
Abstract
Individuals with co-occurring disorders are a difficult population to manage in problem-solving courts. Moreover, despite being one of the most clinically vulnerable and high-risk groups, many programs will not accept people with co-occurring disorders or are not designed to address their unique needs. As such, there is little research on those with co-occurring disorders in treatment courts. Our study adds to this limited body of research by presenting findings from one of only three U.S. Federal Mental Health Courts. Using a sample of 48 participants, we compared two diagnostic groups, mental health disorders only and co-occurring disorders on demographic, criminal history, and diagnosis variables. Comparison of the two groups showed a significantly higher proportion of older participants in the mental health disorder group but no other significant differences. Analysis of correlates related to successful graduation showed that despite more complicated clinical profiles, the co-occurring disorder group had comparable program graduation rates as the mental health disorder only group. These findings imply that the intensity of treatment and wraparound services mental health court participants accessed while under close supervision “leveled the playing field” for those with co-occurring disorders, facilitating their successful graduation from the mental health court.
Introduction
One would expect that most people with a mental health disorder (MHD) in the United States are treated in the community or psychiatric facilities; it is instead the criminal justice system (CJS). Indeed, jails and prisons are the largest providers of mental health treatment in the country (National Center for State Courts, 2020). For many who are mentally ill, their conditions are further exacerbated by the co-occurrence of a substance use disorder (SUD) (National Institute of Drug Abuse [NIDA], 2020a).
One response to address the needs of this burgeoning population is mental health courts (MHCs). Like their predecessor drug court model, MHCs are a type of problem-solving court that takes a non-adversarial approach, often referred to as “therapeutic jurisprudence,” where the focus is on healing and reintegration (Palermo, 2010). Currently, there are just over 600 adult state MHCs and fewer than 30 adult co-occurring disorder (COD) courts compared with more than 1,800 drug courts (National Treatment Court Resource Center (NDRC), 2023). More surprising is that there are only three federal MHCs in the United States.
In this study, we provide findings from an evaluation of the Eastern District of Pennsylvania's Federal MHC. More specifically, we examined participants with CODs compared to those with MHDs only (MHDO) on program graduation rates. The current work is essential as COD participants are considered the most difficult to manage in problem-solving courts (Barsky et al., 2021; Steadman et al., 2013), yet they often comprise the greatest numbers and pose the highest risk for treatment failure, rearrest or reincarceration, and poorer clinical prognosis (Baillargeon et al., 2010; Horsfall et al., 2009; Houser et al., 2019; Kelly & Daley, 2013; Peters et al., 2008; Torrens et al., 2012; Zgoba et al., 2020).
Literature Review
Mental Health Disorders in the Criminal Justice System
One in seven state or federal prisoners meets the criteria for serious psychological distress, with 41% reporting a history of MHD (Bronson & Berzofsky, 2017; Maruschak et al., 2021). Torrey et al. (2010) estimate that there are more than three times as many people with MHDs incarcerated in the United States than there are patients in state psychiatric facilities. This is unsurprising given that the United States has fewer psychiatric beds per capita than existed in 1850 (Snook & Torrey, 2018). The closing of these hospitals became a pathway for many with MHDs to transfer to carceral facilities, a process often referred to as trans-institutionalization (Lurigio & Swartz, 2000).
Despite the large number of incarcerated people with MHDs, Torrey et al. (2010) argues, “jails and prisons are not created to be de facto mental hospitals” (p. 9). Indeed, prisons have neither the resources nor the personnel to respond to their treatment needs (Slate et al., 2013). Estimates suggest that just over half (54%) of state prisoners with serious psychological problems receive treatment (Bronson & Berzofsky, 2017). On reentry, MHD and COD services are often fragmented and difficult to navigate (Kolodziejczak & Sinclair, 2018; Peters & Bekman, 2007) despite findings that wraparound services increase treatment engagement, improve behavioral and trauma symptoms, and reduce substance use and criminal justice involvement (Angell et al., 2014; Pinals et al., 2019; Shaffer et al., 2021; Smelson et al., 2020).
Individuals with MHDs are also at greater risk for substance use (Conway et al., 2016; Yule & Kelly, 2019). The simultaneous occurrence of more than one disorder worsens the clinical nature by intensifying symptoms, reducing treatment compliance and graduation, and increasing relapse and other adverse outcomes (Horsfall et al., 2009; Houser et al., 2019; Gallagher et al., 2018; Peters et al., 2012, 2017; Shaffer et al., 2021; Wilson et al., 2011). Moreover, COD individuals are more likely to be returned to the CJS, require crisis management or emergency room services, and remain in the community and in treatment for shorter periods before returning to prison (Houser et al., 2019; Houser & McCord, 2018; Peters et al., 2012). Thus, this population is both vulnerable and high risk.
Co-Occurring Disorders in the Criminal Justice System
Although rates vary, estimates suggest that about half of prisoners have a COD; rates are much higher than those found in the general population (James & Glaze, 2006 1 ; Peters et al., 2017). These numbers may be conservative as symptoms can vary in scope and severity (Cleveland Clinic, 2022). Moreover, impaired cognitive function, extensive symptom interaction, and limited screening instruments can make diagnosis difficult, particularly among those in the CJS (Peters et al., 2012; Sacks & Melnick, 2007). Further complicating assessment and management, those with CODs are also more likely to suffer from trauma and other comorbid issues that must be addressed as part of effective treatment planning (NIDA, 2020b; Nowotny et al., 2014).
Screening for CODs is integral to diagnostic and treatment protocols (Bureau of Justice Assistance [BJA], 2011). Although one disorder may not cause the other, it is essential that both disorders be treated simultaneously using an integrated design (BJA, 2021; Yule & Kelly, 2019). Services for criminal justice-involved persons with CODs, if they exist at all, are often disjointed and fail to respond to the dual nature of the disorders (Peters et al., 2012, 2017).
Mental Health Courts
Following the implementation of drug courts in the late 1980s, Florida introduced the first MHC in 1997. The purpose of MHCs is to “increase public safety, facilitate participation in effective mental health and substance abuse treatment, improve the quality of life for people with mental illnesses charged with crimes, and make more effective use of limited criminal justice and mental health resources” (Thompson et al., 2007, p. vii). MHCs offer a collaborative approach that relies on judges and teams of CJS professionals (e.g., prosecutors, defense attorneys, probation officers), MHD professionals, and community partners to help participants achieve success while holding them accountable for their behaviors (Marlowe, 2021; Watson et al., 2001). MHCs also employ sanctions and incentives in an effort to motivate compliance and treatment engagement (Almquist & Dodd, 2009).
An unfortunate reality, however, is that not all MHCs allow persons with CODs to participate, and they do not provide integrated programming (Peters & Osher, 2004). Indeed, Gordon (2019) argues that drug courts and MHCs often “fail to provide appropriate treatment for the multiple disorders a single individual might present” (p. 360). This is not surprising given that the effective management of COD participants presents “one of the major challenges faced by court-based diversion programs” (Peters et al., 2012, p. 801) with staff often expressing concerns about a lack of skill and training to effectively work with this population (Pinals et al., 2019). Despite these challenges, problem-solving courts must adapt their programs to address the myriad needs of this expanding population (Peters & Osher, 2004; Peters et al., 2017).
In their national survey of drug courts, MHCs, and freestanding COD dockets (N = 54), Peters et al. (2012) examined adaptations developed by these programs for COD participants. The most common was the implementation of integrated treatment designs that were more supportive and less confrontational than typical programs. They also reported more lenient responses to sanctionable behaviors and more informal and frequent judicial status hearings. Also noted was the use of community treatment partners for intensive wraparound services, peer mentors, and emergency response capabilities to address crises. COD-specific dockets were also more likely to employ a phase structure that aligns with stages of recovery, with twice the number of hours per week in treatment compared with drug courts and MHCs.
Although there has been an increasing awareness and response to COD participants in problem-solving courts, our understanding of current practices, adaptations, court processes, and outcomes remains mixed and limited (Lowder et al., 2016; Peters et al., 2012). Pinals et al. (2019) pre-and-posttest examination of a community wraparound intervention designed to meet the needs of COD offenders in an urban MHC found a reduction in incarceration, behavioral health symptoms, illegal drug use, and post-traumatic stress disorder (PTSD) symptoms among participants. Their findings suggest that support interventions within MHCs for the COD population can enhance successful outcomes. In their evaluation of an MHC with no specific COD provisions, Burns et al. (2012) reported that while there was no association between sociodemographic or clinical variables and MHC graduation, COD participants were 91% less likely to graduate than those without a substance abuse diagnosis.
As part of Lowder et al.’s (2016) examination of recidivism from an MHC, they found that COD participants had fewer jail days served pre-program to post-program compared with MHDO participants. While the authors note that their findings contradict other studies on MHCs (e.g., Cosden et al., 2005; Steadman et al., 2011), they suggest these courts may be effective for high-risk groups. Additional research to assess whether certain “MHC program elements (e.g., support services, substance use testing, length of participation) may account for such an effect” is also needed (Lowder et al., 2016, p. 124).
The Current Study
Our study adds to the literature by examining mutually exclusive and exhaustive disorder groups (MHDO and COD) in one of only three federal MHCs, Strategies that Result in Developing Emotional Stability (STRIDES). Data were collected as a part of an in-depth process and outcome evaluation, which was the first to empirically examine the outcomes of a federal MHC. The U.S. Deputy Attorney General designated STRIDES as a pilot program in response to the 21st Century Cures Act in 2016, which promoted health initiatives, including a range of CJ reform measures. As a part of this, Congress mandated an evaluation of the program to address the dearth of research on federal problem-solving courts. They wanted to determine whether this model is feasible and effective for wider dissemination in U.S. courts to fill the gap for much-needed interventions for the seriously mentally ill under federal custody. Our first aim for this paper is to determine if participants with MHDO and COD can be differentiated on a variety of background factors, criminal history, and diagnoses. Our second aim is to establish program graduation rates for those with MHDO and COD. If differences are found here, this would suggest a need for different treatment trajectories.
The STRIDES’ Program
STRIDES is located in Philadelphia, Pennsylvania, and is the only federal MHC in the northeastern region of the United States; the other two courts are situated in Utah and Missouri. The STRIDES program includes individuals with both pretrial and post-conviction statuses and is designed to integrate recovery-oriented care and support systems. STRIDES has a four-phase structure that addresses treatment requirements including treatment plan and medication compliance, and monitoring conditions including judicial review and probation officer contact. For participants with CODs, drug testing is part of each phase which may also include attendance at recovery meetings. Notably, all participants are required to establish self-reliance and social support networks to develop more prosocial lifestyles as outlined in Substance Abuse and Mental Health Services Administration's (SAMHSA) (2024) Dimensions That Support Recovery which is also included in the phase structure. Each phase lasts a minimum of three months and specifies the number of court appearances, supervision contacts, and other components.
Beyond this general structure, STRIDES is tailored to the performance history and the individual circumstances of the participant. For those who progress through the program, requirements are lessened, while those who struggle may be given additional conditions as well as support. Participants who successfully complete at least 52 weeks in the program will graduate and can earn up to a 1-year reduction in their term of supervision. Unsuccessful discharge may occur due to serious or chronic misconduct. As part of the myriad advances and setbacks that participants experience throughout the length of the program, the STRIDES team actively utilizes incentives and sanctions, imposing rewards for accomplishments and consequences for non-compliance.
The STRIDES team consists of two U.S. Magistrate Judges, Assistant U.S. Attorneys, Assistant Federal Community Defenders, U.S. Pretrial Services, and U.S. Probation Officers, and a Reentry Coordinator; community treatment providers supply the team with monthly participant progress reports, but do not meet regularly with the team. Supervision officers are required to have training to become MHD specialists. Other team members are not required to have social work or MHD backgrounds, though many have experience in these areas; in fact, one of the magistrate judges who sat on the MHC has a doctorate in clinical psychology. Although referrals to the court come from a variety of sources, the Federal Pretrial Office, the Federal Probation Office, and the Federal Defender's Office are the primary referral sources.
Method
Sample
Data were collected with the cooperation of the STRIDES team, and approvals were obtained from the University Institutional Review Board. The sample used for this study consisted of all 58 participants who enrolled in the program from its inception in 2011 through December 2020. Participants were either pretrial (n = 11) (10 of whom re-entered STRIDES after serving their sentences) or post-conviction (n = 47). All were adults (18 years of age or older) with a serious and/or persistent diagnosed MHD, which interfered with an area of social functioning (i.e., work, family, school) as defined in the DSM-IV-TR or a comparable diagnosis from the more current DSM-V (American Psychiatric Association, 2000, 2013).
Most participants were male (63.5%), African American (57.7%), and over 40 years of age (60.9%). The majority reported being single, divorced, or separated (93.8%), had less than a high school education (54.2%), and were either employed or receiving disability benefits (68.8%). Over 60% had three or more prior criminal offenses, and about half had at least one prior technical probation violation or arrest for a new offense while on probation; more than 40% had a moderate- or high-risk assessment score.
Approximately 60% of the total participants had two or more psychiatric diagnoses. The majority were diagnosed with an affective disorder, including 46.8% with bipolar disorder, 40.4% with depression, and 25.5% with PTSD. A little over one-quarter (27.7%) were diagnosed with a psychotic disorder, primarily schizophrenia. Approximately 33% had a SUD (i.e., the COD group). Among them, 15.3% were diagnosed with more than one SUD. Approximately 15% of the total sample had an alcohol use disorder, while 20.8% had a cocaine use disorder, and 20.8% had a cannabinoid use disorder.
Procedure
We employed a mixed methods approach using both quantitative and qualitative data in the larger study. Here, we focused on quantitative findings but used qualitative findings to help interpret these results. Before collecting any quantitative data, a name-id number index was established and maintained by a Federal Probation Supervisor to ensure that all data provided for research were de-identified. Pretrial and probation staff extracted information, including the Post-Conviction Risk Assessment (PCRA) 2 and the Psychological Inventory of Criminal Thinking (PICTS) 3 from participant records and input the data into a web-enabled Qualtrics® database designed for this project. Qualitative data were collected through multiple methods, including (a) systematic observations of the MHC team's pre-court meetings and judicially supervised court hearings, (b) a focus group with the MHC team, and (c) individual and small group interviews with team members.
Measures
Independent Variables
Participants who had diagnostic data available (n = 48) were classified into two diagnostic categories: (a) non-addictive MHD without a SUD (i.e., MHDO) and (b) non-addictive MHD with a SUD (i.e., COD). To further describe the COD group, the SUD simultaneously co-occurred with the non-addictive MHD (e.g., a participant with both bipolar and cocaine use disorders), and the MHD served as the primary disorder. The majority of candidates referred to the program had undergone a recent mental health evaluation; these were either completed by an independent treatment provider or had been ordered through counsel or completed by the Bureau of Prisons. Evaluations that contained a qualifying diagnosis were accepted by the court; if a recent mental health evaluation had not been completed, the court ordered a new evaluation be conducted.
Dependent Variable
Program participant outcomes can be conceptualized and measured in several ways. The approach taken here is to first consider program efficiency by examining why individuals were discharged from STRIDES. So, the questions this part of the study sought to answer were: “What proportion of participants successfully graduated the program?” and “What proportion of participants did not successfully graduate and for what reasons?”
Of the 44 participants for whom discharge status data were available (several individuals were still actively engaged in STRIDES when data collection ended), the majority (50%) successfully graduated from STRIDES, 18% had their probation revoked, 16% left the program before completion, and 16% left for other reasons. For this latter group (i.e., Other), further analyses showed that two individuals who participated during their pretrial supervision left the program because they were sentenced to a period of incarceration, and one individual left the program because their probation expired. These three cases represent outcomes that may be attributed to standard case processing; presumably, given the opportunity, they would have remained in the program. These cases, therefore, were considered successful discharges, resulting in an adjusted successful graduation rate of 57%. Two additional individuals who were discharged because they weren't regarded as appropriate for the program were removed from the analysis, resulting in an adjusted number of discharged participants of 42, yielding an adjusted graduation rate of 59.5%.
Demographic, Criminal History, and Diagnosis Variables
Demographic covariates included age, race, marital status, perceptions of being in a stable relationship, and education level. Age was a dichotomous measure (0 =≤ 40; 1 =≥ 41) as was a participants’ race (0 = African American; 1 = White Caucasian). Gender and marital status were also dichotomous measures (0 = female; 1 = male and 0 = married, 1 = not married [i.e., single, divorced, separated]). We also controlled for participant's perception of being in a stable relationship (0 = no; 1 = yes). Lastly, educational achievement was measured as a dichotomous variable (0 = less than high school; 1 = vocational, high school, or college).
Criminal history variables included: number of prior misdemeanor or felony arrests (a four-level variable; 0 = none; 1 = 1 or 2; 2 = 3–7; 4 = 8 or more); Prior juvenile or adult violent arrests, measured as 0 = no; 1 = yes; and number of varied offense types, a dichotomous measure with 0 = 1 offense type and 1 = 2 or more offense types. In addition, we controlled for violations of supervision (technical or arrests for new crimes) and poor institutional adjustment (i.e., misconduct) while incarcerated (both coded as 0 = no; 1 = yes). Initial PCRA risk level index was a three-level variable (0 = low; 1 = medium; 2 = high). Mental health diagnoses included psychosis, depression, anxiety, PTSD, and bipolar disorder; these were coded dichotomously (0 = not present; 1 = present). SUDs included cocaine, alcohol, cannabis, opioid, and polysubstance use and were coded dichotomously (0 = no; 1 = yes).
Analytic Plan
Data were analyzed in two phases and mapped to the two specific aims of the study. For Aim 1 (differentiate MHDO and COD groups), bivariate analyses compared MHDO and COD groups using Chi-square for categorically scaled variables and a t-test for continuously scaled variables. For Aim 2, identify which participant characteristics were related to graduation (unsuccessful = 0; successful = 1), analyses examined the bivariate relationships between participant characteristics and graduation. Given the small sample size (n = 48) and the presence of uneven group sizes (i.e., n = 19 for COD group and n = 29 for the MHDO group), there were concerns regarding low power. A post hoc power analysis using WebPower (Zhang & Yuan, 2018) confirmed power was indeed low at .06 indicating a higher likelihood of making a Type II error (failing to reject a false null). To overcome the power limitations, the effect size (Φ) is included for each comparison to show the magnitude of difference between groups. However, because Φ does not yield interpretable effect sizes for non-binary categorical variables, K - 1 variables were created so that a variable for each level was created with the same referent category for each (Rosenberg, 2010). For example, for the PCRA risk variable, which had 3 levels, k - 1 (3 - 1 = 2) variables were created for high risk and low risk and medium risk was the referent.
Results
Aim 1: Differentiate MHDO and COD Groups
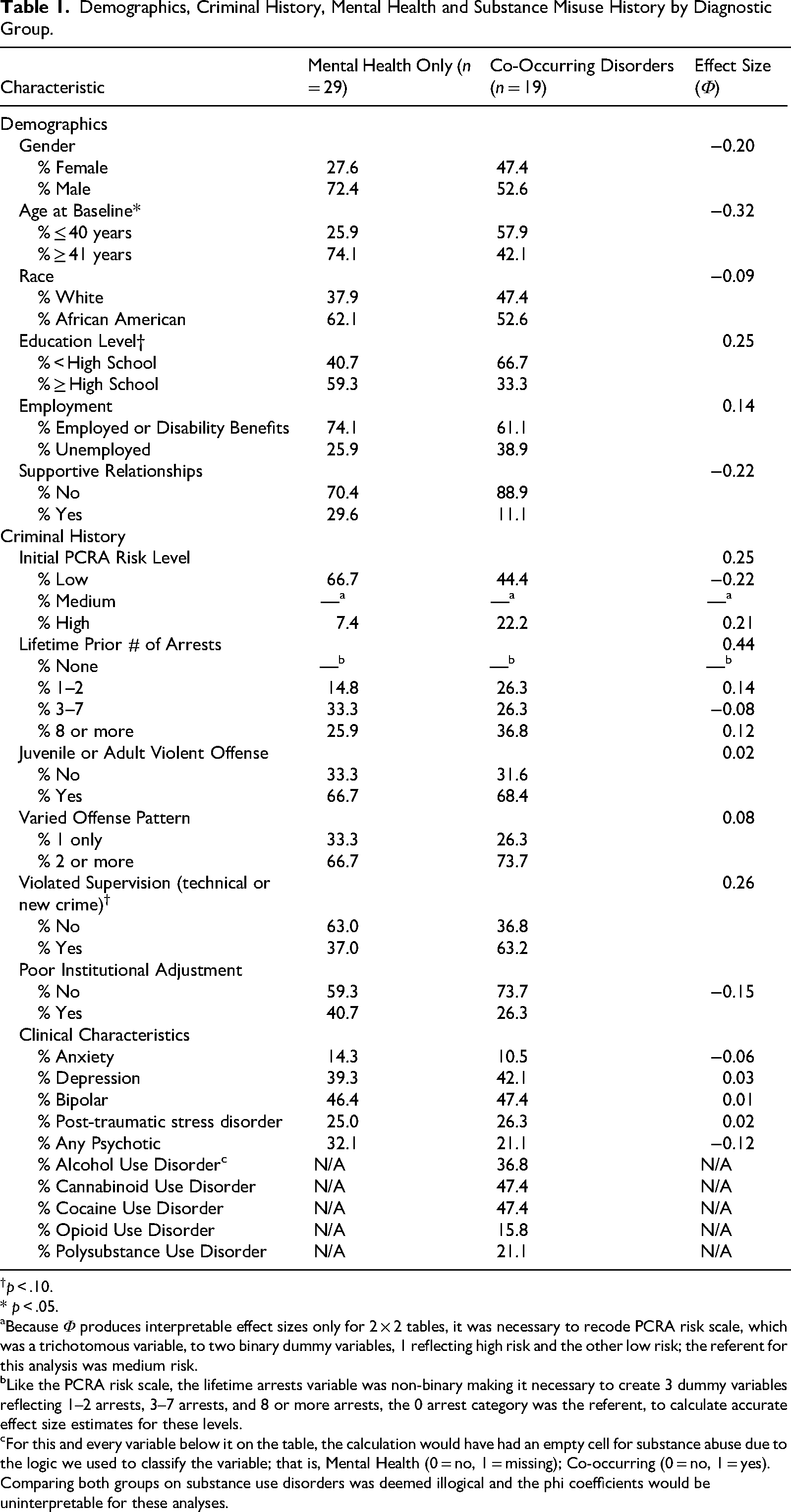
As shown in Table 1, findings indicated only one statistically significant difference in the demographic composition of the MHDO and the COD groups. The COD group had a significantly higher proportion of individuals who were aged 40 years or younger, the MHDO had a larger proportion of those aged 41 or older [χ2(1, n = 46) = 4.79, p = .029, Φ = −0.32]. A marginal difference was found in education level, with a higher percentage of the COD group having a less than high school education, 66.7%, compared to the MHDO group, 40.7%, [χ2(1, n = 45) = 2.91, p = .088, Φ = .25]. No differences were noted in the proportion who were employed nor who were in a supportive relationship.
Demographics, Criminal History, Mental Health and Substance Misuse History by Diagnostic Group.
p < .10.
* p < .05.
Because Φ produces interpretable effect sizes only for 2 × 2 tables, it was necessary to recode PCRA risk scale, which was a trichotomous variable, to two binary dummy variables, 1 reflecting high risk and the other low risk; the referent for this analysis was medium risk.
Like the PCRA risk scale, the lifetime arrests variable was non-binary making it necessary to create 3 dummy variables reflecting 1–2 arrests, 3–7 arrests, and 8 or more arrests, the 0 arrest category was the referent, to calculate accurate effect size estimates for these levels.
For this and every variable below it on the table, the calculation would have had an empty cell for substance abuse due to the logic we used to classify the variable; that is, Mental Health (0 = no, 1 = missing); Co-occurring (0 = no, 1 = yes). Comparing both groups on substance use disorders was deemed illogical and the phi coefficients would be uninterpretable for these analyses.
Comparison of criminal history variables showed only a marginally significant difference between the COD and MHDO group. A marginal difference was noted in the proportion who had a technical violation or had been arrested for a new crime while under court order with a higher percentage of the COD group having a violation or a rearrest, 63.2% compared with the MDHO group, 37.0% [χ2(1, n = 46) = 3.04, p = .081, Φ = .26]. There were comparable proportions of each group within each level of PCRA risk (i.e., High, Medium, and Low). Neither arrest history nor having had institutional adjustment problems differentiated MHDO and COD groups.
Comparison of the study groups on their diagnostic profiles showed no statistically significant differences between the COD and the MHDO group. That is, both groups had similar percentages of participants with anxiety, bipolar, major depression, PTSD, and schizophrenia/psychosis. Findings in Table 1 also present the types and prevalence of SUDs. Although not mutually exclusive, among those with CODs, there were high rates of alcohol (36.8%), cannabinoid (47.4%), and cocaine (47.4%) use disorders. Lower rates were observed for opioid (15.8%) and polysubstance use (21.1%).
Aim 2: Identify Which Participant Characteristics Were Related to Graduation
To complete this aim, a series of bivariate analyses (e.g., Chi square) compared MHDO vs. COD, and several demographic, criminal history, and diagnosis variables. For demographics, findings in Table 2 showed that female participants were marginally less likely to graduate. That is 56.3% of women and 30.8% of men did not graduate [χ2(1, n = 42) = 2.67, p = .102, Φ = .25] the MHC. There were no statistically significant relationships between graduation and race, age, or being in a stable supportive relationship. There was a marginally significant relationship between education and graduation.
Demographics, Criminal History, Mental Health and Substance Use Diagnosis by Graduation Status.
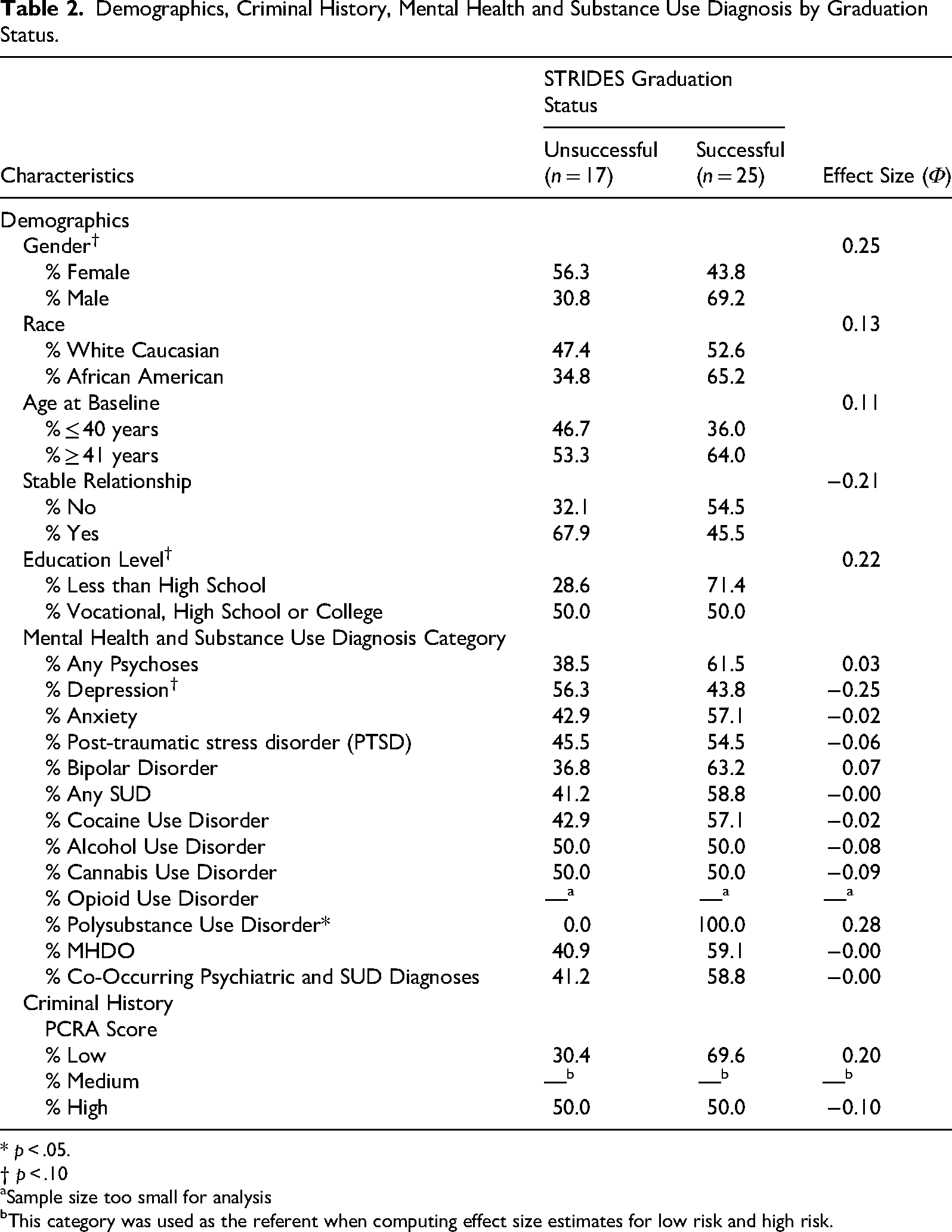
* p < .05.
† p < .10
Sample size too small for analysis
This category was used as the referent when computing effect size estimates for low risk and high risk.
Findings indicated that there was an average of two diagnoses for each group, but this was not related to graduation. Similar rates of successful graduation were observed among participants with and without psychosis, anxiety, bipolar disorder, and PTSD. As shown in Table 2, a possible trend emerged when comparing those with and without depressive disorders. More specifically, participants with a depressive mood disorder were less likely (56.3%) to graduate than graduate (43.8%) [χ2(1, n = 42 = 2.67, p = .102, Φ = −.25].
Bivariate examination of SUDs showed there was no relationship between the number of SUD diagnoses and graduation status [t (37) = .026, p = .612, d = .11]. Likewise, those who had cocaine use disorder, alcohol use disorder, cannabis use disorder, and opioid use disorder were as likely as those without them to successfully graduate from the program. Poly-SUD showed a statistically significant relationship [χ2(1, n = 39) = 3.101, p = .078, Φ = .28], with 100% of these individuals graduating successfully. In this sample, nearly identical proportions of the COD and MHDO groups successfully graduated, 58.8%, and 59.1%, respectively [χ2 (1, n = 39) = 0.00, p = .987, Φ = −.00].
As shown in Table 2, the PCRA risk score was not significantly related to graduation from the program. Findings also indicated there were no associations between graduation and the number of prior misdemeanor and felony offenses, whether one had a violent offense history, offending pattern, or institutional adjustment.
Discussion and Conclusion
Problem-solving courts emerged as a response to the revolving door of the CJS for individuals with SUDs or MHDs. Although the findings are mixed, drug courts and MHCs have generally been found to be a successful approach to reducing recidivism and other adverse outcomes (Lowder et al., 2016; Steadman et al., 2011). The problem, however, is that many offenders are diagnosed with both a MHD and a SUD (BJA, 2011; Peters et al., 2017), making them either ineligible for MHC or placed into programs not designed to address both disorders (Peters et al., 2012, 2017). Thus, the most clinically vulnerable and high-risk offenders are unaddressed or inadequately addressed, reinforcing the critical need for programs that address CODs. We know that MHCs are effective for MHDs (Gallagher et al., 2018), but there is a dearth of empirical research on the benefit of these courts for CODs. Our study expands not only our understanding of participants with CODs in MHCs but also allows us to examine this from the unique perspective of the U.S. Federal Court System.
Findings from analyses that sought to differentiate participants with mental health disorders only (MHDOs) from participants with CODs in terms of sociodemographic, criminal history and diagnostic variables revealed few relationships. Small samples led to low statistical power and to our using effect size analysis to supplement our analyses. Although not statistically significant (p ≤ .10), two variables had approximately medium-sized effect sizes; the COD group had a smaller proportion who had finished high school (Φ = 0.25) and a greater proportion who had previously violated or were re-arrested for a new offense while under community supervision (Φ = 0.26). Lack of statistical significance precludes interpretation of these two variables, but it is interesting that such relatively big effect sizes were observed. This argues for the need to pursue additional research with larger sample sizes to increase the power for detecting a statistically significant difference.
Analyses for determining correlates of graduation produced one statistically significant finding; those with polysubstance abuse disorder were more likely to graduate successfully. This finding is interesting because it suggests that despite more clinically complicated SUDs, participants benefitted from their participation in the MHC. As noted above, effect size analysis was used to supplement traditional statistics due to low statistical power. Three variables emerged with approximately medium-sized effects, including gender (Φ = 0.25), education level (Φ = 0.22), and depression (Φ = −0.25). This also suggests the need for future research to determine whether these variables will show statistically significant relationships with higher statistical power.
In terms of clinical characteristics, our findings showed that despite more complicated clinical profiles, the number and type of psychiatric disorders, the number and type of SUDs (except for poly-SUD), and CODs were unrelated to graduation. Here, the lack of statistical significance with the COD group is telling and implies that the STRIDES program levels the playing field for those with more serious clinical profiles having the same likelihood of successfully completing the program.
Findings from our process evaluation of the STRIDES program can help us to understand how participants with CODs were as likely to graduate as participants with MHDOs. During focus group discussions, team members explained that from the developmental stages of STRIDES, it was structured to be responsive to participants with CODs. As such, the MHC only partnered with programs that offered integrated treatment designs, and those with COD diagnoses were required to participate in this treatment. Moreover, Alcoholics Anonymous, Narcotics Anonymous, and/or obtaining a sponsor or mentor was required at the discretion of the court. Thus, from its inception, STRIDES “built-in” many of the programmatic adaptations that problem-solving courts recommend in response to COD participants (Peters et al., 2012), as well as recommendations delineated in The Essential Elements of a Mental Health Court (Thompson et al., 2007), which is to provide CODs with integrated treatment whenever possible.
In addition, we observed that STRIDES’ status hearings offered qualities that likely enhanced participants’ experience and outcomes. During the hearings, the judges thoughtfully reviewed participants’ improvements or setbacks, as well as asked for updates on personal issues such as family and work. The incentives for progress were plentiful and included verbal praise, certificates of recognition, and gift cards. Equally important, we noted the judge's and other team members’ efforts to fully identify the underlying “driver” of problematic behaviors. Moreover, the team endeavored to address these issues in a supportive and non-confrontational manner, using punishment-based sanctions only as a last resort. Given the more conversational nature of these interactions, it's not surprising that participants often engaged at length with the judges. In fact, STRIDES status hearings averaged 7 minutes; research suggests improved outcomes from problem-solving courts when judges spend at least 3 minutes with participants (Carey et al., 2011). Moreover, many participants who were offered a reduced number of status hearings as they advanced through the phases chose to keep attending on a more frequent basis; this suggests evidence of the supportive benefit of the court.
Similar to the findings reported by Peter et al. (2012), we took note of the many “community linkages,” that were made available to the MHC participants. Not only did the team help participants secure safe housing and employment, but they also personalized the experience, for example, by obtaining hearing aids and reinstating a work permit (i.e., a cosmetology license). Additionally, STRIDES partnered with local universities and law schools to offer pro bono advice on finances, taxes, and legal matters. Wraparound services such as these have been found to improve treatment engagement and reduce substance use for COD participants (Pinals et al., 2019; Shaffer et al., 2021; Smelson et al., 2020). Moreover, the above exemplifies the model of problem-solving courts to incorporate community resources and serve as advocates for their population (Winick, 2003).
Finally, we observed that the team supervision officers helped participants navigate therapy sessions and medical care, which was particularly critical during the pandemic when telehealth became the norm. Maintaining physical healthcare is an integral component in the totality of care for this population, as individuals with MHDs and CODs are more likely to experience comorbid chronic health conditions, including chronic pain (NIDA, 2020b). Indeed, this population is at an increased risk of self-medicating with substances such as opioids (NIDA, 2020b), suggesting the need for specialty courts to focus more attention on physical health.
The emergence of problem-solving courts was a call for a more informed approach to offenders with SUDs and MHDs as the status quo was not effective in keeping this population out of the CJS. While we have seen continued growth and awareness of these courts, we are still in the infancy stages of effectively responding to those with CODs despite their comprising a large percentage of the criminal justice population. Our findings suggest that despite the complicated clinical picture of COD offenders, they can be successful participants in problem-solving courts. As Lowder et al. (2016) suggest, these courts may, in fact, provide the intensity of treatment and wraparound services required to meet the needs of this population.
Limitations
Certain design limitations in our study should be noted. Consistent with research conducted on other federal problem-solving courts, this evaluation had the limitation of a small sample size (see Barsky et al., 2021). In addition, this was a cross-sectional sample of federal MHC participants limited to one geographic location, so caution should be exercised when generalizing the findings. This evaluation did, however, utilize both qualitative and quantitative data in a mixed methods approach, which allowed for a more comprehensive and synergistic analysis of the program. Future research to replicate and expand our findings may encourage the expansion of federal MHCs and the willingness of problem-solving courts to implement integrated treatment protocols in their design that includes collaborative partnerships with mental health and community agencies.
Footnotes
Acknowledgments
The findings reported in this paper required the collaboration of numerous individuals to whom we extend our appreciation for their contribution. We are deeply grateful for the efforts and support of the judges, reentry coordinator and reentry specialist, members of the Department of U.S. Probation and Pretrial Services, and representatives from the Federal Defender Office and U.S. Attorney's Office, without whose help this research would not have been possible. In addition, the authors would like to thank Dr. Jennifer Stanley for her contributions to this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the U.S. Attorney's Office for the Eastern District of Pennsylvania.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.