
Abstract
Despite the well-documented overrepresentation of Latine adolescents in the child welfare system and inequities in their behavioral health outcomes, Latine families experience significant barriers to accessing evidence-based behavioral health care. Limited culturally- and linguistically responsive family-based telehealth services contribute to lower service access rates for Latine systems-impacted adolescents. The present pilot study addresses this gap through culturally adapting an existing, empirically informed family-based intervention, and assessing the feasibility and acceptability of delivering the intervention via telehealth to Latine families impacted by the child welfare system. We conducted a pilot feasibility/acceptability trial of the intervention with eleven Spanish-speaking Latine caregivers and four bilingual Latine adolescents. Families’ and clinicians’ session feedback forms and data collected from individual qualitative exit interviews informed the iterative cultural adaptation process and telehealth intervention feasibility/acceptability outcomes. On session feedback forms (n = 67 caregiver forms; n = 27 adolescent forms), eleven caregivers and four adolescents reported strong acceptability for telehealth sessions and clinicians. Clinicians were rated highly on showing support, listening, answering questions, encouraging discussion, giving information, and keeping sessions interesting (scale = 1–5; average ratings were 4.6–5.0 across domains). Caregivers reported high levels of satisfaction with the telehealth services they or their families received (M = 4.6, SD = 0.4; 1 = strongly disagree to 5 = strongly agree). Themes from qualitative interviews suggest caregivers found the intervention helpful, particularly in improving their emotion regulation and communication with their adolescents. Cultural adaptation of telehealth interventions for Latine families impacted by the child welfare system is feasible, acceptable, and has the potential to fill gaps in behavioral health services access.
Public Significance Statement
A culturally adapted telehealth intervention for Latine Spanish-speaking families with adolescents involved in child welfare system improved caregivers’ perceptions of their communication and emotion regulation. Acceptability and feasibility ratings from caregivers and adolescents suggest this intervention can be successfully delivered via telehealth and its intervention content is helpful in improving caregiver-adolescent relationships.
Latine adolescents are overrepresented in the United States’ (U.S.) child welfare and juvenile legal systems, making up 22% of adolescents in juvenile legal facilities, including residential treatment centers, detention centers, training schools, and juvenile jails and prisons, and 22% of adolescents in foster care (Hockenberry et al., 2016; Sickmund et al., 2017; United States Children’s Bureau, 2024). Not only has contact with the child welfare system and incarceration increased for Latine adolescents over the last 20 years, but there is disproportionate contact with the juvenile legal system for Latine adolescents relative to non-Latine white adolescents. Meanwhile, Latine adolescent system involvement has doubled in multiple U.S. states, including California (Sickmund et al., 2017).
Barriers to Care for Systems-Impacted Latine Adolescents
Many systems-impacted adolescents (i.e., child welfare, juvenile legal) have elevated behavioral health needs (e.g., depression, substance use) and systems-impacted Latine adolescents experience significant inequities in behavioral health services access and engagement relative to non-systems-impacted Latine adolescents (Duong et al., 2021; Garland et al., 2005; Villagrana, 2017). Although studies examine ethnoracial disparities in behavioral health access and utilization (Lu et al., 2021), they often exclude Spanish-speaking families (Garland et al., 2005) and homogenize Latine subgroups (i.e., Mexican, Cuban, Puerto Rican) into one monolithic group. As a result, they are likely not representative of all Latine families, particularly those less likely to utilize behavioral health services, such as monolingual Spanish-speaking families who are less acculturated to the host culture. In a recent qualitative study, conducted in Spanish and English with formerly incarcerated Latine adolescents in the reentry process and their caregivers, Barnert et al. (2020) highlighted that legally involved Latine families experience significant barriers when attempting to access behavioral health services, including fear of deportation due to their immigration status. Garcia et al. (2015), who also focused on child welfare-impacted adolescents, identified lack of cultural competence among providers as a significant barrier to access of effective behavioral health treatments. A lack of services delivered in Spanish is another barrier to behavioral health services’ access for Latine families with adolescents involved in the juvenile legal system (Barnert et al., 2020), which is particularly salient given half of all Latine adolescents involved in the child welfare system are Spanish speaking (Villagrana, 2017).
System-level factors also impact Latine adolescents and families’ ability to engage in evidence-based, culturally responsive treatment. Adolescents are often involved in multiple systems and can fall through the cracks, given challenges with information-sharing and cross-system collaboration (Hirsch et al., 2018). Up to two-thirds of legally involved adolescents have also been involved in the child welfare system at some point in their lives (Herz et al., 2019). Adolescents who are dually involved in the juvenile legal and child welfare systems are disproportionately Latine, have more out-of-home placements, and experience higher recidivism rates than adolescents impacted only in one of these systems (Herz & Dierkhising, 2018). Only an estimated 57% of dually-impacted adolescents access mental health services, regardless of risk level (Hirsch et al., 2018).
Evidence-Based Treatments for Systems-Impacted Adolescents
There is ample evidence documenting the effectiveness of family-based treatment for English-speaking systems-impacted adolescents in improving mental health, substance use, and educational and delinquency outcomes (Yang et al., 2024). Multisystemic Therapy (Ali et al., 2022; Henggeler, 2012), for example, is an efficacious family-based intervention for adolescents with possible problematic substance use who are impacted by the juvenile legal system or are at-risk for out-of-home placement. Unfortunately, such interventions are intensive and not always feasible to implement in often over-burdened and under-resourced settings. Further, a recent systematic review and meta-analysis highlighted that these evidence-based treatments are not available for Latine Spanish-speaking families who need them (Littell et al., 2021). To date, only Familias Unidas, a manualized culturally adapted intervention targeting substance use and sexual risk behavior among Latine adolescents, has been rigorously tested in five different randomized controlled trials (Estrada et al., 2017; Pantin et al., 2003, 2009; Prado et al., 2007, 2012) and was tested for delivery via an online platform (Estrada et al., 2019). While this intervention was not developed for systems-impacted adolescents, one trial found it was efficacious among Latine adolescents who had been previously arrested in reducing past 90-day substance use compared to standard care (Prado et al., 2012). Another recently published study focusing on a family-based, culturally adapted, intervention for youth facing powerful environmental stressors (Culturally Informed and Flexible Family-Based Treatment for Adolescents [CIFFTA]) found significant improvements in family communication and reductions in family conflict (Mena et al., 2024). Although the Familias Unidas and CIFFTA interventions address important cultural adaptation strategies (e.g., delivered in Spanish, targets culturally specific risk factors like acculturative stress), they are intensive (e.g., Familias Unidas is administered over a 12-week period, eight 2-hr multi-parent group sessions and four 1-hr family visits) and do not address the specific barriers experienced by families of adolescents with out-of-home placements. This is a critical gap in access to address given that Latine adolescents are disproportionately impacted by the juvenile legal and child welfare systems and that meta-analytic evidence supports stronger effectiveness for culturally adapted treatments (Arundell et al., 2021; Hall et al., 2016), particularly for culturally adapted digital/telehealth interventions (Ellis et al., 2022) and for culturally adapted substance use treatments for Latine adolescents (Hernandez Robles et al., 2018).
Although not originally available in Spanish, one brief family-based intervention designed for adolescents involved in juvenile drug court and their caregivers, demonstrated reductions in adolescents’ cannabis use and sexual behaviors that increase risk for HIV and other sexually transmitted infections (STIs) is Project Risk Reduction for Adolescents and Parents (RAP; Tolou-Shams et al., 2017). Project RAP is a 5-session family-based intervention based on emotion regulation (Gratz & Roemer, 2004) and social-personal frameworks (Steinka-Fry et al., 2017). The intervention is grounded in the conceptualization that emotion dysregulation is associated with greater substance use and sexual activity that increases likelihood of contracting HIV and other STIs (Devieux et al., 2002; Lucenko et al., 2003). Additionally, it recognizes adolescence as a period of significant emotional, cognitive, and physical changes, considering the interplay between individual, social, and environmental risk. This intervention was recently adapted for telehealth delivery with English-speaking adolescents and families impacted by the child welfare system through the pilot Family Telehealth Project (FTP; Folk et al., 2024; Leo et al., 2023) and found to be feasible and acceptable. Indeed, telehealth interventions hold significant promise for addressing access barriers that disproportionately impact Latine families impacted by the child welfare system (Folk, Gill, et al., 2022; Folk et al., 2024; Leo et al., 2023). Despite potential benefits, no studies to date have examined the feasibility and acceptability of delivering a culturally adapted telehealth intervention for Latine families that are impacted by the child welfare system.
Present Study
To address the aforementioned service needs and barriers, we culturally and linguistically adapted the telehealth FTP intervention for Spanish-speaking families with systems-impacted adolescents (hereafter referred to as FTP-Spanish [FTP-S]). The FTP-S teaches caregivers and adolescents affect management and communication skills to promote healthier family relationships to improve downstream adolescents’ behavioral health outcomes. We hypothesized that families would find the culturally adapted intervention, delivered via telehealth, to be highly feasible and acceptable and would report improved communication and emotion regulation.
Methods
Participants
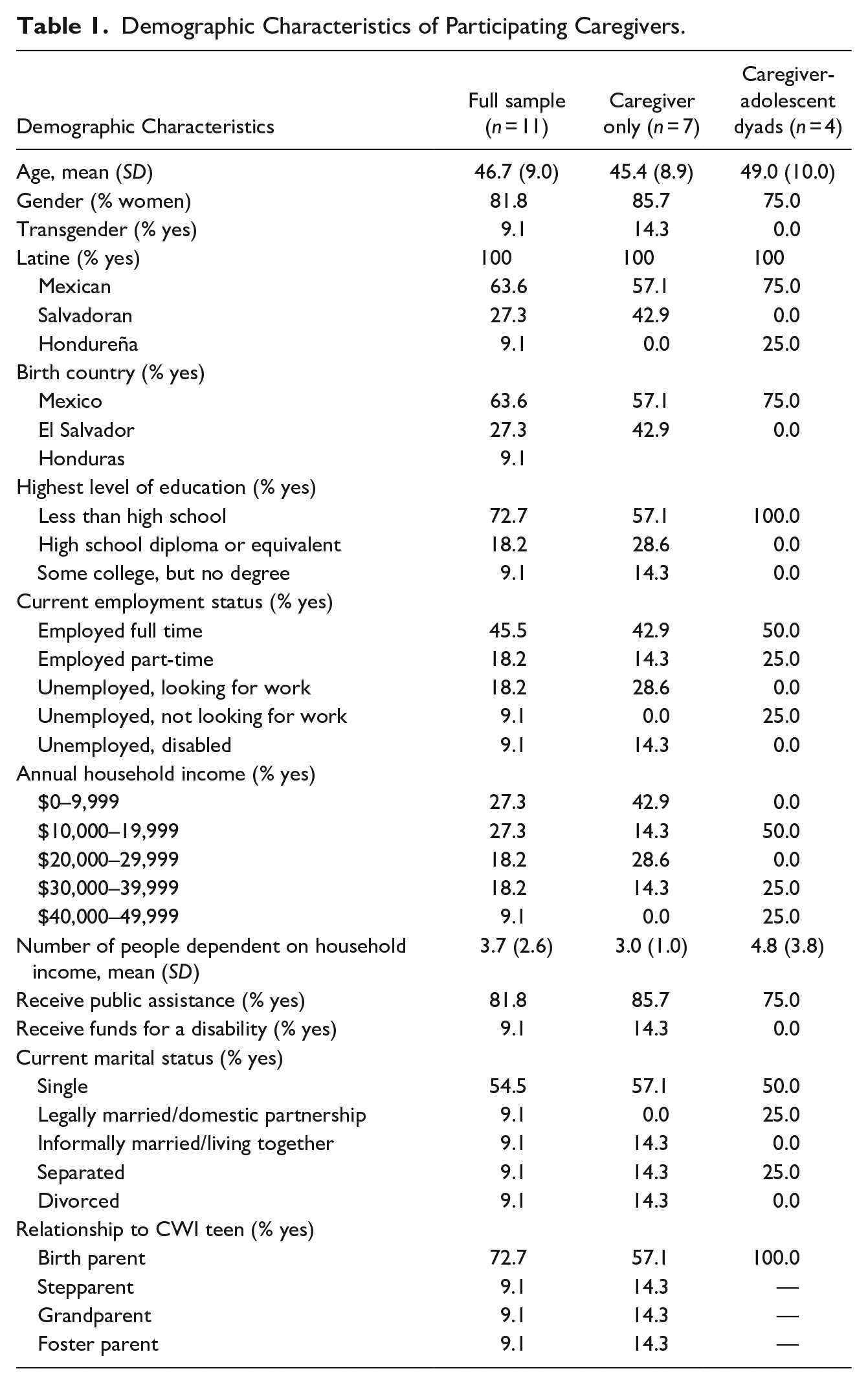
Participants included families involved in the child welfare system within the past 12 months with bilingual adolescents (ages 12–17 years) and Spanish-speaking caregivers. Caregivers (caregivers of origin, kinship caregivers, foster parents) were eligible to participate either individually (caregivers of origin only; n = 7) or with their adolescent (caregivers of origin, kinship caregivers, foster parents, n = 4 dyads). Participating caregivers (n = 11) were predominately birth parents (72.7%) and on average 47 years old (SD = 9 years). Most (81.8%) identified as women and 9.1% (n = 1) identified as transgender. All caregivers were Latine (63.6% Mexican, 27.3% Salvadoran, 9.1% Honduran) and immigrants (from the corresponding countries to ethnic identities). Nearly all (90.9%) had lived in the mainland U.S. for more than 10 years and all identified very closely with other people from their ethnic origin (1 = very closely to 4 = not at all). Over half (54.6%) of caregivers reported an annual household income under $20,000, with on average 3.7 people (SD = 2.6) dependent on this income; 81.8% received public assistance. Participating adolescents (n = 4) were predominately girls (75%), on average 15 years old, and identified as 100% Latine (75% Mexican, 25% Salvadoran, 25% Honduran) and 75% identified as LGBTQ. One adolescent reported they had previously been arrested. All participating adolescents were born in the U.S. and 50% were in a group home placement at the time of their pre-treatment assessment. Additional demographic characteristics are displayed in Table 1. The present study of human subjects was approved by the Institutional Review Board at the University of California, San Francisco (UCSF).
Demographic Characteristics of Participating Caregivers.
Family Telehealth Project Intervention
The FTP intervention, which served as the basis for the present cultural adaptation, was adapted from an existing empirically supported intervention, Project RAP (Tolou-Shams et al., 2017); see telehealth adaptation description in Folk et al. (2024). Adapting the intervention’s English version was conducted iteratively in collaboration with key systems partners (child welfare supervisors, probation officers, judges, attorneys, school wellness staff) and through an open trial of the intervention (Folk et al., 2024; Leo et al., 2023). A caregiver-only version of the intervention was also created, covering the same core content and structure, to be implemented when adolescents are unable to or not interested in participating.
The FTP intervention (procedures described in Folk et al., 2024) involves an initial engagement session, four core individual and family sessions and individual and family booster sessions delivered 3 weeks after the core intervention. Sessions were 1 hr in length, totaling 11 hr of intervention time per person. Core session content includes affect management, parental monitoring, and communication skills. Content topics are displayed in Table A1, by session. The intervention focuses on teaching caregivers and adolescents the same affect management skills (i.e., ability to effectively manage and change the way they feel and cope with various situations) to promote healthier caregiver-adolescent relationships and a more positive family environment that will thereby improve adolescents’ outcomes. Parents or caregivers of origin had the option to enroll in either the dyadic or individual caregiver version of the intervention, while kinship and foster caregivers were only eligible to complete the individual caregiver intervention. The caregiver-only version of the intervention covers parallel content, though does not include any adolescent or family sessions (caregiver only version is total of 6 intervention hours).
Cultural Adaptation Process
Culturally adapting the FTP intervention, which we refer to as FTP-Spanish (FTP-S) was guided by successful cultural adaptation frameworks (Bernal et al., 1995; Domenech-Rodríguez & Wieling, 2005) and included iterative revisions and adaptation based on pilot work, observation, and feedback. We addressed the eight cultural adaptation elements for Latine population interventions outlined by Bernal et al. (1995): (a) language (culturally appropriate, culturally syntonic); (b) persons (role of ethnic/racial similarities and differences between client and therapist in shaping therapy relationship); (c) metaphors (symbols and concepts shared with the population; sayings or “dichos” in treatment); (d) content (cultural knowledge: values, costumes and traditions; uniqueness of diverse Latine groups); (e) concepts (treatment concepts consonant with culture and context: dependence vs. interdependence vs. independence; emic over etic); (f) goals (transmission of positive and adaptive cultural values; support adaptive values from the culture of origin); (g) methods (development and/or cultural adaptation of treatment methods); and (h) context (consideration of changing contexts in assessment during treatment or intervention: acculturative stress, phase of migration, developmental stage; social supports and relationship to country of origin; economic and social context of intervention). See Table A2 for details on the adaptation process.
First, we linguistically adapted the intervention (surface-level cultural adaptation) so the caregiver and family components could be delivered in the caregivers’ preferred and native language. To increase engagement, we also culturally matched families with behavioral health providers who were predominantly Latine and native Spanish speakers (surface-level adaption). Second, we incorporated content for culturally-relevant factors (e.g., intergenerational acculturation conflict) that have been implicated in the risk of family conflict in Latine adolescents as part of our intervention (deep-level adaption; see Santisteban & Mena, 2009; Santisteban et al., 2013). Lastly, through the qualitative interviews presented in this manuscript we elicited in-depth feedback from participating adolescents and families to ensure their perspectives and lived experiences were appropriately incorporated into the iterative cultural adaptation process. Further, we engaged clinicians who had extensive experience working with Latine families, understood the unique risk factors associated with adolescent systems involvement, and had experience delivering the present intervention in the iterative cultural adaption process.
Recruitment
Adolescents and caregivers were referred by organizations serving systems-impacted families in California. Eligible adolescents and families were restricted to those in in California due to the study clinicians’ licensure status. In addition to self-referrals, referrals were accepted from community-based organizations, short-term residential treatment programs and group homes, outpatient clinics affiliated with academic medical settings, and a national organization that serves foster youth and their caregivers.
Procedures
Intervention procedures are consistent with those described elsewhere (Folk et al., 2024). Dyadic participants were assigned two clinicians, one to meet individually with the adolescent and the second to work with the caregiver, and then both clinicians co-lead the family sessions, which allowed for shared skill-building, practice, and discussion. Caregivers who participated individually were only assigned an individual clinician. Clinicians were employees or trainees through the University of California, San Francisco (UCSF). Sessions were held at the convenience of participants, via zoom, typically on a weekly basis, during a 3-month intervention period.
Participants were asked to complete feedback forms immediately after each session that assessed acceptability of specific intervention activities and were used to inform iterative cultural adaptation; participants were compensated $10 for each completed feedback form. Clinicians also completed feedback forms each session to monitor fidelity and identify feasibility issues related to session content. Adolescents and caregivers were invited to participate in individual qualitative exit interviews to obtain in-depth feedback on the intervention; participants were compensated $50 for each interview. Qualitative interviews focused on metaphors, content, concepts, and goals, all dimensions of Bernal et al.’s (1995) cultural adaptation framework. For example, adolescents and caregivers were asked specifically about the perceived cultural relevance of concepts and content (e.g., video clips) used in the intervention. Adolescents and caregivers also completed baseline, post-treatment, and 3-months post-treatment measures of adolescent behavioral health and family functioning; participants were compensated $50 for each completed survey.
Feasibility and Acceptability Survey Measures
Demographics
All participants self-reported their gender and ethnoracial identities, age, and history of systems involvement.
Participant Session Feedback Forms
Participants provided feedback on acceptability of session content through a series of yes/no questions assessing whether they liked the session, found topics discussed important, or thought there were topics not discussed that should be included. Participants rated the helpfulness of specific activities (1 = not at all helpful to 5 = very helpful), their clinician (yes/no of whether they liked their clinician; 1 = poor to 5 = very good on specific clinical skills), and their comfort with telehealth technology (rated 1 = not at all comfortable to 5 = very comfortable; experienced any problems with the technology [yes/no]).
Clinician Feedback Forms
Clinicians completed feedback forms each session to identify issues related to feasibility of covering session activities and whether anything unexpected or adverse arose during sessions.
Telehealth Satisfaction Questionnaire (TSQ)
The 19-item TSQ (Stewart et al., 2021) assessed participant satisfaction with telehealth treatment; 15 items are rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree), 1 item is yes/no, and 3 are write-in questions. This measure has been used with ethnoracially diverse samples and has strong psychometric properties, including strong internal consistency (e.g., Cronbach alpha .80–.89; Villalobos et al., 2023).
Preliminary Outcomes
Preliminary outcomes assessed in this pilot trial were identified based on those in the original pilot efficacy trial of RAP (Tolou-Shams et al., 2017).
Difficulties in Emotion Regulation Scale-Short Form (DERS-SF)
The DERS-SF (Kaufman et al., 2016) an 18-item assessment of ability to manage feelings. Four dimensions of emotional regulation awareness and understanding of emotions were rated on a 5-point Likert scale (1 = almost never to 5 = almost always) and averaged to create a total score. There were six three-item subscales: Strategies, Nonacceptance, Impulse, Goals, Awareness, and Clarity. Higher scores reflect greater difficulty with emotion regulation, with the exception of the Awareness subscale items, which were reverse-scored to be consistent with the remaining subscales.
Parent-Adolescent General Communication Scale (PAC)
The PAC (Barnes & Olson, 1985) is a 20-item assessment of parent-adolescent communication with two subscales: Positive (7 items) and Negative (13 items) aspects of communication. Statements are rated on a 5-point scale (1 = never to 5 = always) and scores are summed to create subscale scores. Higher subscale scores reflect greater positive and negative communication, respectively.
Intergenerational Acculturative Conflict (IAC)
The IAC (Lee et al., 2000) is an 18-item assessment of intergenerational acculturation family conflict. Caregivers were asked to rate their intergenerational conflict with the participating adolescent (or for caregiver-only participants, the adolescents identified at baseline meeting study eligibility criteria) from 1 (almost never) to 5 (almost always) and summed to create an overall score; higher scores reflect a greater degree of conflict. The IAC scales has been used in previous studies with Latine samples (Meza et al., 2024).
Quantitative Analysis
Survey data was collected in REDCap and managed in SPSS and R. All analyses are descriptive and given the small sample size of adolescent participants (n = 4), reflect caregiver report only (n = 11). Individual trajectories on caregiver-rated preliminary outcomes were examined using parallel coordinate charts at baseline, post-intervention, and 3-months post-intervention time points. Charts were created in R using the GGally package’s (Schloerke et al., 2022) ggparcoord() function. Participant trajectories were stratified by the caregiver only or dyadic intervention (see Figure 1). Figure 1 represents only caregivers with complete data at all timepoints (n = 10).
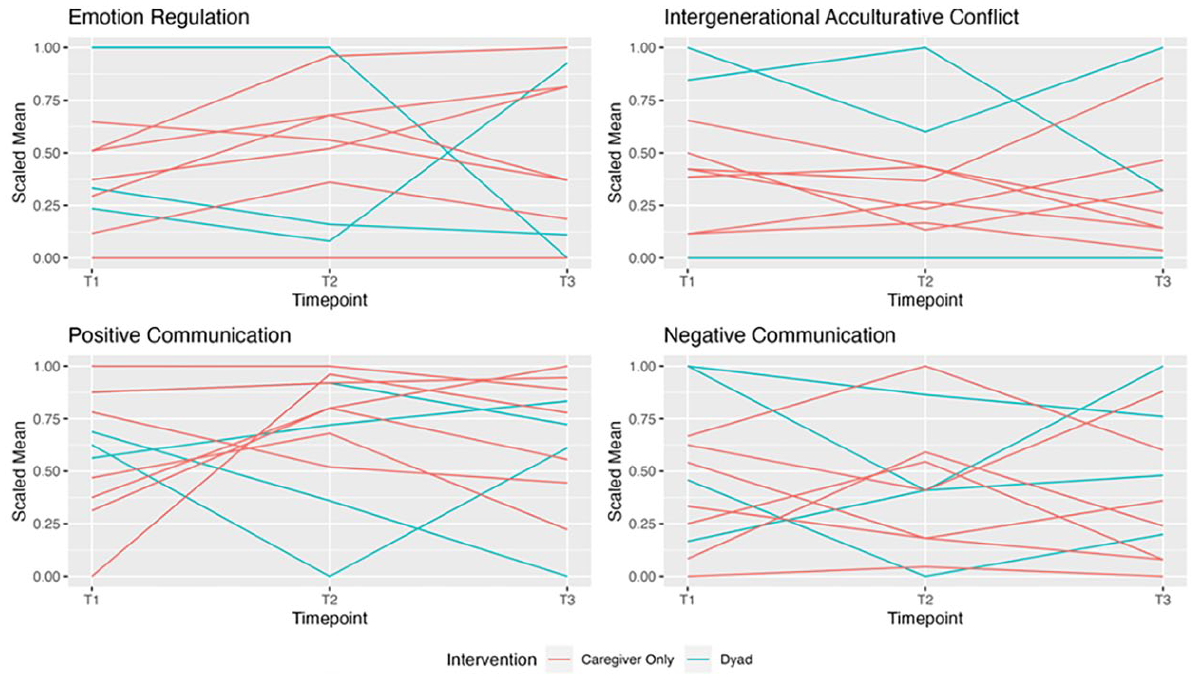
Parallel coordinate charts for main outcomes stratified by intervention type.
Qualitative Analysis
We adopted purposive sampling methods to ensure we captured the narratives of participants from various countries of origin (e.g., Puerto Rico, Central America, Mexico), diverse caregiving relationships (e.g., parent, grandparent), and varying spans of time involved with the child welfare system. Themes were extracted from qualitative interviews using ATLAS-ti, a qualitative analysis software, for coding, text retrieval, intensive data management, and analysis. An initial themes codebook was developed using the cultural adaptation framework and qualitative exit interview guide. Interviewers also developed in vivo codes from participants’ responses as they coded interview transcripts. In vivo codes are useful for understanding colloquialisms and other specialized vernacular that may not have an exact translation available in English (Manning & Kunkel, 2014). Two independent bilingual-bicultural research team coders (JIM, AR) coded all qualitative exit interviews in Spanish and came to a consensus on how they relate to Bernal et al.’s (1995) cultural adaptation framework. After independent coding was completed, themes were discussed, refined, and named for final analysis.
Results
Feasibility
Session attendance was high overall. In the individual caregiver version (n = 11), all participants completed 100% of six possible sessions. In the dyadic version (n = 4 dyads), session completion was on average 96% (of six possible sessions) for individual caregiver sessions, 79% (of six possible sessions) for individual adolescent sessions, and 65% (of five possible sessions) for joint family sessions. Participants primarily used phones for sessions (72.7%), followed by tablets (18.2%) and computers (9.1%).
Clinicians were largely successful in completing content for core sessions 1 and 4 and the booster but noted some challenges to completing session activities in sessions 2 and 3. In particular, they noted running out of time; in some cases, this was due to starting sessions late or needing to spend additional time ensuring participants understood key concepts. Given consistent barriers to activity completion, we modified sessions 2 and 3 during the iterative adaptation process to remove activities less central to the hypothesized mechanisms of change. Additionally, certain activities were not possible with caregivers with limited reading proficiency (e.g., video in English with Spanish subtitles, role plays where the participant was to read from a script). During the iterative adaptation process, we revised all videos with Spanish subtitles to be clips originally in Spanish or dubbed to be, to reduce the reading burden on all participants.
Acceptability
Caregivers and adolescents reported high levels of acceptability with sessions and clinicians on session feedback forms (n = 67 caregiver forms; n = 27 adolescent forms). Caregivers indicated they liked the sessions 94.4% of the time, with average ratings of 4.9 (1 = not at all helpful to 5 = very helpful) for both how helpful and how interesting the session was. These ratings are consistent with adolescents’ reports, who indicated they liked the session 100% of the time and rated sessions as very helpful (M = 4.7, SD = 0.6) and interesting (M = 4.6, SD = 0.7). Caregivers (98.5% agreement) and adolescents (100% agreement) reported session topics as important to them and 100% liked their clinician. Caregivers and adolescents both rated clinicians very positively using a scale of 1 = not at all to 5 = very on domains including showing support, listening, answering questions, encouraging discussion, giving information, and keeping session interesting. Caregiver average ratings were 4.9 to 5.0 across domains; adolescent average ratings were 4.6 to 4.9 across domains.
Caregivers and adolescents were very comfortable with video technology (4.8 and 4.9, respectively on scale from 1 = not at all to 5 = very). Caregivers reported problems with the video technology in 9% of sessions, primarily with the internet or phone battery dying. Adolescents reported problems with video technology in 7.4% of sessions (internet/audio cut out).
Session feedback forms are consistent with results from the TSQ, which were completed by nine caregivers and two adolescents; responses for two caregivers were determined to be invalid for this scale because it appeared they misunderstood the instructions for completing the questionnaire (i.e., the ratings they provided with this scale were inconsistent with their overall feedback on other measures and qualitative interviews) and were therefore excluded from analyses. Of note, caregivers responded that they would not change anything from the intervention, and they described liking the ability to schedule their sessions based on their availability. Using a scale from 1 = strongly disagree to 5 = strongly agree for caregivers (M = 4.6, SD = 0.4; range 3.9–5.0) and a scale from 1 = disagree a lot to 5 = agree a lot for adolescents (M = 3.5, SD = 0.7; range = 3.0–4.0) caregivers and adolescents reported high levels of satisfaction with the telehealth services they/their family received.
Quantitative Findings
Given feasibility challenges of engaging adolescents in the intervention and the small sample size of adolescent participants, we present only findings related to caregiver report in this manuscript. A visual review of the individual trajectories of each participant’s self-reported emotion regulation, intergenerational acculturative conflict, and communication with their adolescent provides an overview of the sample’s experience stratified by participants in the caregiver only or dyadic intervention (see Figure 1). Most caregiver-only participants reported slightly more pre- to post-intervention difficulties with emotion regulation, which held relatively stable until the 3-months post-intervention time point; there was no discernible pattern for dyad participants. For caregiver-only participants, three reported decreases in intergenerational acculturation conflict with their adolescent and four reported similar levels of conflict from pre- to post-intervention conflict. There were no discernible patterns for dyad participants. From the end of the intervention to the 3-month follow-up, results were mixed for all participants. For positive communication, three caregiver-only participants reported from pre- to post-intervention increases, with improvements maintained or increasing during the 3-month follow-up. One caregiver-only participant reported a slight improvement from pre- to postintervention and then a sharp decrease in positive communication during the 3-month post-intervention follow-up period. Results on positive communication were mixed for dyad participants. No discernible patterns were identified for negative communication regardless of the intervention type.
Qualitative Findings
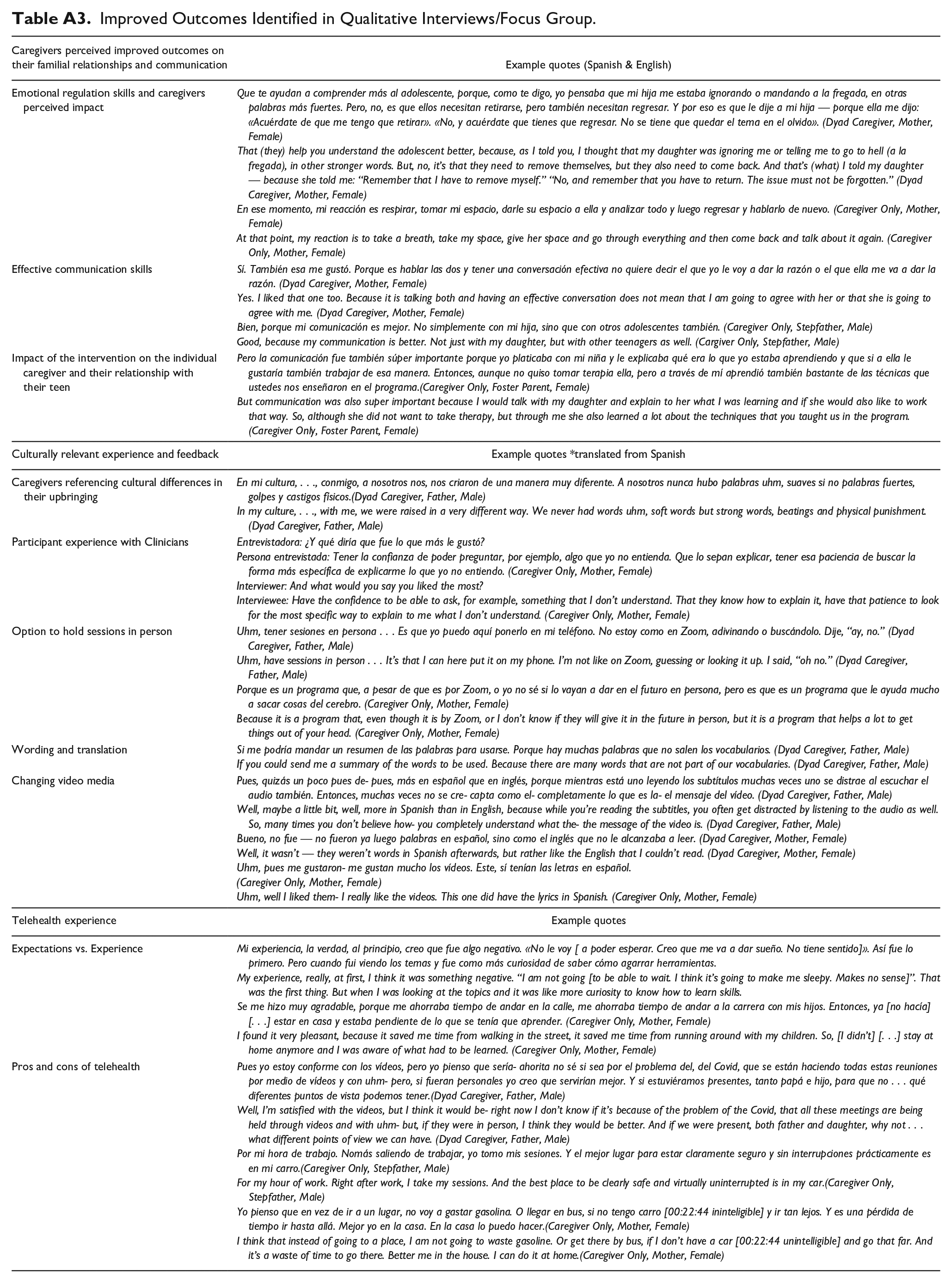
Qualitative analysis supplemented our preliminary outcomes from the pilot and revealed three key themes: (a) caregivers perceived improvement in their familial relationships and communication, (b) culturally relevant feedback, which was used to adapt the intervention, and (c) overall experience with the telehealth modality. See Table A3 for sample quotes reflecting key themes.
Theme 1: Caregivers Perceived Improved Familial Relationships and Communication
Emotion Regulation Skills
Caregivers reported that the emotion regulation skills taught in the intervention helped them communicate with their adolescents by giving them the tools to deescalate a conflict during a conversation and return to it. Caregivers also shared that the topic of effective communication was helpful and that overall, their communication improved for conversations with their adolescent and with other adolescents in their community.
The “3Rs,” one of the core skills, encourages participants to remove themselves from a situation when in an emotionally charged conversation, knowing they can return with a calmer mindset after doing a behavioral activity to release the distress, such as going for a walk. One caregiver shared that before learning these skills they saw their adolescent removing themselves as a sign of “disrespect,” but upon learning these skills and speaking to their adolescent they were able to establish that having a conversation when angry was not effective. One caregiver noted: That (they) help you understand the adolescent better, because, as I told you, I thought that my daughter was ignoring me or telling me to go to hell, in other stronger words. But, no, it’s that they need to remove themselves, but they also need to come back. And that’s (what) I told my daughter — because she told me: “Remember that I have to remove myself.” No, and remember that you have to return. The issue must not be forgotten.
Effective Communication Skills
Caregivers also shared that the intervention helped them learn skills for more effective communication with their adolescents. They noticed more positive communication while simultaneously noting less negative communication. One caregiver recognized that effective communication is not about agreeing with each other but instead understanding where the other person is coming from. This parent noted “Having an effective conversation does not mean that I am going to agree with her or that she is going to agree with me.”
Intervention Impact on Caregiver Relationship With Their Adolescent
While caregivers and adolescents had the opportunity to participate together, most of the caregivers participated in the caregiver-only version of the intervention (n = 7). Despite participating individually, caregivers noticed an improvement in their communication with their adolescents just based on what they learned and experienced in the intervention. One caregiver who participated individually stated: But communication was also super important because I would talk with my daughter and explain to her what I was learning and if she would also like to work that way. So, although she did not want to take therapy, but through me she also learned a lot about the techniques that you taught us in the program.
This vicarious learning helped strengthen their familial relationships and overall communication skills with their adolescents.
Theme 2: Culturally Relevant Experience and Feedback
In the process of culturally adapting this intervention we further asked participants about the content of the intervention’s content to identify possible culturally relevant improvements. Participants were asked to give feedback on media and context they thought was representative of their families and culture (e.g., words, videos, etc.).
Caregivers Referencing Cultural Differences in Their Upbringing
The majority of the participating caregivers immigrated from Latin America and have raised their adolescents in what they perceived to be a very different culture. They mentioned that parenting styles in their upbringing sometimes included corporal punishment and strong language when communicating. Caregivers discussed changing their parenting styles now that they were raising their adolescents in a different culture. Skills in this intervention are more aligned with an authoritative style of parenting in contrast to the more authoritarian styles of parenting the caregivers experienced. One caregiver shared, “In my culture . . ., with me, we were raised in a very different way. We never had words . . . soft words but strong words, beatings, and physical punishment.” Caregivers shared an overall appreciation for learning more authoritative parenting practices that they found were more effective for their adolescents.
Participant Experience With Clinicians
The clinicians facilitating the intervention were fluent Spanish speakers, all but one being bicultural, allowing them to facilitate understanding with the participants and their cultural experience. On their feedback forms, participants reported that they enjoyed working with their clinicians. They also provided positive feedback during the interviews. They felt comfortable asking their clinicians to clarify topics and to further explain. One female caregiver noted: “[I] have the comfort to be able to ask, for example, something that I don’t understand. That they know how to explain it, have that patience to look for the most specific way to explain to me what I don’t understand.”
Wording and Translation
After having the intervention manual and handouts professionally translated, the adaptation team reviewed the scripts, adapted the language so that it was more culturally responsive and accessible, and then delivered the intervention and asked participants for additional feedback on the translations in the exit interviews. Although the adaptation team and clinicians were very careful about using more lay terms to discuss the therapeutic skills, some caregivers still felt like the words used to describe intervention skills were not part of their everyday language. One participant asked clinicians to, “send a summary of the words to be used. Because there are many words that do not appear in [my] vocabulary.” This direct ask informed the investigative team that the terminology should be further simplified to improve understanding and engagement.
Changing Video Media
Prior to applying the feedback to our video media, we had the same content shown in both the Spanish and English versions of the intervention. The English videos included Spanish subtitles, which made it challenging for some participants to read; this was particularly true for caregivers who joined sessions via their phones or with limited reading proficiency. Caregivers shared that the videos were “fine” in relation to what was being discussed in session but provided feedback that they would enjoy the videos more if they were in Spanish and from relevant Latine shows. Some caregivers also relied on their clinicians to further explain or understand the videos since they were not spoken in Spanish. One caregiver noted: Well, maybe a little bit, well, more in Spanish than in English, because while you’re reading the subtitles, you often get distracted by listening to the audio as well. So, many times you don’t believe how- you completely understand what the- the message of the video is.
Based on this feedback, we replaced the videos with examples from popular Latin American shows like “La Rosa de Guadalupe” and “Una Familia con Suerte.”
Theme 3: Telehealth Experience
Participants were also asked about their overall experience with the telehealth modality. It is important to note the project was conducted during the acute phase of the COVID-19 pandemic (2020–2021), when many behavioral health services had pivoted to telehealth (Folk, Schiel, et al., 2022; Oblath et al., 2023). Participants may have come into the program with preconceived ideas around telehealth because of this, which reflects the variation of feedback received on telehealth.
Expectations Versus Actual Experience
In reference to this intervention taking place during the COVID-19 pandemic, participants shared initial uncertainties in participating in this telehealth program. Caregivers also shared how their initial concerns changed over time as a result of participating in the intervention. In particular, one parent noted: My experience, really, at first, I think it was something negative. “I am not going [to be able to wait. I think it’s going to make me sleepy. Has no sense”. That was the first thing. But when I was looking at the topics and it was like more curiosity to know how to learn the tools.
Overall, participants reported some initial mistrust with the technology, but their comfort increased as they gained more experience.
Pros and Cons of Telehealth
Despite some initial hesitation, participants also shared some of their perceived advantages of telehealth, which included the ability to join sessions from wherever they were, without the burden of transportation costs. One participant stated, “Right after work, I take my sessions. And the best place to be clearly safe and virtually uninterrupted is in my car.” Some mentioned that it saved them time and resources since they did not need to travel across the city to participate in sessions. Still, some participants shared that they would like some sessions in person. For example, one said Well, I’m satisfied with the video [sessions], but I think it would be- right now I don’t know if it’s because of the problem with COVID, that all these meetings are being held through videos and with uhm- but, if they were in person, I think they would help more. And if we were present, both father and daughter.
Although some participants acknowledged the advantage of virtual therapy, some still preferred the interpersonal aspects of going to therapy in person.
Discussion
This present pilot study responds to the unmet behavioral health needs of diverse Latine families by culturally adapting an intervention with previous empirical support for improving mental health outcomes among systems-impacted adolescents and evaluating its feasibility and acceptability for delivery via telehealth. This work is novel in several ways: (a) it incorporated both a culturally and linguistically adapted intervention, using empirically based and successful cultural adaptation frameworks, and was delivered by predominantly Latine and all bilingual clinicians, (b) it used telehealth delivery to increase access and address common barriers to treatment receipt, and (c) it integrated key systems partners serving child welfare involved families into the development and design of the study (see Folk et al., 2024 and Leo et al., 2023 for description of community partners’ involvement).
Adolescents of different ethnic and cultural backgrounds vary in their risk factors and prevalence rates for behavioral health problems, yet most evidence-based treatments for behavioral health have been primarily designed and tested with predominantly non-Hispanic white U.S. adolescents (Arora et al., 2021; Hodge et al., 2012). This is an important gap given high rates of unmet behavioral health need among Latine systems-impacted adolescents and preliminary meta-analytic evidence showing culturally sensitive treatments; that is, interventions that incorporate “ethnic/cultural characteristics, experiences, norms, values, behavioral patterns, and beliefs of a target population” into the design and delivery of the treatment program (Resnicow et al., 2000) being associated with greater improvements in adolescents’ behavioral health (Hernandez Robles et al., 2018). It should be noted that the conclusions from the Hernandez Robles et al. meta-analysis were hindered by the small number of studies available (k = 7) for synthesis as only four specifically targeted Latine adolescents, none of the interventions were delivered in Spanish (Burrow-Sanchez & Wrona, 2012; Santisteban et al., 2011; Szapocznik et al., 1983; Wrona, 2013), and only two interventions targeting Latine adolescents included a family component (Santisteban et al., 2011; Szapocznik et al., 1983). Previous cultural adaptations for other ethnoracial minoritized adolescents have been successful (Robinson et al., 2024) because they incorporated a combination of both surface (i.e., adapting the language of the intervention) and deep (i.e., incorporating cultural forces, like racial discrimination, related to health and wellness in that population) level adaptations. Our project addressed these current gaps in the literature in several ways.
First, we examined an understudied topic—how to provide effective and culturally responsive family-based telehealth treatment for systems-impacted adolescents. Accounting for specific responsivity factors such as cultural background and ethnic identity is a best practice in treatment planning for systems-impacted adolescents (Hoge, 2016) and may result in better adolescent behavioral health outcomes (i.e., substance use, mental health). To our knowledge, most family-based intervention research with this population examines an in-person modality. Very little research has focused on culturally-adapted treatment for systems-impacted adolescents, however a meta-analysis of substance use treatment for racial/ethnic minority non-system impacted adolescents (k = 7; Steinka-Fry et al., 2017) and a randomized controlled trial with non-systems impacted Latine adolescents diagnosed with a behavioral health disorder (Burrow-Sánchez & Hops, 2019) provide evidence that culturally-responsive treatment is more effective in improving behavioral health outcomes than non-culturally-informed treatment. Similarly, a meta-analysis with justice-involved Indigenous adults (k = 7; Gutierrez et al., 2018), found those who participated in culturally relevant programs had significantly lower odds of recidivism than those who participated in non-culturally-informed programs.
Second, we specifically focused on an underserved population—Spanish-speaking families of systems-impacted adolescents. Systems involvement can further perpetuate inequities in treatment access for Latine adolescents and make it logistically and practically infeasible for families to participate in interventions to promote healthy and successful reunification. Latine systems-impacted adolescents enrolled in behavioral health treatments and their caregivers have identified a lack of Spanish-speaking clinicians, transportation, and scheduling as significant barriers to treatment (Burrow-Sanchez et al., 2011). Our findings from this pilot feasibility and acceptability trial of FTP-S, a culturally-adapted telehealth intervention, indicated high levels of satisfaction, acceptability and feasibility, which mirror findings from the FTP intervention in English (Folk et al., 2024).
Third, the study used novel (e.g., telehealth technology), interdisciplinary (e.g., behavioral health providers, juvenile legal system partners), and community-engaged (e.g., iterative feedback from adolescents, caregivers, and clinicians) methodological approaches, which have the potential to transform the field. Findings indicate our culturally-adapted telehealth intervention has the potential to improve family-based interventions and mental health outcomes for an underserved population (i.e., systems-impacted Latine adolescents with Spanish-speaking caregivers) given the accessible intervention modality (e.g., telehealth) and the high satisfaction ratings from participants.
Limitations and Future Directions
Despite the aforementioned innovation and strengths from our culturally-adapted telehealth intervention, a few limitations should be noted. First, our small sample did not include sufficient caregiver-adolescent dyads to quantitatively examine adolescent behavioral health outcomes. While the small sample size limits the generalizability of our findings, this pilot study offers valuable preliminary insights into the feasibility and acceptability of a telehealth-delivered, culturally adapted intervention for Spanish-speaking Latine families. These insights lay critical groundwork for future, larger-scale studies designed to evaluate clinical effectiveness and implementation outcomes. Second, we only recruited one male caregiver and most families were from Mexico, El Salvador, and Honduras, which limits the generalizability of our findings. Third, some of the direct translations on our recruitment materials (i.e., the term child protective services) may have caused some worry and distrust among Latine families, which could have impacted our ability to recruit them. Fourth, the cultural adaptation process in this pilot study was informed primarily by enrolled participants and study clinicians, which, while appropriate for early-stage adaptation work, may limit the diversity of perspectives captured. Future iterations will benefit from engaging a broader set of key community partners, including non-participant families and community providers, to further refine the intervention. Fifth, satisfaction ratings were collected immediately after sessions, which may limit participants’ ability to reflect over time. Although surveys were completed anonymously and separately from clinicians in the study, social desirability or response bias may have impacted our participant responses. Additionally, while modest compensation was provided to reduce participation barriers, it may have influenced participant engagement or feedback and should be considered in interpreting acceptability data. Similarly, some caregiver data on the TSQ was deemed invalid because several caregivers appeared to have misunderstood the instructions to complete the assessment form. Careful attention should be given when working with Spanish speaking families who are not familiar with the research process, including more support to ensure all instructions and assessment questions are well understood. Lastly, although caregivers described improvements in their emotion regulation and effective communication skills with their teens during qualitative interviews, these findings were not consistently replicated across quantitative measures. One possibility is qualitative interviews included clarifying prompts and interpersonal connection that allowed caregivers to build more insight into their own improvements across emotion regulation and communication skills.
Conclusion
Using telehealth technology to deliver family interventions not only reduces barriers to accessing family-based treatment for Spanish-speaking families of system-impacted adolescents, but also poses the possibility of subsequently bringing interventions to scale to reach a wide range of families throughout the U.S.; this approach would allow for a large-scale impact on service availability for this underserved population. Our culturally-adapted telehealth intervention also has the potential to enhance collaboration with service delivery systems, health disparities researchers, among others. Further, results of the present study contribute to the limited existing evidence based on specific responsivity factors when developing interventions for systems-impacted adolescents. Despite calls over the last three decades to consider cultural and linguistic specific responsivity factors for justice-impacted adolescents (Hovey et al., 2017), this remains an understudied topic.
Footnotes
Appendix
Improved Outcomes Identified in Qualitative Interviews/Focus Group.
| Caregivers perceived improved outcomes on their familial relationships and communication | Example quotes (Spanish & English) |
| Emotional regulation skills and caregivers perceived impact |
Que te ayudan a comprender más al adolescente, porque, como te digo, yo pensaba que mi hija me estaba ignorando o mandando a la fregada, en otras palabras más fuertes. Pero, no, es que ellos necesitan retirarse, pero también necesitan regresar. Y por eso es que le dije a mi hija — porque ella me dijo: «Acuérdate de que me tengo que retirar». «No, y acuérdate que tienes que regresar. No se tiene que quedar el tema en el olvido». (Dyad Caregiver, Mother, Female)
That (they) help you understand the adolescent better, because, as I told you, I thought that my daughter was ignoring me or telling me to go to hell (a la fregada), in other stronger words. But, no, it’s that they need to remove themselves, but they also need to come back. And that’s (what) I told my daughter — because she told me: “Remember that I have to remove myself.” “No, and remember that you have to return. The issue must not be forgotten.” (Dyad Caregiver, Mother, Female) En ese momento, mi reacción es respirar, tomar mi espacio, darle su espacio a ella y analizar todo y luego regresar y hablarlo de nuevo. (Caregiver Only, Mother, Female) At that point, my reaction is to take a breath, take my space, give her space and go through everything and then come back and talk about it again. (Caregiver Only, Mother, Female) |
| Effective communication skills |
Sí. También esa me gustó. Porque es hablar las dos y tener una conversación efectiva no quiere decir el que yo le voy a dar la razón o el que ella me va a dar la razón. (Dyad Caregiver, Mother, Female)
Yes. I liked that one too. Because it is talking both and having an effective conversation does not mean that I am going to agree with her or that she is going to agree with me. (Dyad Caregiver, Mother, Female) Bien, porque mi comunicación es mejor. No simplemente con mi hija, sino que con otros adolescentes también. (Caregiver Only, Stepfather, Male) Good, because my communication is better. Not just with my daughter, but with other teenagers as well. (Cargiver Only, Stepfather, Male) |
| Impact of the intervention on the individual caregiver and their relationship with their teen |
Pero la comunicación fue también súper importante porque yo platicaba con mi niña y le explicaba qué era lo que yo estaba aprendiendo y que si a ella le gustaría también trabajar de esa manera. Entonces, aunque no quiso tomar terapia ella, pero a través de mí aprendió también bastante de las técnicas que ustedes nos enseñaron en el programa.(Caregiver Only, Foster Parent, Female)
But communication was also super important because I would talk with my daughter and explain to her what I was learning and if she would also like to work that way. So, although she did not want to take therapy, but through me she also learned a lot about the techniques that you taught us in the program. (Caregiver Only, Foster Parent, Female) |
| Culturally relevant experience and feedback | Example quotes *translated from Spanish |
| Caregivers referencing cultural differences in their upbringing |
En mi cultura, . . ., conmigo, a nosotros nos, nos criaron de una manera muy diferente. A nosotros nunca hubo palabras uhm, suaves si no palabras fuertes, golpes y castigos físicos.(Dyad Caregiver, Father, Male)
In my culture, . . ., with me, we were raised in a very different way. We never had words uhm, soft words but strong words, beatings and physical punishment. (Dyad Caregiver, Father, Male) |
| Participant experience with Clinicians |
Entrevistadora: ¿Y qué diría que fue lo que más le gustó?
Persona entrevistada: Tener la confianza de poder preguntar, por ejemplo, algo que yo no entienda. Que lo sepan explicar, tener esa paciencia de buscar la forma más específica de explicarme lo que yo no entiendo. (Caregiver Only, Mother, Female) Interviewer: And what would you say you liked the most? Interviewee: Have the confidence to be able to ask, for example, something that I don’t understand. That they know how to explain it, have that patience to look for the most specific way to explain to me what I don’t understand. (Caregiver Only, Mother, Female) |
| Option to hold sessions in person |
Uhm, tener sesiones en persona . . . Es que yo puedo aquí ponerlo en mi teléfono. No estoy como en Zoom, adivinando o buscándolo. Dije, “ay, no.” (Dyad Caregiver, Father, Male)
Uhm, have sessions in person . . . It’s that I can here put it on my phone. I’m not like on Zoom, guessing or looking it up. I said, “oh no.” (Dyad Caregiver, Father, Male) Porque es un programa que, a pesar de que es por Zoom, o yo no sé si lo vayan a dar en el futuro en persona, pero es que es un programa que le ayuda mucho a sacar cosas del cerebro. (Caregiver Only, Mother, Female) Because it is a program that, even though it is by Zoom, or I don’t know if they will give it in the future in person, but it is a program that helps a lot to get things out of your head. (Caregiver Only, Mother, Female) |
| Wording and translation | Si me podría mandar un resumen de las palabras para usarse. Porque hay muchas palabras que no salen los vocabularios. (Dyad Caregiver, Father, Male) If you could send me a summary of the words to be used. Because there are many words that are not part of our vocabularies. (Dyad Caregiver, Father, Male) |
| Changing video media | Pues, quizás un poco pues de- pues, más en español que en inglés, porque mientras está uno leyendo los subtítulos muchas veces uno se distrae al escuchar el audio también. Entonces, muchas veces no se cre- capta como el- completamente lo que es la- el mensaje del vídeo. (Dyad Caregiver, Father, Male) Well, maybe a little bit, well, more in Spanish than in English, because while you’re reading the subtitles, you often get distracted by listening to the audio as well. So, many times you don’t believe how- you completely understand what the- the message of the video is. (Dyad Caregiver, Father, Male) Bueno, no fue — no fueron ya luego palabras en español, sino como el inglés que no le alcanzaba a leer. (Dyad Caregiver, Mother, Female) Well, it wasn’t — they weren’t words in Spanish afterwards, but rather like the English that I couldn’t read. (Dyad Caregiver, Mother, Female) Uhm, pues me gustaron- me gustan mucho los vídeos. Este, sí tenían las letras en español. (Caregiver Only, Mother, Female) Uhm, well I liked them- I really like the videos. This one did have the lyrics in Spanish. (Caregiver Only, Mother, Female) |
| Telehealth experience | Example quotes |
| Expectations vs. Experience |
Mi experiencia, la verdad, al principio, creo que fue algo negativo. «No le voy [ a poder esperar. Creo que me va a dar sueño. No tiene sentido]». Así fue lo primero. Pero cuando fui viendo los temas y fue como más curiosidad de saber cómo agarrar herramientas.
My experience, really, at first, I think it was something negative. “I am not going [to be able to wait. I think it’s going to make me sleepy. Makes no sense]”. That was the first thing. But when I was looking at the topics and it was like more curiosity to know how to learn skills. Se me hizo muy agradable, porque me ahorraba tiempo de andar en la calle, me ahorraba tiempo de andar a la carrera con mis hijos. Entonces, ya [no hacía] [. . .] estar en casa y estaba pendiente de lo que se tenía que aprender. (Caregiver Only, Mother, Female) I found it very pleasant, because it saved me time from walking in the street, it saved me time from running around with my children. So, [I didn’t] [. . .] stay at home anymore and I was aware of what had to be learned. (Caregiver Only, Mother, Female) |
| Pros and cons of telehealth |
Pues yo estoy conforme con los vídeos, pero yo pienso que sería- ahorita no sé si sea por el problema del, del Covid, que se están haciendo todas estas reuniones por medio de vídeos y con uhm- pero, si fueran personales yo creo que servirían mejor. Y si estuviéramos presentes, tanto papá e hijo, para que no . . . qué diferentes puntos de vista podemos tener.(Dyad Caregiver, Father, Male)
Well, I’m satisfied with the videos, but I think it would be- right now I don’t know if it’s because of the problem of the Covid, that all these meetings are being held through videos and with uhm- but, if they were in person, I think they would be better. And if we were present, both father and daughter, why not . . . what different points of view we can have. (Dyad Caregiver, Father, Male) Por mi hora de trabajo. Nomás saliendo de trabajar, yo tomo mis sesiones. Y el mejor lugar para estar claramente seguro y sin interrupciones prácticamente es en mi carro.(Caregiver Only, Stepfather, Male) For my hour of work. Right after work, I take my sessions. And the best place to be clearly safe and virtually uninterrupted is in my car.(Caregiver Only, Stepfather, Male) Yo pienso que en vez de ir a un lugar, no voy a gastar gasolina. O llegar en bus, si no tengo carro [00:22:44 ininteligible] y ir tan lejos. Y es una pérdida de tiempo ir hasta allá. Mejor yo en la casa. En la casa lo puedo hacer.(Caregiver Only, Mother, Female) I think that instead of going to a place, I am not going to waste gasoline. Or get there by bus, if I don’t have a car [00:22:44 unintelligible] and go that far. And it’s a waste of time to go there. Better me in the house. I can do it at home.(Caregiver Only, Mother, Female) |
Acknowledgements
We would also like to acknowledge the support and work of Dr. Margareth V. Del Cid for providing bilingual and culturally responsive care to the families participating in this trial.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was from the Visa Foundation and the American Psychology–Law Society. Drs. Folk, Holloway, and Tolou-Shams received salary support from the National Institute on Drug Abuse (K23DA050798; T32DA007250; K24DA046569).
Ethical Approval
This study was reviewed and approved by the Institutional Review Board (IRB#15-17258).