
Abstract
Background
Nurse practitioners (NPs) and physicians are essential to providing acute, episodic and palliative care in long-term care (LTC) homes and preventing unnecessary hospital transfers.
Objectives
To explore the attributes of effective NP–physician collaboration in LTC and identify barriers to developing it.
Methods
An exploratory qualitative study was conducted using semi-structured interviews with 10 NPs and six physicians practicing in LTC homes in Ontario, Canada. Recruited individuals were not matched NP–physician dyads. Data were analyzed using inductive thematic analysis.
Results
Two distinct NP–physician practice models emerged: one characterized by successful collaboration, and the other by failed partnership. Findings are presented in the form of vignettes illustrating key differences between the models. Successful collaboration featured resident-centered care, non-hierarchical relationships, and clearly defined roles. Barriers included lack of trust, high NP workload, and role ambiguity.
Conclusion
NP–physician collaboration can improve care for LTC residents. Successful implementation requires clear communication, role clarity, and leadership engagement to support NP integration and foster effective interprofessional relationships.
• This study reveals how NPs and physicians overcome interpersonal, organizational, and systemic barriers to build effective collaboration in LTC, demonstrating adaptability and shared commitment to resident care. • It offers practical insights into how collaborative practices are enacted, informing more effective implementation and policy design to strengthen interprofessional care in LTC settings.
• The findings underscore the importance of intentional efforts to develop collaborative relationship from NPs and physicians • The study emphasizes the need for leadership engagement and structural supports to sustain collaborative models. • The findings provide a framework for further exploration of successful development of NP–physician collaboration models that enhance care quality in geriatric populations.What This Paper Adds
Applications of Study Findings
Background
The evidence is consistent on the positive impact of nurse practitioners (NPs) in timely access to care for residents of long-term care (LTC) homes, increasing staff’s capacity and morale and the overall quality of care (McGilton et al., 2022). NPs rose to the challenge during the COVID-19 pandemic in providing medical care to LTC residents when healthcare rationing prevented their transfer to hospitals (McGilton et al., 2021, 2022; Vellani et al., 2021). Post-pandemic, there is a call to optimize the role of NPs in LTC homes in a sustainable fashion in light of residents’ increasing complexity (Frank et al., 2021; Morley et al., 2022) and preexisting scarce supply of primary care and geriatric physician workforce (Drummond et al., 2022; Duong & Vogel, 2023; Frank et al., 2006). However, recruitment of NPs is not a panacea, and increased efficiency and effectiveness of care in LTC homes require successful implementation of NP–physician collaborative practice in addition to implementing policies and strategies to retain NPs. Poor collaboration between NPs and physicians serves as a barrier to effective care for LTC residents (Kaasalainen et al., 2007).
Using a scoping review methodology, we examined the structures, processes, and outcomes of NP–physician models of care in LTC homes (Haslam-Larmer et al., 2024), and the nature of their collaboration (Haslam-Larmer et al., 2025), guided by the Structured Collaborative Practice Model (Way D, 2000). Key enablers of effective collaboration included shared goals, mutual respect, clearly defined roles, and open communication, supported by strong leadership and enabling organizational policies. These findings underscored complexity of NP–physician collaboration due to interpersonal and structural factors. The specific strategies and behaviors that differentiate successful from failed collaboration remain poorly understood. Given the expanding role of NPs in LTC homes, there is an urgent need to examine how collaborative practices are enacted to inform more effective implementation of NP role and to optimize resident outcomes. This study aims to deepen understanding of the factors that shape effective collaboration between NPs and physicians in LTC homes. The insights generated may have wide-reaching implications for improving provider satisfaction and enhancing outcomes for residents, families, and staff. Accordingly, we sought to address the following research questions: 1. What are the attributes of an effective NP-physician collaborative practice in LTC homes? 2. What are the key challenges in developing collaborative practices between NPs and physicians, from both professional perspectives?
Methods
Given the limited literature on this topic, the study employed an exploratory generic qualitative research design. Generic studies are theoretically interpretive studies interested in how people understand their experiences (Merriam & Tisdell., 2009). An exploratory generic design was used as it provides methodological flexibility to gather participants’ perspectives and generate thematic understanding of the NP–Physician collaborative practice in LTC homes. Generic approach helped us acquire rich descriptive insights capturing participants’ perspectives in everyday terms. Ethics approval was obtained from the University Health Network Research Ethics Board (REB#22-5284) prior to the study activities.
Participants
Study participants were recruited via emails sent out by organizations with NP and physician members in Ontario, Canada: Nurse Practitioners’ Association of Ontario [NPAO] representing NPs, Ontario Long-Term Care Clinicians [OLTCC] representing physicians and NPs working in LTC, Ontario Long-Term Care Association [OLTCA] representing private and municipal LTC homes, and AdvantAge Ontario representing not-for-profit homes. The email contained a recruitment letter outlining the study purpose and eligibility criteria. Individuals were eligible to participate if they were trained as an NP or a physician and had experience working with a physician or an NP in LTC, respectively, and who were interested in talking about collaborative relationships between physicians and NPs. The final sample size was determined based on the principle of information power and saturation, where no new themes emerged from successive interviews (Malterud K, 2016).
Data Collection
Using a semi-structured interview guide, study participants were invited to reflect on their collaborative practices (see Appendix A). The guide was pilot tested with a non-participating NP working with older adults. It was modified based on their feedback before using it with the participants. Informed consent was obtained electronically through REDCap from all participants before their interview. All interviews were conducted via telephone by the research coordinator (RC) [AK], with experience in qualitative methods. Interviews occurred between February and June 2023, were audio-recorded, and lasted for 1 h on average. In addition to the interview, study participants were asked socio-demographic questions. Individuals who participated in the interview received a $50 e-gift card.
Data Analysis
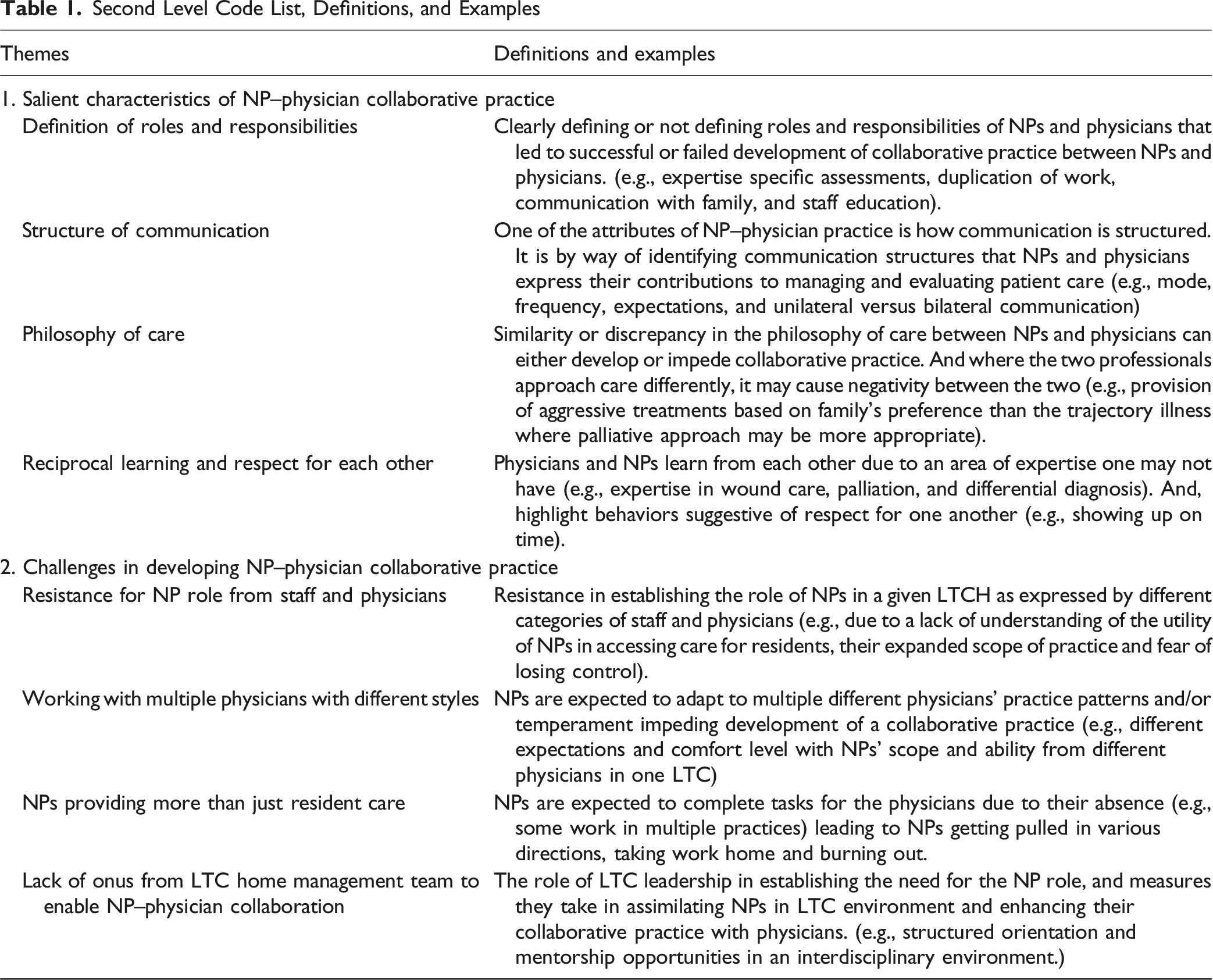
Second Level Code List, Definitions, and Examples
Results
Demographic Characteristics of Study Participants
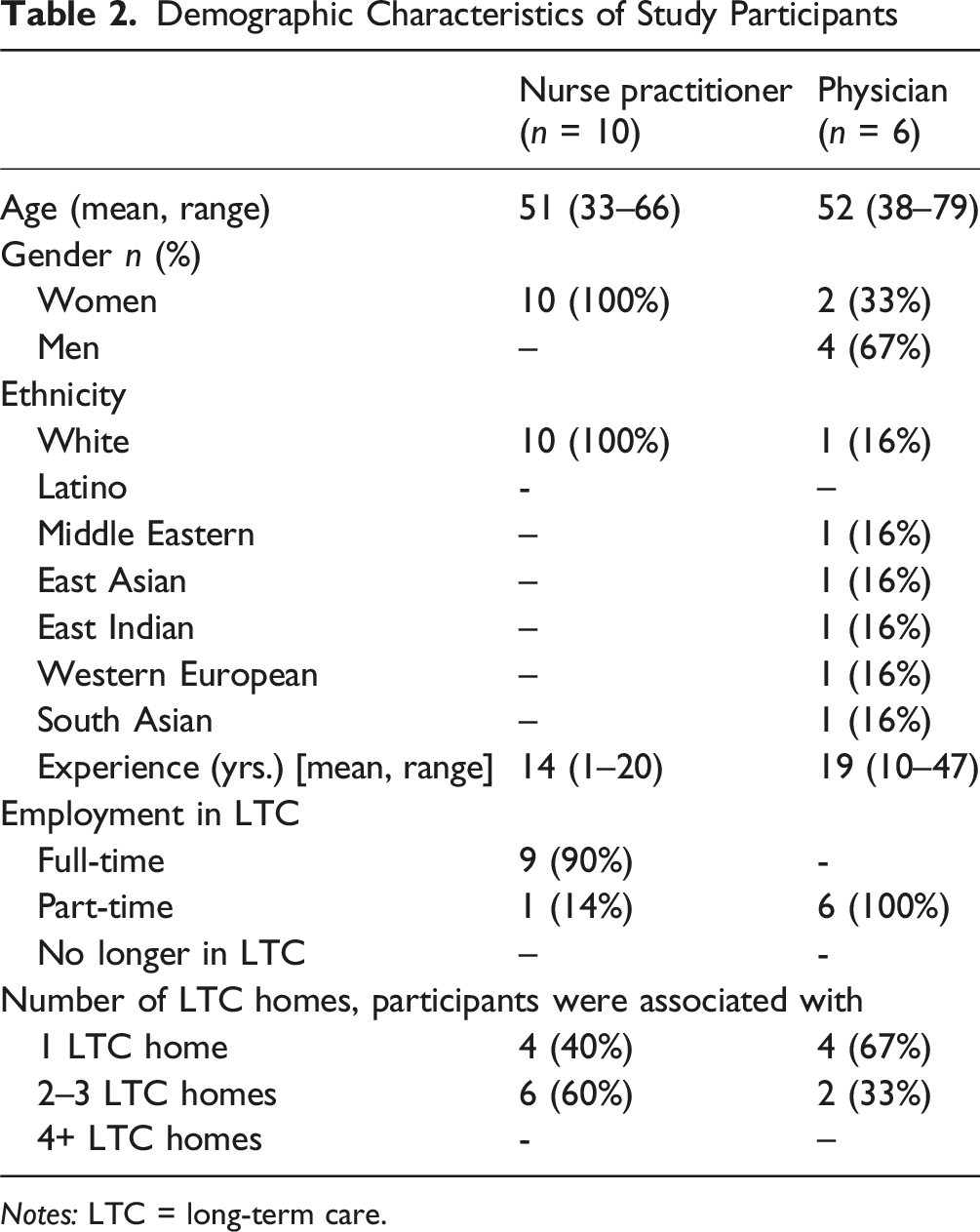
Notes: LTC = long-term care.
Participants articulated similar reasons for implementing the NP role in LTC homes: access to a full-time provider on-site to address residents’ medical needs; education to LTC staff; and participation in leadership and quality initiatives. Two divergent models of NP–physician partnership emerged, which are presented below in the form of two vignettes.
The first model was characterized by the successful development of a collaborative practice between NPs and physicians. In contrast, the second model was characterized by a failure to develop collaborative practice including situations where there was no reciprocation to collaborative effort. Vignettes are compared according to two categories derived from our findings: (1) salient characteristics of NP–physician collaborative practice and (2) challenges in developing NP–physician collaborative practice. Under each category, the findings are further divided according to sub-themes (see Table 1 for themes and their definitions).
Salient Characteristics of NP–Physician Practice Models
Four areas were repeatedly highlighted by the participants that either led to a successful or failed development of a collaborative practice. These included: definition of roles and responsibilities, structure of communication, philosophy of care, and reciprocal learning from and respect for one another. Each of these characteristics is described below in the context of successful versus failed development of NP–physician collaborative practice:
Definition of Roles and Responsibilities
In the first vignette, clearly defined roles and responsibilities was the most frequently cited element in developing a successful NP–physician collaborative practice. Successful development of the NP–physician collaborative practice involved articulating each other’s roles and responsibilities at the outset and appreciating that it will evolve and strengthen over time. One physician explained, “We’re not there at the same time. So, we had to make sure we didn’t duplicate each other’s roles. So really, just having clearly defined roles and responsibilities helped to overcome those barriers” (18 Physician).
For some, collaborative agreements served as a starting point in clarifying roles and responsibilities based on the regulatory requirements. Spending time together in the practice environment, taking time to re-evaluate roles and collaborative agreement over time, and learning about each other’s interests, expertise, and work style also helped build seamless collaboration. Some physicians described that due to NPs’ presence in the LTC home, they are able to participate in more challenging aspects of patient care while also see a larger number of patients, which would not have been possible otherwise.
Conversely, vignette two describes a failure to develop an NP–physician collaborative practice. One of the prime reasons was neither professional sought or offered the opportunity to discuss their role aspirations and expertise. One NP compared their past collaborating experience with the current job at an LTC home, “…the workload falls on me sadly, rather than it be a collaborative. Which often leads to ‘Oh did you notice this?’ or ‘Oh did you notice that? Let’s discuss this’ or ‘Let’s work on making this one better’” (14NP).
Poor role definition also led to duplication of work and inefficient use of resources. Hence, a failure to learn about one’s expertise, roles, and responsibilities served as a barrier to developing an NP–physician collaborative practice.
Structure of Communication
Participants in vignette one highlighted open and bilateral communication as a major facilitator in building a collaborative practice. There was a sense of trust in NPs’ clinical skills and legislated scope of practice. At the same time, NPs reached out to physicians when they needed to discuss clinical matters. One physician explained, “I think that you really need a high functioning team who’s willing to be flexible, willing to accept feedback, really good at communication, I mean that’s the formula for any kind of successful intervention in long-term care” (19 Physician).
Participants had established means and frequency of communication such as through scheduled in-person rounds, communication binders, phone, and text messages and how to access each other in urgent situations. Many alluded to open communication that also involved sharing ideas and reaching mutual consensus on various issues, for example, in matters related to complex clinical management, such as wound care, end-of life planning and/or situations involving ethical and moral distress. One physician noted, “…if we hit a bump at some point and you’re stuck, or you think you’re gonna get stuck, let me know we’ll talk it through” (11Physician).
Where there was failed development of NP–physician collaborative practice, participants either lacked opportunities to discuss clinical concerns or NPs were expected to excessively communicate with the physician. NPs described over-communicating to prevent the physician from feeling skeptical about them and to develop a good working practice. There was also a sense of nervousness about NPs’ knowledge base and ability to make clinical decisions impacting residents’ outcomes. One physician explained, “We have to know what they don’t know … if they don’t talk to us, then we don’t know what they don’t know and they can be making dangerous decisions without us knowing” (07 Physician).
Some NPs also shared their inability to engage in verbal discussions with physicians as they preferred texts or emails due to their busy schedules while some physicians noted that open communication was important but that in-person presence of both NPs and physicians is a duplication of service.
Philosophy of Care
A similar philosophy of care served to be a major factor in developing the NP–physician collaborative practice. For example, participants highlighted that integrating a palliative approach to care in providing resident-focused care helped flourish their practice, as comments by this physician illustrate: I have to highlight that most of the NPs I've worked with in long term care, like palliative care and that kind of person-centred care was always a strength of theirs and that is something I really enjoyed in my role as a medical director. (08 Physician)
Participants in vignette two described that having different values in caring for LTC residents negatively influenced building collaborative relationship. One NP described: If you’ve got a physician who … would do aggressive management because the family wanted that but there was not that conversation to say what that would look like and that’s where I struggled with some of the physicians. (04NP)
Participants appreciated the reality of having different values and approaches in dealing with situations but these led to conflicts. NPs spoke about the inability to move their plans of care forward if the Physician did not agree with the approach to care.
Reciprocal Learning From and Respect for Each Other
Participants in vignette one also identified that being open to learning from one another and respecting each other’s viewpoints were important characteristics in developing a successful collaborative practice. Participants identified that they could not possibly know everything, but they discussed the plan of care in a rational and evidenced-informed manner. One NP noted, “My doctors are learning how to think like a nurse. And we learn how to think like a doctor. So, then you both move a bit toward each other, and I think it gets better” (03 NP). Participants highlighted the importance of skill building through providing and accepting feedback and respecting their time and ability for clinical decision-making in addressing resident concerns.
On the contrary, participants in the second vignette displayed a lack of openness to learn from each other and respect each other. Some participants challenged the idea of NPs being independent practitioners because they are trained differently than physicians resulting in difficulty identifying a list of differential diagnoses. One physician explained using an example of a rash that NPs order broad diagnostic tests when, “… a physician can look at it and say, well it is not number 1, or 2, or 3, or 5, but it could be 7, 8, 9 and it’s probably one of these things, so let’s just order one test to confirm it” (08 Physician).
Many NPs shared their perception that despite years of experience, it took many months to years of proving their abilities for a physician to respect NPs’ clinical decision-making and competence. Disregarding NPs’ time was also highlighted as a source of disrespect, leading to failed development of NP–physician collaboration.
Challenges in Developing a Collaborative Practice
This theme describes major challenges in establishing a successful collaborative practice between NPs and physicians in caring for LTC residents. Five areas were prominently emphasized: (1) resistance for the NP role from staff and physicians, (2) working with multiple physicians with different styles, (3) NPs’ providing more than just resident care, and (4) lack of onus from the LTC leadership to enable collaboration. Participants who successfully established collaborative relationships described how they navigated these challenges. The following sections explore each challenge in the context of both successful versus failed development of NP–physician collaborative practice.
Resistance for the NP Role From Staff and Physicians
Participants shared a range of perspectives where some did not experience resistance for the NP role from the outset, some experienced resistance in the initial phase of NP role implementation, while others were unable to effectively implement the NP role leading to conflict and loss of NP. Resistance was displayed by physicians and other staff. It also involved a lack of appreciation and acceptance of the expanded scope of NP practice. In vignette one, participants described overcoming resistance through education about NPs’ scope and role in uplifting resident care; and NP role advocacy by medical directors and other physicians. One NP shared their experience: For the most part, the nursing leadership was on board but then other people on the leadership team didn't understand what that role was and why would they use this chunk of money to hire another clinician when they could hire three PSWs (personal support workers). So, Once I got into the home and met everybody, all of that kind of went away. (05NP)
Participants who successfully developed NP–physician collaborative practice also noted that accepting the role of NPs led to exemplary care for their residents. On the other hand, participants in vignette two described that some physicians would not want NPs to be involved in their residents’ care making it difficult to establish collaboration. “I’ve also seen sometimes physicians will literally tell an NP that they don’t want the NP to be involved, and they can manage things on their own. And that’s not ideal. Right?” (21Physician). In these situations, if the LTC leadership team hired an NP without input from their physician, “It starts out with a conflictual relationship right off the bat” (05 NP). Many NPs reported resistance to their role through restricted scope of practice. While most physicians were aware of the NP scope, some remained reluctant to fully embrace it, citing perceived legal responsibility and the need for oversight.
NPs Working With Multiple Physicians With Different Styles
Several participants identified working with multiple physicians in one LTC home, which posed a variety of challenges in developing a collaborative practice. One physician noted “I think it takes time … when there are so many different physicians—like 8 different personalities, it is not funny, it is pretty tricky to get that buy-in sometimes” (07 Physician). Participants in vignette one were able to build a collaborative practice despite challenges related to having multiple physicians at one site. NPs expressed the importance of being aware of different physicians’ views on the treatment of various conditions, so they can emulate their style of work for a better collaboration on resident care. Physicians in vignette one expressed their appreciation for having an NP to collaborate with while also describing NPs’ ability to work efficiently with multiple physicians. As such, participants in vignette one were able to develop a collaborative relationship but NPs served to be the major driver for developing and sustaining collaboration.
Conversely, participants in vignette two described challenges in building NP–physician collaborative practice due to having multiple physicians in one home. NPs described a sense being pulled in different directions to stay abreast of different routines, practices, and temperaments of physicians. Participants described that each physician in the group may impose different expectations for NPs, for example, “he only lets me clean ears and that was it” (01 NP); and some may feel “threatened” (16 NP) by the clinical decisions NPs made. One NP shared their frustration, “so for some of the physicians who may feel that I am imposing instead of proposing, you have to learn to almost dance around that,” (16NP) to provide for residents’ medical needs.
NPs Providing More Than Just Resident Care
Most of the participants alluded to physicians’ overreliance on NPs and NPs heavy workload in LTC homes. As advanced practice leaders, NPs are expected to engage in staff education, and other quality improvement initiatives. Clinically, they provided medical care for acute, episodic and emergent issues, in addition to their expertise-based care such as wound care and palliative care. In the wake of challenges associated with heavy workloads, participants in vignette one managed to develop collaborative practice over time. Many talked about boundary setting, for example: There are parameters - I will not do physicals ... I’ve been in the industry for over 25 years and I know exactly where the gaps are and how the NP role could fit in and really demonstrate a resident-focused care approach. (16 NP)
Physician partners in vignette one displayed appreciation and respect for the NP role in LTC and described their efforts in working collaboratively by developing processes for care and communication to prevent NPs’ burnout.
Conversely, participants in vignette two demonstrated difficulty building a collaborative practice because of a high degree of reliance on NPs to perform the tasks expected of physicians. This led to a further increase in the already unrealistically heavy workload of NPs due to a growing complexity of residents and regulatory requirements placed on the LTC sector. Some physicians expressed there are physicians who like to spend more time in their other practice settings knowing NPs will address concerns experienced by their residents and “she’s basically putting out fires” (07 Physician). Some NPs described physicians delegating their regulatory tasks to NPs, for example, admission physicals and “all the episodics and the chronics. One physician, I always leave his physicals for him because otherwise he would almost see no one ever” (09 NP).
Overall, overreliance on NPs and their heavy workload lead to job dissatisfaction and in many cases, NPs moving on to other positions in community or acute care settings.
Lack of Onus From LTC Home Leadership to Enable NP–Physician Collaboration
The role of leadership was positioned as a critical component in establishing the NP role in LTC care. However, it can also present challenges in establishing and enhancing a collaborative practice between NPs and physicians. Many participants in vignette one identified their leadership team as the enabler for collaboration. One NP articulated: I think the support from the administrator, and director of care, especially comes in before the NP comes, talking about that role, what it means, how it’s going to benefit the home, the staff, the residents. So that when you do come in it’s almost like a celebration. (05NP)
Leaders were also important in inculcating respect for NPs and advocating for collaboration among staff and physicians. Participants who successfully developed a collaborative practice identified leaders as mediators in strengthening NP–physician collaboration. Leaders did this through facilitated discussions to help identify mutually agreeable processes and solutions between NPs and physicians, “I think that’s part of the role of the medical director, the nursing director of care, plus the executive director, the administrative team as well—its part of their role to work as a mediator in a sense” (07 Physician).
Conversely, participants in vignette two experienced challenges in developing a collaborative practice where the LTC home leadership team was not actively involved in NP role implementation and assimilation in LTC. One NP explained the importance of leadership team clearly articulating the need for the NP role and the frustration when it is not done well: I think it needs real clarity - what do they want from this role (NP). Is everybody including the medical director on board with that? It's getting old after all these years to have to keep fighting the fight. It shouldn't be. I mean we contribute a huge amount to the residents and we also contribute to the physicians, whether we like it or not, makes their life hugely easier. (09NP)
New NPs were faced with conflicts with staff and physicians because leadership failed to introduce the role prior to bringing the NP on-board. Participants also noted a lack of mentorship opportunities for a new NP leading to failure to retain them. Participants in vignette two also identified that administrators and directors of nursing had heavy responsibilities related to LTC regulations and operations; hence, they did not have time to be involved in enhancing NP–physician collaboration. As such, participants highlighted the critical role of LTC home leadership in the development of a collaborative practice between NPs, physicians, and all categories of staff.
Discussion
We completed an exploratory qualitative study involving NPs and physicians working in LTC homes to examine how they envision working in a collaborative practice, the attributes of an effective NP–physician collaborative practice, and common challenges in establishing collaboration. Four characteristics were repeatedly highlighted by the participants that either led to a successful or failed development of a collaborative practice. These include definition of roles and responsibilities, communication structure, philosophy of care and reciprocal learning from and trust for each other. Examination of challenges in building a successful collaborative relationship revealed four common areas: resistance for NP role, working with multiple physicians with different practice patterns in one setting, NP’s heavy workload, and the role of LTC leadership in establishing NP role and fostering collaborative relationship.
To meet the complex care needs of LTC residents, the healthcare system must continue to adapt and identify innovative models of care where clinicians can practice at their full scope and leverage their specialized knowledge and skills. The NP–physician collaborative model is one such example and has demonstrated decrease in avoidable hospital transfers (Ouslander et al., 2011), and evidence of cost-effectiveness with better patient outcomes (Lacny et al., 2016). Despite this, prior work by our team and others has identified significant gaps in the literature regarding the elements, nature, and dynamics of NP–physician collaboration in LTC homes (Haslam-Larmer et al., 2024, 2025; Katz et al., 2023) for others to develop such models customized to their context. This study addresses some of these gaps by examining the characteristics of successful collaborative relationship and exploring how such relationships evolve. With the implementation of new NP positions and an increase in full-time physicians in LTC homes (Goodwin et al., 2021), it is critical that both providers understand the key components of collaborative practice and the processes necessary to develop and sustain it, to optimize resident-centered care that is comprehensive, timely and accessible.
Developing a collaborative practice is a process that evolves over time. Our findings provide a clear comparative articulation of salient features that served as proxies for the successful or failed development of a collaborative practice from the perspectives of both professionals which was missing in the extant literature. NPs and physicians who flourished in an interdisciplinary collaborative environment focused on a resident-centered approach to care, had a collegial rather than a hierarchical mindset and helped each other grow as team players.
Our findings also highlight several factors that hindered the development of a collaborative practice. NPs often worked with multiple physicians, each with distinct work styles, competing priorities, and expectations for NPs to complete specific tasks on their behalf. These demands compounded the already high expectations placed on NPs including leading quality improvement initiatives, system navigation and coordination of care, and staff education. Many LTC physicians had several competing demands in addition to their clinical role in an LTC home. For example, administrative duties, large caseloads due to limited physician staffing and multiple work sites (other LTC homes, primary care practice, and hospitals). As such, the process of developing NP–physician collaboration is marked by notable interpersonal, organizational and systemic challenges, yet, many participants were able to develop it successfully demonstrating their adaptability and commitment to shared clinical goals. It is important to also highlight the relationship between role ambiguity and collaborative failure. Ambiguity can lead to decision-making conflicts, task duplication or neglect, diminished professional autonomy, and communication breakdowns, ultimately undermining trust and care quality (Reese et al., 2021). To address these challenges, non-hierarchical collaboration models with clearly specified tasks offer a promising alternative. These models emphasize shared leadership, mutual respect, and role clarity without reinforcing traditional hierarchies. By aligning responsibilities with expertise rather than title, and fostering structured communication and accountability, such models can mitigate the negative effects of role ambiguity and enhance team cohesion and resident-centered care (Koldeweij et al., 2025).
Collaborative practice is a dynamic process that requires commitment from professionals as well as organizations. Evidence-informed models, such as the Structured Collaborative Practice model, can serve as an approach to facilitate a successful collaborative relationship between NPs and physicians in LTC by implementing its seven core elements (Way D, 2000). These include responsibility and accountability, coordination, communication, cooperation, assertiveness, autonomy, and mutual trust and respect (Way D, 2000). Assertiveness involves the ability to integrate one’s expert knowledge and experience to drive resident-centered care solutions (Haslam-Larmer et al., 2025). Our findings indicated that NPs were frequently the drivers of establishing collaboration where many adapted to physicians’ expectations, styles, and temperaments to build trust and implement synergistic resident-centered care plans. On the contrary, many NPs failed to drive the development of a successful collaborative relationship raising the question about the importance of clinical expertise and years of experience in flourishing assertiveness which is one of the elements in developing NP–physician collaboration. As such, future work is needed to explore the role of assertiveness in developing and enhancing collaboration between practitioners.
The role of LTC leadership is critical in establishing the need for the role of an NP, educating staff and physicians on it, recruiting, assimilating, and retaining NPs, as well as facilitating a collaborative practice between NPs and physicians. LTC home leadership has a critical role in planning, implementing, and evaluating NP role in LTC homes that is driven by the healthcare needs of the residents. At the same time, it is also crucial to identify strategies to retain NPs after successful recruitment. Healthcare organizations are challenged by high turnover of NPs (Yun et al., 2025) due to a lack of competitive pay and benefits, ineffective management, high-stress work environment, and insufficient staffing (Hnath et al., 2023). Resources such as the participatory, evidenced-based, patient-focused process for advanced practice nursing role development, implementation and evaluation (PEPPA) framework (Bryant-Lukosius & Dicenso, 2004), and the nursing retention toolkit by Health Canada (Canada, 2024) can guide LTC leadership in identifying and implementing strategies to recruit and retain NPs in LTC environment. An engaged leadership team should also foster collaborative practice between physicians and NPs and mitigate professional hierarchies. This is particularly important with NPs and physicians who are novice to the LTC environment. These clinicians often encounter multiple challenges, including navigating a highly regulated healthcare context, caring for a clinically and socially complex resident population, experiencing limited opportunities for professional growth, and operating within broader structural constraints such as persistent health human resource shortages. Future work should examine how transformational leadership fosters collaboration amongst new NPs and physicians through shared decision-making, mentorship, and interprofessional governance. Policy efforts should create enabling conditions, such as clear role delineation, supportive funding, and leadership development, to strengthen integration of new clinicians. Research should further investigate how leadership approaches influence collaboration, care quality, and workforce sustainability in LTC.
Limitations
Although this study provides new insights into the evidence involving collaborative practices between NPs and physicians, it has limitations. It is an exploratory study involving a small sample of NPs and physicians working in (x-country) LTC homes. However, they worked in geographically diverse regions and in both private and not-for-profit homes. We did not compare the experiences of NPs and physicians working in the same LTC home. This was due to the availability of participants. Our research did not explore the role of clinicians’ experience, sex, race, culture, or the location and size of the home on collaborative practices. These factors may be an insightful consideration for future policy, practice, and research endeavors. As such the findings may not be transferable and should be interpreted according to the context.
Conclusions
Fostering a successful collaborative practice between NPs and physicians in LTC settings requires intentional efforts to establish clear roles, facilitate open communication, and promote mutual respect and shared care philosophies. Equally important is the active involvement of LTC leadership in supporting and championing the NP–physician care model to enhance care delivery and improve resident and system-level outcomes.
Supplemental Material
Suppplemental Material - Making it Work: A Qualitative Study of Nurse Practitioner-Physician Collaboration in Long-Term Care Homes
Suppplemental Material for Making it Work: A Qualitative Study of Nurse Practitioner-Physician Collaboration in Long-Term Care Homes by Shirin Vellani, Alexandra Krassikova, Lynn Haslam-Larmer, Astrid Escrig-Pinol, and Katherine S. McGilton in Journal of Applied Gerontology
Footnotes
Acknowledgments
We acknowledge all nurse practitioners and physicians who participated in this study.
Ethical Considerations
Ethics approval was obtained from the University Health Network Research Ethics Board (REB#22-5284) prior to the study activities.
Consent to Participate
All participants provided informed consent before participating in data collection.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Canadian Institutes of Health Research [180976] and the Walter and Maria Schroeder Institute for Brain Innovation and Recovery [K. M.] supported this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Additional data can be available upon appropriate requests.
Supplemental Material
Supplemental material for this article is available online.