
Abstract
Young people struggle to seek help for their mental health, despite having different resources available. As the coping process is very complex, and elements such as trust and availability of resources have been said to influence it, this study aimed to understand how young people cope with their own or a friend’s symptoms of poor mental health. Eleven young people (13–15 years old) were interviewed. Thematic Analysis of the interviews showed that participants reported different coping strategies for dealing with their own hypothetical symptoms and those of a friend. Participants identified the social impact of experiencing symptoms of poor mental health and choice of resources as the main factors influencing their coping strategies. For their own symptoms, young people expressed concern about being judged and that they would only disclose to someone they trust. Participants would not disclose a friend’s symptoms because they did not want to break their trust. Finally, choice of resources was mainly influenced by the severity of symptoms being experienced, especially when it comes to asking for professional help. This study contributes to a better understanding of the different ways in which young people cope with their own symptoms and symptoms experienced by a friend.
One in five adolescents experience symptoms of poor mental health, such as depression or anxiety (Deighton et al., 2018). A recent meta-analysis, showed that 41.5% of individuals experience their first symptoms by the age of 14 years old, irrespective of the mental illness diagnosis (Solmi et al., 2021). Despite this, young people still struggle to seek help when experiencing mental health difficulties (Collinson, 2017; Naughton et al., 2018). Lack of confidence about how to cope due to low mental health literacy (Hart et al., 2018; Mason et al., 2015) and social pressures (e.g., stigma) (Lannin et al., 2016; Schnyder et al., 2017) have been highlighted as negatively impacting how young people deal with these issues.
Young people who experience symptoms of poor mental health report higher levels of stress as a result (Auerbach et al., 2011; Moksnes et al., 2010). Adding to this, adults and mental health campaigns from different organizations such as Young Minds (UK), See Me (Scotland), and headspace (Australia) encourage young people to disclose their symptoms to others in order to get help. Young people often choose to disclose to a friend (Griffiths et al., 2011), mainly because they have a sense of comfort and higher levels of trust around their peers (Camara et al., 2017). However, most studies focus on how young people cope with their own symptoms of poor mental health and neglect to consider how a young person might react and deal with such a disclosure by a peer (Raviv et al., 2000; Rickwood et al., 2005; Yap et al., 2011b). Furthermore, research has not explored which possible factors might be playing a role in the coping strategies selected by young people when dealing with a friend’s symptoms of poor mental health when in comparison to their own symptoms. Gaining insight into what coping strategies are used by young people when dealing with a friend’s disclosure, could aid in implementation of provisions that facilitate help-seeking by young people.
Thus, this study aims to understand the differences in coping in young people when dealing with their own versus a friend’s symptoms of poor mental health. We utilized the Transactional Theory of Coping (Lazarus & Folkman, 1984) as a framework to understand how the coping process develops. This is very timely research as the restrictions caused by the current COVID-19 pandemic have created extra pressures on young people’s mental health (Dodson, 2020). Adolescent mental health has deteriorated throughout the pandemic (Creswell et al., 2021) and young people have experienced higher levels of stress as result (Singh et al., 2020). A better understanding of young people’s coping process can help us to provide appropriate support at this time.
The Transactional Theory of Coping (TTC)
Lazarus (1993) defined coping as a response to “ongoing cognitive and behavioural demands that are taxing or exceeding the resources of the person” (p. 237). The Transactional Theory of Coping (TTC) proposes that a multitude of factors play a role in the coping process, making it highly complex. Contributing to its complex nature, coping is constantly changing over time, and is both situation and person specific (Lazarus & Folkman, 1984). The TTC proposes that there are two main components in the coping process: cognitive appraisals and coping strategies. Figure 1 shows how these are proposed to interact in this study.

Transactional Theory of Coping (TTC).
According to the TTC, cognitive appraisals can be divided into primary and secondary appraisals. Primary appraisals correspond to the evaluation that the individual makes of the situation as (a) harmful, where there was harm or loss caused by the stressful situation; (b) threatening, where there is potential for physical or emotional harm to occur, and/or (c) challenging, where there is space for growth and mastery. These appraisals are not mutually exclusive, meaning that they can occur simultaneously, for example, when an appraisal of harm occurs it is likely to be preceded by an appraisal of threat (Lazarus, 1999).
Secondary appraisals are the evaluation a young person makes of the resources available to them and to what extent these can be harnessed to deal with the stressful event (Lazarus & Folkman, 1984). Despite their names, primary and secondary appraisals can occur simultaneously and influence each other (Frydenberg, 2019). For example, it is more likely that a young person will find an event threatening if they do not identify any available resource to help them. Overall, the appraisal process is where differences in coping may start to emerge as an individual assesses the situation, their skills, and resources in order to achieve an optimal outcome (i.e. overcome the stressful situation).
Once a situation has been appraised, the individual deals with the stress by implementing coping strategies. Two overarching categories of coping have been proposed: problem-focused coping (i.e., dealing with the cause of the distress) and emotion-focused coping (i.e., regulating the emotion resulting from the distress) (Lazarus & Folkman, 1984). As the aim of the present study is to understand differences in coping in young people when seeking help for their own symptoms of poor mental health or for a friend’s symptoms of poor mental health, these two overarching categories were used to bring to light possible differences between coping with one’s own and with a friend’s symptoms.
Coping With Symptoms of Poor Mental Health
Research with young people has associated negative appraisals (i.e., threat or harm), with negative life events (Cole et al., 2019; Fosco & Lydon-Staley, 2019), such as symptoms of poor mental health. For example, higher levels of depression are associated with higher threat levels (Cole et al., 2019; Folkman & Lazarus, 1986). One appraisal that can influence the coping process is self-efficacy (Bandura, 1997). If a young person believes that they are well equipped to deal with their symptoms then they are less likely to ask for help and more likely to try to cope independently. Girls are reported to be more likely than boys to report a situation as threatening (Cole et al., 2019) and more likely to perceive a situation as stressful (Rose & Rudolph, 2006) and severe (Velasco et al., 2020).
Also important in the coping process is resource availability during a stressful situation. During the appraisal process, young people will consider the resources available and will evaluate how these may help them (Lazarus & Folkman, 1984; Rowe et al., 2014). There is a clear distinction between formal (e.g., mental health professionals) and informal (e.g., parents, friends) sources when considering mental health help-seeking behaviors, and young people will more often disclose their symptoms to parents and friends than to professionals (Camara et al., 2017; Rickwood et al., 2007). Adolescents report feeling that they can trust informal sources more than formal sources, and the possibility that confidentiality will be breached in a professional setting is one of the main barriers that they report when considering seeking professional help (Leavey et al., 2011).
When it comes to choosing a coping strategy, type and severity of symptoms both seem to play a role. For example, Cong et al. (2019) concluded that adolescents using problem-focused strategies reported less depressive symptoms. Furthermore, Horwitz et al. (2011) reported that adolescents with high levels of self-reported depressive symptoms tended to use more maladaptive coping strategies such as self-blame (i.e., emotion-focused coping). However, young people experience gender related changes that are social, emotional, and behavioral in nature that can influence how they cope (Frydenberg, 2019). A study by Brytek-Matera (2007) concluded that girls coping with anorexia nervosa are more likely to use emotion-focused coping by managing their emotions and avoiding focusing on the problem (e.g., finding a solution). In addition, girls tend to seek more help overall (Slone et al., 2013) though this is focused on specific forms of social support like the support of friends (Sesar et al., 2016). On the other hand, boys dealing with symptoms of poor mental health, report using avoidance and recreational activities as a way to gain control over their symptoms (Rose & Rudolph, 2006).
Adding to the already complex nature of the coping process, online interactions are now central in everyday life for adolescents (Horgan & Sweeney, 2010; Houghton et al., 2015). Considerations such as simplicity, accessibility of information, and privacy can influence young people’s decisions to use the internet as a source of support for sensitive issues (Gibson & Trnka, 2020; Pretorius et al., 2019). A young person might prefer to go online and independently search for professional services so that they can maintain their privacy and control over the information (Frost et al., 2016), rather than, for example, asking their parents for help. For this reason, the internet is considered as an additional source of support in the present study.
Coping With a Peer Disclosure of Symptoms of Poor Mental Health
Adults encourage young people to talk with someone about symptoms of poor mental health in order to cope and overcome their difficulties (Griffiths et al., 2011). Whereas we have some understanding about how young people cope with their own symptoms of poor mental health, little is known about either how young people cope with a peer’s disclosure of poor mental health or what their emotional response to this situation might be (Raviv et al., 2000). This is important since young people often prefer to disclose symptoms to informal sources such as friends (Camara et al., 2017). Additionally, in the context of the TTC, young people dealing with their own symptoms report experiencing appraisals of threat or harm/loss (Cole et al., 2019; Fosco & Lydon-Staley, 2019). It is still unknown if the same is true when they are coping with a friend’s disclosure of symptoms of poor mental health.
Similarly, the coping strategies selected by young people after a friend’s disclosure are also not known. In general, adolescent girls are more likely than boys to provide emotional support and to seek professional help for a friend if they perceive the need for it (Raviv et al., 2009; Rickwood et al., 2005). As coping capabilities develop as a result of maturation and development (Rickwood et al., 2015), older adolescents are more willing to refer a friend to professional help and offer emotional support to peers struggling with symptoms of poor mental health, than younger adolescents (Yap et al., 2011a).
It is also the case that young people are more likely to refer a friend who is experiencing mental health problems to a professional than to refer themselves for the same problems (Raviv et al., 2009; Rickwood et al., 2005). The reasons for this are not clear, however, it is known that self-stigma is related to less help seeking (Lannin et al., 2016) and it is possible that in the context of someone else needing help, there is a lower level of self-stigma. As such, professional help can be seen as more viable for a young person to recommend. Moreover, the level of threat might be influenced by previous experience. Thus, this study will explore how young people differ in their coping process depending on whether they are dealing with their own symptoms of poor mental health or a friend’s symptoms.
The Present Study
The present study aims to explore how young people cope with symptoms of poor mental health. The following research questions guided this study: How do young people understand and cope with their own symptoms of poor mental health? How do young people cope with disclosures of a friend’s symptoms of poor mental health? What differences and similarities exist in young people’s appraisals and coping strategies across their own and friends’ symptoms? By using a qualitative approach, we hope to explore young people’s meanings and insights about the topic at hand (Levitt et al., 2017), that would allow for a better understanding of the differences between both situations.
Methodology
Participants
Eleven young people from the United Kingdom aged 13 to 15 years old (M = 13.55, SD = 0.69) were interviewed (six female, five male). Three were interviewed online, and eight were interviewed face-to-face. Two participants lived in England and nine resided in Scotland. Ethnicity and race data were not collected during interviews.
Materials
A semi-structured interview was developed considering the TTC elements. Prior to data collection, the interview was piloted with two young people to check question clarity and duration. This was audio recorded, took place through videoconference (i.e., Skype), and led to minor changes in phrasing of questions. The researcher started by establishing a consensus with the participants about the definition of “mental health problems.” Young people were asked what they thought a mental health problem was, and then the researcher provided the following adapted definition from World Health Organization (WHO, 2018) “when someone is having troubled thoughts, emotions, and behaviors. Or it can even be when a person is having trouble relating to people around him or her. Some examples of this could be depression or anxiety.” This was done in order to allow for all the participants to share the same understanding of what was being discussed throughout the interview.
Next, participants were asked to imagine that they were experiencing symptoms of poor mental health and were asked what they would do and how they would feel about it. The researcher also asked about their primary appraisals of this hypothetical situation (e.g., “Can you think of anything good or bad that can come from having a mental health issue?”) and what coping strategies they would use to deal with it (e.g., “If you had to think about acting about it, what would you do?”). They were asked how confident they would feel about using that strategy (i.e., secondary appraisal) and, finally, about what type of support they would look for in this situation (i.e., information, emotional support, or professional help) (e.g., “Would you ask for information/emotional support/ professional help?”). All participants answered the same set of questions for a second scenario in which they were asked to imagine that a friend disclosed symptoms of poor mental health to them.
Procedure
Ethical approval was obtained from the School Ethics Committee at the administering institution. Participants were recruited through community groups (e.g., Scouts, Guides, etc.) and private schools. Active parental and participant consent was sought prior to data collection. Consent to audio record the interview was asked from both parents and participants. Parents and participants were given an information sheet describing the aims of the study, and data storage procedures to guarantee informed consent. After obtaining consent, young people were interviewed either online or face-to-face and no one else was present during the interviews.
For online interviews, two forms using Qualtrics.com were created: one for parental/guardian consent and a second for children’s consent. Recruitment in community groups proceeded via an advertisement of the details of the study disseminated by email, phone, or using a paper advert. An advert was posted on the lead author’s social media platforms. The researchers asked groups and people who came in contact with the advert to share the links with parents/guardians so that, if interested, they could have access to the information sheet with details about the study and give consent for their children to be invited to take part in the study. After consent was obtained, the parent/guardian was asked to share a second link for their children to have access to the participants information sheet and, if they so desire, give consent to take part in the study. During the completion of the consent forms, a time and date suitable for the interviewee was requested. The interviewer then contacted the parents/guardians to confirm said date and time for the interview.
In schools, initial recruitment involved randomly selecting (by registration number) 15 potential participants (i.e., five from three different year groups) and sending information sheets and consent forms to parents. The overall parental consent form response rate was 60%. By year group, parental response rates were 40%, 80%, and 60% respectively. Data were collected from August 2018 until May 2019 and interviews ranged from 30 to 45 minutes. All interviews were conducted by the lead author. At the end of the interviews, all participants were provided with a support sheet with information about where to get help and advice when experiencing symptoms of poor mental health.
Interviews were transcribed verbatim, and data were pseudo-anonymized (i.e., transcribed interviews were given a code name). When transcribing the interview, any information that could possibly identify a participating organization (whether school or community group) or person was redacted. Finally, to improve transparency and help replication, this study was preregistered using the template by Haven and Van Grootel (2019). All the materials (including full interview schedule) and plans for data analysis can be found here: https://osf.io/wshfn/.
Analysis
A deductive approach to Thematic Analysis (i.e., theory-driven) was used. Braun and Clarke’s (2006) six stages for conducting Thematic Analysis were followed. The analysis aimed for a critical and detailed exploration of the themes extracted (Howitt, 2010). The TTC framed the development of the interview schedule. This means that four main elements were explored during the interviews and framed the initial analysis: (1) Mental health understanding; (2) Cognitive appraisals (i.e., primary and secondary); (3) Coping strategies (i.e., problem- and emotion-focused); and (4) Differences between coping with self and a friend’s symptoms.
It has been shown that multiple coders can help reliability in the coding process (Olson et al., 2016). As such, after all interviews were initially coded by the first author, they were then doubled coded by an independent person. However, this can lead to inconsistencies in coding between the coders (Olson et al., 2016). In order to counterbalance this, discussions between all the researchers about the meaning and interpretation of the data took place in order to reach an agreement (Levitt et al., 2017). In this study, there were no meaningful discrepancies between both coders. Finally, data were managed and stored using NVivo (version 12).
Results
The two main themes were social impact and choice of resources, containing three subthemes each. A thematic map displaying themes and subthemes and subsequent relationship is provided in Figure 2.
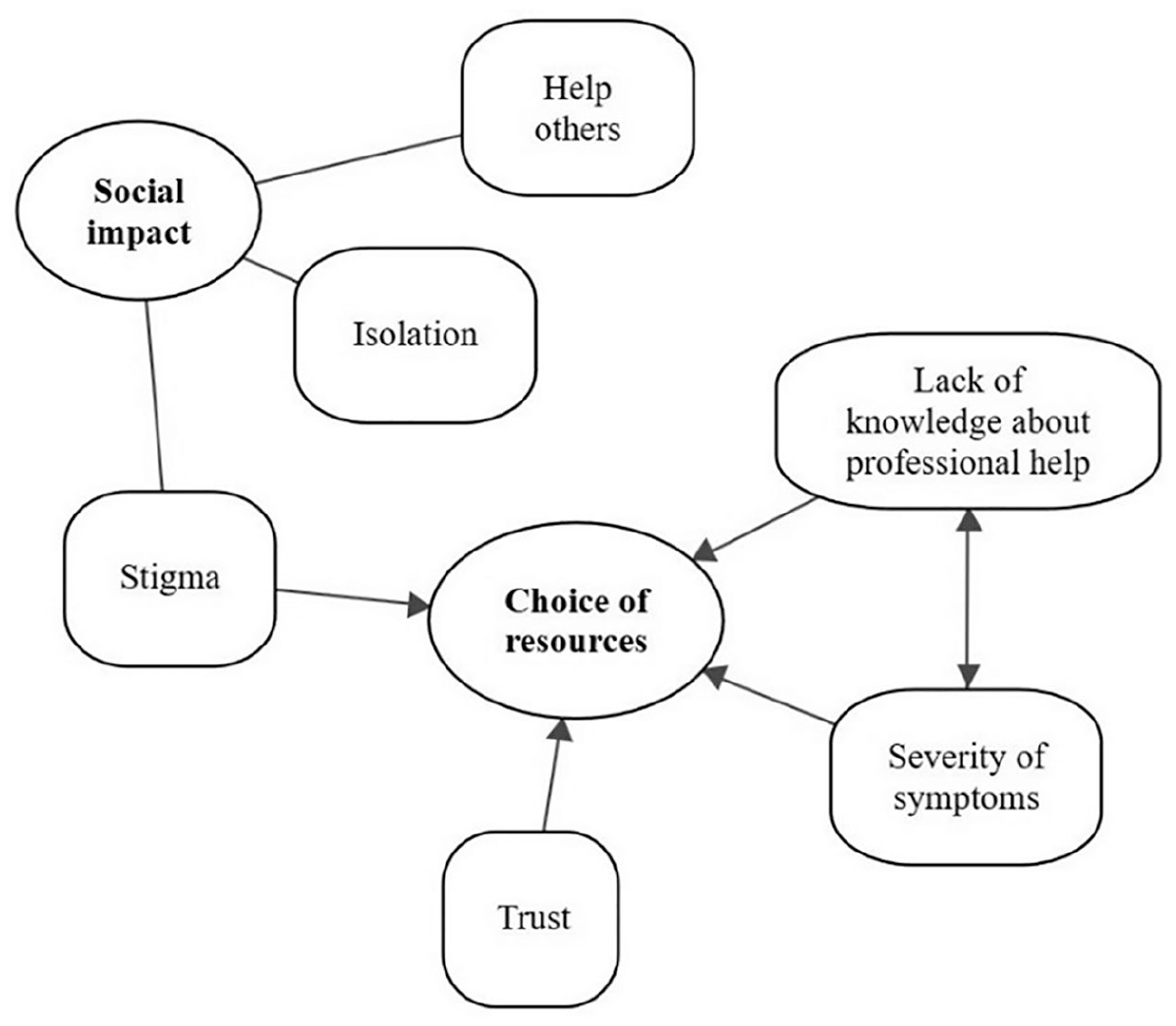
Thematic map.
Social Impact
When exploring the appraisals of exposure to symptoms of poor mental health, participants mainly focused on the social impact. Participants were able to identify positive and negative social consequences in both situations (i.e, exploring to their own symptoms and a friend’s symptoms of poor mental). As a form of positive consequences (i.e., primary appraisal of challenge), participants expressed that if they were able to overcome the symptoms they experienced, then they would be able to help others in the future. As negative consequences (i.e., primary appraisals of threat), young people expressed concern about possible isolation, and fear of being stigmatized because they would behave and feel different from others. These three subthemes will be further explored next and differences between participants’ own symptoms, and a friend’s symptoms, will also be explored in each of these.
Help others
Young people view being able to learn from their experiences, and consequently helping others, as a positive outcome. This was expressed in both situations (i.e., they or a friend experienced symptoms of poor mental health). According to the TTC, this could be interpreted as a challenge appraisal. One participant stated that if he went through this, he would be able to help others who are struggling to cope, emphasizing his own empowerment as a result: “I guess like it would actually make you stronger at things. And having the experience you could help others with it” (Boy, 13 years old).
Some participants also indicated that if they were faced with this situation, it would make them feel better prepared for the future. For example, one 14 year old boy said that having a mental health problem “can teach you, like, how to deal with it. . .”. Similarly, one girl (13 years old) sees it as gaining a “new set of skills” that would allow her to help others struggling. She goes on to say that, if a friend discloses to her, and if she were to have experienced it before, they both could “go together and talk about your experiences.” This shows an element of support that is clearly present in young people’s appraisals.
Also, participants put emphasis on the future and how this could be impacted by being able to “learn from your mistakes,” especially when helping a friend after they have gone through something similar. A 13 years old boy adds that, if he goes through the same situation again, he might be able to “(. . .) just rethink what [he] have done, [and] maybe do it differently in the future.” Finally, one girl made a clear relationship between being able to help others through her own experience and fighting feelings of isolation: “(. . .) it might make you feel stronger about yourself once you dealt with it. And then you will have a story to tell and will show other people that they are not lonely.” (Girl, 13 years old).
The next two themes focus on the possible negative consequences highlighted by young people when experiencing symptoms of poor mental health. These map on to the TTC as threat appraisals, since young people fear possible isolation and stigma as a result of poor mental health symptoms.
Isolation
Young people revealed concerns about feeling isolated from others as a result of experiencing symptoms of poor mental health, when considering their own or a friend’s symptoms of poor mental health. Participants said: “Well, they [friend] might be really depressed and might sit by themselves” (Girl, 13 years old). “Whereas if you are dealing with your own [symptoms] you feel more lonely, you feel more upset and you think that no one gets you” (Girl, 13 years old).
Specifically, when faced with a friend’s symptoms, a 13 year old girl expressed concern about the possible impact on their own well-being: “if they [friend] are feeling lonely, it kind of rubs off on you so it can sometimes makes you feel sad (. . .).” She goes on to say that it might influence their time together as she would “always keep thinking about it (. . .)”, showing concern about possible changes in their friendship and their interactions.
Finally, one 14 year old girl was worried that she would not be able to “go out with friends (. . .)” and that “they might start to wonder why [you] can’t go anywhere.” Another participant stated that if she ever experienced any symptoms, she would “(. . .) feel isolated from other people because they are not like the same as you.” She goes on to explore the reasons why she would feel different by saying that “[they] cannot relate in the same way as you and feel the same way around you” (Girl, 13 years old). These participants expressed fearing that they would be misunderstood by their friends, as well as feeling like others will not be able to relate to their experiences, so they would be more comfortable isolating themselves. There is a clear concern about others judging and not accepting them because of their symptoms.
Stigma
A 13 year old girl said that she “would be worried about them [friends] judging me. . . if people knew about it and especially because nowadays some people use mental health as a joke.” Stigma seems to play a bigger role when young people are dealing with their own symptoms of poor mental health than when they are faced with a friend’s symptoms. Participants also provided details about how perceived stigma could then impact their lives. One girl (14 years old), when asked about both situations, said that when dealing with her own symptoms she would “fear getting stuff wrong and not being able to do certain things.” Thus, focusing on how the symptoms might influence her own levels of confidence when interacting with others, further elaborating that it could be “hard to like leave the house (. . .) and find opportunities to do stuff.” However, when asked about coping with a friend’s symptoms, she said: “Personally, I wouldn’t mind what other people thought about [it]. I would just be trying my best to support them and not really care with what other people thought (. . .).”
Participants were able to attribute origins to the stigma. One girl (14 years old) referred to the role that media can play: “Probably because of the media. . . and the internet and seeing things just about depression and anxiety, and that it is not a good thing to have.” Also, one participant highlighted that stigma might be person-specific, influencing who they would disclose their symptoms to: “I think that some people would judge me because of it. It depends on the person. . . at my school people judge other people just because of their appearance so. . . Some people might judge me others might try to get to know me and what it is going on.” (Boy, 13 years old)
When it comes to choosing a resource to disclose to, one participant said that she “would be concerned” about what others might think, and that: “(. . .) I wouldn’t tell anybody specially my age because they would not be able to understand and they would be like ‘oh you feeling this way. . .and why are you behaving this way?’”(Girl, 13 years old). Thus, as she fears that her peers would judge her, she will most likely not disclose or ask for help from them. She goes on to say that she might use alternative sources of help in order to cope, in turn making her feel less exposed to potential judgment:
“I would go on the internet so that I don’t have to see someone about it and feel embarrassed.”
A girl (13 years old) explained seeing the value in talking to others, but because of fear of judgment she might not want to ask for help:
“But I know that I could [talk with someone] but I’d probably feel uncomfortable so I wouldn’t tell them. . . I just wouldn’t feel comfortable with it. [Interviewer: Why?] Maybe because people would judge me.”
Choice of Resources
Participants mainly reported using problem-focused strategies to deal with symptoms of poor mental health, for example getting information to deal with their symptoms: “I think I would try to like understand what it all meant and why I was like feeling that way. What I could do to change that and if I could. . . like work around it.” (Boy, 14 years old) “I think I would want to. . . like. . . know what it is happening and why it is happening. . . like ask questions to understand why I am (. . .) feeling like that. . .” (Girl, 13 years old).
Participants also often stated the need to ask for help from someone in order to deal with symptoms of poor mental health, since they felt unprepared to cope with it on their own. This became evident when dealing with a friend’s symptoms. Participants often referenced seeking help from their parents to better understand how to help a friend overcome their symptoms. Factors highlighted by participants that influence resource selection are: trust levels, lack of knowledge about professional help, and perceived severity of the symptoms.
Trust
This subtheme was present in both situations (i.e., own and friend’s symptoms), but interpreted differently. However, in the context of the TTC, trust could be interpreted as a secondary appraisal. In relation to a friend’s symptoms, participants felt that if they needed to talk to someone about it (e.g., to ask for help) they would be concerned about breaking their friend’s trust: “(. . .) say that a teacher went up to them and says it [that they have told them about the symptoms] and they have no idea [that they told], that would be a bit. . . they would feel like their trust was betrayed, I think.” (Boy, 15 years old) “I don’t want them to lose their trust in me (. . .).” (Girl, 14 years old)
They also highlighted the need to keep their friend’s privacy and anonymity when considering disclosing to a third-party. One girl (14 years old) said that she “(. . .) probably wouldn’t say their names (. . .)”, and that if she had to disclose, she would ask what “(. . .) advice to give them or if [she] could do anything to help them (. . .).” In addition, young people stated their concerns about not knowing if their friend would want others to know, so they would prefer to not ask for help from others when a friend discloses symptoms to them: “Because I am not sure if my friend would want me to share that with a teacher (. . .)” (Boy, 14 years old). “(. . .) I don’t know if they feel like talking with other people. Like. . . not sure if they want to share stuff with others” (Girl, 14 years old).
Moreover, suggesting professional help to a friend was viewed as something that would potentially damage the friendship. One girl (14 years old) said that she feared that “(. . .) they might not trust you as much then [after suggesting professional help].” She goes on to explore the reasons why by saying that they probably would think that “(. . .) they can do it by themselves.” This point of view is supported by another participant who, when asked about suggesting professional help to a friend, said: “Not sure (. . .) it would be hard because, like I wouldn’t want them to like, lose their trust in me. They might not take that very well” (Girl, 13 years old).
Trust was also highlighted when young people were the ones experiencing symptoms. In this case, participants identified the need to feel comfortable and trusting someone prior to disclosing or asking for help. A girl (14 years old) said:
“I would maybe go and talk to a close friend that I (. . .) that I know that they wouldn’t go and speak to anyone about it. (. . .) it would just be between me and them. Just take them away and have a chat with them about it.”
However, young people do not hold much trust in resources other than parents and friends. For example, when asked about online resources, participants talk about not trusting chatrooms or websites where people share their experiences: “(. . .) for example those people online that are feeling suicidal and talk about it and try to hide it, I don’t think I would trust those people” (Boy, 13 years old). “(. . .) I wouldn’t probably just go off from some source of Google, because it is not really reliable (. . .).” (Boy, 13 years old).
Moreover, it seems that school staff are not considered to be a resource for dealing with symptoms of poor mental health. Participants expressed feeling uncomfortable disclosing these hypothetical symptoms to teachers. One participant (Girl, 13 years old) said that although she is “with the teachers everyday”, she does not think she “would be as comfortable going up to them with something so serious.” Another young girl (13 years old) said:
“I would be comfortable talking with family and friends, but when it comes to my pastoral care at school not really.”
She goes on to emphasize the lack of trust and issues pertaining to confidentiality that could be broken if confiding in a teacher at school who provides support for students’ emotional wellbeing. Additionally, a 14 year old boy, when asked if he would consider talking with someone at school, said no because “they are not people that I know well and trust (. . .)”; indicating a need for rapport to be built beforehand in order to feel comfortable disclosing.
As with school staff, young people show an overall lack of trust in using professional help. They said that they “would be a bit nervous to open up about it [symptoms] to a doctor that I don’t really know that well (. . .)” (Girl, 13 years old). Lack of trust in professionals could be related to an overall lack of understanding about this resource.
Lack of knowledge about professional help
Overall, participants did not consider professionals to be their main source of help. If in need of professional help, participants said that they would be unsure about how to find it and would most likely resort to using other resources, like parents or online information, to cope: “I probably would have to ask my parents about it [where to go for professional help] (. . .)” (Girl, 14 years old). “(. . .) I would probably start off by like Googling specialist help at first, to see the places I could probably go. And if there is none near me, then probably ask my parents if they know places (. . .)” (Boy, 13 years old).
One participant (Boy, 14 years old), when asked if he would consider professional help, shared that he “(. . .) would go to a therapist (. . .)”; however, he was unsure about “(. . .) how to go and find them (. . .).” As a result, he would have to ask his parents for help or “(. . .) probably the school help to find professionals.” Nonetheless, he also said earlier: “If it is something like bullying maybe [he would share with parents]. . . but if it was something more, I would probably keep it to myself.” He added that he would not disclose to a teacher since he feels that he cannot trust them with that type of information. On the one hand, this participant is capable of identifying a strategy (i.e., professional help) that he considers would be beneficial for him; yet he also expresses the difficulty in accessing it. Thus, because he does not feel comfortable disclosing to either teachers or parents, he might not ask for professional help even if he was in need of it.
A lack of overall knowledge about professional sources is also present when young people say they would “just look up what the symptoms are online and be sure before you go somewhere. Make sure that that it is really how you are feeling and speak to someone that have dealt with it before” (Girl, 13 years old). This shows a need to confirm their feelings and symptoms prior to asking for help from a mental health professional.
Severity of symptoms
Overall, young people said that the more severe they perceived symptoms to be, the more likely they are to ask for professional help. This was true for their own and for a friend’s symptoms. According to the TTC, this could be considered as a threat appraisal. When asked about what he would do when faced with a friend’s symptoms, one participant considered severity of symptoms as a way to decide what to do: “It depends. . . if it was suicidal I would get help first thing, because I would not risk it because. . . I don’t know what would happen. But if it wasn’t and was just pressure or mad at themselves for something they have done (. . .) I would try to get to the bottom of it first, and if I didn’t know what to do, I would get professional help” (Boy, 13 years old).
Participants often said that they would ask for professional help if it was “severe enough” or if it got “too bad.” When asked about what they meant by this, young people referenced suicidal thoughts or intentions to self-harm: “If it was severe. . . like you can’t stand your life and stuff.” (Boy, 14 years old) “(. . .) like when they are hurting themselves or they don’t want to be here anymore (. . .)” (Girl, 13 years old). “(. . .) more severe, like harder to deal with. Like suicide or self-harm type of things” (Girl, 14 years old). “(. . .) if they thought about suicide and those things. I wouldn’t be able to help them” (Boy, 15 years old).
This theme is even clearer in a quote by a 13 years old girl where she states her distinction between what can be consider minor and severe symptoms:
“I think if it got to quite a bad time I’d probably go to professional help. But if it’s just like depression I would probably just keep it going with my friends and family.”
Discussion
This study aimed to understand the coping process when young people deal with their own symptoms or a friend’s symptoms of poor mental health, highlighting similarities and differences.
Cognitive Appraisals
Primary appraisals
Participants attributed an appraisal of challenge by expressing possible gains when helping others once they themselves overcame their symptoms. This reflects Lazarus and Folkman’s (1984) description of challenge appraisals where an individual overcomes a stressful situation and expresses feelings of confidence and growth from it. However, reflecting previous literature (Cole et al., 2019; Fosco & Lydon-Staley, 2019), participants mostly highlighted negative appraisals when confronted with possible symptoms of poor mental health (whether their own or a friend’s). Feelings of embarrassment and possible isolation were important to the participants when assessing exposure to symptoms. When considering differences between both situations, young people feared more the impact of public stigma when they themselves experienced hypothetical symptoms. The results from this study are in line with a systematic review (Schnyder et al., 2017) that also reported that young people are less likely to seek help for their symptoms if they perceive high levels of public stigma.
Secondary appraisals
When it comes to secondary appraisals, supporting previous research (Rickwood et al., 2007), young people preferred to talk to a friend or to their parents if they were experiencing symptoms of poor mental health. When dealing with their own hypothetical symptoms, participants said that they would only disclose to someone who they consider trustworthy. This is in line with previous research which has shown that young people expressed the need to keep control over the information being shared and to whom this is later shared with (Buchholz et al., 2015; Huggett et al., 2018). When considering a peer disclosure, young people say that they might feel threatened by the possibility of losing a friend if they (i.e., young person) decide to ask for help from a third-party. Indeed, in the context of mental health discussions, young people report social isolation as a result of losing a friendship and breaking their friend’s trust (Huggett et al., 2018).
Coping Strategies and Resources
The young people in this study did not spontaneously mention school staff as a source of support, and did not feel school staff would be helpful when asked directly about them. Rickwood et al. (2015) also highlighted that, adolescents are unlikely to turn to school staff when seeking help for mental health difficulties, despite the existence of relevant services within school grounds. Since this research provides further evidence of the lack of use of school staff by young people when dealing with symptoms of poor mental health, future research should focus on understanding why this is the case. It might be helpful to understand the underlying reasons why adolescents do not feel comfortable reaching out to school staff, despite schools highlighting that staff is available to help students with their mental health. Thus, understanding where this lack of confidence stems from could help to adapt school services approaches in order to provide better support to young people.
Young people infrequently mentioned turning to online sources of support to cope with the issues raised in the interviews. This was even the case when they were directly asked about accessing this type of help. This was unexpected given the high levels of engagement with electronic media by this age group (Houghton et al., 2015). Furthermore, participants were critical judges of available online support and did not trust chat rooms or websites where people share their experiences. Previous work has raised concerns about unsupervised information online and how this can negatively influence coping strategies (Calancie et al., 2017; McCrae et al., 2017). Thus, the fact that the young people in this study reported being skeptical about the trustworthiness of online information is encouraging, when we consider sources that are not from reputable sources. However, this could be problematic for online resources from trustworthy services, such as the websites of the WHO or a country’s National Health Services, that offer support online.
Type of coping strategy also differed depending on the situation to which young people were exposed. When dealing with their own hypothetical symptoms, young people reported that they would be mostly focused on getting information and dealing with symptoms (i.e., problem-focused coping). This could be interpreted as being consistent with Lazarus and Folkman’s (1984) assertion that problem-focused strategies are more often used to deal with situations considered changeable. The young people in this study may therefore perceive they have the skills or resources to deal with their symptoms, and consequently, a higher self-efficacy. It is possible that when helping a friend, young people struggle with fears of inadequacy and “doing the right thing” as they are unsure of what they should do in order to help their friend. This in turn impacts their coping strategies. On the one hand, they can refer their friend to a trusted adult but, on the other hand, they could refrain from acting as a result of the fear of not knowing what is the right thing to do. Research relating to young people’s mental health literacy has focused on implementing programs designed to aid symptom recognition and, consequently, help-seeking intentions for a friend (Hart et al., 2018; Mason et al., 2015). Future research should explore the potential role that investing in mental health literacy programs could play in young people’s responses to a friend’s mental health distress.
In this study, severity of symptoms was presented as being one of the main influences on seeking professional help. Young people reported that they would only consider professional help as an option if they or a friend were experiencing suicidal thoughts or self-harming behaviors. Reporting that higher levels of threat would make them seek help from a professional. This contradicts research showing that the higher the severity, the lower the likelihood of adolescents seeking help (Velasco et al., 2020). The contradiction can be a result of research mainly exploring help-seeking behaviors when dealing with their own symptoms and not a friend’s. This theme could suggest that higher levels of threat are linked with higher levels of help-seeking when coping with a friend’s symptoms. While higher levels of threat would be linked with lower help-seeking behaviors when young people are dealing with their own symptoms of poor mental health.
Furthermore, it is interesting to note that, at the beginning of each interview, when asking the young people to define what mental health problems meant to then, none of the participants mentioned suicide or self-harm. Instead, definitions mainly referred to symptoms of anxiety and depression such as sadness, stress, and isolation from others. Future research should explore how young people view severity of symptoms and in what way this can influence their help-seeking behavior more broadly.
Strengths, Limitations, and Future Directions
This study has many strengths. By using a qualitative methodology to understand the coping process, this study has described how coping strategies may differ when symptoms of mental health problems are experienced compared to when a peer discloses such symptoms. This study also provides further understanding of how young people may cope with a peer disclosure. Knowledge about the coping process (i.e., appraisals, resources, and strategies used) can be helpful in order to provide better mental health support to young people through these difficult times. It is also important to note limitations. The interviews were based on hypothetical scenarios. Responses from a sample of adolescents with lived experiences may reveal different themes.
It is worth mention that although background information other than gender and age was not collected, these results should also be interpreted considering the cultural context young people live in. It is known that young people from minority groups have a harder time seeking help when it comes to their mental health (Okur et al., 2016). Thus, future research should aim to understand differences between coping with one’s own and a friend’s symptoms in light of cultural background characteristics. Similarly, the results do not allow for conclusions to be drawn about age differences, due to the restricted age range of the sample. Future research should look into lived experiences and explore age differences so that further insight can be gained about young people’s coping strategies across the breadth of late childhood and adolescence.
Additionally, when analyzing the data, it was noticeable that participants did not consider online resources as a source of help. They highlighted that they would only use online resources if they had doubts about what symptoms meant (i.e., information seeking). Participants did not mention conversations online with peers or family members when asked about online help-seeking behaviors, despite online interactions with friends via social media being one of the most used ways of communication in adolescence. This might be due to how the question was asked. In the future, it will be helpful to probe in more detail how online interactions influence help-seeking behaviors. This could be accomplished by, for example, asking participants about each specific online interaction (e.g., social media, visiting websites, gaming). Further research exploring the link between coping strategy used and the source of support chosen could be beneficial to understand the relevance of online sources for young people when dealing with symptoms of poor mental health.
Finally, it is relevant to note that this study aimed to document the differences and similarities when comparing a situation where young people deal with their own symptoms of poor mental health and a situation where they deal with a friend’s symptoms of poor mental health. The emotional effects of a friend’s disclosure were not assessed here. Future research could explore the effects on adolescents’ mental health and the stressors that emerge when they are the source of help for their peer’s disclosure of symptoms of poor mental health.
Implications
The implications of this study are of interest to schools, parents, and mental health professionals. These findings emphasize the negative role that stigma plays when seeking help. There was a connection between stigma and young people’s own symptoms of poor mental health, and, notably, this was absent when dealing with a friend’s symptoms. Thus, stakeholders like schools, parents, and mental health professionals could focus attention on reducing the effects of stigma when a young person experiences symptoms themselves, but not when they are exposed to it by a friend.
Additionally, when it comes to seeking professional help, this study speaks to the potentially harmful belief that young people hold of mostly only seeking help from professionals when symptoms are characterized as severe. Thus, this finding can provide some support for the improvement of young people’s awareness of the preventive nature of mental health professionals rather than a last resort solution. Finally, findings from this study revealed a reluctance by young people to seek help from school staff. Efforts should focus on improving young people’s confidence with respect to disclosing to school staff and this is linked to wider discussions concerning the creation of a safe environment in schools for young people to disclose their symptoms.
Conclusion
This study provides a contribution to our understanding of how the coping process unfolds in young people when dealing with symptoms of poor mental health. The findings highlight the need to invest in anti-stigma campaigns that focus on helping adolescents’ access helpful resources and demonstrate how those resources can be of benefit. Additionally, anti-stigma campaigns could also play a role in reducing social isolation by giving adolescents a lived experienced example which they can relate to. Investment in these campaigns is also very timely given the negative consequences for young people’s mental health due to the current COVID-19 pandemic.
This study also showed that the severity of symptoms experienced seems to impact the choice of resources and how coping unfolds, for their and a friend’s symptoms. As such, further exploration of the relationship between severity and coping strategy, coupled with the influence of stigma and trust, could prove helpful in order to better support young people coping with symptoms of poor mental health. Finally, the lack of confidence in approaching school staff when coping with symptoms of poor mental health needs to be further explored in order to provide the most adequate support to young people.
Footnotes
Acknowledgements
We would like to extend our sincere thanks to all involved in this study: the young people that took time from their day to be interviewed for this study; the Parents/Guardians who gave consent for their child to be approached about the study; and finally, a special thank you to all the organizations that supported the recruitment process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Information
Ethical approval was obtained by the Ethics Committee of the School of Psychological Sciences and Health of the University of Strathclyde (reference number 06/01/05/2018/A).