
Abstract
Legalization of non-medical cannabis in Canada was intended to protect youth health and safety by limiting access and raising awareness of safety and risks. The purpose of this qualitative research was to explore youths’ perceptions of their cannabis health literacy and future educational needs. A convenience sample of youth aged 13 to 18 residing in Newfoundland and Labrador, Canada who may or may not have consumed cannabis were included. A qualitative study using virtual focus groups with semi-structured interview questions was conducted. Ethics approval was obtained. All sessions were audio-recorded and transcribed. Inductive thematic analysis used a social-ecological framework for adolescent health literacy. Six focus groups (n = 38) were conducted with youth of all ages and from rural and urban areas. Three main themes were identified: (i) micro influences (age, gender, and beliefs), (ii) meso influences, (family, peers, and school enforcement), (iii) macro influences (cannabis legalization and social media), and (iv) evidence-informed information (harm reduction and cannabis properties). They desired evidence-informed education using harm-reduction principles, integrated early, and interactive. The findings provide support for a cannabis health literacy framework that will inform youth cannabis education programs. Interactive approaches with real-world application should support their autonomy, share knowledge, and minimize stigma.
Background
The Cannabis Act brought forth good intent to prioritize awareness and education programs to support public health (Branch, 2020). To date, there continues to be a gap in the implementation of cannabis-relevant education across contexts (e.g., in the workplace, medical vs. non-medical consumption) or targeted resources for specific age groups (e.g., youth, young adults, and elderly; Health Canada, 2021). The lack of accessible cannabis education is of particular concern as Canadian youth are associated with the highest rate of cannabis consumption compared to other developed countries (e.g., United States, England, New Zealand, and Australia; Hammond et al., 2020). Data from the National Cannabis Survey indicated an exceptionally high prevalence of cannabis consumption in Canada amongst school-aged youth (age 15–17) of 19.2%, alongside a report of 7.9% of Canadians over the age of 15 having engaged in almost daily use (Rotermann, 2020). The commonality is further illustrated by findings of the Monitor the Future survey with reports of lower rates of cannabis consumption amongst American youth ranging from 11.8% in 8th grade to as high as 35.7% by 12th grade, with almost daily consumption reported by 6.4% of those aged 12 to 17 (National Institute on Drug Abuse, 2021).
These statistics are alarming, as youth are particularly vulnerable to experience significant cognitive, social, and psychological deficits with regular consumption (Jacobus & Tapert, 2014). Adolescence is also a turbulent time in life where youth undergo critical life transitions coupled with substantial brain development; therefore, early cannabis initiation coupled with regular consumption can increase the risk of cognitive impairment, which can impact learning and memory by almost two-fold (Hall et al., 2020). Chronic consumption of cannabis among youth also poses the potential to increase the risk of mental health (MH) concerns, such as psychosis, schizophrenia, anxiety, depression, cannabis use disorder, and suicide (Hall et al., 2020; Horwood et al., 2010). Furthermore, patterns of cannabis consumption tend to escalate over time, as opposed to a reduction or cessation of use (Zuckermann et al., 2019, 2020a).
Health Literacy
Health literacy is a multi-faceted concept characterized by an individual’s ability to critically evaluate, comprehend, and make informed decisions in a manner that prioritizes one’s health (Kickbusch, 2008; Rootman & Gordon-El-Bihbety, 2008). Evidence-based guidelines for lower-risk cannabis consumption can help reduce the risk of adverse health consequences by supporting informed behavioral choices, including abstinence, non-frequent consumption, avoiding early age initiation, use of non-inhaled low potency cannabis products, abstaining from cannabis-impaired driving, and avoiding combing risky behaviors (Fischer et al., 2022). The Government of Canada (2021) released a Blueprint for Action for reducing school-related substance use harms, which highlights the importance of encouraging open discussion in schools to facilitate prevention, reduce stigma, reduce harm, and diversify content delivery. With a greater focus on the delivery of substance use education in schools, it may enhance youth engagement in making healthy behavior change, thereby improving their substance use health literacy.
Existing Cannabis Education
Adolescence is a crucial period for the integration of education to inform decision-making, as cannabis habits are predominantly formed in adolescence, with 40% of cannabis initiation beginning before 14, of which one in six later developing a cannabis use disorder (George & Vaccarino, 2015). This further emphasizes how critical early education with skills training can help protect the health and safety of youth. Currently, cannabis education suitable for school-aged children is scarce, and accessible public awareness campaigns remain limited or overemphasize the potential harms (Watson et al., 2019). There is also little cannabis education incorporated into current primary and secondary school health curricula, and educators have expressed feeling ill-prepared to deliver the content or constrained by time (Hout et al., 2012; Johnson et al., 2008). The Drug Abuse Resistance Education (D.A.R.E.) program has been implemented in schools across the United States and Canada since the 1980s and is an example of a program that places an emphasis on the harms of drugs and employs an abstinence approach (D.A.R.E. America, 2021). The D.A.R.E. program has been deemed effective for some youth; however, long-lasting improved educational outcomes and influence on future behavior change remain small with a decline over time (Cohen, 2005; Pan & Bai, 2009; Tremblay et al., 2020).
The Canadian Students for Sensible Drug Policy (CSSDP) developed a realistic and evidence-based cannabis toolkit to help guide parents and educators in having informed and non-judgmental conversations with youth and supports the lower-risk cannabis use guidelines (Canadian Students for Sensible Drug Policy, 2018; Fischer et al., 2022). Harm reduction programs have also been created including community programs such as the Youth Cannabis Awareness Program (YMCA, 2021) and a film-based program titled Cycles (UBC School of Nursing, 2018). Despite their open availability, there is inequity in school cannabis prevention programs with only 50% of students in grades 7 to 12 having reported receipt of cannabis education (Mammen et al., 2017) and only 1 Canadian high school out of 88 reported offering cannabis education (Zuckermann et al., 2020b). Despite a lack education, 78% of Canadian youth were aware of cannabis-related physical impairment and one-third reported previous exposure to public health messaging (Leos-Toro et al., 2020).
Social-Ecological Model of Health Literacy
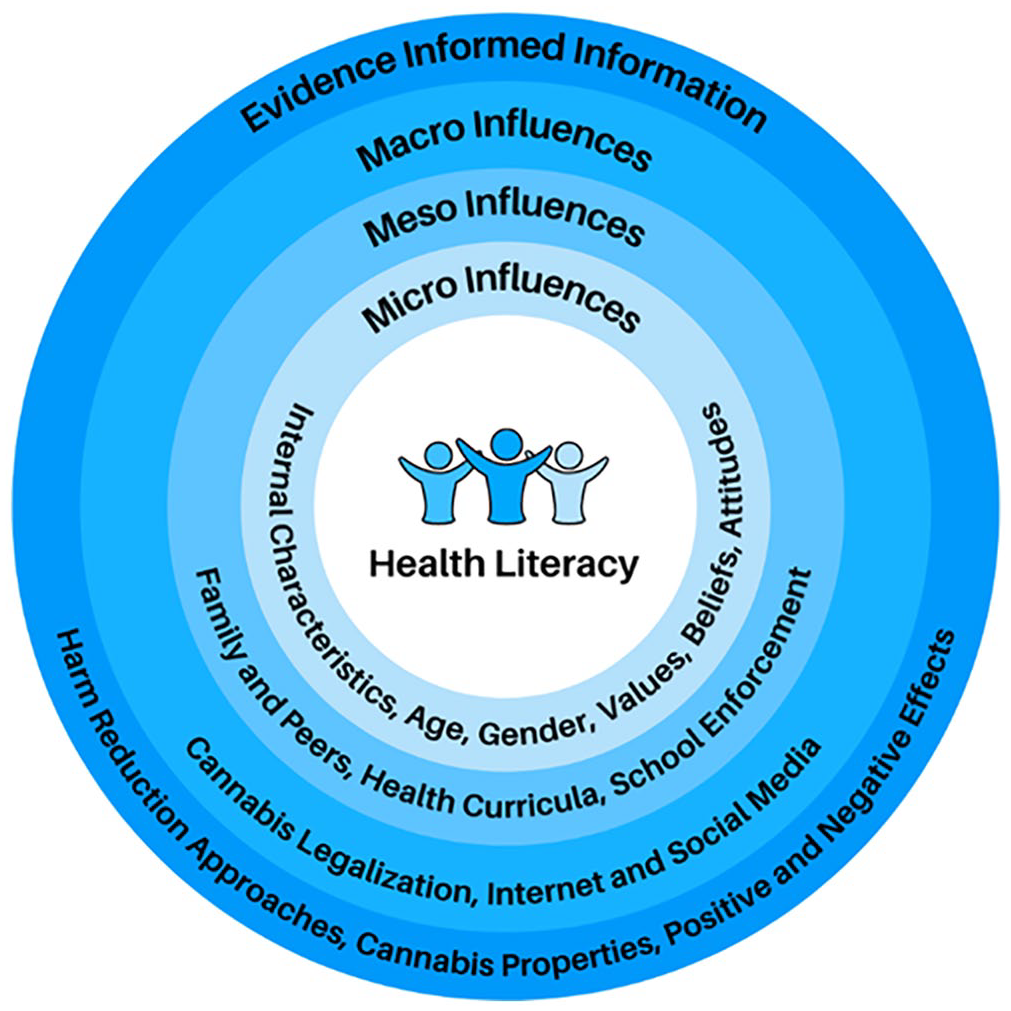
When considering the cannabis health literacy needs of youth, the Higgins et al. (2009) social-ecological model of adolescent health literacy in classroom health education is relevant. This framework acknowledges the role and interactions between intrapersonal, interpersonal, social, and community factors to support health promotion among youth across macro, meso, and micro contexts (Figure 1). Although this framework was used in the context of a healthy living course, enhancing our understanding of the factors that influence cannabis health literacy can help support the development of youth cannabis education.
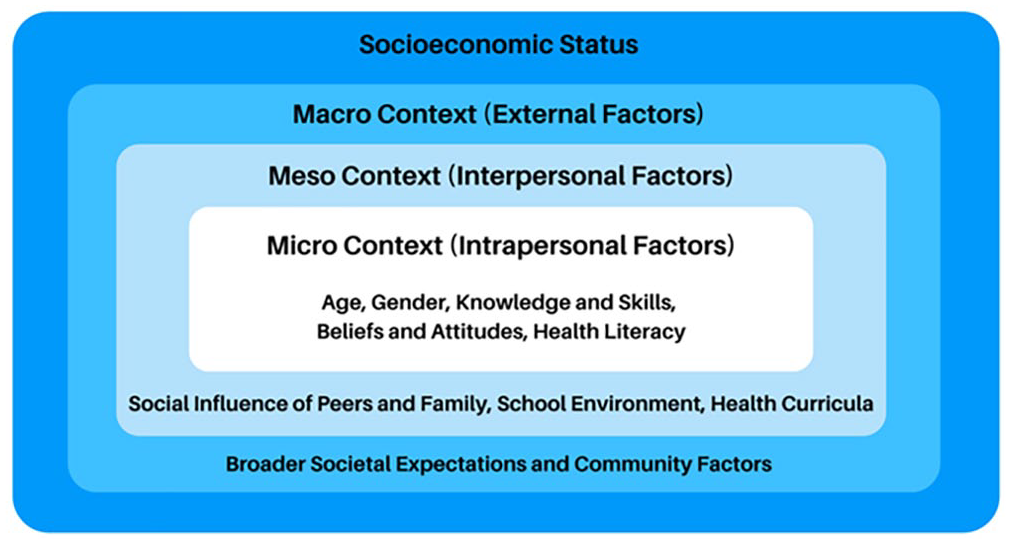
Summary of Higgins et al. (2009) social-ecological model of adolescent health literacy.
The Present Study
Our Cannabis Health Evaluation and Research Partnership (CHERP) in Newfoundland and Labrador (NL), Canada strives to examine how cannabis legalization has affected Canada’s health and public safety by evaluating related policies, cannabis behaviors, and educational campaigns. Our team conducted a needs assessment with the public and stakeholders where we identified that youth cannabis consumption is concerning and there is a gap in cannabis health literacy for youth (Donnan et al., 2021). As a result, we have made it a priority to engage with youth across our province to identify factors that affect their cannabis health literacy. The purpose of this qualitative research was to explore NL youths’ perceptions of their cannabis health literacy and future educational needs. Using the social-ecological model for adolescent health literacy, we sought to provide support and extend the application of the model for youth cannabis health literacy (Higgins et al., 2009).
Methods
Study Design
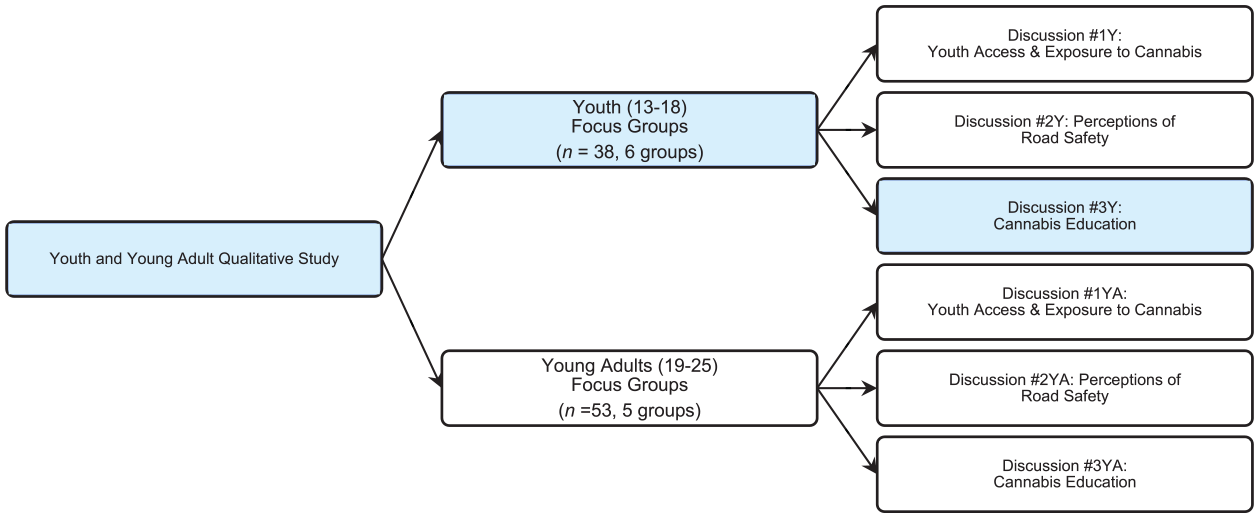
We conducted a qualitative study with youth with the goal to better understand the perspectives of youth about their cannabis health literacy. This was part of a larger study that explored youth and young adult’s perceptions about cannabis access, road safety, and health literacy (Figure 2). Focus group (FG) discussions were conducted using a semi-structured interview format between May and June 2021 (Figure 3). Each FG was scheduled for 2 hours (broken into three discussion topics) with a maximum capacity of 14 participants, permitting breakout rooms of 3 to 7 participants to focus on each discussion topic. Our findings reported herein only pertain to relevant discussions about cannabis health literacy. The objectives of our research on cannabis health literacy were to gain a better understanding of where youth obtain cannabis education, their current cannabis health literacy, their gaps in education, and their insights on effective modalities for the delivery of cannabis education. Ethics approval was received from the Interdisciplinary Committee on Ethics in Human Research (ICEHR #20211278).
Focus group facilitation flowchart.
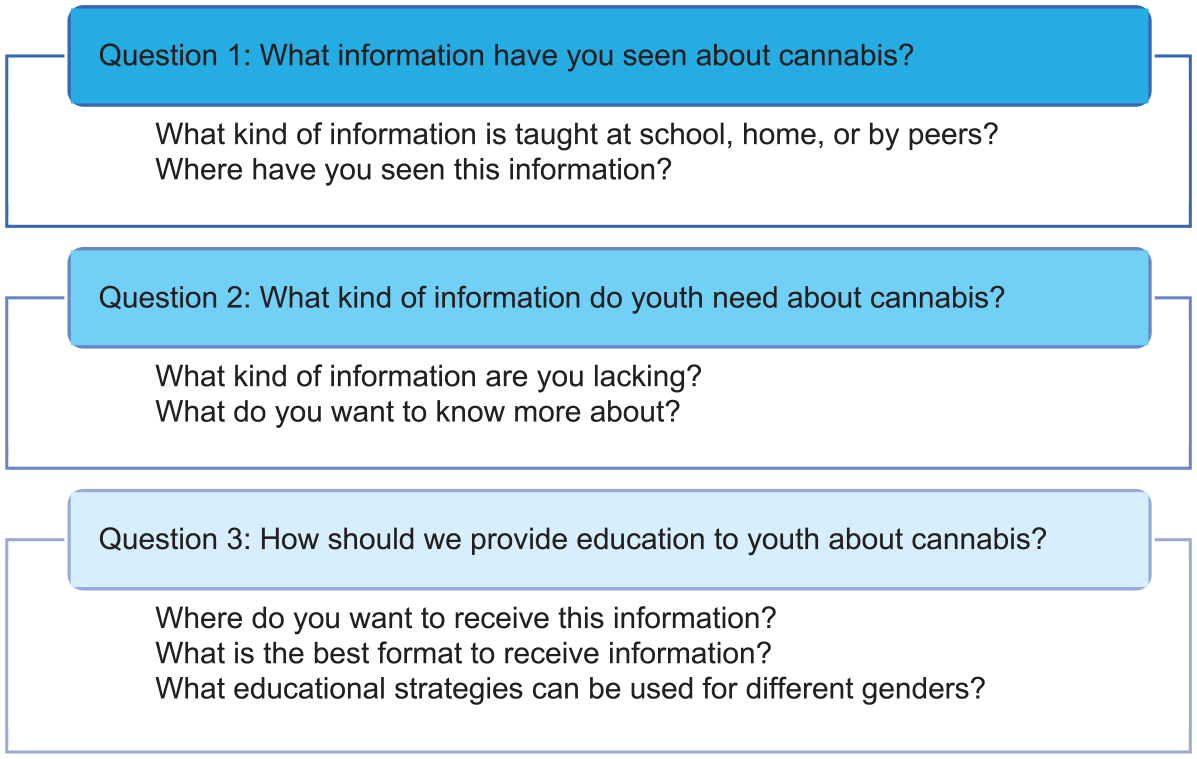
Semi-structured interview questions and probes for cannabis education discussion.
Participants and Recruitment
A convenience sample of youth was recruited using targeted recruitment efforts to gather perspectives across a variety of demographics with respect to age, gender, and size of residential communities (e.g., urban vs. rural) in NL. Urban communities represented the two largest cities in the province and were classified as those with population sizes greater than 30,000 residents, towns with 5,000 to 30,000 residents were categorized as larger rural communities, and those belonging to smaller rural communities were represented by towns with fewer than 5,000 residents. Strategies were not specifically tailored to recruit from Indigenous communities or recent immigrants.
A mixture of recruitment modalities included (a) correspondence with community youth networks (provincially funded independent youth programs), (b) promotion through local government, (c) posts on social media (e.g., Facebook, Twitter, Instagram, and Snapchat), (d) sharing via our citizen and stakeholder panels, and (e) snowball sampling through youth as well as parents. Interested youth connected with our team via email for further information and to register for a FG session. Youth were included if they were English speaking, lived in NL, were between the ages of 13 and 18, and were willing to participate in a 2-hour discussion. Prior experience with cannabis consumption was not required for eligibility. All prospective participants and their guardians were provided with an information letter prior to providing informed verbal consent. Participants were provided with a $50 gift card as a token of our gratitude.
Data Collection
Prior to participation, participants completed a brief demographic survey. FGs were hosted on Zoom to enable a wider representation of participants and encourage a lively discussion. They were facilitated by young adults from different genders and cultural backgrounds to help make the participants more comfortable. All facilitators were also trainees in health-related disciplines (e.g., psychology, pharmacy, and epidemiology). Questions were shared in the chat forum and responses were read aloud for those who felt more comfortable responding in writing. All FG were audio-recorded, de-identified, transcribed using NVivo, and verified by E.C.R. or D.H.D. prior to analysis.
Thematic Analysis
An inductive thematic analysis approach, informed by the social-ecological model of adolescent health literacy (Higgins et al., 2009), was utilized to code themes presented across the transcripts. This model (Higgins et al., 2009) was applicable to the context of the present study as it acknowledges there are influences across multiple contexts that are bidirectional in nature, which is also true for cannabis health literacy. The micro context considers youths’ knowledge, skills, and attitudes related to cannabis complemented with their ability to access, understand, and assess their own health literacy in the context of internal factors (e.g., age, gender, beliefs, and experience). Whereas the meso context recognizes the role of health educational curricula, teaching approaches, and the role that external social influences may have on youth (e.g., family, friends, and peers).
The model further allows for the recognition of the role of social-ecological factors present within macro contexts and their impact on youths’ ability to refine their cannabis health literacy (e.g., government policies, social media, and socioeconomic factors). Therefore, it is important that a holistic consideration of the social-ecological influences across contexts is considered when examining cannabis health literacy to account for health determining factors that may hinder or promote healthy behaviors, access to social supports, and improved educational outcomes such as increased coping skills to mitigate risk for early cannabis initiation or frequent consumption.
NVivo software was utilized for the coding of themes, organization, and storage of the data. D.H.D. and E.C.R. independently analyzed two transcripts for reliability and consistency of coding identified themes in the transcripts, and they each then coded the remaining transcripts utilizing an inductive line-by-line approach. The coders, in consultation with other team members, developed a codebook with continual revision to incorporate newly identified themes in relation to micro, meso, and macro contexts until no new themes were uncovered. Efforts to increase credibility were made by having D.H.D. and E.C.R. cross-reference their coding alongside co-authors’ review of the thematic coding to ensure the classification of themes was reliable across transcripts and coders. As knowledge about cannabis health literacy is scarce, an inductive approach was used alongside a constant comparison to explore relationships between and across thematic codes between coders to ensure consistency. Disagreements were discussed between coders and team members until a consensus was reached.
Results
Sample Characteristics
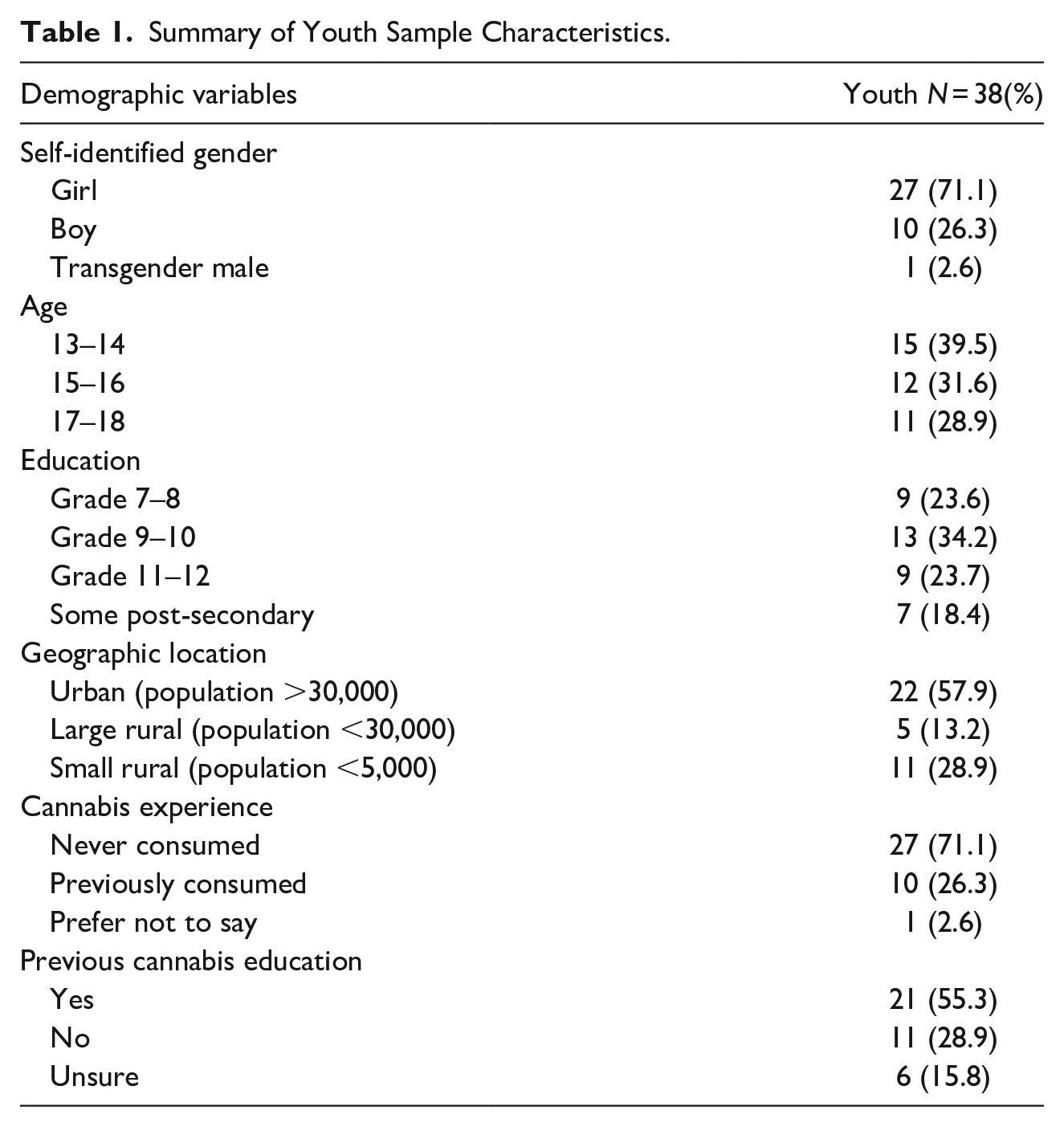
A total of 38 youth participated in six different FGs. Youth predominantly self-identified as girls (71%), with one transgender (TG) male representative. They were, on average, 15 (SD = 8.1) years old. Youth living across NL in urban communities (58%), small rural towns (29%), and large rural (13%) communities were represented. The majority (71%) reported having never consumed cannabis. Fifty-five percent noted that they had previously received some cannabis education (Table 1).
Summary of Youth Sample Characteristics.
Cannabis Health Literacy Themes
The health literacy FG discussions were on average 27 minutes (SD 7.2), ranging from 20 to 37 minutes. Four main themes complementary to Higgins et al. (2009) social-ecological model of adolescent health literacy emerged: (1) micro influences, (2) meso influences, (3) macro influences, and (4) evidence-informed information (Figure 4). Some quotes have been edited for clarity. Participants’ self-reported gender identities are noted throughout.
Emerging cannabis health literacy themes and sub-themes.
Theme 1: Micro Influences
Youth across FGs highlighted that their drug education was incongruent with a variety of youths’ intrapersonal factors and their ability to access, comprehend, and apply new knowledge. The two sub-themes aligned within the micro context, including (i) internal characteristics and (ii) values, beliefs, and attitudes.
Internal characteristics
The intrapersonal factors relating to age and gender appeared to influence their health literacy. As one youth noted, an earlier introduction to cannabis education can have a lasting impact:
I think (cannabis education should be delivered) at a young age because I think it sticks with you more and sticks with you longer. Anything that I learned when a younger age sticks with because it was mainly how you were taught and raised (Rural Girl 18).
Some noted that although they received education at an early age, they could not recall what they had learned, “I don’t remember ever even getting the D.A.R.E. program and I don’t know what we were taught” (Rural Girl 22). Designing a program that aligned with the age and life experiences of the youth and building on this content was felt to be important. As one youth commented,
I think as you move on to grade 10, I think that (education) would be more about the effects of driving because that is when people are getting their driver’s license. If it built on every year from junior high to grade 10, and more about the effects in general than the dangers (Urban Boy 13).
Some expressed the need to consider different experiences depending on one’s gender identity. One participant noted the different approaches to learning between girls and boys: “I know the guys in my school think they know everything, but the girls would try to listen to them and get as much out of it as they can” (Rural Girl 22). Some also suggested that education that is physically engaging is more effective for boys, while girls are more open to a variety of approaches. As a youth noted,
I think men learn better with interactive types of things because personally, from my observations, the boys tend to be more reckless around the fact of learning. They’ll often skip off on the worksheets to fool around with their buddies instead of really focusing. I think girls will probably be fine with pretty much anything depending on their mindset (Rural Girl 27).
Gender differences were also noted when viewing content on social media. One youth discussed how boys only watch the content, while girls pay more attention to the influencers,
For influencers, I think it would be more effective with girls than boys because we (boys) just want to see the content, nothing about sponsorships (for the content) as I don’t watch that. I just skip that. I don’t care and watch the content, but girls pay attention more to influencers (Urban Boy 59).
One participant also shared that in the small rural community in which they resided, there was a noticeable difference in the discussion about cannabis based on gender.
Speaking for my region in particular, I’ve noticed that [. . .] the girls brag about it more and they always have very loud conversations [saying] ‘oh, I got high in the bushes yesterday’. The boys, they do it [but] they don’t really talk about it (Rural Girl 70).
Values, beliefs, and experience
Youth emphasized the importance of considering their values, beliefs, and experiences. Many were not receptive to deterrence approaches to drug education as it did not align with their values. One youth expressed their concern about promoting abstinence, fearing that it may lead to greater consumption: “I guess it is really strict with ‘don’t do it’ and the more authoritative, the more likely that youth will do it behind their back or keep it as a secret” (Urban Boy 13). Many referred to the D.A.R.E program when sharing examples of past substance use conversations, suggesting that a scare tactic approach failed to align with youths’ beliefs. As one youth expressed:
I think one thing we’ve learned from drug education all these years with the D.A.R.E. program is that scare tactics don’t work on us (youth) very well and honestly it should be more focused on being responsible than anything (Urban Girl 60).
As another participant expressed, the beliefs of adolescents are also bound to change over time as they learn more or gain experience with cannabis:
There is research out there, but its not being pushed on people and youth aren’t going to be reading research articles. . . When I was in junior high, I really, honestly, believed when people told me that the juice in a vape was water and it was water vapor. I didn’t think it had an effect until I grew older, I started to learn more people were being affected by vaping (Urban Girl 24).
Moreover, youth discussed how they value education more when it is presented in a manner consistent with their lived experiences or someone who can genuinely relate to them. As one youth shared: “I definitely think people closer to our age because when its people are older, even if they try to kind of keep up, they still sound outdated and then that just turns into a joke” (Urban Girl 6).
Theme 2: Meso Influences
Many youths discussed several interpersonal and school influences that had an impact on their cannabis health literacy. These factors are related to the meso and macro contexts with the inclusion of the influence of (i) family and peers, (ii) health curricula, and (iii) school enforcement. In particular, youth openly shared the modalities they were most receptive to and the elements that were important for incorporation into health curricula.
Family and peers
It was discussed by many that increasing their cannabis knowledge was dependent on their own initiative to seek more information, with little information coming from family and peers and minimal guidance coming from school. As one youth stated, “Everything I’ve learned about cannabis was from my friends or me searching or my parents. I’ve never ever learned anything from school, which is kind of sad” (Urban Girl 25). Attempts by caregivers to discuss cannabis were noted as a rare conversation at home. As this youth shared: “I’ve never actually had the conversation (about cannabis) with my parents. It’s mostly when I’m going to high school parties when they will say not to get on the ‘wacky bandwagon’” (Rural Transgender Male 64).
In other homes, the primary focus often involved advisement of the punishment that would follow should parents learn of their consumption. This often promoted the need for youth to conceal their consumption, as this youth discussed:
I don’t think we’re overly taught about it at home. . . it is more about the consequences if they found out you’re doing it. It also causes a lot more youth to hide the fact they are doing it so it’s not as educational as it is more a fear of getting punished (Rural Girl 27).
On one hand, youth indicated that they often learn the most about cannabis through casual discussion with older peers, stemming from their lived experiences, as expressed by one youth: “it is more from the firsthand experiences of friends that I’ve gotten any knowledge of it or seeing it done at parties” (Rural Transgender Male 64). However, many noted that the information learned from peers was often vague and presented in a positive or neutral manner. This youth also mentioned that they hear about cannabis in the hallways at school: “That is where I learned a lot of it, and you can hear just in the hallways at school” (Rural Transgender Male 64).
Health curricula
Youth expressed many of their concerns about their current health education on illicit substances and discussed a variety of recommendations for inclusion in future health curricula for in-school delivery. Most noted that discussion about cannabis-related topics at school often involved the use of a scare tactic in message delivery, which they felt was not effective. As shared by this youth, they were informed that consumption of cannabis may result in the development of psychiatric disorders:
Honestly, what they teach you in school is that if you do weed you will end up like this one person in the documentary who had a family history of mental disorders and ended up getting schizophrenia and dying. Which isn’t really happening the vast majority of the time and scare tactics don’t really work well on kids (Urban Girl 60).
As discussed by some, receptibility to furthering their learning about cannabis also depends upon the priority that youth place on actively engaging in their own education. As such, incorporating cannabis education into the school curriculum may inspire some apprehensive youth to become more engaged in the content being taught. As this youth suggested,
Everybody is in school and it forces everybody to listen even people that are like ‘oh this is stupid, I don’t want to do this.’ If you’re in school and it is a part of your mark or something important, you’re going to want to do it. I think social media is a really good platform to use to try to give education but I don’t feel that a lot of youth would get reached by it or be intrigued enough to go looking for it if it’s not right in front of their faces (Rural Girl 27).
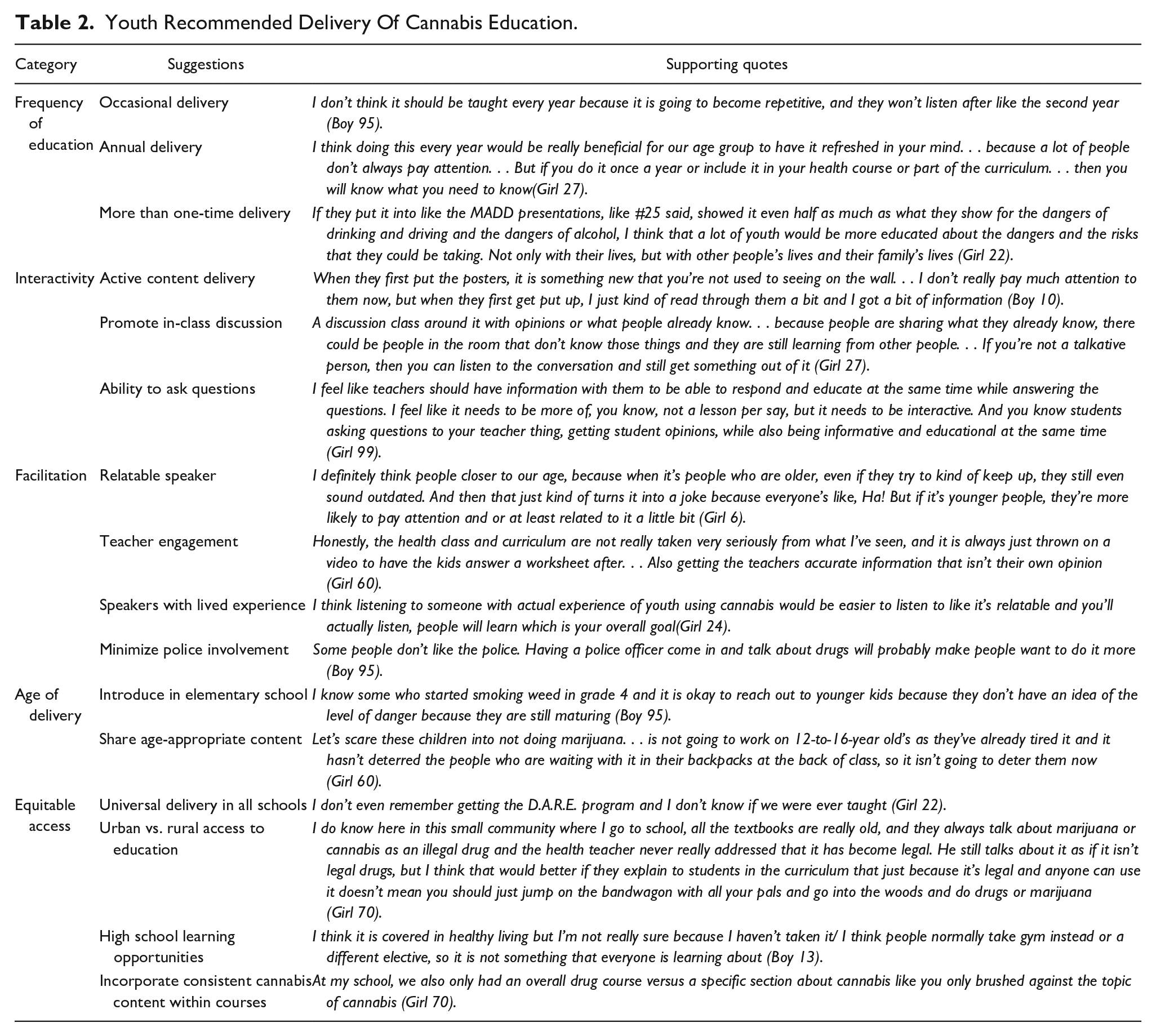
Youth provided many useful suggestions about the delivery of in-school health curricula. There was variation in how frequently the education should occur, as some felt that it shouldn’t be repeated every year, while others felt that the repetition was beneficial. However, it was evident that more than a one-time delivery was important. They noted that interactive sessions were more engaging, as it provided an opportunity to ask questions and share opinions. There were also mixed feelings regarding who was best to facilitate the sessions. Many discussed having people closer to their age or with lived experience would be more engaging. However, if it was delivered by teachers, they should be informed and present facts and not opinions. Although police officers deliver D.A.R.E. in some schools, there was concern that not all youth have a good rapport with police, which may have a detrimental impact on their willingness or comfort in attending police-delivered education. In terms of when to start education, starting in elementary school before first exposure to cannabis was suggested as some observed consumption as early as grades 3 or 4. Delivering age-appropriate content at the various grade-levels was emphasized. Moreover, providing universal cannabis education across schools and within similar courses was highlighted to ensure equitable access to education. Quotes to support these suggestions are noted in Table 2.
Youth Recommended Delivery Of Cannabis Education.
School enforcement
Youth also discussed how it was difficult for cannabis to be taken seriously when enforcement on school property was not a priority. As one participant shared, a greater concern was sometimes allocated to other types of behaviors than cannabis consumption during school:
People just got suspended because someone got in a fistfight in the park like a 10-minute walk from the school but people are going behind the school barely off school property, getting stoned, and coming back to class. They don’t get in trouble but the two kids in a random fight did (Urban Girl 60).
Moreover, concern for the lack of action taken in the classroom when students were visibly under the influence of cannabis or an illicit substance leaves the potential for mixed messages to be sent to youth. As this youth noted:
I’ve seen so many people just come to class (high) and teachers either ignore it or don’t notice it. . . In eighth grade, for a month or so someone had very strong or tainted edibles and people would come to class full on hallucinating and then be sick so bad they had to close the gym because a student puked all over the floor and teachers just didn’t notice. The girl was straight up imagining a massive hole in the ceiling and we’re all like ‘okay you shouldn’t be here’ and the teacher was like ‘okay, why don’t we just continue on with science class’ completely oblivious to it, it was absurd (Urban Girl 60).
Similarly, youth expressed concern about the frequency of cannabis consumption in school bathrooms and the impact on all of those in the building. As mentioned by one youth, “It’s happened in my school bathroom. We have an issue of where you can smell it through the school coming from certain bathrooms” (Rural Transgender Male 64).
Theme 3: Macro Influences
Participants placed an emphasis on the impact of community factors from their surrounding macro environments that hinder or support their health literacy. The environmental influences most commonly discussed were the impact of (i) cannabis legalization and (ii) internet and social media.
Cannabis legalization
The legalization of cannabis was also discussed as a contributing factor to how normalized cannabis consumption and related behaviors have been integrated into modern society. One youth compared the difference in their perceptions between pre- and post-legalization:
If you were to ask me that question, like three years ago, I would say [that] I would be afraid of marijuana. I would have a bias against people that smoked it or however they chose to use it, that anyone who did do cannabis was a skeet or were not up to good things. But nowadays, I don’t know if that came with age or if it came with the legalization or normalizing the fact that more people smoke weed. I think [now]that it’s a lot more normalized. I wouldn’t classify anyone that uses marijuana as a skeet or going nowhere. I would just think it’s like such a normal thing nowadays (Urban Girl 24).
Youth also spoke to how the normalization of cannabis consumption has also been illustrated in their personal observations of how often teachers may be unaware that students are under the influence as it’s a common occurrence. As shared by another youth:
There’s a lot of people at my school that go behind the school and smoke a bong or smoke a joint, and they just come into the school to write a test and go on with their day. The teachers have no idea that they’re high because they’re just high all the time (Rural Girl 22).
Internet and social media
Greater acquisition of knowledge about cannabis was obtained through social media or on the Internet. This youth discussed learning from friends on social media: “You hear and see a lot on Snapchat stories where people are just talking about it (cannabis) or the different kinds and stories where they share”(Rural Transgender Male 64).
Youth mentioned it was common for information to be presented neutrally by sharing both the negative and positive effects of cannabis. However, some youth expressed the need for more detailed information on cannabis and faced difficulty locating additional resources.
I think I’ve gotten more education on what’s in weed and the different kinds of it on Tik Tok, which sounds so crazy that it’s more than I ever have from school. . . The internet is definitely where you go like Facebook, Twitter, Instagram, Tik Tok, and even Snapchat, you always see different articles or things about cannabis. It is very prominent on the Internet and its stuff that is never talked about through school (Urban Girl 99).
The use of social media as an alternative vehicle to educate youth was indicated as the most popular avenue to target youth outside of the classroom. They noted that information posted on social media has the potential to reach many youth, but it is essential that the content aligns with current social media trends and be short in duration. As explained by one youth:
It would be a pretty effective method of getting the information across because if its keeping with the trends it would be more interesting to people than just a boring documentary style thing. Having the information be more entertaining and eye catching to the demographic will be more effective (Urban Boy 10).
Tik Tok was the most commonly recommended platform to share content related to cannabis online. As this youth discussed:
On Tik Tok, there is a lot of people like doctors that tell me what to do and what not to do but they also keep it in with the trend so that people around our age group actually watch it and not just click off right away” (Rural Girl 19).
Theme 4: Evidence-Informed Information
An emerging theme in our research that was an extension beyond the Higgins et al. (2009) model focused on the need for greater empirically informed cannabis knowledge. As one youth shared, there is often a delay in sharing up-to-date information and were hopeful to receive more current education in the future, which was especially true in their rural location:
I do know in this smallish community where I go to school, all of the textbooks are really old and still include marijuana or cannabis as an illegal drug and the health teacher never really addressed that it has become legal. . . It would be better if they explain to students that just because it is legal and anyone can use it, doesn’t mean you should jump on the bandwagon with all your pals (Rural Girl 70).
There was a consistent recommendation for prioritization of content on (i) harm reduction approaches, (ii) cannabis properties, and (iii) positive and negative effects, as described below and in Figure 5.
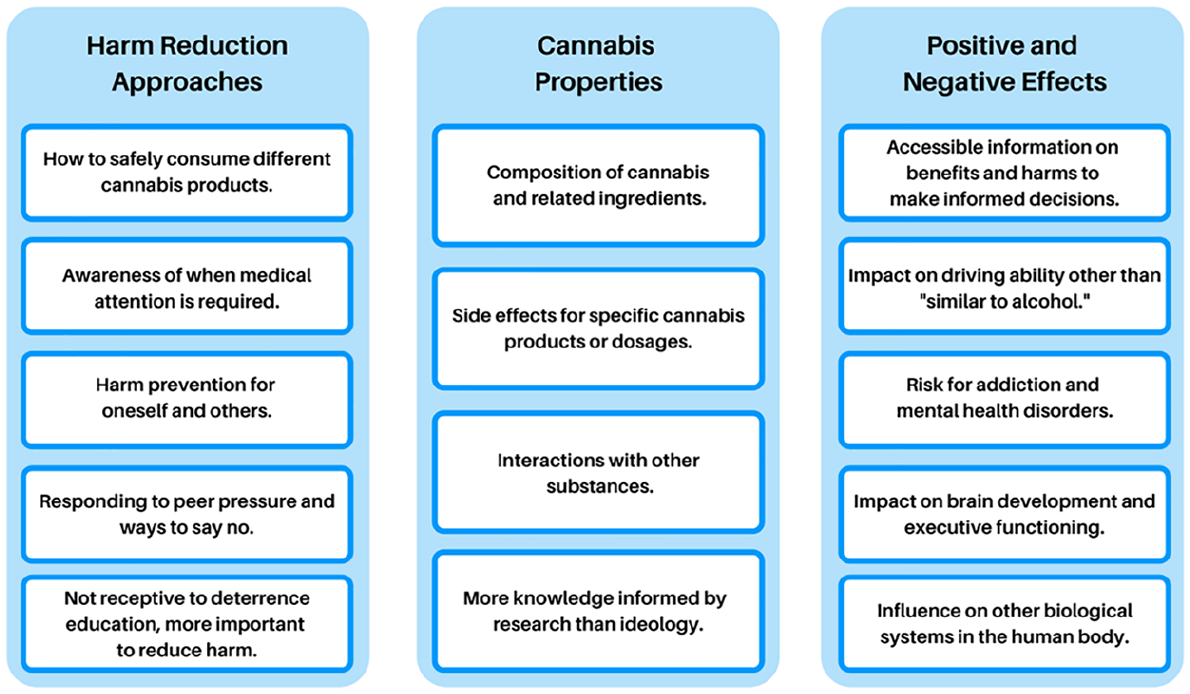
Youth desired health literacy.
Harm reduction approaches
A strong sentiment was the need to learn how to safely prevent harm to oneself or others using a harm reduction approach. As one youth shared, youth are going to experiment, but they need to be informed about how to handle situations where their peers or themselves may be experiencing adverse effects:
You know they are going to do it anyways then you see people getting sick or hurt or drugged smoking something because we don’t know what’s in it. They never know how to handle the situation because it’s something that we were never educated on. We’re all just told not to do it (Urban Girl 99).
It was explicitly stated that youth were not receptive when deterrence from consumption was the primary focus. Instead, youth preferred to learn how to reduce the harms of cannabis consumption, as noted by this youth: “If you were taught or shown the difference between safe weed and weed that’s been laced that could probably save some people’s lives” (Rural Girl 22).
Participants also shared the importance of learning that cannabis consumption can have a secondary impact on others. As shared by one youth “Maybe how it affects others too. I was thinking if your friends use it, that it could affect you or if someone were using and driving that it could affect someone” (Rural Girl 88).
Cannabis properties
Several participants noted the lack of reliable youth-friendly information on cannabis. Many commented that they do not know much about cannabis and the impact it can have on youth. There were several aspects about the properties of cannabis that they indicated they would like to know, including: “different uses and ways people use weed” (Urban Girl 9), “how to use it and how much you should” (Urban Boy 10), “how long lasting are the effects and what amounts are safe to use” (Rural Girl 2). The desire for reliable information was also evident when this youth shared their frustrations with respect to failed attempts to find useful resources:
I was really curious about the side effects of cannabis vape or oil pens. . . . I actually had a really hard time finding anything at all and I know it’s new with not much research done on it (Urban Girl 25).
Positive and negative effects
Youth were keen to learn about both the positive effects and potential harms associated with cannabis so they could make informed decisions on whether to engage in cannabis-related behaviors. Many held the belief that there was minimal harm due to its natural properties. As one youth expressed:
I think a factor is that it’s natural and a grown plant like shrooms. I haven’t seen any long-term effects of shrooms either and I feel like since people just say ‘it’s a plant’ that it won’t hurt you.” (Urban Girl 25).
It was noted that driving risks associated with cannabis are often advertised, but there was a lack of information about other risks, “I feel that more of the risks should be advertised because the main one that is talked about is driving under the influence, but a lot of people don’t understand the rest of the side effects” (Urban Girl 5). However, several youths also discussed the need to provide evidence-based information about how cannabis affects driving ability. As one participant openly stated in conversation, “Yeah, (education) like besides just the basic stuff saying, ‘it’s dangerous.’ I don’t really know how cannabis effects you on the wheel” (Urban Boy 10).
There also appeared to be confusion between the benefits of medical cannabis and the harms advertised with non-medical consumption. One youth mentioned that when they were learning about cannabis, they were told that “it is bad but has a medical purpose” (Rural Transgender Male 64), which was confusing. It was suggested that education in schools should bring more clarity with respect to the associated harms of cannabis and be cautious of the comparisons to nicotine, as shared by a youth:
We are always told ‘smoking [weed] is safer than drinking’ and ‘smoking weed is safer than smoking nicotine because it’s not addictive.’ When I was younger, I heard this, and I always believed it was according to some evidence to back it up but it wasn’t until I came into high school that a lot of my past friends from junior high all smoked. You know, people saying smoking (cannabis) isn’t addictive, but they smoke every day to the point where smoking weed wouldn’t get them high enough anymore that they went to the next drug and the next (Urban Girl 99).
Many youths wished to learn about the effects cannabis has on mental health, including anxiety and depression. For instance, this participant noted:
The only thing I’ve really ever seen about the long-term effects of cannabis is that if you use it a lot for extended periods, that it can have a toll on your mental health or it could increase depression or anxiety but even that is not taught in school (Rural Girl 22).
Discussion
Grounded in the social-ecological model for understanding adolescent health literacy (Higgins et al., 2009), we sought to gather insight from youth regarding their cannabis health literacy experiences and needs. It was apparent from our work that there are multifactorial influences on health literacy that align with Higgins et al. (2009) conceptual model and our novel discovery of the model’s application to cannabis health literacy. Overall, our findings suggested that youth’s individual factors, such as their age, gender, experiences, and beliefs, influenced their cannabis health literacy. Interpersonal influences also played a role, including minimal discussions or scare tactics at home, inconsistent or abstinence-based drug education at school, and unreliable information from peers. The youth expressed a need for evidence-informed cannabis education, early integration of related knowledge into the curriculum, and development of interactive programming in schools paired with additional reach via social media.
Noteworthy discovery was made when youth reported that drug education was not universally experienced by students across the province and further represents equity concerns within the meso context (Higgins et al., 2009). Some youth reported participation in the D.A.R.E. program in grade 6, where a police officer educated students on how to refrain from the consumption of illicit substances and to resist peer pressure (D.A.R.E. America, 2021). Secondary school courses were elective and only experienced by some students, further increasing the number of youths who were not exposed to cannabis education. These findings parallel previous observations in Ontario where only 50% of students in grades 7 to 12 reported having received any cannabis education (Mammen et al., 2017). Moffat et al. (2017) also noted that cannabis consumption was often absent from school drug education programs in Canada. This is particularly concerning given the post-legalization environment in Canada, and the tendency for adolescents to consume cannabis as it is often utilized as a coping mechanism for psychological and emotional needs (Hall, 2020).
Many of the youth in our study were not receptive to the ongoing use of deterrence strategies employed at home and in school as connected to broader societal expectations across macro contexts (Higgins et al., 2009). While the D.A.R.E. program may offer short-term benefits by eliciting anti-drug attitudes, meta-analyses on the efficacy of the program consistently report minimal to no impact of the program on drug use and psychosocial behaviors (Ennett et al., 1994; Pan & Bai, 2009; Tremblay et al., 2020; West & O’Neal, 2004) and when a small effect has been found it is believed to diminish over time (Cohen, 2005). D.A.R.E. has since launched a new prevention program, the Keepin’ it REAL curriculum, with an emphasis on academic knowledge and emotional awareness; however, limited evaluations have been conducted to assess the impact of the program on drug-related behaviors (Caputi & McLellan, 2017).
The inherent harm of an abstinence approach is that it fails to consider the variability in youths’ experience or intent to consume cannabis (Watson et al., 2019). A more effective strategy places less emphasis on the risks and fosters an environment where non-judgmental conversations can be used to support cannabis-related decision-making (Hyshka, 2013; Valleriani et al., 2018). Promotion of health-conscious cannabis consumption as informed by the low-risk cannabis use guidelines (Fischer et al., 2022) can be emphasized further with the implementation of the (Public Health Agency of Canada, 2021) Blueprint for Action framework through: neutral in-classroom discussion, sharing research that aligns with stated claims, and fostering a safe space for youth to equitably access harm reduction resources (Public Health Agency of Canada, 2021). As such, the youth in our study felt it was imperative they are provided with balanced information on the benefits and risks, with an emphasis on harm reduction strategies.
Youth in our study pointed out that regardless of the education provided, many will decide to consume cannabis due to their own beliefs and consideration of intrapersonal factors within the micro context (Higgins et al., 2009). Evidence suggests that some of the most well-intended programs tasked with reducing consumption can actually elicit more harm by inadvertently motivating youth to consume drugs (Allara et al., 2015; Werb et al., 2011). The desire for the promotion of safe consumption practices over abstinence may be achieved by an approach that facilitates authentic conversation between students and facilitators or mentors (Watson et al., 2019). A meta-analysis conducted by Porath-Waller et al. (2010) examined the effectiveness of school-based programs and determined that the greatest efficacy was achieved by those blending prevention models through interactive delivery, using outside facilitators. The key component in this approach is to eliminate or minimize the power dynamic. Youth are particularly responsive when their insight is valued and when the harms align with their lived experiences so clear connections can be drawn between content with reality (Moffat et al., 2017).
Given the observation by youth in our study of children in grades 3 or 4 consuming cannabis, they felt that cannabis education was an important topic worthy of early integration into the school curriculum. Previous research identified that nearly 30% of youth began consuming cannabis before 14 years old, with early initiation predicted by the presentation of mental health concerns, participation in crime or violence, and experience of past trauma (Hawke et al., 2020). Future examination of contributory factors to an earlier age of initiation can help determine what other social supports or education may be beneficial to serve as protective factors across a multitude of meso (e.g., supported by health curricula or school environment) and macro contexts (e.g., environment of surrounding communities; Higgins et al., 2009). In parallel to the early introduction of education, the youth in our study suggested that cannabis education should be age-appropriate and should build on their skills. This approach has been shown to be of benefit to opioid education where programs facilitating youth development in a manner that aligns with the stages of adolescent development have reduced the frequency of prescription misuse (Spoth et al., 2013). Moreover, programs that provided opportunities to refine social skills (Velasco et al., 2017), build relationships with community organizations (Compton et al., 2019), or participate in a single motivational interviewing session led to reduced substance use (Jensen et al., 2011).
It was impressive that the youth desired empirically informed content about cannabis to help inform their decision-making, indicating a promising potential for behavior change with the presentation of accurate information. Significant development of the frontal lobe and limbic system occurs during adolescence, so youth are more likely to engage in risky behavior and impulsive decision-making (Williams, 2020). Equipping youth with knowledge about cannabis will help provide them with the information to make informed decisions, which has the potential to change cannabis consumption motives and behaviors even with infrequent exposure to cannabis education or follow-up (e.g., reduced motivation and cannabis use has been observed with as little as three sessions with a health educator; Blevins et al., 2016).
Effective health literacy must go beyond classroom education and consider the wider community and social influences across micro, meso, and macro contexts (Higgins et al., 2009). Although Higgins et al. (2009) social-ecological model of adolescent health literacy did not include social media within their framework, social media has now become one of the most modes of communication and access to information in modern society. Social media is an accessible and cost-effective avenue to disseminate cannabis education with a wide reach amongst youth. Previous research has reported high social media use among adolescents aged 8 to 18 spending, on average, 7.5 hours a day on screens across all sources, including television, social media, and video games (Centre for Disease Control and Prevention, 2018). The youth in our study suggested that it would help to disseminate cannabis education via social media, with a preference for Tik Tok due to the ease of viewing, entertaining content, promotion of authentic content, the ability to interact with others, and the short duration (Han, 2020). The potential for promoting health by enhancing cannabis health literacy using Tik Tok can be achieved in collaboration with youth-engaged influencers. This brings forth a new medium to connect with youth to allow for a greater reach and wider impact.
Limitations and Future Directions
There were some limitations to this research. One barrier arose as parental consent was required to permit participation, as required by our ethics board. Some youth may have been reluctant to ask the parent/guardian for consent for fear of them being questioned about their cannabis consumption. Data on self-identified ethnicity or belonging to specific ethnocultural communities were not collected in the demographics, therefore, consideration of cultural differences of those belonging to Indigenous or other historically excluded groups was not explored. The demographic questionnaire inquired about whether they received previous cannabis education, but the extent or form of education was not gathered. Given the age range of participants, some youth may have been too young to have received cannabis education, thus limiting the depth of their previous cannabis education.
The applicability of the findings of our research may be limited beyond NL but are transferable to other contexts involving youth and their related environments. It is recommended that future endeavors aim to explore youths’ perspectives from other provinces or countries so cross-cultural or regional differences can be considered within those contexts. Future research should examine the effectiveness of cannabis health literacy education in reducing the risk of cannabis-related harms to youth. As well, research should explore youth, parents, and educators’ receptiveness to using a harm-reduction approach for cannabis education. The impact of socioeconomic status on youths’ health literacy and the effectiveness of using social media as a means of educating youth warrant further investigation.
Conclusion
Using a social-ecological model for understanding cannabis health literacy, there are multifactorial influences on youths’ health literacy. Considering their intrapersonal, interpersonal, and community or societal influences is essential for providing an effective educational approach. Our findings highlight the shortfalls of current substance use education programs targeting youth and the gaps in knowledge that youth wish to have addressed. Using an evidence-informed harm reduction approach that is delivered in an engaging manner is essential in preparing youth to make informed decisions, thereby helping to protect their health and safety. This educational approach can be used to support the development of youth-centric cannabis health literacy programs applicable to school curricula and social media.
Footnotes
Acknowledgements
We would like to thank all the youth who participated in the study. A special thank you to our students Alicia Blackmore, Rita Huang, Joseph McGraw, Mitchell Preston, Sandi Schuhmacher, and Omar Shogan for their assistance with the facilitation of the focus groups. We would also like to express our thanks to our partners: Memorial University, Department of Health and Community Services of Newfoundland and Labrador and the Newfoundland & Labrador Centre for Health Information.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Interdisciplinary Committee on Ethics in Human Research at Memorial University of Newfoundland (ICEHR #20211278).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support for the conduct of the research from the Canadian Institutes of Health Research (Grant No. 201910CPV-429120) and the Canadian Centre of Substance Use and Addiction for the Partnerships for Cannabis Policy (Grant No. 201910CPV-429120) inclusive of this research.