
Abstract
In a sample of youth aged 10–16 years with chronic physical illness, this study examined psychometric properties of a modified Psychological Sense of School Membership (m-PSSM) scale; described longitudinal trends in perceptions over 24 months; and, identified factors associated with school belonging. Youth were recruited from a pediatric hospital in Canada. A total of 105 youth attended school in the past year and provided self-reports. The four-item m-PSSM had a unidimensional structure which was measurement invariant between youth in elementary (10–13 years) versus secondary school (14–16 years). Internal consistency was (ω > .80). There was no evidence that m-PSSM scores changed significantly over time (η2 = 0.05). Predictors of lower perceived school belonging were being in secondary school, having psychopathology, reporting lower quality of life in the domains of social support and school environment, experiencing peer victimization, and living in a community with higher residential instability and lower material deprivation.
Background
The need to belong motivates the formation of social bonds, the absence of which has negative consequences to individual physical, mental, and social health outcomes (Baumeister & Leary, 1995). Perceptions of belonging can be context specific. For youth, their sense of belonging at school is of paramount importance (OECD, 2015), as it often conditions self-reported mental and psychosocial health, as well as academic achievement. Goodenow (1993) defined school belonging as the extent to which students perceive they are accepted, respected, included, and supported by others in the school environment and applied this definition in the development of the Psychological Sense of School Membership (PSSM) scale.
Predictors and Trajectories of School Belonging
Research shows robust associations between perceived school belonging and emotional, social, and academic outcomes (Allen et al., 2018). There is also ample evidence showing that factors associated with positive perceptions of school belonging are multilevel and align with the socioecological model of human development (Allen et al., 2016, 2023; Bronfenbrenner, 1979)—including individual: younger age, non-marginalized race/ethnicity, mental health; microsystem: higher levels of peer/teacher/parent support; mesosystem: school type (elementary vs. secondary), participation in extracurricular activities; and, exosystem: safer schools and communities (Slaten et al., 2016). Evidence regarding trajectories of perceived school belonging over time are mixed—some suggest perceptions are stable (Vaz et al., 2015), while others show declines (Anderman, 2003; Gillen-O’Neel & Fuligni, 2013; Witherspoon & Ennett, 2011). Despite a call for work aimed at understanding school belonging among marginalized youth, including those with chronic physical illness or disability (Stiefel et al., 2018), research in this population remains limited.
School Belonging Among Youth with Physical Illness
One study showed that youth with physical illness reported lower perceptions of school belonging compared to their healthy counterparts (d = 0.23), and that the association between belonging and on-time graduation was stronger for youth with physical illness (OR = 1.63 for diagnosis-belonging interaction term) (Kirkpatrick, 2020). This latter finding was consistent with previous reports (Lum et al., 2017). There are no studies of the predictors of perceived school belonging (cross-sectionally or longitudinally) among youth with physical illness. Importantly, Kirkpatrick (2020) examined the properties of their school belonging scale and found it to have acceptable internal consistency reliability (α = .76) and to be measurement invariant between youth with versus without physical illness—that is, both groups interpreted scale items and the school belonging construct similarly.
Knowledge Gaps and Present Study
While studies examining perceptions of school belonging among youth with physical illness have laid important groundwork in the field, knowledge gaps remain. First, longitudinal studies that have modeled trajectories of perceived school belonging did not stratify by health status (i.e., presence/absence of physical illness) (Jose et al., 2012; Vaz et al., 2015) and thus may not generalize to youth with physical illness. Such findings are needed to inform opportunities for intervention to promote school belonging that may be universal for all youth or targeted to those with physical illness. Second, there have been no studies modeling predictors of school belonging over time in youth with physical illness—knowledge needed to inform policy that would aim to promote school belonging within the socioecological model of human development (Bronfenbrenner, 1979). Third, study samples typically had narrow age ranges, which limits the inferences that can be made to the broader population of youth with physical illness.
Individuals with chronic physical illness often experience stigmatization on account of their condition or its sequelae; thus, understanding their perceptions of connectedness is a cornerstone to promoting quality of life and psychosocial functioning (Berkelbach van der Sprenkel et al., 2022; O’Donnell & Habenicht, 2022). Because youth spend a substantial proportion of their waking hours at school, school belonging is an important aspect of their overall sense of connectedness (Baumeister & Leary, 1995; Goodenow, 1993). For youth with physical illness who may be less likely to participate in extracurricular activities (State of Play 2020 | Pre-Pandemic Trends, Ages 13–17—The Aspen Institute Project Play, 2020), schools are a primary setting for academic and social development—key outcomes conditioned on perceived school belonging (Allen et al., 2018). Thus, the aim of this study was to describe longitudinal perceptions of school belonging over a 24-month period in youth aged 10–16 years with chronic physical illness and identify factors associated with school belonging over time. The selection of predictors was informed by Allen et al. (2023, 2016) who, guided by the socioecological model of human development (Bronfenbrenner, 1979), provided robust evidence that factors associated with school belonging are multilevel. It was important to ensure that the scale measuring perceived school belonging was psychometrically robust, because of the relatively wide age range in the sample. This study used a modified brief version of the Psychological Sense of School Membership (m-PSSM) scale. While there is evidence supporting the psychometric properties of the full PSSM (Goodenow, 1993; You et al., 2011), and Kirkpatrick (2020) showed that an m-PSSM was invariant between youth with versus without a physical illness, there remains a paucity of research. Thus, prior to addressing the main objectives of this study, psychometric analyses were first conducted on the m-PSSM with particular focus on estimating its factor structure (i.e., factorial validity) and testing measurement invariance across age in youth with chronic physical illness (i.e., comparing youth in elementary school [10–13 years] vs. those in secondary school [14–16 years]).
Methods
Participants and Recruitment
Data come from Multimorbidity in Youth across the Life-course (MY LIFE), an on-going study of children with physical illnesses (Ferro et al., 2019; Ferro, Lipman, et al., 2021). Recruited from outpatient clinics at a pediatric hospital in Canada, participants are being followed over 48 months (data from recruitment, 6, 12, and 24 months were used in these analyses). To be included, children must have been aged 2–16 years at recruitment, had parents with (and for youth aged ≥10 years) sufficient command of the English language to complete study measures, and been diagnosed by a physician with a chronic physical illness. Within clinics, research staff verified eligibility and obtained written permission from families who wished to be contacted further about participation. Research staff then contacted parents to schedule a time for data collection. Data were collected using structured interviews and self-reported questionnaires on laptops or paper for mail packages. Parent reports were collected for all children, and youth ≥10 years provided self-reports. Informed consent and assent were obtained from participants. Ethical approval for this study was obtained from the Waterloo Human Research Ethics Board (#31010) and Hamilton Integrated Research Ethics Board (#2797).
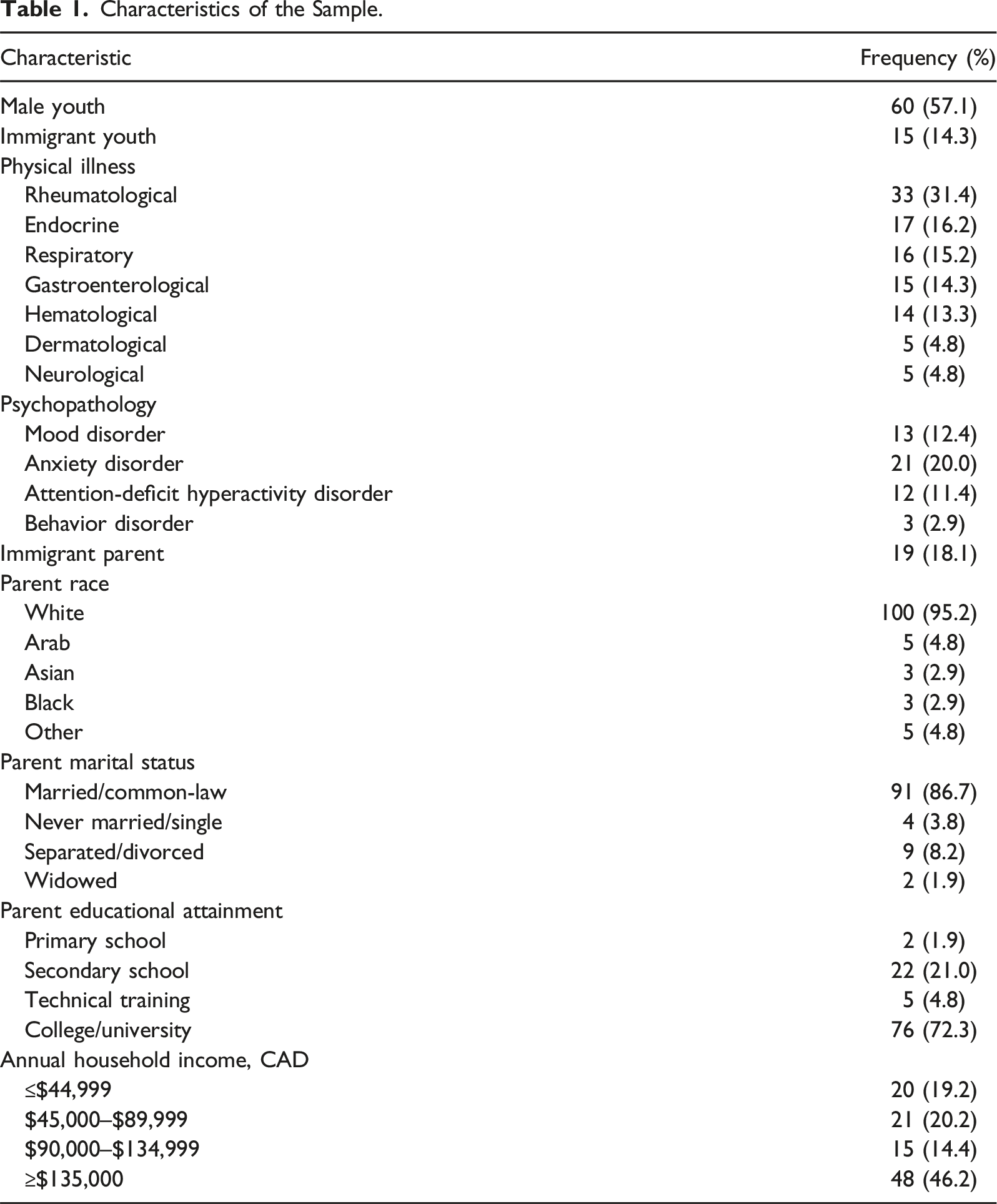
Sample Characteristics
Characteristics of the Sample.
Measures
Perceived School Belonging
The m-PSSM used in this study was adopted from the version used in the Ontario Child Health Study (Boyle et al., 2019; Goodenow, 1993) and included four items: “I feel close to people at my school,” “I feel like I belong at my school,” “I am happy to be at my school,” and “I feel safe at my school.” A five-point Likert scale was used (1 = “strongly agree” to 5 = “strongly disagree”) and the response options of “disagree” and “strongly disagree” were collapsed due to sparse data in the latter category. Lower scores on the m-PSSM indicated a greater perception of school belonging.
There was one missing item score for item 4, wave 4 (“feel safe in my school”). For this youth, their mean score from items 1–3 were used to impute their score for item 4. There were no other missing item-level data and there were no wave-level missing data in the study (n = 105 at each assessment). During the 24-month follow-up, 55 youth aged into the study (i.e., turned 10 years of age and were age-eligible for self-reports). These youth were not included in the study because they did not complete baseline data collection and thus could not be included in tests of measurement invariance.
Measurement Invariance Testing of the m-PSSM
Confirmatory factor analysis was used to model the factor structure of the m-PSSM using baseline data and a robust weighted least squares estimator with a diagonal weight matrix. To test whether the m-PSSM was invariant by age, a multiple-group confirmatory factor analysis with baseline data was performed whereby youth were stratified into primary school (10–13 years, n = 59) and secondary school (14–16 years, n = 46) groups. Simulation evidence suggests that a group size of n = 40 is sufficiently powered (1–β > 0.95) to estimate a four-item, one-factor model with factor loadings ≥.65 (Wolf et al., 2013). Established guidelines for invariance testing whereby increasingly stringent equality constraints were specified for model parameters between groups were followed using several model fit indices: χ2 goodness-of-fit p > .05, comparative fit index (CFI) ≥ 0.950, and standardized root mean residual (SRMR) < 0.08 (Chen, 2007; van de Schoot et al., 2012). Adequate model fit was achieved if ≥ 2 indices met these thresholds. The root mean square error of approximation (RMSEA) was included for completeness, but not used in decisions surrounding fit or invariance due to arguments against its use in small samples and factor models with few degrees of freedom (Kenny et al., 2015). The systematic approach to adding model constraints allow the identification of aspects of the factor structure that contribute to model misfit and ultimately, differences in the interpretation of the latent construct between groups, in this case, perceived school belonging (van de Schoot et al., 2012). Configural invariance suggests that the construct has the same factor structure in both groups; equal factor loadings (i.e., metric invariance) suggest that groups attribute the same meaning to the construct; equal factor loadings and item thresholds (i.e., scalar invariance) suggest that meaning of the items that comprise the construct is the same between groups; and, equal factor loadings, item thresholds, and residual errors (i.e., strict invariance) suggest that the explained variance is the same and the construct is measured identically between groups. To determine the presence of measurement invariance, changes in model fit indices were examined in relation to the following thresholds indicating a non-substantial worsening of fit: ΔCFI ≥–.010, and ΔSRMR ≤.030 (Chen, 2007). Measurement invariance was present if ≥ 2 change scores met these thresholds.
Measurement Invariance of the m-PSSM by Age.
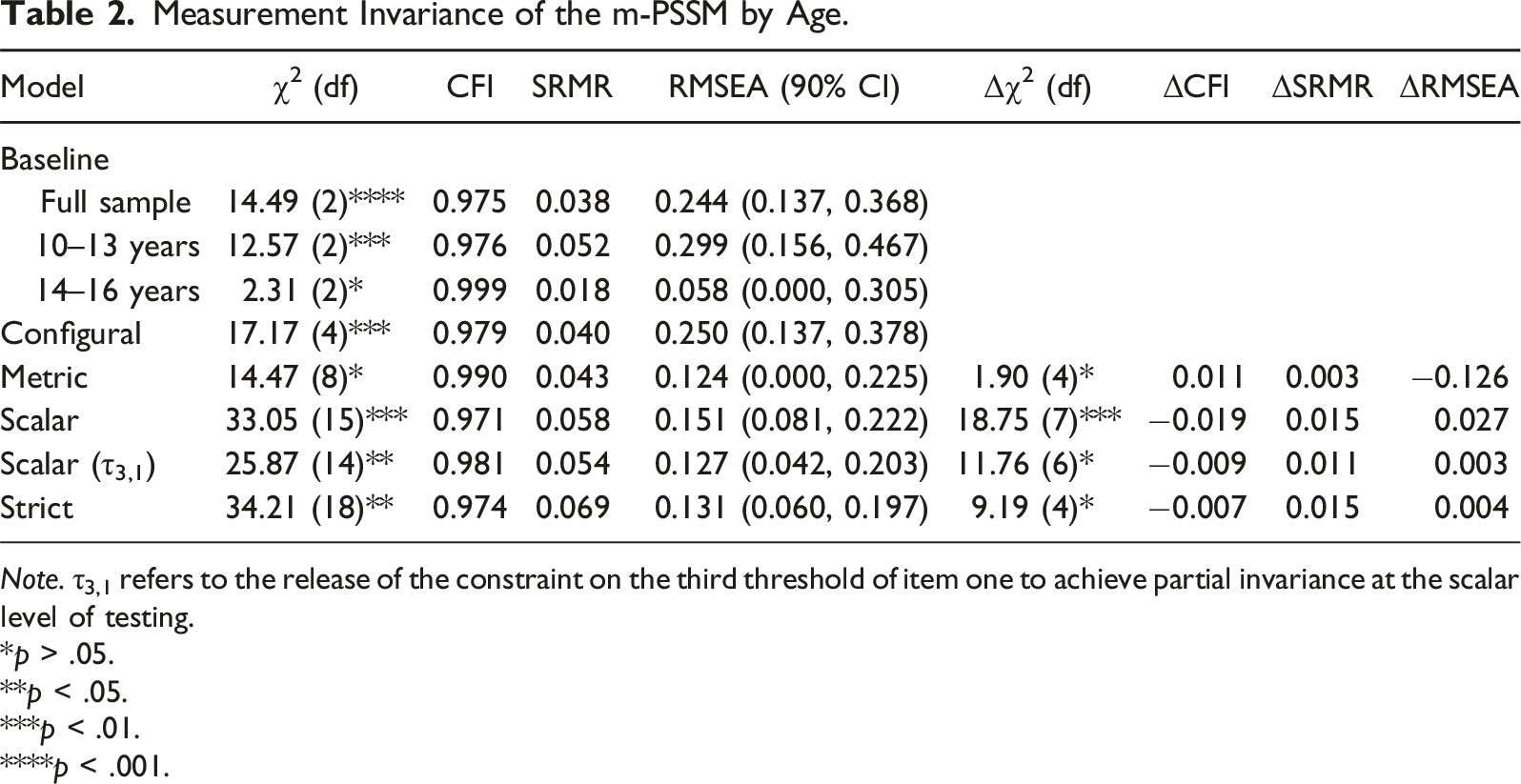
Note. τ3,1 refers to the release of the constraint on the third threshold of item one to achieve partial invariance at the scalar level of testing.
*p > .05.
**p < .05.
***p < .01.
****p < .001.
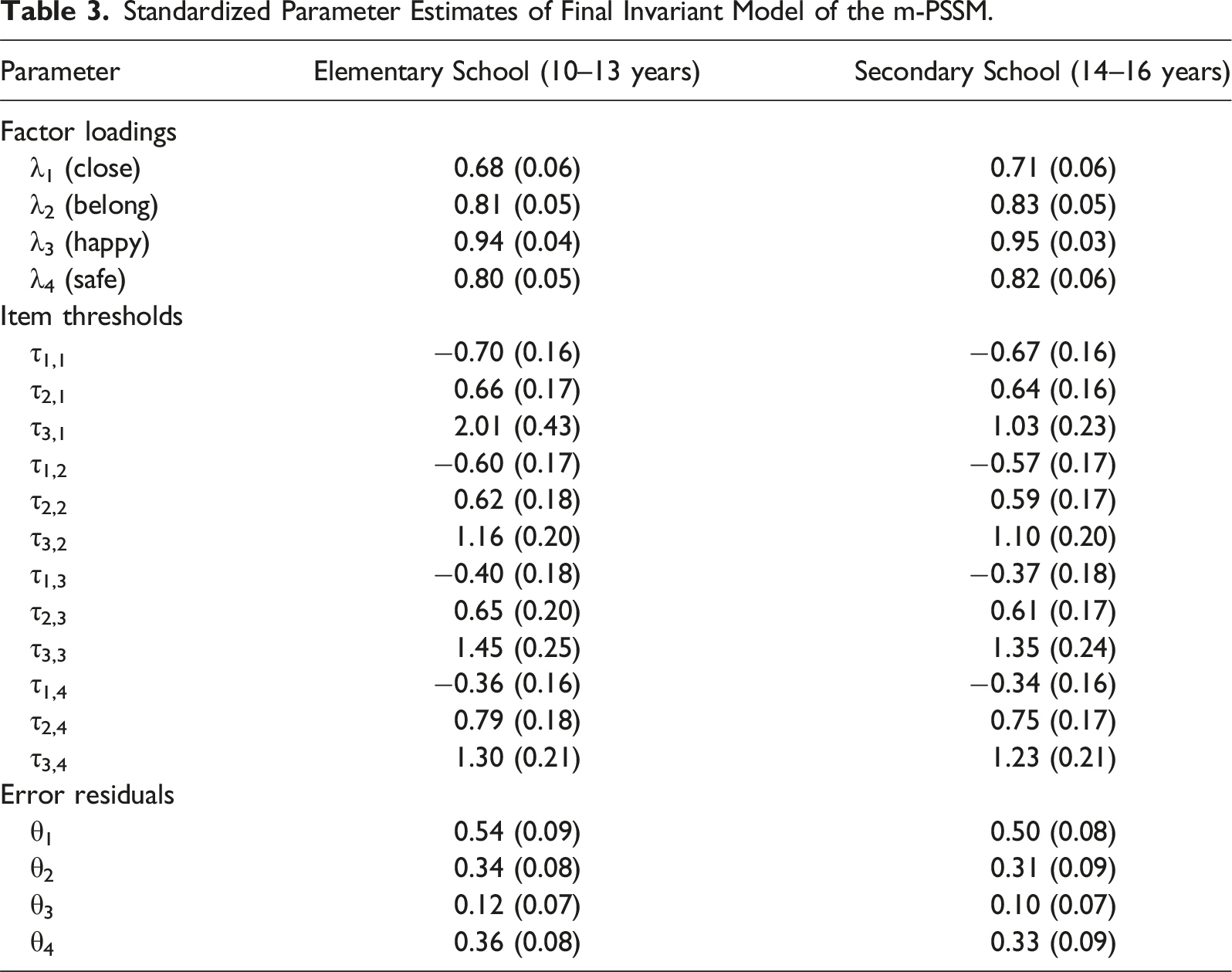
Standardized Parameter Estimates of Final Invariant Model of the m-PSSM.
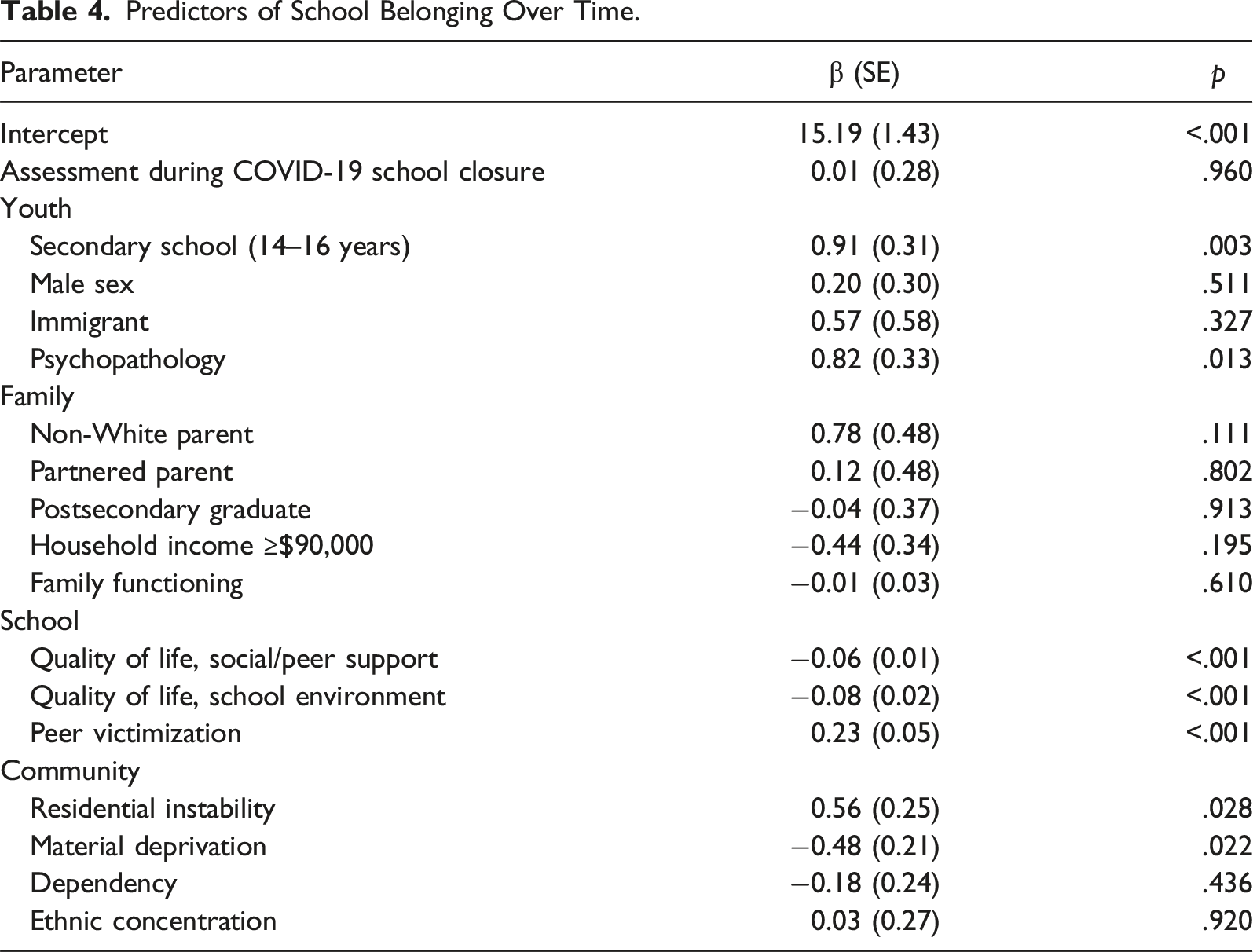
Predictors of School Belonging Over Time.
Peer Victimization
Peer victimization was measured using items from the 2009 School Crime Supplement to the National Crime Victimization Survey (National Center for Education Statistics, 2009). Youth were asked, “During this school year, how many times has any other student done any of the following:” The experiences were, “Made fun of you, called you names, or insulted you either in person or online?”, “Spread rumors about you?”, “Threatened you with harm?”, “Pushed you, shoved you, tripped you, or spit on you?”, and “Excluded you from activities on purpose?”. Responses were: 1 = “never,” 2 = “once or twice this school year,” 3 = “once or twice this month,” 4 = “once or twice a week,” and 5 = “almost every day.” A sum score was computed whereby lower scores indicated fewer experiences of peer victimization. The mean score was 7.2 (SD = 2.8). Internal consistency was ω = .81.
Quality of Life
The youth-reported KIDSCREEN-27 was used to measure quality of life during the past month (Ravens-Sieberer et al., 2014). For these analyses, the social/peer support and school environment domains were used, each containing four items. Domain scores were converted to T scores [51.5 (SD = 10.5) and 50.9 (SD = 9.6), respectively], whereby lower scores indicated worse quality of life. Internal consistencies were ω = .82 and ω = .75, respectively. The KIDSCREEN-27 has been validated in youth with chronic illnesses (Ferro, Otto, et al., 2022).
Psychopathology
Youth psychopathology was measured using the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID) (Duncan et al., 2018; Sheehan et al., 2010). The MINI-KID is a structured interview which was administered by trained research staff to youth. Those who screened positive for ≥1 mental illness were classified as having psychopathology (n = 30, 29%). The MINI-KID has been used successfully in children with chronic illness (Ferro et al., 2024; Ferro, Qureshi, et al., 2022).
Family Functioning
Family functioning was measured using the general functioning subscale of the McMaster Family Assessment Device (Byles et al., 1988). It assesses parent-reported overall health/psychology of a family using 12 items which reflect problem solving, communication, roles, affective responsiveness, affective involvement, and behavior control. Items are rated using a four-point scale whereby lower scores indicate better functioning. The mean score was 27.8 (SD = 5.1). It has been validated in families of children with chronic illness (Oltean et al., 2020). Internal consistency was ω = .80.
Community Marginalization
The Ontario Marginalization Index (ON-MARG) was used to measure community-level marginalization (Matheson et al., 2021). The index consists of four factors: residential instability (area-level concentration of individuals facing housing instability), material deprivation (lack of access and attainment of basic material needs), dependency (area-level concentration of those without income from employment), and ethnic concentration (individuals identifying as a visible minority or recent immigrant). Each factor is reported as a z-score, obtained using participant postal codes linked to dissemination areas according to the 2017 Statistics Canada’s Postal CodeOM Conversion File Plus (Statistics Canada, 2017). Higher ON-MARG scores indicated greater marginalization. Mean z-scores for residential instability, material deprivation, dependency, and ethnic concentration were −0.38 (SD = 0.78), −0.34 (SD = 0.90), −0.22 (SD = 0.95), and −0.20 (SD = 0.68), respectively.
Sociodemographics
Sociodemographics were included in statistical analyses using items and response options developed by Statistics Canada. Youth reported on their age, sex, and whether they were born in Canada. Parents reported on their marital status, educational attainment, household income, race, and whether they were born in Canada. In the multivariable model, sociodemographic variables were dichotomized as race (White or non-White), marital status (partnered or not), educational attainment (postsecondary graduate or not), and income (≥$90,000 or <$90,000). These binary coding were used to avoid small cell counts for some response options (and subsequently inflated standard errors) and increase interpretability of results. In the case of income, $90,000 represents the gross median income of households with >1 persons (Statistics Canada, 2016).
Data Analyses
Mean scores on the modified PSSM were compared over time using repeated measures ANOVA, such that effect sizes of η2 = .01, .06. and .14 are, respectively, considered small, medium, and large (Cohen, 1988). Linear mixed modeling with an unstructured covariance matrix was used to investigate youth, family, school, and community-related factors associated with school belonging over 24 months. Estimates of association from the model are expressed as standardized coefficients, whereby β = 0.10–0.29 are small, β = 0.30–0.49 are medium, and β ≥ 0.50 are large (Cohen, 1988). Because youth enrolled in MY LIFE were in active follow-up during lockdown ordinances in response to the COVID-19 pandemic, we included a time-varying predictor in our model which reflected whether data were collected during school closures (Patte et al., 2023). Mplus 8.8 was used to conduct the factor-based analyses and SPSS 28 was used to model school belonging over time. Hypothesis tests were two-sided with α = .05.
Results
Changes in Perceptions of School Belonging Over Time
Mean scores on the m-PSSM were 7.98 (SD 3.07), 8.01 (SD 2.65), 7.65 (SD 2.83), and 8.39 (SD 3.44), at baseline, 6, 12, and 24 months, respectively. The range of scores on m-PSSM were 4–20 across all time-points. There was no evidence to suggest that m-PSSM scores changed significantly over time (η2 = 0.05, F = 1.44, p = .232).
Predictors of Perceived School Belonging
As shown in Table 4, youth in secondary school (vs. those in elementary school) reported lower perceptions of school belonging over time (β = 0.91, p = .003), as did youth with psychopathology (vs. those without psychopathology, β = 0.82, p = .013). Whereas youth with positive social/peer supports (β = −0.06, p < .001) and school environments (β = −0.08, p < .001) reported more school belonging, and those who experienced peer victimization were more likely to report lower school belonging (β = 0.23, p < .001). Youth living in communities with higher residential instability reported lower school belonging (β = 0.56, p = .028). In contrast, youth living in areas of higher material deprivation reported greater perceptions of school belonging (β = −0.48, p = .022). Whether youth completed the m-PSSM during COVID-19 lockdown ordinances had no impact on their perceptions of school belonging.
Post Hoc Tests
Changes experienced by youth during the transition from elementary to secondary school may be masked by the lack of change reported by youth who remained in their respective school during the study. Thus, as a post hoc sensitivity analysis, mean scores on the m-PSSM for the subset of youth (n = 45) who were 11–13 years at baseline (and thus would have transitioned to secondary school during the follow-up) were examined. Findings again showed no significant change in m-PSSM scores over time among youth who transitioned to secondary school (η2 = 0.06, F = 1.87, p = .140). While the sample size for this sensitivity analysis was relatively small, it was sufficiently powered (1–β = .92) to detect observed effects.
Discussion
Measurement Properties of the m-PSSM
These findings suggest that the items and construct of perceived school belonging, as measured using the m-PSSM, are interpreted similarly between youth with physical illness in elementary versus secondary school. Because threshold three on item one (“I feel close to people at my school”) was freed during invariance testing, partial invariance of the m-PSSM was established. Given their developing cognitive processes, it is possible that younger youth (i.e., those in elementary school) may not be able to distinguish between a neutral versus disagree/strongly disagree disposition of feeling close to people at their school. Hence, this threshold would be different for younger versus older youth, whose cognitive processes are more mature. Indeed, evidence suggests that compared to adolescents, children are more likely to provide responses at the extremes (e.g., strongly [dis]agree) when rating their emotions (Chambers & Johnston, 2002). Partial invariance is considered sufficient for comparing latent variable means between groups (Steinmetz et al., 2009). Non-invariant thresholds (or intercepts) can substantially influence latent variable comparisons, particularly in the presence of non-invariant factor loadings (in the current study, all factor loadings were invariant) (Steinmetz, 2013). However, evidence suggests that having ≥2 invariant factor loadings and one invariant threshold set\intercept is sufficient for valid comparisons (Baumgartner & Steenkamp, 1998). This is relevant for group-based comparisons or comparisons over time that aim to model the natural course of perceived school belonging or in the evaluation of school-based policies that aim to promote school belonging among students—differences or changes observed in reports on the m-PSSM reflect real differences and are not an artifact of measurement error related to differential interpretation of school belonging.
Perceptions of School Belonging Over Time
Evidence from this study suggests that youth with physical illness have stable perceptions of school belonging, a finding that is consistent with a report examining changes during the transition to secondary school (Vaz et al., 2015), but inconsistent with previous reports of decline in broader samples of youth (Anderman, 2003; Gillen-O’Neel & Fuligni, 2013; Witherspoon & Ennett, 2011). Given this stability, it is reasonable to consider that school belonging is established as a relatively fixed perception early in this population of youth. Indeed, evidence shows that one-third of the variance in secondary school belonging is explained by elementary school factors (Vaz et al., 2015). Thus, investments to foster positive dispositions to school and learning environments early in life, especially among those with physical illness, are critical and may lead to longer term effects during school years. More research is needed to substantiate this hypothesis in youth with physical illness. Despite evidence to the contrary (Jose et al., 2012), it is also important to consider that a 24-month follow-up may not be sufficient to detect significant changes in perceptions of school belonging. Consistent with previous work (Vaz et al., 2015), findings from post hoc analyses showed no evidence to suggest that changes in perceived school belonging were experienced by youth who transitioned to secondary.
Predictors of School Belonging
Consistent with the socioecological model of human development, adapted for perceived school belonging (Allen et al., 2016; Bronfenbrenner, 1979), findings showed that predictors of school belonging were multilevel, acting at the individual, microsystem, and exosystem levels.
Youth Predictors
At the individual level, youth with psychopathology reported lower perceived school belonging compared to youth without psychopathology, a finding similar to previous reports comparing youth with physical illness to healthy controls (Kirkpatrick, 2020). There are likely multifaceted processes that can provide insight into this association. First, evidence suggests that youth with physical-mental comorbidity have lower quality of life in the domain of school environment compared to healthy norms and youth with physical illness only (Ferro, Qureshi, et al., 2021), and these effects increase with increasing number of mental comorbidities (Ferro, Qureshi, et al., 2021). Second, physical and mental illness independently contribute to more school absences and lower academic achievement in adolescent populations and it possible that these detrimental effects are compounded among adolescents with physical-mental comorbidity (Kirkpatrick, 2020). Third, physical and mental illness are also associated with increased likelihood of experiencing peer victimization (Fang et al., 2022), and for adolescents with physical-mental comorbidity, this association is further increased (Sitthi et al., 2022). While in the current study quality of life and experiences of peer victimization were measured at baseline and used to predict changes in perceived school belonging, it is possible that such psychosocial processes exhibit bidirectional relationships with school belonging over time. Formal tests of the directionality of these effects and potential mediational processes (e.g., using random intercept cross-lagged panel analyses) in the context of physical-mental comorbidity are needed in larger samples of adolescents. Such analyses would be useful in generating evidence to identify additional targets for school-based programming to foster a sense of school belonging among these vulnerable youth. It is also possible that educational accommodations that serve to promote academic achievement among youth with physical-mental comorbidity may inhibit feelings of school belonging. These youth may perceive less social acceptance from their peers due to being singled out for their need for supportive resources or through internal comparisons of their academic competence (Freeman & Alkin, 2000). Conversely, a lack of accommodations for youth with physical-mental comorbidity may contribute to lower perceived school belonging. Given the often-invisible nature of mental illness, accommodations to support individual education plans (e.g., extra time to complete work, alternative forms of assessment) may be overlooked or overshadowed by the physical health needs of adolescents with physical-mental comorbidity. This hypothesis is speculative and warrants further investigation using quantitative and qualitative research methodologies.
School Predictors
At the microsystem level, students with higher reported quality of life in the domains of peer support and school environment, also had a greater sense of school belonging, whereas those who reported more experiences of peer victimization had a lower sense of school belonging. With regards to the former, this association may be a function of two processes. First, because youth spend a large portion of their waking hours in school, those with supportive peer relationships and who do well academically are likely to feel a sense of belonging in the school environment (Baek, 2023). This is particularly relevant for youth with physical illness who are less likely to participate in extracurricular activities with their peers (e.g., community sports) outside of school (Arakelyan et al., 2020). Second, shared method variance on account of similar items between the KIDSCREEN-27 and m-PSSM may also drive the association. For instance, both scales ask youth about whether they are happy at school. The school environment domain of the KIDSCREEN-27 also asks about whether youth help/rely on their friends, which may be a proxy for m-PSSM items that target perceptions of feeling safe or close to people at school. With regards to the latter, there is ample robust evidence describing the association between peer victimization and poorer mental, social, and academic outcomes, including constructs of school belonging or connectedness (Baek, 2023; Korpershoek et al., 2020). School boards must continue to implement initiatives to eliminate peer victimization. Particular attention should be placed on youth with physical illnesses, as evidence suggests they are at increased risk for peer victimization (Pinquart, 2017).
Community Predictors
Findings related to community-level characteristics (exosystem) and perceived school belonging were novel. While evidence has shown that community and related contextual factors influence youth mental and social development, as well as academic achievement (Georgiades et al., 2007; Kingsbury et al., 2020), the current findings provide a more nuanced understanding of the multilevel influences on school belonging. The movement of families in and out of neighborhoods, which perpetuates residential instability, can negatively impact opportunities for youth to develop meaningful friendships with peers, leading to tenuous social bonds and lower social cohesion (Kingsbury et al., 2020). Given the time spent per day in school, the quality of peer and social bonds is critical to youth perceptions of school belonging—feelings of closeness, belonging, happiness, and safety are inherently interconnected with presence or absence of friends within school settings. The effect may be more pronounced for youth with chronic illness—physical, mental, or both—who already experience psychosocial disadvantage (Ferro, Qureshi, et al., 2021) and may not be able to reinforce peer bonds via other extracurricular activities (e.g., community sports beyond the neighborhood level) (Arakelyan et al., 2020).
Further, the findings showed that higher levels of community material deprivation were associated with a greater sense of school belonging. In these disadvantaged communities, schools, which receive government funding, may provide havens for youth to access resources not available outside of the school setting. These may include breakfast and lunch clubs, supervised play areas, library and technology resources (e.g., Internet-enabled devices), and opportunities to participate in extracurricular activities (e.g., sports, clubs) in a safe environment (Fredricks & Eccles, 2006; Hill et al., 2023). Because families who have children with physical illness often experience socioeconomic disadvantage (Spencer et al., 2013) and thus may be more likely to reside in communities with increased marginalization, such opportunities in school settings can foster a sense of school belonging. More research is needed to comprehensively understand the extent to which community context influences perceptions of school belonging among youth, with specific emphasis on evaluation studies assessing the impact of school funding policies that promote equitable access to resources in marginalized communities and subsequent psychosocial outcomes for vulnerable youth. For instance, evidence has shown that school connectedness mediated associations between income inequality and peer victimization (Pabayo et al., 2022).
Study Limitations
This study is not without some limitations. First, this sample of youth with physical illness were recruited from a single pediatric hospital, and underrepresented immigrant and non-White families, potentially limiting the generalizability of the findings. In a related vein, the small sample size prevented comparisons of perceived school belonging across different physical illnesses. Second, challenges abound when assessing individual perceptions of complex constructs, in this case, school belonging. Although the m-PSSM demonstrated sound psychometric properties in this sample of youth with physical illness, it is unknown whether perceptions accurately reflect actual belonging. For instance, an individual may report feeling unsafe at school despite the school having low occurrences of peer victimization, active playground monitoring by teachers, adequate resources, and being in a low-crime/non-marginalized neighborhood. While it may not be possible to measure actual school belonging, knowledge users must be cognizant that perceptions may be a poor indicator of reality. In a related vein, there was no information about school characteristics collected in the study. This information could be used to validate perceptions of school belonging, as well as offer school-level factors that could be included in the modeling (Allen et al., 2023). Importantly, the opportunity to examine cross-level interactions between school and community factors was not possible due to their sample size requirements. Third, perception of school belonging is an important psychosocial outcome; however, information on academic achievement or whether youth in the sample had individualized education plans was not collected and thus could not be used to understand the extent to which school belonging influences these academic outcomes in youth with physical illness.
Conclusions
The m-PSSM was found to have evidence of factorial validity, as well as sound internal consistency reliability in this sample of youth with chronic physical illness. Youth in elementary and secondary school both interpret the items and construct of school belonging, as measured by the m-PSSM, similarly. Perceptions of school belonging are stable over time for youth with physical illness, including during the transition from elementary to secondary school. Factors associated with school belonging are multilevel and align with the socioecological model of human development, with larger effects found for older youth, those with mental comorbidity, youth who have been peer victimized, and those living in communities with higher levels of residential instability and material deprivation. Given the stability of youth perceptions and that predictors are relatively non-modifiable, early and upstream efforts to promote school belonging are critical for youth with physical illness.
Footnotes
Acknowledgments
The authors acknowledge the children, parents, and health professionals and their staff without whose participation this study would not have been possible. We especially thank Jessica Zelman, Robyn Wojcicki, and Charlene Attard for coordinating the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This was supported by the Canadian Institutes of Health Research (PJT-148602). Drs. Ferro and Patte are supported by the Canada Research Chairs Program.