
Abstract
Medical waste management in Taiwan is a crucial issue due to its highly environmental and human health risks. The main objectives of this paper were to analyse the status of medical waste generation and treatment in recent years, and also address the discussions on the impacts of coronavirus disease 2019 (COVID-19) on its generation in the first half of 2020. It showed that the reported quantities have slightly increased from 35,747 metric tonnes (Mt) in 2016 to 40,407 Mt in 2019, showing an average increase by 4.17%. This rate of increase was consistent with the hospital services. When classified by the reported codes, the C-type waste (infectious waste) accounted for about 89% of the reported quantities, which indicated an annual increase by 4.14% during the same period. In addition, the medical waste treatment in 2019 was mainly dependent on the commissioned treatment (80.18%), followed by the recycling (18.53%) and the self-treatment (1.29%). Furthermore, the impact of COVID-19 on the medical waste generation in Taiwan was not significant in the first half of 2020 compared to the data during the years of 2016–2019. It was indicated that the consistent trend was observed at the daily confirmed COVID-19 cases in Taiwan during this period. Obviously, the reduction in the hospital medical services during the COVID-19 outbreak should be offset by the increase in medical waste generation from the medical services. In order to try to ensure safe and complete destruction of the COVID-19 virus, all the waste generated from the healthcare facilities should be treated in the incineration plants.
Introduction
Medical waste, also called healthcare or healthcare waste (World Health Organization, 2014), refers to all the waste generated by healthcare activities and related sources, including hospitals, clinics, nursing homes for the elderly, animal research and testing laboratories, blood banks and collection services, and biomedical research centres and laboratories. Regarding the medical waste management, there were significant differences between low-income, middle-income and high-income countries (Caniato et al., 2015). In general, high-income countries may generate on average up to 0.5 kg of hazardous medical waste per hospital bed per day (World Health Organization, 2018). This quantity was different from the local study by Cheng et al. (2010), showing that the overall average value of infectious waste generated from the clinical or healthcare facilities in Taiwan was as high as 1.0 to 2.0 kg/bed/day. In order to handle medical waste properly, it is necessary to predict its generation rate beforehand. In the study by Tesfahun et al. (2016), the authors developed the predictive model for the medical waste generation rate, revealing that this rate has a strong linear correlation with the number of inpatients. Because of its health and environmental risks, medical waste should be separated into hazardous or non-hazardous wastes for the purposes of collection, storage and treatment. According to the report by the World Health Organization (2018), about 85% of the total quantities of waste generated by healthcare activities was general, non-hazardous waste. The remaining 15% was considered to be hazardous due to its infectious, toxic or radioactive characteristics. In particular, hazardous medical waste could contain potentially harmful microorganisms that can infect hospital patients, healthcare workers and the general public. In addition, the percentage of plastic waste (one of combustible materials) in medical waste may be as high as about 20% to 30% (Huang and Lin, 2008; Lee et al., 2002). Based on the sustainability assessment of medical waste treatment systems (Makan and Fadili, 2021), the rotary kiln system was often adopted by high-temperature incineration facilities to control the emissions of toxic air pollutants (e.g., dioxins, heavy metals and acidic air pollutants) in compliance with the official standards (World Health Organization, 2020a), but poor incineration techniques have been used by Asian developing countries for a long time (Khan et al., 2019). For example, a comprehensive inspection survey was performed for 14 hospitals located in Sistan and Baluchestan Province (Islamic republic of Iran) (Bazrafshan and Mostafapoor, 2011), showing that medical waste segregation in the hospitals had not been conducted properly.
Since the first outbreak of coronavirus (COVID-19) early in 2020, more than 40 million confirmed cases of COVID-19 have been reported worldwide as of 21 October 2020 (World Health Organization, 2020b), causing confirmed deaths of over one million people. The multi-dimensional effects of the COVID-19 pandemic have happened at all levels (Cheval et al., 2020). More seriously, this pandemic outbreak could trigger acute respiratory diseases, which will further lead to septic shock and kidney failure. It can be expected that the COVID-19 pandemic has led to a reduction in hospital medical services, and rates of transmission of influenza and other respiratory viruses. Due to the massive use of personal protective equipment (PPE) and related implements during the COVID-19 pandemic, the significant increase of medical waste in large hospital services and healthcare centres will be an unavoidable outcome in modern societies across the world (Fan et al., 2021; Peng et al., 2020; Yang et al., 2021; Zambrano-Monserrate et al., 2020). Although there was no evidence that the coronavirus can be transmitted in any way through medical waste (World Health Organization, 2020b), the safe management of the used PPE such as masks and protective clothes must be implemented rigorously to prevent the spread of COVID-19 (Rhee, 2020).
Obviously, medical waste management is a high priority public health and environmental concern issue. In the past, medical waste, especially generated from small healthcare facilities, was often mixed with municipal solid waste (MSW) and thus disposed of in sanitary landfills or MSW incineration plants in many countries such as Korea (Jang et al., 2006) and Taiwan (Huang and Lin, 2008; Kuo et al., 1999). In Taiwan, the regulatory measures for the issues of medical waste management are based on the Waste Management Act (WMA). In the Act, the waste is grouped into two categories: general waste; and industrial waste. The former is equivalent to the scope of MSW (Rhyner et al., 1995), but it additionally incorporates the waste generated by the employees in the industries into this type of waste in Taiwan. The latter, including medical waste, is divided into general industrial waste and hazardous industrial waste. In 2019, the reported quantity of industrial waste (about 19.8 million metric tonnes (Mt)) in Taiwan was about 2.0 times as great as general waste generation (about 9.8 million Mt) (Environmental Protection Administration, 2020a). Among the industrial waste, the reported quantities of medical waste in 2019 only accounted for about 40,000 Mt, including 35,723 Mt for those hazardous and 4684 Mt for those non-hazardous.
Regarding the overview of medical waste management in Taiwan, almost no relevant reviews have been published in recent years. In the study by Huang and Lin (2008), it was revealed that the majority of medical waste was general industrial waste based on the data between 2003 and 2005, accounting for about 78% of total medical waste and others for infectious industrial waste. In addition, the impacts of the COVID-19 pandemic in Taiwan were relatively minor as compared to other countries. Figure 1 shows the profile of confirmed cases from 1 January 2020 to 31 August 2020 (Our World in Data, 2020). However, the studies on the impacts of COVID-19 on medical waste generation in Taiwan have not been reported in the literature. Therefore, this paper was structured by three important issues. First, the trend changes on the reported quantities of regulated medical waste and its current treatment methods were analysed to compare the hospital medical services in Taiwan. Second, the legal framework and relevant requirements for medical waste treatment were updated. Finally, the discussions on the impacts of the COVID-19 pandemic on medical waste generation in the first half of 2020 were addressed to be in response to the expected increase or not.
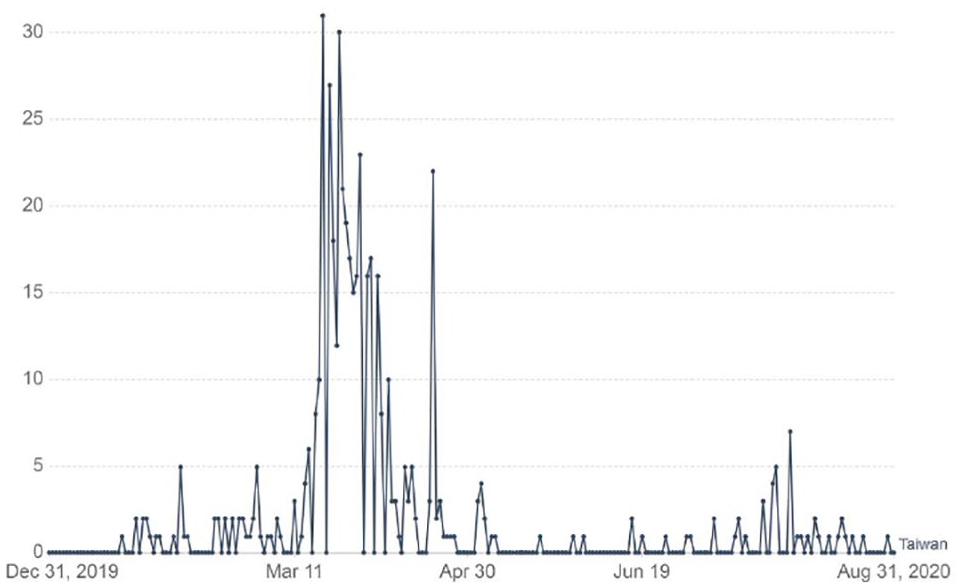
Daily confirmed COVID-19 cases in Taiwan during the period of 31 December 2019 to 31 August 2020 (Our World in Data, 2020).
Methodology
To present an overview of the latest knowledge about the medical waste management in Taiwan, the updated data on the statistics of medical waste generation and the status of its treatment methods were gathered from the official yearbook (Environmental Protection Administration, 2020a) and the database (Environmental Protection Administration, 2020b). These factsheets were surveyed to present an analytical description about their trend changes in recent years (2016–2019). On the other hand, the regulatory requirements for the clearance and treatment of medical waste were reviewed by using the official laws and regulations website (Ministry of Justice, 2020). According to the official databases established by the central competent authorities (Environmental Protection Administration, 2020a, 2020b; Ministry of Health and Welfare, 2020; Ministry of Justice, 2020), the discussions on the impacts of the COVID-19 pandemic on medical waste generation were also addressed in this study to correlate with the epidemic control and prevention measures and the profile of confirmed cases of COVID-19 in Taiwan ( Our World in Data, 2020), and to be in comparison with their reported quantities in the first half of 2019 and 2020 (Environmental Protection Administration, 2020b).
Results and discussion
Current status of medical waste generation and treatment
In Taiwan, the legal framework for medical waste clearance and treatment was authorized by the WMA (Ministry of Justice, 2020). In the WMA, the wastes are classified into two groups: general waste; and industrial waste. Industrial waste refers to waste that is produced from industry activities (but excluding waste generated by the employees themselves), including “hazardous industrial waste” and “general industrial waste.” Hazardous industrial waste is produced by industry that is toxic or dangerous with the concentration or volume sufficient to influence human health or pollute the environment. According to the regulation (“Standards for Defining Hazardous Industrial Waste), medical waste (also called “biomedical and infectious waste”) refers to waste, which is produced in the course of medical treatment, medical testing, post-mortem examinations, quarantine inspections, research, or the manufacture of chemical agents or biological materials by medical treatment organizations, medical testing institutions, medical laboratories, industrial and research organization laboratories of biological safety grade two or above, or laboratories engaged in genetic or bio-technological research. The medical waste generators that are designated and officially announced by the central competent authority (i.e., Environmental Protection Administration (EPA)) shall perform the required measures, including the submitted industrial waste management plan and the reporting to the local competent authorities via the Internet. The contents of the plan included the status of generation, storage, clearance, treatment, reuse, export, transit and transshipment of the waste at issue). Furthermore, medical waste treatment, with the exception of that subject to reuse methods, shall be generally performed in accordance with the following options: self-treatment; joint-treatment; and commissioned treatment. In contrast, the specific legislation dedicated to medical waste management is a recent practice in most of the countries (Ali et al., 2017).
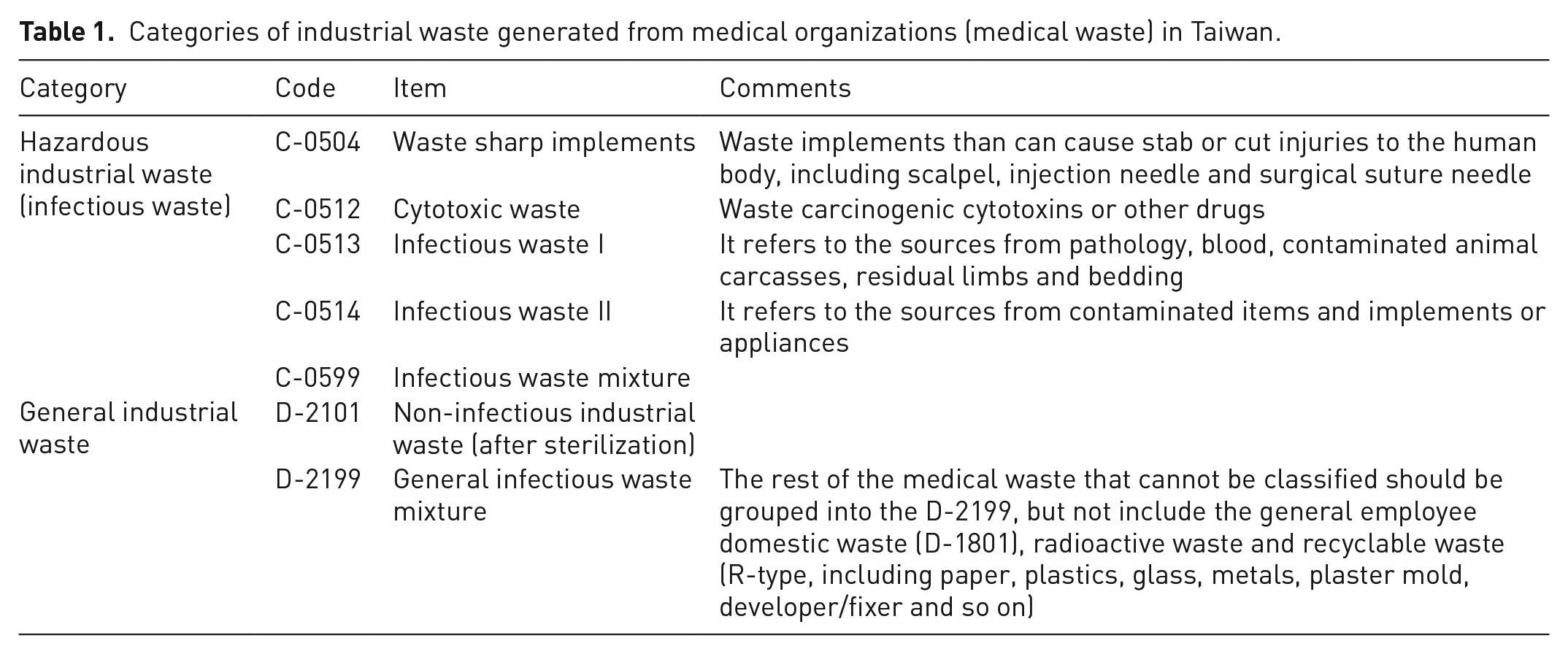
In order to promote pollution prevention, waste reduction and resource recycling in medical institutions, the central competent authority (i.e., Ministry of Health and Welfare (MOHW)) commissioned a non-profit organization to establish the platform (“Medical Waste Treatment Information”). Table 1 lists the categories of medical waste in Taiwan, which must be reported to the competent authority based on the platform information. It can be seen that the medical waste can be grouped into infectious waste (coded as C-types waste, one of hazardous industrial wastes) and general industrial waste (coded as D-type waste). Table 2 shows the variations of the quantities of medical waste generation in Taiwan according the reported codes, using the yearly data for the years 2016 to 2019 (Environmental Protection Administration, 2020a). Some important features were further addressed as follows:
(a) total reported quantities of medical waste have slightly increased from 35,747 Mt in 2016 to 40,407 Mt in 2019, showing an annual average increase by 4.17%. This rate of increase was consistent with the hospital medical services, increasing from in 2016 to in 2019 ( Ministry of Health and Welfare, 2020). When classified by the reported codes, the C-type waste (infectious waste) accounted for about 89% of the total reported quantities of medical waste, which indicated an annual increase by 4.14% during the same period. It should be noted that waste generated by the hospital’s employees themselves is recognized as general waste or recyclable waste (e.g., waste paper and waste plastics), and according to the WMA, there is no need to report it by C-type and D-type codes. Therefore, the fractions of infectious waste as shown in Table 2 are so high as compared to the report by the World Health Organization (2018); and
(b) regarding the quantities of C-type waste in 2019, reported by the rankings, C-0599 occupied 50.51%, C-0514 contributed 36.07%, C-0504 constituted 6.67%, C-0513 accounted for 5.08%, and C-512 shared 1.67%. By contrast, D-2199 provided 87.30% of the reported quantities of D-type waste in 2019.
Categories of industrial waste generated from medical organizations (medical waste) in Taiwan.
Reported quantities of medical waste in Taiwan.*
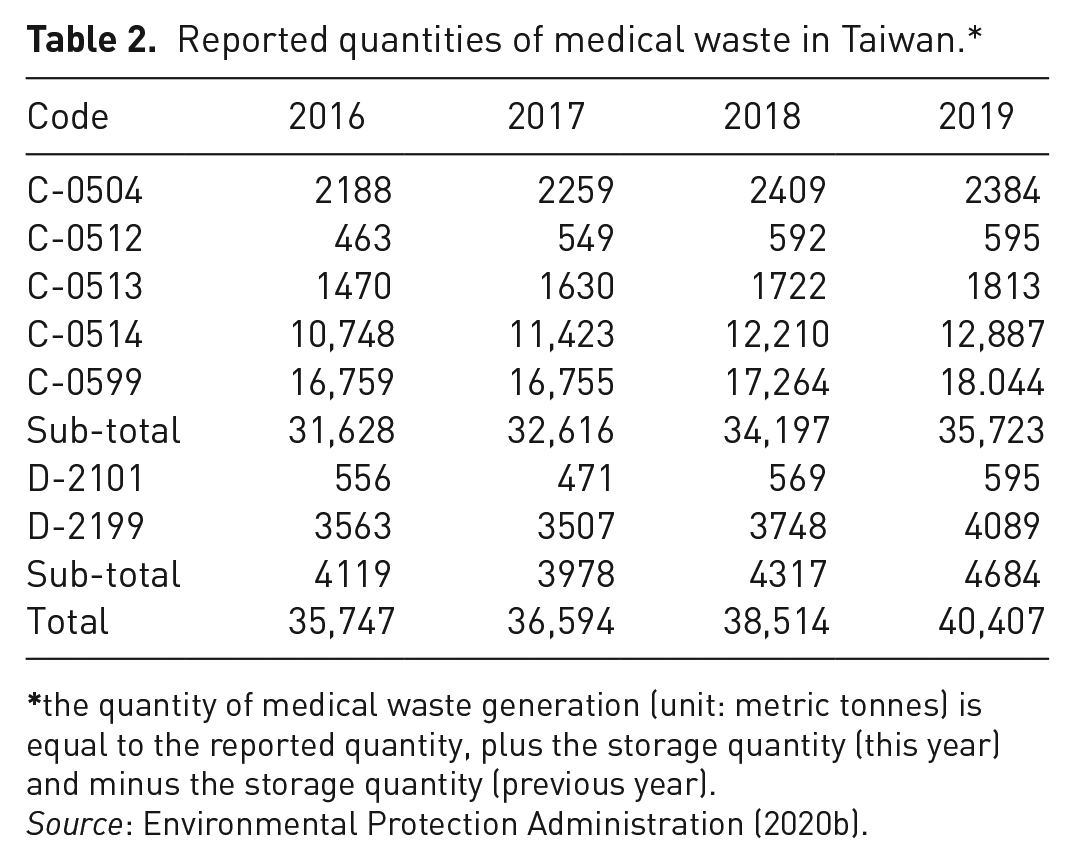
the quantity of medical waste generation (unit: metric tonnes) is equal to the reported quantity, plus the storage quantity (this year) and minus the storage quantity (previous year).
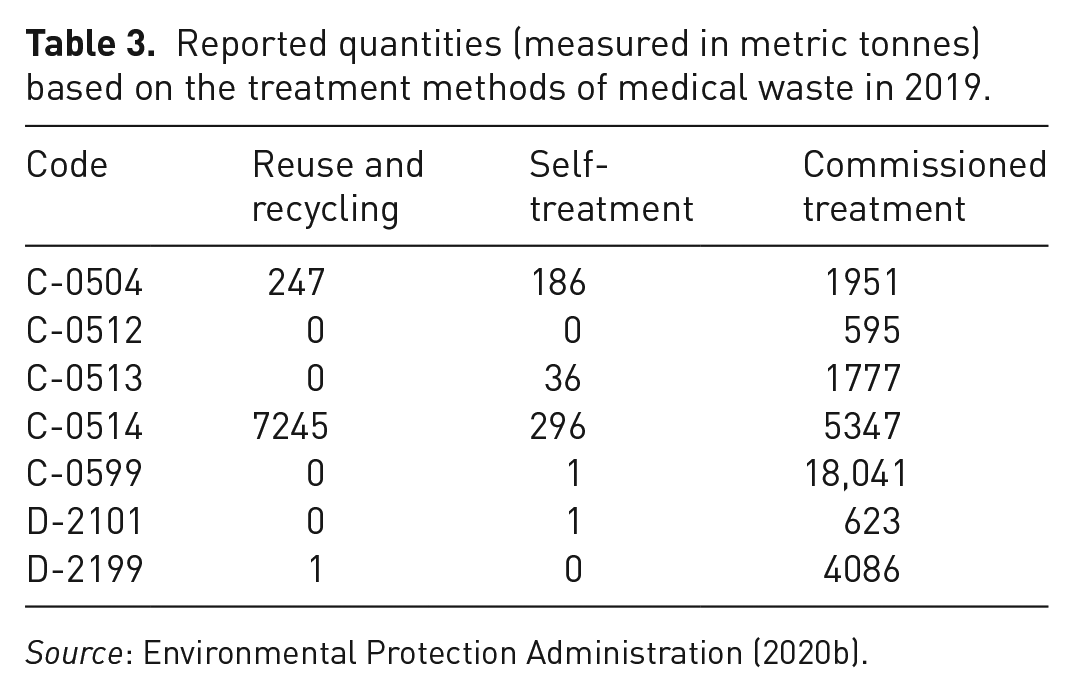
On the other hand, Table 3 lists the reported quantities based on the treatment methods of medical waste in 2020 (Environmental Protection Administration, 2020a). Obviously, the medical waste treatment was mainly dependent on the commissioned treatment (80.18%), followed by the reuse and recycling (18.53%) and the self-treatment (1.29%). Herein, the self-treatment means that the generators treat medical waste by themselves under the approval of the central competent authority (i.e., EPA) in conjunction with the central industry competent authority (i.e., MOHW) based on the WMA. When classified by the reported waste codes, it should be noted that the treatment methods of C-0514 waste (the sources from contaminated items and implements or appliances) were provided by the reuse and recycling (56.21%), the commissioned treatment (41.49%), and the self-treatment (2.30%) during the years 2016 to 2019.
Reported quantities (measured in metric tonnes) based on the treatment methods of medical waste in 2019.
Regulatory measures on medical waste management in Taiwan
According to the WMA in Taiwan, the medical waste management enterprises shall be recorded in detail and kept for at least three years in accordance with the regulations governing the operation and monitoring for methods and facilities for its storage, clearance and treatment. In addition, the medical waste treatment facilities with high-temperature incinerators must control the emissions of toxic air pollutants (e.g., dioxins, heavy metals and acidic air pollutants) in compliance with the Air Pollution Control Act in Taiwan. For example, the medical waste incineration plants in Taiwan must comply with the dioxins’ emission limit of 0.1 ng/m3 based on toxicity equivalency quantity, which may be the most stringent limit value on dioxins emission around the world (Dopico and Gómez, 2015).
Regarding the methods for the storage of medical waste, the management enterprises shall comply with the following regulations (Ministry of Justice, 2020):
(a) “Waste sharp implements” shall be stored separately from other medical waste, sealed in not readily perforated sturdy containers for storage within one year.
(b) “Infectious waste” shall be stored separately from other medical waste. Those that use thermal treatment methods shall seal the infectious waste in leak-proof, non-destructible red plastic bags, or red combustible containers. Those that use sterilization treatment shall seal and store the waste in leak-proof, non-destructible yellow plastic bags, or yellow containers. Herein, “sterilization” refers to treatment methods involving the use of physical (such as microwave treatment) or chemical principles to sterilize microbes in industrial waste within a certain time period. The indicator microbe reduction rate shall attain at least 99.999%. Those using high temperature high pressure steam sterilization shall test for Geobacillus stearothermophilus spores. Those using other sterilization methods shall test for Bacillus subtilis spores. The storage conditions of infectious waste shall comply with the following requirements:
– waste producing organizations may store infectious waste more than 5°C for a maximum of one day. These medical organizations may refrigerate it in the range of 0 to 5°C for a maximum of seven days, and freeze it below 0°C for a maximum of 30 days; – clearance organizations may not store infectious waste, but those that require transfer shipments due to particular circumstances may refrigerate or freeze it below 5°C for a maximum of seven days upon approval by the local competent authorities; and – treatment organizations may not store infectious waste at more than 5°C. These treatment organizations may refrigerate it in the range of 0–5°C for a maximum of seven days, and freeze it below 0°C for a maximum of 30 days.
Regarding the methods for the clearance of medical waste, the management enterprises shall be in accordance with the following principles:
(a) Medical waste that has been stored in differently coloured containers may not be cleared in a mixed state.
(b) Medical waste may not be compressed or arbitrarily opened during the transportation period.
(c) Refrigeration measures shall be provided during the transportation period, and normal operation shall be also maintained.
(d) The doors of the clearance vehicles shall remain shut and locked if there are no personnel present during the loading and unloading processes.
Regarding the methods for the thermal treatment of medical waste, the management enterprises shall meet the following standards:
(a) The central temperature of the combustion chamber at the outlet position shall be maintained above 1000 °C. Combustion gas residence time shall be over one second.
(b) Combustion efficiency shall be over 99.9%.
(c) Destruction and removal efficiency (DRE) shall be over 99.99% for chlorinated organic compounds, over 99.999% for polychlorinated biphenyls and dioxins (polychlorinated dibenzo-p-dioxins/polychlorinated dibenzofurans), and over 99.9% for other principal organic hazardous constituents.
(d) Treatment facilities shall possess devices for automatic monitoring and control of combustion conditions, the recording of the output central temperature of the combustion chamber, and emergency response.
Analysis of medical waste generation during the COVID-19 pandemic
As described previously, the impact of the COVID-19 pandemic on waste management due to the epidemic control and prevention measures such as lockdown and social distancing has been reviewed by several researchers (Eroglu, 2020; Fan et al., 2021; Kulkarni and Aantharama, 2020; Sarkodie and Owusu, 2020; Silva et al., 2021; Zambrano-Monserrate et al., 2020). More seriously, this pandemic could cause acute respiratory diseases, thus triggering the rapid demand for PPE. As a consequence, the medical waste containing plastic materials will be generated by the excessive use and consumption of PPE (e.g., masks and gloves) and other plastic-containing articles (e.g., disinfectants and spray bottles) during the pandemic (Silva et al. 2021). For instance, the most commonly used materials in the face masks include non-woven fibrous plastics such as polypropylene (O’Dowd et al., 2020). However, it should be noted that polyvinyl chloride (PVC) is still the most used plastic material for disposable medical devices due to its unique properties (Jang et al., 2006). Therefore, adopting effective decontamination for reprocessing of PPEs will reduce plastic waste generation and also help to prevent the formation of dioxins from these disposable medical devices containing incinerated PVC (Parashar and Hait, 2021).
It is generally recognized that the increase in the number of confirmed COVID-19 cases could be positively correlated with the medical waste generation due to the increased usage of disposable PPE. For example, a 27% increase in medical waste was reported following the COVID-19 outbreak in Malaysia (Agamuthu and Barasarathi, 2020). Although the medical waste generation in 2020 was yet to be availably obtained by accessing on the official database in Taiwan (Environmental Protection Administration, 2020a), it might be roughly observed by the monthly variations of the reported quantities of medical waste in Taiwan. Table 4 provides the data on the reported quantities of medical waste generated during the Q1/Q2 2019 and the Q1/Q2 2020 (Environmental Protection Administration, 2020b). Figures 2 and 3 depict the monthly trends of hazardous medical waste (C-type) and general medical waste (D-type) generation in Taiwan since January 2019, respectively. As compared to the data in the Q1 2019, it showed an increase by 4.6% in the Q1 2020 due to the COVID-19 outbreak. It seemed to be in parallel with the trend by the daily confirmed COVID-19 cases in Taiwan (Figure 1), when the most serious situation occurred in March 2020. Subsequently, the daily confirmed COVID-19 cases in Taiwan showed a declining trend since April 2020. In addition, the statistics of hospital medical services in the first half of 2020 versus the first half of 2019 have decreased by about 10% (Ministry of Health and Welfare, 2020), which should be attributed to the serious anti-epidemic measures in the medical institutions and the successful personal health care. When comparing the reported quantities of C-type medical waste in Taiwan during the first half of 2019 with the first half of 2020, it only showed a slight increase by 1.95% (17,335 Mt vs. 17,674 Mt, which were obtained from the accumulated data shown in Table 4 and Figure 2). Similarly, the reported quantities of D-type medical waste in Taiwan at the same period also indicated a consistent increment by 0.22% (2233 Mt vs. 2238 Mt, which were obtained from the accumulated data shown in Figure 3). In summary, the impact of COVID-19 on the medical waste generation in Taiwan was not significant in the first half of 2020 as compared to the annual increase by about 4.1% during the years of 2016 to 2019. Obviously, the reduction in the hospital medical services should be offset by the increase of medical waste in services such as medical services. Due to the effective control of the COVID-19 outbreak in Taiwan, the findings of the current work were different from other studies (Agamuthu and Barasarathi, 2020; Rhee, 2020).
Total medical waste generation in Taiwan (Q1/Q2 2020 vs. Q1/Q2 2019).
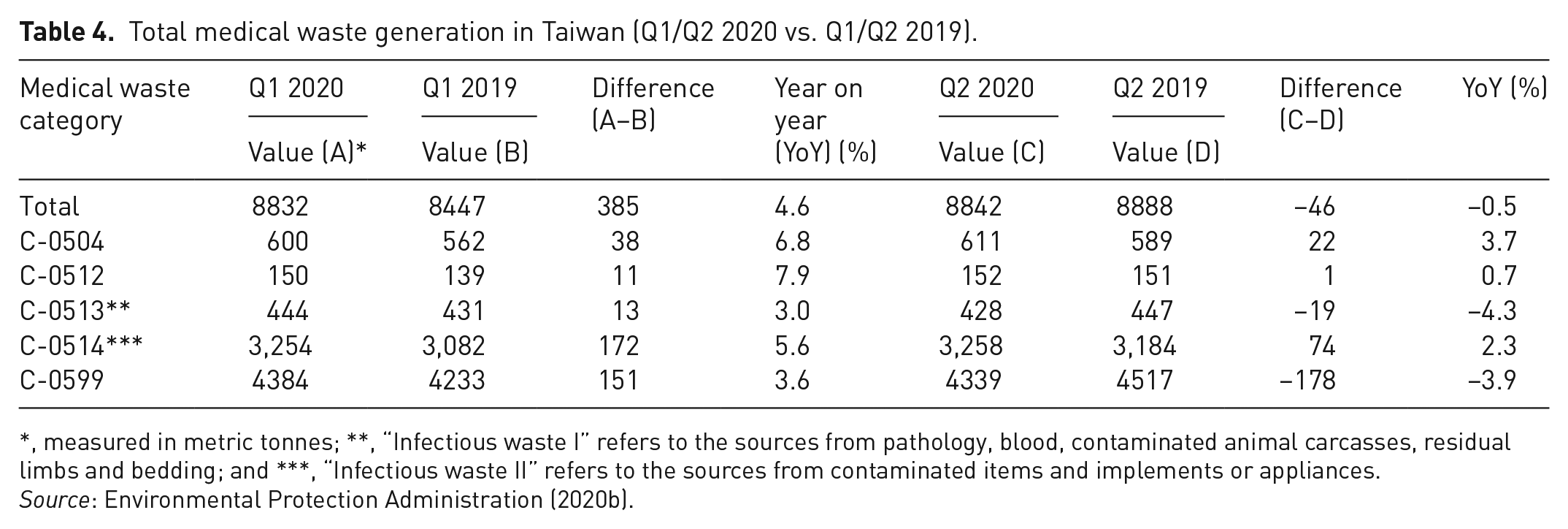
*, measured in metric tonnes; **, “Infectious waste I” refers to the sources from pathology, blood, contaminated animal carcasses, residual limbs and bedding; and ***, “Infectious waste II” refers to the sources from contaminated items and implements or appliances.
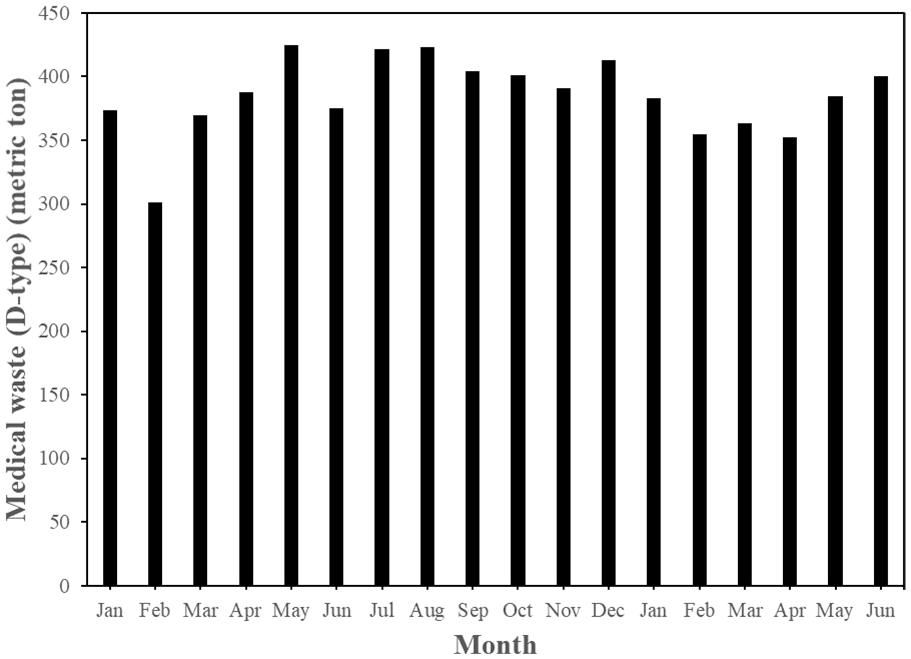
Monthly trends of general medical waste (D-type) generation in Taiwan since January 2019 (Environmental Protection Administration, 2020b).
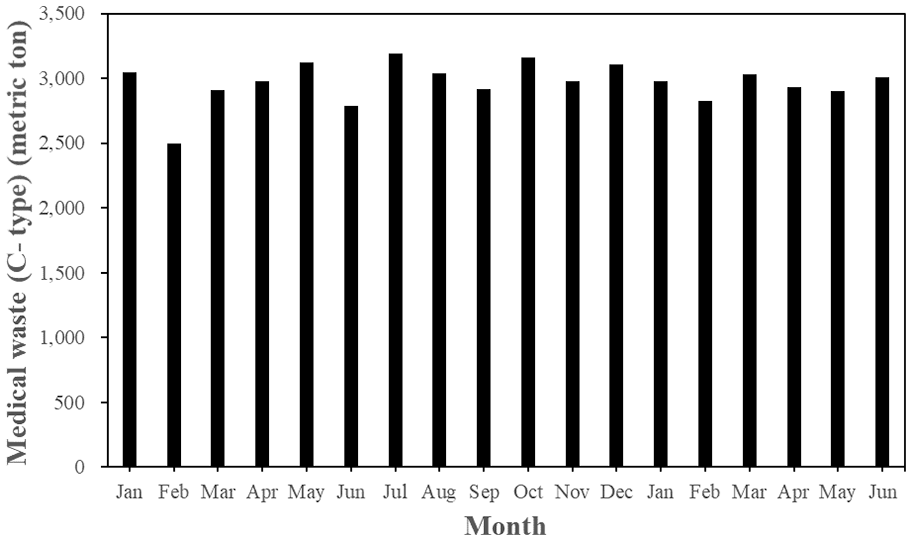
Monthly trends of hazardous medical waste (C-type) generation in Taiwan since January 2019 (Environmental Protection Administration, 2020b).
Conclusions
Due to the wide adoption of single-use disposable items or articles in the healthcare facilities, it has been revealed that the generation of medical waste in Taiwan indicated an increasing trend in recent years (2016–2019). This increased rate was close to the hospital medical services. Regarding the current waste treatment methods by the healthcare facilities, it mainly relied on the commissioned treatment and the recycling. The majority of medical waste was treated by the certified high-temperature incineration facilities to be in compliance with the official regulations. On the other hand, the impact of the COVID-19 pandemic on the medical waste generation in Taiwan was not significant in the first half of 2020 as compared to the annual increase by about 4.1% during the years of 2016 to 2019. Obviously, the reduction in the hospital medical services should be offset by the increase of medical waste in services such as medical services.
In order to try to ensure safe and complete destruction of the COVID-19 virus to help to prevent it from spreading during the COVID-19 pandemic, some suggestions were addressed as follows:
(a) All the waste generated from the healthcare facilities during the COVID-19 pandemic should be treated in the officially certified incineration plants.
(b) The operation temperature at the municipal waste incineration plants shall be properly increased to kill viruses effectively because urban waste may be mixed with medical waste.
(c) In order to reduce the excessive use of single-use plastics, preferably non-plastic personal PPE (e.g., face masks) should be developed.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.