
Abstract
With the spread of the new Coronavirus, there was an increase in the generation of contaminated waste. Thus, healthcare waste management (HCWM) became even a greater challenge in hospitals due to Coronavirus easily spread. In this context, it was necessary to create tools that could aid healthcare facilities in evaluating their HCWM. Therefore, the objective of this article was to elaborate a support tool that helps in identifying the shortcomings of hospitals’ HCWM. For this purpose, the Health Service Waste Management Index was developed based on the selection of indicators in the area. The index was applied to six hospitals in the state of Minas Gerais, Brazil. Its application meet the purpose of this research, since the results in the form of an index objectively summarize the reality of the HCWM in healthcare facilities. From the six hospitals investigated, four were classified as highly efficient. However, even though most of them were well evaluated, they still have difficulties with properly training their employees, which can be even a worse problem during a pandemic, when every precaution is extremely important to reduce the spread of the disease. Therefore, beyond this article contribution related to sustainability by demanding the hospitals to check which points of HCWM should be improved, it also adds academically by developing a tool with indicators that evaluate operational, human, economic and environmental factors in an innovative way.
Keywords
Introduction
Since the beginning of 2020, with the spread of the new Coronavirus, many concerns have been raised over its high contamination rate, symptoms and still uncertain treatment. However, another issue often overlooked is the greater amount of residues generated with the treatment and prevention of COVID-19, which, because of its high propagation rate, can easily contaminate objects and residues; thus, remaining a problem for human health if not managed properly.
One of the measures to fight COVID-19 is the use of face masks by the entire population. In the case of health professionals, along with other personal protective equipment, it is essential to ensure patients’ and employees’ safety (Das et al., 2020). Therefore, hospital waste has increased significantly, contributing to environmental pollution, as most of the masks used are made of non-renewable petroleum-based materials (Thomasnet, 2020).
The increase of waste in hospitals due to the Coronavirus Pandemic can be illustrated in three of the hospitals evaluated in this article. In a hospital located in the south of Minas Gerais, Brazil there was an 81% increase in waste generation. In the second scenario, in Jequitinhonha Valley, the waste generation rose by 100%. However, the most impressive change occurred in a hospital from a metropolitan region of Belo Horizonte where it was estimated with an increase of 425%.
These residues can be classified as healthcare waste (HCW), which also include sharps, contaminated blood, blood, body and tissue parts, chemicals, pharmaceuticals and radioactive materials (World Health Organization (WHO), 2014). They are discarded stem from different healthcare establishments, however, according to André et al. (2016), hospitals are responsible for the greatest volume of HCW.
More than ever, reverse logistics (RL) has become an important alternative for the proper management of HCW since one of its responsibilities is the management and disposal of hazardous or non-hazardous waste from packaging and products (Kroon and Vrijens, 1994). It can also be used as an economic and social tool (Alves et al., 2021), being, therefore, an essential part to make solid waste management viable (Gonçalves et al., 2018, 2019). Govindan et al. (2016) also state that an effective RLs programme has a huge potential to help environmental and social issues, as RL and sustainability are interconnected.
Nevertheless, despite RL being very important for healthcare waste management (HCWM), other tools need to be created in order to help managers to evaluate and monitor the entire waste management process. Fagundes et al. (2017) explained that there is a significant interest in the development of techniques and tools for the management of solid waste, since many products and waste have their final disposal, at the end of their life cycles, in the environment.
Therefore, this article aimed to elaborate a support tool that helps hospitals to evaluate the HCWM. To this end, the creation of the Health Service Waste Management Index (IGeReS) is proposed, directed to hospitals of all sizes and types (e.g. public, private or public-private). For this, the research included the stages of construction, application and analysis of IGeReS from the analytic hierarchy process (AHP) as a methodological support tool. The index was applied in six hospitals in three regions of Minas Gerais, Brazil, strategically chosen because of their different socioeconomic characteristics. Thus, it is expected that, by using IGeReS, hospitals will have a facilitating and helpful tool through which managers can identify the main points of HCWM that should be improved at first.
Methodology
The elaboration and application of the IGeReS depended, firstly, on three stages. Stage 1 concerns the selection of HCWM indicators that will be the basis for stages 2 and 3: the formulation of the index and its application in hospitals.
Stage 1: Selection of indicators
To select the HCWM indicators, a bibliographic search was carried out in which six indicators were identified in the literature. Ventura et al. (2010) proposed the three sub-indicators under employee training, whilst the permanent committee to support HCW management (Copagress, 2011) was responsible for frequency of workplace accidents, investments in HCWM and costs of workplace accidents. However, some of these indicators had to be adapted to better fit the areas of interest of this study (e.g. operational, human, environmental and economic) and to facilitate their evaluation.
Additionally, it was necessary to develop other indicators so that the HCWM assessment could be performed more comprehensively. For this, the most current legislation was used, in particular the Agência Nacional de Vigilância Sanitária Resolution (Brazilian National Health Surveillance Agency) published in 2018. It was the basis for the development of indicators, such as generation, segregation, packaging, internal collection, storage, external collection, treatment, occupational safety and RLs. The Conselho Nacional do Meio Ambiente Resolution (National Council of the Environment) (2005) and the National Policy for Solid Waste (Brasil, 2010) supported two indicators, final disposal and no generation/reduction of HCW, respectively.
All the indicators were organized hierarchically in the following groups: operational, human resources and environmental economic management.
Stage 2: Formulation of the IGeReS
After the HCWM indicators were defined and organized hierarchically, the criteria were analysed and their relative weights calculated. The multi-criteria analysis method called AHP was used. In order, to make a decision in an organized manner and prioritize the criteria, it is necessary to carry out the following steps, namely define the problem, structure the decision hierarchy based on an objective, build a set of pair-wise comparison matrices and use the priorities obtained in the comparisons to weigh them at the level immediately below (Saaty, 2008).
The definition of the problem and the hierarchical structuring were executed in Stage 1. In this step, nine matrices were constructed to include the selected groups, indicators and sub-indicators.
These matrices were evaluated by nine specialists in waste management that had academic and professional experience in both public and private sectors. The experts evaluated the matrices according to paired comparisons based on a scale proposed by Saaty (1980). After the assessments, the aggregation method given by the geometric mean was performed, generating a normalized matrix, which indicates the relative weights of each group: indicators and sub-indicators.
The calculation of the IGeReS is given by equation (1). However, it depends on the evaluation of the indicators from a hospital. The hospitals chosen for this study and their scores for each indicator at the time of the assessment are informed in Stage 3.

where fi is the group weight of criterion i obtained from specialists, ci is the weight obtained from specialists si is the sub-indicator weight obtained from specialists wi is the normalized score (0 < w < 1).
The analyses of the IGeReS were performed using the results obtained which could vary from 0 to 1, that is from minimum and maximum limits, respectively. Values close to 0 indicate that the hospital has poor HCWM performance, whilst values close to 1 indicate that the HCW is managed efficiently. To facilitate understanding, Table 1 presents the classification scale adopted in this work based on the one by Capelini et al. (2009).
Classification of healthcare waste management.
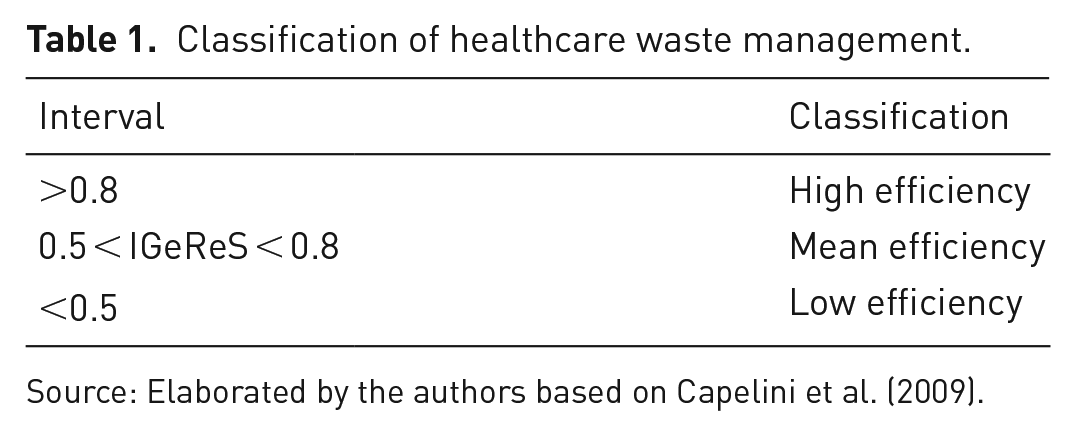
Source: Elaborated by the authors based on Capelini et al. (2009).
Stage 3: Application of IGeReS
Six hospitals were chosen from three different regions of the state of Minas Gerais (Brazil): two from the south region, two from the metropolitan area of Belo Horizonte and two from the Jequitinhonha Valley. Most of them were of public–private legal nature, but one exclusively public and one exclusively private were also investigated.
These three regions were selected because they have different socio-economic indices. Data released from 2010 by the United Nations Development Program reported that two of the hospitals evaluated in this research are located in a municipality that has a Human Development Index (HDI) of 0.810, which is considered very high, according to the evaluated criteria. On the other hand, another hospital is located in a municipality that has an average HDI of 0.633 (PNUD Brasil, 2010).
Moreover, in order to provide confidentiality and comfort so that hospitals could share their reality concerning HCWM, this study decided to identify neither their names nor municipalities. Thus, the investigated hospitals will be referred to as Hospitals A, B, C, D, E and F, respectively.
Data collection was carried out from May to July 2019 during technical visits to hospitals for interviewing those responsible for the waste management sector. All interviews were based on a previously prepared questionnaire in which the indicators were evaluated according to the scale proposed by Milanez (2002). However, if indicators were favourable in the investigated hospital, they would receive a score of 1; if unfavourable, a score of 0.5; and if very unfavourable, a score of 0, are depicted in Table 2 (Enomoto and Lima, 2007).
Scores of the indicators.
Source: Elaborated by the authors based on Milanez (2002) and Enomoto and Lima (2007).
Results
Altogether, 13 indicators and 12 sub-indicators were divided into three groups: operational, human resources and environmental/economic management. Figure 1 shows their hierarchical structure and Table 3 shows the degree of importance of the groups, indicators and sub-indicators considered in this research.
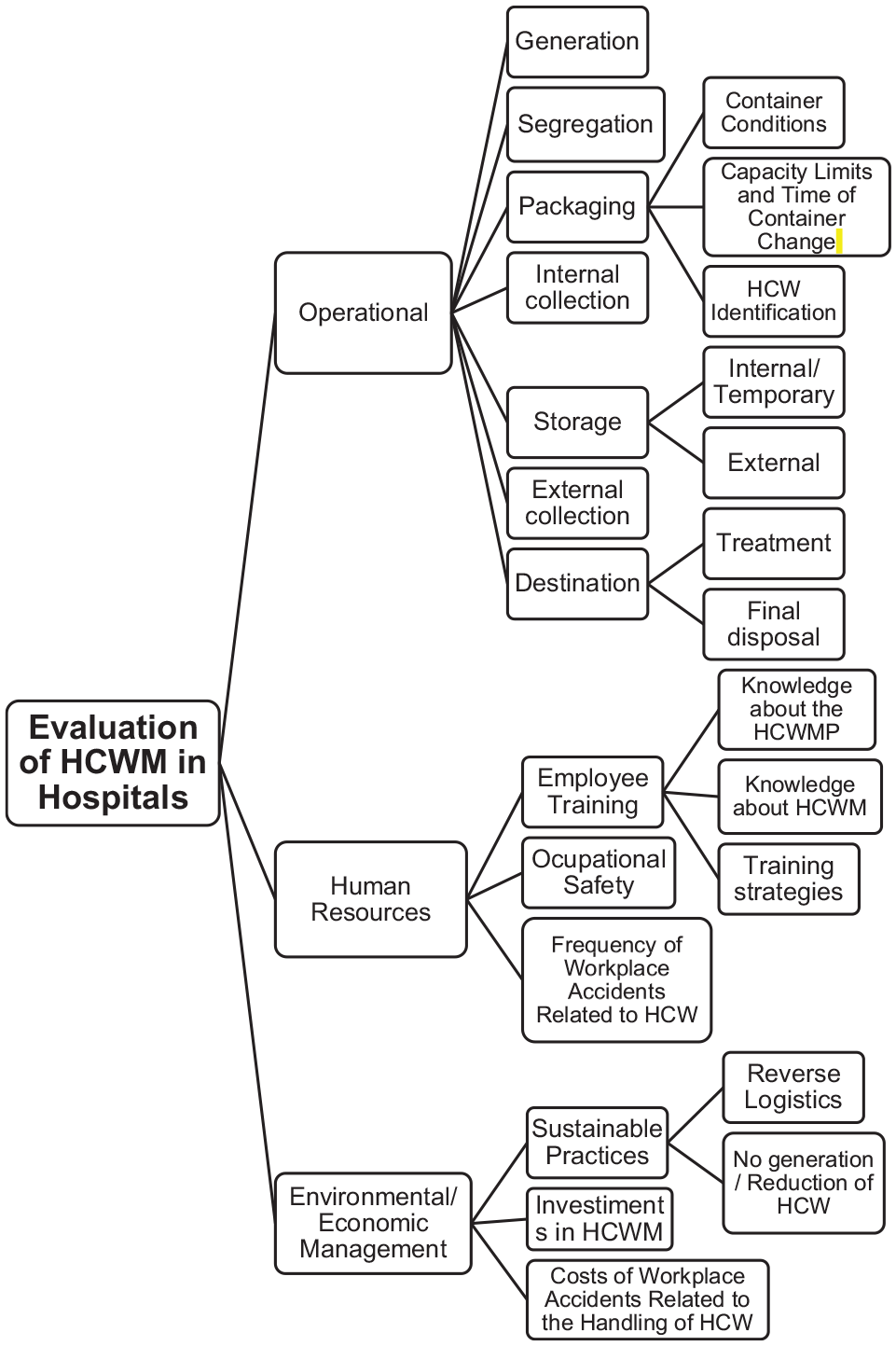
Hierarchical structure of HCWM indicators.
Degree of importance, indicators and sub-indicators of HCWM.
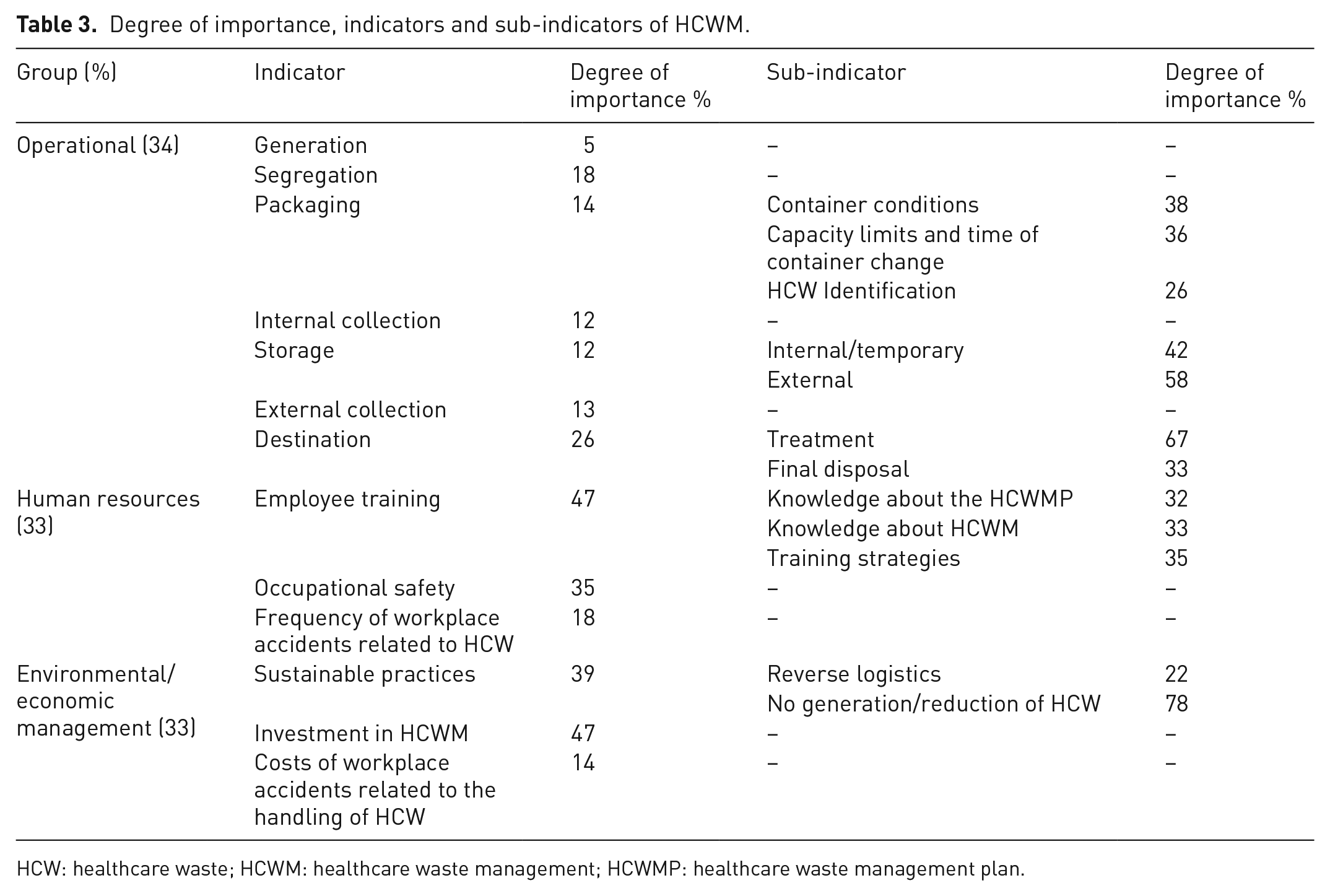
HCW: healthcare waste; HCWM: healthcare waste management; HCWMP: healthcare waste management plan.
After evaluating these indicators in the six hospitals, the IGeReS for each of them was calculated using equation (1). The plot with the results of the indexes of hospitals A, B, C, D, E and F is shown in Figure 2.
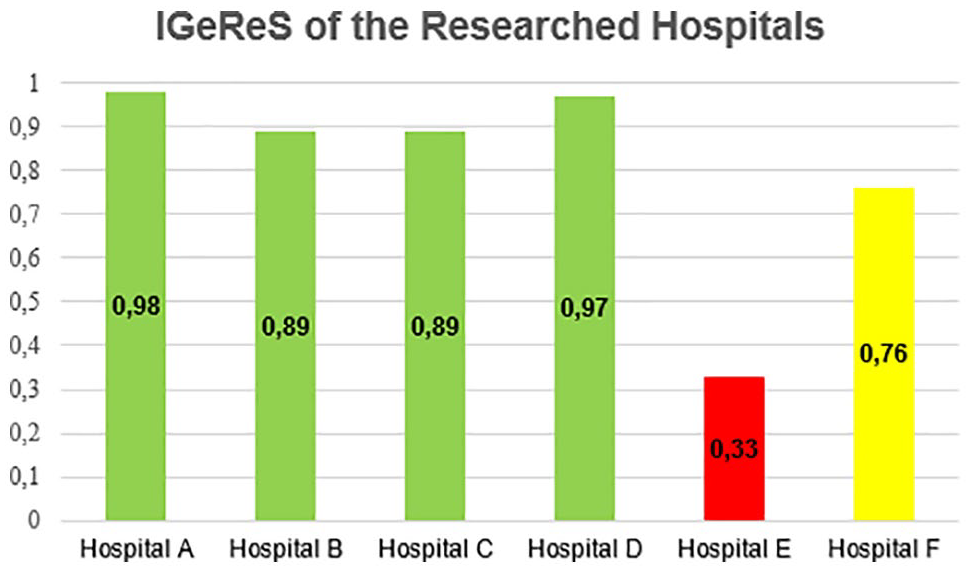
IGeRes of the researched hospitals.
The indices considered highly efficient are those greater than 0.8. Thus, Hospitals A, B, C and D proved to be very efficient when it comes to managing HCW, since they obtained IGeReS above the stipulated value. Two hospitals, however, were not considered highly efficient: Hospital F with a mean efficiency IGeReS; and hospital E with an IGeReS of 0.33, which is much lower than desirable. Coincidentally, these two hospitals are located in the most economically disadvantaged region of the state (Jequitinhonha Valley).
Furthermore, the results for the IGeReS of the analysed groups indicate that environmental/economic management scored the worst, as seen in Figure 3.
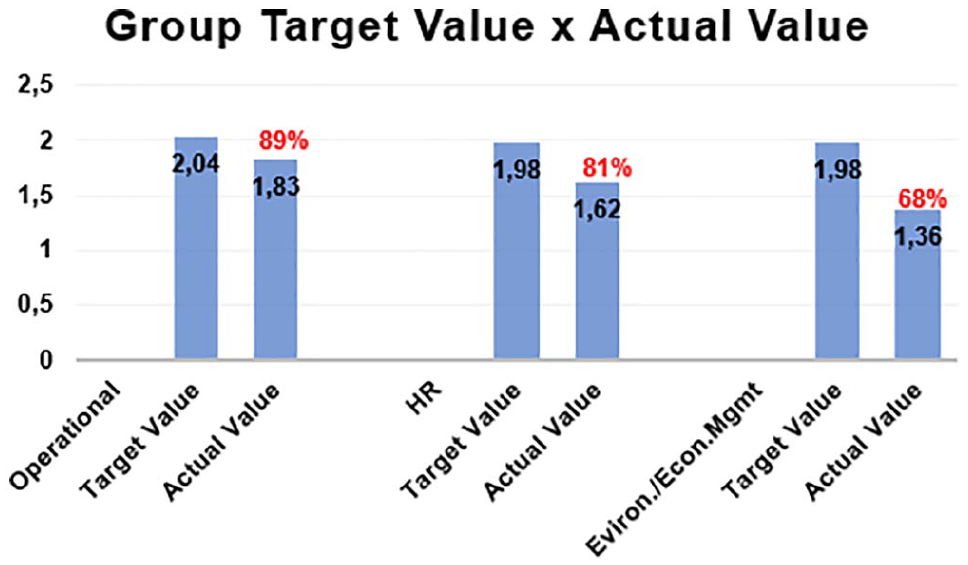
Plot of the groups’ target values × actual values.
These scores can be explained because, from the six hospitals investigated, four (B, C, E and F) do not practice general waste ‘RLs’ and/or do not encourage or only encourage for some types of waste the habit of ‘not generating or reducing HCW’. These two sub-indicators are found under the sustainable practices indicator. Despite not being the most important of the group, they have a very high relative importance, which may undermine the final results in case they are poorly evaluated. In addition, the two hospitals (A and D) that practice RLs were the ones with higher scores for the IGeReS, which means that such habits are actually important for HCWM.
Another point that also affected the results for environmental/economic management, was the indicator Investment in HCWM. Although it was poorly evaluated in only two hospitals (E and F), this criterion is the most important for the group, which led to a decrease in the overall group rate and, consequently, contributed to it having the worst results.
The second worst-rated group was human resources. According to the evaluations, employee training, especially the sub-indicator knowledge about HCWM, was the criterion that most influenced this group’s results. Except for hospitals A and B, the others claim that not all employees are aware of the importance of HCWM. Many of the hospitals train only the employees who have greater contact with the waste and, therefore, these are the only ones who have the appropriate knowledge about it. Thus, since it is the most important indicator in the group, the IGeReS for this group ended up being impaired.
Finally, the operational group was the one with the best IGeReS. In fact, even in the hospitals with the worst results (E and F), the operational part was the one that most positively influenced their indices due to the usage of weighted linear combination, an aggregation method. However, this is a more technical area in which the rules and procedures to be followed have already been stipulated, therefore, facilitating the understanding of what must be done.
Poor indicators and suggestions for improvement
Generally, from the evaluations, most hospitals have difficulties with employee training – in the human resources group – and sustainable practices – in the environmental/economic management group. Among the six hospitals, four had poor evaluation results for both indicators.
Therefore, to achieve a better performance of the IGeReS, some improvements can be suggested for these two indicators. Regarding employee training, the biggest problems reported were lack of employee knowledge about the HCWM and the fact that not all employees are properly trained and/or oriented to the healthcare waste management plan (HCWMP) and HCWM.
Both problems can be solved at the same time. It is known that training requires time and availability of staff, for this reason, it should be focused on all those directly involved with HCW (e.g. cleaning staff, nurses, nursing technicians and doctors). These trainings would be at the discretion of the hospital; nevertheless, these courses should teach not only the correct handling of HCW (segregation, packaging, etc.) but also the importance of properly managing it and how it can affect the environment and human health.
In these trainings, more sustainable practices can also be encouraged, especially in the sense of not generating or reducing waste. Many of the hospitals analysed have this policy, mainly concerning disposable cups and paper. This is already a great start, but they must be more creative, trying to reduce the generation of hazardous waste as well.
It is acceptable for many to believe that this could put the lives of patients and employees at risk, but this reduction and not generation of waste, if done consciously, will only bring benefits, including economic ones. Voudrias (2018) discusses several ways to reduce the generation of dangerous HCW, such as: (a) reduction through the purchase of medical materials and supplies, especially those less dangerous, that produce less waste. Thus, hospitals should aim to eliminate mercury products and replace them with alternatives that do not require specialized disposal; (b) good management and control practices, particularly in the purchase of chemicals, pharmaceuticals and other supplies. The author also suggests that hospitals should use the Life Cycle Assessment software tool in order to make healthcare a greener sector.
Hence, in spite of the fact that hospitals reported greater difficulties with employee training and sustainable practices, these criteria have simple solutions, since they are almost independent of financial resources. Such solutions depend basically on the effort and goodwill of all those involved in the HCWM to support and recognize the importance of the cause, including those in the hospital management.
Sensitivity analysis
Although the suggestions for improvement are of great importance to the academic community and the health sector, it is also necessary to verify how much the proposed changes would affect quantitatively the indices. This work, thus, carried out a sensitivity analysis based on a proposition of scenarios that alter the unfavourable and very unfavourable scores of the indicators. As a consequence, assuming that changes are made primarily in the negatively evaluated indicators, hospitals will have their scores changed favourably.
Seven scenarios were suggested considering the realities of the hospitals. Scores would only be changed to higher values in case the changes were feasible in the near future. The scenarios sought to change isolated groups, pair-wise combinations and the three simultaneously. They are as follows:
Scenario 1: Changes in the scores of the poorly evaluated indicators in the operational group.
Scenario 2: Changes in the scores of the poorly evaluated indicators in the human resources group.
Scenario 3: Changes in the scores of the poorly evaluated indicators in the environmental/economic management group.
Scenario 4: Scenarios 1 and 2.
Scenario 5: Scenarios 1 and 3.
Scenario 6: Scenarios 2 and 3.
Scenario 7: Scenarios 1, 2 and 3.
Figure 4 shows the new results for the hospital indices based on the proposition of these seven scenarios. The current indices are shown on the left and the proposed scenarios on the right.
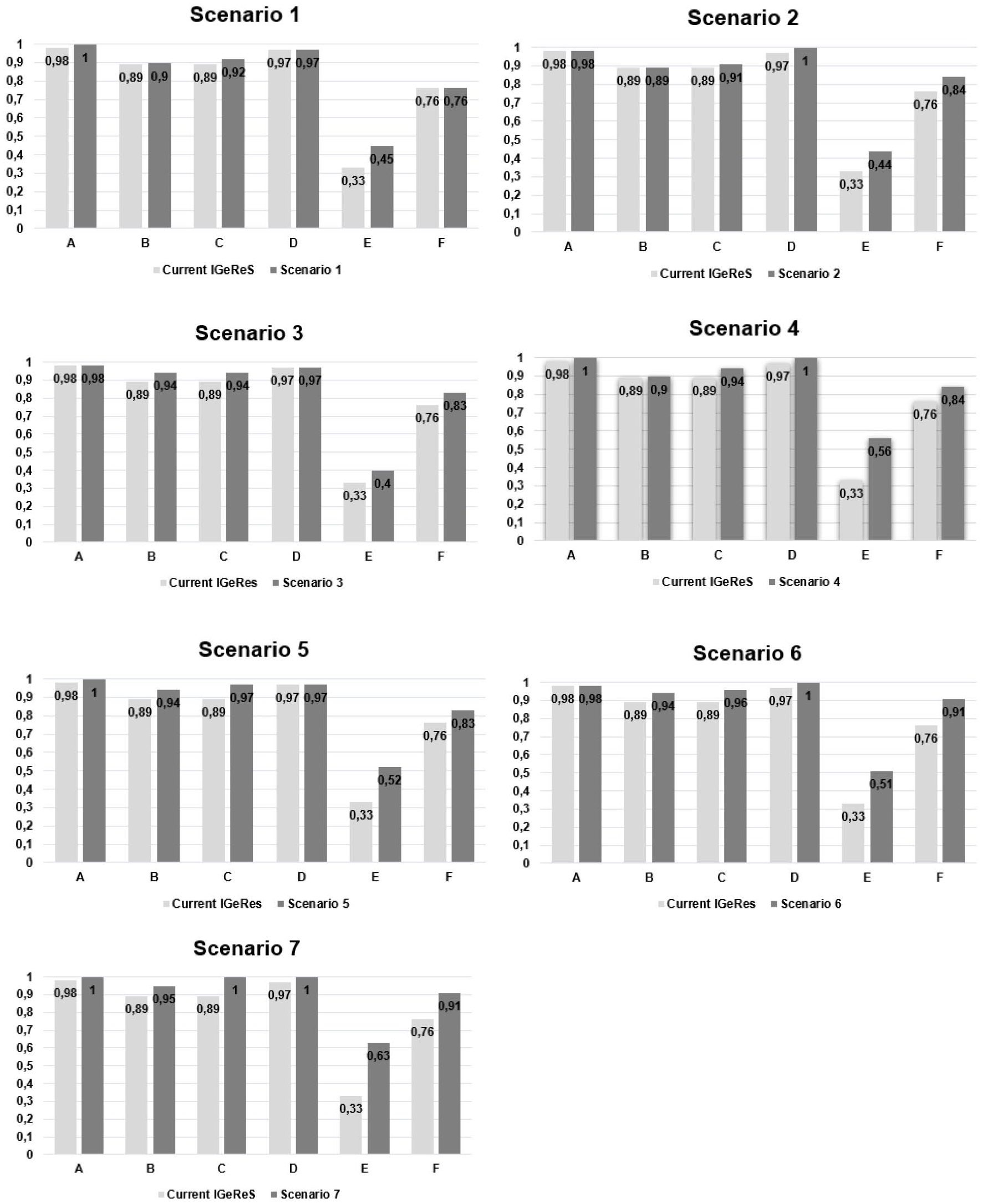
IGeReS results for the new scenarios.
As expected, Scenario 7 showed the best result, as it proposed changes in the three dimensions, obtaining an average increase of 22% in the indices. Even though, hospital E was unable to raise its index to high efficiency. However, the index of hospital E could not reach 0.8, its IGeReS increased more than 90% with the proposition of this scenario, which indicates that the changes previously proposed may have a very positive impact in the hospital’s HCWM if carried out.
Additionally, another scenario that proved to be very efficient without requiring financial investments was Scenario 4. Improvements in the operational and human resources groups affected very positively all the hospitals’ indices. Although the results of the IGeReS of hospitals E and F were not the best among all the proposed scenarios, the index of the former increased by almost 70%, changing its classification to mean efficiency, whilst the latter managed to increase its index by 10%, enough to being classified as a highly efficient in HCWM.
Discussion
Several recent studies have pointed out the importance of hospital waste management. Although all of them have different approaches, at the end they corroborate the idea that further research is needed on the subject, especially in the context of the COVID-19 pandemic, as more contaminated waste is generated. Among these studies, some themes stand out, such as: the best location for the final disposal of HCW (Chauhan and Singh, 2016; Manyoma-Velásquez et al., 2013; Thakur and Ramesh, 2017); choosing the best HCW treatment technologies (Baati et al., 2014; Hinduja and Pandey, 2018; Kalhor et al., 2016; Karagiannidis et al., 2010; Lee et al., 2016; Voudrias, 2016); and the criteria for choosing HCWM suppliers (Faisal et al., 2011; Ho, 2011; Hsu et al., 2008; Ishtiaq et al., 2018).
Moreover, another significant topic for the HCWM, which is similar to this research, is the assessment of waste management in health facilities using performance indicators. The works of Ventura et al. (2010), Assis et al. (2017) and Aung et al. (2019) addressed this topic and most of their results were validated in this work. Employee training is a problem, particularly for waste management, proving to be a factor of concern not only in Brazilian hospitals but also in foreign ones. According to Delmonico et al. (2018), the lack of employees’ awareness regarding the separation of waste is also pointed out as one of the main barriers to be overcome by the HCWM.
Furthermore, as indicated by Barbosa and Mol (2018), the elaboration of HCWM indicators proved to be of great importance for the assessment of waste management in hospitals, as they provide adequate risk management in health environments, favouring the identification of problems and helping with the management process. In addition, the indicators proposed in this research can be used to compare and rank hospitals, if they are of interest to future researchers, as done by Moreira and Günther (2016), who contributed to decision making in waste management practices.
The indicators were also important to show how they can influence the final result of the index. From the sensitivity analysis, the IGeReS was proven to be very sensitive to small changes in the indicator scores. Slight variations can even change the HCWM classification of hospitals, as occurred with hospital F, for example in Scenario 2. This is only possible because the weighted linear combination was used as a method for aggregating the weights of the criteria, which allows good indicators to outweigh bad ones as affirmed by Moraes et al. (2020) who identified deficiencies in waste management in Brazilian cities.
Another important point in this research was the use of AHP to prioritize the indicators. This tool was essential for the achievement of final results, since it better reflects the complexity of the problems involved in the management of HCW, as stated by Aung et al. (2019) who checked the urgent need for better waste management regulation in their country. Additionally, similar to the work of Moraes et al. (2020), the weights of the indicators from the impartial assessment of different specialists in waste management could be found due to the AHP.
This prioritization of indicators, along with evaluations of the hospitals, was responsible for the preparation of the IGeReS. According to Jannuzzi (2004), author of a book that addresses concepts and applications of social indicators, the index is an essential operational tool to monitor and assist with the planning, implementation, execution and evaluation of programmes, projects and services. The IGeReS, therefore, aimed to show quantitatively the situation of the HCWM in hospitals, facilitating the understanding of managers about which points need to be improved in order to achieve greater efficiency in the waste sector.
Finally, the number of hospitals investigated was a limiting factor for this research, since it was not possible to find the influencing agents of the HCWM. However, it is believed that this fact did not hinder the results whereas the objective of the research was achieved by the creation of an evaluation tool that proved to be very effective in determining in a simple and precise way the points of HCWM that should be improved, which contributes to the hospital’s management and consequently to the sustainability and human health. This article has also an academic contribution through the development of a tool with indicators that evaluate operational, human, economic and environmental factors in waste management in an innovative way. Therefore, in order to continue this study, other hospitals in different regions should be evaluated, so that the general situation of the HCWM can be analysed.
Conclusions
This work aimed to evaluate the RLs and HCWM in hospitals. From this purpose, a support tool (IGeReS) was developed to help managers understand the main points to be tackled for improving the sector. Thus, the AHP was used as an instrument to support decision making applied to RL and waste management. It is noteworthy that the IGeReS developed in this work can be used in other hospitals, since it is a tool that can be easily used and understood by the evaluator.
The application of the index allowed for the verification that, in general, the facilities studied carry out satisfactory waste management, since out of the six hospitals investigated, four had their IGeReS classified as high efficiency. The two hospitals that did not achieve this classification are located in the poorest region of the state, which may be an indication that location is an influencing factor in the HCWM. Additionally, the hospitals with the best IGeReS are the largest among those investigated, which can point out that it also affects the HCWM.
Through the application of the IGeReS it was possible to verify with which indicators the hospitals had greatest difficulties. One of them is employee training, considering that it was reported that not all health facility employees have adequate knowledge about and training in the importance of HCWM. However, because it is not considered as an essential competence for health institutions, waste management is not seen as a priority by them. The other indicator the hospitals demonstrated to have great difficulty with was sustainable practices, as the facilities have timidly promoted mainly the reduction of the generation of hazardous waste.
Accordingly, it was concluded that the IGeReS can be a very useful tool for the evaluation of HCWM in hospitals since the results in the form of an index quantitatively demonstrated the reality of this sector. Thus, expanding the application of IGeReS to different regions, it would be possible to analyse whether the factors identified in this work as possible influencers of the HCWM are in fact real.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to acknowledge the Brazilian agencies Foundation for the Promotion of Science of the State of Minas Gerais (FAPEMIG) and Brazilian National Council for Scientific and Technological Development (CNPq) for the financial support provided to this research.