
Abstract
Worldwide, there is a growing concern about the negative effects of infectious medical waste produced during the COVID-19 pandemic and the contamination risks associated with waste management. Therefore, measures to ensure that medical waste is managed safely and in an environmentally sound manner will avoid negative health and environmental effects from such waste, thus protecting the health of patients, health workers and the public in general. Despite that infectious medical waste generation rate is important for management planning and policy development, there is a limitation on national data availability and its accuracy, particularly in developing economies. This study analyses the infectious healthcare waste generation rates and management patterns in Lebanon before and after the COVID-19 pandemic. The estimated average of COVID-19-related infectious healthcare waste generation in this study is 39,035 kg per month or 1.3 tonnes per day, which constitute between 5% and 20% of total infectious healthcare waste in Lebanon. This study illuminates on the impact of COVID-19 on the existing challenges of waste management in Lebanon. It highlights the need for proper management and disposal of the amounts of medical waste generated to reduce contamination risks or related environmental threats, particularly during the pandemic. It also shows that Lebanon has a defective system for monitoring of waste from healthcare institutions and gaps in waste statistics. Finally, the study summarizes recommendations related to medical waste management, which can provide valuable insight for policymakers.
Keywords
Introduction
The COVID-19 pandemic has triggered diseases and deaths, created immense confusion for the world and modified solid waste management profiles (Klemeš et al., 2020; Penteado, 2021). This pandemic changed the behavioural and consuming patterns of people, resulting in a sudden change in the generation amount, composition and disposal rate (timing and frequency) of municipal solid waste (MSW), depending on location. However, the prediction is that the overall MSW generation would slightly decrease during COVID-19 (Fan et al., 2021; Klemeš et al., 2020). It also proposed that the use of plastic products for the prevention of the epidemic expanded during the COVID-19 pandemic (Zhou, 2021). A major rise in plastic use has been associated with packaging requirements and single-use products due to the demand for distribution and take-out of food/goods as well as the demand for plastics for medicinal uses (Fan et al., 2021). On the other hand, because of the fear of inadequate food supply during the outbreak, people continued to conserve food and thereby decreased food waste (Jribi et al., 2020). In their evaluation of the expected trend of medical waste flow along with the epidemic/pandemic crisis, Klemeš et al. (2020) showed that medical waste generation increased sharply, reaching up to a 370% increase in some places such as Hubei Province, China. In Wuhan, medical waste rose from a normal level of 40 tonnes per day to a peak of approximately 240 tonnes per day, reaching a maximum capacity of 49 tonnes per day for incineration (Tang, 2020). According to the latest published report by the United Nations Environment Programme (UNEP, 2020), the rise in healthcare waste from COVID-19-associated healthcare facilities was reported to be 3.4 kg per person per day worldwide, and approximately 2.5 kg per bed per day of COVID-19 healthcare waste was produced in developing countries. The COVID-19 pandemic has equally affected the management systems of MSW. In this context, recommendations were presented by several different organizations (Basel Convention, 2020; CDC, 2020; European Commission, 2020; ISWA, 2020; OSHA, 2020; UNEP, 2020; USEPA, 2020; WHO, 2020) with various scopes at worldwide, regional or national levels to address different actors such as waste generators (citizens), waste collectors, employers (service providers) and local governments. Among them, the recommendations of the International Solid Waste Association (ISWA, 2020) at worldwide level stand out as the most comprehensive and detailed. The main measures and recommendation for MSW handling and management include the following: providing adequate personal protective equipment (PPE) and ensuring enhanced personal hygiene standards; discontinuing immediately manual sorting of mixed waste or commingled recyclables, including disabling and substituting the manual stages in mechanical-manual systems; and providing other adequate information on COVID-19.
Overall, the number of COVID-19-infected persons worldwide has increased from 5 million in March 2020 to over 90 million as of 14 January 2021, and continues to grow (Our World in Data, 2021). With the rise in the number of COVID-19 infections, almost every region of the world has an expected increase in medical waste from healthcare facilities, such as hospitals, clinics, laboratories, temporary quarantine centres and research laboratories. Therefore, measures to ensure that medical waste is handled and managed appropriately and in an environmentally sound manner will help to avoid harmful health and environmental effects from such waste, including the accidental release into the atmosphere of chemical or biological contaminants, including drug-resistant microorganisms, thus protecting the health of patients, health workers and the public at large (WHO, 2018). For the assessment of environmental effects and the design of management strategies, site-specific data relating to the infectious healthcare waste generation rate is important for planning and policy development (Graikos et al., 2010; UNEP, 2020). To the best of the authors’ knowledge limited studies have been conducted to assess the amount of infectious medical waste generation during the COVID-19 pandemic, particularly in developing countries (Agamuthu and Barasarathi, 2020; Mihai, 2020; UNEP, 2020).
Lebanon had a population of 6,007,000 in 2016, a life expectancy at birth (male/female) of 74/79 in 2019 and a total expenditure on health as a percentage of the gross domestic product of 6.39% in 2014 (WHO, 2021). In the past, healthcare waste was not being adequately and properly managed, thus resulting in significant environmental problems such as air, soil and water pollution as a direct implication of the haphazard burning and dumping of healthcare waste (MoE/UNDP/ECODIT, 2011). Starting in 2002, and after the implementation of Decree 8006 (dated 11 June 2002) on the proper handling of healthcare waste in Lebanon, many hospitals and institutions began to manage their medical waste in an environmentally sustainable manner. In 2003, a local non-governmental organization (NGO) named Arcenciel started treating (autoclaving) and collecting potentially infectious healthcare waste and became active in several regions in Lebanon. As of 2010, 55–60% of the total healthcare waste stream (about 90% of Beirut’s waste stream) collected from 81 public and private hospitals is being treated by Arcenciel. Therefore, autoclaving became the main method for treating waste generated by hospitals. The remaining portion (around 35–40%) of the healthcare waste is either incinerated at hospitals without permits or illegally dumped with MSW (MoE/UNDP/GEF, 2016). Note that to this day, in Lebanon, MSW incineration is not practised and the Lebanese Decree 13389/2004 prohibits incineration of potential infectious medical waste and recommends treatment using a sterilization method. Starting in 2003, autoclaving conducted by Arcenciel significantly reduced the amount of medical waste incinerated in hospitals or medical facilities from 1250 tonnes per year in 2003 to 60 tonnes per year in 2015 (MoE/UNDP/GEF, 2019). However, it should be highlighted that incineration carried out at the different medical establishments is without monitoring and contributed to a total of 1050 tonnes of CO2 equivalent of greenhouse gas emissions per year (MoE/UNDP/GEF, 2016). Uncontrolled and unlicensed incineration of healthcare waste in many hospitals was also associated with the release of persistent organic pollutants and other pollutants (MoE/UNEP/GEF, 2017). Moreover, current technologies for medical waste treatment are not adequately monitored. There was no assessment of the efficacy of medical waste treatment using autoclaves. Currently, it is estimated that around 80–85% of infectious healthcare waste in Lebanon is being treated by Arcenciel in close collaboration with other stakeholders (MoPH, 2018). The majority of treated medical waste is then disposed of in landfill or dumpsite at the available site. All medical waste should, however, be adequately treated and disposed of, so the Ministry of Environment (MoE) should continue to force institutions to comply with the related decree.
The trend of new COVID-19 cases is increasing with more than 252,000 cases and 1906 deaths reported as of 17 January 2021 in Lebanon (MoI, 2021). A similar rise in the production of medical waste is expected in Lebanon. However, limited recent and accurate information is available on the amounts of infectious medical waste produced in healthcare facilities, which are necessary to determine healthcare waste sorting and management procedures (Maamari et al., 2015), especially during the COVID-19 pandemic.
To fulfil the gap, this study provides a rapid assessment method to estimate COVID-19-related waste generated in Lebanon. This analysis is useful for other developing economies, which face gaps in waste statistics data, as an alternative way to quantify the potential waste flow associated with COVID-19 necessary for decision-makers to reduce other contamination risks and related environmental threats. Furthermore, the estimated infectious medical waste generation rate in this study can facilitate benchmarking among countries, by allowing them to compare their generation rates against other countries. Therefore, this will help them to identify possibilities to improve the efficiency of their medical waste management system and predict their associated costs. This study can potentially guide both academicians and policymakers to draft medical waste management strategies to meet sustainable development goals.
We analysed infectious medical waste generation rates and patterns in Lebanon before and during the pandemic. We also conducted a review of existing medical waste policies, regulations and management procedures. This study illuminates the impact of the COVID-19 pandemic on the existing challenges of medical waste management in Lebanon. Finally, this study provides key recommendations for improving medical waste management in Lebanon and supporting decision-makers.
Methodology
This article is divided into two parts for assessing the infectious medical waste management in Lebanon before and after the COVID-19 pandemic.
The first part reviews the existing policy and legal and institutional framework, as well as the generation and management of medical waste prior to the COVID-19 pandemic. The review is carried out using published state reports, journal articles, sources from the Internet, official public documents and interviews with main stakeholders responsible for regulating the healthcare waste management sector in Lebanon (such as the MoE, Ministry of Public Health and Arcenciel).
The second part consists of analyzing the impact of COVID-19 on medical waste management in Lebanon. It also provides information on the monthly amount of COVID-19-related infectious medical waste generated between March and October 2020 in Lebanon, allowing the benchmarking among countries. The current average quantities of infectious healthcare waste generated in Lebanon were estimated using the monthly records of Arcenciel, a service provider for waste collection and treatment in Lebanon since 2003.
It should be noted that medical waste can also be known as healthcare waste, clinical waste or scheduled waste (DOE, 2009). It includes all the waste generated inside healthcare facilities, hospitals, research centres and laboratories related to medical procedures, according to the World Health Organization (WHO) guideline reports. It also involves the waste generated in homes (WHO, 2014, 2017). The composition of healthcare waste can be heterogeneous, including both hazardous and non-hazardous, and can also be classified into the following groups: infectious waste, pathological waste, sharps waste, chemical waste, radioactive waste, cytotoxic waste, pharmaceuticals waste and non-hazardous or general waste (WHO, 2014). Of the overall amount of waste produced by healthcare operations, about 85% is non-hazardous general waste. The remaining 15% is known to be hazardous materials that may be infectious, toxic or radioactive (UNEP, 2020). However, in low-income countries, healthcare waste is also not classified into hazardous or non-hazardous waste, making the total volume of hazardous waste even larger (WHO, 2018).
In Lebanon, Decree 13389/2004 defines healthcare waste into four categories: 1 = non-hazardous waste (e.g. generated from the administration offices, the cafeteria, the kitchen of the hospital, the patients’ rooms, etc.), 2 = hazardous waste (including infectious and non-infectious), 3 = special waste (such as pharmaceuticals, chemical waste, cytotoxic and pathological), and 4 = radioactive waste (MoE/UNDP/ECODIT, 2011). Infectious healthcare wastes are defined as ‘any waste material that came in contact with blood and other potentially infectious fluids of the body, sharps, any waste produced by an isolated patient and biological fluids, small anatomic parts, tissues, cultures and stocks of infectious agents’ (Maamari et al., 2015). Among the total healthcare waste generated, 80% is considered as MSW or general waste (non-hazardous) and 20% as hazardous medical waste. The 20% of hazardous medical waste is divided as follows: 80% (or 16% of the total healthcare waste generated) potentially infectious waste and 20% (or 4% of the total healthcare waste generated) other hazardous waste (such as chemical, genotoxic, pharmaceutical, cytotoxic and radioactive). The estimated medical waste in this study is infectious waste because it is sorted at the point of generation in the majority of hospitals and other healthcare institutions and then weighed immediately before collection. In this context, it is easier to estimate infectious healthcare waste. However, accurate estimation of non-infectious medical waste generated from these institutions is lacking as this waste is considered to be part of MSW.
Results and discussion
Overview of medical waste management in Lebanon
Existing policy and legal and institutional framework
The healthcare sector is perceived to be one of the country’s largest and most advanced service-providing sectors and is dominated mainly by the private sector (World Bank, 2020a).
In the past decade, Lebanon has enacted key legislations related to healthcare waste management. Decree 8006 (dated 11 June 2002) is amended by Decree 13389 (dated 18 September 2004). This decree is the actual focal point for national regulations pertaining to waste management by healthcare institutions. It classifies the different healthcare waste categories and indicates the proper management and disposal of each category. In accordance with this decree, all hospitals and medical institutions/organizations are responsible for the management of their generated medical waste in an environmentally appropriate manner. In 2011, the government, through the MoE, tried to enforce the decree with continuous follow-up with all the medical institutions (mainly hospitals). Moreover, hazardous waste is regulated under Law 64, which dates back to 1988. Lebanon has also ratified three main international conventions dealing indirectly with the issue of healthcare waste management: (a) the Stockholm Convention on persistent organic pollutants (ratified by Law 432/2002); (b) the Basel Convention (ratified by Law 387/1994, 29/2015) (UNEP and Secretariat of the Basel Convention, 2003) on the control of the transboundary movements of hazardous wastes and their disposal (Laceco/Ramboll, 2012); and (c) the Minamata Convention on mercury (acceded by Law 2/2017), which is a global treaty to protect human health and the environment from the adverse effects of mercury. More details on the legal framework in Lebanon in relation to healthcare waste are available in Supplementary Material (Table SM.1).
Decree 13389 also established the permitting mechanism for infectious healthcare waste treatment facilities. Under this decree, healthcare waste should be treated at specialized treatment facilities licensed by the MoE before being disposed of. It is important to highlight that environmental guidelines for the establishment and operation of healthcare waste treatment facilities and the licensing of healthcare waste transportation vehicles are still lacking in the Lebanese legal framework. Recently, new decisions, memoranda and administrative circulars were circulated, such as Decision 2824/1 in 2015 regarding the formation of a committee to treat medical waste and Memorandum 34 (dated 4 December 2019) relating to the obligation to fulfil health and environmental conditions by hospitals, in order to regulate the role of the Ministry of Public Health and promote a proper and comprehensive management of healthcare waste in Lebanon.
According to local legislations, the responsibility of the regulation and management of healthcare waste is distributed among a number of authorities, namely MoE, Ministry of Public Health, Ministry of Interior and Municipalities, and Council for Development and Reconstruction. The various public authorities responsible for regulating the healthcare waste and their duties in this area are summarized in Supplementary Material (Table SM.2).
Generation of medical waste
In Lebanon, the total amount of healthcare waste generated from all sources, particularly from clinics, is very difficult to estimate, as it is neither officially documented nor registered. In fact, most of the research carried out in relation to the healthcare waste is concentrated on hospitals that provide an approximate estimation. Table 1 displays the estimated hospital healthcare waste generation in Lebanon based on previous studies.
Estimated healthcare waste generation in Lebanon during the past years.
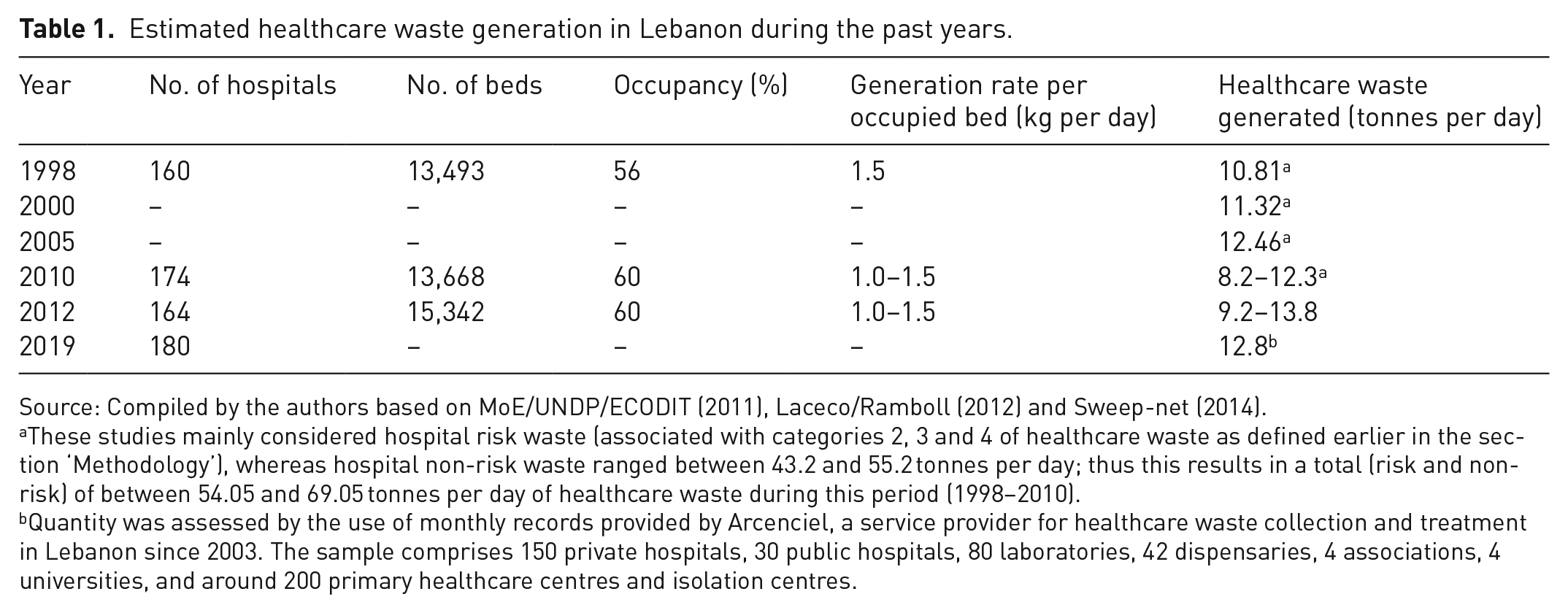
Source: Compiled by the authors based on MoE/UNDP/ECODIT (2011), Laceco/Ramboll (2012) and Sweep-net (2014).
These studies mainly considered hospital risk waste (associated with categories 2, 3 and 4 of healthcare waste as defined earlier in the section ‘Methodology’), whereas hospital non-risk waste ranged between 43.2 and 55.2 tonnes per day; thus this results in a total (risk and non-risk) of between 54.05 and 69.05 tonnes per day of healthcare waste during this period (1998–2010).
Quantity was assessed by the use of monthly records provided by Arcenciel, a service provider for healthcare waste collection and treatment in Lebanon since 2003. The sample comprises 150 private hospitals, 30 public hospitals, 80 laboratories, 42 dispensaries, 4 associations, 4 universities, and around 200 primary healthcare centres and isolation centres.
In 2012, assuming 60% occupancy and an average generation rate of 1.0–1.5 kg per bed per day, Lebanon generated about 9.2–13.8 tonnes of risk healthcare waste daily (about 3358–5037 tonnes per year) from 164 public and private hospitals (about 15,342 hospital beds) (MoE/UNDP/GEF, 2016). Approximately, a total of 69 tonnes of healthcare waste was generated per day (25,200 tonnes per year) divided into risk waste (14 tonnes per day) and non-risk waste (55 tonnes per day) in Lebanon (MoE/UNDP/ECODIT, 2011).
A study by Maamari et al. (2015) estimated that the total infectious healthcare waste generation rates in Lebanon was equal to 6,383,806 kg per year based on data records for the years 2009–2013 (assuming 15,342 hospitals beds). The study also showed that for large private hospitals (over 200 beds), the infectious healthcare waste generation average was 2.45 kg per occupied bed per day. For other hospitals, that is public hospitals, and private hospitals under 200 beds, the rate is 0.94 kg per occupied bed. The weighted mean is estimated at 1.14 kg per occupied bed per day (assuming an average hospital occupancy rate of 58%). These values are greater than the reference levels of WHO for the Middle East (0.54 kg per bed per day), but very close to reported infectious healthcare waste generation levels by Sanida et al. (2010) for Greece (0.85 kg per occupied bed per day).
In 2019, we estimated the quantities of infectious healthcare waste generated to be around 4,666,754 kg per year or 12.8 tonnes per day, based on the monthly records of Arcenciel, which have slightly decreased in comparison with previous years (Table 1). This estimate is for 150 private hospitals, 30 public hospitals, 80 laboratories, 42 dispensaries, 4 associations, 4 universities, and around 200 primary healthcare centres (PHCs) and isolation centres, from which infectious healthcare waste is collected on a regular basis by Arcenciel. In this context, it is worth noting that Lebanon is facing a multi-faceted crisis, combining a financial and economic collapse, a political crisis, a health crisis and a waste crisis. Starting in October 2019, the economic and financial crisis in Lebanon has greatly limited the ability of the health sector to deliver affordable and accessible services. This was attributed to many problems, such as the following: (a) persistent delays in government payments to hospitals; (b) a lack of dollars and uncontrolled limits on the access of depositors to their accounts, and hampering the importation of vital medical facilities, drugs and supplies; and (c) a rise in unemployment rates, contributing to a rise in the number of uninsured residents, especially among middle-income communities needing government assistance. In addition, the drop in the values of salaries has forced hundreds of doctors and nurses to leave the country altogether. The COVID-19 pandemic further aggravated the health sector’s financial strains (World Bank, 2020a).
The situation was exacerbated on 4 August 2020, when a massive explosion rocked the port of Beirut, destroying much of the port and severely damaging dense residential and commercial areas within 5 km of the site of the explosion. Multiple public and private hospitals centrally located in Beirut reported extensive damage and were not able to welcome patients. Therefore, several facilities are still not operating at their pre-blast capacity. The explosion also caused damage to solid waste management facilities as well as damage to the healthcare waste storage facilities of three hospitals in Beirut, and the healthcare waste was then collected and outsourced for treating to an external contractor (World Bank, 2020b). Lebanon has been suffering since 2015 from a waste crisis after the premature closure of the main landfill (Naameh) that served as the primary largest sanitary landfill in the country serving more than half the total population (El-Fadel and Maalouf, 2020; Maalouf and El-Fadel, 2019). The problem was exacerbated following the Beirut explosion, which generated large quantities of debris and demolition waste and severely damaged two key sorting, recycling and composting facilities that were helping to reduce the amount of MSW that goes to landfills.
Collection and treatment of medical waste
According to the MoE, most of the medical waste generated is being collected and treated (mainly autoclaving) by the private sector. The role of private sector participation is to centralize treatment, particularly in urban areas, where the majority of medical facilities are located, thereby reducing costs and enhancing service quality. As of 2010, 33% of private hospitals, 20% of public hospitals and only 2% of private laboratories/clinics treat their healthcare waste either on-site or in off-site units (inside and outside hospital premises, respectively). Other health centres/hospitals located in Beirut are reported to export a small amount of their hazardous waste under the Basel Convention (Sweep-net, 2014).
A recent assessment of waste management in 213 PHCs, conducted by the Ministry of Public Health in 2017 (MoPH, 2018), in an attempt to assess the situation of infectious waste, revealed that 80.5% of surveyed centres (169 out of 210) sort their medical waste; yet, there is an uncertainty in the proper disposal of infectious waste. Moreover, only 39% (82 out of 210) have a contract with specialized companies (Arcenciel, Mirage and Safe) for proper disposal of their infectious waste and 27.6% (58 out of 210) hand them over to hospitals. About 1.5% (3 out of 210) have incinerators and the rest (32% or 67 out of 210) have their infectious waste dumped in landfills directly or through municipalities. The assessment also tackled 31 public hospitals. The results showed that 67.7% (21 out of 31) of the contacted hospitals hand them to specialized companies (Arcenciel or Safe), and 22.6% (7 out of 31) did not answer, have an autoclave or are in transitory phase and looking for a solution. The remainder 9.7% (3 out of 31) dispose of them in municipal dumpsites or simply burn them. Thus, the above assessment indicates that the amount of medical waste is not adequately managed, and that hospitals and PHCs have a weak waste management monitoring system. Moreover, this highlights the need for a more comprehensive survey covering all types of healthcare institutions/facilities (e.g. private hospitals, clinics, laboratories) in order to identify the various potential major and minor sources of medical waste in Lebanon.
The total number of licences issued by the MoE for healthcare waste treatment facilities using autoclaves amount to seven. These treatment facilities are either built within the hospitals premises and thus operated by the hospital itself or are off-site from the hospitals premises and operated by Arcenciel. There are only two on-site treatment centres in two private hospitals and five off-site treatment centres operated by Arcenciel (Sweep-net, 2014). The unit cost as charged by Arcenciel for the collection, treatment, training and provision of bins is 0.64 USD kg–1 for hospitals and 1.72 USD kg–1 for laboratories, dispensaries, associations, universities and PHCs (MoPH, 2018). More details on the existing healthcare waste treatment units in different locations in Lebanon are available in Supplementary Material (Table SM.3).
Overall, around 80–85% of infectious healthcare waste in Lebanon is managed through a national infectious healthcare waste management network operated by Arcenciel in close collaboration with the MoE, the Ministry of Public Health, the Syndicate of Hospitals and Healthcare Institutions, and municipalities (MoPH, 2018). This network provides training and awareness for administrative employees, cleaning workers and healthcare staff on healthcare waste sorting and management. Infectious healthcare waste sorting is conducted at the generation point in most hospitals and other healthcare institutions.
On a daily basis, Arcenciel collects infectious healthcare waste from hospitals and other healthcare institutions based on a prepared collection route. Only yellow bags that contain sorted potentially infectious healthcare waste and sharps containers are collected by Arcenciel. There is no collection of opened bags or bags containing hazardous waste other than potentially infectious healthcare waste or identifiable anatomical parts. In fact, in compliance with the Lebanese Decree 13389/2004, identifiable anatomical parts should not be processed in autoclaves. To ensure that there is no radioactive content in the stored bins, a radioactivity detector is used. In each healthcare institution, the infectious healthcare waste is weighed directly before collection, in the presence of a hospital/institution representative who signs the waste tracking document. The infectious healthcare waste is then transported to the network’s closest treatment centre. Five treatment centres serving all regions of Lebanon are part of the network. Each treatment centre contains one medical waste autoclave which will, when needed, be a backup system for the other centres. Infectious waste is transported through an optimized route, designed in such a way to minimize travel distances, using specially equipped vehicles exclusively used for potentially infectious healthcare waste transportation, which is systematically cleaned and disinfected. Arcenciel requires healthcare institutions to have a cold storage room as a pre-condition to sign a contract with them, in order to facilitate the collection scheme. The collection frequency depends on the amount of infectious healthcare waste generated and the availability or capacity of the refrigerated storage room inside the hospitals and healthcare institutions. In fact, infectious healthcare waste may be preserved more than a week before treatment, providing that it is kept cool or refrigerated, ideally at a temperature not exceeding 3–8°C (WHO, 2013). Arcenciel sends reports to the MoE every trimester, including the amounts collected from each hospital and healthcare institution.
The majority of the generated medical waste is treated by autoclave associated with shredding. During sterilization, healthcare waste shredding decreases the likelihood of accidental injury or sharp incision, raises the total exposure of waste to heat and renders healthcare waste unrecognizable. As a consequence of this process, the crushed and sterilized waste obtained is not identifiable and is no longer hazardous. Using this method decreases the total waste volume by 80% (HCWH, 2001). Moreover, waste segregation before processing will eliminate harmful gas emissions during autoclaving (Karagiannidis et al., 2010). The minimum performance for the autoclaving process is to achieve a sterility assurance level of 6-log reduction (10−6) to provide the greatest assurance of sterility for critical products such as implantable devices or injectable drugs and to reach 90% reduction in microbial population. According to Mosley (2008), a process that achieves a 6-log reduction (10−6) will theoretically reduce an initial population of one million organisms to very close to zero.
In central sterilization treatment systems, sterilized healthcare waste at the end of the treatment process can then have the characteristics of domestic solid waste (Karagiannidis et al., 2010). Sterilized waste is thus transported and disposed of at a MSW sanitary landfill. Therefore, once treated, the infectious waste is sterilized and is no longer considered as hazardous waste.
As for the other types of hazardous waste, the Council of Ministers Decree 5606/2019 determines what is related to integrated hazardous waste management in Lebanon. It is worth noting that, until now in Lebanon, no landfill has been engineered for hazardous waste. Hazardous waste is mainly exported under international recommendations and mandates (e.g. Basel Convention).
The remaining portion (around 15–20%) of the healthcare waste, which is not being collected or managed by Arcenciel or other waste operators, is either incinerated at hospitals without permits or illegally dumped with MSW (MoE/UNDP/GEF, 2016). This highlights the need for proper management and disposal of the amounts of medical waste generated to reduce contamination risks or related environmental threats.
Management of COVID-19-related medical waste
In the face of the COVID-19 era, healthcare centres such as hospitals, clinics, laboratories, temporary quarantine centres, research laboratories hospitals and public health centres, and even homes, will produce COVID-19-related medical waste. As the source of medical waste relating to COVID-19 has been complex, the initial management of medical waste from the source control is important. The detailed composition of COVID-19-related infectious medical waste is not well documented in Lebanon. However, the COVID-19-related waste could be composed of swabs, syringes, needles, sharps, blood or body fluid, excretions, mixed waste, laboratory waste, material or equipment contaminated with the virus, masks or disposable gloves, and PPE that are used for screening and treatment for COVID-19-infected patients (Agamuthu and Barasarathi, 2020).
Policy and regulations in relation to the COVID-19 pandemic
During the COVID-19 pandemic, no new policies or regulations were introduced for the management of COVID-19-related waste because they are classified under the category of infectious healthcare waste. Therefore, the management of waste generated from COVID-19-related cases has been managed in compliance with existing regulations related to infectious healthcare waste. However, additional training and awareness programs related to COVID-19 waste management in Lebanon were carried out mainly on the proper use of PPE, especially for the waste collectors. Moreover, Arcenciel is asking healthcare facilities to mark the COVID-19 waste for tracking and data purposes in terms of reporting to the MoE and Ministry of Public Health. It should be noted that the only enforcement of existing rules and regulations is through the trimestral report that is submitted by Arcenciel to the MoE and the yearly renewal of their permits, which include an inspection of their treatment facilities.
The WHO (WHO, 2020) has recommended disposal methods in healthcare facilities, such as controlled thermal treatment conditions or the use of conventional biocidal agents that are successful in removing the coronavirus (Kampf et al., 2020). All medical waste produced by patients associated with COVID-19 should be safely gathered in designated containers and bags, treated, and then disposed of or treated safely, or both, preferably on-site. If waste is transported off-site, identifying where and how it will be treated and discarded is important. Necessary PPE (boots, apron, long-sleeved gown, heavy gloves, mask, and goggles or a face shield) should be used by those treating healthcare waste, and hand hygiene should be carried out after the PPE has been removed (WHO, 2020).
Generation of COVID-19-related medical waste
Initially, medical waste was expected to increase greatly because the number of COVID-19 patients reported will probably increase. The comparison of medical waste generation before and after the COVID-19 pandemic in Lebanon is displayed in Figure 1 from March to October between 2019 and 2020. The total average amount of infectious medical waste generated monthly in 2020 (355,171 kg) was 9% lower in comparison with 2019 with a monthly average of 388,896 kg of infectious medical waste. This can be mainly attributed to the fact that hospital assessment was substantially reduced for most patients with generally mild conditions due to concern of COVID-19 infection. In addition, the decrease of infectious healthcare waste generated from 2019 to 2020 could be attributed to the national economic and financial crisis that affected hospitals and other healthcare facilities that were forced to reduce their staff members and work at half capacity, which reflected on the number of patients they received as described in the section ‘Generation of medical waste’. Another reason behind this decrease is the fear of the public of heading to hospitals because of COVID-19. Therefore, the large majority of cases in healthcare centres are COVID-19-related, except for a few urgent non-COVID-19 cases which are allowed to be taken care of in hospitals. However, in August 2020 a sudden change in the pattern occurred, when thousands of people were admitted to hospitals following the Beirut port explosion.
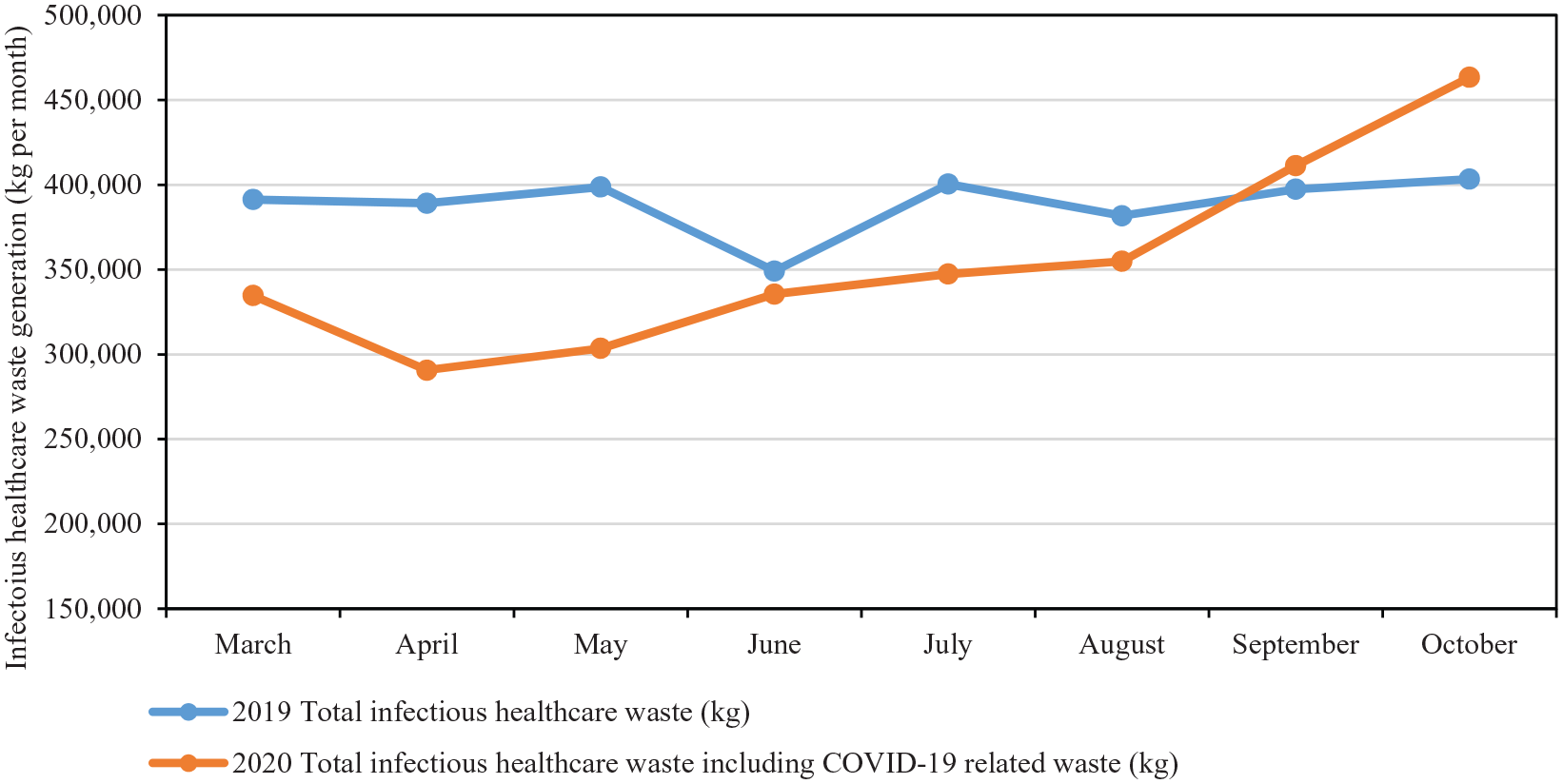
Changes in the pattern of medical waste generation due to COVID-19 in Lebanon.
The amount of isolated COVID-19-related medical waste generated in 2020 has increased with the spread of COVID-19 from February 2020. From March to April 2020, the amount of isolated infectious medical waste generated was about 71% higher and the generation amount of isolated medical waste has increased more than double after August 2020 as shown in Figure 2. The correlation between COVID-19 patients and isolated COVID-19-related infectious medical waste from February 2020 is clearly shown in Figure 2. The isolated COVID-19-related infectious medical generation in 2020 ranged between 18,351 and 91,352 kg per month, which constituted 5–20% of total infectious healthcare waste. The estimated average of COVID-19-related infectious healthcare waste per month is 39,035 kg or 1.3 tonnes per day.
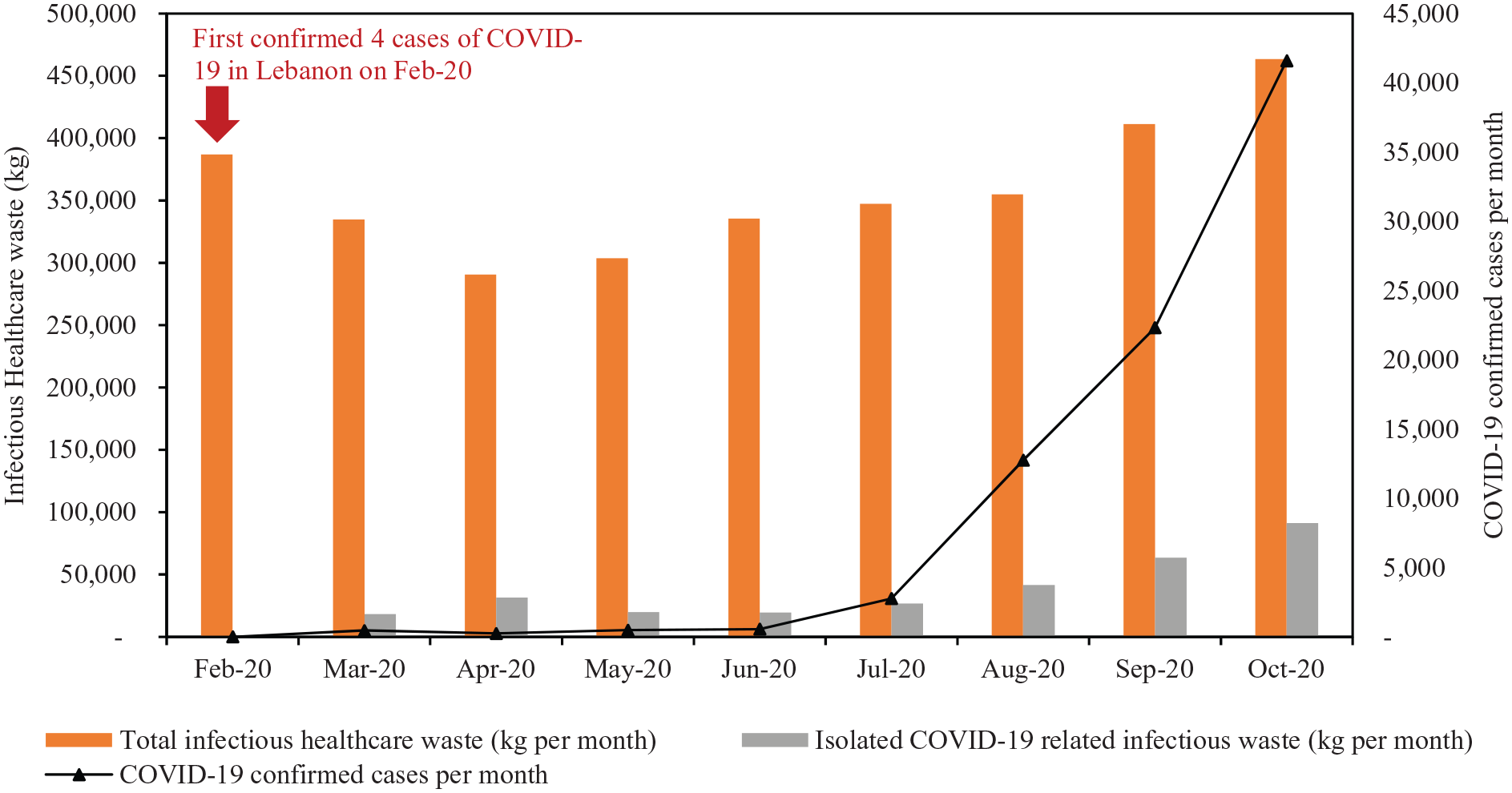
Medical waste generation with the spread of COVID-19 in Lebanon.
Figure 3 shows the monthly relationship between isolated COVID-19-related infectious waste generation and COVID-19-confirmed cases between March and October 2020. The results show that the degree of COVID-19 waste generation depends substantially on the number of cases. This result supports the observations of other scholars (Agamuthu and Barasarathi, 2020). Forecasting of COVID-19-related medical waste generated per month can be carried out using the regression model (presented in Figure 3) that correlates the number of COVID-19-confirmed cases per month with the infectious medical waste generation. This model can allow other countries, with similar context to Lebanon and with limited data availability, to make their extrapolations. Therefore, this will help them to identify possibilities to improve the efficiency of their medical waste management system and predict their associated costs.
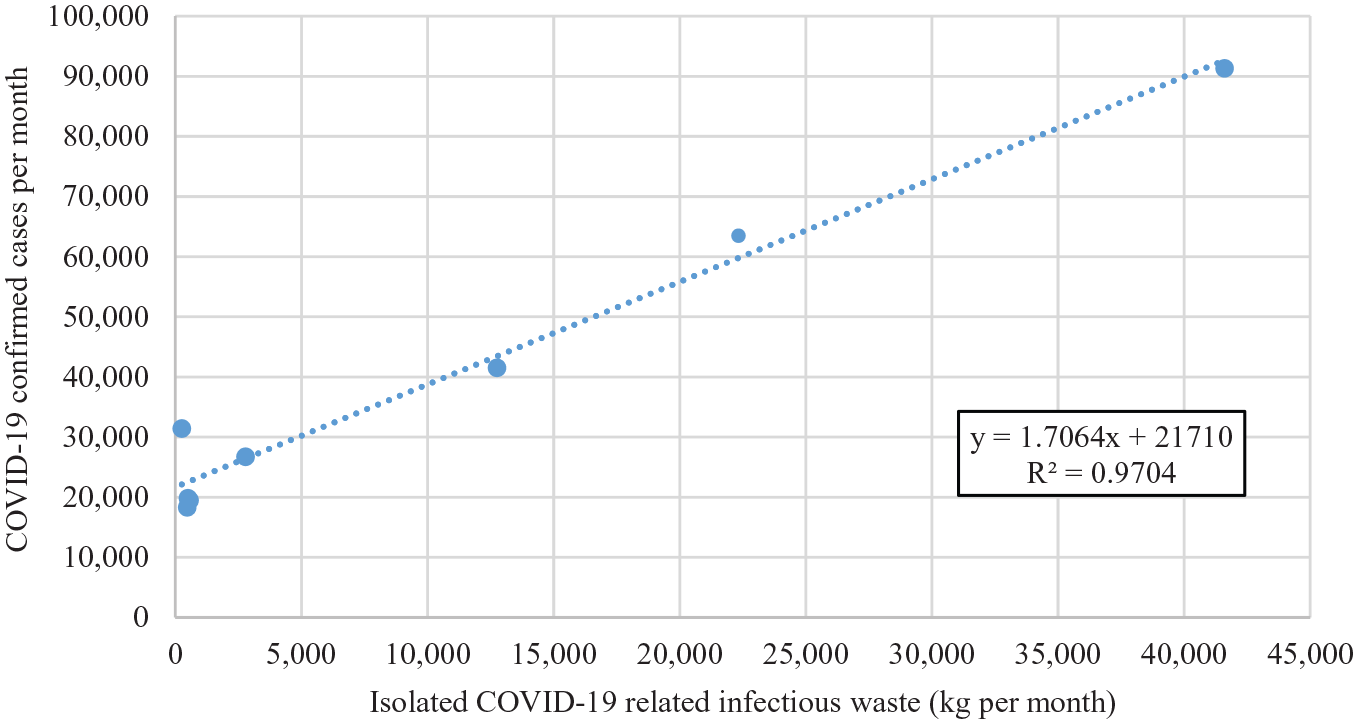
Monthly relationship between isolated COVID-19-related infectious waste generation and COVID-19-confirmed cases between March and October 2020.
The COVID-19 pandemic creates additional challenges in management of waste generated through both households (MSW) and healthcare facilities in Lebanon. Lebanon already lacks appropriate healthcare and MSW management practices due to technological, operational, economical and/or financial constraints and is particularly vulnerable during the COVID-19 pandemic, with its new risks and challenges. The challenges associated with MSW management during the pandemic mainly include the following: (a) increased amount of mixed waste including infectious waste as there is no waste segregation at source; (b) increased littering, open burning and illegal dumping of MSW, including infectious COVID-19-related waste, which are still commonly practised in many areas; (c) increased negative impacts from potential exposures to informal workers in contact with waste mixed with infectious waste such as gloves, masks and tissues; and (d) lack of daily supply of PPE to waste collectors and awareness regarding waste handling, which caused in July 2020 the coronavirus infection of 133 workers from a waste management company in Lebanon as reported by the Ministry of Public Health (Reuters, 2020). It should be noted that in Lebanon estimates on amount of household infectious waste being generated related to COVID-19 is lacking as there is no MSW separation at source (Maalouf et al., 2019). Therefore, the estimated amount of COVID-19-related waste reported in this study is only associated with waste generated through healthcare facilities and not through households.
The medical waste amount and management issues reported in this study have been focused on Lebanon. For a more conclusive understanding of better management during a comparable crisis, a comprehensive evaluation is required, taking into account wider regions, preferably worldwide.
Further recommendations
Based on the overview of medical waste management and the additional management issues raised by COVID-19 spreading in Lebanon, a set of recommendations is proposed at the country level to better monitor the COVID-19-related waste flow and the medical waste stream in general. The following recommendations provide valuable insights and key support for decision-makers:
Conduct a comprehensive survey/statistical study to determine the waste generation rates (kg per bed per day) in different regions in Lebanon while covering the various sources of generation (public and private hospitals, laboratories, PHCs, etc.) and types of healthcare waste (with special attention to COVID-19-related waste) including a wider range of indicators supported by experimental studies to determine medical waste composition data;
Maintain intensive control and monitoring of autoclave operations, hazardous waste collection, open burning and illegal dumping or incinerating activities supervised by special environmental committees with interinstitutional members, especially during the COVID-19 pandemic;
Emphasize more fully medical waste prevention and reduction as well as sorting at source, particularly for source separation of the hazardous fraction into infectious and toxic sub-fractions, because improper sorting may lead to increased amounts of infectious medical waste and thus increased costs of disposal. Therefore, healthcare institutions should further enhance their waste management monitoring system;
Put more effort in place for the enforcement and implementation of existing rules and regulations;
Provide special regulations/amendments to report data on detailed national waste statistics about the medical wastes collected, treated and disposed of monthly as well as on environmental authorization, and annual environmental performance of waste operators, which can be made available in electronic format to the general public (open data).
Conclusion
This study enables the establishment of reference values for infectious medical waste generation related to COVID-19 in Lebanon. The estimated average of COVID-19-related infectious healthcare waste per month in Lebanon is 39,035 kg or 1.3 tonnes per day, which constituted 5–20% of total infectious healthcare waste. The analysis showed that the isolated infectious medical waste has greatly increased with the increased number of confirmed COVID-19 cases, which more than doubled after August 2020, and continue to increase. However, the total infectious medical waste in 2020 has decreased in comparison with previous years due to the financial and economic crisis in Lebanon, which equally affected the implementation of an effective healthcare waste management plan. Therefore, for the first time this study has provided detailed information on the COVID-19-related infectious healthcare waste generation in Lebanon, allowing benchmarking among countries. The estimated generation rates may serve as a reference for healthcare institutions’ administrations and an alerting sign for local authorities that are controlling sorting and waste management practices. Furthermore, monitoring of COVID-19-related waste through the proposed model in this study is essential for decision-makers, particularly in developing economies like Lebanon with gaps in waste statistics, to reduce other contamination risks. The study showed that the correlation between the COVID-19 cases and the generation rate is strong. However, many factors may play an influencing role on the generation rate such as the monthly occupancy rates relative to each hospital or other healthcare institutions. Therefore, further studies are needed to assess other influencing factors, such as sorting methods and policies, financial means, quality standards, degree of awareness and perception of risk, which may vary between healthcare institutions. It should be noted that the management of COVID-19-related waste is according to existing legislation and regulations for the management of infectious waste. However, there appears to be little enforcement effort put forth at the country level.
Medical and municipal waste management services are both critical around the world, and these systems need to overcome serious challenges, particularly in developing economies. Therefore, further investigations and research studies are needed to adjust to COVID-19-related waste flows in Lebanon and other developing countries impacted at substantial levels by this pandemic.
This study provides an overview of healthcare waste management and an analysis of existing waste management policies and regulations in Lebanon while pointing out critical issues related to medical waste management. The estimated generation of healthcare waste is 1.0–1.5 kg per bed per day or about 9.2–13.8 tonnes of risk healthcare waste daily (about 3358–5037 tonnes per year). The reported infectious medical waste generation rate in this study can allow other countries, with similar context to Lebanon and with limited data availability, to make their extrapolations, which will help them to identify possibilities to improve the efficiency of their medical waste management system and predict their associated costs.
Almost 80–85% of the total healthcare waste stream collected from 150 private hospitals, 30 public hospitals, 80 laboratories, 42 dispensaries, 4 associations, 4 universities and around 200 PHCs and isolation centres is being treated by Arcenciel (a local NGO) through autoclaving. The remaining healthcare waste is either incinerated at hospitals without permits or illegally dumped with MSW. Therefore, immediate corrective actions should be taken to mitigate and prevent harm to human life, health and the environment. Finally, this study highlights some important recommendations and research needs that should be urgently tackled given the danger to human health and life raised by potential uncontrolled dumping or burning of healthcare waste.
Supplemental Material
sj-pdf-1-wmr-10.1177_0734242X211003970 – Supplemental material for Impact of COVID-19 pandemic on medical waste management in Lebanon
Supplemental material, sj-pdf-1-wmr-10.1177_0734242X211003970 for Impact of COVID-19 pandemic on medical waste management in Lebanon by Amani Maalouf and Hani Maalouf in Waste Management & Research
Footnotes
Acknowledgements
We appreciate and thank the NGO Arcenciel and Mr Mario Goraieb for providing us with the relevant information on the infectious healthcare waste management in Lebanon.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.