
Abstract
This article is temporarily under embargo.
• This research adds to the sparse literature on long-term care settings in Puerto Rico. • Caring for older residents and patients during and after disasters is incredibly complicated and this research adds important insights into caring for them post–Hurricane Maria.
• The need for long-term care and home- and community-based services for older adults continues to be profound in Puerto Rico, especially with increased outmigration of younger Puerto Ricans. This study provides lessons learned and identifies gaps that can be improved upon during and after future disasters. • Coordination of disaster response efforts needs to start at the local level rather than federal level to ensure older adults and those caring for them receive necessary resources in a timely way following disasters.What This Paper Adds
Applications of Study Findings
Introduction
Hurricane Maria devastated Puerto Rico in September 2017, described as the worst storm to hit Puerto Rico in 100 years. With winds upward of 155 miles per hour, the eye of the hurricane hit the island directly and decimated the island’s power grid (Halverson, 2018) which was already damaged from Hurricane Irma striking 2 weeks before (Zorrilla, 2017). A 2018 study that surveyed households across Puerto Rico post–Hurricane Maria showed that mortality rates were likely up to 70 times greater than the initial official estimate of 64 deaths (Kishore et al., 2018). A subsequent independent report in 2018 estimated nearly 3,000 additional deaths from Hurricane Maria from September 2017 to February 2018, with most of these among older adults and those in low-income areas (Project Report: Ascertainment of the Estimated Excess Mortality from Hurricane María in Puerto Rico, 2018). This is significant as the overall population of Puerto Rico in 2017 was 3.3 million (Glassman, 2019). The death toll from this report was ultimately accepted as the official death toll by Puerto Rico’s government, and the report found that those living in the poorest areas had the highest risk of dying, with older male Puerto Ricans’ risk of death 35% higher than expected (Dare Croxton, 2018).
Disasters have been occurring globally with more regularity, ferocity, and unpredictability. Simultaneously, the Puerto Rican population is aging more rapidly than almost all other countries, with 21% of the population over age 65 in 2019 (Matos-Moreno et al., 2022). Adding to complications, Hurricane Maria hit amidst one of Puerto Rico’s worst economic recessions in its history (Weiss et al., 2018). Much of the younger Puerto Rican population has been steadily migrating to the United States (US) mainland for years, further affecting Puerto Rico’s economy (Caraballo-Cueto, 2021), and the potential number of caregivers for its older adults (Laguarta Ramírez, 2018; Matos-Moreno et al., 2022; Sepulveda et al., 2018). As large swaths of young people left the island amidst dismal fiscal policies implemented by Puerto Rico and the US pre-Maria, this trend continues in the years post-Maria (Matos-Moreno et al., 2022). Physicians and other healthcare providers have also migrated to the US, which increased post-Maria (Santiago-Santiago et al., 2024) and has been partially attributed to low and delayed Medicare and Medicaid reimbursement payments (Pérez & Ailshire, 2017; Perreira, Lallemand, et al., 2017; Solomon, 2019; Varas-Díaz et al., 2023).
Puerto Rico is also at a disadvantage compared to US states, because as a US territory, funding for Medicaid is capped in Puerto Rico. Thus, once all Medicaid funds are used in a fiscal year, no further federal support is granted (McSorley et al., 2024). High poverty and unemployment rates have led to Puerto Ricans’ greater reliance on Medicaid, with about 47% of adults covered in 2021 (Park, 2022). This is relevant because for states, Medicaid serves as the largest source of long-term or nursing home care for those who need it (Davis et al., 2013). However, Medicaid in Puerto Rico has historically not covered nursing home or home health services (Puerto Rico Medicaid facts, 2022), though a 2024 memo from the Puerto Rican health department notes some long-term services and supports may soon be covered (Public Notice for Adding Home Health, Hospice, and Non-Emergency Medical Transportation Services, 2024). Most Puerto Ricans in need of long-term care (LTC) receive it in home-based settings as there is minimal institutionalized LTC infrastructure and insufficient funding to expand it (Perreira, Peters, et al., 2017). Additionally, studies have shown that older adults are especially vulnerable during disasters (Malik et al., 2018). The combination of significant poverty, high unemployment, outmigration, and lack of traditional LTC increases Puerto Ricans’ vulnerability in the face of disasters, can negatively influence their resilience, and slow the recovery following a significant disaster like Hurricane Maria.
Overall, there is very little research published to date on LTC or in-home care in Puerto Rico, nor on the impact of those living and working in these settings after a major disaster. Therefore, describing the experiences of individuals receiving and providing care in LTC settings, both home-based and in more traditional nursing homes in Puerto Rico during and after Hurricane Maria is critical. This qualitative study focuses on perspectives of individuals providing care or residing in nursing homes in Puerto Rico during Hurricane Maria, as well as individuals providing in-home LTC to individuals during Hurricane Maria. This study presents a unique opportunity to learn from the difficult aftermath of Hurricane Maria, to inform future disaster mitigation efforts and preparedness plans relating to caring for older adults, and to avoid repeating mistakes during and after future disasters.
Methods
Study Design
This study utilized a qualitative case study design (Yin, 2018) of LTC settings, both traditional and in-home, in Puerto Rico, post-Hurricane Maria. The study design was informed by the social vulnerability and health model (Thomas et al., 2013) as well as Bourdieu’s writings on various forms of capital (Bourdieu, 1986, 1998) (see previous publication for conceptual model (Haverhals, 2022)). The study was conducted following the Standards for Reporting Qualitative Research (SRQR) to ensure reliability and transparency (See Supplemental Material for checklist). The research team who conducted interviews included the author who is a gerontologist, social scientist, and qualitative methodologist with over 20 years of research experience and a research assistant fluent in Spanish with extensive qualitative research experience. The study was approved by the Colorado Multiple Institutional Review Board and VA Eastern Colorado Health Care System Research and Development Review Board #18-1809.
Sample
The sampling approach was purposive (participants were recruited from specific groups) and a convenience sample (participants were willing and available to participate) (Onwuegbuzie & Collins, 2007). Individuals providing care or residing in Puerto Rican nursing homes were sampled for this study, as well as those who provided in-home LTC privately in the home of the individuals. Nursing homes in Puerto Rico have some similarities to traditional nursing homes on the US mainland; however, they often care for fewer residents—usually around 20—and are usually family-owned and operated with some paid staff. Residents receive around-the-clock care provided by facility staff, have complex needs such as dementia and Alzheimer’s, and are often bedridden. Additionally, those sampled providing care in individuals’ homes were hired by the individual or their family. Patients receiving care in-home had complex care needs and financial means to arrange care. Individuals volunteering and working in disaster response for community or health organizations and non-profits in Puerto Rico following Hurricane Maria were also sampled.
Recruitment
Participants were recruited primarily using snowball sampling techniques, where one participant recommends others they know to participate (Small, 2009). This study is part of a larger study conducted in the Department of Veterans Affairs (VA) (Haverhals, 2022), thus initial contacts with staff at the San Juan, Puerto Rico VA Medical Center led to suggestions of participants to interview for this project. Flyers explaining the research study were also distributed in-person and via email to potential participants. No incentives were offered to participants.
Data Collection
Three semi-structured interview guides, specific to participant type (one for residents/patients; one for nursing home staff/in-home caregivers; one for volunteers or those who worked in disaster response and recovery), were created and translated into Spanish. Interview guides were designed with grounded follow-up probes (e.g., “Please give me an example” or “Tell me more about”) to encourage participants to expand on responses (Sayre & Young, 2018) and are included as supplemental materials. Data were collected from January 27 to March 14, 2019, with interviews taking place in-person at three nursing homes in three Puerto Rico municipalities (one in an urban area in the northeast with 69 residents, one in a rural area in the southeast with 20 residents, and one in rural central Puerto Rico with 20 residents), and in individuals’ private residences. One research assistant fluent in Spanish and the author conducted N = 20 interviews in either English or Spanish. To ensure trustworthiness of the data, the author was present during all interviews conducted in Spanish. The author has a working knowledge of Spanish, and asked clarifying questions as needed. Interviews were conducted during four visits to nursing homes to interview (n = 9) nursing home staff and (n = 3) nursing home residents. Participants’ roles in nursing homes included nursing home administrators, social workers, nurses, and certified nursing assistants. We also interviewed (n = 4) caregivers providing in-home care, three nurses and one family member, in their private residences, and individuals volunteering in disaster response or working in hospice (n = 4), three by phone, and one in-person in their office. The author and research assistant debriefed following each interview and home visit.
Since data collection started 16 months after Hurricane Maria, care was taken to account for recall bias. Participants often showed photos from their phones with interviewers following Hurricane Maria, which primed their memories. Interviews were audio recorded with the consent of participants, and participants were assured responses were confidential. Interviews ranged from 19 to 75 minutes. Interviews were transcribed verbatim, and two research assistants fluent in Spanish translated interview recordings from Spanish to English.
Data Analysis
An inductive and deductive approach to thematic qualitative analysis was applied to interview data (Braun & Clarke, 2006). Data was analyzed using the qualitative data analysis software Atlas.ti (Atlas.Ti, 2020). The author acted as sole coder and contacted the research assistant as needed to assure credibility and trustworthiness of the coding process (Elo et al., 2014; Morse, 1997). Deductive codes were generated based on interview guides and initially applied as a primary coding structure. Inductive codes emerged from the data to identify relevant constructs that a priori codes did not capture. Analytic memos were created to record thoughts on the analytic process and document early emergent themes. As coding finished, the author created conceptual categories to organize codes into groups. The author reviewed these code groups and used the query function in Atlas.ti to identify where codes and code groups overlapped. Outputs of the data were reviewed and summarized to determine main themes.
Results
Demographics of Study Interview Participants
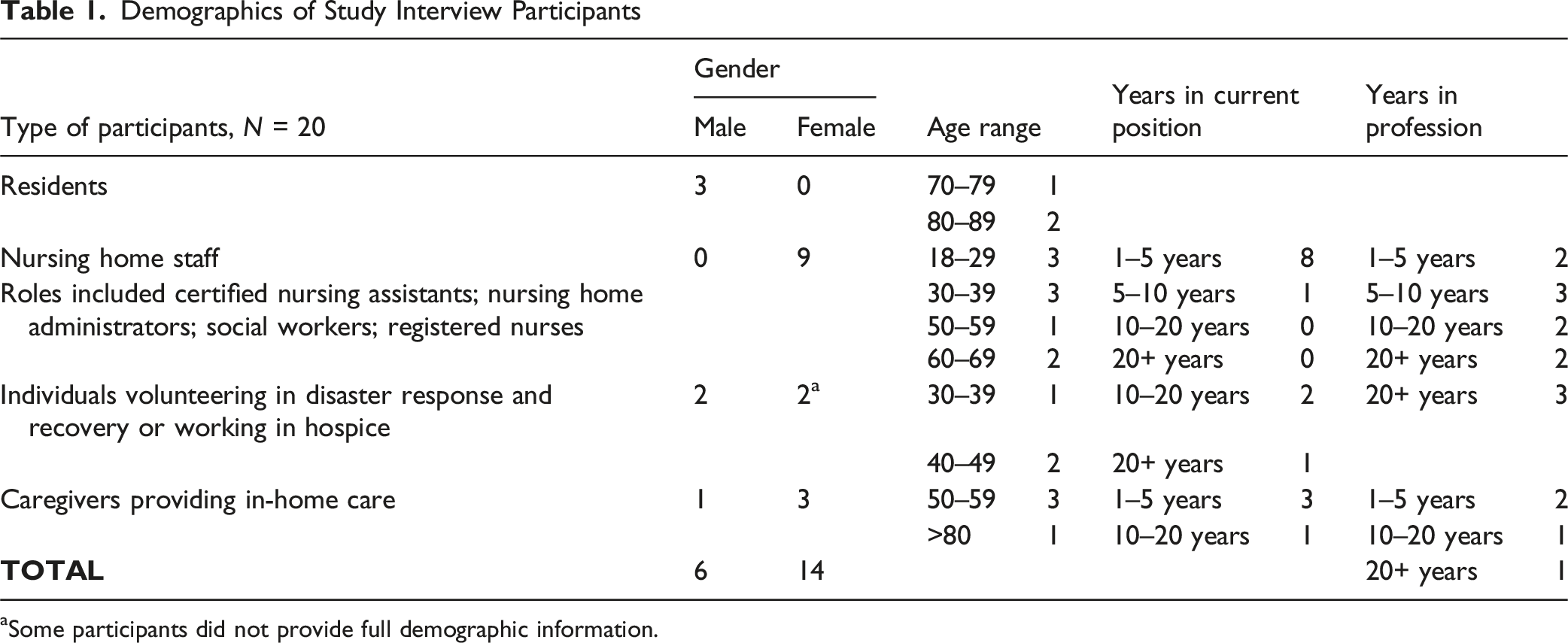
aSome participants did not provide full demographic information.
Qualitative Themes and Illustrative Quotes
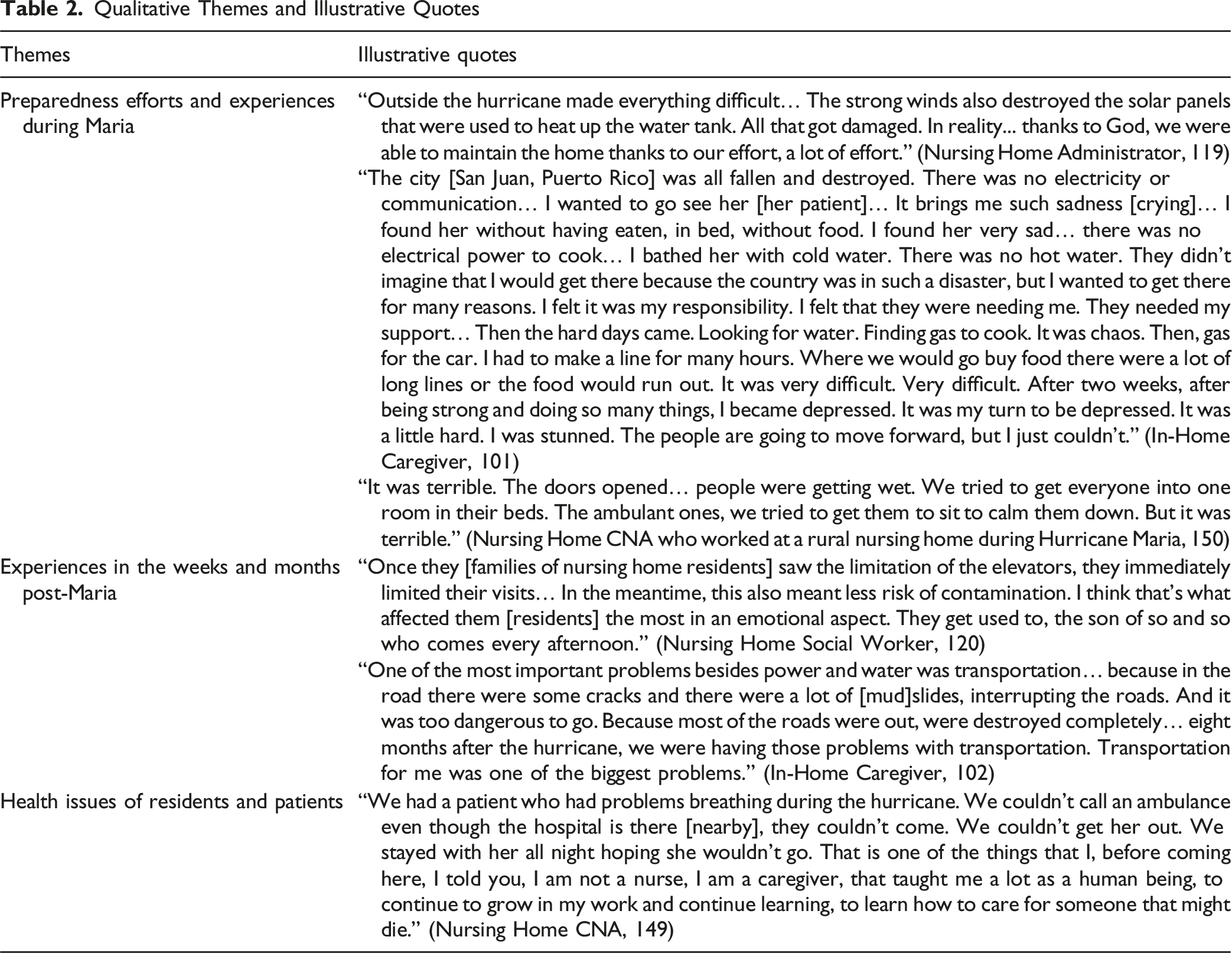
Preparedness Efforts and Experiences During Maria
Preparedness efforts were more formalized in nursing homes compared to those providing in-home care. Certified nurse assistants (CNAs) shared how they “prepared mentally” to care for residents, even though it was “very stressful” and they prayed “the whole time.” One CNA walked a half an hour after Maria to get to the nursing home because her car did not run, and then stayed for 3 days. Around 15 staff members in the urban nursing home cared for residents there during Maria, with a generator operating, providing limited power. To continually fuel it, they arranged for diesel to be brought from neighboring towns every other day, until power was restored on December 10, 2017. This nursing home only had three residents whose families removed them during Maria. One CNA described a comment from one of her residents with dementia during Maria. I was on the floor, very anxious doing the shift changes, and she [resident] gets up and tells me, “Look, honey, tell that man to stop washing the windows with the pressure washer.” It’s that the winds were so strong. (Nursing Home CNA, 149)
The smaller nursing home in southeastern Puerto Rico was well prepared with a stocked pantry, plenty of water in their cistern, and one generator. A few days before Maria, the facility physician visited as administrators were concerned about residents watching television becoming anxious about Maria. The administrators—a wife and husband—and their adult daughter who worked there stayed with residents during Maria. As the facility was concrete, they felt it could sustain the storm. However, one administrator said, “In reality we didn’t really plan much because we didn’t think it would be so destructive” (Nursing Home Registered Nurse, 131). One resident in the central region nursing home compared his experiences during Maria to Hurricane Katrina, as he had been living in Biloxi, Mississippi, when Katrina hit. He said with Maria he had some issues sleeping the first three or four days after because he was worried. I looked out the window and could see rain… Then my mind started thinking about Katrina. It was loud. I was scared. I was scared because I thought the window was going to break because it [the storm] would move it… I have a small radio. I put the news on [in the morning]. It had passed. They spoke about death, destroyed homes, lost vehicles, boats flooded. It was very strong. I started thinking more would come when I would hear just a little wind. (Nursing Home Resident, 130)
Two residents at the nursing home in central Puerto Rico said they had excellent care during and after Maria. Nursing home staff there shared that since Maria was such a long storm it was harder on residents than a faster moving hurricane. One nurse explained they had two on-property warehouses with supplies including diapers, food, and water because they were so far from any town. They also had a 25-day supply of food before Maria. Ten employees worked at this nursing home, and eight had children. Thus, they planned pre-Maria as to who would care for residents and who would be home with their families. Six employees worked during Maria, including the owner. One nurse stayed for five days before she went home to check on her own family.
One in-home caregiver spent Maria in her home, alone. Shortly after winds died down, she drove to visit one of her patients and their family. Normally a 20-minute drive, it took several hours. A lot of water had entered their apartment near the ocean, and she helped them clean up. Another in-home caregiver cared for two patients in their 90s during Maria. They decided after the hurricane it was no longer safe for them to live independently. She also took care of eight older neighbors in her apartment building during Maria, some with mobility and blood pressure issues. As the storm raged through the night, water entered hallways and the elevator, and she used a broom to try and sweep it out. She shared, The challenge was surviving… I provided refuge to others from my condo complex. I live on the 11th floor... I went up to the 18th floor to bring them down to my floor… There are people that get so anxious, that they are unable to function. (In-Home Caregiver Nurse, 105)
Experiences in the Weeks and Months Post-Maria
While LTC staff covered for each other in the weeks and months after Maria, they valued the companionship of colleagues and neighbors and described coming “together in those difficult moments.” The larger nursing home in the urban area had two small generators; thus, elevators were not powered unless they turned off all lights, and operation and weekly maintenance of the generators cost them an extra $2,100 a week: “It was an extraordinary expense” (Nursing Home Administrator, 119). They avoided moving residents to the main lunchroom and activity area when power was out and fed them in their rooms. Families were able to come as soon as a day after Maria, though visits were limited. This negatively affected residents’ psychological and emotional health. The administrator shared that when power returned, she wept, as it had been so challenging on her staff, carrying everything up and down the stairs for so long. It was a very beautiful experience, in the sense that our employees kept working regardless of what was happening in their own homes. We survived thanks to God. We give thanks to all the people that helped use during that time. After the light came back, we were we so happy. I took a weight off me. Everyone was shouting with joy. It was very beautiful. (Nursing Home Administrator, 119)
In the rural central nursing home, they gave residents sleeping medication at night and encouraged them to stay in their rooms as there was water everywhere in the common areas. They kept their generator running at night, so residents could use the bathroom: “They could fall, so we preferred for them to sleep well and go without electricity during the day. We would sacrifice one thing for another” (Nursing Home Registered Nurse, 131). After a few weeks, they bought another small generator to run fans during the day and the television to help things feel more normal.
Families soon started to arrive, and the administrator of this nursing home noted she would comfort residents’ families as they arrived crying and frustrated because of the difficulty reaching the nursing home because of the extent of Maria’s damage: “Some of them [residents’ families] were already on their way, finding their way through the trees with machetes with everything” (Nursing Home Administrator, 132). Only one resident was taken out of the nursing home by their family during Maria, which worried staff: “I was over here ready to go get a helicopter to go find her. I would ask myself ‘Dear God how is she doing?’ But two days later they brought her back” (Nursing Home Registered Nurse, 131).
At the southeastern nursing home, staff washed clothes in rivers in the months following Maria. They also bathed residents with limited water to preserve as much as possible. One resident said his faith helped him after Maria, as well as thinking about others. We have to believe in God. We have to help those in need… I learned that everyone has hardships in the world. That everyone has limitations. That you have to learn to live with those limitations. That really helped me. It took me a while to learn that. (Nursing Home Resident, 130)
The patient census increased in the 6 months post-Maria at this nursing home, as they received licensure approval and expanded to provide more services. We had a long list of elderly whose children took care of them at home, but they had no water. They saw this home as a place where their family member could be better off… They wanted to bring them here. We started noticing that the list was getting extensive. Every day there were more and more. (Nursing Home Registered Nurse, 131)
Additionally, they made some changes post-Maria. Besides adding generators, they installed a larger cistern, solar panels, and a 30-day supply of food and 3 months of water. The emergency plan, we improved it, so the employee can come even if they have to bring their kids with them. But you get here for your shift. That way you have them here and they’re not worried about their kids being out there. (Nursing Home Administrator, 132)
In the first weeks after the hurricane, one nursing home administrator shared that she would not want to have the responsibility and stress of caring for older and disabled patients during another hurricane, but her perspective changed as time passed. At the beginning I would say if another hurricane comes everyone has to take their relatives. I’m going home, and they [the nursing home residents] can go with their children. It is stressful to constantly think about what you will feed them tomorrow. Our medicine reserve started to decrease, and no one was arriving with medicine. If they don’t have medication, they are going to be unbalanced. This is going to get worse. But then people started arriving and I said, “Wait this is getting better.” Today I would pass another event here with them. I would prefer passing it with them here. (Nursing Home Registered Nurse, 131)
At the central rural nursing home, staff not present during Maria arrived in all-terrain vehicles 1 to 6 days later, sharing stories of travelling on roads that had fallen apart. This nursing home was without power for 7 months, their main power generator was damaged, and they lost their solar heater. They were building a new gazebo for residents to enjoy time outside, located where one warehouse had been blown away, and had rebuilt the warehouses larger and with cement.
One resident shared that since they were so rural, helicopters came and dropped some supplies to them, and they relied on the few neighbors they had for help. A nurse noted the owner was advocating in nearby towns for military aid, including food and water: “We couldn't keep food that needed to be refrigerated any more. So, he would go in the mornings and look for supplies… It was [a] team effort” (Nursing Home Nurse, 142). This nurse said in the future they hope to have more volunteers during such severe storms to help care for residents and manage the crisis. At this nursing home, most residents were not close with their families. This was a challenge for one nurse, as residents’ families were so detached. That is what impacted me the most… sometimes I cry because it is not just the hurricane. For us, it is always, they [the residents] need us. They pay us to be here with them. But they show us, every day, a bit of affection... could their children know that they still—many don't remember their children—but when one of their children come here, maybe it’s been six months and they haven’t come. They get here, you look at their faces and they recognize them [their children] because that smile they show. They have to know, she has to know that person is something of mine… That is what affected me that most I think. The distance, the indifference. Maybe if they were babies, they would be more affected or worried. They are not babies age wise, but they are babies in their feelings. (Nursing Home Nurse, 142)
One in-home caregiver noted that in the first few weeks after Maria, she cared for one patient at night and one during the day, and stood in long lines for food, water, and gas: “It was very difficult. Very difficult. After two weeks, after being strong and doing so many things, I became depressed. It was my turn to be depressed. It was a little hard. I was stunned” (In-Home Caregiver Nurse, 101). One of her patients eventually relocated to Florida. She also chose to leave for the US mainland a month after Maria because she had trouble accessing needed resources, sharing, “This is why I left Puerto Rico. It was a very difficult situation because you would fix one thing, but then something else wouldn’t work” (In-Home Caregiver Nurse, 101).
Added challenges were acquiring food because grocery stores were empty: “The supermarket doesn’t have a way to get the products because they are stuck at the airport, because there’s no ships leaving the US” (In-Home Caregiver Family Member, 102). This in-home caregiver provided care to his wife, and noted their condo was without power for three months and they were not permitted to use a generator; thus, they used a manual bicycle pump to inflate the air mattress his wife slept on, which took three hours every time. When power was restored, blackouts were constant. Transportation was also a challenge due to damaged infrastructure. He continued saying that it was very difficult to return to a feeling of normality post-Maria because they were living in an “environment of scarcity” (In-Home Caregiver Family Member, 102).
Some volunteering with disaster response efforts shared that disaster response was mishandled by the federal and local governments. This led to citizens’ mistrust of federal and Puerto Rican governments, and older adults in need relying on non-profits. The response wasn’t good from the federal government… people actively didn’t have water and food. They [Federal Emergency Management Association or FEMA] were talking about ending water and food services when it hadn’t even been addressed yet. So, I feel like there was so much missed communication… But they [FEMA] were taking actions that did not make any sense… Then these nonprofits really help communicate or express the means of the communities that were so isolated. So, I think, I have a new respect for non-profits. (Volunteer, 159)
Another volunteer attempting to obtain medical equipment for older and disabled patients noted that relief efforts at the federal level were complicated from issues at customs post-Maria and the overall distrust. There was this lack of help, again from the government, meaning state [Puerto Rican] government and federal government. Because federal government just sent stuff and gave it to the [Puerto Rican] government or to the big shelters or FEMA-like things, but never to these people who, were the people were actually going to need it. (Volunteer, 148)
Disaster recovery efforts were more effective when local organizations worked together, making recovery efforts a “Movement of the people from the bottom up rather than from the top down” (Volunteer, 148). Another volunteer assisting an older patient who was wheelchair bound and diabetic, and did not have electricity or promised funds from FEMA to repair his home for several months, shared that: The thing that struck me the most was that there was no help. There was no help coming from the government. What’s the point of having this island of people who are supposedly US citizens if you’re just gonna abandon them? And it wasn’t the American people who did that. It was the government. (Volunteer, 134)
Health Issues of Residents and Patients
In-home caregivers, informal caregivers, nursing home staff, and volunteers shared that residents and patients navigated many health issues. These included being bedridden or wheelchair bound, living with Alzheimer’s or dementia, diabetes, high cholesterol, feeding tubes, cancer, and being oxygen dependent. One nurse noted that most residents’ mental health was affected, “Because they didn’t know if it was day or night. Sometimes we’d take them outside, and we’d say, ‘Look, it’s day’” (Nursing Home Nurse, 142). Communication was described as the most significant challenge by almost all participants. One nursing home resident noted he felt “really down” until some communication was restored. Some of the changes that I found affected me. It took away my stamina. I didn’t have strength. I didn’t have energy. I didn’t have… it’s like I lost interest. Once we could start communicating through radio and television, things changed. I had a time when I was down. Really down. (Nursing Home Resident, 130)
An in-home caregiver who moved to the mainland US arranged care for her remaining patient in Puerto Rico with another caregiver she knew well and trusted; however, the patient died a few months later. The lady I was taking care of, who loves me a lot. Her husband visits me [still]. He loves me a lot. I left another nurse in charge… so she could take care of her… after I left, she passed away. She was stable, but there were no oxygens tanks, the doctor didn’t go see her, and she herself got depressed. Her daughter told me that when I left, she said “I have nothing left… my caregiver left.” And she died. (In-Home Caregiver Nurse, 101)
This patient had been very sick and bedridden for many years, but the caregiver noted, “I think there were too many problems which caused her to go faster. She went too fast because there were too many problems in Puerto Rico” (In-Home Caregiver, 101). The husband of this patient noted that it was difficult to treat his wife’s pressure ulcers, and he had called an ambulance four times in the two months post-Maria. His wife had problems swallowing and bronchitis; thus, they had to find ways to puree her food without electricity. She was also in terrible pain from the tumor on her spine. He said her doctor visited her one month after Maria, because the doctor’s office was destroyed by Maria: “He [the doctor] knew [she] could pass away if he don’t come because of the problem with her breathing. He knew that. He knew after the hurricane the risk was double or triple without electricity” (In-Home Caregiver Family Member, 102).
An executive director of a home hospice agency shared that many of their patients lived in rural areas. They visited their patients within three days of Maria, as it was critical to get them medications. It was complicated. One of the things that we did was we advanced medical supplies, we doubled the supplies to patients… we advanced two week’s supplies, food, diapers, all that was advanced so that if the suppliers were delayed, their service would not be affected. (Hospice Executive Director, 160)
An in-home caregiver who was finishing nursing school went out with the military and other students to older adults’ homes for three months post-Maria. These patients were mostly bedridden and many homes were without roofs. She took them water and food, addressed physical health issues, bathed them, and cared for many with depression. Talking to patients proved critical as they had been so isolated since Maria: “People needed to talk. They were like, ‘Oh, we finally see other people’. They felt good to see people. Because they had not seen others. There were people that were alone [until] we had arrived at their homes” (In-Home Caregiver Nurse, 139). She noted that many worried they would run out of medications: “Elderly people, their first meal is the medications. That is what maintains them” (In-Home Caregiver Nurse, 139). She treated many with breathing difficulties, as she specialized in that field since her husband had ALS and been on mechanical ventilation for many years. She knew of some complex patients, including one with leukemia, who moved to the mainland US for treatment after Maria, staying there. I think many people died throughout the hurricane… from frustration. For example, the anxiety... to be able to get their medications. Diabetic people. If you don’t have insulin [you suffer]. There are patients that have psychological issues. I think there is still the panic that exists due to the hurricane. (In-Home Caregiver Nurse, 139)
Discussion
This study captured experiences of older adults, nursing home staff, in-home caregivers, and others who provided care to older adults during and after Hurricane Maria, sharing their experiences 16–18 months post-hurricane. Hurricane Maria has and will continue to have lasting impacts on Puerto Ricans and those connected to Puerto Rico, especially as disaster response was slow, government mistrust was high, Puerto Rico has significant health inequalities, and older Puerto Ricans have significant health disparities compared to older adults on the mainland US (McSorley et al., 2024; Padilla et al., 2022; Rodríguez-Madera et al., 2021). With Puerto Rico’s rapidly aging population and the continual and steady outmigration of younger people to the US mainland, meeting LTC needs today and in the future for older adults remains highly lacking (Peterson et al., 2021; Robbins, 2025). Because there is not traditional LTC infrastructure and not enough home health services (Dixit & Rivera‐Hernandez, 2023), many older adults needing LTC and home- and community-based services go without or rely on friends and neighbors for help and support. Combined with increased threats of future disasters, Puerto Rico’s colonial status, high poverty, and significant infrastructure issues, older adults needing LTC level services are especially vulnerable (West, 2023).
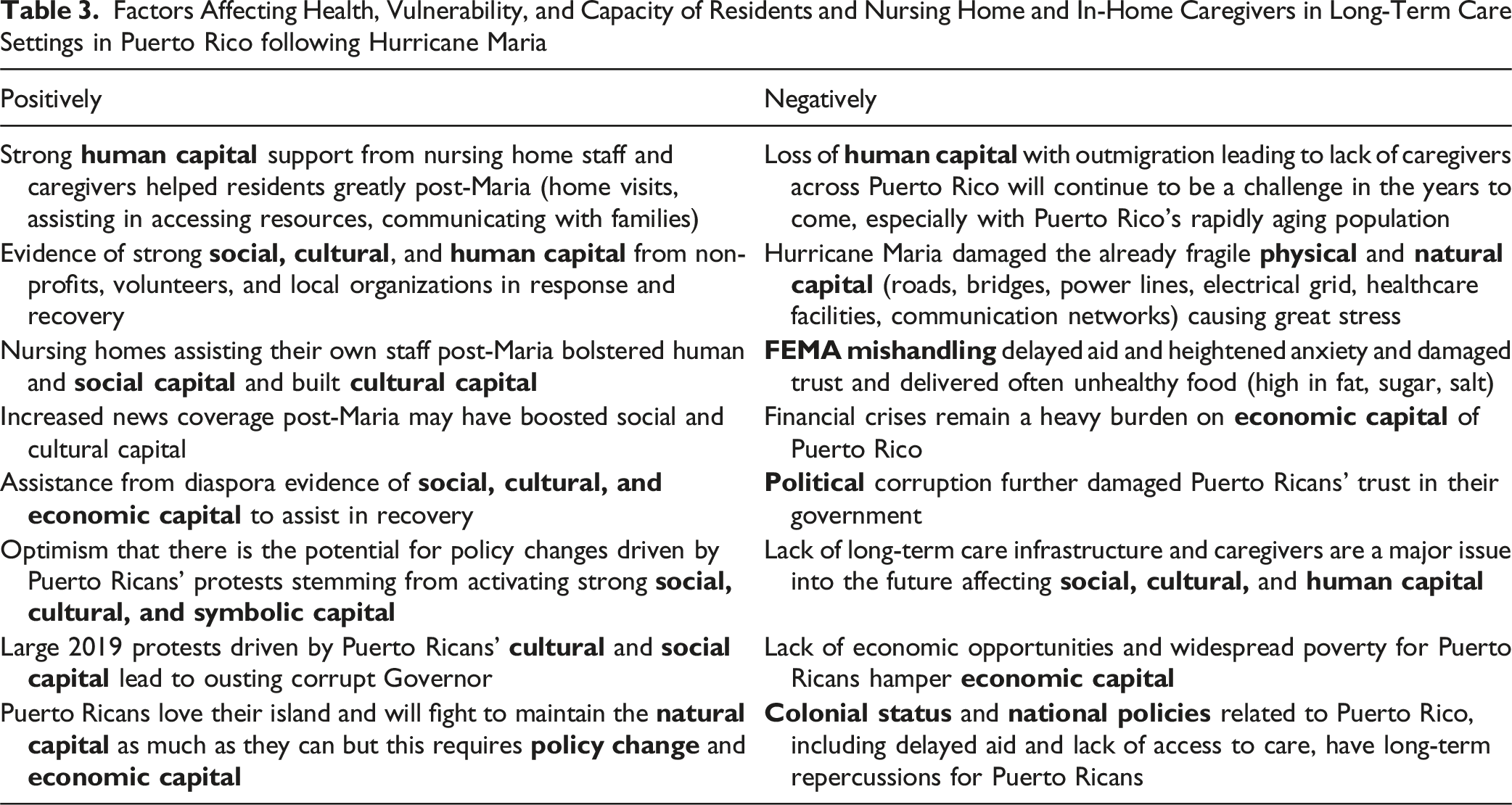
Factors Affecting Health, Vulnerability, and Capacity of Residents and Nursing Home and In-Home Caregivers in Long-Term Care Settings in Puerto Rico following Hurricane Maria
The long-term physical and mental healthcare implications from Maria are beginning to be reported (Buckley & Burnette, 2023; López-Cepero et al., 2022; Schwartz et al., 2024). In this study, all participants described feeling depressed, stressed, and anxious, and recent research on older adults in Puerto Rico also reported similar findings (Santiago-Santiago et al., 2025). These stressors led some individuals to leave Puerto Rico, and almost everyone interviewed knew people who had moved following Maria. Continuing to live in such high levels of uncertainty has been shown to negatively impact health, especially of older adults (Parker et al., 2016). The fact that many older adults reside in rural areas adds to challenges (Andrade, Jula, et al., 2023; Straub, 2021). A 2021 Rand Corporation report outlined health and social services needs pre-and post-Maria, including courses of action to address many challenges, which if implemented could lead to positive change (Chandra et al., 2021).
Finally, Puerto Rico’s colonial status, history of unreliable receipt of federal government aid, and navigating corruption are well documented and additional hindrances preventing citizens to thrive (Haverhals, 2022; Martin & Pace, 2025; Robinson et al., 2023). Studies like this one provide important insights into how to better support older adults and those who care for them, including their reliance on neighbors, families, and community-based organizations post-disaster (Andrade, Barrett, et al., 2023; Engelman et al., 2022). The reality of the rapidly aging population and lack of LTC providers and healthcare providers in Puerto Rico remains a challenge (Pleasant & Jespersen, 2024). Until these problems are specifically targeted, Puerto Rico’s older adults remain highly vulnerable not only during and after future disasters but in their day-to-day lives.
Limitations
This study is limited by a small sample of 20 nursing home staff, in-home caregivers, informal caregivers, LTC residents, and disaster response individuals. To ensure a more comprehensive picture of LTC and in-home care in Puerto Rico, a larger study should be developed. Additionally, involvement with local communities and older adults to design such studies would be advantageous. Finally, interviews were conducted at one moment in time, and designing a study that is longitudinal in nature will allow for more insights related to implications of Hurricane Maria, and subsequent disasters, on Puerto Rico’s older adults, nursing home staff, and in-home caregivers.
Conclusion
The importance of disaster preparedness in Puerto Rico’s LTC and in-home care settings cannot be understated. Lessons learned must shape future preparedness, recovery, and response efforts. The reality of Puerto Rico’s colonial status and economic fragility, leading to decades of citizens living in poverty with systemic social vulnerabilities among fragile infrastructure, played an enormous role in Maria’s devastation of the island and its recovery (Caraballo-Cueto, 2021; Guerra Velázquez, 2022). The continued outmigration of young Puerto Ricans while older citizens remain will be a continued challenge. As disasters increase, the hope is research like this will help prevent some of the devastating consequences of future disasters. Future studies might address healthcare inequities and vulnerabilities of older Puerto Ricans, and their care providers, through engaging the large Puerto Rican diaspora, healthcare providers, researchers, government agencies, and older adult advocates to cultivate creative solutions to better support the in-island aging population. Ultimately, Puerto Ricans may continue to rely on various forms of social and cultural capital to navigate major disasters like Hurricane Maria.
Supplemental Material
Supplemental Material - The Impact of Hurricane Maria on Puerto Rico’s Long-Term Care Settings
Supplemental Material for The Impact of Hurricane Maria on Puerto Rico’s Long-Term Care Settings by Leah M. Haverhals in Journal of Applied Gerontology.
Supplemental Material
Supplemental Material - The Impact of Hurricane Maria on Puerto Rico’s Long-Term Care Settings
Supplemental Material for The Impact of Hurricane Maria on Puerto Rico’s Long-Term Care Settings by Leah M. Haverhals in Journal of Applied Gerontology.
Supplemental Material
Supplemental Material - The Impact of Hurricane Maria on Puerto Rico’s Long-Term Care Settings
Supplemental Material for The Impact of Hurricane Maria on Puerto Rico’s Long-Term Care Settings by Leah M. Haverhals in Journal of Applied Gerontology.