
Abstract
There are conceptual and ethical challenges to defining adolescents’ autonomy to access health care, and these can lead to health care norms and practices that could be maladjusted to the needs and preferences of adolescents. Particularly sensitive is access to sexual and reproductive health care services (SRHS). Yet, while there has been substantial conceptual work to conceptualize autonomy (e.g., as independence), there is a lack of empirical research that documents the perceptions of adolescents regarding on how they access or wish to access health care services. The main objectives of this research were to (a) understand how adolescents in Colombia interpret the concept of “autonomy,” (b) describe how these adolescents articulate their autonomy (i.e., preferences) in accessing SRHS, and (c) analyze the ethical issues emerging from these data. Forty-five semi-structured interviews were conducted with participants aged 14 to 23 years old in the Departments of Antioquia and Valle del Cauca in Colombia. Our study showed that participants’ understanding of autonomy was context-based and highly dependent on personal experiences, and these influenced their choice in how to access SRHS. Seen through the ethical lens of a reproductive justice framework, our results highlight the unequal opportunities for adolescents in terms of autonomy to access SRHS.
One of the core ethical principles in contemporary bioethics, anchored in widely shared value systems and legal norms in North American and Western European liberal democracies, is respect for individual autonomy, whether in participation in research or access to health care (Beauchamp & Childress, 2001; O’Neill, 2008). This entails recognizing individuals’ right for self-determination and their ability to make choices for themselves, based on their view of what is in their best interest. The duty on the part of health professionals to adhere to this ethical principle is enshrined in contemporary codes of ethics, particularly in North America, and is part of an explicit rejection of strong medical paternalism. Contrary to competent adult patients, in the case of adolescents, respecting autonomy can become complex. One issue is how adolescents themselves understand the principle of autonomy and how it applies to them in their access to health care. Another is how parents or health care professionals determine when, how, and to what extent to respect an adolescent’s choice regarding health care services, a topic that can be particularly challenging when the service relates to sexual and reproductive health (Bekaert & Southgate, 2018).
Adolescence is a period of transition—physically, psychologically, and socially—between childhood and adulthood (O’Donohue et al., 2013; Sawyer et al., 2012). It is marked by the development of greater autonomy (e.g., as liberty, independence) and competencies (e.g., ability to rationally evaluate different choices). Adolescents are no longer children and in general have much greater capacity to make important decisions about their personal interests, but they are not yet adults. Furthermore, adolescence is a time when individuals begin exploring and engaging in “adult-like” behaviors such as sex. Yet, there are also no objective or universal biological markers to define exactly when a person is no longer an adolescent and becomes an adult capable of making independent decisions (Dahl et al., 2018; Ledford, 2018). Nor are there specific biological markers to define the age at which an adolescent should have their autonomy respected in health care decisions (e.g., some jurisdictions have “mature minor” laws enabling 14- or 16-year-olds to make health care decisions without parental consent).
There are different overlapping definitions of autonomy that may create challenges to implementation, for example, autonomy as independence, as volition, as agency, as maturity, or as liberty (Soenens et al., 2017). Furthermore, determining the scope and limits of adolescent autonomy in health care is inherently a socio-legal and cultural issue, anchored in societal value systems (Kagitçibasi, 2017, p. 194); it can thus vary across regions, cultures, and type of health care service in question. This diversity in the characterization of adolescence was a factor in the introduction in global health policy of a new definition of adolescence. According to Sawyer et al. (2018), adolescence should be defined as being a stage of life between the ages of 10 and 24. One of the purposes for this extended age range is methodological, that is, it can allow for a more accurate description of how a person transitions from childhood to adolescence and from adolescence to adulthood, while also clarifying the similarities and differences between individuals within this age range. The latter points are especially relevant for studying the question of autonomy in adolescents with regard to health care in general, and sexual and reproductive health care services (SRHS) in particular.
The need to address barriers to adolescents’ access to health care, some of which are related to their autonomy and competency, can be justified on public health grounds. Adolescents are one of the groups that least use health care services, despite having important health-related needs (Patton et al., 2018). This point has been highlighted as a serious problem to be tackled by the United Nations’ Sustainable Development Goals and with the Global Strategy for Women’s, Children’s and Adolescent’s Health (World Health Organization [WHO], 2015). Given the absence of consensus regarding how to determine the scope of adolescent autonomy to access health care services, as well as the lack of quantitative biological markers, clinicians and policy makers may lack the evidence needed to guide decision making regarding the provision of care to adolescents (e.g., with or without parental oversight).
Determining the scope of adolescent autonomy with regard to health care services requires the inclusion of adolescents’ perspective. Designing public policies that ensure health care service delivery that best meets the actual needs of adolescents (and thus increases their uptake of these services) requires an understanding of how adolescents experience and understand autonomy and its connection to their access to health care services, such as those related to sexual and reproductive health.
The qualitative study presented in this article involved semi-structured interviews with 45 adolescents in five Colombian cities—Medellin, Rionegro, Santa Fe de Antioquia, Palmira, and Cali. The first objective was to describe how these adolescents understood the concept of autonomy, and their preferences and challenges in the context of accessing SRHS. 1 No specific definition of autonomy was used. As adolescence involves the development of different components of one’s autonomy, participants were free to expand on the topic during the interview. Building on this information, the second objective was to analyze the ethical issues that emerged regarding adolescent autonomy to access SRHS, using the conceptual framework of reproductive justice. The goal was not to argue for specific positions with regard to adolescents’ autonomy in accessing SRHS, nor to propose an age at which adolescents’ autonomy should be fully respected in health care. Rather, this article aims to show—through a presentation of the descriptive data and an ethical analysis—the types of underlying ethical issues related to adolescent autonomy that arise in accessing SRHS in Colombia.
Reproductive Justice Framework
The reproductive justice movement—as developed by women of color in the United States in the 1990s—stresses the importance of creating contexts that are enabling and equitable for all, so that people can make genuine and free choices related to sexual and reproductive health (Luna & Luker, 2013; Price, 2010; Ross & Solinger, 2017). For example, while contraceptives may be available, if they involve high fees, not all people will have the same opportunities to use them. People with limited economic resources (which oftentimes apply to adolescents as a group) will be restricted in their choice of contraceptives in comparison with people with greater economic resources. Hence, two core ethical principles of a reproductive justice framework are autonomy and justice. As the analysis of the study data below shows, not all participants had equal access to SRHS, raising issues of justice and equity.
Research Context
Around 90% of research done on adolescents is performed in high-income countries (HIC) even though 90% of adolescents worldwide live in low- and middle-income countries (LMIC) (Blum & Boyden, 2018; Vandermorris & Zulfiqar, 2017). It is thus pertinent to conduct research with adolescents in different socio-cultural contexts to understand the different lived realities and experiences of adolescents around the world, and specifically in LMIC, such as Colombia, a country that does not have specific parental consent laws regarding minors accessing SRHS. Colombia also has different governmental initiatives advocating for adolescent health, including sexual and reproductive health. For example, the Profamilia network of non-profit clinics is present throughout Colombia and provides specialized access to SRHS (e.g., abortion, contraceptives, vaccination) to the population, including for adolescents. (Profamilia was involved in this research and helped with some of the recruitment of participants.)
There are different reasons for choosing to focus on access to SRHS as opposed to other types of health care services (e.g., oncology). Sexual health and sexuality may be sensitive topics for discussion with parents, or even a taboo subject that is simply not discussed. Furthermore, research in various cultural contexts, such as the United States (Brittain et al., 2015), Ethiopia (Berhane et al., 2005), the United Kingdom (Burack, 2000), or India (Sivagurunathan et al., 2015), has shown that adolescents prefer their parents not knowing they are accessing SRHS. Yet, some of the leading causes of deaths and disability for adolescents worldwide are related to sexual and reproductive health (e.g., childbirth, HIV; Patton et al., 2016). These issues underscore the need to explore adolescents’ autonomy to make SRHS more accessible and youth friendly.
Method
Data Collection and Analysis
To better understand Colombian adolescents’ perception of autonomy as it relates to accessing SRHS, a qualitative study was conducted in Colombia using semi-structured interviews during 2019 and 2020, allowing participants to share in detail their opinions and personal experiences on the topics of autonomy and access to SRHS (Gaudet & Robert, 2018). Collected data were analyzed by applying a reproductive justice framework.
The first author conducted the interviews. Before recording the interview, participants were asked demographic questions (e.g., age, gender, with whom they lived, highest level of education, whether they had an income). Participants could choose where to do the interview; the majority chose a private room in a clinic, library, or a public park. Interviews were conducted in Spanish, were audio-recorded and transcribed by the first author, then coded and analyzed manually on paper and with Microsoft Word. To protect participant confidentiality, participants were given a pseudonym. The interview excerpts presented in the current article were translated by the first author.
All participants had the same interview guide that was composed of the same central themes presented as core questions (e.g., interpretation of the concept of “autonomy,” barriers of access to SRHS, how the participants would want their autonomy fostered to access SRHS). However, each core question per theme had subcategories of questions depending on the participant’s context. For example, a participant who had never accessed SRHS was not asked the same follow-up questions in comparison with a participant who had previously accessed SRHS. This latter participant would then be asked questions about experiences relating to their autonomy with the health care professional, whereas participants who had never accessed SRHS were asked how they would want to interact autonomously with a health care professional when they accessed SRHS. The interview guide was not piloted. The length of interviews was between 16 and 47 minutes. While the researcher would invite participants to develop their answers (e.g., asking whether they could “explain” or “elaborate” their answers), many participants kept their answers short and concise which led to some interviews ending more quickly than others. Many participants asked how long the interview would take, to which the researcher would respond that it was left to the discretion of participants, but that on average would last around 30 minutes. This clarification seemed to please participants more than the initial 60 minutes stated on the information and consent forms (it was initially believed that participants would talk much more during their interviews). On a methodological note, for future reference for conducting interviews with this population, aiming for shorter length of interviews could facilitate recruitment and encourage participation.
The coding of the interviews consisted of first regrouping participants’ answers for the same interview question (e.g., How do you interpret the concept of “autonomy”?). Then, for each question, participants’ answers were coded and regrouped based upon similarities of content. This approach allowed for the identification of some patterns and differences between participants’ answers, while taking into consideration demographic factors (e.g., age, gender). When applying a reproductive justice framework to the analysis, it was possible to identify some of the ethical issues emerging from what participants shared during the interviews (e.g., whether there were unequal opportunities to access SRHS for adolescents based on autonomy).
Initially, when developing the research, the minimum recruitment sample size was 20. The goal was to have at least 10 participants who had never accessed SRHS and 10 participants who had previously accessed SRHS. The goal was to identify and analyze the differences between groups around the question of autonomy. The maximum recruitment sample size was 60, because the researchers wanted to have a diverse sample of participants. Recruitment stopped at 45 participants because the research project was coming to an end and the researchers had reached their objective of having a diverse sample of participants.
Recruitment
Participant recruitment took place at different locations and in various contexts over 6 months, from August 2019 to February 2020. The Profamilia network displayed recruitment posters in their clinics (e.g., waiting area) in the cities of Medellin, Palmira, and Cali, inviting participants to contact the researcher. Health professionals (e.g., youth psychologists, social workers) also shared information about the research project with their adolescent patients. When young people participated in activities with Profamilia (e.g., youth or activist groups) in and outside the clinics themselves, information about the research was shared with those present. One nurse also presented the research in a high school. This recruitment strategy was supplemented by snowball sampling, with participants sharing information about the research with their friends and peers. As such, there was a variety of participant profiles as some had never used SRHS for different reasons (e.g., prohibition from parent) and others had used SRHS from clinics besides Profamilia (e.g., family doctor or other clinics). For this study, the only inclusion criteria were to be aged between 10 and 24 years old; adolescents from different backgrounds (e.g., gender, level of education) were invited to participate.
Ethics
The Science and Health Research Ethics Board of the University of Montreal approved the research, reference number: CERSES-19-049-P and the Profamilia Research Ethics Committee approved the study. Participants were asked to read and sign the consent form before participating in the interview. Participants were given a copy of the consent form and a list of resources to contact if they needed assistance (e.g., psychological support). Parental consent was not requested because it was deemed to be a potential barrier to participating in the research, notably because of its sensitive topic. The decision to not ask for parental consent was based on Guideline 17 (Research Involving Children and Adolescents) of the International Ethical Guidelines for Biomedical Research Involving Human Subjects (Council for International Organizations of Medical Sciences, 2017), where it is argued that under certain conditions, it is possible to waive parental permission when it is not possible nor desirable and the research involves low risk for participants.
Results
Participant Profiles
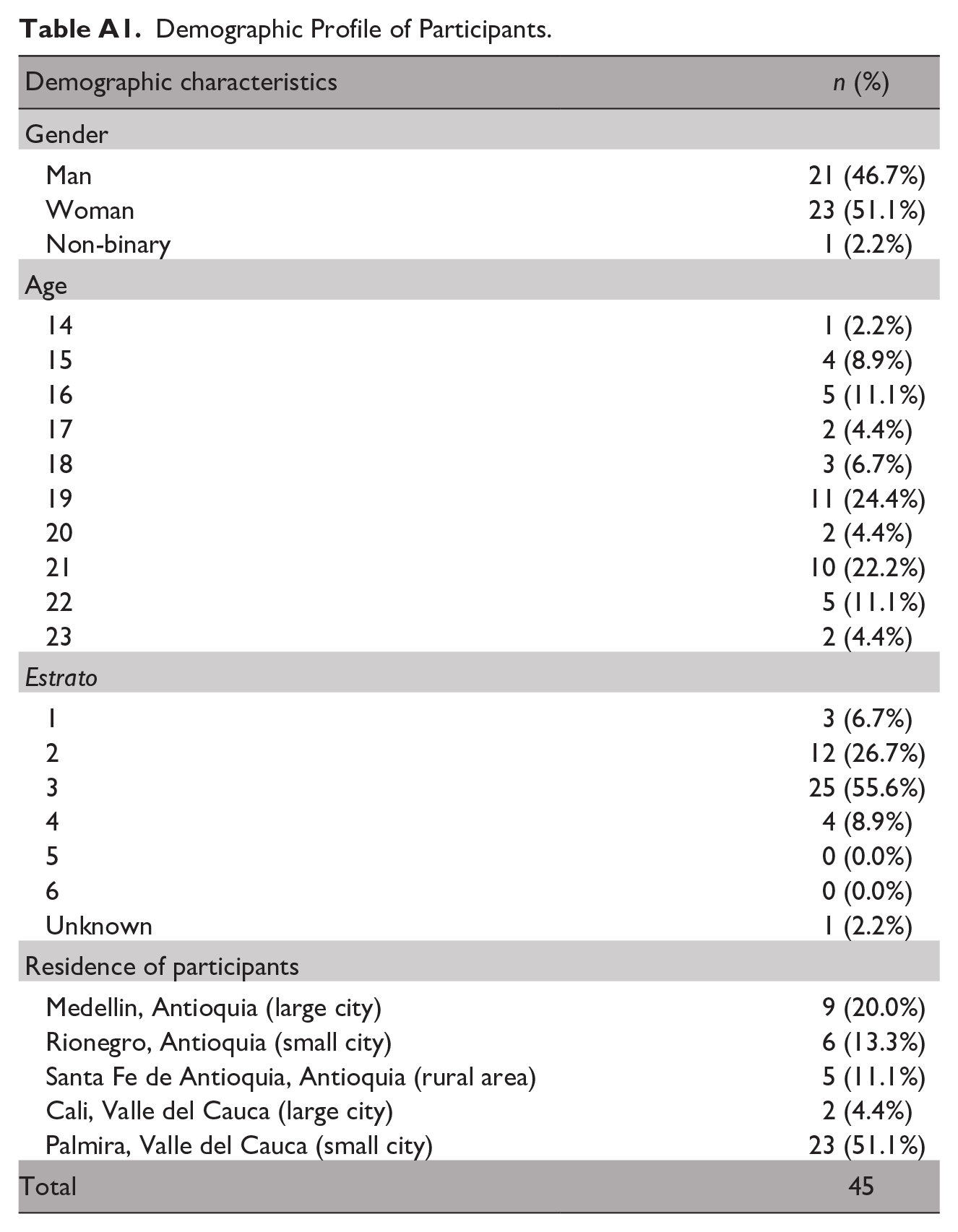
A total of 45 participants were interviewed (a table summarizing these profiles is presented in the appendix): 23 adolescent girls, 21 adolescent boys, and one gender non-binary adolescent. The age range was 14 to 23, with an average age of 19 and a standard deviation of 6.4. There were 20 participants from the Department of Antioquia: nine from Medellin (large urban region), six from Rionegro (small urban region), and five from Santa Fe de Antioquia (rural area). Twenty-five participants came from the Department of Valle del Cauca: two from Cali (large urban region) and 23 from Palmira (small urban region).
Colombia has six official socioeconomic classes (estratos) assigned to citizens based on their area of residency: 1 being the lowest, 6 the highest. Among the participants, three participants belonged to Estrato 1, 12 to Estrato 2, 25 to Estrato 3, four to Estrato 4, and one participant did not know their estrato. This distribution of estratos among participants reflects the general distribution of estratos within Colombia, where the majority of the population belongs to the lowest three estratos and a minority belongs to the three upper estratos.
Three participants lived on their own, two with their romantic partner, 15 with both parents, and the remaining 25 participants had different living arrangements with various family members. For example, some lived with grandparents, aunts, or with a single parent. All participants 18 years or below were students enrolled at school at the time of the interview. For participants older than 18 years of age, all had completed the equivalent of a high school diploma; some were enrolled or had completed the equivalent of post-secondary education with a “technical diploma,” whereas others were enrolled in or had completed university.
Themes
The following three sections are divided by the central questions that participants were asked during the interviews. Within each subsection, participants’ answers (the names are pseudonyms) are categorized by similarities of responses, allowing differentiation of the emerging themes and patterns.
How Do You Understand the Concept of Autonomy?
One of the opening questions of the interview was how participants understand or interpret the concept of autonomy. Beginning with this question enabled the researcher to establish the groundwork or baseline of the participant’s understanding of the concept, so that later on during the interview, he could make reference to the participant’s definition when discussing other topics (e.g., their access to SRHS). As the following excerpts show, there were different understandings of the concept among the 45 participants.
The unfamiliar and the very informed
One of the most significant differences in participants’ answers was that some were not familiar with the concept of autonomy.
Sofia (21-year-old, Estrato 3): Autonomy . . . Well . . . It’s like . . . I dunno Santiago (15-year-old, Estrato 3): I don’t know that word. Silvia (16-year-old, Estrato unknown): To be honest I don’t understand the word autonomy. Alberto (19-year-old, Estrato 1): I don’t know what that word means. By contrast, as the following interview excerpts demonstrate, others were very informed about the concept. Juliana (20-year-old, Estrato 4): Autonomy, I interpret the word as deciding for your own body, without having anybody decide for you. Carolina (21-year-old, Estrato 4): Well autonomy is the power to decide for one’s self, based upon what one believes, from their own principles, the possibility to decide for yourself. Manuel (20-year-old, Estrato 3): I would say that autonomy is the faculty to take things by your own account. The ability to decide on a personal basis for whatever and in whichever theme. David (19-year-old, Estrato 3): Well, I interpret the word like knowing your rights and how to access them. It’s like knowledge. Autonomy is the ability to access that. It is your own will.
“Autonomy as independence,” “autonomy as choice,” or as a mix of both
Among the participants who were familiar with the concept of autonomy, there were two common interpretations of the concept—autonomy as independence and autonomy as choice (liberty)—although for some, the definitions were a mix of both interpretations.
Francia (22-year-old, Estrato 3): The liberty to do the things that I want to do. That’s how I interpret it (autonomy). It’s like a synonym of liberty. Diego (21-year-old, Estrato 3): Well, that you make the decisions yourself and that you go and find out without depending on anyone. “I want to go and find out,” “I want to try this and that.” You do that on your own. Mateo (19-year-old, Estrato 3): The capacity for someone to develop, to take decisions. Rafael (16-year-old, Estrato 4): It is the capacity for someone to do things by themselves. And when someone grows up, they are able to do more things alone without the help of anybody. That’s how I would define autonomy.
Autonomy as a symbol of individuality, personality, and responsibility
A third common interpretation of autonomy was related to individuality, personality, and responsibility.
Sebastian (21-year-old, Estrato 3): The concept of autonomy, I think it means like, the determination, the value that someone attaches to themselves, to one’s life. To respect yourself, to value yourself, to take care of yourself among other things. Martin (21-year-old, Estrato 3): Autonomy . . . It could mean like the way you think, your own way. I would say that’s what is autonomy, the authentic way each person is. It can be like your personality, your way of being, your way of thinking. Paola (18-year-old, Estrato 3): Like, something that is your own. It is something that you do. It’s kind of like “do-it-yourself,” it’s kind of like what you can do. To make your own decisions. To identify yourself. Juan Martin (16-year-old, Estrato 3): Like it comes from yourself and having a very high autonomy and all that. It’s like having a responsibility. Hugo (16-year-old, Estrato 2): Autonomy is like the knowledge of yourself.
Do You Have Autonomy? When Did Your Autonomy Start? When Will You Have Complete Autonomy?
After asking participants how they interpreted the concept of autonomy, they were invited to explain how the concept relates to them: whether they believe they have autonomy, and if so, since when. For those who were unfamiliar with the concept, some general definitions were shared by the interviewer (e.g., explaining that autonomy can be synonymous with independence in choosing which music to listen to). This explanation helped some to better understand the concept, whereas others remained uncertain. It became rapidly clear that some felt they had complete autonomy, whereas others felt they did not have complete autonomy for various reasons (e.g., economic dependence on parents). Some recalled a specific event that served as a trigger moment to define the start of their autonomy, while for others the development of autonomy was experienced as a gradual process.
Recognition of having autonomy
Most participants were able to recognize having at least some form or degree of autonomy. Nonetheless, while most could recognize having some autonomy, two female participants (16 and 19 years old) did not know whether they had autonomy or not. The following two excerpts highlight the contrast of experience between some participants.
Silvia (16-year-old, Estrato unknown)
Are you someone that has autonomy?
To be honest, I don’t know, I don’t know if I have autonomy.
Martin (21-year-old, Estrato 3)
Would you say that you have autonomy at this moment?
Yes, thanks to God. My autonomy is very much rooted, and I can do and express what I feel.
Can you give me some examples?
Let’s say that in this moment I can, for example, go out and dress myself how I want in my own way [. . .] So yes, I am an autonomous person in my way of being, to speak, to think, to act.
Complete versus incomplete autonomy
For most participants, autonomy was perceived as a gradual process. Some felt they had reached complete autonomy, whereas others experienced partial autonomy.
Elena (22-year-old, Estrato 2)
Do you feel like a person that has autonomy?
Not completely because I am not that independent, and I don’t have my own resources to do the things how I want it, how I would want it. But in the choices and the things I can choose, yes I am autonomous.
Can you give me some examples in which you have autonomy?
Like . . . Like to take care of my own health, the way that I want to see myself in the decisions that I take. That if someone asks me something I can answer by my own will.
Hugo (16-year-old, Estrato 2)
Would you say that you have autonomy?
Yes, more or less. I take care of myself.
Can you give me examples for which you do not have autonomy?
I don’t know, maybe for the fact that I still live with my parents and I can’t go out whenever I want.
Jaime (22-year-old, Estrato 3)
Now you are 22 years old, would you say you have complete autonomy?
Complete autonomy, no.
What are you missing to have complete autonomy?
Become independent from the house.
That’s the only thing?
Yes, that’s what I’m lacking.
Juliana (20-year-old, Estrato 4)
Would you consider yourself an autonomous person?
I consider myself an autonomous person in many ways, but I also depend on others for other things. And I think that when you depend on others you lose a bit of autonomy.
Can you give me examples in what you have autonomy or not?
I have not reached financial autonomy, because I am still dependent on my parents. I decide for me, for my own body, I can decide what I want to do and do not want to do, for things that go against my principles and for things that go with my principles. I do not act in a way that others ask me to do things, but I do it out of my own will, thoughts, and principles.
Trigger event: personal or general
For many participants, their sense of autonomy started after a very specific event, such as a personal experience or a general marker (e.g., a birthday), as opposed to being understood as a gradual process.
Rosa (19-year-old, Estrato 3)
When would say you started to have more autonomy?
More than anything else, I would say when my dad died. My mom had to start working a lot. I was 12 years old, so I had to start looking into what was good, what was bad, if I would do it, if I would not do it. So since that age I’ve been taking care of myself.
Andres (23-year-old, Estrato 3)
My transition of boy to adolescent was around 14–15 years old, that’s how I felt it (having autonomy).
Why is that?
Because that’s when I had my first sexual contact with a woman. That’s the moment that I felt it (autonomy). I felt that I stopped being a boy, because everything that I imagined actually happened and that’s how I felt that change (of having autonomy).
Elena (22-year-old, Estrato 2)
When did you start to have autonomy?
I think since I was an adolescent, since I was 15 years old.
And why at 15?
It is like at 15 people think they are already big. At 15 you’re already starting to be a grown up.
So at 15 years old you are an adult?
No but like you start feeling like you’re already getting closer to being an adult. Obviously, you can’t start doing all the things that an adult would do, but you start wanting to do them.
For you, it is at 15 years old you felt you started to feel more as an adult?
Well, not to feel it. But that’s when I started to think of things, like wanting to do things like an older person. Like wanting to travel, to discover new things, to start living by myself. Things like that, like to go out without asking for permission or not saying at what time I’ll be back home.
Jaime (22-year-old, Estrato 3)
When did your autonomy start?
There was one event, or well, there were events that brought me to have an autonomy very early on. Since I was 12 years old, more or less.
And what happened at 12 years old?
The separation of my parents. I went to live with my dad. My mom left to live by herself. To be honest, I was even younger, I was 11 years old. So that’s when that my autonomy started because my dad was traveling a lot, so I was left alone at home with my little brother who’s younger by 3 years. Look, how can I explain it to you . . .
To me it sounds like you had to take care of a house and a kid.
Yes! Exactly! I had to take care of everything when my dad wasn’t there. So that’s why I’ve had a lot of autonomy since I was 11–12 years old.
Autonomy as a process
In comparison with participants who interpreted autonomy as starting after a specific event, others believed autonomy to be a developmental process.
Paola (18-year-old, Estrato 3)
Would you say that you have autonomy?
Yes
And when did this autonomy start?
Well I would say that my autonomy was developed through a process. For example, in my childhood, my parents would say “do you want this or that? what is it that you would like? what do you want to study? what would you like to do as a career? what are your dreams?” So since then I started to develop autonomy as a process for the rest of my life.
Sebastian (21-year-old, Estrato 3)
This autonomy of mine started when I started to learn from my own mistakes, so I started to educate myself and to listen to others. To learn from people who have good results in life and from there I was able to start to meet that autonomy in my life.
And when did this start? When you were an adolescent?
Yes, I was an adolescent. I was around 18 years old. I was in high school and I was a very capricious young person, with my parents and in school. That’s because I was not around good friendships and so on. So I think that my autonomy started in school, when I started to realize that I had to worry about myself, to take care of my things, to take care of myself, to love myself. So it’s from there that this change all started, all this developmental process to reach my complete autonomy.
Unequal understanding of the concept of autonomy and its application
Autonomy is a core principle in Western bioethics. Health care professionals must respect patient autonomy, and this is especially relevant in the case of sexual and reproductive health. From the participants’ answers, we see apparent differences in their understanding of autonomy. Some adolescents were very knowledgeable and capable of linking the concept to themselves (e.g., recognizing that they have some form of autonomy and its limits), whereas others were unfamiliar with the concept. The distribution of those who were unfamiliar with the concept was more or less equal between genders, ages, and estratos. Some younger adolescents were more familiar with the concept than their older peers, even some who were considered by definition to be adults (i.e., 18 years old or older) and as such are fully autonomous from a legal perspective. Participants who were more knowledgeable tended to be older and had attended university (likely a representation bias because most participants older than 18 had been enrolled in university).
Lack of knowledge regarding the notion of autonomy, and how it applies to oneself, represents an ethical challenge from a reproductive justice perspective because it can limit or impede the exercise of autonomous decision making regarding sexual and reproductive health. Moreover, adolescents cannot hold health care professionals accountable for their responsibility to respect patient autonomy if they do not know or understand what autonomy is. This relates to a possible power imbalance whereby professionals know they must respect patient autonomy, yet the patient does not have the same knowledge. On the flip side, if professionals have a specific understanding of the principle of autonomy that does not resonate or apply to the adolescent patient’s own understanding and experience, this can potentially lead to suboptimal care (e.g., involving miscommunication).
Finally, equity concerns arise when some adolescents are more knowledgeable than others about the foundation and significance of the principle of autonomy as it applies to SRHS. When some are in a more privileged position than their peers and are capable of advocating for their rights and interests compared with others (who are unfamiliar with the concept of autonomy and with their rights), a discrepancy is created in access to care. From a reproductive justice framework, these unequitable opportunities constitute challenge and call for initiatives to address this inequity, particularly as it relates to access to SRHS as will be shown in the following section.
How Do You Want Your Autonomy to Be Respected to Access SRHS?
Participants were invited to share their opinions and personal experiences regarding their autonomy and ability to access SRHS. For example, participants were asked whether they preferred going to a health clinic by themselves or whether they wanted the assistance of someone (e.g., parent, friend) in deciding about a contraceptive option.
Knowledge of sexual and reproductive health
One must first have some knowledge of sexual and reproductive health in order to access SRHS when needed, for example, one needs to know that contraceptives exist and how they work before seeking to access them. Prior to starting the interview, each participant was asked whether they had received sex education in school. Nineteen of the 45 participants (42%) said they had received sex education in school while 13 (29%) had not; the remaining 13 participants (29%) explained that they had received “more or less” or “very bad” sex education. As the following excerpt from Manuel illustrates, some adolescents start from a more privileged position in comparison with participants who had never received sex education, whether from school or parents.
Manuel (20-year-old, Estrato 3)
When I was younger, when I was 12 years old, my mom hired a psychologist so she could talk to me about those themes (sexual and reproductive health). I don’t know if it was specifically to talk about those themes, but the psychologist talked to me about those themes. She explained how reproductive organs work. She explained how to make a child, she explained how to use a condom, contraceptive methods, about sexually transmitted infections. So yes, my mom paid this for me.
And did you like that your mom did that?
Yes, totally, absolutely. Because we can say that here, in Colombia, at 12 years old you don’t know anything about that. Absolutely nothing. You only know that you have a penis and that’s it. So yes, I find it cool.
Knowledge on how to access SRHS
The following interview excerpts show that many participants wished they had received education not only about sexual and reproductive health but also regarding how to access SRHS (e.g., information about whether an adolescent is allowed to access SRHS without their parents and how to do so).
Alvaro (17-year-old, Estrato 2)
So for you it is important that we teach you about your rights (to access SRHS)?
Yes sir, to help me do things responsibly.
Did they teach you about your rights in the sexual education you received in school?
Well, they said “you have rights” and that’s it. They taught me other things, but they never explained our rights nor how to care for our rights (on how to access SRHS).
You would have liked for this be part of your sexual education?
Yes sir, I would have appreciated that.
Juliana (20-year-old, Estrato 4)
You didn’t know about Profamilia? (in relation to a 15-year-old friend asking the participant at 15 years old for help to get an abortion 2 )
I didn’t know Profamilia. Exactly for this lack of information. I only knew the “Pharmacy 3 Bad Death” (la farmacia mala muerte). So I brought her there and it was very traumatizing for her because it wasn’t a legal way, the pharmacy was underground.
It was done through pills?
Yes, it was through pills. But she was in her third month, so it was something very horrible for her. And if we would have had better information, we wouldn’t have done it like that. She wanted to get an abortion, but her mom was super Catholic, so we were not able to ask for help. The baby was already quite big, my friend went to the bathroom and it came out in parts. It was super traumatizing. I was with her the whole time. We had to go to the hospital because the baby was coming out in parts [. . .] We had to go sell a gold ring in a shop to pay for the pills. We lived in a precarious neighborhood, we didn’t have information, and abortion in this neighborhood is seen like sinful. So it was super difficult. I say that if we would have had more information, we wouldn’t have made this huge mistake by going to an underground pharmacy.
Assistance to access SRHS
While some participants were unfamiliar with some aspects of how to access SRHS (e.g., their rights), others had the help of a parent to access SRHS.
Juan Martin (16-year-old, Estrato 3)
Have you ever used sexual and reproductive health services?
Yes
At what age was your first time?
Since I was 12 years old.
And where was it?
At Profamilia. They gave me condoms and they also gave condoms to my dad and he gave them to me.
So the first time was at 12 years old?
Yes. It is my dad that went there because in my school they did not give out condoms. So Profamilia gave them to my dad and after he gave them to me.
Is it you who asked for them or your dad gave them to you?
I asked my dad for the condoms.
Miguel (22-year-old, Estrato 3)
At what age was that (first time to access SRHS)?
I was 20 years old
Did you go alone?
I went alone, but it was my mom who scheduled the appointment.
It was your mom who scheduled the appointment?
Yes, it was my mom who wanted me to go. It was her who asked for the appointment with joven sano (health program for youth focusing on sexual and reproductive health, for example, HIV testing).
What is your opinion that your mother took this decision for you?
Let’s see . . . I should have scheduled the appointment once I had started my sexual life, but there hadn’t passed that much time either since I had started it. However, I think it’s important that parents be interested in the sexual health of their kids, or whichever theme. If the son doesn’t schedule the appointment, the parents should do it. For me it seems important.
Francia (22-year-old, Estrato 3)
At what age was the first time (using SRHS)?
It is my mom who got me started by buying me injections for family planning at 15 years old. When she asked if I had a boyfriend, it had already been a year and a half I was with him, so I replied that I did have a boyfriend and I had already been intimate with him.
She asked you that?
Yes. It was quite uncomfortable, but she asked me. She did it by phone. She called me and asked me, so I told her.
And why was it not in person?
I don’t know. Like I was telling you before, maybe it’s because of the lack of education on the topic. For example, my mom told me that she didn’t have this conversation when she was pregnant at 19 years old. So she is with this fear, this fear that the same thing that happened to her, will happen to me. So she asked me, I told her “yes,” and she said “alright, we’ll start (family) planning with the injections” and she didn’t let me choose anything. Everyone has different ways to do (family) planning and in my case it wasn’t like that, “you’re going to start with this and that’s it.”
So it is her who chose for you?
Exactly. And I asked her why this way and she replied that one of her friends uses injections. So I started to use them every month at the EPS (subsidized health promoting entities in Colombia).
And when you would go to the EPS, would you go by yourself or with your mom?
By myself.
As the previous example illustrates, some adolescents had their parents make decisions for them regarding access to SRHS, limiting or supplanting the adolescent’s autonomous decision making. Some appreciated the involvement of parents, whereas others, such as Francia, disliked this involvement by a parent. Other participants wanted a stronger implication on the part of their parents (mothers in this case), but it was impossible for them to have such assistance for different reasons (e.g., contextual, personal beliefs).
Isabella (14-year-old, Estrato 2)
Do you have any barriers to access sexual and reproductive health services?
Yes, my mom. My mom doesn’t let me.
And why won’t she let you?
She says I am not at an age to plan (planificar).
And you don’t want to go to the clinic anyways?
No. No I didn’t do it because I want to respect her point of view. I want to respect the opinion of my mom.
You would like for her to go with you to the clinic?
Yes, I would much prefer that.
Mariana (19-year-old, Estrato 1)
Did you go by yourself (the first time to use SRHS at 19 years old)?
Yes
Did you want to go by yourself?
Well, I wanted to go accompanied, but my mom told me “no.”
Why?
She said that I had to go by myself because I am at a new stage in life.
But you wanted your mom to go with you?
Yes, so that she could be part of the whole process.
Elena (22-years-old, Estrato 2)
At what age was the first time (to access SRHS)?
At 18.
Did you go by yourself or with your parents?
I went alone.
Was it important for you to go alone?
No. The truth is I was in Argentina, I wasn’t here.
Your parents weren’t in Argentina with you?
No.
But if you would have had the possibility, you would have preferred to go with your parents?
Yes, I would have liked to go with my mom.
While some participants wanted a parent present when accessing SRHS, others like Ariel and Bianca did not want to be accompanied by a parent.
Ariel (21-year-old, Estrato 3)
Yes, I went by myself (to get contraceptive pills at 15 years old).
Was this important for you to go by yourself?
Yes, I wanted to go by myself. I decided to go by myself because I didn’t know how my dad was gonna take it, because if you are doing family planning it is obvious that you are sexually active and that can generate conflict with parents. I didn’t want to worry them either. I had easy access to the contraceptive, so I went by myself.
[. . .]
And after, when you had that bad reaction to the contraceptive pills, did you also go alone to see the gynecologist?
No. For that I had to go with the wife of my dad. She accompanied me in the process.
But you wanted to go alone?
Yes. Actually, there was something that I didn’t like. They did a transvaginal echography and she was present for that procedure and that was very uncomfortable, and I did not like it. Beyond a question of being young or an adult, it is my sexuality.
How old were you?
15 years old. I wasn’t a child, but it is my sexuality, my privacy, and I should have been able to decide if I want to be accompanied or not.
Bianca (22-year-old, Estrato 2)
The first time you went, did you go alone or accompanied (at 19 years old)?
Alone
Was that important for you to go alone?
I wanted to go alone because it was a decision in relation to my sexual life, so something very private with my health.
Unequal opportunities to exercise autonomy
From the participants’ interviews, their understanding and recognition of autonomy are highly contextual and depend on personal experiences. This means that they have unequal opportunities, particularly regarding access to SRHS. For example, 16-year-old Rafael’s father had died, and his mother was obliged to work long hours, sometimes 6 to 7 days a week. Similarly, when Jaime was a young adolescent, he was alone at home for long periods without a parent present. In such situations, it would clearly be very challenging for an adolescent such as Rafael or Jaime to have a parent accompany them to a clinic for SRHS. Another example is that of 12-year-old Juan Martin, whose father got him condoms at Profamilia when he asked for assistance, while 14-year-old Isabella wanted her mother’s help to access contraceptives but did not have the same possibility because her mother refused for her daughter to be sexually active.
Participants shared these and other examples of unequal opportunities associated with their personal preferences regarding how to access SRHS. Some wanted the assistance of a parent but could not have it, others had such assistance available should they wish, while others explicitly stated wanting to access SRHS alone, but not always being able to do so. From a reproductive justice framework, this reality represents two serious ethical challenges:
Adolescents have unequal opportunities to access SRHS based on various contextual factors (e.g., unavailable parent to accompany them to the clinic).
Adolescents do not have their personal preferences equally respected in terms of autonomy in their access of SRHS.
While some participants described themselves as more autonomous than others, many still wanted or appreciated the assistance of a parent to access SRHS (e.g., scheduling the appointment for them or accompanying them to the clinic). Other participants described themselves as having less autonomy but would have preferred to access SRHS independently. Thus, participants’ responses showed that their perception of whether or not they have complete (or almost complete) autonomy does not correlate with their wish to access SRHS independently (i.e., without a parent).
Adolescents may see themselves as very autonomous, but still want to be accompanied by or have the assistance of a parent to access SRHS. This observation challenges some of the common critiques in bioethics of third-party involvement in medical decision making that have sought to limit medical or parental paternalism to protect individual autonomy and freedom. Nonetheless, for the adolescent participants in our study, the majority (although not all) saw the involvement of their parents in access to SRHS as welcomed or even desired. This finding is different from the experiences identified in similar research conducted on the topic in other cultural contexts, such as in North America, where adolescents generally did not want their parents’ involvement and saw this as a constraint on their autonomy to access to SRHS (Lehrer et al., 2007).
Ethical Analysis Based on a Reproductive Justice Framework: The Need to Foster Adolescents’ Autonomy to Access SRHS
Respect for autonomy means allowing adolescents to make choices based on their needs and preferences. Respect for justice means they should have equitable opportunities to access SRHS and have their preferences respected. How can we address the ethical challenges related to adolescents’ unequal opportunities to autonomously access SRHS? In 2017, the WHO introduced the Global Accelerated Action for the Health of Adolescents (AA-HA!). The objective of AA-HA! is to develop initiatives to ameliorate the health of adolescents. Within AA-HA!, the WHO suggests “fostering the autonomy” of adolescents to empower them to access health services to protect them from potential harm. However, the AA-HA! lacks in-depth ethical justifications for why and how the autonomy of adolescents should be fostered. The present study shows the ethical pertinence of fostering autonomy to access health services, to help promote equity by ensuring adolescents have equal opportunities to access SRHS regardless of their unique life circumstances.
From the stories participants shared, it is evident that they did not have the same opportunities to access SRHS based on their own preferences. Some were taught how to access SRHS or even appreciated having their parents schedule appointments for them, which supported their autonomy. Others had limited autonomy because they had no knowledge about how to access SRHS or because parents made decisions for them without taking into consideration their own wishes.
One possible way of fostering adolescents’ autonomy to access SRHS in their community would be through educational initiatives, notably within a sex education curriculum. Historically, sex education for adolescents has focused on prevention (e.g., prevention of sexually transmitted infections [STIs] like HIV, and pregnancy with condoms). However, there has not been the same effort to discuss and provide knowledge to adolescents regarding the principle of autonomy and decision making in health care (which should go beyond sexual and reproductive health) or explaining how to access SRHS if needed. For example, explain how to navigate one’s local health care system and teach adolescents about their rights and limitations to access SRHS, such as clarifying whether or not parental consent is required. Since during adolescence one starts to develop more independence and maturity, it is crucial that adolescents be provided with the knowledge on how to access health services and how to exercise their rights in medical contexts (e.g., the right to ask questions of health care professional, the right of confidentiality). As the ethical principle of autonomy constitutes a core principle in health care, a person should not have to wait to reach adulthood to be taught the value and application of autonomy in health care.
A concrete example of a previous intervention that demonstrated the pertinence of engaging in initiatives to foster adolescents’ autonomy to access SRHS is Meuwissen et al.’s (2006) quasi-experimental intervention study in Nicaragua. Adolescent girls from disadvantaged contexts in Managua were given vouchers to access SRHS. The vouchers “could be used for 1 consultation and 1 follow-up visit for counseling, family planning, pregnancy testing, antenatal care, STI treatment, or a combination of these services” (Meuwissen et al., 2006, p. 56.e2). Compared with participants who did not receive vouchers, those with vouchers had significantly higher access to SRHS, which led them to increased use of contraceptives. Such an intervention highlights how providing tools to foster adolescents’ autonomy to access SRHS can have very beneficial results. Taking Meuwissen et al.’s intervention into consideration for the present study, it is thus fair to suggest that by educating adolescents about their rights and autonomy to access SRHS, this would likely lead to increased access to SRHS, because when needed these adolescents would possess the required knowledge to exercise their autonomy.
Another challenge emerging from the data is related to the role of parents. If an adolescent wishes to be accompanied to a clinic by their parents, but the parents are unavailable or do not wish to assist in accessing SRHS, another ethical issue arises, namely, parents’ rights and obligations in the context of their child’s sexual and reproductive health. This would require further research, particularly with parents themselves (e.g., exploring their understanding of their adolescents’ autonomy to access SRHS). Some parents may prohibit their adolescent from accessing SRHS, for example, because of cultural or religious beliefs, whereas others may accompany their adolescents to clinics. This discordance between the experiences recounted by our participants highlights other important and complex ethical challenges raised by adolescents’ access to SRHS. It points to the need for further research on the topic, especially because the reproductive justice framework is not obviously equipped to address this ethical question.
To highlight the complexity surrounding these questions, we may use the previous examples of Isabella (14 years old) and Juan Martin (12 years old). Isabella’s mother did not want her to use contraceptives, because she believed her daughter was too young, whereas Juan Martin was given condoms by his father when asked for them at an even younger age. It is possible to observe some clear differences between the two young adolescents’ access to contraceptives. Both participants display a form of autonomy in wanting to use contraceptives, yet the parents’ reactions are quite different, which in turn influences their access to SRHS. This research did not interview the parents of adolescents to understand their perceptions of their adolescents’ autonomy to access SRHS. Notwithstanding, cultural understandings of gender arguably shape approaches toward the question of adolescents’ autonomy to access SRHS. Throughout Latin America, robust gendered roles and ideologies are present, which are commonly known as marianismo (Englander et al., 2012; Stevens & Pescatello, 1973) and machismo (Gutmann et al., 2002). Marianismo pushes for women to be virgins, passive with men, and to become wives and mothers, whereas machismo pushes men to be assertive and sexually adventurous with women. If such gendered ideologies are transposed to adolescents, this can perhaps explain why Juan Martin’s father got him condoms at 12, but Isabella’s mother refuses for her 14-year-old to get access to contraceptives. If adolescents have unequal access to SRHS based upon a gendered ideology held by their parents, the situation makes it profoundly unjust from a reproductive justice perspective. It further points to the need to engage in initiatives with parents to help address the issue, perhaps through educative interventions with the parents of adolescents, although more research is needed on the topic.
Limitations
It is important to take into consideration the limitations of this study. One critical limitation is the sample’s representation bias. There are many significant socio-demographic differences across Colombia, some of which are particularly important to consider regarding adolescents’ extreme vulnerability due to poverty and violence (Higgs, 2020). Colombia has one of the world’s highest rates of internally displaced people—approximately a tenth of the Colombian population has been displaced because of internal conflict (Reyes et al., 2019). Arguably, Colombian adolescents’ autonomy to access SRHS varies between those living in precarious contexts with limited resources and more prevalent paramilitary presence, and those in stable contexts with more resources. There are adolescents in much more privileged situations, such as those from the upper estratos, who might have very different experiences; however, no adolescents from the Estratos 5 and 6 participated in an interview for this research. As such, this study’s conclusions cannot be generalized for the whole Colombian population due to the limited sample size and the locations of data collection—For example, the Pacific coast and the Caribbean coast have different cultural contexts than the capital Bogota or the Amazonian region. Future research on the topic should look into exploring the question with different socio-demographic groups of adolescents and also compare with similar studies in other Latin American countries.
Another source of potential bias is single interviewer and data coding; a double coding approach could have helped improve reliability. Such factors should be taken into consideration for future research.
Conclusion
Global health literature has shown that adolescents insufficiently use health care services despite having important health-related needs that can and should be addressed (Mazur et al., 2018; Patton et al., 2016). There are many reasons for this phenomenon, some of which are connected to adolescents’ autonomy to access health care services, such as parental consent laws, economic barriers, and lack of knowledge on how to use health care services. As the findings of our study show, Colombian adolescents have diverse experiences and understandings regarding autonomy when it comes to accessing SRHS. From a reproductive justice framework, unequal opportunities to access SRHS represent a serious ethical challenge.
To address this challenge, we argue in favor of fostering adolescents’ autonomy to access health care services, for example, through educational initiatives. As shown by other studies, education is one of the greatest determinants of adolescent health (Viner et al., 2017). UNESCO’s (2018) International technical guidance on sexuality education underscores the importance for comprehensive sex education for adolescents to be based on a human rights approach and to develop life skills needed to support healthy choices. As our findings and those of other studies show, it is essential to engage in initiatives with adolescents to promote their knowledge around the concept of autonomy and how to access SRHS, namely, in the name of equity for adolescents.
Furthermore, on a policy level, recognition of and respect for autonomy should be anchored in a more nuanced understanding of adolescents’ preferences, which can legitimately involve (a) accessing SRHS by themselves, that is, autonomy as independence (a model often advocated in North America and Europe) or (b) being accompanied by a parent (or another person) in accessing SRHS. The present study did not interview parents of adolescents. However, the answers of participants underscored that parents seem to play a crucial role around the question of adolescents’ autonomy to access SRHS. Future studies should investigate how to mobilize or engage with the parents of adolescents to help foster the autonomy of adolescents to access SRHS. One possibility might be through comprehensive sex education for parents of adolescents.
Footnotes
Appendix
Demographic Profile of Participants.
| Demographic characteristics | n (%) |
|---|---|
| Gender | |
| Man | 21 (46.7%) |
| Woman | 23 (51.1%) |
| Non-binary | 1 (2.2%) |
| Age | |
| 14 | 1 (2.2%) |
| 15 | 4 (8.9%) |
| 16 | 5 (11.1%) |
| 17 | 2 (4.4%) |
| 18 | 3 (6.7%) |
| 19 | 11 (24.4%) |
| 20 | 2 (4.4%) |
| 21 | 10 (22.2%) |
| 22 | 5 (11.1%) |
| 23 | 2 (4.4%) |
| Estrato | |
| 1 | 3 (6.7%) |
| 2 | 12 (26.7%) |
| 3 | 25 (55.6%) |
| 4 | 4 (8.9%) |
| 5 | 0 (0.0%) |
| 6 | 0 (0.0%) |
| Unknown | 1 (2.2%) |
| Residence of participants | |
| Medellin, Antioquia (large city) | 9 (20.0%) |
| Rionegro, Antioquia (small city) | 6 (13.3%) |
| Santa Fe de Antioquia, Antioquia (rural area) | 5 (11.1%) |
| Cali, Valle del Cauca (large city) | 2 (4.4%) |
| Palmira, Valle del Cauca (small city) | 23 (51.1%) |
| Total | 45 |
Acknowledgements
The authors would like to thank all the workers at Profamilia, especially Claudia Patricia Pérez, who have helped with the development of this research. Their support is tremendously appreciated. The authors would also like to thank all the participants who generously volunteered their time to participate in this research. The first author would like to thank Alejandra Trossero at UNICEF who helped spark a strong interest in adolescent health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was financed by Julien Brisson’s Canadian Doctoral Award to Honour Nelson Mandela awarded by the Canadian Institutes of Health Research (201610GSD-385545-283387).