
Abstract
Healthcare waste (HCW) refers to all waste generated in establishments whose activities are focused on human and animal healthcare. Among such establishments are clinical laboratories, which are potential generators of that type of waste. HCW can pose significant risks to public health and the environment if not managed according to good environmental practices. This study analyses the processes involved in the management of HCW in 36 clinical laboratories in Belo Horizonte city, Brazil, using data from Healthcare Waste Management Plans. Non-hazardous waste constitutes 70.5% (290.9 kg day−1) of the total waste generated in those laboratories, whereas hazardous one (composed of HCW with biological, chemical and sharps-related risks) represents 29.5% (121.8 kg day−1). However, the study evidenced a percentage increase in the classification of HCW as hazardous in establishments that underwent technical inspections compared to those whose approval was solely based on declared data. Both segregation and collection stages revealed significant weaknesses in terms of data availability for profile analysis, which may reflect higher operational safety risks. Incineration was the treatment method most frequently adopted in the laboratories studied. Low recycling rates for non-hazardous HCW and indications of a lack of data on external HCW management processes were observed, suggesting a need for further studies on the topic. Improvements in HCW management processes through environmental education campaigns and implementation of public policies for encouraging participation in selective waste collection are also emphasized.
Keywords
Introduction
Healthcare waste (HCW) is all waste generated in human healthcare facilities (Agência Nacional de Vigilância Sanitária [ANVISA], 2018; Chartier et al., 2014) and animal healthcare ones (ANVISA, 2018), regardless of its being a direct or indirect result of healthcare activities. However, its classification is based on the risks it poses to human health and the environment – it is considered hazardous if the risks are biological, chemical, radiological or physical and non-hazardous if it poses no additional risks compared to domestic waste (Chartier et al., 2014). Practices for HCW management including waste minimization, proper segregation, recovery, treatment and disposal are integral to achieving sustainability in clinical laboratories, as claimed by GreenLab, and should always be prioritized (Idris and Samsudin, 2024; Lopez et al., 2017).
According to the World Health Organization (WHO), clinical laboratories are among the major sources of HCW (Chartier et al., 2014) and are expected to generate sharps waste (e.g. needles and lancets), biological waste (e.g. culture media and containers with bodily fluids), chemical waste (e.g. chemical reagents and organic solvents) and common waste, including plastic and paper packaging (Chartier et al., 2014; Pereira and Dias-Ferreira, 2023). Although HCW involves a portion of hazardous waste, if properly managed, that portion is not expected to exceed 25% of the total waste generated in healthcare facilities, as reported by Chartier et al. (2014). On the other hand, that percentage has been exceeded in previous studies conducted in clinical laboratories (Askarian et al., 2012; Chartier et al., 2014; Graikos et al., 2010; Kalogiannidou et al., 2018; Komilis et al., 2012; Mazloomi et al., 2019). Both quantitative and qualitative characteristics of HCW generated in healthcare facilities vary in function of type of service provided (Chartier et al., 2014; Komilis et al., 2012); however, the hazards can be reduced through proper segregation (Barbosa and Mol, 2018).
An effective implementation of HCW management procedures promotes public health and sustainability by minimizing the risks associated with that waste (Chartier et al., 2014; Lopez et al., 2017). On the other hand, it faces challenges, particularly in developing countries. Pereira and Dias-Ferreira (2023) pointed to segregation failures and limited access to off-site HCW management technologies in clinical laboratories associating such issues with disease transmission and environmental contamination. Prem Ananth et al. (2010) highlighted the influence of financial availability on the proper application of HCW management, and Anderson et al. (2021) emphasized the low number of studies detailing the environmental costs of healthcare facilities in low- and middle-income countries, which hinders the planning of water, sanitation and hygiene services, including HCW management.
In Brazil, HCW management is governed by federal regulations designed to ensure safe handling practices that protect public health and the environment. The main regulatory framework includes CONAMA Resolution No. 358/2005, which sets procedures for HCW management aligned with the National Solid Waste Policy (Law No. 12305/2010; Brasil, 2010; CONAMA, 2005). Additionally, ANVISA Resolution RDC No. 222/2018 establishes detailed requirements covering segregation, packaging, identification, internal transport, storage, treatment and final disposal, with an emphasis on best practices and mitigation of biological risks (ANVISA, 2018). Recent studies highlight the Brazilian HCW management scenario and the persistent challenges in implementing these regulations, including failures in segregation, insufficient staff training and infrastructural limitations, particularly in smaller facilities and socio-economically disadvantaged regions (Barbosa et al., 2025; Da Silva et al., 2005; Ribeiro et al., 2020). Understanding this regulatory context and its practical challenges is essential for interpreting results related to HCW management in the country.
Diaz et al. (2008) stressed the challenges imposed on HCW management by the limited availability of information on the qualitative and quantitative characteristics of that waste, especially in developing countries. Recent studies have shown the lack of data still hampers such a management within healthcare facilities and on a broader scale in developing countries (Fadaei, 2022; Tadesse and Dolamo, 2022).
Given the risks posed to public health, the importance of management, and the need for comprehensive data for a better process planning, this study analyses the management of HCW in clinical laboratories in the city of Belo Horizonte, Brazil, using their Healthcare Waste Management Plans (HCWMPs) for improving practices and promoting public health.
Methods
Data on the management process of HCW generated in 36 clinical laboratories in the city of Belo Horizonte, Brazil, were sampled. They were provided by Superintendência de Limpeza Urbana (Urban Cleaning Superintendence), the body responsible for approving and overseeing HCWMP in the city, in accordance with local legislation (Belo Horizonte, 2016).
The city was selected due to its significant population and limited number of scientific studies on the topic for Belo Horizonte, the most populous city and the capital of Minas Gerais state, as well as the sixth largest city in Brazil (IBGE, 2025). However, the scientific literature on the subject includes few studies, with no specific ones focused on procedures in clinical laboratories.
HCWMP is a mandatory document under Brazilian legislation (ANVISA, 2018) and must be submitted to a regulatory body. The selection criterion adopted in this study was to access the HCWMP of establishments that exclusively perform human and veterinary clinical laboratory functions and whose technical content has been approved and/or verified through an inspection by the competent authority. Data from hospitals, outpatient clinics, medical practices, retail services or other healthcare facilities that also performed activities related to clinical laboratories were not considered unless they included data on waste generated specifically from clinical laboratory activities.
The adoption of the approach was based on the understanding of Chartier et al. (2014) and Komilis et al. (2012), that is, the activities of an establishment influence the characteristics of the HCW generated and its management. Therefore, the information analysed had to refer to the activity that generated the HCW under study towards the obtaining of a profile that accurately reflected that of clinical laboratories. Veterinary clinical laboratories were included in the sample alongside human laboratories, for their activities are similar and their waste is expected to be comparable, following the understanding of Mazloomi et al. (2019) and Pereira and Dias-Ferreira (2023).
Data (see Table 1) were collected from all processes involved in HCW management according to the definitions of Brazilian legislation (ANVISA, 2018), organized into a spreadsheet and analysed with the use of R software (version 4.3.1).
Data collected from HCWMP of clinical laboratories from Belo Horizonte, Brazil.
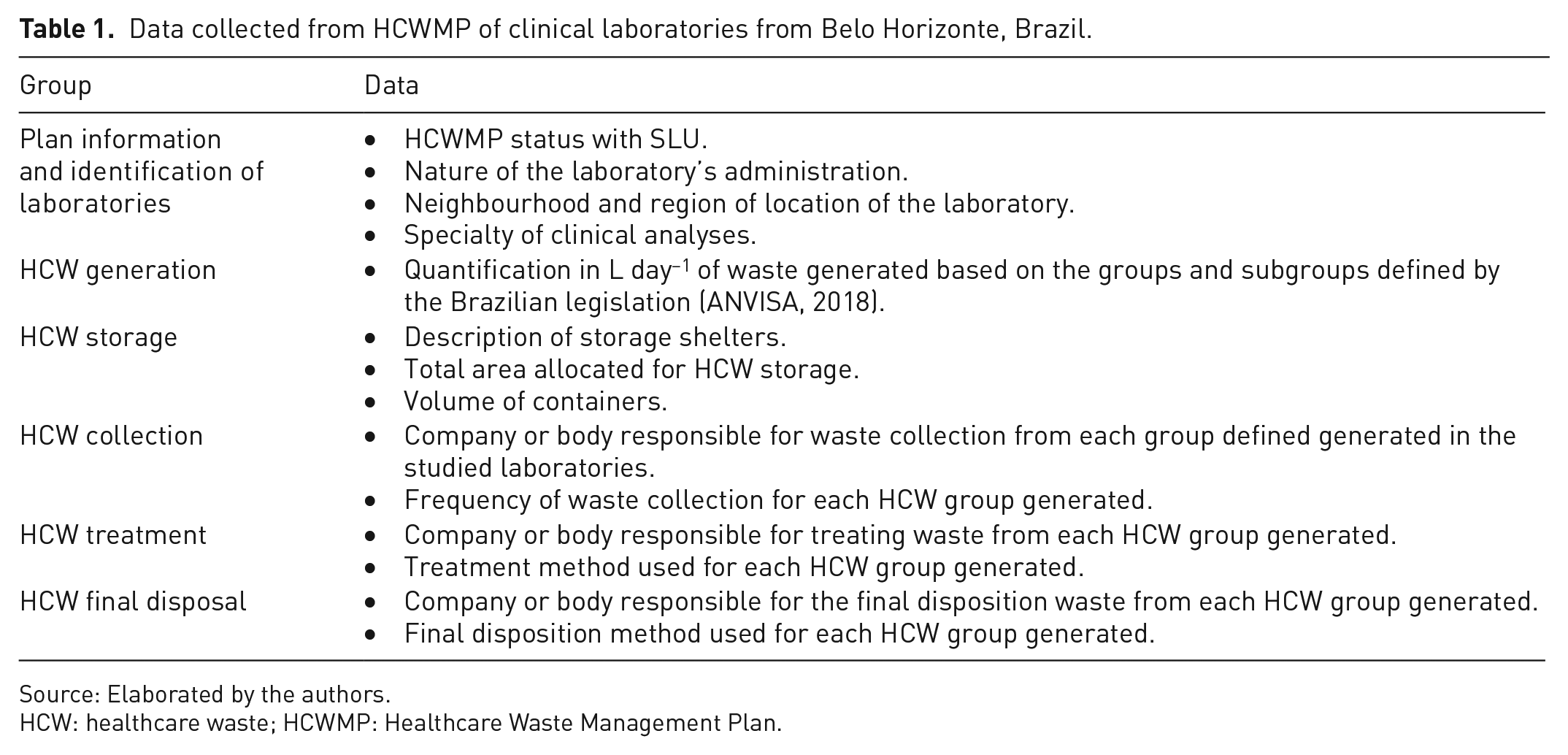
Source: Elaborated by the authors.
HCW: healthcare waste; HCWMP: Healthcare Waste Management Plan.
Waste generation values were converted from L day−1 to kg day−1 using the density values described in the methodology of Neves et al. (2022), that is, 100 kg m−3 for chemical and biological waste, 150 kg m−3 for non-hazardous waste, and 200 kg m−3 for sharps waste.
Results and discussion
Identification of laboratories
Among the 36 HCWMPs from which data were collected in this study, 6 (16.7%) were from veterinary clinical laboratories and 31 (83.3%) were from human clinical laboratories. Data from the latter were sampled from both analysis laboratories and collection points. All sampled plans came from privately administered laboratories and only 8 (22.2%) of such plans had an ‘implemented’ status at the time of data collection, that is, their content was confirmed through on-site inspections. The others had an ‘approved’ status, with their content approval based on a comparison between what was declared by the establishment and by the current legislation. The clinical laboratories were concentrated in the Central-South region of the city, with 23 HCWMPs (65.7%). Such a distribution pattern has been observed in other studies focused on HCW management from other types of waste generators, indicating potential inequalities in access to healthcare in the city of Belo Horizonte (Sousa et al., 2024). Figure 1 displays the geographic distribution of the establishments studied, and the quantification of the sampled HCW Management Plans by facility specialty is presented in Table 2.
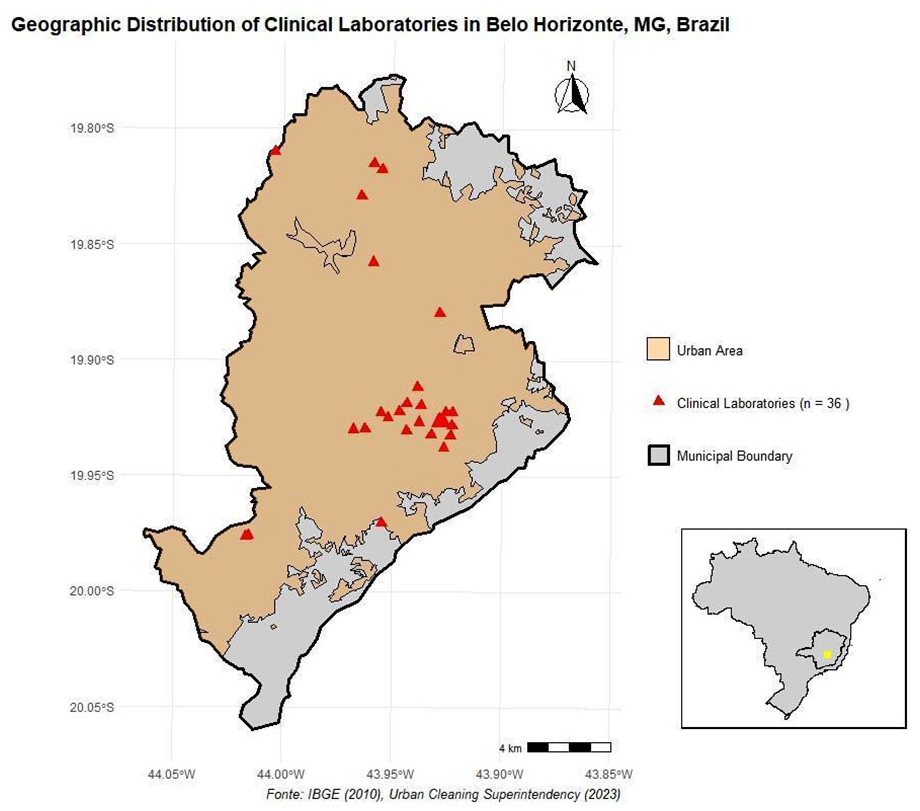
Geographic distribution of clinical laboratories in Belo Horizonte, MG, Brazil.
Number of sampled HCWMPs by facility specialty.
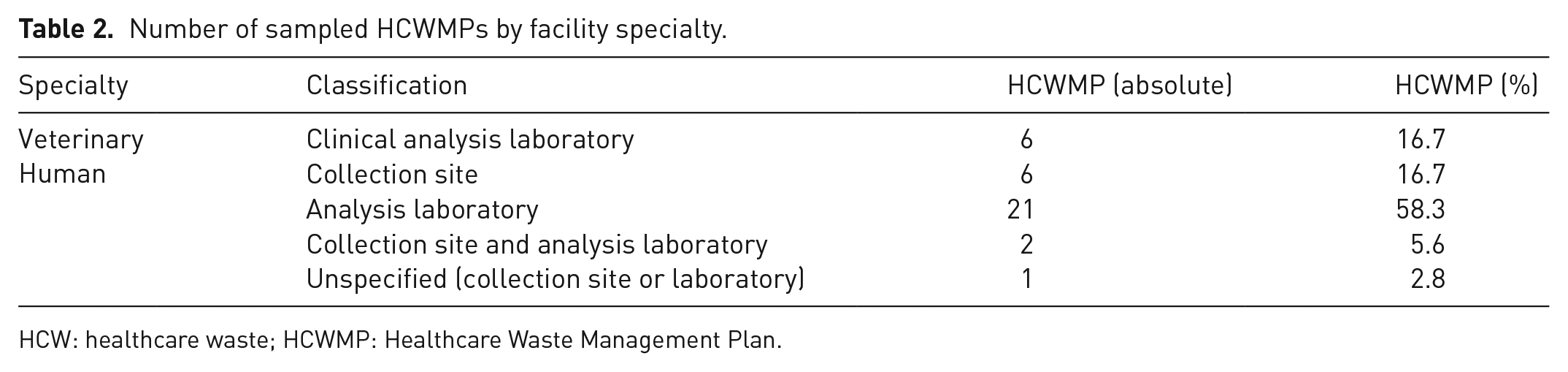
HCW: healthcare waste; HCWMP: Healthcare Waste Management Plan.
Intra-facility management
The generation, segregation, and storage of HCW are management stages that take place within the healthcare facility, in accordance with ANVISA (2018). The following section presents an analysis of how these procedures are implemented in clinical laboratories in Belo Horizonte.
Specifically, both human and veterinary laboratories included in our sample perform highly comparable activities in terms of sample collection, laboratory analysis processes and waste generation characteristics. As a result, the official evaluation process does not differentiate them in terms of waste generation rates or management typologies. For this reason, and to remain consistent with the regulatory framework in which the data were generated and reviewed, we analysed and presented the results for all laboratories together.
HCW generation
The average daily generation of HCW from clinical laboratories in Belo Horizonte was 412.8 kg day−1 (3115.1 L day −1), with a 11.5 kg day−1 (86.5 L day−1) rate per establishment studied, a value close to the 15.1 kg day−1 reported by Askarian et al. (2012). The percentage of non-hazardous HCW among establishments with approval with no on-site inspection was 81.2%, whereas that among those that underwent inspection was 61.7% (Figure 2). Such profiles may indicate a change in the classification of hazardous HCW during inspections by competent authorities. The generation profiles among establishments located in the Central-South region and other regions of the city showed similarities, suggesting a geographic distribution within a same city exerts minimal influence on HCW generation for a same healthcare activity (Figure 2).
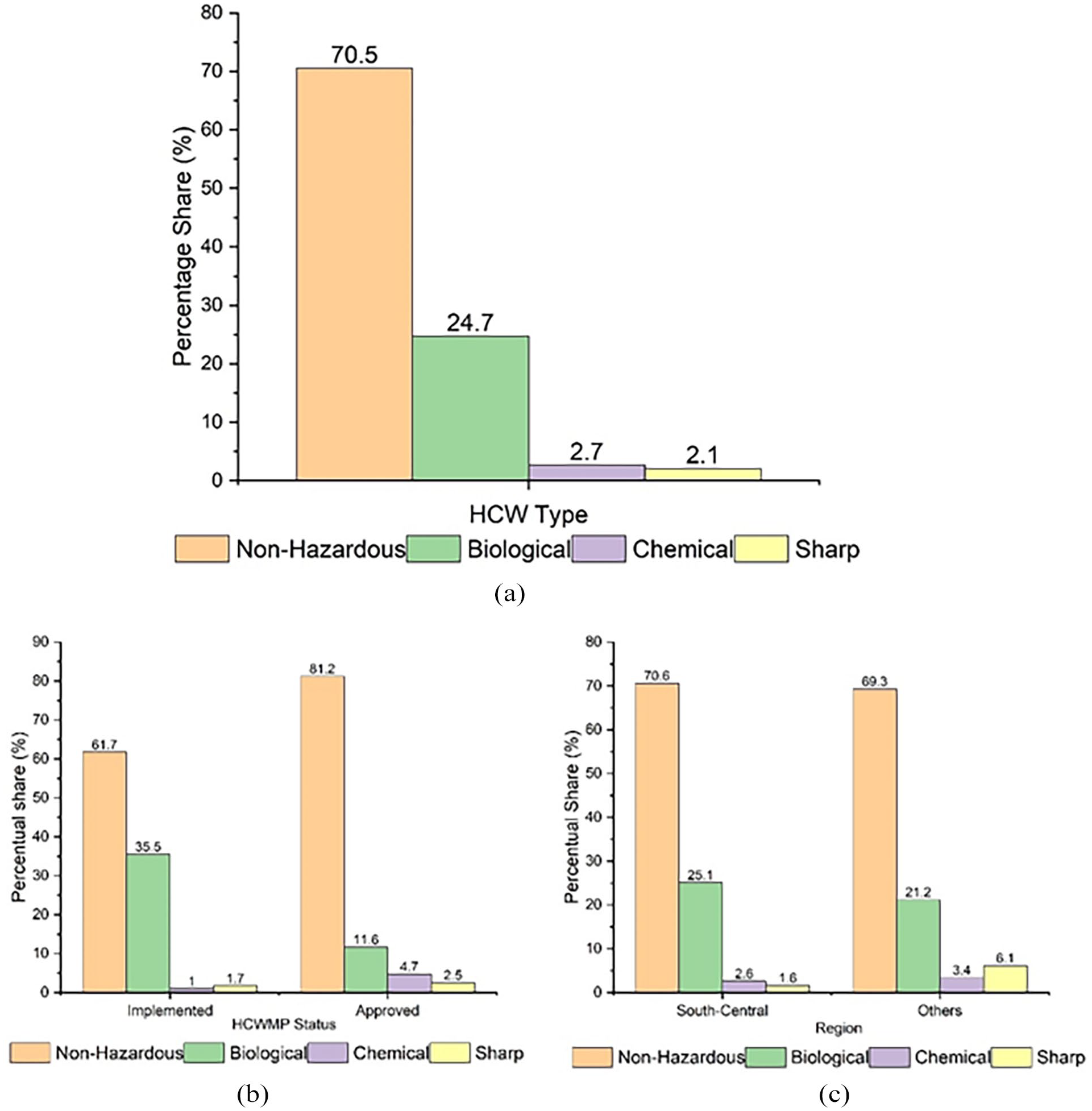
Percentage composition of healthcare waste generated in laboratories in Belo Horizonte: (a) overall composition in all clinical laboratories, (b) comparison of waste generation by HCWMP status (implemented vs approved) and (c) comparison of waste generation by region (central region vs other locations).
Non-hazardous waste was predicted in all plans consulted, showing recurrence in generation among laboratories, as observed by Hussein (2022) and Pereira and Dias Ferreira (2023). The rate of waste generation was 290.9 kg day−1 (1898.1 L day−1), representing an 8.1 kg day−1 (52.7 L day−1) average generation per establishment. Non-hazardous waste accounted for 70.5% of the total mass generated in the city, which is lower than the ideal 75% suggested by Chartier et al. (2014) for non-hazardous waste in healthcare facilities. However, the value found is higher than that reported in previous studies on HCW management specifically in clinical laboratories (52%; Askarian et al., 2012, 37%; Mazloomi et al., 2019, 2–4%; Kalogiannidou et al., 2018, 65%; Komilis et al., 2012, and 8%; Graikos et al., 2010). The percentage of non-hazardous HCW proposed by Chartier et al. (2014) is based on average generation across various healthcare typologies and may not be factual for certain specialties due to the specificities of each activity. That proposition is reinforced by studies on HCW generation in other medical typologies in Belo Horizonte, which reported different percentages for hazardous HCW, namely, 3% in pharmacies (Sousa et al., 2024), 18% in hospitals (Neves et al., 2022) and 26% in dental clinics (Sousa et al., 2024).
Hazardous waste (World Health Organization [WHO], 2018) accounted for 121.8 kg day−1 (1939.6 L day−1), that is, 29.5% of the total waste generated in laboratories. Its largest portion corresponded to biological waste, followed by chemical and sharps waste. The generation of at least one of those three waste groups was verified in all establishments studied, with no generation of radiological waste observed.
Biological waste
The recurrence of infectious waste generation in clinical laboratories is presumed due to the activities performed in those establishments. Therefore, laboratories are expected to have biological waste with infectious characteristics among their HCW, such as tubes and other containers with blood and bodily fluids, culture media and human and animal tissues (Chartier et al., 2014).
Biological HCW represents 24.7% of the total waste and 83.7% of the hazardous waste generated in the studied laboratories. The generation rate of biological HCW was 102.1 kg day−1 (1021.3 L day−1), representing a 2.9 kg day−1 (29.2 L day−1) average per establishment studied, a value close to the 3.86 kg day−1 reported by Endris et al. (2022) for that waste group. Such a type of waste was predicted in 35 of the 36 establishments studied.
WHO (2018) suggests a 10% average participation of biological HCW in the total waste generated in healthcare facilities under good HCW management conditions. However, previous studies reported a higher percentage of biological HCW than the average prescribed. Kalogiannidou et al. (2018) found 15% in Greek laboratories, and Graikos et al. (2010) and Komilis et al. (2012) reported 35% and 83%, respectively, in the same region. Askarian et al. (2012) and Mazloomi et al. (2019) found 56% and 43% of infectious waste, respectively, in Iranian laboratories in different locations. Those values support the understanding of clinical laboratories as healthcare activities with a high potential for generating infectious waste, which impacts the total amount of hazardous waste.
The largest portion of biological waste observed in this study belongs to subgroup A4 of ANVISA (2018), which corresponds to empty transfusion bags and clinical analysis containers with urine, faeces, or secretions from patients without confirmed infection by pathogens of epidemiological importance, or containers without free fluids. That subgroup of biological HCW also showed the highest generation rates when analysed by establishment status (approved or implemented) and location within the city (Central-South region or others), as shown in Figure 3.
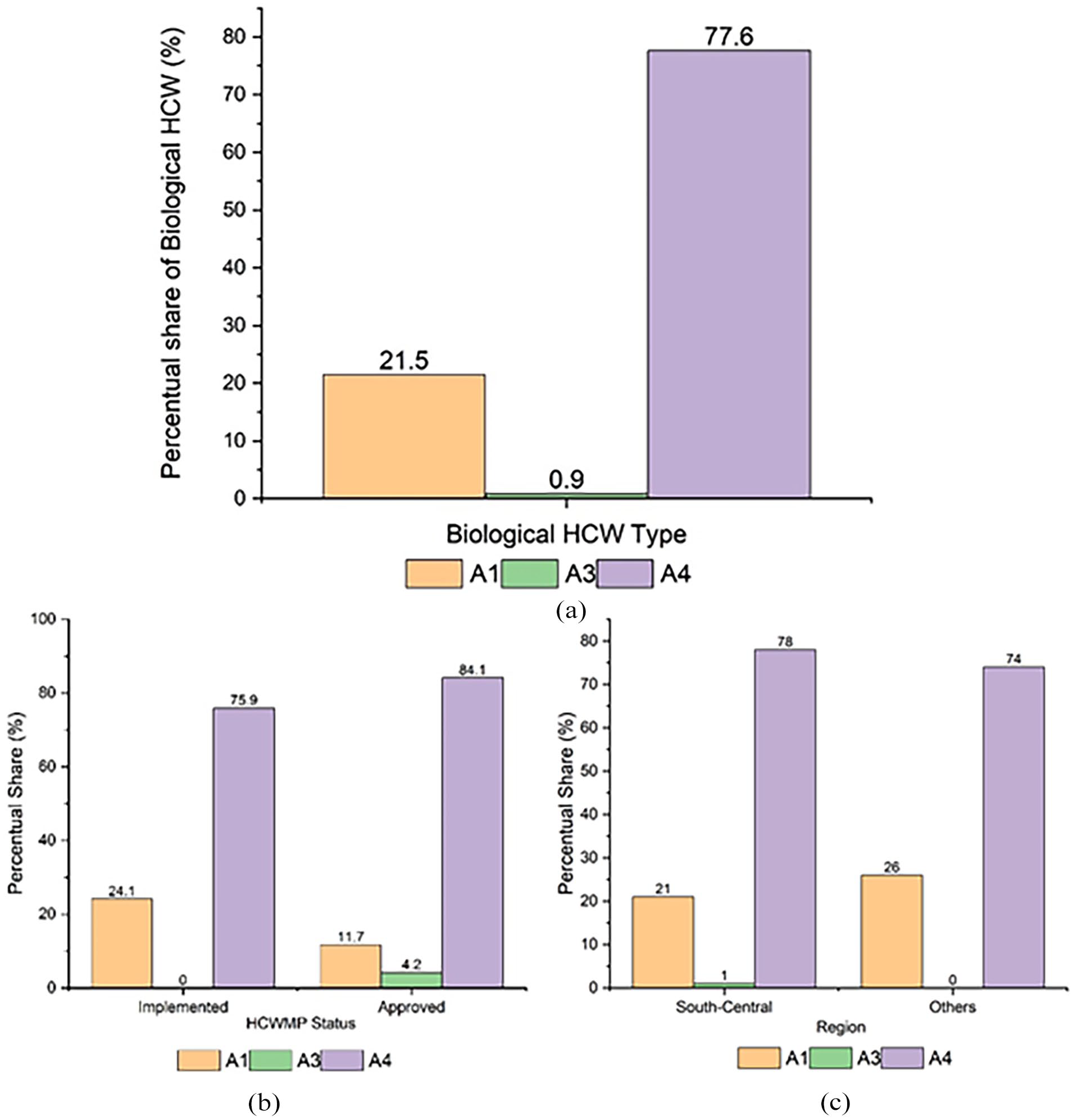
Percentage composition of biological healthcare waste generated in laboratories in Belo Horizonte: (a) overall composition in all clinical laboratories, (b) comparison of waste generation by HCWMP status (implemented vs approved) and (c) comparison of waste generation by region (central region vs other locations).
In addition to having the highest volume among biological HCW, the subgroup showed the highest frequency of generation among the studied establishments, being listed in 35 of the 36 plans that predicted biological waste generation. This result is consistent with the literature – Hussein (2022) pointed to the high frequency of generation of that type of biological HCW in studies of HCW generated in clinical laboratories. Despite the significant HCW generation, that is, corresponding to 79.3 kg day−1 (792.7 L day−1) in the city and 2.3 kg day−1 (22.6 L day−1) per establishment, representing 19.2% of the total HCW and 65.1% of hazardous waste, that subgroup is considered the one of lowest potential risk to human health (Mol et al., 2017).
The second type of biological HCW with highest generation belongs to subgroup A1, which corresponds to culture media, vaccines with live, attenuated or inactivated microorganisms, transfusion bags containing free blood and sample residues containing free blood or other fluids (ANVISA, 2018). Such waste was generated in 16 (44%) out of the 36 HCWMPs consulted. Hussein (2022) also verified a low frequency (22%) of that biological waste among the clinical laboratories studied, with a 22.0 kg day−1 (219.6 L day−1) generation rate, which is equivalent to 5.3% of total waste and 18.0% of hazardous waste. A higher percentage of that subgroup was observed in the total biological HCW generated in laboratories that underwent inspections compared to those that only obtained approval (Figure 3). The result is similar to that discussed elsewhere for total HCW, indicating an increase in HCW with higher associated risks due to a better characterization during the inspection process.
Brazilian legislation allows laboratories to dispose of bodily fluids in the sewage network, provided they comply with the rules established by environmental agencies and competent sanitation services (ANVISA, 2018). The permission is not restricted to the Brazilian context or to a single type of healthcare facility. Chartier et al. (2014) described laboratories as contributors to presence of blood in wastewater from the disposal of samples in sewage networks in an international context and Khan et al. (2021) pointed to differences in wastewater treatment regulations in hospitals among various countries, which increases the risk of contamination by chemical and biological agents. Therefore, disposal in the sewage network may justify the low participation of that subgroup.
Waste classified as A3, that is, human anatomical parts or products of fertilization without vital signs (ANVISA, 2018), showed the lowest generation rate among biological waste (0.9 kg day−1; 9.04 L day−1), corresponding to 0.2% of total waste and 0.7% of hazardous one. Such biological waste was verified in 5 out of the 36 establishments studied; however, none of them were among those that underwent inspection (Figure 3).
No biological waste containing animal carcasses or inoculation products, subgroup A2 (ANVISA, 2018), or human tissues with high infectivity due to prions, subgroup A5 (ANVISA, 2018), was found. Similarly to the study of total HCW generation, no significant indications of influence of geographic variables on the composition of biological HCW generated in the analysed laboratories were observed.
Chemical and sharps waste
The generation rate of chemical HCW was 11.1 kg day−1 (111.1 L day−1), of which most (99.94%, 11.10 kg day−1 or 111.0 L day−1) consisted of medications – expired or used medications and reagents in the analysis process. The remaining chemical waste was sporadically generated and included fluorescent lamps, batteries and accumulators. Chemical HCW accounted for 2.7% of the total HCW (Figure 2) and 9.1% of hazardous waste. Such a low participation can be interpreted as a reflection of the low frequency of generation of that HCW in clinical laboratories. That waste is less often listed among ANVISA (2018) groups with verified generation, having been observed in 24 out of the 36 HCWMPs (66.6%). Hussein (2022) also reported a lower frequency of chemical HCW generation compared to biological, sharps and non-hazardous waste, but with a lower percentage in comparison to the present study (22.0%). However, some previous studies focused on clinical laboratories highlighted a lack of segregation of that waste, which implies a lack of knowledge on the mass percentage of chemical waste (Askarian et al., 2012; Graikos et al., 2010; Hussein 2022; Kalogiannidou et al., 2018; Komilis et al., 2012; Mazloomi et al., 2019; Pereira and Dias-Ferreira, 2023).
Despite the small proportion of chemical HCW in the total waste generated, Chartier et al. (2014) highlighted the importance of properly managing solvents in laboratories due to their inherent characteristics and associated health risks. The issue is further exacerbated by the lack of knowledge on proper management practices for such waste. According to Hussein (2022), chemical HCW is the type of waste that causes most uncertainty among laboratory staff regarding its management, with the sewage collection system frequently cited as the ideal disposal method. Pereira and Dias-Ferreira (2023) also reported failures in the segregation of chemical waste in all laboratories analysed in their study, and Patel et al. (2024) highlighted a frequent lack of internal regulations for the disposal of chemical waste from hospital laboratories. The risks associated with such HCW, along with deficiencies in segregation and disposal, represent a significant challenge for environmental sanitation, including both solid waste and liquid effluent treatment, as emphasized by Khan et al. (2021) in their study on HCW management in hospitals.
Sharps waste, found in all establishments studied, was the hazardous HCW group with highest generation frequency. Hussein (2022) pointed to a high frequency of generation for such HCW, and Pereira and Dias-Ferreira (2023) suggested more careful attention should be given to sharps HCW due to the higher perceived risk associated with it, which may explain its presence in most laboratories. A similar behaviour has been observed in other healthcare typologies. Al-Khatib (2024) reported an adequate container for sharps waste separation was found only in the clinical laboratory among all units of the hospital studied. The legislative and regulatory framework also plays a significant role in the segregation of sharps waste. Kalogiannidou et al. (2018) and Komilis et al. (2012) did not report specific quantities for sharps waste, as it is typically classified together with biological waste. This highlights the role of risk perception and enhanced segregation practices for this category, despite the constraints posed by legislative frameworks.
Sharps waste showed the lowest quantitative generation among the other HCW groups – an 8.6 kg day−1 (43.0 L day−1) rate in Belo Horizonte and a 0.2 kg day−1 (1.2 L day−1) average per establishment, representing 2.1% of the total HCW and 7.1% of hazardous waste (Figure 2). The rate is considerably lower than that observed by Endris et al. (2022), namely, 1.01 kg day−1 per establishment, whereas the literature reports variations in the percentage of sharps HCW. The one found is similar to that provided by Mazloomi et al. (2019; 2%), but lower than that observed by Askarian et al. (2012; 5%). The percentage share of sharps HCW in the total waste generated may be due to the small proportion represented by those wastes, which can lead to significant percentage variations even with minor changes in mass, as well as segregation characteristics, as aforementioned.
Storage
All laboratories studied had separate containers for common, biological, chemical and sharps waste, following the guidelines of Brazilian legislation (ANVISA, 2018) and meeting the minimum requirements for good practices outlined by Chartier et al. (2014). However, only 3 of the plans reported the dimensions of the storage shelters, whereas the remaining 33 provided the number and volume of containers allocated for each type of waste. Such a fact can be explained by the provisions of local (Brasil, 2020) and national (ANVISA, 2018) legislation, which exempts Brazilian establishments from constructing temporary shelters if the waste generation and collection frequency prevent the accumulation of HCW (ANVISA, 2018). At the local level, small generators are exempt from constructing dedicated HCW shelters, since municipal regulations permit the storage of waste in dedicated rooms with restricted access, provided the amount of waste does not exceed 1000 L per collection (Brasil, 2020).
Shared storage between sharps waste and biological waste was observed, for such a management strategy is permitted by Brazilian legislation for non-hospital healthcare facilities (ANVISA, 2018). It shows some similarity to the Greek legislative definitions described by Kalogiannidou et al. (2018) and Komilis et al. (2012), despite Brazilian legislation requiring quantification of those materials in separate groups.
The lack of information on the characteristics of the storage strategy used in the laboratories in this study hinders evaluations of the application of correct management practices. An adequate storage of HCW in appropriate and specific containers for each type of waste and in a location restricted to patients or passer-by is an essential measure for prevention of accidents and reduction of risks, as claimed by Al-Khatib (2024) and Pereira and Dias-Ferreira (2023). Cook et al. (2023) emphasized both storage and transportation phases of HCW are those during which professionals are most exposed to risks due to their closer proximity to the materials, thus requiring increased vigilance and adherence to good practices.
Extra-facility management
The HCW management stages analysed – collection, treatment and final disposal – take place outside healthcare facilities. The analysis of the studied plans concerning these procedures revealed a marked lack of data. This pattern may be related to the limited access that clinical laboratory professionals have to knowledge about the environmental aspects and impacts associated with their work activities, as described by Yurt et al. (2025). Therefore, it is necessary to expand the role of environmental sciences in both formal education and continuing training for healthcare professionals to promote a systemic understanding of the environmental implications of poor planning or failures in HCW management, ultimately improving processes and protecting health.
Regarding environmental education campaigns, greater emphasis can be placed on designing targeted initiatives for laboratory professionals that address the specific challenges of HCW management. For example, training modules could focus on practical aspects such as proper segregation of hazardous and non-hazardous waste, understanding local and national regulations and recognizing the environmental and public health implications of inadequate waste handling (WHO, 2018; Windfeld and Brooks, 2015). Workshops and continuing education programmes can be delivered in partnership with local health authorities, universities and environmental agencies to ensure alignment with current guidelines and best practices. Additionally, developing accessible resources such as manuals, posters or digital tools tailored to the laboratory context can support day-to-day decision-making (Patel et al, 2024). These initiatives should be designed to be participatory and context-specific, fostering critical reflection and behaviour change among professionals while reinforcing institutional commitment to safe and sustainable waste management.
Waste collection
Inefficiencies in waste collection related to frequency and availability of suitable vehicles are commonly observed in developing countries. The scenario has been described for both non-hazardous waste (Ferronato and Torretta, 2019) and hazardous one (Al-Khatib, 2024; Ferronato and Torretta, 2019; Pereira and Dias-Ferreira, 2023), leading to waste accumulation and increased risks associated with vectors and environmental contamination.
However, such a scenario was not observed in the present study. The collection of HCW in the laboratories studied was performed at sufficient frequency to prevent waste accumulation in healthcare facilities, in accordance with local regulations.
Regarding collection practices, although the overall adequacy of collection was reported, it is important to consider the variability in collection frequency and its potential implications. Variations in collection schedules may lead to operational inefficiencies, such as increased temporary storage requirements or higher risk of improper segregation if containers remain full for longer periods (Ribeiro et al., 2020; Windfeld and Brooks, 2015). Moreover, inconsistent collection can pose environmental and health risks, especially for infectious or sharp waste fractions that require timely removal to prevent accidents and contamination (Chartier et al., 2014). Therefore, further analysis of collection frequency variability is recommended to identify opportunities for standardization and to ensure both safety and efficiency in HCW management systems (WHO, 2018).
Non-hazardous waste
The non-hazardous waste generated in the laboratories studied is collected by municipal services and sent to landfills – it occurs in 33 laboratories, with no information on the procedures for the remaining 3 ones. The collection frequency varied among the establishments – the highest one refers to daily collection and the lowest one denotes collection three times a week, as shown in Figure 4. Due to the high frequency of non-hazardous HCW collection, the median volume collected was lower than that observed for hazardous HCW (Figure 5).
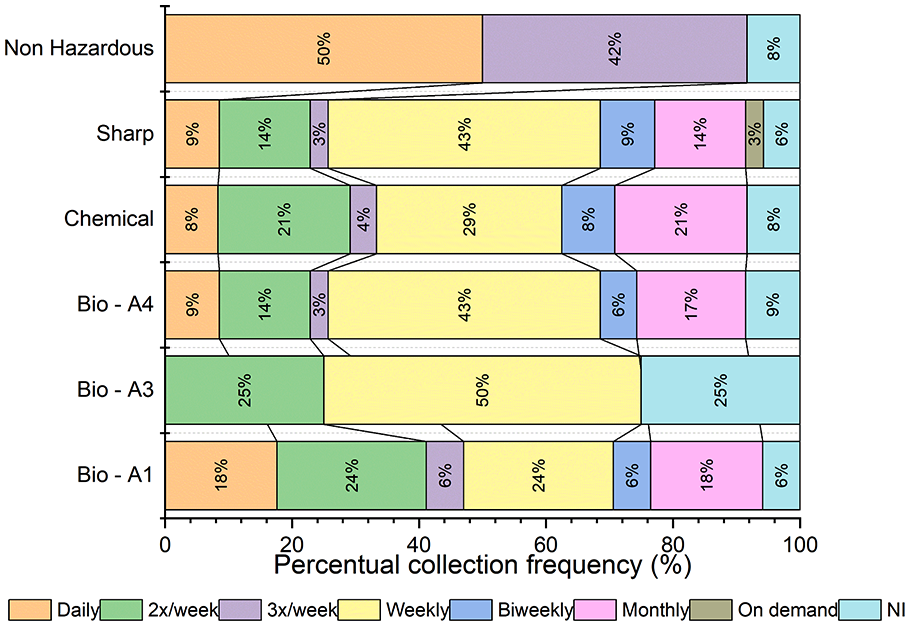
Comparison of collection frequency by type of HCW in clinical laboratories with percentage distribution across different collection intervals.
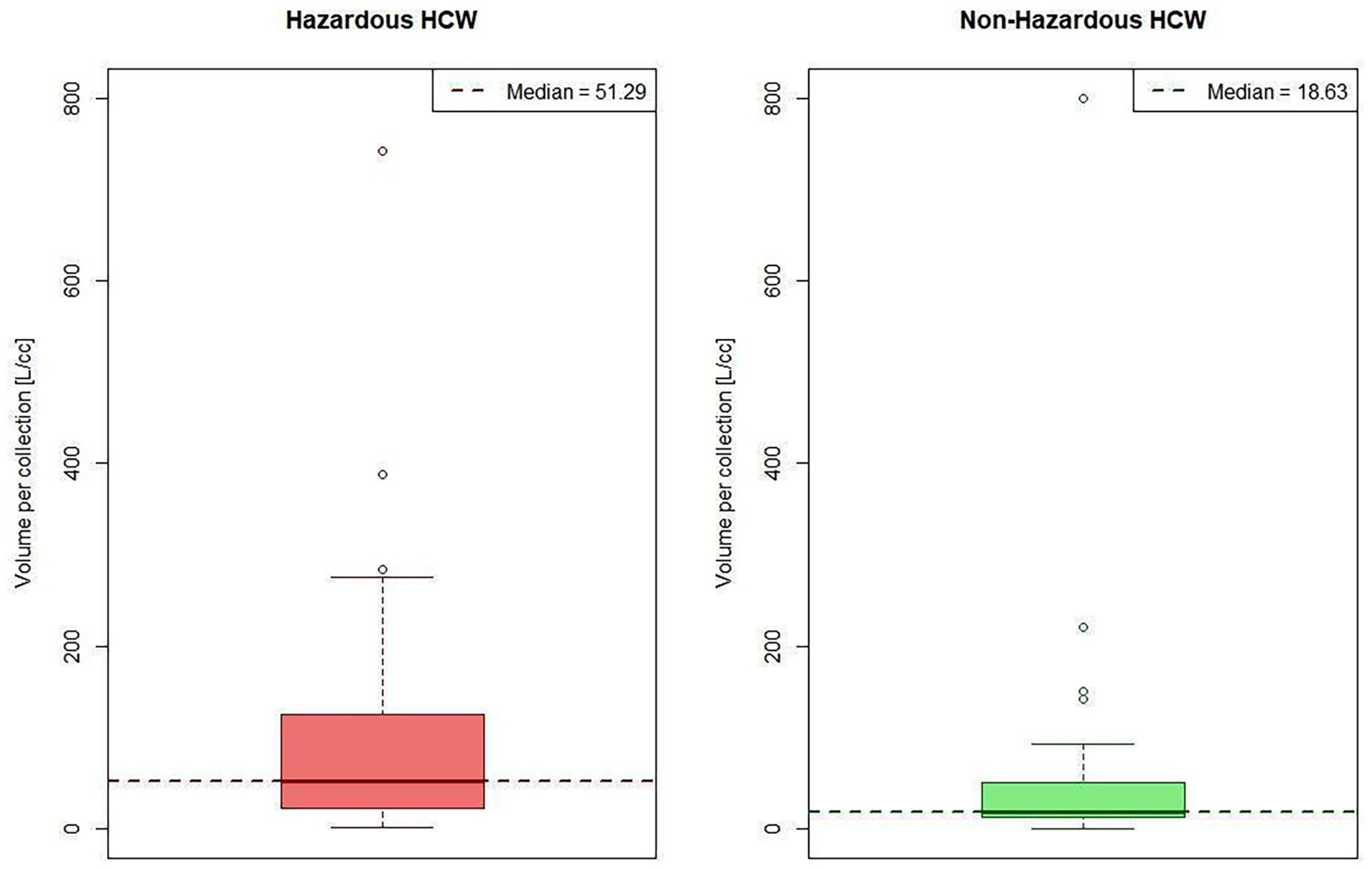
Comparison of hazardous and non-hazardous HCW volume per collection (L cc−1).
Despite the significant generation of non-hazardous waste, a reduced allocation for the selective collection was observed. The non-hazardous HCW destined for recycling totalled 6.2 kg day−1 (41.6 L day−1), corresponding to 2.1% of the total non-hazardous HCW and 1.5% of the total waste generated by the laboratories. Among the establishments that allocate waste for selective collection, the average generation was 0.6 kg day−1 (4.2 L day−1), representing 28.3% of common HCW. The value contrasts with the average allocation of common HCW for undifferentiated collection, which amounts to 7.9 kg day−1 (52.7 L day−1) per establishment.
Apart from the low volume, there was limited participation among the establishments – only 10 out of the 36 laboratories consulted in this study (27.7%) planned to send their waste for selective collection. That number can be interpreted as a result of the low coverage of door-to-door selective collection in the capital of Minas Gerais, rather than to the characteristics of common HCW. Almeida and Mol (2020) highlighted the low coverage of door-to-door selective collection in Belo Horizonte, which may reflect difficulties in healthcare facilities’ adherence to the service, as reported in previous studies conducted in the city (Sousa et al., 2024).
The phenomenon is not limited to Belo Horizonte. Joseph et al. (2021) pointed to low recycling rates of plastics in healthcare facilities worldwide due to segregation failures and legislative barriers. According to Chartier et al. (2014), the common HCW expected in laboratories is mostly composed of packaging made from recyclable materials such as plastics and cardboard, a pattern observed by Komilis et al. (2012) and Pereira and Dias-Ferreira (2023). Therefore, the amount of HCW destined for recycling in clinical laboratories can be potentially increased. Improvements in management can be achieved by increasing both the number of laboratories served by selective collection through sectoral efforts with the public sector and the HCW segregated at the source through a better laboratory management. However, waste management must be seen not only as a process necessary for compliance with environmental legislation but also as a tool for promoting public health (Lopez et al., 2017) and sustainable development (Pereira and Dias-Ferreira, 2023).
The recently published Brazilian National Circular Economy Plan includes among its objectives the goal of keeping materials circulating within value chains for as long as possible. To achieve this, it proposes, among other instruments, the creation of a database to support entrepreneurs in adopting circular practices and the expansion of selective collection networks so that discarded materials can enter the recycling stream, thereby consolidating circular economy practices for post-consumer packaging (Brasil, 2021b). As noted, post-consumer packaging is the main type of non-hazardous waste generated by clinical laboratories (Chartier et al., 2014). This approach aligns with the Brazilian National Solid Waste Policy (Brasil, 2010), which prioritizes resource recovery through recycling and establishes landfilling as the last resort for materials that cannot generate value. According to Dutra et al. (2018), investments in recycling systems have shorter payback times compared with the costs associated with disposing of potentially recyclable materials, while also delivering better environmental performance and generating decent jobs – principles of a just transition towards a circular economy as envisioned in Brasil (2021b). In addition to these legal frameworks, Brazil has a financing mechanism established by the Recycling Incentive Law (Law No. 14260/2021), which provides access to resources that can be invested in structuring recycling programmes (Brasil, 2021a). Therefore, the context analysed here reveals opportunities to improve waste management through existing public policies aimed at strengthening recycling systems. Continued research is needed to assess the potential generation of recyclable materials in the territory, as in this study, and public authorities have an essential role in ensuring the effective implementation of these legal instruments.
Hazardous waste
The most frequently reported collection frequency for hazardous waste occurred weekly, as shown in Figure 4. Despite the variability in frequency, none of the establishments exceeded the 1000 L per collection limit set by Brazil (2020), which would require the construction of waste storage shelters. Figure 5 shows the distribution of the volume of hazardous waste per collection in L day−1. The median value obtained was 51.29 L per collection.
Treatment and final disposal
Incineration, commonly reported as the most widely used technology for HCW treatment (Udayanga et al., 2023; Yoon et al., 2022), was the one most frequently cited among the laboratories studied (see Figure 6). Manupati et al. (2021) defined it as the most suitable method for the post-COVID-19 context, provided attention is paid to its environmental liabilities.
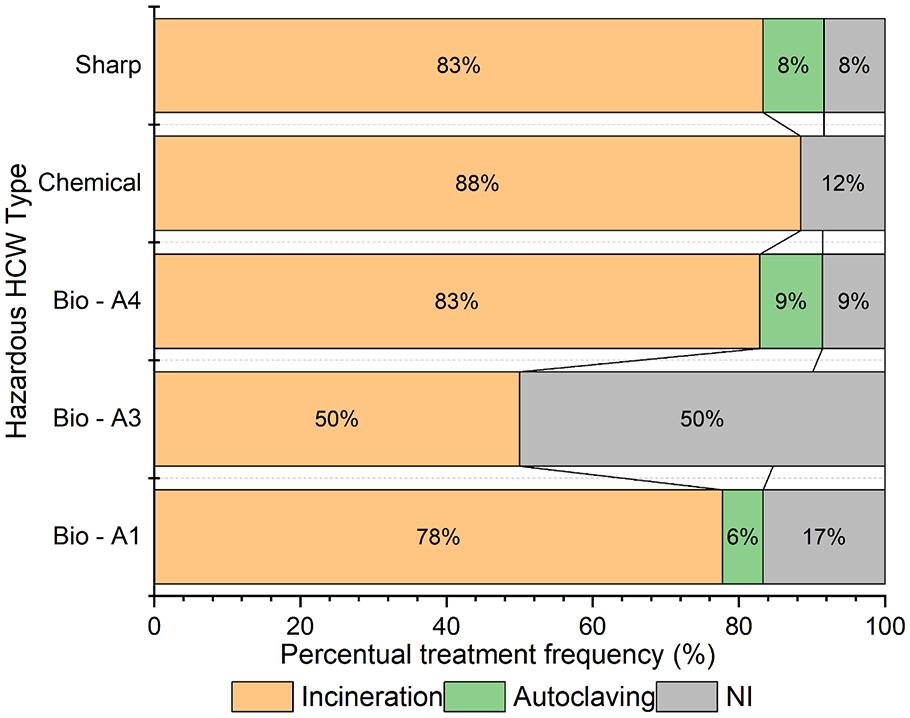
Percentage frequency of hazardous HCW treatment by type.
According to Kiliç and Kuzu (2021), autoclaving for the treatment of biological and sharps HCW was listed as the second most used method for HCW treatment in Turkey, with lower adoption rates than incineration alone. The procedures planned for waste treatment align with practices authorized by Brazilian legislation, for both aforementioned methods, are classified as environmentally appropriate by ANVISA (2018). Two laboratories indicated the recycling of chemical waste as an additional method to incineration, suggesting albeit on a small scale, such a GreenLab practice described by Lopez et al. (2017) has been adopted.
Three laboratories consulted did not describe the method or company responsible for treating their waste, despite having an active contract with the service provider. This fact may indicate a disconnection between healthcare professionals and the procedures necessary to ensure environmental preservation and public health associated with HCW, as highlighted by Sousa et al. (2024) in their study on HCW management in dental clinics in Belo Horizonte.
Regarding the final disposal of hazardous waste after treatment, all plans that included information on off-site management (91.6%) indicated final disposal in a licensed landfill authorized to receive that waste. Consistently with findings for non-hazardous HCW, all plans that reported off-site management indicated that waste was disposed of in municipal landfills.
It is important to note that the results of this study were discussed in comparison with other studies of the same type, which are sometimes conducted in different regions where normative, legislative and operational differences can influence the quantitative and qualitative aspects of the data. The limited participation in local-, regional- or even national-level discussions is associated with the lack of detailed and up-to-date information consolidated in national solid waste management systems in Brazil, as also reported by Barbosa et al. (2025) and in other developing countries according to the review by Zhang et al. (2024). In this context, there are significant challenges to conducting large-scale research on solid waste in developing countries, which is reflected in their underrepresentation in the scientific literature compared to studies describing management in the Global North (Zhang et al., 2024). In light of these challenges, research using performance indicators and assessing healthcare professionals’ knowledge can be valuable both for enriching the scientific literature on the topic and for providing better support to decision-makers (Barbosa and Mol, 2018; Barbosa et al., 2025). Patel et al. (2024) described the application of the WHO’s Healthcare Waste Management Rapid Assessment Tool, designed for developing countries, which integrates information on all management stages, healthcare workers’ knowledge and the legislative framework into quantitative management performance indicators. Conducting future research with a systemic approach that integrates the physical aspects of waste management and the knowledge of the professionals involved is of paramount importance for advancing the field, making access to funding and up-to-date data essential (Tadesse and Dolamo, 2022).
Conclusions
This study provided a comprehensive description of the procedures adopted by the studied clinical laboratories, thus contributing to the development of directives aimed at HCW management in those healthcare facilities. It also highlighted the concentration of clinical laboratories in the Central-South region of Belo Horizonte, which is consistent with previous studies on other types of healthcare facilities. However, no significant influence of geographic variables on the composition of HCW generated by establishments with the same healthcare activity in the city was observed.
The percentage of hazardous waste is close to the general standard prescribed by WHO, unlike previous studies on the same activity that demonstrated the adoption of good practices in the municipality. However, an increase in the percentage of hazardous HCW was observed in establishments that underwent inspections by the responsible authority compared to those whose approval was based on the content declared by the entrepreneur, indicating a better classification of HCW through inspections. Regarding the generation of common waste, low adherence to recycling was observed among those establishments, which is also consistent with previous studies in the city. Nevertheless, improvements must be made in the process towards the promotion of public health and sustainable practices beyond those drawn by legislation.
A lack of descriptions of temporary storage shelters and variability in collection frequency among the studied establishments was perceived, which points to greater fragility in the two management stages concerning occupational and environmental health protection. The treatment method most widely used for hazardous waste was incineration, followed by autoclaving and final disposal occurs in licensed landfills authorized to receive ashes and autoclaved HCW.
Despite the existence of signed contracts, a lack of data on the processes required for off-site HCW management was evidenced in the consulted plans. Therefore, closer engagement with professionals is suggested towards the identification of critical points and development of environmental education campaigns and actions for increasing healthcare facilities’ adherence to selective collection through expanded routes are recommended. This process should take into account the main questions and uncertainties raised by professionals during waste management, as well as studies aimed at including a greater emphasis on environmental education in the training of new professionals – an aspect already provided for in Brazilian legislation.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support provided by Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq).