
Abstract
This study is one of the first systematic attempts to examine the possibility of a common treatment facility (CTF) to treat infectious healthcare waste (HCW) in Nepal. First, the survey was conducted in 14 healthcare facilities (HFs) ranging from health posts to large hospitals selected from 120 total HFs in Nepalgunj sub-metropolitan city (SMC), a rapidly urbanising city of Nepal to investigate the current practices of HCW management (HCWM) and to estimate the waste generation and characteristics in the different HFs. The result shows that the average unit waste generation rate for health posts, clinics, urban health centres, and hospitals was estimated at 1.397 kg day−1, 1.608 kg day−1, 0.178 kg day−1 and 1.818 kg bed−1 day−1, respectively. Of the total 1242 kg day−1 HCW generated in Nepalgunj SMC, 73% is infected in the current situation, but if fully sorted at source, only 32% of the waste will be infected. Based on these HCW generation data and fraction of infectious waste, including waste management practices, three different scenarios are proposed for the capacity assessment and designing implementation modality of the CTF to treat infectious waste from all HFs of Nepalgunj SMC as a case study where an integrated solid waste management facility including material recovery facility and sanitary landfill site for municipal solid waste management is already in operation. The different implementation analyses are discussed, and the best implementation arrangement has been recommended for the sustainability of the project. This approach can be replicated in other cities alone or regions with many neighbouring cities of Nepal and explores a workable solution for HCWM in the rapidly urbanising cities of developing countries to help them improve their condition.
Keywords
Introduction
Healthcare waste (HCW) is posing a growing problem, particularly quickly in developing countries, like Nepal. In healthcare facilities (HFs) of many cities, especially in rapidly urbanising cities of Nepal, the amount of solid waste being generated is increasing rapidly as healthcare services are expanded. HCW management (HCWM) has become even more complex because of the disposal of highly infectious waste like disposable needles, syringes, and similar infectious waste together with municipal solid waste (MSW). There are many potential hazards associated with handling HCW, posing risks not only to the patients and healthcare workers but also to the community and the environment (World Health Organization (WHO), 2005). HFs generate large amounts of diverse waste, which require proper treatment and disposal to protect the person’s handling it and the environment. Thus, an integrated HCWM approach, including waste minimisation, segregation, collection, transportation, treatment, storage and disposal of infectious and hazardous waste in each HF, is required to reduce the risks to human health and the environment. HCWM is also considered one of the essential components of good infection prevention practices as an early recovery of the patient and health of clinical staff directly depends on the infection prevention practices used in HFs (Ministry of Health and Population (MoHP), 2020).
Several studies have been carried out in the HFs in Nepal and other countries in the past. Many of them are either to estimate unit waste generation, total waste generation and their characteristics in different HFs or others to investigate the current HCWM system, including segregation, collection, transportation, treatment and disposal practice in individual HFs. MoHP of the Government of Nepal (2003) revealed that the HCW generation is 1.7 kg bed−1 day−1 with 22% risk wastes. Paudel and Pradhan (2010) reported that the average HCW generated in the Narayani Sub-Regional Hospital was found to be 0.8 kg bed−1 day−1. The average HCW generation rate in hospitals in Pokhara city was estimated at 1.22 kg bed−1 day−1 (Enayetullah et al., 2011). According to a study conducted by the Support to the Health Sector Program (S2HSP) of Gesellschaft fürInternationaleZusammenarbeit (GIZ) in 2017 in district hospital, private hospitals and other smaller HFs in Nuwakot district of Nepal, the 50-bedded Trishuli Hospital generated the average 1.09 kg bed−1 day−1 with 73% average occupancy, and 15-bedded Nuwakot City Hospital generated 1.14 kg bed−1 day−1 (Support, Health Sector Program (S2HSP) GIZ, 2017). According to a recent study by MEH consultants private limited and management4health (m4h) in two large hospitals of far western Nepal, Dadeldhura Sub-Regional Hospital generated 38 kg of waste per day with 61% occupancy, and this yields a waste generation rate of 0.85 kg bed−1 day−1 (MEH Consultants P. Ltd. and m4h, 2018). This study also reported a waste generation rate of 1.07 kg bed−1 day−1 in Seti Provincial Hospital, which generated 141 kg of waste per day with 60% occupancy (MEH Consultants P. Ltd. and m4h, 2018). Several studies have been carried out in the HFs of Nepal and outside the country to estimate unit HCW generation and characteristics. For example, Komilis et al. (2012) calculated the infectious HCW unit generation rates in Greece. In the same manner, an investigation in HCW management in Iran was conducted by Farzadkia et al. (2015). A few studies identified the prevailing problems with a HCW management system using an integrated management tool. For example, Ferronato et al. (2020) developed an indicator set for assessing HCWM in developing cities, implemented in La Paz (Bolivia) as a case study. In the current context of the COVID-19 pandemic, it was observed that HCW is generated from both healthcare and non-healthcare settings including quarantine centres, holding areas, designated hotels and households associated with suspected and confirmed COVID-19 patients. Experience from some countries like China shows that the hospital’s infectious medical waste increased by 600% while treating the COVID-19 cases (Asian Development Bank (ADB), 2020). In Wuhan of the People’s Republic of China (PRC), the generation of HCW for treating COVID-19 patients ranged from 0.6 to 2.5 kg bed−1 in a day for each patient (Yu et al., 2020). Agamuthu and Barasarathi (2020) reported that the daily amount of all medical wastes at the Hospital Seberang Jaya, Malaysia is about 800–1000 kg day−1 of medical wastes and the COVID-19-related medical waste is about 120 kg day−1. Their findings show that a 27% (by weight) increase in the generation of HCW was primarily attributed to COVID-19-related waste in Malaysia. Similarly, in Tehran, the capital city of Iran, hospital waste generation has increased by 17.6%−61.8% due to the COVID-19 pandemic (Zand and Heir, 2020). On increasing the amount of HCW, the amount of waste that should be disposed of at sanitary landfills is also growing significantly because of the disruption in the waste separation and recycling programs. It is happening globally after the COVID-19 pandemic situation due to the lack of an appropriate HCWM system and the fear of spreading the Coronavirus at solid waste transfer stations and recycling facilities, especially in the cities of developing countries, including municipalities of Nepal. Zand and Heir (2020) reported that landfilling of wastes in Tehran has increased by 35% during the COVID-19 pandemic.
Even in a normal situation, HFs ranging from large hospitals to small clinics do not have the appropriate system to treat the infectious waste and generally practicing open burning and burial in developing countries like Nepal. These practices are hazardous to both human health and the environment. As per the current legal provisions in the Nepal Solid Waste Management Act 2011 (Government of Nepal, 2011), all HFs are legally and financially responsible for treating and managing infectious HCW and other hazardous waste onsite to minimise risks to human and the environment. However, there is a chance that all HFs will not be able to use the technology for treating infectious waste in an economically cost-effective way by itself. Due to the lack of a continuous and systematic monitoring system, it is difficult to monitor each small health facility whether they have strictly followed the legal provisions to treat infectious waste generated onsite. Hence, the establishment and operation of the infectious HCW treatment and management system in each health facility ranging from health posts to large hospitals in the cities of Nepal seems impractical and further seems to create problems rather than provide an economic and environmentally friendly solution. In this context, a common treatment facility (CTF) for treating infectious waste generated from the hundreds of health facilities is only possible at a place with the involvement of health facilities, local government, private sector and other stakeholders. An integrated HCWM system is not only the development and operation of the CTF to treat the infectious waste from all the HCFs but also a comprehensive program that includes waste minimisation, source segregation, separate collection and transportation, recovery of recyclable materials after treatment and finally safe disposal of waste materials that cannot be recovered and recycled. It also provides comprehensive training to health facility managers and staff including doctors, administrators, nurses, healthcare workers, waste handlers and equipment operators to achieve optimal segregation, which allows treating only infectious HCW and ensuring a healthy and safe environment in HFs and communities. Once the infectious waste is treated at CTF, it is further sorted to separate recyclables and the waste materials that have to be disposed of at the landfill sites. Recyclables are also separated according to their types and stored at separate chambers to send either directly into recyclers or municipal integrated solid waste management (ISWM) facilities. The proposed CTF site should be constructed separately from the municipal waste handling facility but on the same premises to further integrate the treated HCW into the municipal ISWM system for its sustainability. Therefore, the development and operation of such a CTF to incorporate the idea of an integrated HCWM approach is beyond the capacity of the municipal government those who do not already have an operational integrated municipal solid waste management facility. Nepalgunj sub-metropolitan city (SMC) is one of the rapidly urbanising cities where an ISWM facility including source segregation practices, material recovery facility, manual-cum-mechanical sorting system, composting facility and sanitary landfill site for MSW management is in operation since 2019. This is taken as the first model ISWM system in Nepal. But for the management of HCW, the ISWM site does not have any option. As untreated infectious waste from health institutions cannot be sent to the ISWM site and not picked up by the municipality, a major challenge is its safe management. In this context, we have proposed the CTF under different infectious waste management scenarios and recommended its implementation modality for all the HFs of Nepalgunj SMC as a case study. As accurate estimates on waste generation and waste characteristics are crucial to implement proper waste management strategies or to optimise the design of the required waste management infrastructure and facilities (Pathak et al., 2020), first, we quantified the total amount of HCW, its composition and estimated the amount of infectious waste to be treated in the health facilities of Nepalgunj SMC. Second, we explored the existing scenarios for the capacity assessment and implementation modality of CTF to treat infectious HCW. This study is one of the first systematic attempts to examine the possibility of CTF for treating infectious HCW in Nepal and can be replicated to other similar cities alone or in regions with many neighbouring cities of developing countries.
Materials and methods
Study area
A study was conducted within the selected health facilities ranging from health posts to large hospitals in Nepalgunj SMC, Nepal to identify the generation and composition of various HCW and their existing management practices and future treatment technology, their capacity and implementation modality for CTF as a pilot study. Because of the growing number of health facilities, including medical colleges and other large hospitals, this city is pronounced as a medical hub city where many patients are also treated from neighbouring cities and patients from neighbouring Indian cities.
Nepalgunj SMC is located in Banke district of Nepal on the Terai plain near the southern border with Bahraich district, Uttar Pradesh state of India. It is 85 km southwest of Ghorahi and 16 km south of Kohalpur and 35 km east of Gulariya (Nepalgunj SMC, 2018). Nepalgunj has a sub-tropical climate. Temperature sometimes exceeds 40°C from April to June. According to the new local level structure recently approved by the Government of Nepal, while implementing federalism in line with the Constitution promulgated in September 2015, the part of the previous Nepalgunj SMC, except ward no 23 is merged with ward no 7 of Harimaniya village development committee (VDC) to form a new local level structure, called Nepalgunj SMC. The new SMC is divided into 23 wards as shown in Figure 1. The total area of SMC is 93.78 km2. According to the census of 2011, the population of Nepalgunj SMC is 138,951 with 27,892 households (Central Bureau of Statistics (CBS), 2011). With a 3% average annual growth rate, the projected population for 2020 is estimated to 186,738.
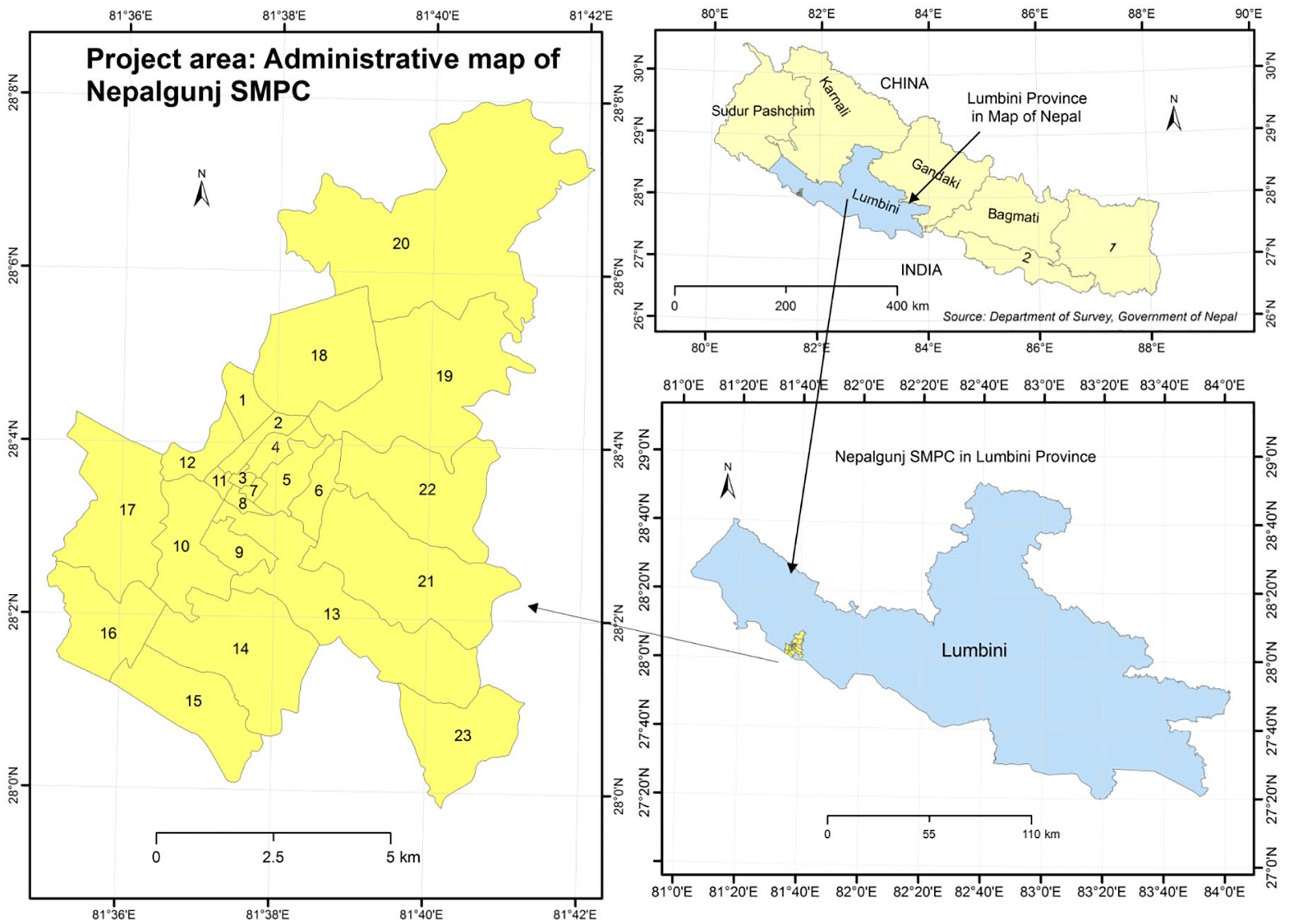
Study area-administrative boundary of Nepalgunj sub-metropolitan city (SMC).
Besides many institutional and commercial establishments, there are over 100 health institutions. Among them, there are eleven health posts, seven urban health centres, four fundamental health service centre, one private teaching hospital with 250 beds, one federal government hospital with 200 beds, five private hospitals ranging from 25 to 100 beds and over eighty pharmacy and clinics in Nepalgunj SMC (Nepalgunj SMC, 2018).
Sampling and survey design
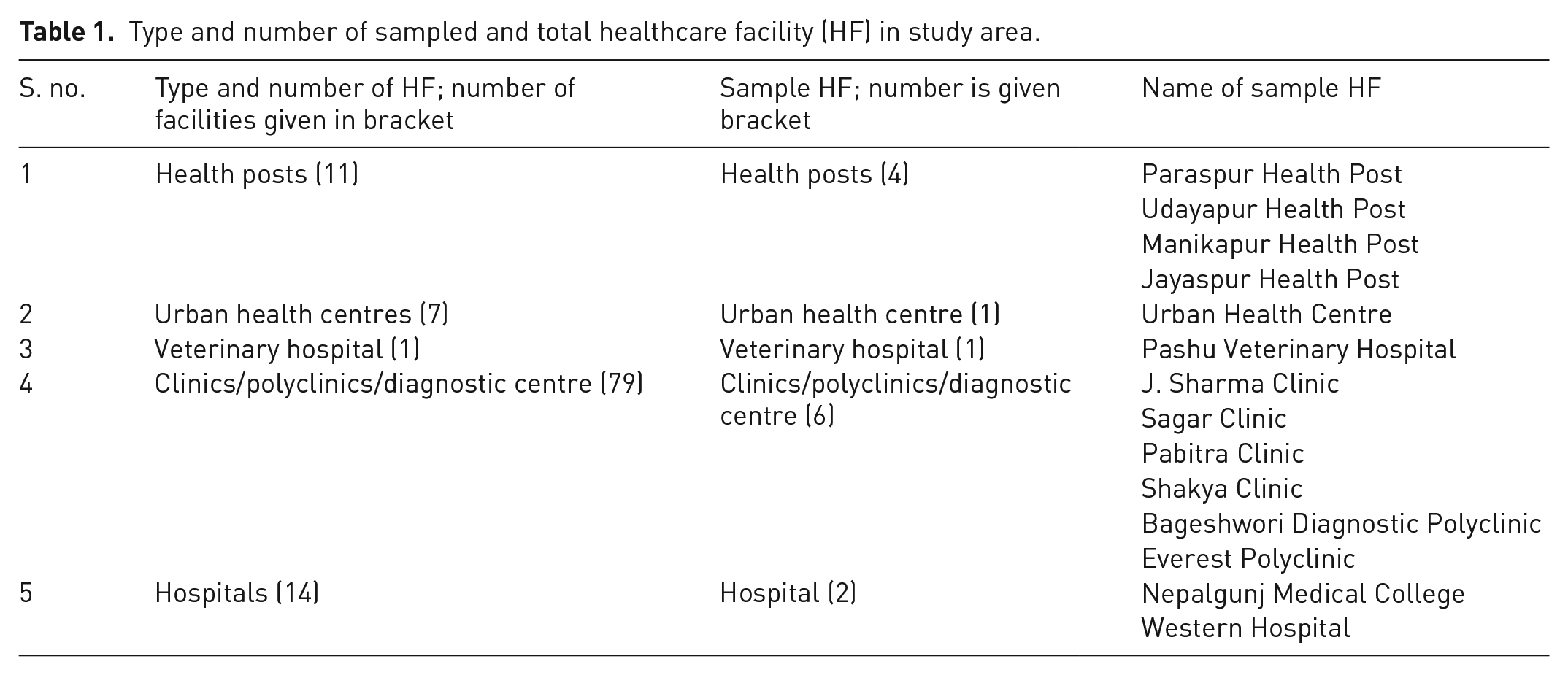
Altogether fourteen health facilities were surveyed, which comprise four health posts, one urban health centre, one veterinary hospital, four pharmacies and clinics, one diagnostic polyclinic, one private teaching hospital with two hundred fifty beds and one private hospital with hundred beds as shown in Table 1. The sampling was purposive and was intended to cover a wider representation of private and public HFs. For the survey, the health posts and hospitals were selected purposively with a basis of outdoor patient department (OPD) cases per day at the hospitals and health posts. Similarly, a diagnostic centre that generates infectious waste and the pharmacies with clinic operation were taken for the study.
Type and number of sampled and total healthcare facility (HF) in study area.
Field survey planning and assessment
A weekly diagnostic assessment of HCW waste was conducted in Nepalgunj SMC by S2HSP, GIZ. We carried out this assessment from the 21st of December 2019 to the 30th of December 2019. The HCW quantification and characterisation study was carried out by physical measurement (waste audit) and waste management practices through standard questionnaires and observation in the surveyed HCFs. Likewise, we combined the HCW data of Bheri Hospital recently conducted by a management division of department of health services of the MoHP (2015).
With the motive for putting safety first, the assessment team was provided with the required personal protective equipment (PPE) for use during the assessment period. Tongs were also given to the survey team members for separation of the waste to avoid direct handling of waste and prevent needlestick injury.
Orientation to surveyors
The field data collection team included one team leader, one field coordinator and four enumerators. For the support on daily waste collection, transportation and separation, the support staff of each sampled HFs were identified. Four support staff from the teaching hospital, two support staff from 100-bedded private hospital and one support staff from each health posts, urban health centre and other clinics were selected to be involved in the assessment process. Before involving the team in the survey, all the enumerators and support staff involved in the assessment process were trained on the data collection procedures, waste assessment methods, segregation practices and waste handling during the period.
Healthcare waste generation, characterisation and existing practices
To get the result of waste generation, characteristics and existing practice, the following process was adopted during the survey:
Standard questionnaire
Standard questionnaires were used as defined by Minimum Service Standard 2076, MoHP, Government of Nepal to collect the information regarding the waste management practice and other aspects of HCW handling, such as capacity building, behaviour change training, personal hygiene, use of PPE, etc., in each HF (MoHP, 2020).
Data analysis
All the data were entered into an Excel sheet and analysed. Before data analysis and to produce necessary charts and graphs, data were cleaned like consistency check, extreme case check, etc. Then, we calculated the average daily unit waste generation in different types of surveyed HCFs based on weekly recorded data. The unit waste generation was expressed in kg per bed per day for hospitals and calculated using the following formula:

where,
Similarly, the average unit waste generation was expressed in kg per HF per day for a small non-bedded HF and calculated using the following formula:

where,
For small HCFs, the average unit waste generation was also expressed in kg patient−1 day−1. It was calculated by dividing daily total HCW produced by total number of patients visited on the same day. Based on this unit waste generation rate (kg bed−1 day−1) and the total number of beds in the hospitals of Nepalgunj SMC, the total amount of wastes generated in hospitals was estimated. Similarly, a total HCW for non-bedded HCFs was calculated by multiplying the unit waste generation rate and the total number of HFs across the study area.
Infectious waste treatment scenarios and capacity assessment of treatment technology
In this study, based on the amount of infectious waste to be treated in different HCFs, the following three scenarios are considered for the capacity assessment of required treatment technology to deal existing worst case scenario and the future improved scenario. The three scenarios are as explained below.
Based on the volume of infectious waste to be treated in each scenario, numbers of required autoclave, their capacity and the number of treatment cycle were estimated.
Estimation of investment and operation cost
Finally, the total investment cost was calculated based on the cost for civil infrastructures (treatment centre), cost of treatment technology and cost of special vehicles to transport infectious wastes from HCFs. The engineering design, detail drawings and cost estimate of the HCW treatment centre for Nepalgunj SMC were carried out in December 2020 by S2HSP GIZ (Pathak and Rana, 2020). The unit rate of each item was calculated as per the latest district rate authorised by Nepalgunj SMC (Banke District Administration Office (DAO), 2020). Operation cost was calculated based on the current market price of required utilities (water, electricity, etc.) and required human resources for operating plant and their wages. The electricity cost for running autoclave per cycle was calculated by multiplying electricity consumption to run autoclave for a cycle with unit price of electricity for three-phase line fixed by Electricity Tariff Fixation Commission (Nepal Electricity Authority (NEA), 2021).
Results and discussion
Existing practices of HCWM
Different diseases are being spread through HCW, such as HIV/AIDS and hepatitis. According to Pepin et al. (2014), unsafe injections were still responsible for 33,800 new HIV infections, 1.7 million hepatitis B infections and 315,000 hepatitis C infections in 2010. HFs including hospitals generate different waste. A proper management of HCW is still an enormous challenge in Nepal, even in normal situations. It is common practice that the general waste is being mixed with highly infectious waste and being disposed of at municipal containers (Karki et al., 2020). Sometimes, untreated wastes are seen on the streets putting human health and the environment at risk. In Nepal, it is a current practice that different categories of waste remain unsegregated due to lack of proper waste segregation activity at sources inside the HFs. Most of this waste is managed by the method of incineration. If not incinerated or by not having a properly functioning incinerator, this HCW ultimately goes to the municipal solid waste disposal site. Many HFs are dumping or throwing waste in the backyard, ditches, rivers, open fields, corners of hospital buildings, nearby ponds, or anywhere around the premises (MoHP, 2020).
The study’s findings show that placing of buckets was not always found to be satisfactory in many surveyed HFs. Only 24% were found to be labelled in sampled health posts. Improper, inconsistent and inadequate labelling might have added to the problem of waste segregation. Although segregation practices can be observed in the health posts, wastes were mixed during transportation. All the facilities were burning the waste. In clinics, only 19% of the bins were labelled, and 33% bins were cleaned. The segregation practices could be rarely seen in these clinics. Regarding the labelling of the bucket in big hospitals, the condition was observed worse than in small facilities. Out of 377 buckets, only 9% were found to be labelled, and only 16% bins were cleaned in hospitals. Most of the labelled buckets were in wards, and labelling standards were found to be inconsistent. It clearly shows that there is an urgent need to improve bucket labelling. Nearly 45% of the waste materials can be sent for recycling if the wastes are properly segregated. Although a few huge HFs collect and send limited quantities for recycling, the quantity can be increased by improving the segregation practices at the source and making it safe by treating. Only cardboard, plastic bottles and metals are being sent to recycling at present.
There were no trolleys for the transportation, but the waste was collected and transported to the disposal sites by the support staff in all the small HFs, including health posts, clinics and urban health centres. None of these facilities assessed had a non-burn waste treatment method being applied for waste treatment. The study also shows that the waste collection bins in hospitals were empty and some were overflowing, which illustrates some gaps in the transportation system and the bucket size used. The same ramp available for the transportation of patients was used for the transportation of the waste in hospitals. A waste collection trolley was used for collection, which was accessible to the public. The open trolley was used for the transportation of the wastes. Any treatment technology for on-site treatment of waste could not be observed in the surveyed hospital. All the generated wastes were stored in containers and transported for open dumping. Open burning is also another common practice in the HCFs of the study area. The infectious and hazardous wastes were stored along with the recyclable materials. There was no daily collection system for the infectious wastes that could increase the potential hazards associated with handling of the wastes, which has been further expedited due to this COVID-19 pandemic.
The person responsible for the collection was not using proper PPE, hence enhancing the risk of infection. During the field assessment and questionnaire survey, it was reported that waste handlers were not vaccinated against hepatitis B. The PPE used in the HFs for waste handling was not found to be entirely appropriate. The survey findings also show that over 75% of support staff were not trained on effective use of PPE and were not using the PPE properly.
As mentioned here, similar findings from HFs of other cities and hospitals in Nepal were reported by several studies in the past. The study conducted at many hospitals of Nepal by the MoHP with the support from the WHO (MoHP, 2012) reported that the waste management system is poor, and only 39% of hospitals have adopted correct segregation of HCW. Not only in Nepal but also in other South Asian countries, such as India, Bangladesh and Pakistan, lack of proper waste treatment facilities, training programs and safety measures are very common (Ali et al., 2015; Ansari et al., 2013; Harhay et al., 2010; Patil and Shekdar, 2001).
Healthcare waste generation in different HFs
The HCW generation from different HFs was estimated based on the weekly assessment by considering the type of services and the average patient flow in the HFs. With the emerging new health facilities and expanded services, the HCW generation is rising, increasing the potential hazards to the environment and human health in the rapidly urbanising cities of developing countries like Nepal. Table 2 shows the daily unit waste generation rate and total waste generation in different HCFs of Nepalgunj SMC. The result shows that the average unit waste generation rate for health posts, clinics, urban health centres and the veterinary hospital was estimated at 1.397 kg day−1, 1.608 kg day−1, 0.178 kg day−1 and 0.321 kg day−1 respectively, whereas 0.99 kg bed−1 day−1 and 1.818 kg bed−1 day−1 in Bheri Hospital and other hospitals, respectively. The unit waste generation in each HF depends on many factors, such as type and level of HFs, number of hospital beds, number of patients treated daily, bed occupancy rate and local cultural and socioeconomic conditions (Al-Khatib et al., 2009; Tabasi and Marthandan, 2013).
Unit total healthcare waste (HCW) generation from different health facilities in Nepalgunj sub-metropolitan city (SMC).

Number of HFs.
Number of beds.
Unit waste generation in kg per day for non-bedded small HFs.
Unit waste generation in kg per bed per day for hospitals.
Based on unit waste generation and the number of HFs and beds, the total HCW generated in the city assuming 100% of occupancy was estimated to be 1242 kg day−1 as shown in Table 2. HCW generation differs not only from country to country but also varies from one HF to another HF within a country, as shown in Table 2. Although the unit HCW generation and composition figures of different HCFs in Nepal reported by several past studies are not consistent, the waste generation rate is found significantly correlated with bed capacity, patient flow rate, etc., in all the reports. The study’s findings are also in line with these previous reports from the different HFs of similar cities in Nepal. Moreover, the HCW generation studies in the different HCFs outside of Nepal also show a similar pattern of unit HCW generation rate. Generally, low- and middle-income countries generate less HCW compared to high-income countries. The HCW generation in high-income Asian countries varies from 2.5 to 4 kg bed−1 day−1, whereas it is from 1.8 to 2.2 kg bed−1 day−1 in low-income countries (Prüss et al., 1999). According to the WHO, developed countries generate on average up to 0.5 kg of hazardous HCW per hospital bed per day; whereas low-income countries generate on average 0.2 kg of hazardous HCW per hospital bed per day (WHO, 2011). In South Asian countries, it was observed that Pakistan and India share the highest waste generation rate, which is 2 kg bed−1 day−1 and a few Indian regions, such as Lucknow and West Bengal, have a much lower HCW generation, which is 0.5 kg bed−1 day−1 and 0.08 kg bed−1 day−1, respectively (Khan et al., 2019a). Similarly, Bangladesh, which is almost similar in size but much higher in population to Nepal, had a similar HCW generation rate, which was 1.58 kg bed−1 day−1, whereas the lowest reported rate was 0.5 kg bed−1 day−1 (Alam et al., 2008; Patwary et al., 2009; Syed et al., 2012). However, Khan et al. (2019b) reported more than 2 kg day−1 in small non-bedded HCFs, like clinics of Hyderabad, Pakistan, which is slightly higher than in small HCFs of Nepalgunj SMC. The unit HCW generation rates from other developing countries outside South Asia also have a similar range. For example, the average hazardous HCW generation rate at Jenin’s district of Palestine was reported in the range of 0.54–1.82 kg bed−1 day−1 with a weighted average of 0.78 kg bed−1 day−1 (Al-Khatib et al., 2020).
Characteristics of HCW
The characteristics of the wastes differ from place to place according to the specialisation of the hospitals. The types of wastes depend upon the type of service provided by the hospitals and HFs. Table 3 shows the average % by weight of different waste fractions after the separation of the HCW. In the health posts, nearly 40% of the wastes generated are pathological waste. It is mainly because of the birthing centre in the health posts. The infectious waste and sharps cover about 20% of the waste, and the remaining are the general waste. But 39% and 27% of the total waste are papers in clinics/polyclinics and a veterinary hospital, respectively. Likewise, the risk waste comprises 24% of the waste generated in clinic/polyclinics in the study area as shown in Table 3. The infectious waste was 18%, whereas syringe, bottle/cans and plastics are 8%, 15% and 10% in the veterinary hospital, respectively. In urban health centres, almost half of the waste is paper, and plastics are more than one-quarter, which can be sent to recycling if appropriately separated at source. Infectious waste in urban health centres is only 3%, as shown in Table 3. There was a significant amount of infectious waste, that is, 31% in hospitals. Likewise, the biodegradable waste comprises 18%, and paper and plastics are 25% in hospitals.
Average waste composition of the waste generated from different type of healthcare facility.

As shown in Figure 2, when all sources of wastes are combined using a weighted average method, the average composition of HCFs for Nepalgunj SMC was: biodegradable waste 17%; bottle/cans 12%; unbroken glass 5%; plastics 11%, paper products 17%; sharp metal 1%; syringe 1%; sharp glass 1%; pathological waste 1%; infectious waste 29% and others 2%.
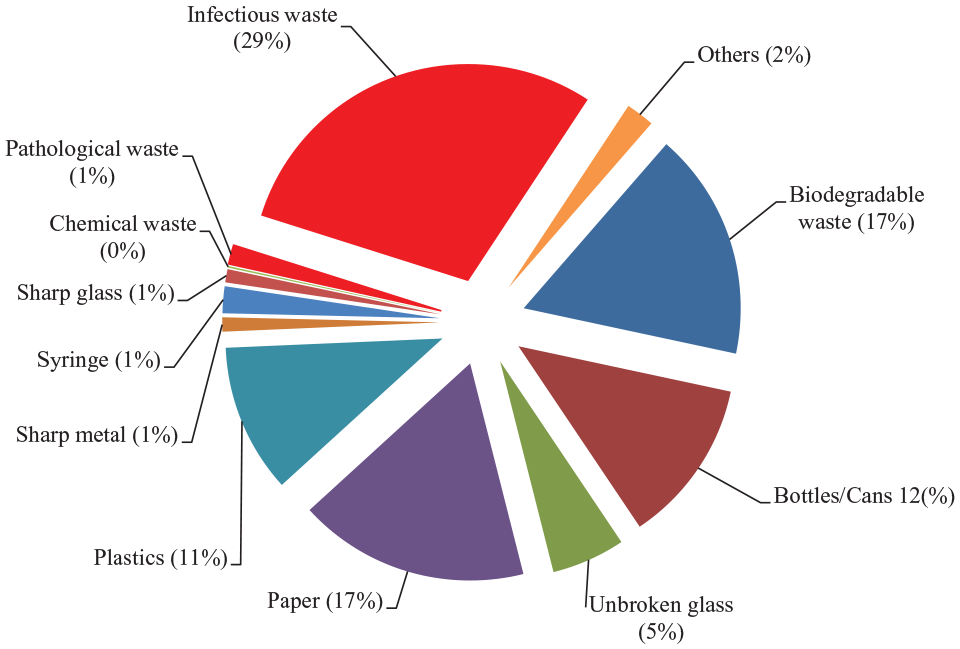
Average healthcare waste (HCW) composition of different healthcare facilities in Nepalgunj sub-metropolitan city (SMC).
Estimation of infectious waste
The fraction of infectious and hazardous waste varies from one HF to another facility. The risk wastes (infectious and hazardous waste) were 79% in the health posts of Nepalgunj SMC, which is too higher than WHO’s report based on several studies from different countries (WHO, 2014). Even after the proper separation of risk waste at sources, 59% were risk wastes in health posts. It is mainly due to the generation of more pathological waste in the health posts with birthing centre. Pathological waste was 39% of the total waste generated in the health posts of Nepalgunj SMC. During the survey, the risk wastes were 75% in the clinics/polyclinics, which can be drastically reduced to 24% after the separation. It demonstrates the lack of proper waste segregation in the facilities assessed. In a veterinary hospital, risk waste generation was 73%, which can be reduced to 26% if risk waste is segregated at sources properly. However, there were a small fraction of risk wastes even in current poor segregation practices in the urban health centres, which was only 22%. It can be reduced to 3% if the urban health centre will implement improved segregation practices. In hospitals, the risk waste generation can be reduced to 36% from 74% of risk waste with the implementation proper segregation program.
Overall, 73% of the total waste generated from the HFs of Nepalgunj SMC is risk waste in the current situation. Figure 3 shows that the risk wastes will be only 32% if HCFs segregate wastes at sources properly. The overall percentage of infectious waste in the HCFs of Nepalgunj SMC is higher than WHO’s report even after the implementation of a proper source separation program. The WHO reports about 10%–25% of HCW is hazardous (WHO, 2014). Nevertheless, the percentage of infectious waste in HCFs of Nepalgunj SMC is almost equal to the infectious waste in different HCFs of other cities of Nepal (Enayetullah et al., 2011; MEH consultants P. Ltd. and m4h, 2018; MoHP, 2003; S2HSP GIZ, 2017). Eslami et al. (2017) also reported similar findings from 165 hospitals of Tehran, the capital city of Iran, where about 38% were infectious before the COVID-19 outbreak that is much higher than the WHO estimated value for hospitals (<15%).
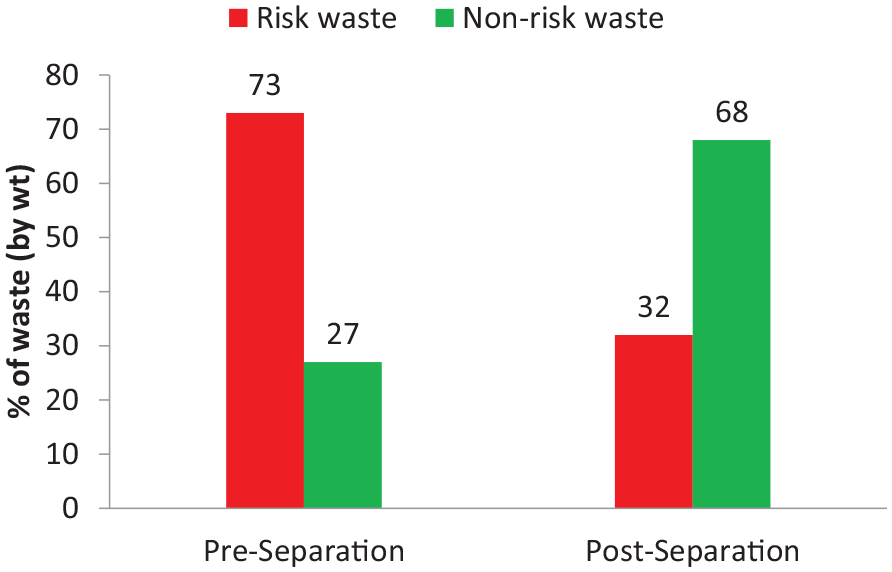
Current status and future perspective of risk waste in the healthcare facility of Nepalgunj sub-metropolitan city (SMC).
Estimation of capacity of treatment technology for CTF under different management scenarios
As mentioned in the previous section, the total HCW from all health facilities of Nepalgunj SMC was 1242 kg day−1. Of total HCW, 73% is the infectious waste in the current situations due to lack of proper waste segregation practices in the surveyed health facilities. The capacity of treatment technology and the number of required cycles per day for CTF has been estimated for different waste management scenarios to address current worst scenarios and the improved HCW management scenario in the future. In the future, the treatment capacity of the technology needs to increase significantly because of an increase in the number of patients and beds in the HCFs if the infectious waste is not properly sorted at sources. If the segregation practice will be significantly improved to reduce the current 73% infectious waste into 32% in the future, the treatment facility designed to address current situations will work for the expanded capacity of HCFs. National legislation (the Solid Waste Management Act of 2011) and the HCWM standard operating procedures (MoHP, 2020) stipulate that waste must be segregated at source. Proper segregation systems are currently started in a few hospitals and can be improved in the future by providing training and implementation support to each health facility. The classification of HCW and its segregation in HFs play a key role in the techno-economic optimisation of the complete management systems (Cesaro and Belgiorno, 2017). Therefore, three scenarios are considered in this analysis for the capacity assessment of required treatment technology to deal with the existing worst scenario and the future improved scenario. The three scenarios are:
Investment and operation cost of CTF
For CTF, a separate HCW treatment, sorting and temporary centre is required at the ISWM site, where above-mentioned treatment technologies should be installed. Based on amount of risk wastes to be treated in Nepalgunj SMC, the total area required for the treatment centre was calculated to 182 m2. The cost of each item of HCW treatment centre was calculated as per detail drawings, and the unit rate of each item was approved by Nepalgunj SMC (DAO, 2020). The engineering design, detail drawings, unit rate analysis, quantity and cost estimate can be available elsewhere (Pathak and Rana, 2020). Accordingly, the total cost of only civil infrastructures of CTF facility was estimated to US$ 55,000 (US$ 1 = NPR 115). The cost of two pre-vacuum advanced autoclaves with 400-L capacity each has become US$ 100,000, whereas the cost of vehicles to transport infectious waste from HCFs to CTF and other required accessories is nearly US$ 90,000 as per the current market price. Based on these calculations, nearly US$ 255,000 is required to invest for CTF including civil infrastructures, treatment technology, that is, autoclaves, special vehicles for transportation of treatment wastes and other required accessories. Besides the central waste treatment equipment, other peripheral equipment will be needed for personal protection, waste segregation and transportation and to ensure the proper functioning of the central equipment, for example by ensuring stable power and potable water.
Also, the annual operating cost for the operation of CTF has been estimated. The yearly operating cost is computed based on the water and energy consumption and their unit market price, collection and transportation cost, human resource cost for operation of the plant and others as per requirement. Pre-vacuum autoclaves with 400-L capacity consume 21 kW for a heater, compressor and water pump. Hence, the average electricity consumption per cycle is about 28 kWh. The cost of a three-phase line to operate such an HCW treatment facility is US$ 0.108 kWh−1 (NEA, 2021). Based on this unit electricity price and consumption rate, the cost of electricity becomes US$ 3 per cycle for the treatment of infectious waste. Similarly, for each cycle, the proposed pre-vacuum autoclaves use about 20–25 L of water to produce steam within the chamber for sterilising, and about 15–20 L to feed vacuum pumps and drain condensers (S2HSP GIZ, 2020). On average, about 40 L of pure water is required for the autoclave for running a complete cycle. Besides treatment, water for other purposes like washing buckets, trolley, autoclave, personal hygiene of workers and working area is around 500 L water is being used to handle one cycle of waste (Waste Service P. Ltd., 2021). The cost of required water for the treatment of infectious wastes is estimated to US$ 0.9 per cycle. The sum of electricity and water consumption cost per cycle is calculated to US$ 3.9. With an average density of 0.15 kg day−1, 60-kg infectious waste can be treated with an autoclave of 400 L capacity in one cycle. As a result, the combined electricity and water consumption cost is calculated to US$ 0.065 kg−1. Other relevant costs, such as human resources (operators and waste sorters), collection and safe transportation, annual operation and maintenance, etc., are estimated as per the current market price to US$ 0.1 kg−1, US$ 0.07 kg−1 and US$ 0.02 kg−1, respectively. Combining these all values, the operating cost for the treatment of 1-kg infectious wastes is found to be US$ 0.255. Since the current amount of daily infectious wastes that need to be treated is 680 kg, the annual operating cost to run CTF in Nepalgunj SMC is calculated to US$ 63,291 if the plant runs throughout the year.
Implementation modality of CTF
A public–private partnership (PPP) model is considered as an option to operate a CTF. The PPP-oriented option in principle appears very attractive; however, some cautions shall be taken into consideration, such as the involvement of logistical capabilities of the municipalities and the involvement of private operators. As an ISWM system is already in an operational stage in Nepalgunj SMC, the integration of HCW into the MSWM system by constructing CTF will be a practical and sustainable solution. Once this approach is successfully implemented in the Nepalgunj SMC, the ultimate target should be the establishment of CTF in other regions of the country and its operation in PPP model. Simultaneously, all local governments would be ready and capable to establish CTF as they are currently strengthening their capacity in technical, institutional, legal and financial aspects to develop an ISWM system following their changing roles and responsibilities. Once the system is developed to run CTF, operation of the system would be made more effective through involvement of competent private sectors. It would be a different modality to operate such a CTF where the options are explained below.
From the experience, the municipal governments in Nepal have faced difficulties in managing municipal waste based on the first implementation modality. So going to the first of the above three options may lead to the failure of the system in place. Therefore, for proper and sustainable management of HCW, the second and third options are best to be preferable. Based on the success of this implementation modality, the same model can be replicated in other cities of the country and equally applicable to similar cities and regions from other developing countries. For the selection of the second and third option, it depends on the technical and financial capacity of the private sectors and the institutional capacity of the municipal government. The agreement period must be longer if the third option is recommended for implementing CTF to treat the infectious HCW. But both partners in the PPP arrangements should be competent in terms of technical, financial and institutional.
Conclusions
HCW is posing a growing problem, particularly in developing countries, like Nepal where the quantity of waste generated is increasing rapidly as number of HFs are growing, and lacks the technological and financial tools to ensure the proper management of HCW. This study is one of the first systematic attempts to examine the possibility of a CTF to treat infectious HCW in Nepal. The survey was conducted in 14 HFs ranging from health posts to large hospitals selected from 120 total HFs in Nepalgunj SMC of Nepal.
The result shows that the average unit waste generation rate for health posts, clinics, urban health centres and hospitals was estimated at 1.397 kg day−1, 1.608 kg day−1, 0.178 kg day−1 and 1.818 kg bed−1 day−1, respectively. Of the total 1242 kg day−1 HCW generated from the health facilities of Nepalgunj SMC, 73% was infected in the current situation, but if fully sorted at sources, only 32% of the waste will be infected and hazardous.
The capacity of treatment technology and the number of required cycles per day for CTF has been estimated for three different waste management scenarios to address current worst scenarios and the improved HCW management scenario in the future. Findings showed that the individual health facility has various limitations on financing, capacity development, monitoring and compliance and technical shortcoming to establish proper HCWM system. CTF may ease these barriers by sharing resources and responsibility within private, public and other sectors with an aim to reduce infectious waste and increase resource recovery for the betterment of public and environmental health. As an integrated municipal solid waste management system is already in an operational stage in Nepalgunj SMC, integrating HCW into the municipal solid waste management system by constructing CTF will be a practical and sustainable solution. Once this approach is successfully implemented in the Nepalgunj SMC, the ultimate target should be establishing CTF in other cities alone or in other regions of the country and its operation in the PPP modality. This approach builds up enough confidence to all stakeholders and explores a feasible solution for HCW in the rapidly urbanising cities of developing countries to help them improve their condition.
Footnotes
Acknowledgements
We thank the editor and anonymous reviewers for their constructive criticism and helpful comments, which have surely helped us to improve the quality of this work. The authors would like to thank all the surveyors, officials and supporting staff from the respective health facility for their time and efforts in carrying out the survey in the HFs of Nepalgunj SMC. The authors would like to acknowledge the Mayor, Deputy Mayor and other officials from Nepalgunj SMC for their support in conceptualisation of this project. We would also like to thank Hrishita Badu, Caldwell University, USA for her careful reading of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Deutsche Gesellschaft für Internationale Zusammenarbeit (GIZ).