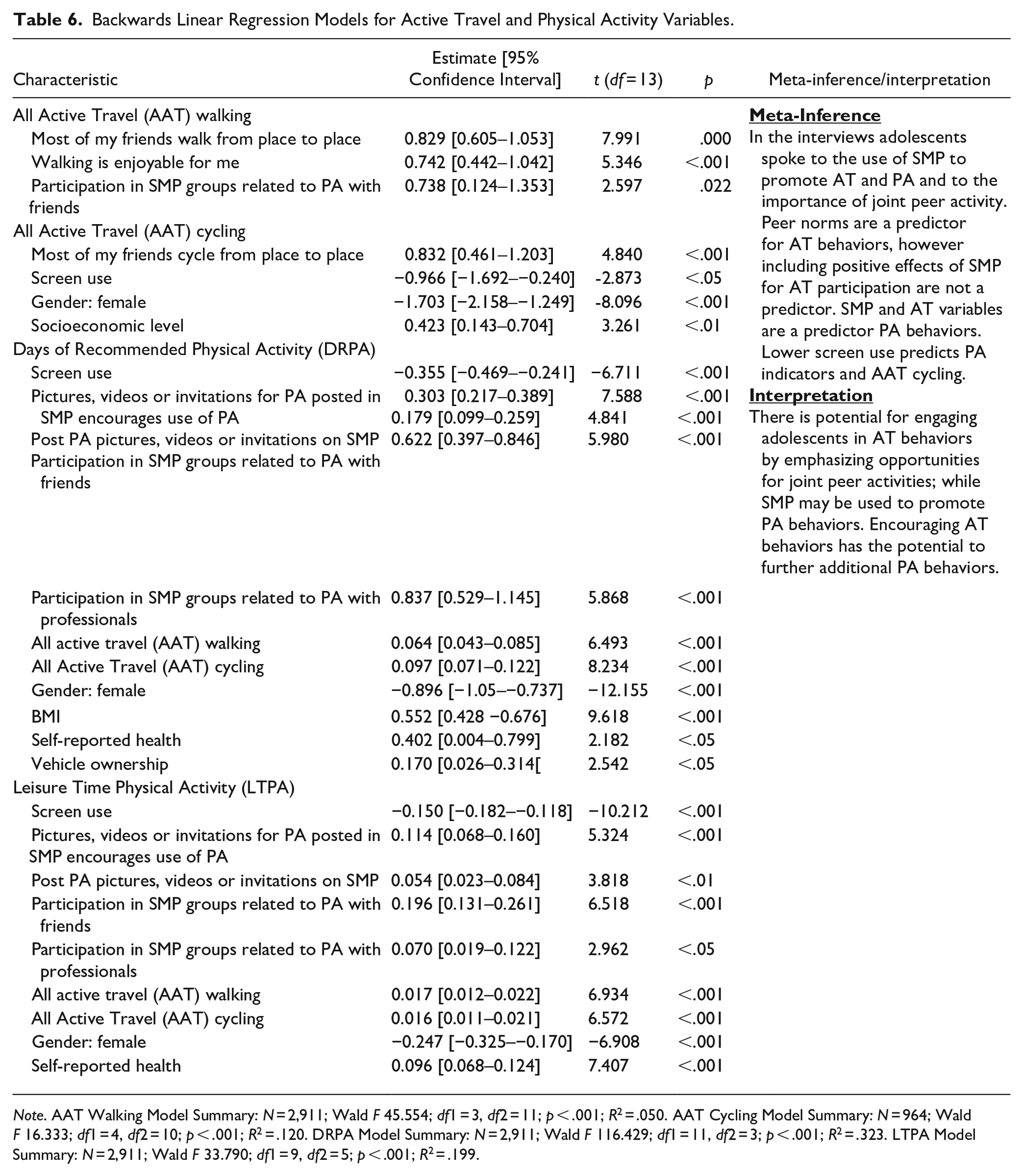
Note. AAT Walking Model Summary: N = 2,911; Wald F 45.554; df1 = 3, df2 = 11; p < .001; R2 = .050. AAT Cycling Model Summary: N = 964; Wald F 16.333; df1 = 4, df2 = 10; p < .001; R2 = .120. DRPA Model Summary: N = 2,911; Wald F 116.429; df1 = 11, df2 = 3; p < .001; R2 = .323. LTPA Model Summary: N = 2,911; Wald F 33.790; df1 = 9, df2 = 5; p < .001; R2 = .199.
We find that peer norms are associated with both AAT walking and cycling behaviors. In addition, enjoyment and participation in SMP groups for PA with friends helped to predict high levels of AAT walking. Positive effects of SMP for PA participation, posting of PA messaging on SMP, and participation in SMP groups for PA with friends and professionals were all associated with high levels of PA. Simultaneously, high overall screentime is associated with low levels of AAT cycling and PA. Both walking and cycling AT have a significant positive contribution to DRPA and LTPA. While some covariates (including male gender) are related to AAT cycling, DRPA and LTPA; none have a significant association with AAT walking.
Discussion
Healthy adolescent development and wellbeing are supported by key behaviors including PA and AT. Adolescence is also an opportunity to establish lifelong healthful habits. This mixed-methods study was designed to explore motivations for adolescent AT and PA with a focus on the relationship between peer engagement and use of SMP and these health behaviors.
We find that PA and AT are interrelated, there are positive contributions of both AT walking and cycling to PA behaviors. This is in line with other studies that have found that AT is related to higher rates of PA among children and adolescents (Burns et al., 2019; Henriques-Neto et al., 2020; Larouche et al., 2014; Levi et al., 2022). It is important to note that DRPA and LTPA measures are based on self-report of total time spent active; therefore, adolescents may include AT minutes within their PA measures. At the same time, adolescents indicated that AT is not perceived as PA, and even those who are uninterested in PA may still use AT, consequently there is value in increasing AT behavior across both active and inactive teens.
The findings point to the contribution of peer social support and peer norms to AT; similar to previous research on the contribution of peers to both AT and PA (Ikeda et al., 2018; Martins et al., 2014; Sallis et al., 2000; Wang et al., 2017). The role of peers is emphasized in the qualitative interviews as a motivation for increased utility and enjoyment of AT and the quantitative findings further confirm that peer norms are associated with higher levels of walking. Adolescents also voiced that AT and PA are methods that enable increased peer interaction during the pandemic. This is of interest as COVID-19 lockdowns and restrictions were reported to be associated with reduced PA in many countries (Aubert et al., 2022; Kharel et al., 2022). Adolescent perspectives of these health behaviors as a method to engage with peers may be carried through to social media and intervention programs during routine as well as emergency periods in the future.
We find that the mixed methods approach offered an opportunity for in-depth exploration of the duality of the relationship between SMP and screen use with AT and PA. Research has pointed to the potential contribution of SMP to PA behaviors, although evidence regarding AT is scarcer (Dunn et al., 2021; Goodyear et al., 2019; Günther et al., 2021). In both the qualitative and quantitative phases of this study, we find evidence that SMP has the potential to encourage adolescents to use AT and participate in PA. However, we also find that excessive screen time does not lend itself to an active lifestyle as has been identified in previous research (Stiglic & Viner, 2019). This is in line with findings regarding positive effects of certain types of peer interactions on SMP during the COVID-19 pandemic to promote friendship and shared experiences; similarly, online activities may be utilized to promote healthy active behaviors (Marciano et al., 2022).
The study further introduces the unique contribution of AT and PA as an opportunity for higher quality peer interactions without the distraction of screens. Findings of the quantitative study confirm that most adolescents view AT as an opportunity for quality time with peers, in particular walking. It is possible that the reason we did not find a correlation between AT behaviors and the view that walking is an opportunity for conversation, is that nearly all adolescents agree that walking is an opportunity for talking, even non-walkers. These different findings support the position that there is a degree of complexity related to use of technology, SMP and screen time and their effects on adolescent health and development, for example, the necessity of differentiating between potentially harmful verses beneficial behaviors.
These findings regarding effects of peers and SMP on adolescent health behaviors relate to both individual and social identity development theory. Adolescent identity is influenced by the peer and social context (Erikson, 1968). Shared AT and PA activity and SMP behaviors may contribute to positive self-identity and self-efficacy characterized by healthy lifestyle and well-being (Sets & Burke, 2010). Moreover, participation in social groups that are characterized by healthy behaviors may further bolster positive views of these in-group activities (Reynolds et al., 2000; Tajfel et al., 1979). In accordance with the social ecological model the findings point to sources of influence on adolescent AT and PA behaviors at the individual, interpersonal, and community levels considering personal characteristics, peer norms and interactions and the broader sphere of the SMP environment (Sallis et al., 2015).
Study Strengths and Limitations
The mixed methods study design was selected to allow for in-depth analysis and interpretation of the research question, with each phase contributing to the other. The quantitative phase expands the validity of the qualitative phase and generalizability of key constructs that were identified; while the quantitative phase benefited from the findings in the qualitative phase which enabled the addition of newer concepts related to the effects of SMP and peers on AT and PA behaviors. The study also included a variety of different measures for PA, AT, screen use, and SMP. Of note is the inclusion of adolescent leisure AT behaviors.
The study also had several limitations. The design does not allow for determining causality. The analysis method was tailored to the complex survey sample design; a stratified two-stage cluster design. Further, the data is based on self-report, and therefore, may be susceptible to recall bias. As noted above, the PA measures ask that respondents add up time spent physically active, which may result in misrepresentation of the exact amount of activity and time spent on AT. The study was limited to the Hebrew-speaking population therefore, the findings may not be representative of adolescent experiences across the entire population in Israel. Future research that includes additional cultural and ethnic groups will contribute to the design of applicable interventions for different communities. A future survey tailored to investigate latent constructs that are related to adolescent PA and AT, in particular in line with SMP behaviors, could also be beneficial to better understand influencing factors.
Conclusions and Implications
Emphasis on peer social support, communication of AT social norms, as well as potential of AT and PA to increase peer-to-peer experience may serve as positive messaging to increase adolescent health behaviors. Future research may further explore the role of AT as an opportunity for peer-to-peer communication, as well as quantitative measures of exposure to and promotion of PA and AT in SMP. Development of comprehensive intervention approaches to bolster adolescent AT and PA that systematically target mechanisms of change at the individual, intrapersonal, and community levels of influence may also simultaneously focus on individual behaviors, peer interactions, and positive use of SMP and the digital environment. As adolescent access of technologies and SMP will not likely decrease substantially in the near future, further consideration of the potential of these mediums to increase awareness, positive perceptions and promote opportunities for both AT and PA is recommended. This may lend itself to development of additional digital interventions to promote health behavior (Oh et al., 2022). Another perspective is provision of media literacy training that will enable adolescents to engage in SMP and technologies in a more positive fashion (Goodyear & Armour, 2021). Adolescent views regarding AT as an opportunity for peer-to-peer communication without distractions may simultaneously assist in promotion of AT and PA as well as reduction of sedentary screen time. A more balanced and thorough understanding of the associations between peer engagement and SMP to adolescent AT and PA is especially important in light of the potential benefits of adopting AT and PA behaviors and habits in adolescence for both present and future health and wellbeing.
Footnotes
Acknowledgements
We affirm that all of the individuals who contributed significantly to the research are listed. We wish to thank all the participating students and schools that took part in the study. Initial findings from the study were presented at the 2022 International Society for Physical Activity and Health (ISPAH) Conference.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.