
Abstract
Malaysia recorded 8904 coronavirus disease (COVID-19) cases and 124 deaths as of 27 July 2020. Globally, everyday there are thousands of new cases of COVID-19 being recorded. Due to the high number of infections globally and nationwide the increase in the amount of clinical waste (CW) generation was expected. Malaysia has reported a 27% (by weight) increase in the generation of CW which was mostly attributed to COVID-19 related waste. This article presents the impacts of COVID-19 in waste generation, policy and regulation of CW management (CWM) in Malaysia and a case study on the CWM at a selected hospital used as a COVID-19 focal point. The current practice of CWM due to COVID-19 related cases follows the existing policy and legislation of CWM detailed in the Schedule Waste Regulation (2005), Environmental Quality Act, 1974, and with the standard operating procedure provided by the Ministry of Health, Malaysia. The case study conducted through survey and questionnaire interviews revealed that the CWM in government hospitals followed existing guidelines for CWM for COVID-19 waste, with some additional precautions and rules by the waste management contractors.
Introduction
Coronavirus disease (COVID-19) has been reported to first begin in December 2019 at Wuhan, People’s Republic of China (PRC) which can be transmitted by human to human (Yu et al., 2020). COVID-19 is likely a zoonotic infection, which was transmitted from an unknown animal source to humans (Abdullah et al., 2020). Since then the number of infections is increasing rapidly and has caused a global emergency. The World Health Organization announced the COVID-19 outbreak as a pandemic in March 2020, and it is rapidly spreading all over the world. The total number of cases reported globally on 27 July 2020 was 16,659,001 and the total death toll has reached 656,849 (Worldometer, 2020). The death toll due to COVID-19 is 6.2% from the number of people infected of COVID-19 (Gardner, 2020). The spreading of COVID-19 is via human-to-human transmission with an average basic reproductive rate (R0) of 2.2 meaning for each patient, 2.2 other individuals become infected (Abdullah et al., 2020).
People infected with the COVID-19 virus will experience mild to moderate respiratory illness and recover without requiring special treatment. However older people, and those with underlying medical problems such as cardiovascular disease, diabetes, chronic respiratory disease, and cancer are more likely to develop serious illness. The COVID-19 virus spreads primarily through droplets of saliva or discharge from the nose when an infected person coughs or sneezes (World Health Organization, 2020a). For now, there are no specific vaccines or treatments for COVID-19. However, there are many ongoing clinical trials evaluating potential treatments. On average it takes 5–6 days from infection with the virus for symptoms to show, however it can take up to 14 days. The COVID-19 constitute the subfamily Orthocoronavirinae, in the family Coronaviridae, order Nidovirales, and realm Riboviria. It is an enveloped virus with a positive-sense single-stranded RNA genome and a nucleocapsid of helical symmetry. The genome size of coronaviruses ranges from approximately 26 to 32 kilobases and it is one of the largest among RNA viruses. It has club-shaped spikes that project from their surface, which in electron micrographs creates an image reminiscent of the solar corona (Cherry et al., 2017; World Health Organization, 2020a).
Many countries globally have enforced city lockdowns or movement control order (MCOs) to break the chain of infection.
In Malaysia the healthcare waste is basically categorized into five main categories: clinical waste (CW); radioactive waste; chemical waste; pressurized containers; and general waste (Department of Environment, 2009). CL is waste that contains human or animal tissue, blood or body fluids, excretions, drugs, pharmaceutical products, soiled swabs or dressings, syringes, needles, and sharps – any waste that has come into contact or been mixed with any of the clinical types of waste and any waste unless rendered safe may prove hazardous to any person coming into contact with it (Department of Environment, 2009).
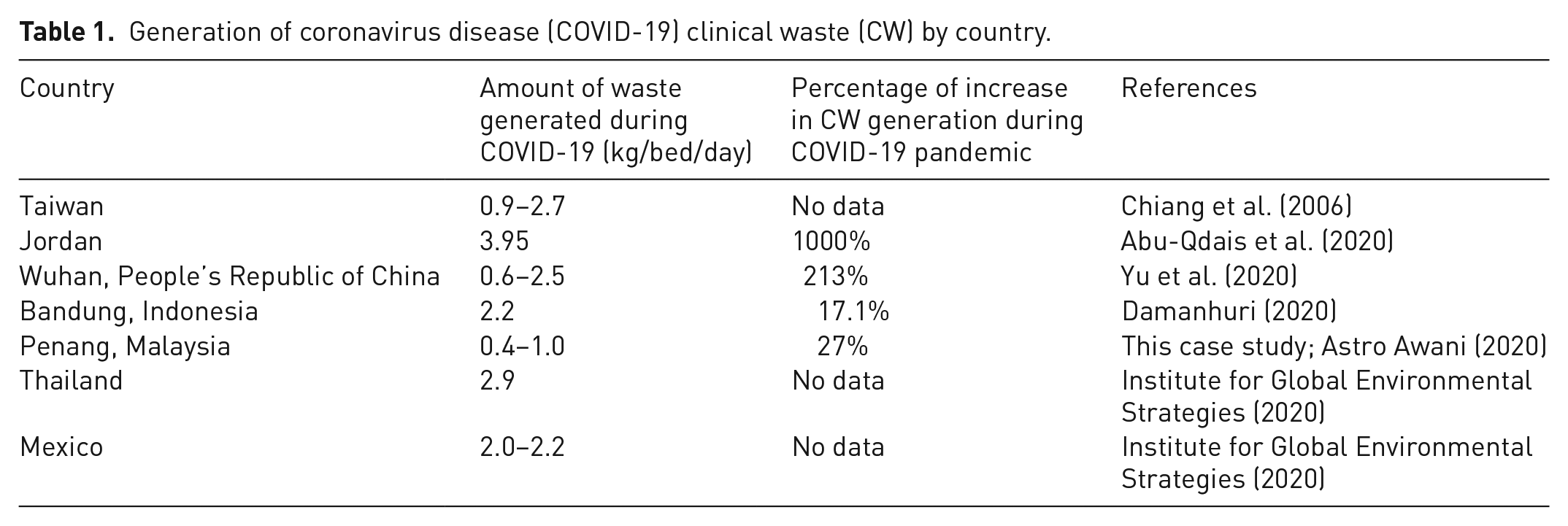
The increase in the number of infections of COVID-19 can be correlated to the increase in the healthcare waste in healthcare centres such as hospitals, clinics, laboratories, temporary quarantine centres, and research laboratories in almost every part of the world. The Malaysian government announced an MCO from 18 March 2020. The trend of new cases is increasing with more than 8904 cases and 124 deaths reported as of 27 July 2020. With the increase in the new cases almost every day and the number of tests being done the amount of CW seems to be increasing. In Malaysia alone, a 27% increase in CW is reported by the MoH following the COVID-19 outbreak. The increase is mainly attributed to the increased usage of disposable gloves, face masks and personal protective equipment (PPE) by the medical staffs (Astro Awani, 2020). The generation of COVID-19 related waste according to countries is described in Table 1. Besides that, the usage of face masks and disposable gloves by the public to restrict infection from others is also well noticed. Incidentally, improper disposal of the waste along shop lots, rubbish bins and public areas, is noticed even though there is no published article on this matter. According to the World Health Organization (2018), healthcare waste contains potentially harmful microorganisms that can easily infect other patients, healthcare workers or the general public if it is not handled and disposed of in a proper way, and this, of course, includes the COVID-19 related waste.
Generation of coronavirus disease (COVID-19) clinical waste (CW) by country.
The viable COVID-19 virus could be detected in different conditions for up to 3 hours post aerosolization; up to 4 hours on copper; up to 24 hours on cardboard; and up to 2–3 days on plastic and stainless steel (Doremalen et al., 2020; Mol and Caldas, 2020). This relatively long viability on studied materials suggests potential of the virus in wastes and therefore proper storage and disposal is necessary to avoid spreading of the virus to the healthcare workers and public (Doremalen et al., 2020; Mol and Caldas, 2020). As per World Health Organization (2020b) advice, if decontamination cannot be performed in the laboratory area or on-site on the CW, the contaminated waste must be packaged in an approved manner, for transfer to another facility with decontamination capacity. The proper management of hazardous waste from those activities becomes an area of increasing concern. Besides that, it also could spread from the healthcare facilities to the environment if there is lack of proper handling and clinical waste management (CWM). Some of the adverse effects to human health associated with CW and byproducts are as follows: sharps-inflicted injuries; toxic exposure from pharmaceutical products in particular antibiotic and cytotoxic drugs released to the environment; substances such as mercury and dioxin; air pollution arising from results of the particulate matter during incineration of CW; and thermal injuries occurring in conjunction with open burning and operation of CW and radiation burn. Disposal procedures in healthcare facilities have been proposed by the World Health Organization (2020b) such as controlled conditions of thermal treatment or use of traditional biocidal agents, which are effective in eliminating the coronavirus (Kampf et al., 2020). All CW generated from COVID-19 related patients should be collected safely in designated containers and bags, treated, and then safely disposed of or treated, or both, preferably on-site. If waste is moved off-site, it is critical to understand where and how it will be treated and destroyed. All who handle healthcare waste should wear appropriate PPE (boots, apron, long-sleeved gown, thick gloves, mask, and goggles or a face shield) and perform hand hygiene after removing the PPE (World Health Organization, 2020b). The objectives of this paper are to: -
(a) review on the policy and guidelines for managing CW during the COVID-19 pandemic;
(b) establish the CW generated and its composition; and
(c) present a case study on the CWM at Hospital Seberang Jaya, Penang, Malaysia.
Study methodology
This article is classified into two sections: to review the existing policy and guidelines for CWM in Malaysia; and another section based on a case study carried out through interview questionnaires to know and understand how the CWM related to COVID-19 is carried out.
The review of the policy is carried out using various sources from the Internet, journals, and guidelines prepared by the Department of Environment, Malaysia and Ministry of Heath, Malaysia on CW in Malaysia titled “Guidelines on the Handling and Management of Clinical Wastes in Malaysia”. The interview follows the sample questionnaires. The interviews consist of various questions which are related to CWM in hospitals and were directed to the supervisor of CWM at Hospital Seberang Jaya, Penang, Malaysia.
The list of questions directed to the hospital supervisor who handles CW in the Seberang Jaya Hospital is as follows:
Name, Contact No, Email, Place of work and role/responsibility/experiences in your organization especially for medical waste management (MWM)
Policy and institutional arrangement for MWM
(a) Policy, regulation, and plan for MWM?
(b) Any newly developed COVID-19 waste management specific policy, regulation, plan, incentives and programmes?
(c) National agency (national level) responsible for MWM.
(d) Local agency (state level) responsible for MWM.
(e) Responsible authorities for day-to-day COVID-19 MWM (municipalities or central/provincial governments?)
(f) Any discussion for technical and financial options for COVID-19 waste management in your country and/or city?
(g) Any training and awareness programme related to COVID-19 waste management in your country, city and/or facility?
(a) Number of health facilities in your part of Malaysia? (b) Number of licensed (private) waste management companies to manage medical wastes including COVID-19 waste? (c) Daily amount of all medical wastes (both hazardous and non-hazardous) generated (kg/day)? (d) Daily amount of COVID-19 wastes generated (kg/day)? (e) Any data on healthcare waste composition such ashazardous/non-hazardous, or pathology/infectious/sharps/pharmaceutical/chemical waste? (f) Number of incinerators installed in your region inMalaysia? (g) Number of medical autoclaves installed in your country, city, health facility? (h) Number of disposal sites where it could be acceptable for medical waste including COVID-19 waste?
(a) Any existing infectious MWM plan? (b) Any newly developed specific COVID-19 waste management plan? (c) CWM practices highlighting the differences between the general practice and COVID-19 specific practice, and introduction of practical treatment technologies applied for mass PPE (such as gloves, masks, coats, etc.): - source separation; - PPE; - storage at source; - transportation; - treatment methodology for medical waste in general; - specific treatment for COVID-19 waste; and - disposal. (d) New technology and alternative options for medical waste currently being discussed, pipelines and planned? (e) Awareness programme for healthcare staff and waste management companies as well as the informal sector?(f) Training for health staff? (g) Any specific practices currently implemented for COVID-19 waste management?
Results and discussion
Policy guidelines for managing CW and COVID-19 related waste in Malaysia
More than a decade ago, serious concerns had been raised regarding the potential for spreading pathogens, as well as causing environmental contamination due to the improper handling and management of clinical and biomedical waste. While full regulatory programmes and guidelines to control waste from such institutions have been introduced in most developed countries, in Malaysia, the Mistry of Health (MoH) prepared preliminary guidelines for the management of hospital waste in 1998. The MoH has published national guidelines for management of clinical and related wastes and similar biomedical management guidelines have also been produced at the state levels. This is to rationalize and recommend methods for the management of healthcare wastes within Malaysia. In addition, guidelines were drafted for the management and safe disposal of hospital wastes and the MoH produced the “Hospital Waste Management Manual,” which included detailed guidelines for handling and disposing wastes (Saw, 1994). The Malaysian Department of Environment (DOE) has formulated the Waste Pollution Prevention and Control Law and/or the Regulations on management of biomedical hazardous wastes. However, hospital waste is generally collected and disposed of together with other domestic wastes on the basis of the guidelines provided. In some of the larger states, individual hospitals have installed on-site incinerators for the disposal of CL (Department of Environment, 2009; World Health Organization, 1994). No new Policy or Regulations were enacted during the COVID-19 period. The Environmental Quality Act 1974, which is the mother Act, is being used with more recent amendments. In Malaysia, scheduled waste related to hazardous, clinical or biomedical waste is categorized into a few categories according to its contents ( Department of Environment, 2009). According to the Malaysian DOE and Ministry of Environment and Water, the national authorities that are responsible for clinical/biomedical waste management come under the Federal Government, but Local Municipal Councils are also responsible. The responsible authorities for day-to-day COVID-19 MWM are the Federal Government and DOE. The Environmental Quality Act 1974 with recent amendments is currently used in Malaysia. The biomedical, CW or any hazardous waste is listed as scheduled waste and is categorized according to Environmental Quality (Scheduled Wastes) Regulations 2005 (“Regulations”) which serves as a key legal framework that deals specifically with hazardous waste. Subsidiary legislation which falls under this are: (a) The Environmental Quality (Prescribed Premises) (Scheduled Wastes Treatment and Disposal Facilities) Order 1989; and (b) The Environmental Quality (Prescribed Premises (Scheduled Wastes Treatment and Disposal Facilities) Regulations 1989. A comprehensive framework of federal, state, regional, and local laws, licenses, and permits govern virtually all aspects of MWM processes from start to the end – including labelling and identification, on-site storage and management, transportation, treatment, and disposal – are clearly addressed in Malaysia in the form of “Guidelines on the Handling and Management of Clinical Waste in Malaysia (2009) (Ambali and Bakar, 2012).
CWM in Malaysia according to the scheduled waste regulation 2005, Environmental Quality Act 1974
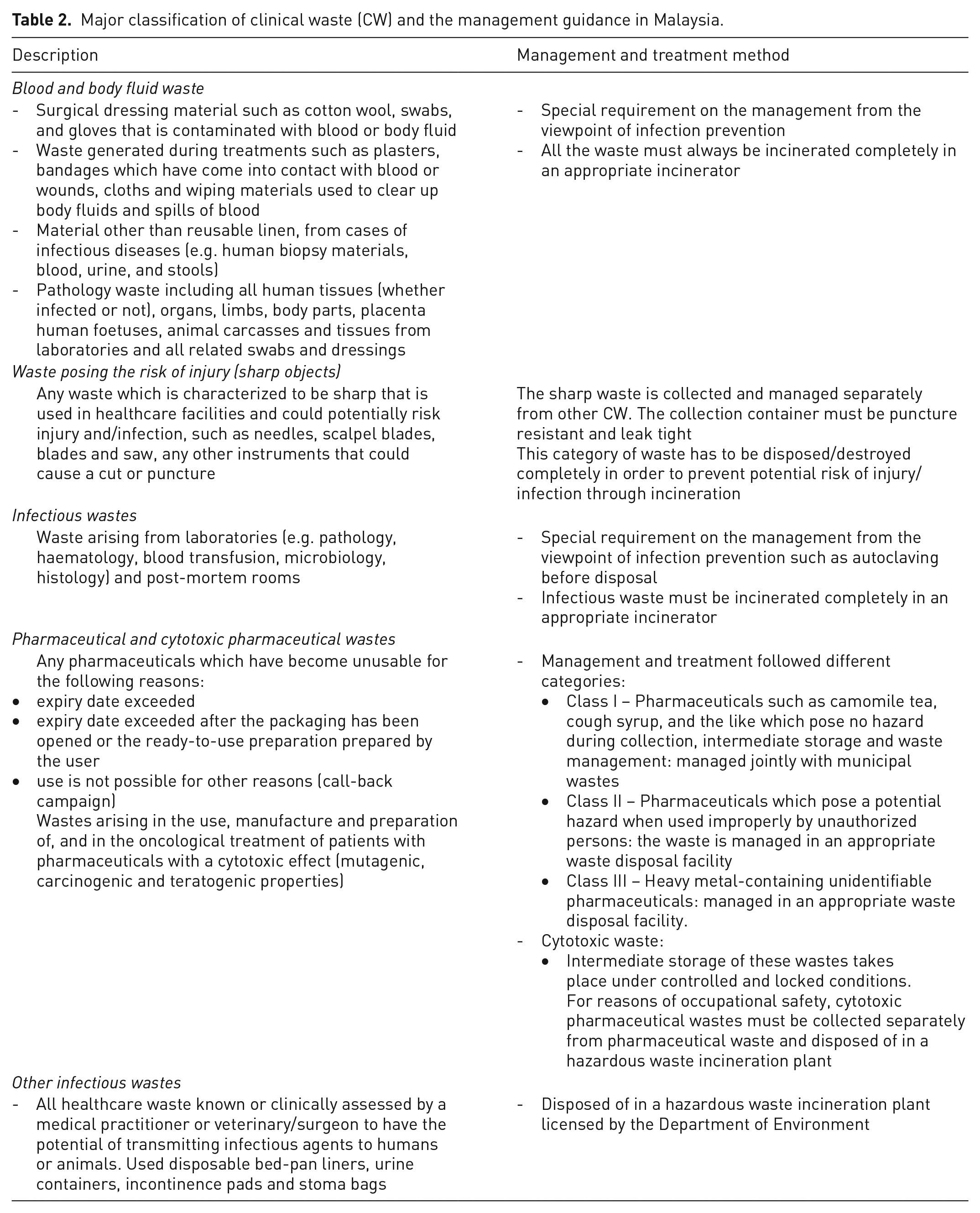
Appropriate handling and disposal of CW generated from hospitals, clinics, research laboratories or any healthcare institutions is important to avoid any adverse impacts to the public health and environment, including the handling of CW generated during the COVID-19 pandemic. In Malaysia, there are currently 144 government hospitals with 42,000 beds and 240 private hospitals with 16,000 beds which generate CW on a daily basis. CW can consist of infectious and contaminated substances, human tissue, body fluid, blood, needles, swabs and excretion drugs (Department of Environment, 2009). Further classification of CW and their treatment methods are described in Table 2. Additionally, any radioactive waste generated in healthcare facilities is sent to the Malaysia Nuclear Agency for further treatment and disposal.
Major classification of clinical waste (CW) and the management guidance in Malaysia.
The CWM guideline comprising the regulations together with specific requirements, states that such scheduled wastes shall as far as possible, before disposal, be managed properly as they could be harmful. The generators of scheduled waste need to notify the DOE of any scheduled wastes generated and keep up-to-date inventory of scheduled waste generated, treated and disposed as per regulation. Scheduled wastes may be stored, recovered and treated within the premises of a waste generator. Incineration, disposal, off-site storage, and waste generators shall conform to the requirements of the consignment note system when transporting wastes to ensure it reaches the approved destination, that this is carried out by a licensed transporter, and the treatment shall only be carried out at prescribed premises licensed by the DOE. The storage of CW must be by using durable waste containers with clear labels, and lastly the waste generators shall provide information to a transporter regarding the nature of the wastes transported and action to be taken in case of accidents (Department of Environment, 2009).
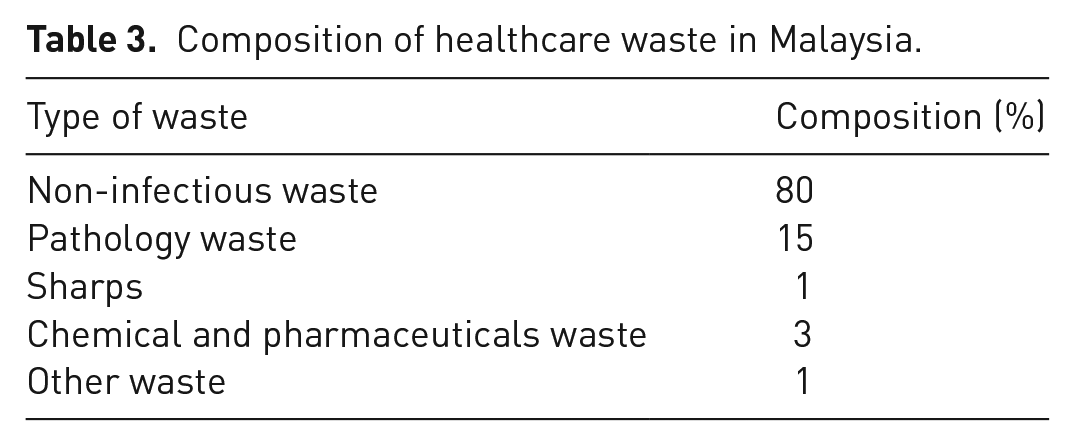
According to the DOE, from the total of amount of healthcare waste generated in hospitals, about 20% to 40% of the waste consists of CW which is potentially infectious and poses risk whereas the remaining of 60% to 80% accounts for general waste. The general waste in hospitals is defined as any waste that is generated in the healthcare facilities such as from canteens and offices and is disposed of as municipal solid waste. The composition of healthcare waste is presented in Table 3.
Composition of healthcare waste in Malaysia.
The daily generation of healthcare waste in year 2013 was 50 metric tonnes (Mt) per day and 18,000 Mt annually, and currently it is estimated that the generation of biomedical waste is 90 Mt/day or 33,000 Mt annually whereby about 75% to 80% is non-pathogenic waste (Astro Awani, 2020;Department of Environment, 2009). Based on the 27% increase on the generation of biomedical waste during the COVID-19 pandemic, about 25 Mt is COVID-19 based biomedical waste.
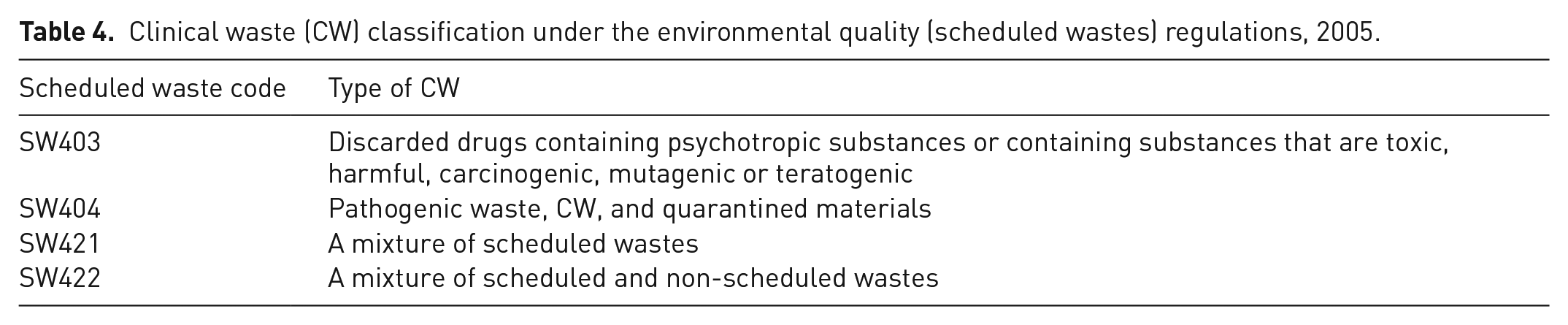
During the COVID-19 pandemic, the increase in CW generation could be from swabs, syringes, needles, sharps, blood or body fluid, excretions, mixed waste, laboratory waste, material or equipment contaminated with the virus, masks or disposable gloves, and PPE that is used for screening and treatment for COVID-19 infected personnel. The CW generated is basically classified into four different categories as stated in Scheduled Waste Regulations 2005 as described in Table 4. The amount of CW generated in Malaysia increased to 17% in February 2020 as compared to the previous month, a figure which is sourced from various healthcare facilities, hospitals, clinical and research activities (Astro Awani, 2020).
Clinical waste (CW) classification under the environmental quality (scheduled wastes) regulations, 2005.
The disposal of CW is done by separating the CW from generated waste, which, in turn, is labelled and disposed of into proper containers and bags which are then collected by the licensed contractors for disposal and treatment at 12 different incineration facilities nationwide. The waste is disposed of according to colour-coded containers or plastic bags (Zaimastura, 2005). This is in line with the Environment Quality Act (Scheduled waste) 1989 which stipulated that all healthcare establishments in Malaysia must adopt the colour coding standard in classifying biomedical waste. A blue plastic bag/container is used for CL to be autoclaved and a yellow bag is used for CL that is to be incinerated (Department of Environment, 2009). CW requiring autoclaving, or other equivalent treatment before final disposal or incineration shall be stored in light blue autoclave bags before such treatment but should be placed in yellow plastic bags after autoclave completion for further treatment by incineration. Any other general wastes generated at the healthcare facilities is disposed of in black bags. All bags and drum containers used for CW disposal must be identified at the point of generation and should be indelibly and clearly marked with a biohazard symbol. The date the scheduled wastes are first generated, name, address and telephone number of the waste generator shall be included in the container. There are seven licensed companies in Malaysia which are responsible to collect, transport, treat and dispose waste. All are private companies. These companies were originally managing CW and now that includes COVID-19 waste too. The licensed contractors for CWM in Malaysia are granted their license under the Section 18 (Environmental Quality Act 1974) regulation provided by the Malaysian DOE. Five out of seven companies are concession companies such as Radicare Sdn Bhd, Edgenta Medisure Sdn Bhd, Medivest Sdn Bhd, Sedafiat Sdn Bhd and One Medicare Sdn Bhd. These are appointed by the Malaysian government through the MoH, Malaysia to manage the CW generated in hospitals, government clinics, or medical institutes as part of the CWM system. Kualiti Alam Sdn Bhd and Future Nrg Sdn Bhd are the companies responsible for CWM from private hospitals and clinics.
Some hospitals store the CW generated at cold rooms as a temporary storage till the dedicated lorry arrives. Collection can be daily or three times a week depending on the quantity. Transportation is done only by the special lorries licensed to transport hazardous waste and these belong to the waste companies. Almost all CW in Malaysia is incinerated. The Bukit Nanas Integrated Waste Treatment Facility is the Malaysia’s first comprehensive incineration treatment plant possessing various facilities with high temperature, physical and chemical treatment. Privatization of Malaysian CWM and hospital support services in 1995, allowed regional and on-site medical waste incinerators in Malaysia (Ambali and Bakar, 2012). Most of the waste collected is incinerated and some waste may be pre-treated, if necessary, by autoclaving. Only one state (Penang) has implemented recycling of non-pathogenic waste after sterilization but this is not practised for COVID-19 related CW. All the ash from incineration of CW from the incineration plants are taken to the Integrated Hazardous Waste Treatment Centre and it is solidified with cement before disposal into the special landfill. The monitoring of CWM is done by the DOE which is responsible for all aspects of CWM from collection, transportation, treatment and disposal using an online system called Electronic Scheduled Waste System in order to be sure that the companies comply with the environmental regulations accordingly.
It is also estimated that the increase in the amount of CW could increase the cost of CWM and this will increase the overall cost since the CW quantity has increased by 27% in March 2020. A training and awareness programme related to COVID-19 waste management in Malaysia was carried out mainly on the proper use of PPE. The public was given awareness through all social media on proper sanitation and washing hands regularly. Regular periodic training is provided by the Malaysian DOE, MoH and the hospitals for their staff.
The DOE also has an additional regulation that the public are not allowed to handle and dispose of any type of scheduled waste including CW without a proper license, and those found guilty can be given a mandatory prison sentence and maximum fine of RM500,000 (115,000 USD) (Department of Environment, 2009).
Case study: current practices/response in managing medical waste during the COVID-19 pandemic at Hospital Seberang Jaya, Penang, Malaysia
This case study discussed the results of the questionnaire directed to Edgenta Medisure Sdn Bhd personnel who are responsible for MWM for COVID-19 at Hospital Seberang Jaya. Edgenta Mediserve is the national agency responsible for MWM and the interviewed personnel worked as a supervisor of the MWM unit in Hospital Seberang Jaya. According to the supervisor, the workers of Edgenta Mediserve are dealing with day-to-day COVID-19 MWM in all the government hospitals throughout Malaysia.
Characterization of the hospital
Hospital Seberang Jaya is located in Jalan Tun Hussein Onn, Seberang Jaya, 13700 Permatang Pauh, Pulau Pinang and it is a government hospital. It has a total of 12 wards and 314 beds for admission for various cases. At Hospital Seberang Jaya few places are identified and reserved as areas for COVID-19 medical waste which included the severe acute respiratory infection (SARI) ward, the emergency department, the paediatric ward and central sterile services department (CSSD).
Management of COVID-19 CW
Hospital Seberang Jaya currently has seven cleaners who help in the cleaning and collecting the COVID-19 related CW from the four different areas. Three cleaners are in charge of the SARI ward working in three shifts, one cleaner in-charge of the emergency department (observation ward, COVID-19 screening booth and decontamination room) and three more in-charge of the paediatric ward and CSSD unit. The COVID-19 medical waste is collected in the medical waste bags (yellow bags) and then labelled as COVID-19 medical waste. These yellow bags will be placed into the properly labelled COVID-19 collection bins which are well locked. Only the designated cleaners who are dealing with the COVID-19 medical waste have the access key. The collection bin will be changed daily. The collection bin with COVID-19 medical waste will be stored in cold storage while waiting for the lorry to transport it to the incinerator outside the hospital (Kamunting, Perak) on a daily basis.
Amount of CW generated
All materials used in the health procedures dealing with COVID-19 are treated as CW. The daily amount of all medical wastes at Hospital Seberang Jaya, is about 800 to 1000 kg/day of medical wastes and the COVID-19 related medical waste is about 120 kg/day. In comparison at Wuhan, PRC the generation of CW for treating COVID-19 patients ranged from 0.6 to 2.5 kg/per bed in a day for each patient (Yu et al., 2020). The medical waste generated at Hospital Seberang Jaya consists of sharps, needles, scalpels, knives, and blades. Infectious waste includes: waste that can transmit infection to human beings; waste suspected to contain pathogens such as laboratory culture, swabs, gauzes, bandages; pathology waste such as human tissue or fluid, body parts, blood, and body fluids; and chemical waste such as laboratory reagents, disinfectant or pharmaceutical waste-expired drugs.
Source separation of CW
The cleaners handling CL segregated the generated CW according to the guidelines provided by government as follows:
(a) Sharps – needles, scalpels, knives, and blades.
(b) Infectious waste which may transmit infection to human beings and waste suspected to contain pathogens – laboratory cultures, swabs, gauzes, and bandages.
(c) Pathology waste, human tissue or fluid, body parts, blood, and body fluids.
(d) Chemical waste – laboratory reagents and disinfectants.
(e) Pharmaceutical waste – expired drugs.
Separation at source includes the biohazardous waste, sharps, chemical risk and waste without associated risk, and is necessary before the waste is packaged for transport and disposal (Brazil, 2018). The CW is further classified according to Scheduled Waste Regulations 2005 as SW403 chemical and pharmaceutical waste, SW404 pathology waste, SW421 mixture of hazardous waste, and SW 424 mixture of hazardous and non-hazardous waste.
Storage of CW
All the medical waste storage bins will be stored in cold storage while waiting for transport to be sent to other sites for incineration. Those COVID-19 medical waste collection bins will be labelled and locked.
Transport and treatment of CW
Treatment of CW is important before it is disposed of in the ground due to its impacts on human health and the environment (World Health Organization, 2018). The treatment of CW could be autoclave, incineration and chemical disinfection. All the CW storage bins including the COVID-19 waste is transported by dedicated lorries from the concession contractor on a daily basis to a specific site in Kamunting to incinerate the COVID-19 waste. All the CW including the COVID-19 waste will be incinerated and the ash is disposed of after incineration. Hence, the need for incineration to decontaminate the medical waste by subjecting it to thermal destruction process at high temperature (1100–1600°C) under controlled operational conditions. The products of combustion are ash residue, water and carbon dioxide (Olanrewaju and Fasinmirin, 2019).
Training related to CWM related to COVID-19
Training is conducted from time to time in order to equip the staff with adequate knowledge and information to prevent them from contracting the infection while dealing with COVID-19 medical waste. The healthcare staff are trained on the correct technique of donning and doffing of PPE, and they are trained on the correct technique to dispose of the general medical waste and the COVID-19 waste.
PPE
Any personnel handling the covid-19 related cases or handling CW which includes the cleaners are well equipped with PPE including: 3-ply surgical masks; disposable gloves; disposable gowns; and some additional PPE such as face shields, caps, and shoe covers.
Specific practices currently being implemented for COVID-19 waste management
There are no specific practices that are being implemented for COVID-19 waste management at Seberang Jaya Hospital; however, the following practices are practised for safe handling of COVID-19 waste:
(a) Only specific Edgenta Mediserve Staff are handling COVID-19 waste in Hospital Seberang Jaya.
(b) All the COVID-19 waste collection bags are being properly labelled.
(c) All the COVID-19 waste collection bags are being placed into the collection bin which is properly labelled and locked.
(d) Only those assigned staff who are handling COVID-19 waste are allowed to use the access key to open the COVID-19 waste collection bin.
(e) On top of the usual PPE that the staff are wearing (3-ply surgical masks, disposable gloves, and disposable gowns) those who handle COVID-19 waste have to put on additional PPE such as caps, face shields and shoe covers.
Conclusion
The appropriate handling and disposal of CW generated from hospitals and other healthcare institutions and facilities are essential. This will avoid any unwanted infection and adverse health and environmental consequences as the CW possibly contains infectious and contaminated human tissues, blood, body fluids, excretions drugs, needles, and other related materials. The practice is the same for COVID-19 related waste whereby with a proper management and disposal system any unwanted infection or spreading of the virus can be avoided. In Malaysia, CWM is regulated by the Federal Government and DOE. The Environmental Quality Act 1974 with recent amendments is currently being implemented in Malaysia. The composition of CW from the healthcare facilities is about 20% to 40%. The amount of CW generated in Malaysia increased by 17% in February 2020 as compared to the previous month, a figure which is sourced from various healthcare facilities, hospitals, and clinical and research activities during the COVID-19 pandemic. From the case study it is well established that CWM and COVID-19 related management waste is properly regulated according to the Malaysian Schedule Waste Regulation (2005) under the Environmental Quality Act 1974 by the management team of Seberang Jaya Hospital.
Footnotes
Acknowledgements
We appreciate and thank the management of Hospital Seberang Jaya, Penang, Malaysia, Edgenta Mediserve Sdn Bhd and supervisor Ms Suguna Krishnan for providing us with the relevant information on the clinical waste management.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.