
Abstract
Correlational research finds that transgender youth who have been homeless are more likely to have attempted suicide; however, there is not yet research explaining why this correlation might exist. To understand connections between housing insecurity and suicidality for transgender people the present study analyzed in-depth interviews with 30 transgender young people (ages 15–25) in the United States who had experienced homelessness. Interviews took place in LGBTQ community centers, and were analyzed for inductive themes using Qualitative Content Analysis. In contrast with theories suggesting that homelessness predicts increased suicidality because of the stressors of homelessness, this study found that gender-based parental rejection and other dysfunctional family dynamics interacted to create a hostile environment that contributed to both suicidality and homelessness for trans participants. In fact, suicide attempts occurred most often while participants still lived in disaffirming homes and usually ceased after participants left the unsafe home, suggesting that leaving a disaffirming family home, even if it results in homelessness, may decrease suicidality for some youth. Findings suggest that service providers working with transgender youth experiencing homelessness must consider familial gender disaffirmation, other familial stressors, and lack of access to shelter as equal threats to trans youth’s wellbeing and design interventions accordingly.
Transgender populations experience high rates of suicidality: In the United States, population-based studies have found that between 30% and 50% of transgender participants reported attempting suicide at least once in their lifetimes (James et al., 2016; Toomey et al., 2018). The Gender Minority Stress and Resilience model (Testa et al., 2015) can explain this increased suicide risk. Specifically, the model demonstrates how the gender-based stigma that transgender people face is inherently stressful and leads to three additional minority stress processes: expectations of rejection, internalized transphobia, and identity concealment (Testa et al., 2015). These chronic stressors then compromise health, including by increasing risk of suicidality (Austin et al., 2022; Testa et al., 2017). In other words, suicidality is not inherent to being transgender; instead, cisnormative cultural norms and societal institutions create a transphobic environment that harms trans people’s mental health. Understanding these norms and institutions and how they impact transgender people is the first step to changing them so that they are no longer hostile to trans life. Extant research has identified several specific factors that increase a transgender person’s risk for attempting suicide. Of these risk factors, past or present homelessness, familial rejection based on gender identity, and being younger than age 26 are some of the most consistently strong predictors (James et al., 2016; O’Brien et al., 2016); however, these three risk factors can overlap, and research has not yet investigated the nuances of how these experiences might intersect in trans young people’s lives to influence suicidality. The present study seeks to further illuminate how a history of homelessness might interact with familial relationships to affect suicidality for transgender adolescents and young adults.
Currently, limited research specifically focuses on trans youth’s experiences of homelessness (rather than LGBTQ samples more generally); however, the little research we do have suggests that transgender young people are overrepresented among homeless youth populations and are more likely to experience homelessness than their cisgender LGBQ peers (DeChants et al., 2021). Importantly, it appears that family environment can be a primary driver of trans people’s trajectories into homelessness (Shelton et al., 2018). According to the US Transgender Survey, transgender people who had been rejected by their families were twice as likely to have experienced homelessness (James et al., 2016). Furthermore, research investigating the family experiences of trans women of color found that many of the women in their study described their familial relationships as hostile, neglectful, or distant (Koken et al., 2009). It was these unsupportive familial environments that most often led to children being kicked out by parents or deciding to leave home before reaching adulthood, demonstrating that gender-based family rejection can begin a trajectory that ends in homelessness for trans people (Koken et al., 2009).
Shelton and Bond’s (2017) study further illuminates why trans youth may be more likely to become homeless by considering the impact of cisgenderism (i.e., both purposeful and inadvertent barriers that limit transgender people’s access to resources and supportive relationships). Researchers found that even though not all familial conflict that led to participants’ homelessness was directly related to their trans identity, it was often indirectly related. For example, participants described abuse based on nonconforming gender presentation (rather than transgender identity, per se), parents using homophobic or transphobic slurs when any kind of conflict occurred, and being kicked out because of substance use that they began because of fear of rejection and internalized transphobia. Additionally, cisgenderism meant that participants continued to experience instability after a family break, as they were denied access to social institutions (e.g., shelters, foster families) based on their trans identity.
Other research corroborates that institutional barriers intensify the harm that a rejecting family can do to a transgender young person. Research with transgender women living with HIV found that when trans participants had to leave home because of family violence, which was often driven by transphobia, they were then unable to find employment because of transphobic discrimination, which ultimately led to homelessness and engagement in sex work (Lacombe-Duncan & Olawale, 2022). Homelessness and engagement in sex work then increased these women’s vulnerability to police violence and HIV (Lacombe-Duncan & Olawale, 2022). In one study comparing healthcare outcomes and access for transgender and cisgender adolescents who had run away from home, transgender adolescents reported worse overall health, were more likely to have forgone needed medical care, and received less helpful care from medical providers than their cisgender peers (M. Ferguson et al., 2022). Finally, trans people who are homeless report difficultly finding safe shelter and accessing homeless services because of discrimination and lack of understanding from shelter staff (McCann & Brown, 2021).
Shelton (2016) reiterates many of the findings from the studies previously described but approaches its qualitative analysis from a perspective of resilience. Results interrogate the assumption that homelessness is, by definition, a more negative experience than remaining at home when families are rejecting, by showing how participants described both living on the streets and living at home as equally dangerous. Although participants described the ways in which being homeless was dangerous for them, they also described how leaving a rejecting family environment allowed them to connect with a community of other trans people and to pursue living as their authentic selves. Ultimately, leaving the home was described as an act of self-preservation by youth in this study, some of whom said that they would have killed themselves had they remained at home. Craig et al. (2021) similarly found that connecting to trans community was a powerful, positive experience for trans young people navigating homelessness and was an important part of developing a self-concept that allowed for resilience, even in challenging circumstances.
The Current Study
The current study used a feminist family framework (Allen & Jaramillo-Sierra, 2015; Few-Demo et al., 2014; Smith & Hamon, 2016) to explore links among family relationship patterns, homelessness, and suicide attempts for transgender youth by describing: (1) participants’ family relationship patterns, (2) how participants coped with minority stress perpetrated by family members, and (3) how family dynamics and coping mechanisms related to homelessness and suicidality for participants. Feminist family theory examines how systemic hierarchies organize families by normalizing certain family roles, structures, and processes while simultaneously marginalizing others (Few-Demo et al., 2014). Importantly, the core of feminist family theory is praxis: feminist family researchers seek to explain how power works upon families in order to help marginalized people resist oppressive power enacted through the family system. Feminist family theory, therefore, offers the present research the ability to examine how transphobia affects transgender youth’s lives at both the interpersonal and systemic levels.
We used the following key elements of feminist family theory to guide the present research. First, the theory centers research on marginalized voices and diverse family types, including recognizing the importance of chosen families/fictive kin (Allen & Jaramillo-Sierra, 2015). Transgender youth are often marginalized within the family system based on their gender identity and age. Even supportive and accepting cisgender-heterosexual parents may lack queer cultural knowledge, leading many queer youth to build strong ties with chosen families, which can provide caretaking, emotional, and material support (Levin et al., 2020). Although there is extant research that makes suggestions about how to respond to LGBTQ homelessness (e.g., Fraser et al., 2019; Prock & Kennedy, 2017), few specifically focus on the needs of transgender youth, including the important role that chosen family have in these young people’s lives. Second, feminist family theory recognizes the importance of considering individuals in context (Smith & Hamon, 2016), as opposed to studying trans people’s mental health in isolation of their family and community experiences. Third, feminist theory considers the implications of intersecting power dynamics and how they can affect one’s experiences (Few-Demo et al., 2014). Trans youth experiencing homelessness find themselves at a disadvantage with regard to several systems of inequality, including their gender, age, and class. Additionally, because of the impacts of racism and ableism, LGBTQ youth of color (DeChants et al., 2021) and disabled people (United States Interagency Council on Homelessness, 2018) are overrepresented in homeless populations. Although we do not specifically have data about the rates at which disabled trans youth and trans youth of color experience homelessness, given the data we do have, it is important to ensure that the experiences of disabled trans youth and trans youth of color are represented in research about homelessness. Particularly relevant to the present research’s focus on suicidality, intersectional analysis can draw attention to the unique experiences of transgender people living with chronic mental illness. Any research about trans youth experiencing homelessness that does not consider these axes of inequality in its analyses is likely to fundamentally misconstrue this population’s experiences. Finally, feminist theory expects scholars to do research that supports social justice. The current study has the potential to inform efforts to better support trans people experiencing homelessness and to develop interventions to reduce suicidality in this population.
Reflexivity
The first author is a White, bisexual, nonbinary person. The second author is a White, cisgender queer woman. We both live in the United States and have never been homeless. Our experiences are privileged in some important ways compared to our participants in that we do not experience marginalization because of our race, and we have never had to navigate the vulnerabilities of homelessness. Keeping this in mind, in our work with transgender communities, we do not believe it is our job to “give trans people a voice” but instead to help magnify the diversity of voices we know exist within the trans community. Related to this goal, we come to this work with a desire to highlight the agency of transgender people, particularly in our research about suicide and other coping behaviors that are often labeled as maladaptive. We believe that all behavior is adaptive in some context, and it is important to structure research to better understand those contexts if we want to best support people in finding the coping mechanisms that will bring them the least harm.
Methods
Participants
This research received full review by the Institutional Review Board (IRB) from Washington State University and was approved for subject assent with no parental consent required by minors under age 18. This distinction was important in order to be able to recruit and include young people who were homeless or estranged from their families. The ability to include participants based on subject assent was obtained by arguing that the harm to the population of transgender youth caused by not including youth who were estranged from families in the study was greater than the harm of participating in the interview (which was minimal).
The present study is a secondary qualitative analysis. The subsample analyzed for the present study included 30 transgender youth from eight cities in the United States, aged 15 to 26 years (M = 21.5, SD = 2.9), who had affirmed in their interviews that they had been homeless, couch-surfed, or experienced unstable housing at some point in their lives. The sample was recruited through community centers, youth group leaders, transgender listservs, and snowball sampling. Interviews were conducted between 2010 and 2014, and took place in-person at community centers that offered transgender-specific support groups for youth.
In the subsample of youth with histories of homelessness, 53% reported at least one racial or ethnic minority identity: 23% Latine/Hispanic (n = 7), 10% African American (n = 3), 10% Native American (n = 3), 7% Asian (n = 2), and 3% another ethnic/racial background (n = 1). Subsample participants primarily identified as genderqueer (n = 12; 40%), followed by transgender women (n = 10; 33%), and then transgender men (n = 8; 27%). Participants used 25 unique labels to describe their sexuality, which the researchers categorized into six major domains: queer (n = 6; 20%), straight (n = 4; 13%), gay or lesbian (n = 10; 33%), pansexual (n = 4; 13%), bisexual (n = 3; 10%), and asexual (n = 3; 10%). Twenty participants (67%) reported growing up in religious families; almost all (n = 19) of these families practiced some denomination of Christianity. Three participants had spent time in foster care, and five had ever been sexually assaulted. Twelve participants (40%) had run away from home at some point, and 10 (33%) had been kicked out of their home by their parents. An overview of data available in the interviews about participants’ homelessness experiences is presented in Table 1. An overview of participant demographics is presented in Table 2.
Overview of Participants’ Homelessness Experiences and Family Conflict Patterns.
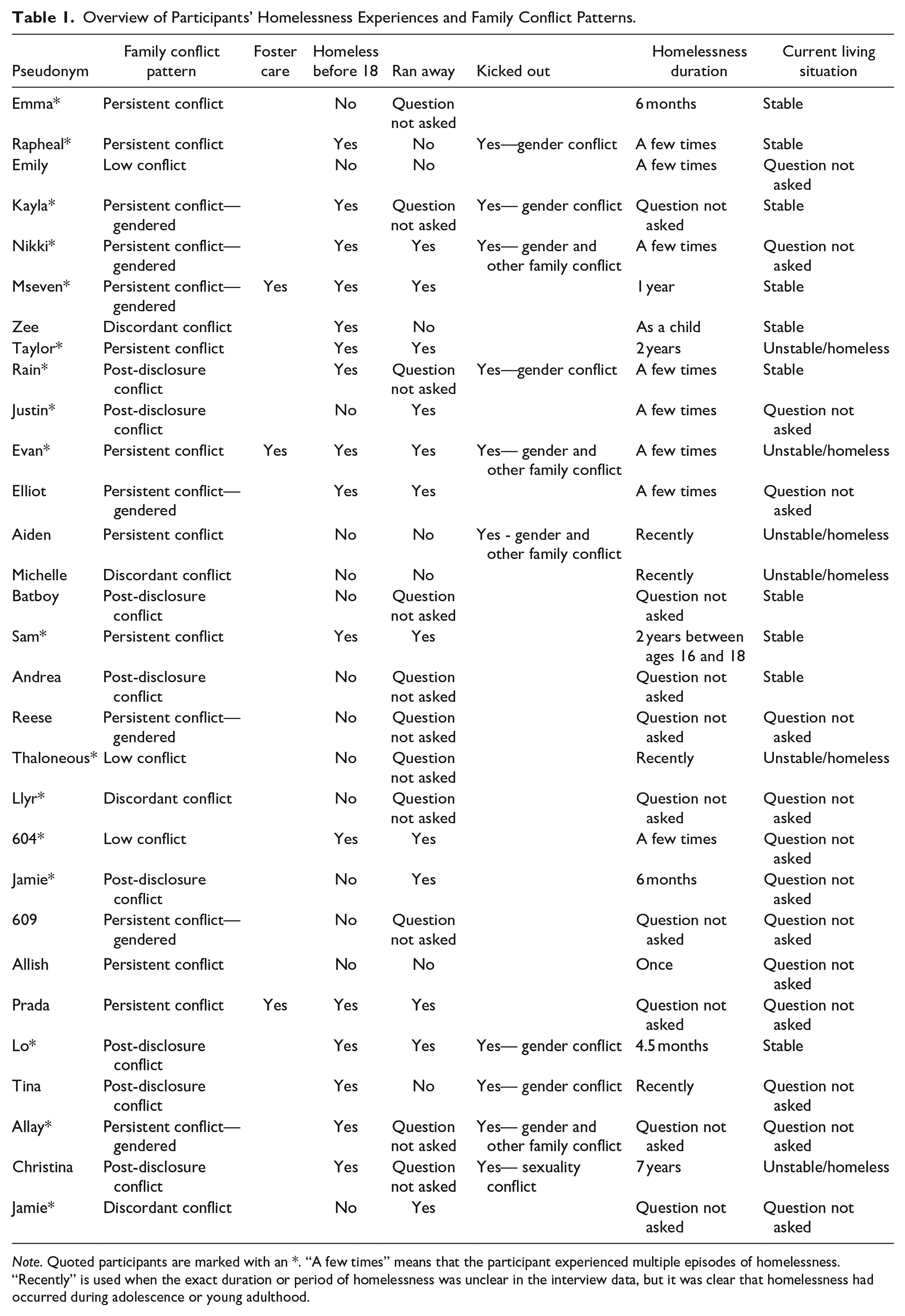
Note. Quoted participants are marked with an *. “A few times” means that the participant experienced multiple episodes of homelessness. “Recently” is used when the exact duration or period of homelessness was unclear in the interview data, but it was clear that homelessness had occurred during adolescence or young adulthood.
Participant Demographics.
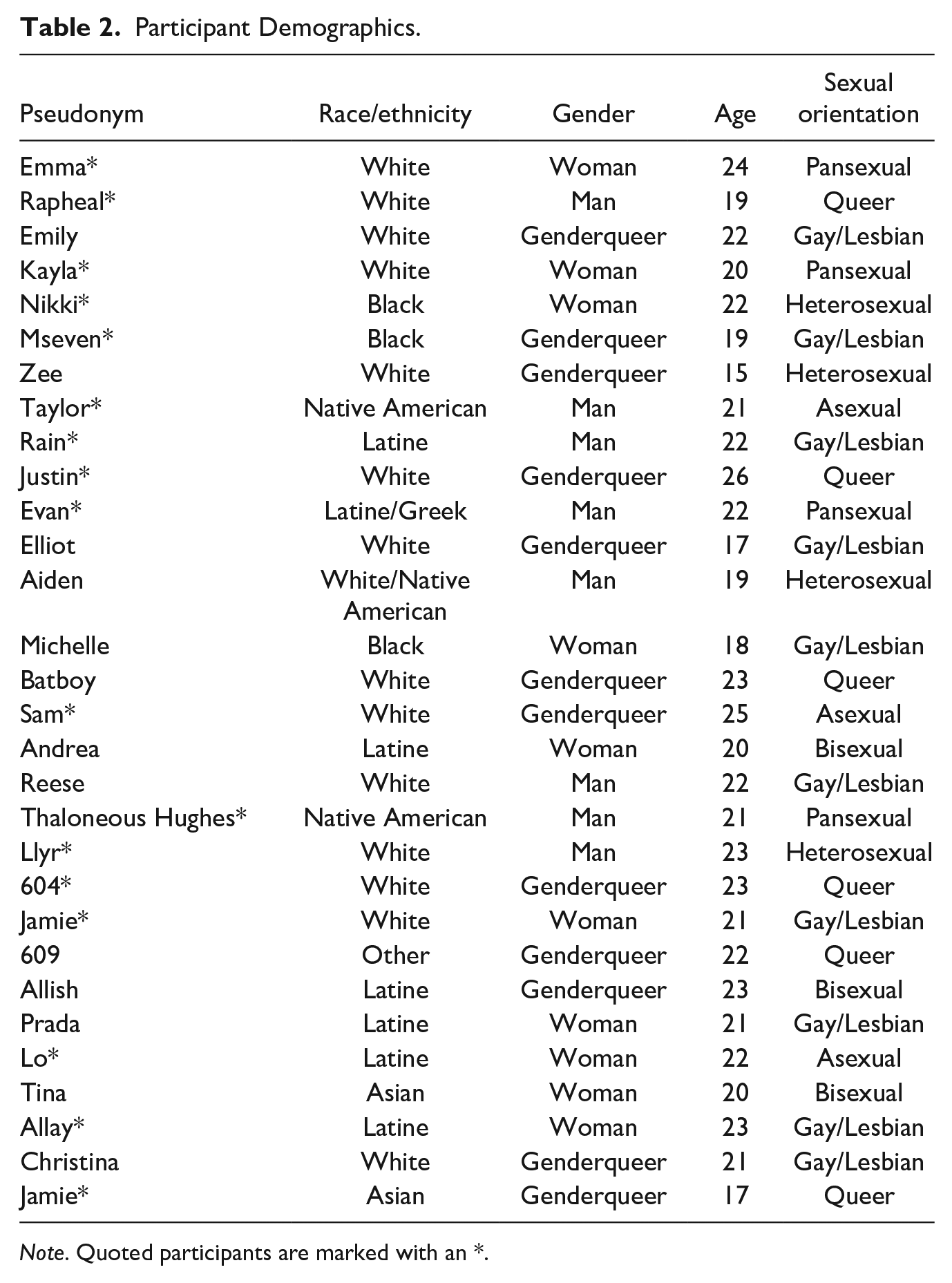
Note. Quoted participants are marked with an *.
Interview Guide
Interviews lasted between 90 minutes and 2 hours, and were conducted by a team of seven researchers: the second author was the primary interviewer, and was assisted by three graduate students and three undergraduates. One researcher would conduct the interview, while another took notes. Each interview was voice recorded and then later transcribed. Participants chose their own pseudonyms, and were compensated 20 US dollars for their time.
Procedure
In semi-structured interviews, participants were asked to describe their relationships with their parents/guardians, siblings, and extended family members, including how family members responded after they came out, level of conflict with parental figures, and family supportiveness regarding their gender identity. Additionally, participants were asked if they had ever been homeless or couch surfed, if they had ever run away from home, and whether or not they had ever considered or attempted suicide, among other topics.
Researchers used Qualitative Content Analysis (Schreier, 2012), to develop inductive themes regarding participants’ relationships with their parental figures and other family members over time, and to link those themes with participants’ experiences of homelessness and suicide. The analysis occurred in four steps: (1) reading without notations to familiarize oneself with the data, (2) identifying concepts in the data essential to homelessness, familial relationships, and suicidality (3) categorizing essential concepts into themes, and (4) selective coding based on these inductive themes. Additionally, the research team specifically coded responses to interview questions about suicidality for presence or absence of suicide ideation or attempt. For participants who described any suicide attempts, the research team further coded for the number of attempts, the timing of each attempt, and any triggers for the attempt (e.g., did the participant state that the attempt was because of a certain environmental stressor or a biological mental health issue).
Trustworthiness
Method and theory triangulation (Carter et al., 2014) were used to increase analysis trustworthiness. Multiple methods (audio files, transcripts, and researcher memos/journals) were used during the analysis process. The first author completed coding individually and then discussed various interpretations of participants’ reports with the study’s primary interviewer until both researchers came to consensus about the analysis. Additionally, feedback and support were solicited from colleagues with expertise in other fields, including clinicians who work with trans youth and researchers who study the impact of religion in families with LGBT children. An experienced qualitative researcher, who was not part of the research team, provided independent comments and feedback throughout the analysis process to assist the research team in conducting a trustworthy analysis.
Results
Family conflict and managing ongoing family relationships emerged as significant themes throughout participants’ interviews during open coding. Subsequent analyses identified typologies of family conflict, coping mechanisms for managing ongoing relationships, and connections between family relationship factors, homelessness, and suicidality. During the analytic process, we did not see homelessness itself acting as a primary risk factor for suicide in trans young people. Instead, we found an abundance of connections between: (1) family environment and suicidality, wherein participants described family conflict as a significant contributing factor to their mental health; and (2) family environment and housing instability, wherein family conflict and participants’ efforts to manage that conflict in order to protect their wellbeing could result in homelessness for participants. This data suggests that unsafe family environments may contribute to both risk of suicide and risk of homelessness for trans youth. Participants coped with challenging family environments through enforcing boundaries with parents, building chosen families, and access to other institutional supports (e.g., transitional housing programs); these coping mechanisms appeared to reduce suicidality but were often not enough to develop housing stability. Throughout the remainder of the results, we provide thematic frequencies and thick description of participants’ experiences as evidence for these findings. Participants are quoted using their chosen pseudonyms and pronouns. When describing participants’ demographics, we refer to their gender and not their sex assigned at birth.
Trajectories Into Homelessness
Participants described a number of factors that began their trajectory into housing insecurity or homelessness. Nearly all of these factors directly related to participants’ family of origin. Some participants (n = 6) experienced homelessness because of an adverse family circumstance that prevented their family from being able to provide housing support to the participant (usually poverty, although in one case, the untimely death of a parent was the precipitating event). Other participants (n = 3) became homeless after leaving foster care because they lacked a social/familial safety net. Importantly, in 73% of cases, participants became homeless directly because of family conflict: either because they were kicked out of their home by a parent (n = 10) or because they refused to return home due to perceiving the family environment as unsafe (n = 11). In some cases, these factors overlapped (e.g., a participant was initially kicked out but then refused to return home). Only four participants felt that they could turn to their family of origin for housing support if they couldn’t find another housing solution.
Suicidality
Eleven participants (37%) reported at least one suicide attempt and 18 (60%) reported any suicide ideation, which closely matches suicidality estimates from other community-based trans samples (O’Brien et al., 2016).
Contributing Factors for Suicide Attempts
Participants described a variety of contributing factors for their suicide attempts, including mental illness (n = 3), death of a loved one (n = 2), being a victim of sexual assault (n = 2), and gender/sexuality-based rejection from family members (n = 7). Oftentimes, two or three of these risk factors would co-occur, precipitating the suicide attempt. For example, Evan (man, age 22, Latine and Greek) described how several family stressors, including parental gender disaffirmation, came together to lead him to attempt suicide: There were a lot of things going on. . . Two of my family members were shipped out to Iraq so I was freaking out about that because I don’t agree with that, I don’t agree with war. So I was freaking out about that. My parents [were] definitely not supporting my decisions as to how I was dressing, how I was. Like, I was just falling apart.
Describing Family Conflict Patterns
Because the majority of participants implicated family conflict, especially with parents or guardians, in their discussions of homelessness and suicidality, we explored family conflict more in-depth. Overall, participants described four types of family conflict patterns based on level of conflict before and after coming out: post-disclosure conflict, persistent conflict, discordant conflict, and low conflict. Conflict could be gendered (i.e., related to participants’ gender nonconformity or transgender/LGB identity) or general (i.e., any other extreme conflict). Whether or not conflict was “extreme” was somewhat subjective, but included physical abuse, name-calling, any conflict that ended with police or Child Protective Services involvement, or a description of relationship cut-off (e.g., “I don’t really have a relationship with my parents”). Although gender and sexuality are distinct constructs, we decided to include conflict related to an LGB identity because many participants’ narratives about coming out or about gender-based conflict with their parents were intertwined with sexuality. For example, a parent might attribute their trans child’s gender expression to them “being gay” rather than to the child’s trans identity, but participants saw these experiences as being related to their trans identity; sexuality and gender were not always neatly distinguishable in these stories, but they were still very much trans stories.
Post-Disclosure Conflict
In the post-disclosure conflict relationship pattern (n = 8), participants described having warm and positive relationships with parental figures prior to disclosing their gender identity (or sometimes their sexual orientation), which became conflictual at the point of disclosure. Parents’ gender expectations for their children appeared to play a role in whether or not a previously-supportive parent-child relationship became conflictual post-disclosure; however, trans youth in this study reported great efforts to conceal their gender nonconformity in childhood from others due to fear of rejection and internalized transphobia, so parents were not always privy to the entirety of their child’s gender exploration. Emma (woman, age 24, White) described how her parents’ disbelief of her trans identity led to conflict: I feel like [my parents have] always known, but they claim that they didn’t. In fact, that’s the main reason why they wouldn’t accept my transition. They would’ve been okay with me being gay, but they wouldn’t accept me as being trans because they didn’t see me as being girly when I was younger. But I feel like from a pretty early age, I learned to suppress it as much as possible and hide it.
Some previous research suggests that parents of trans children can be disaffirming when their child first comes out but become more supportive over time (Riley et al., 2011). For the young people in this study, post-disclosure conflict with parents was not necessarily transitional. For example, Justin (genderqueer, age 26, White) described how his relationship with his family had changed since he had come out: I grew up very close to my family, especially [during] elementary school we were a very close family. . . I went and saw them for the first time in May since I started hormones and my mother called my voice alarming. . . For the past four years every time my mom looks at me she looks like she is about to cry.
In some cases, participants’ extended family members felt disaffirming parents were acting inappropriately and would step in to advocate on the participants’ behalf; however, these extended family members did not always have enough power in the family system to fully compensate for the lack of support from parents. For example, Lo (woman, age 22, Latine) described how her grandmother and her aunt supported her after her mom kicked her out but were unable to give her a place to stay because her uncle was unsupportive: [After my mom kicked me out for being trans] I went to my aunt’s [house] and I told her everything that I felt about my mom and how I was so angry with her and stuff. Because even when I had cancer, friends that came here and the staff would call me [my chosen name] because that’s the name I used to went by and [my mom] knew that, she knew that I identified that way. She just didn’t want to accept it, ya know. . . And you would think that she’d be more accepting of it because my grandmother’s accepting of it. Like, she’s the one actually that talked to my mom and told her flat out that [she was] stupid for doing that to her granddaughter and that she really needed to sit down and think about what she is feeling personally and whether that’s so important. . . verses loving her daughter and accepting her. So my grandmother stepped in and advocated for me and I told her I was thankful and I went to go to stay with her but she’s living with my uncle and my uncle doesn’t accept it, so.
Persistent Conflict
In the persistent conflict relationship pattern (n = 15), participants’ familial relationships were strained or abusive before identity disclosure, and participants’ trans identities or gender expression intensified existing conflict and dysfunction. Interestingly, participants in the persistent conflict group were more likely to be homeless before age 18 (n = 10; 63%) than after age 18 (n = 5; 36%). In fact, homelessness before age 18 was a more common occurrence for participants raised in persistent conflict than for any other conflict type (post-disclosure conflict [n = 4; 50%], discordant conflict [n = 0], or low conflict [n = 0]), suggesting that broader family dysfunction in combination with gender-related conflict may be a particular risk factor for earlier age of homelessness (see Table 1).
Untreated mental illness or substance abuse in the family could play a role in persistent conflict. For example, Taylor (man, age 21, Native American) explained how one of his mother’s bipolar episodes ended in him being sent to the hospital: “My mom stabbed my dad with a key and chased me down the street with a knife.” This, combined with gender disaffirmation creates a generally unsafe family environment: “[My] family, they don’t respect me whatsoever, so it’s hard.” Taylor described throughout the interview that his mother refused to use his chosen name and disaffirmed his gender publicly on Facebook, his father stopped speaking to him after he came out as trans, and his extended family was generally hostile regarding his gender.
As another example, Raphael (man, age 19, White) described a family environment that was persistently unsafe because of domestic violence and substance abuse: Me and my mom, like we kind of have a relationship now, but not really. Like it’s just. . . hey like you’re my mom. That’s about it, like we don’t really talk that much or anything and my dad, like he’s just completely out of my life. . . Him and my mom got divorced because like all of the mental abuse and the physical abuse that was going on and like he started stalking us or whatever so we moved out of [state] and like I was just done with it. . . [My mom and I] used to be really close but she’s became an alcoholic after she divorced my dad and stuff.
However, more recently, Raphael’s trans identity has also indirectly become a source of conflict between him and his mother, as Raphael was having a difficult time finding a job because of his trans identity. Ultimately, this conflict led to Raphael becoming homeless: “My mom’s kicked me out, quite a few times. . . Just for not getting a job, and not doing anything with myself.”
A substantial subset of participants in the persistent conflict group (n = 7) described parents or guardians reacting negatively to their gender expression prior to disclosure, meaning this subset of trans youth faced stigma from parents for their gender nonconformity even before coming out. For example, Nikki (woman, age 22, Black) described how her feminine gender expression, in combination with domestic violence in her household, created distance in her relationship with her family: I’ve seen my mom get hit once before by my sister’s dad and I jumped in and then she still picked his side and that made me feel real bad . . . and that was one incident that made me kind of back away from her and then I was getting so much grief from my uncles for being so very flamboyant and not wanting to play sports and wanting to hang out with my friends and all my friends are females and just giving me so much grief about nothing.
This conflict with her family eventually led Nikki to first run away and to later be kicked out by her family, resulting in homelessness.
Discordant Conflict
In the discordant conflict relationship pattern (n = 4), participants had one supportive parent and one disaffirming parent. All participants who described this pattern had parents who had divorced or separated; however, discordant conflict only described the experiences of a minority of all study participants with divorced parents (n = 15). Jamie (genderqueer, age 17, Asian) described how differently their mom and their dad have responded to their gender. Their father was not accepting of their lesbian identity or gender expression, and so Jamie didn’t feel safe to even come out as genderqueer to their father: I don’t really talk to my father. . . he knows that I’m a lesbian but he doesn’t know anything else beyond that about who I really am and who I feel I am and everything else like that. . . He’s super, super Christian. . . so he really doesn’t like it. Like, I kinda think that he’s hoping I’ll become a girl because he sends me all these girly things like purses, perfume, and necklaces and. . . I try to say thank you to him but it’s just like, that’s not really what I want. I guess it’s like I wish he would accept me more but I know he’s not going to any time soon. . .
Alternatively, their mom responded so well to their coming out as a lesbian that Jamie also felt safe coming out as transgender to her. Although this is not always the case, Jamie’s mother ended up being just as supportive about their transness as she had been about their sexuality: I just figured out being transgender so I did tell [my mom] and. . . she’s perfectly fine with that. . . She just lets me buy what I want and she’ll be like, “Try this on!” or “That would look cute!”. . . She’s not at all like, “Oh, don’t wear that because it makes you look like a guy,” or “Don’t wear that. That makes you look too girly,” or anything. She’s just perfectly fine with anything really.
Having one affirming parent could be protective for participants because they could turn to their supportive parent for help even when struggling with their disaffirming parent; however, the disaffirming parent could reduce their child’s access to that support, especially when they were the custodial parent. For example, when Llyr (man, age 23, White) wanted to move in with his dad because of the more supportive environment, his mom convinced him not to: [After the divorce] my mom remarried this man who was super abusive and I think my mom finally admitted a year ago that he was hitting us. . . Meanwhile my dad remarried [a woman] who is someone I could totally talk to later. She is a great person. . . So my dad’s home was pretty good. They’re very liberal, super, super liberal. And so my mom was always like, “your dad is crazy. . .” I had an opportunity, [my dad] lived next to an art school and I could’ve gotten in and lived with him and gone to art school and it would have been incredible, but my mom was like, “Your dad is crazy,” so I didn’t go. . . [Dad’s] a lot more supportive than my mom keeps on saying. My mom tried to send me to a gay [conversion] camp.
Instead of staying with his father, Llyr went to a different art school and had to pay for his own housing, leading to housing insecurity. Eventually, Llyr could not continue to pay his rent. He said, “I couldn’t afford an apartment by myself and I couldn’t find two people to move in with me, but it was like, that was really bad.” It is not entirely clear from his interview how Llyr solved the situation as he did have housing at the time of the interview, but at another point in the interview, Llyr states that he had paid for his art school using a combination of student loans and $500 monthly stipends from his father.
Low Conflict
The least common relationship pattern was the low conflict pattern (n = 3), in which participants described consistently warm relationships with their parents, even after disclosure. For example, Thaloneous Hughes (man, age 21, Native American) described his experience coming out to his mom and discussing his future plans for having children: We were driving up to [the city] that day so I was going to tell her that morning and it was interesting. I was telling her about this conference I went to and she stopped me and said, “Hey, I was watching Oprah the other day and there was this trans guy on there who is having a baby, Thomas Beatie.” And she said, “Is that anything you’ve ever considered?” And I said, “Ya know, as a matter of fact it is.” And so my mom has been nothing but supportive.
For participants in the low conflict group, homelessness occurred because of other family factors, such as family economic insecurity. Thaloneous Hughes explained later in his interview: I am moving out of my place on Friday and I don’t have anywhere set up and that’s nerve-racking to me. I think that class issues and poverty have always been something that I worry about. I mean, I grew up on welfare and food stamps and the whole thing so it, it bothers me not to know where my housing is coming from. . . We have applied for subsidized housing, but haven’t heard whether or not that’s been approved yet so, pretty much can’t afford anything but subsidized housing so we’ll see what happens when I get there.
Disentangling the Influences of Homelessness and Family Conflict on Suicidality
Timing of Suicide Attempts
The timing of participants’ suicide attempts suggests that homelessness could not have been a primary contributing factor to suicide for most youth in this sample, as the majority of participants had attempted suicide before ever becoming homeless. Eight participants attempted suicide for the first time while still living with their family of origin, and before becoming homeless. Of these participants, seven did not have any additional suicide attempts after permanently leaving their family homes. The timing of one participant’s attempt was unclear.
Family Conflict Patterns and Suicide Attempts
Because homelessness did not predate suicide attempts for most of this sample, the research team looked for other contextual factors that might influence suicidality for participants. Analyses identified certain family conflict patterns as largely overlapping with suicide attempts. Of the 11 participants who attempted suicide, 10 came from unilaterally disaffirming families: eight described family environments of persistent conflict, and two described post-disclosure conflict with their families. Kayla (woman, age 20, White) discussed how persistent gendered abuse from her father and feelings of hopelessness about her prospects for living as her authentic gender led to both of her suicide attempts: Several years before [leaving home] I had attempted suicide twice. . . It was just, I knew I was different than everyone else. And I couldn’t really live the way I wanted to, I was always told by my dad, “Are you a man or a mouse?” And so, I was like, “I’m a mouse!” and I’d continue to cry and then he’d slap me, or punch me, or kick me, or whatever. So I attempted suicide twice. . . [In my early teens] I took like a whole bottle of ibuprofen tablets and ended up having to go to the hospital for it. And they also put me into the mental hospital, which I was in the youth ward, and I was there for a couple months. . . Then in my late teens after I had come out, when I was starting to see, “Hey, I’m never going to be able to live like this. . . even if I’m not living with my parents.” So I attempted again, and it was with cutting. . . and then I was put in the hospital and was in there for quite a while.
Importantly, having at least one supportive parent (n = 7) appeared to be protective for suicide among participants: only one of the participants in the low conflict group and none of the participants in the discordant conflict groups reported a suicide attempt.
The Role of Chronic Mental Illness
The three participants who attempted suicide after permanently leaving their family homes all directly connected their attempts to severe mental illness (two participants had been diagnosed with bipolar disorder, and one participant had been diagnosed with obsessive compulsive disorder) that began before their period of homelessness. For example, Sam (genderqueer, age 25, White) described the lifelong nature of their experiences with obsessive compulsive disorder and how the associated intrusive thoughts resulted in their two suicide attempts: I was like 8 and there was a fire at my school and that was really unhappy making and probably prompted the OCD type behaviors for a while. So they took me to a counselor at that point and I was acting depressed apparently when I was 11 so I started medication on and off and so I had a team. And then in my late teens it really like exploded with really more distressing OCD symptoms, a lot of suicide [ideation], in and out of the hospital, tons of different medications and that’s pretty much been my whole life. . . Sometimes dozens or maybe a hundred times a day I would be having intrusive thoughts about hurting myself or killing myself and that would sometimes end up manifesting as like, “Fine, I’m just gonna kill myself,” or whatever in a more active sense.
Similarly, the one participant (604: genderqueer, age 23, White) from the low conflict group who reported an attempt connected their attempt to a combination of bipolar disorder and PTSD from the recent suicide of a friend: Bipolar disorder runs in my family. . . I noticed the onset of symptoms around puberty. And my manic episodes tend to not be the fun kind of mania but the angry kind where I am angry for no reason. So I would say that I go, depending on the cycle I go from severe to moderate depression. And then when I was. . . 21 something happened to me and for a period of time after that I suffered from a little bit of PTSD. . . I went with a bunch of my friends and classmates [on a trip]. . . we got there, checked into our hotel. . . and at around 5:00 AM or so there was. . . frantic pounding on the door. . . and I was like, ‘Oh my god the police are here. What’s going on?’ and they told me that my friend. . . had died, had killed himself in the hotel. . . That happened in November and in early January I tried to kill myself.
Indeed, the need for accessible, trans-affirming mental health care arose as a significant concern for participants across interviews. For participants from family systems with post-disclosure or pervasive family conflict, access to trans-affirming mental health services that simultaneously provided housing stability and protection from the brunt of family conflict were was especially impactful. For example, Evan (man, age 22, Latine and Greek) grew up in and out of foster care, and starting self-harming at age 13. After attempting suicide at age 15, Evan’s self-harming behavior and conflict with his family intensified to the point that his parents placed him in a group home. Evan described this as a turning point: I went into this group home at 17. My parents just couldn’t take it anymore. They tried locks because I kept running away. Finally they were like, let’s try a group home. So I. . . stayed there till my 18th birthday and I started to do better. I. . . stopped cutting. Wasn’t doing that stuff anymore. Um, and started to become more mature as an adult, so I could start to function as an adult. And it was a good year. . . In particular I did get attached to [one of my therapists] and I was able to share things that I hadn’t been able to share without freaking out. . . From the moment she [the therapist] met me she was like. . . “You are working on some trans issues I see.” And I’m like looking at my outfit and I’m like, “Yeah.” She goes, “Understandable.” And I’m thinking, wow, like, this doctor isn’t like anybody I have ever seen. . . By the time I was ready to leave [the group home], I was perfect. [I was] happy and I was myself.
Although Evan was able to significantly improve his mental health through this intervention, he was still unstably housed at the time of the interview. The institutional support available to Evan to help him in lieu of his family of origin was inadequate at responding to the full range of his needs for both mental health care and long-term stable housing.
Managing Ongoing Familial Conflict
In accordance with prior research showing that many trans people maintain relationships with family members even when they have been rejected (Grant et al., 2011), many participants in the present study still had some form of relationship with their families at the time of interview. Even when participants said they had come to an understanding with disaffirming family members, these relationships remained complicated because participants had to balance the potential benefits of keeping a family tie with the potential costs of inviting further harm.
Boundary Enforcement as Coping
Establishing and maintaining boundaries with parents and guardians was emphasized as being important for wellbeing (n = 11), even when maintaining these boundaries resulted in homelessness. Boundaries included refusing to interact with family members who were disaffirming or abusive, sometimes by running away from home, or limiting the degree to which they relied on family members to provide support. Jamie (woman, age 21, White) described her decision to stay in a shelter instead of living with her parents when she was unemployed: I was unemployed. . . and I lived with my aunt and uncle for like four or five months. They were like ok it’s time to go. . . and so I didn’t have money, like hardly any money at all. . . So I decided, I don’t know, I didn’t want to be a burden on my aunt and uncle and I didn’t want to pay for rent and I didn’t want to live, you know, at my parents’ house so I lived at a homeless shelter on and off for like a month.
Participants in familial systems with discordant conflict had some protection from homelessness when they chose to enforce boundaries because they could turn to their affirming parent. For example, when Jamie (genderqueer, age 17, Asian) ran away from their disaffirming father’s house, they were able to call their affirming mother: I ran away from my dad’s house, again that’s when I stopped talking to him. [It] was around 8th grade-ish. . . My dad called the cops on me. . . but I did run away from his house because I didn’t want to deal with him anymore. It’s just that he’s really mentally kind of abusive I would say. . . He’s also really controlling so it’s like if you don’t do something his way he’ll make you feel about it. . . and it’s like, I didn’t want to do that anymore because I wanted to tell him how I really felt and that I had a girlfriend and I couldn’t do that because I was just so afraid. . . So I just ran away from his house cuz I just didn’t want to deal with that and I had my mom come pick me up and everything, I wrote him a note and just left.
However, boundary enforcement could still lead to legal problems if the disaffirming parent decided to involve law enforcement, as did Jamie’s father.
Instrumental Support
Some participants reported continuing to receive instrumental support (e.g., occasional financial support) from family members; however, many participants were wary of this support because they saw it as a way for generally unsupportive family members to attempt to re-establish control over their lives. For example, Rain (man, age 22, Latine) described how his parents offered some financial assistance with the stipulation that he not use it to pay for his transition: I came out to [my parents] and they stopped financially supporting me for quite a while and I lived in my friend’s kitchen. . . They partially reinstituted a bit after that, but then they were convinced that I was saving up for surgery. So any time I would ask for help with rent, they’d be like, “You’re saving up for surgery, we’re not gonna give you money. . .” I’m like, “Are you fucking kidding me? I’m in massive debt and I can’t feed myself. I’m like, stealing food from work here.”
Ultimately, this situation was untenable. Rain continued, “I had been struggling, but obviously the power play of pulling my financial assistance didn’t work in making me back into a girl. . . I would be like, ‘Fuck you, I’m not talking to you. . .’ I didn’t trust them, at all, to give me any financial support.” Rain had to find other ways to pay for housing.
Therefore, when relationships continued to be strained, some participants decided to refuse instrumental support from family, even if that support could help them access necessities. For example, Emma (woman, age 24, White) talked about refusing to reconnect with her parents, even though it could help her access health insurance to pay for her transition: I had a found a place I could get prescribed for very, very little money and I could see a doctor. So I was just buying my hormones. I didn’t have insurance, I still don’t. . .. [When asked if she would be willing to go back on her parent’s health insurance] No, because that means I have to be willing to talk to them. I can work enough to just pay for it without insurance. That’s what most people seem to be doing.
Reconciliation
Even when participants found some sort of reconciliation with family members, they often still described a degree of emotional or physical distance as a form of self-protection, and did not feel that they could turn to parents/guardians as primary support systems. For example, Allay (woman, age 23, Latine) described how the birth of her younger brother led to a tentative reconciliation with her mother after her mother kicked her out and refused to provide any financial support for 7 years; however, reconciliation did not solve ongoing tensions in the relationship: . . .it’s awkward because she’ll bring up stuff that to her it’s willy-nilly and to me I think, “You actually abused me and you’re laughing about it now.” So it’s strange still to this day and even now, little comments that she makes, [like] “Oh, your hair, you like it like that?” or “Oh your outfit, is it supposed to look like that?” You know, just little things like that.
Importantly, reconciliation with her mother did not improve Allay’s housing situation; she still needed transitional housing services at the time of the interview. Allay described the process of receiving transitional housing through the emergency shelter: “First, it was more trying to just stabilize myself if I could through my family. Didn’t work out. And so then the [transitional] housing opportunity came on.”
Chosen Family
Most participants (n = 23) created chosen families to make up for support they lacked from their families of origin. Rain (man, age 22, Latine) talks about moving away from where he grew up in order to find a more-affirming support system: [My parents and I] live 3000 or 4000 miles apart and it works better that way. . . I had such a hard time, trusting them after that whole experience [of them cutting me off financially] for obvious reasons. . . I decided that I really didn’t ever want to talk to them again. I didn’t want to see them; I didn’t want to have anything to do with them. Our relationship was not. . . supportive or good or anything that I wanted from parents. You know, I have a really great and supportive friendship community [here], you know, I have everything I’ve wanted, and my parents stressed me out more.
Participants felt that their chosen families acted as equally-strong or stronger emotional support systems than their families of origin. For example, Mseven (genderqueer, age 19, Black) described how their partner, an important member of their chosen family, supported them: She’s very supportive in everything that I do and everything that I chose to do [including my transition]. . . Like if I have a hard time or whatever, or anything that I’ve ever gone through she’s always there. Whenever me and my mom get into it, she’s there.
However, similar to extended family, chosen families were not often able to provide the kinds of wrap-around instrumental support that families of origin generally provide to their children.
Bringing All of the Pieces Together: Nikki’s Case Study
Oftentimes, the process of attempting to reconcile with family members was long, and the instability created trying to cope with familial conflict could simultaneously threaten participants’ mental health and leave them with essentially no place to go. Each participant’s narrative was unique, but Nikki’s story provides a good example of the overall picture painted across interviews about how familial conflict could result in both suicidality and homelessness. Nikki (woman, age 22, Black) described how she began contemplating suicide at age 13: It was just that I was so suicidal because I felt like no one understood me and. . . I’m like, “Ok so what’s the point of me being here if nobody understands me?” So I’m just like, “Ok, I’m just gonna go and kill myself don’t nobody wants me to be around,” or “Don’t nobody cares about what I’m going through,” and that’s what made me suicidal.
These feelings of thwarted belonging seemed to arise from a family pattern of persistent conflict wherein domestic violence combined with gender-based rejection to make Nikki’s childhood household unsafe.
After attempting suicide for the first time at 13, Nikki began a prolonged period of homelessness: [I was homeless] off and on because I was usually running away or getting kicked out of the house or you know so it was off and on from 13 up until now I guess you can say. The first time I ran away. The second time I got kicked out. The third time, they brought me back and then I got kicked out again and from that point I just stayed away. . . Then when I moved up here [at age 17], I knew for a fact I was really gonna be on my own because I have no family up here.
This period of housing instability, interlaced with continued family conflict, led to further suicidality. Nikki explained, “It felt like I was just steady going from place to place to place and I’m like, I’m so tired of this, I just want to just fucking kill myself.” Nikki attempted suicide two more times during this period. It was ultimately when she decided to enforce boundaries with her family of origin by moving to a different state that Nikki was finally able to begin to break this negative mental health cycle: “I feel like when I moved up here, I was like, trying to basically start over. . . cuz it’s the first state I moved to other than growing up in [city], so I figured new place, new attitude, new life, new everything so I quit drinking, quit smoking.”
Right after the move out of state, Nikki made her third and final suicide attempt. She then spent a period of time inpatient receiving mental health care before she entered a homeless shelter. The homeless shelter served as a place where Nikki could rebuild a support network; while at the shelter, she met the group of people who she described as her “adopted family.” Nikki’s chosen family provided her with the emotional and instrumental support that she had not been able to safely access in her family of origin.
I met [my adopted family] and they’ve been basically taking care of me, you know, [they] let me stay with them or if anything happens, they’re there for me. . . I feel like I can talk to them more about [trans] stuff than my own family and they’re more understanding about the situation because they have a couple of gay people in their family so, they’re like, “Oh you fit right in.” They welcomed me from day one.
It was because of access to mental health care and the shelter system, as well as the support of her chosen family, that Nikki was finally able to find the stability she needed to improve her mental health, although she was still living with housing insecurity.
Discussion
This study contextualized the family experiences of trans adolescents and young adults who have been homeless as a way to better understand potential risk and protective factors for suicide at the intersection of transgender identity, age, housing status (socioeconomic status), and mental illness (disability). Most participants described complex relationships with family members that involved managing conflict and rejection by seeking opportunities for reconciliation when safe and creating distance when relationships were not supportive. In accordance with extant research (e.g., Fraser et al., 2019), conflictual family relationships and participants’ efforts to manage those relationships could lead to homelessness, either because the trans young person was kicked out of their household, ran away to protect themselves from violence, or decided to reject potential instrumental support from disaffirming family members.
Although homelessness was undoubtedly a stressor for participants, when considering risk and protective factors for suicide, the absence of affirming parental figures and other dysfunctional family dynamics were more likely to be implicated as contributing factors. Specifically, most participants attempted suicide while still living with disaffirming family members and before becoming homeless, and ceased suicide attempts after permanently leaving the disaffirming environment. Chosen families, in particular, were frequently mentioned as important supports that could buffer the lack of affirming parents (see Levin et al., 2020 for a targeted study of queer kinship and caretaking). The minority of participants who attempted suicide in supportive family homes all described their attempts as being primarily related to life-long, severe mental illness, such as bipolar or obsessive-compulsive disorder. Indeed, regardless of parental support, access to trans-affirming mental healthcare was consistently mentioned as important for wellbeing across participant interviews. Despite their import to wellbeing, however, chosen families and mental healthcare could not reliably provide housing security.
Participants’ narratives about family reconciliation and boundary maintenance coincide with previous research in general homeless youth populations that found identity protection to be an important consideration for youth when they are deciding whether or not to engage with formal and informal support services (Samuels et al., 2018). Our findings also reinforce concepts from feminist family theory about “doing family” as an active, ongoing process, rather than as a static state of “being family.” Many of the participants maintained some sort of relationship with their disaffirming relatives, and some even managed to improve their relationship over time; however, this reconciliation usually occurred because of ongoing action and sacrifices on the part of the trans child and not because parents gave up their transphobic beliefs (at least not completely). For this sample, reconciliation required the youth to decide the relationship was worth preserving in spite of gender disaffirmation, but lack of acceptance still created distance and pain in the relationship. For those youth who were unwilling or unable to accept their legal guardians’ disaffirmation, forgoing physical necessities, such as stable housing or healthcare, sometimes became the cost of protecting their sense of self. The connection between gender-based rejection and suicide for the youth in the present study suggests that protecting this fundamental sense of self can be just as important as fulfilling more-obvious physical needs. For these youth, homelessness was by no means a safe option, but it was still perceived by many youth as safer than remaining with the family of origin, as evidenced by the fact that over one-third of participants experienced homelessness because they refused to accept housing or other support from disaffirming family members.
Implications
These findings call into question conceptualizations of homelessness itself as a primary risk factor for suicide in trans young people; instead, unsafe family environments may contribute to both risk of suicide and risk of homelessness for trans youth. In accordance with previous research (Cramer et al., 2022), over half of participants described family gender disaffirmation as a trigger for at least one of their suicide attempts, and disaffirmation did not necessarily give way to more supportive behavior from families over time. The varied types of familial conflict observed in the present study also can inform attempts to reduce harm to trans youth. In contrast with popular narratives about trans homelessness, gender disaffirmation after gender identity disclosure (i.e., post-disclosure conflict) was not the only cause of family conflict for participants. Instead, the persistent family conflict pattern was most common, in which the family environment was unsafe both because of gender disaffirmation (which could occur even before identity disclosure) and also because of non-gender specific familial challenges, including domestic violence and substance abuse.
Family of Origin Interventions
In consideration of these findings, service providers working with trans youth experiencing homelessness ought to be cautious when employing interventions based singularly around family reintegration. Although family reintegration programs, such as the Family Acceptance Project and the Family Preservation Program (K. M. Ferguson & Maccio, 2015), provide important and appropriate strategies for some youth, these programs either focus on helping families become more trans-affirming (e.g., Family Acceptance Project), or on helping families manage other more general home stressors (e.g., Family Preservation Program), but not intersections of how trans-specific conflict and other family conflict may interact. Results in the current study suggest that assessing home safety for trans youth requires considering whether or not the home is trans-affirming, and not just whether physical abuse or neglect are present in the home. Service providers need to consider the likelihood that the family environment may be unsafe in intersectional ways that require complex levels of intervention, and some youth may be better served in alternative placements.
That none of the participants from the discordant conflict group attempted suicide suggests that having even one affirming parent may buffer the impact of another parent’s rejection on suicidality. Trans youth experiencing homelessness who are from families with discordant conflict may be especially strong candidates for family reintegration programs if the youth can live with the affirming parent; however, trans-supportive parents can sometimes face custody challenges from non-affirming parents for affirming their child’s gender (Kuvalanka et al., 2019). Service providers may further benefit youth in this situation by providing the supportive parent/guardian with skills and resources to help them manage the influence of an unsupportive parent and navigate legal challenges when necessary. Additionally, future research should further investigate the effects of parental divorce in general trans youth populations, as custody placements that allow trans children to live with their more-affirming parent after a divorce may be the most beneficial living situation for the mental health of a trans child.
Social Policy Interventions
Intervention in families with post-disclosure or persistent conflict patterns may not always be possible in a timely manner; many participants stated that their parents were resistant to changing their perspectives about their child’s transness and the patterns of domestic violence, poverty, and substance abuse described by participants living with persistent family conflict can also be challenging to influence via clinical intervention alone. Therefore, considering how social policy impacts the resources transgender young people experiencing homelessness have available to them is critical.
Because subsidized housing and other social safety net programs are vastly underfunded by the U.S. federal government, American transgender youth who have to leave home have few options for finding housing (Kingsley, 2017). Therefore, parental rejection does not only mean a break in an important attachment relationship but also can lead to a lack of access to basic necessities, such as adequate food and shelter. This may make the stress of expected parental rejection (and resulting risk of suicide) even greater for trans youth in cultures that give people under age 18 little agency apart from their parents because youth realistically recognize that parental rejection can be an existential threat, as well as an emotional one. This might cause trans youth who fear parental rejection based on their gender to feel like they have no good options available to them, thereby increasing distress and potential for suicidality. Indeed, participants in the current study were often able to find consistent emotional support from chosen and extended family, but chosen families were less likely to be able to make up for the material needs that parents often provide their children. Trans-affirming, trauma-sensitive mental health interventions that employ harm reduction frameworks and support trans youth in fostering stable chosen family systems can bolster some of the resiliency behaviors we observed our participants naturally engaging in. As such, these interventions are important to scale up in order to meet needs associated with the high rates of mental illness experienced by trans youth populations (for examples of programs already being used by some service providers, see K. M. Ferguson & Maccio, 2015). Mental health interventions are not enough alone; in order to have physical, emotional, and mental wellbeing, trans youth (including young adults who often still need support with living expenses) need viable options for housing and financial security. Even when family conflict is low, poverty itself is a risk factor for homelessness (Robinson, 2018): several participants in the present study had supportive families of origin but experienced homelessness due to family poverty.
Results from the present study combined with extant research suggest that one of the most straightforward and impactful interventions to reduce suicidality and homelessness for trans youth is to expand government-based social safety net programs, including (but not limited to) universal health care, supplemental nutrition programs, direct cash transfer programs, and housing-first initiatives (Daniels & Morton, 2023; National Alliance to End Homelessness, 2016; Neighly et al., 2022). Social safety net programs can insure that regardless of their family environment, trans youth have access to basic necessities, and should be seen as high priority components of any inclusive LGBTQ-rights platform. In relation to these goals, advocacy efforts seeking to support the trans homeless population should work toward implementing enumerated anti-discrimination policies that include sexual and gender minority people as a protected class to reduce the likelihood that trans people are barred from accessing supportive services, housing, employment, health care, education, or fair treatment in legal proceedings.
Cohort Effects and (the Lack of) Systemic Change
Data used in the present research were collected between 2010 and 2014. In some ways, things have changed for trans youth since these interviews, including the COVID-19 pandemic and the proposal/passage of a slew of anti-trans legislation in the United States. However, we do not believe that any of these cohort differences fundamentally have changed the dynamics we observed in the present study regarding how family conflict, suicidality, and homelessness can interact for trans youth today for several reasons. Culture in the United States remains cisnormative. Increasing visibility of queer people and identities has caused more trans people to come out at younger ages, but has not reduced experiences of stigma that lead to negative mental health outcomes (Russell et al., 2022). Research measuring mental health during COVID-19 found that transgender youth reported more difficulty accessing mental health treatment and less familial social support than cisgender youth (Hawke et al., 2021). In fact, 63% of trans youth reported not receiving mental health care that they needed during the pandemic (Hawke et al., 2021). This is similar to what we observed in the present research, even before the pandemic—our participants did not have supportive family, which negatively impacted their mental health, and they had additional challenges accessing affirming mental health care.
Due to a lack of affordable housing, homelessness in the US has been increasing since 2016 (Henry et al., 2021). Because of the impacts of transphobia and racism, transgender youth and people of color are overrepresented in homeless populations (de Sousa et al., 2022), suggesting that trans youth of color are likely also overrepresented. Many overburdened housing programs simply failed to meet the further-increased demands presented by the pandemic, which led to an increase in unsheltered homeless populations that persists at time of writing (de Sousa et al., 2022). It is not unreasonable to assume that this especially affected trans people, who are often barred from accessing supportive services due to transphobia (Shelton & Bond, 2017), giving even greater urgency to the present research’s call for programs that provide stable housing, rather than only temporary shelter, paired with enumerated anti-discrimination policies.
Most of the anti-trans legislation currently proposed or passed in the US is related to preventing access to medical transition for trans youth and access to safe, LGBTQ-inclusive education (ACLU, 2023). This legislation is dangerous to trans people and should be adamantly opposed in all instances. That said, access to medical transition for trans youth under 18 has always required guardian consent (Coleman et al., 2022), and 23 of our 30 participants did not have any affirming guardians. These young people could not have accessed medical transition even before the passage of recent anti-trans legislation because they would not have been able to acquire the necessary guardian consent. Similarly, even before the passage of legislation that requires that schools disclose students’ queer identities to parents, school officials might have done this anyway at any time, which prevented many trans youth from being able to feel safe in their gender at school, further increasing the mental health burden of an unsafe home by removing access to potentially-supportive connections outside the home (Kahn et al., 2018). Even before legislation that restricted teachers from discussing LGBTQ issues at school, most schools did not teach LGBTQ-inclusive curriculums, leaving trans youth without life-saving, life-affirming knowledge of queer community, queer history, or inclusive sexual education (Kahn et al., 2018). All this to say, recent anti-trans legislation has only served to further enshrine existing anti-trans prejudice by validating transphobic norms and punishing parents, clinicians, educators, and trans people who attempt to subvert those norms.
Considering these realities, the pandemic and passage of anti-trans legislation may have actually intensified the processes we observed in the present research. Until uncompromising, systemic interventions opposing transphobia, ageism, ableism, racism, and homelessness are implemented in the family, in schools, in social services, and in policy, we can do this research 10 years in the past or 50 years in the future, and nothing will fundamentally change.
Strengths and Limitations
The present findings, as well as their implications, must be viewed in light of this study’s strengths and limitations. The qualitative, in-depth nature of the data and the breadth of the interview protocol of the present study brought to light several important processes that can explain well-established findings in extant suicide research in trans populations. Specifically, the nuances of participants’ relationships with their families both before and after coming out as transgender, and the quantity, timing, and triggers for participants’ suicide attempts, including whether the attempts occurred before or after leaving home, captured how various contextual factors related to family environment, homelessness, and suicide can interact in ways not immediately evident in extant research. Additionally, although the present study is not a representative sample of trans youth experiencing homelessness, efforts were made during data collection to recruit a broad range of identities from within the transgender umbrella, including trans men, trans women, and nonbinary/genderqueer people, as well as a breadth of race/ethnic identities and broad geographic representation. Moreover, the sample reported rates of suicide ideation and attempts similar to those reported in larger quantitative studies of transgender people, suggesting that the sample was a good representation of suicide patterns within this population.
Despite significant strengths, the present study also has several important limitations. First, this project is a secondary analysis of data from a project exploring family environment and mental health in trans youth, and is somewhat limited by that narrow focus. Although interviewers asked participants whether they had ever been homeless, couch-surfed, or were insecurely housed, the purpose of the study was not to interrogate homelessness experiences. Therefore, the interview protocol did not delve into participants’ specific experiences with homelessness. In some cases, participants shared information about when they were homeless and for how long, but in other cases, they did not. In fact, the prevalence of homelessness in this community sample of trans people surprised the researchers and suggests that future research about trans populations ought to consider including specific questions about homelessness more often, as it is a fairly common experience for young trans people living in the United States: 23% of transgender people between the ages of 18 and 25 experience homelessness (DeChants et al., 2021). Furthermore, although efforts were made to recruit a racially and ethnically diverse sample, the interview protocol did not explicitly ask any questions about racialized experiences, and interviewers were not sensitized to probe for more information about race when participants spontaneously discussed it. Therefore, no themes cohered around how race affected participants’ experiences, even though race likely impacted participants’ experiences (see McCann & Brown, 2021). For example, chosen families/fictive kin are common in the Black community, which may affect how family systems function for Black trans youth (Soler et al., 2018). Additionally, racism itself acts as a minority stressor that trans youth of color have to navigate, which contributes to the overrepresentation of LGBTQ youth of color in homeless populations (DeChants et al., 2022; Glick et al., 2019). This is a point of caution for future researchers: the intersection of race was invisibilized by the interview protocol despite the diverse sampling strategy, which leaves an important gap for future research.
Secondly, the interview protocol primarily included questions about participants’ relationships with their parents or guardians. Questions also asked about extended family, siblings, and other trusted adults, but in significantly less depth. Future research still needs to investigate the impact of these important non-parental relationships on the wellbeing of trans youth with histories of homelessness. Finally, the present study was unable to find any patterns related to suicide ideation. It is possible that the threshold for suicide ideation is low enough that most trans people have enough risk factors to consider suicide at some point in their lives, but it is also possible the questions asked by the present study were not constructed in order to best capture variation in factors related to suicide ideation. Regardless, more research is needed to better understand the mechanisms that can lead suicide ideation to become a suicide attempt.
Opportunities for Future Research and Concluding Thoughts
The findings of the present study raise a number of questions for future research, especially in terms of applying intersectional methodologies when studying trans homeless populations. The present study did not include a strong measure of socioeconomic status, but a few participants’ interviews referred to low familial SES as a particular stressor, and previous research has linked lower family socioeconomic status to increased risk for homelessness (Robinson, 2018) and increased risk of suicide attempt (Cramer et al., 2022; Goldblum et al., 2012) for trans people. Indeed, access to social capital appears critical to preventing homelessness for trans youth. Although not specifically focused on trans people, Robinson’s (2018) qualitative study sought to further understand why LGBT people from low income, racial minority families are more likely to experience homelessness than white, wealthier trans youth, despite the fact that LGBT people across all backgrounds are rejected by their families. Specifically, the study demonstrated how under-resourced parents’ attempts to be good parents by socializing their child to adhere to gender norms could lead parents to reject a gender nonconforming child. Additionally, because these parents were under-resourced, they lacked access to supports that could help them come to terms with their child’s identity, and the young people lacked access to a broader network of people who could intervene in the face of family rejection to prevent homelessness. Future research should specifically investigate whether family SES is associated with trans youths’ familial experiences and whether these experiences might explain some of the variance in suicidality based on SES. Additionally, previous research has identified foster care as a predictor of homelessness for LGBTQ youth (DeChants et al., 2021). Indeed, all the participants in the larger study from which the present sample was derived who had spent time in foster care had also experienced homelessness at some point; however, research about trans youths’ experiences in foster care and long-term outcomes is still almost nonexistent, leaving an important gap for further study.
Participants in the current study often described complex family experiences that were unsafe because of a mix of gender-based rejection and other factors, which could drive suicidality and trajectories into homelessness. Family reconciliation may not always be appropriate or safe for these young people. Participants showed resiliency through enforcing boundaries with parents and building chosen families; these coping mechanisms appeared to reduce suicidality but were often not enough to develop housing stability. Therefore, professionals who work with this population need to be mindful of potential familial stressors and facilitate their clients’ agency in establishing appropriate boundaries with disaffirming family. Additionally, efforts to support trans youth must focus on advocating for the expansion of social safety net programs that provide access to basic necessities in order to proactively reduce harm to transgender people regardless of their specific family circumstances.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material is based upon work supported by the National Science Foundation Graduate Research Fellowship under Grant No. 2237827. Any opinions, findings, and conclusions or recommendations expressed in this material are those of the author(s) and do not necessarily reflect the views of the National Science Foundation.