
Abstract
As older adults’ assistance needs increase, aging in place may become difficult due to high costs or limited care. A new approach of care (Vieillir chez soi, VCS) was implemented within an existing seniors’ residence (SR) to provide evolving and person-centered care. Drawing on an embedded mixed-methods approach combining survey data with individual interviews, this study documented residents’ (n = 10) and informal caregivers’ (n = 15) perspective regarding the VCS approach. Overall, it promoted a positive long-term vision, allowing participants to continue living at the SR and engaging in meaningful activities and maintain their relationships. However, they shared a desire to be more informed and involved in care planning, highlighting communication gaps with the SR’s staff. Challenges with cohabitation also emerged, such as the potential loss of belonging. This study underscores the relevance and challenges of providing evolving living environments to enable older adults to age in place despite increasing assistance needs.
Keywords
• Being able to age in place with their life partner despite diverging assistance needs is important for older adults and their family, and favors a positive long-term vision of life. • Cohabitation may promote positive relationships among older adults with diverse assistance needs, foster volunteering opportunities, and provide a safer and meaningful environment for those who can live with their loved ones. • Aging in place may however bring some challenges in continuing engaging in meaningful activities as the surrounding of the residents’ changes over time, especially for those who lived at the seniors’ residence before the project.
• Living environments that offer evolving care while promoting cohabitation represent a promising housing option. • While these settings provide personalized support, they may not be suitable for everyone and should be integrated into a broader care ecosystem that reflects the diverse needs of the aging population.What This Paper Adds
Applications of Study Findings
Introduction
It is estimated that by 2030, one in four Canadians will be 65 years or older (Statistics Canada, 2024). When their increasing needs exceed what caregivers can provide at home, older adults may choose to move into collective dwellings, such as seniors’ residences (SR), to access the care and services they require (Cohen et al., 2025; Garner, 2018). In Québec (Canada), SRs are categorized into four levels based on the inclusion of services, including meal, security, recreational, and domestic assistance services (all levels), medication distribution (levels 2 to 4), personal care services (levels 3 and 4), and nursing care (level 4) (Regulation respecting the certification of private seniors’ residences, 2025). However, living in SRs may become unsustainable over time due to relatively high costs associated with pay-per-service and/or limited care and supervision. This can force older adults to relocate to long-term care (LTC) public facilities, despite the known physical and psychological toll of care transitions (Ryman et al., 2019). In addition to domestic assistance, personal aid and nursing care, LTC facilities may provide medical and rehabilitation care, including support currently not provided in SRs, such as palliative care (Direction des communications du Ministère de la santé et des services sociaux, 2018). Given the long wait times for admission to LTC and evidence that approximately one in ten relocations could have been avoided with adequate support (Canadian Institute for Health Information, 2025), there is a need for affordable housing options that offer older adults access to evolving levels of care as their needs change.
A novel care approach called “Vieillir chez soi” (VCS, i.e., Age at home in English) was co-developed in close collaboration with an existing level-4 SR and the public home care services. Located in the province of Quebec (Canada), the SR of 111 individual rooms was already providing care to older adults living with mild to moderate cognitive impairments, most of them being relocated to LTC when assistance needs became too important. Based on the person-centered approach (Fazio et al., 2018), which recognizes the multidimensions and psychological needs of individuals with dementia (Kitwood, 1997), the VCS approach aims to provide evolving care adapted to older adults’ increasing needs and promote aging in place in their environment of choice (Gagnon-Roy et al., 2026). Throughout its implementation, the SR’s team was supported in integrating best practices, going beyond the person’s assistance needs and recognizing their needs for occupation and identity, made possible by the documentation of their life stories. Other interventions were implemented, all in relation to the residents’ life stories, to promote a sense of continuity and safety within their living environment (Nolan et al., 2004). Supported by financial support and specialized interventions from home care services, interventions included (a) Reorganizing care and services to provide evolving and personalized care (e.g., delay the morning routine and upgrade the number of personal support workers [PSWs]) (Aubry et al., 2020); (b) Staff training to improve communication and interactions with residents, including those with challenging behaviors (Rijnaard et al., 2016); and (c) Adapting the environment to create engaging spaces, such as a little farm and a bistro-themed living space. These new environments were inspired by continuing care retirement communities like small-scale living environments and Green Care Farms models (De Boer et al., 2018), which offers different levels of care in distinct floors or settings (Shippee, 2009). The VCS approach contrasts from the latter, as it promotes cohabitation and inclusion between residents with different care levels, and the ability to move freely across the SR’ three floors. Overall, the VCS approach enabled the SR’s staff to admit older adults with significantly higher assistance needs and delay their relocations in LTC (Gagnon-Roy et al., 2026). More specifically, results suggested that the VCS approach could delay relocation by an average of 3.5 months and facilitate residents’ return to the SR after hospitalization. For those whose relocation to LTC was unavoidable, the move occurred significantly closer to the end of life.
Such promising results highlight the relevance of implementing and maintaining the VCS approach over the long term, enabling older adults to age in place within a small and adaptative community (i.e., SR). However, although the success indicators based on medical and administrative data (e.g., hospitalization and level of independence) were positive, little is known about the lived experience of the ones directly impacted by the VCS approach, that is, the residents and their informal caregivers. This study thus aims to document the perceptions of families and residents regarding the VCS approach, including perceived advantages and challenges. As key stakeholders in the VCS co-development (Gagnon-Roy et al., 2026) and advocates for their relatives’ care, documenting the perceptions of both informal caregivers and residents is essential to support further improvements and ensure the sustainability of the care approach, aligned with residents’ needs and lived experience.
Methods
Study Design
An embedded mixed-methods design (Creswell & Clark, 2017) was used, combining quantitative data (caregiver survey) with a primarily qualitative approach (semi-structured interviews with caregivers and residents). While qualitative methods provided in-depth insights into caregivers’ and residents’ experiences with the VCS approach (Sandelowski, 2000), the survey offered an exploratory quantitative strand that captured broader caregiver perspectives and refined emerging findings. Integrating both approaches yielded a more comprehensive understanding of participants’ experiences, while accounting for caregivers’ burden and constraints. The COnsolidated criteria for REporting Qualitative research (COREQ) was used (Tong et al., 2007). The study was approved by the Ethical Board of the CIUSSS de l’Estrie – CHUS (2023-4741).
Researchers and Reflexivity
Although the research team closely collaborated with the SR management team to co-develop the VCS approach, it remained independent from the SR and had no conflicts of interest. Data collection was conducted by three female researchers (MGR, SN, SRA), all experienced in qualitative methods and independent from the SR. Having previously been involved in the VCS co-development process, they were able to provide background information and contextualize participants’ experiences within the SR. SN had ten years of experience as a PSW working with older adults; SRA, an occupational therapist, specialized in implementation and organizational culture change; both held master’s degrees in gerontology with the principal investigator (VP). MGR, also an occupational therapist, was a postdoctoral fellow in health sciences with a focus on participatory research. Two of these researchers were also involved in data analysis and interpretation. As emerging themes were shared with stakeholders to enhance care in the SR—reflecting a shared commitment to improving care for older adults—this process may have introduced some positive bias in the analysis and interpretation. Nonetheless, the analysis was validated by an independent researcher (DMB) with no prior contact with stakeholders.
Participants
Family and informal caregivers (IC) were contacted by email by the SR management team. All caregivers who had cared for a resident in the past year (September 2023–August 2024; 150+ total) were invited to participate anonymously, with a reminder sent one month later. At the end of the survey, caregivers could indicate willingness to be contacted for an individual interview. To ensure data saturation, all consenting caregivers were emailed by the research team to schedule an interview. No financial compensation was offered.
A convenience sample of residents (R) was recruited for individual interviews on their lived experience. Eligibility required the ability to communicate in French or English and at least one month of residence at the SR. Exclusion criteria included residents with difficulties in instrumental and/or basic activities of daily living, due to a moderate to severe cognitive impairment, as indicated by their ISO-SMAF profile (e.g., profiles 4, 7–8, or 10–14) (Dubuc et al., 2004). This indicator was used since the ISO-SMAF Profile is routinely assessed and accessible to the SR’s management team. Based on these criteria, 14 residents were identified and contacted by the SR’s team to explore their interest in participating to the study; one was approached directly by the research team after expressing prior interest. Eleven residents agreed to participate and were interviewed, though one was later excluded for inability to answer. Participants received $20 in compensation.
Procedures and Data Collection
Quantitative Data: Survey With Caregivers
A bespoke 20-minute, 40-item survey was co-developed by the research and SR management teams specifically for this study (see Appendix I). The survey collected sociodemographic data (age, gender, length of stay at the SR, and relationship to the resident) and, using a four-point scale, documented caregivers’ experiences with care (involvement, quality, and communication) and the VCS approach (understanding, financial model, and activities). Open-ended questions followed each section. Items were adapted from published satisfaction and care questionnaires (Kiely et al., 2006). The survey was pre-tested by a family caregiver involved in VCS co-development (Gagnon-Roy et al., 2026) and administered via Microsoft Forms. The survey was not validated.
Qualitative Data: Semi-Structured Interviews With Caregivers and Residents
Interviews With Caregivers
Interview Guide with the Informal Caregivers
Interviews With Residents
One-hour interviews were conducted in residents’ rooms to ensure confidentiality. A seven-question guide explored their experience with the VCS approach, including likes, dislikes, and willingness to recommend the SR. Specific components (e.g., small farm, bistro-themed room, and use of life stories to personalize care) were discussed. Additionally, as behavioral and psychological symptoms of dementia (BPSD) were increasingly observed at the SR, two case studies on aggressive behaviors and room intrusions were presented to elicit residents’ experiences and reactions (see Appendix II). Breaks and digressions were allowed to foster engagement and natural conversation. Sessions were audiotaped and conducted by the same interviewers.
Data Analysis
Qualitative Data Analysis
Following transcription, an inductive thematic analysis was conducted using Miles, Huberman, and Saldana’s method (Miles et al., 2019). Interview and survey verbatims were coded by the first author (MGR) to capture participants’ experiences with the VCS approach. Separate coding lists were created for caregivers and residents. To ensure fidelity, 30% of the data was reviewed by a second author (DMB), an external qualitative researcher, with discrepancies discussed collaboratively. Themes were then developed by regrouping codes across participants and validated by two authors, including one interviewer (DMB, SRA).
Analysis and Convergence of Quantitative Data
Quantitative data were analyzed using a data transformation approach (Fetters et al., 2013). Survey items were translated into sentences reflecting participants’ general experience. The research team developed and validated a matrix to compare themes across surveyed caregivers, interviewed caregivers, and interviewed residents. Qualitative codes and caregiver sentences were first grouped into themes, and then divided by participant group. This matrix revealed divergences between individual and collective caregiver experiences, as well as similarities and differences between caregivers and residents. Final codes are presented in Appendix III.
Results
Characteristics of Informal Caregivers and Residents Who Participated in the Interviews
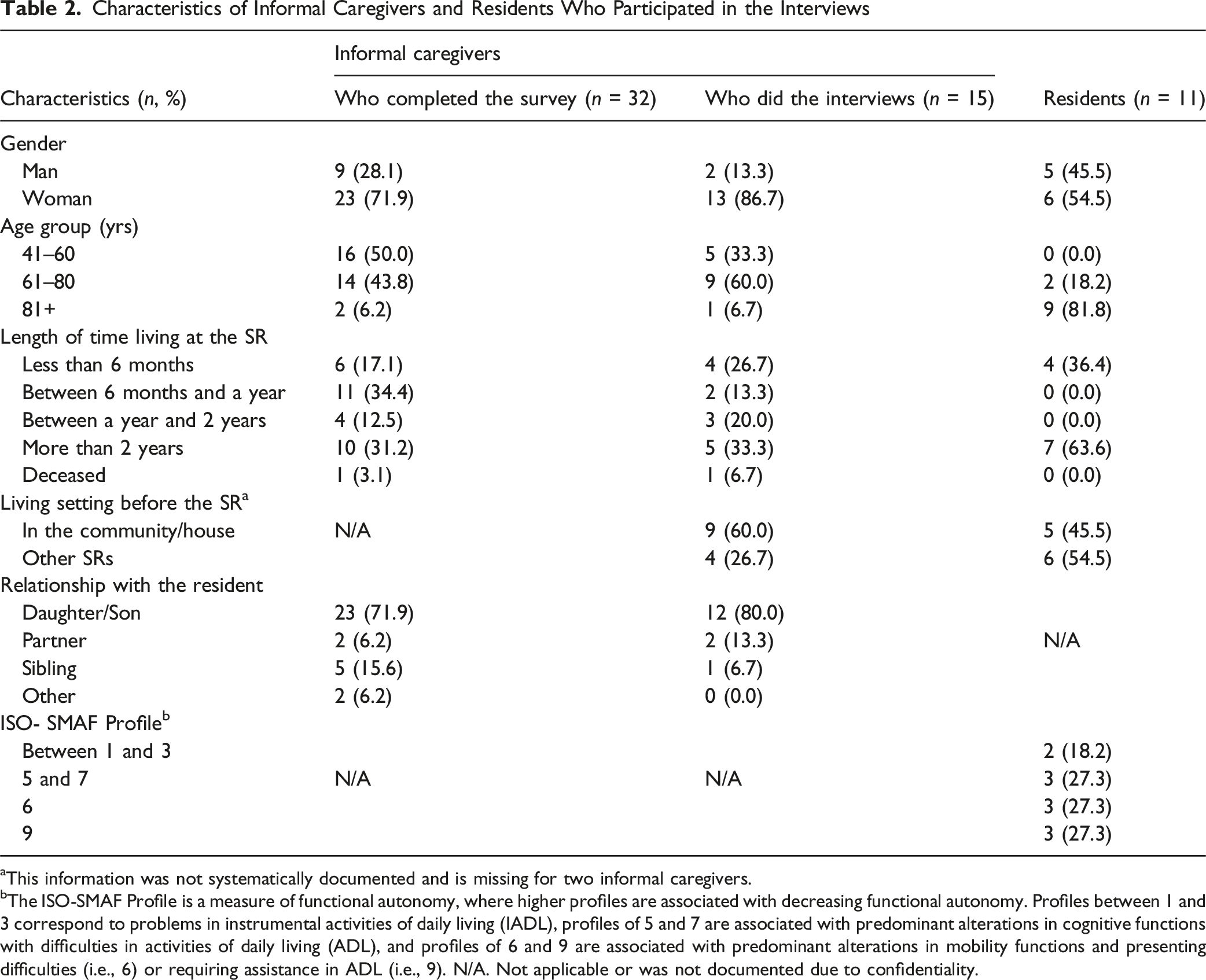
aThis information was not systematically documented and is missing for two informal caregivers.
bThe ISO-SMAF Profile is a measure of functional autonomy, where higher profiles are associated with decreasing functional autonomy. Profiles between 1 and 3 correspond to problems in instrumental activities of daily living (IADL), profiles of 5 and 7 are associated with predominant alterations in cognitive functions with difficulties in activities of daily living (ADL), and profiles of 6 and 9 are associated with predominant alterations in mobility functions and presenting difficulties (i.e., 6) or requiring assistance in ADL (i.e., 9). N/A. Not applicable or was not documented due to confidentiality.
Perceived Advantages and Challenges of Aging in Place With the VCS Approach of Care
Advantages and Challenges of Aging in Place With the VCS Approach of Care
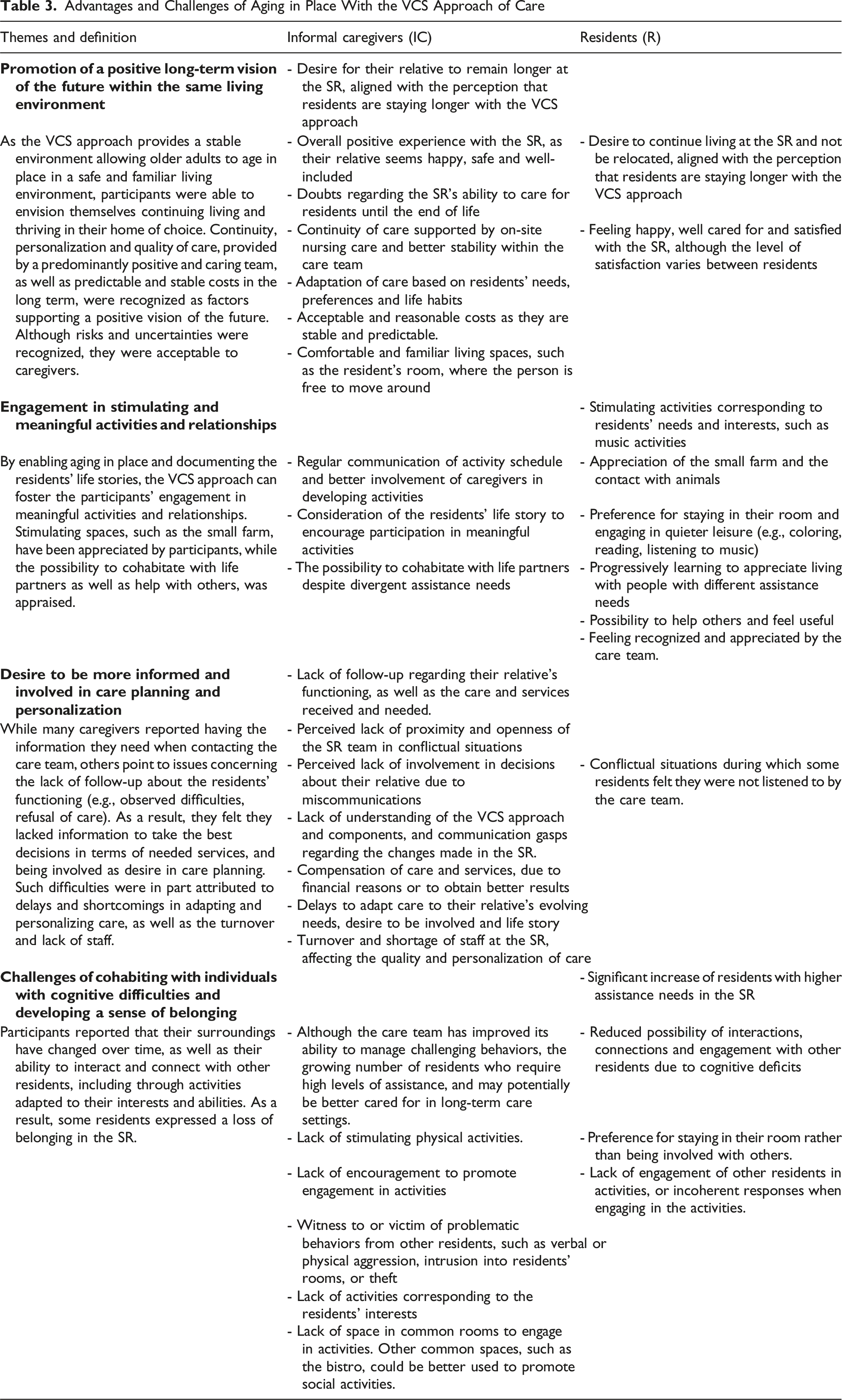
Promotion of a Positive Vision of the Future Within the Same Living Environment
One of the main advantages emerging from the participants’ narrative was the impact of aging in place on their perception of the future, as the VCS approach enabled them to envision themselves continuing to live and thrive within the same environment. This goal, central to the VCS approach, was appreciated by almost all the surveyed caregivers (97%), aligned with their wish for their relatives to remain at the SR for as long as possible: “I for sure pray that [my parents] will stay there for the rest of their lives” (IC11). This positive vision of the future was further supported by caregivers’ and residents’ overall satisfaction with the VCS approach, as well as the safety and familiarity of living spaces. In fact, most surveyed caregivers felt their relatives were happy (72%) and safe (87%) at the SR. Quality of care, both in terms of continuity and personalization, was also highlighted as promoting a positive long-term vision. More than 80% of surveyed caregivers felt comfortable with the way care was provided, corresponding to their relatives’ needs, despite half of respondents having reported an undesirable event (e.g., instances of missed care). The continuity of care and the positive interactions with the care team were especially appraised, providing a more proactive, accommodating and personalized care approach: “When [my mother] is sick, I call the infirmary […]. Then they’ll look, they'll take the [needed] steps” (IC12). Using the residents’ life story, the care team could also better know the residents and further adapt their approach based on their needs, preferences and life habits, a relevant aspect that was appreciated by 84% of surveyed caregivers. Despite expressing some doubts regarding the SR’s ability to care for residents until the end of life, caregivers further highlighted the stability and positive vision provided by the VCS approach as only relocations in LTC may be needed in certain situations (e.g., aggressive behaviors towards other residents and palliative care).
In addition, financial support ensured that residents could remain within the same living environment despite increasing assistance needs. With the VCS approach, financial support was provided to the SR for all residents with an ISO-SMAF Profile of 7 or higher, ensuring that care costs remained stable and comparable to LTC expenses. Caregivers thus described the costs as acceptable, reasonable, and predictable in the long term.
Engagement in Stimulating and Meaningful Activities and Relationships
Residents and caregivers highlighted that the approach could foster their engagement in meaningful activities and relationships. By promoting aging in place, the VCS approach allowed life partners to cohabitate despite divergent assistance needs, and maintain highly meaningful relationship, as explained by IC13s: “If one of [my parents is] sick, he could stay anyway. […] So, they could go and see the other one every day if they wanted to.” One resident (R4) further highlighted how cohabitation was beneficial for his wife living with dementia, allowing him to continue playing his role as a caregiver and life partner: “Since I’ve been sleeping with her, she’s much better behaved.” Although cohabiting with people living with cognitive impairments may be challenging, three residents expressed that they learned to accept the people surrounding them, and to appreciate interactions with them. For other residents, cohabiting was an opportunity to help and engage with others, such as for R5 who frequently made sure residents were well-seated and oriented in space. Continuity and personalization of care based on the residents’ life stories were also appraised in ensuring a better relational continuity with the care team.
Stimulating activities and spaces were also proposed to residents, in-line with their life stories, further fostering their engagement. A major highlight was the installation of a small farm in the SR’s backyard, encouraging positive and stimulating interactions between the residents and the animals: “There are lots of people who go there, even people who are a little more cognitively impaired. Zootherapy is good for everyone” (IC12). While only 50% of the surveyed caregivers were satisfied by the activity schedule, the hiring of a leisure technician a few weeks after the survey was highly appraised by participants. Since her arrival, activities increased while better corresponding to the residents’ interests and life stories: “There’s bingo, there’s coloring. My mother likes to color a lot, they play music, they do all kinds of stuff” (IC9). Level of participation, however, varied between residents: while a portion of them were involved in planned activities, others preferred to stay in their room and do their own things, such as coloring, reading, listening to music or watching TV. These preferences in engagement and choice of activities are illustrated by R3: “I do my activities, my crosswords, my diary... I have an active brain.”
Desire to be More Informed and Involved in Care Planning and Personalization
One of the main challenges faced by caregivers concerns their ability to be informed and actively involved in their relative’s care. Although communications between caregivers and the care team were generally positive and adequate, around 60% of them also raised challenges in trying to obtain follow-up regarding their loved one functioning, and the care and services they received. This lack of follow-up impacted their ability to adequately define the level of care their relative needed, and provide the right information during medical follow-ups, as explained by IC5: “It’s hard for me to get this information. […] I think the lack of follow-up is the hardest thing to accept, to deal with.” The alignment between the desire to be informed, and the level of information provided by the SR nonetheless varied across participants, as 78% of surveyed caregivers felt fully involved in decisions concerning their relatives. Communication challenges also influenced participants’ understanding of the VCS approach’s components, and their perspective of the changes brought within the SR. While caregivers understood that the provided care will adapt over time according to the residents’ needs, less than 60% felt that they were well informed of the project and its true implications, and less than 70% understood its objectives. As a result, caregivers emphasized the need to be better informed, which could in return promote their involvement with their relative.
These challenges in informing and involving participants in care planning as desired were in part associated with a lack of resources. Despite staff training and best intentions to provide personalized and evolving care, both residents and caregivers pinpointed delays in the SR’s ability to adapt care to specific needs, residents’ life story and desire to be involved. Participants frequently attributed these delays to staff turnover, shortages, and variations in the quality of care among PSWs. As they had to adapt to residents with increasingly heavier assistance needs, the turnover rate was high over the first two years of the approach. Consequently, a quarter of the interviewed caregivers decided to compensate by themselves for perceived missing care and services, whether for financial reasons, to reduce potential refusal or to ensure better results. For example, IC5 explains that each time she visits her husband, she helps him do “things that are more difficult. He doesn’t want to go to the bath downstairs, he refuses. So, the first thing I do is OK, let’s take a shower.” While some caregivers such as IC5 took on this responsibility as care co-providers, others felt they had to so that their relative received the care and services they needed.
Challenges of Cohabiting With Individuals With Cognitive Difficulties and Developing a Sense of Belonging
Although participants expressed advantages with being able to live with their partner and age in place, their lived experience also highlighted how cohabitating with individuals having various levels of cognitive abilities may be challenging. Most residents and caregivers raised the issue of managing other residents’ challenging behaviors, as they have been witnesses to or victims of verbal or physical aggression, intrusion into residents’ rooms, or theft. This situation was illustrated by IC12, who explained: “My mother, it’s been 3 times, even 4 times... Once she was bitten, the other time it was her arms. Enough to leave marks” (IC12). As a result, six residents and four caregivers felt that older adults living at the SR had increasingly heavier assistance needs and questioned their place within this living setting, but also their own sense of belonging. Two residents further underscored the loss of community they felt as their social environment changed over time: “It’s a bit difficult. Especially when there are people who come up to you, then they are completely incoherent” (R4). Due to the experienced challenges with cohabitation and the presence of residents with more important cognitive difficulties, these residents expressed their frustration with the SR’s choice of enabling aging in place, highlighting how the VCS approach may not apply to all. This was the case of R6: “There should just be Alzheimer’s. [...] The mix of the two, it doesn’t make any sense.” Other residents, despite not wanting to engage with others, were less negative and preferred staying on their own, such as R2 who explained that she “cannot live in there” and that “[she is] feeling good in [her] own little corner.”
Due to the diversity of abilities and interests among residents, being able to engage in activities with others emerged as an issue, especially with residents with cognitive impairment. For some residents with lower assistance needs, engaging with others in the proposed activities was disappointing, as explained by R11 who decided to stop participating: “I’m all alone. [The residents] are asleep and they don’t say anything, so I’m not interested.” For residents with greater assistance needs, more encouragement than what is actually provided by the PSWs may be needed to engage in activities: “When there’s an activity, I’d like them to go and get [my parents]. Even if they’re told there’s a thing going on, they’re not going to go” (R11).
Discussion
Using an embedded mixed-methods design, this study examined caregivers’ and residents’ experiences with the VCS approach in a SR. By fostering aging in place and cohabitation, the approach was perceived as promoting a positive vision of the future. Relational continuity and stimulating environments (e.g., small farm) enabled residents to build meaningful relationships and engage in activities within a safe, stable setting. Challenges included adapting care to evolving needs, involving residents and caregivers in planning despite limited resources, and managing interactions among residents with varied levels of cognitive abilities.
While aging in place enabled caregivers and residents to project themselves living in the same environment over the long term, the lived experience with cohabitation differed markedly among residents. Some residents’ narratives highlighted the strengths of cohabitation, as it provided them opportunities to help others and playing a role in their “community.” Such opportunities can be considered as volunteering, which has been associated with psychosocial benefits such as reduced symptoms of depression, greater life satisfaction, and improved quality of life (Filges et al., 2020). Cohabitation can also help shift care to a more relational approach, recognizing the importance of relationships in empowering residents in helping others, and engaging more dependent residents in activities through meaningful socio-emotional support (Rockwell, 2012). Recognizing and promoting meaningful and positive relationships, such as with life partners, staff, and caregivers, could also foster a sense of continuity, belonging, and purpose for the person (Nolan et al., 2004). Conversely, cohabitation with residents experiencing progressive cognitive decline was found to be challenging, particularly for those interacting with the ones directly affected by these changes. As their entourage changed over time, they grieved and lost the social environment they had originally chosen. The risk of residents not wanting to live alongside those with moderate to severe cognitive impairments have been previously documented, highlighting the tension between inclusion and segregation of residents with dementia in similar living settings (Zimmerman et al., 2022). These findings thus emphasize the importance of residents and caregivers fully understanding the challenges and strengths of cohabitation to make informed decisions, but also to support them in their acceptation and adaptation process. Aging in place goes beyond adapting the physical spaces and supporting the care staff in providing personalized care. It should also recognize how the person and their place coevolve, as how the person defines being in place and the way the latter adjusts to the person’s needs continuously change through care situations (Rhodus & Rowles, 2022). Understanding the value of being in place, as well as giving the time to adapt to this new place, could thus support adjustments and help promote a positive view of cohabitation.
By encouraging cohabitation among residents, this study also underscored the delicate balance between respecting older adults’ autonomy and ensuring their physical and psychological safety. Despite cognitive impairments, residents could move freely within the SR, leading some to experience or witness disruptive behaviors, such as aggression or room intrusions, that affected their sense of safety and belonging. A third of the residents preferred staying in their rooms over socializing. These findings highlight the need to foster interactions among residents with diverse abilities, while also providing safe spaces for engagement with peers who share similar levels of independence (Weinstock & Bond, 2018).
Communications gaps between caregivers, residents and the SR’s care team also emerged, supporting their desire to be more informed and involved in care planning. Caregivers expressed how difficult it can be to advocate for the care and services their relatives need without regular communication about their functioning. Such communication issues have been previously described in the literature, impacting the caregivers’ ability to play an active role in their relatives’ care planning (Allen et al., 2023). Engaging caregivers is nonetheless essential considering their extensive knowledge of the residents’ life stories, values, and preferences, but also as a meaningful relationship and tie to their relatives’ self (Qualls, 2016). As resources and time are limited, notably due to staff shortage and turnover, it is necessary to optimize communications and foster the caregivers’ involvement in care in a way that could naturally be integrated within the work routine without increasing the staff burden. Paper-based tools (e.g. residents’ life stories) were tested in the SR but seldom used by PSWs due to low visibility. Optimizing existing digital tools for staff and enhancing information exchange with caregivers could improve communication and foster their involvement in care decisions (Martínez-Alcalá et al., 2016).
This study captured the advantages and challenges of the VCS approach from caregivers’ and residents’ perspectives, 2 years after its implementation. Qualitative interviews provided in-depth insights into their lived experiences, while the survey completed by a larger number of caregivers added broader nuance to the findings. A rigorous method—including validation of over a quarter of the verbatim—allowed for the identification of key themes describing the participants’ experiences, as well as comparison of caregivers’ and residents’ perspectives. Nonetheless, the study has certain limitations. As participation was voluntary, caregivers and residents who willingly enrolled in the study may not represent the overall experience of their respective groups (i.e., self-selection biases). Although caregivers are predominantly women (Xiong et al., 2020), their high proportion in the sample may have introduced bias. However, the survey—completed by a broader group, including more men—helped nuance the emerging themes, with nearly half of the residents also being male. Moreover, while data saturation was reached among caregivers, confidentiality and feasibility constraints prevented full representation of residents’ varying levels of autonomy, meaning those with greater assistance needs may have experienced the VCS approach differently. Biases such as social desirability may have also influenced the information shared during interviews, although participants were informed that the interviews were confidential. Finally, despite being co-developed and validated with the SR team, and pre-tested with a caregiver, the survey validity and reliability were not formally assessed. When possible, significant individual responses were nonetheless validated with the caregivers during the interviews. Finally, findings were not validated by the participants to minimize potential burden. However, themes were validated by the SR’s management team, who shared similar feedback from the caregivers and residents.
Implications for Practice and Policy
This mixed-method study offers a comprehensive view of the VCS approach from families’ and residents’ perspectives. By revealing its benefits and cohabitation challenges, the findings support its broader implementation across existing SRs. As part of an ecosystem offering living settings adapted to the diverse needs of older adults, the VCS approach provides a stimulating and evolutive environment for older adults requiring personal care assistance (level-4 SR), while delaying or even avoiding future relocations. Although relocations may be unavoidable due to limited medical coverage, aging in place remains relevant for most residents, highlighting how adapted and personalized environments can foster a sense of continuity and safety (Nolan et al., 2004). To ensure success, favorable conditions are needed: (a) financial support to stabilize costs and comparable to those incurred in LTC; and (b) developing a close partnership between the SR’s team and home care services through regular coordination meetings. With financial support, the VCS approach may foster more equitable access to evolving care, reducing relocations to LTC driven solely by financial constraints—as was previously the case (Gagnon-Roy et al., 2026). As transitions are often challenging, residents and caregivers must understand both the strengths and limitations of cohabitation. Such awareness can foster informed housing decisions and encourage meaningful engagement in the SR, including volunteering. Awareness-raising and preventive activities could help residents interact more effectively with individuals living with dementia and promote overall wellness (Falardeau et al., 2023). Identifying resident characteristics and values that favor cohabitation—such as prior caregiving or volunteering experience (Choi & Chou, 2010)—may also guide decision-making. With these conditions, along with stakeholder leadership and openness to change, the VCS approach could be extended to other level-4 SRs and similar settings. Future studies should examine its long-term outcomes and cost-effectiveness.
Supplemental Material
Supplemental Material - Staying Together Through Evolving and Personalized Care: Perspectives of Informal Caregivers and Residents on Aging in Place Within a Seniors’ Residence
Supplemental Material for Staying Together Through Evolving and Personalized Care: Perspectives of Informal Caregivers and Residents on Aging in Place Within a Seniors’ Residence by Mireille Gagnon-Roy, Didier Mailhot-Bisson, Sarah Rahimaly, Monia D’Amours, Solange Nkulikiyinka, Nathalie Delli-Colli, Bessam Abdulrazak, Chantal Viscogliosi, and Véronique Provencher in Journal of Applied Gerontology
Ethical approval and informed consent statements
Supplemental Material
Supplemental Material - Staying Together Through Evolving and Personalized Care: Perspectives of Informal Caregivers and Residents on Aging in Place Within a Seniors’ Residence
Supplemental Material for Staying Together Through Evolving and Personalized Care: Perspectives of Informal Caregivers and Residents on Aging in Place Within a Seniors’ Residence by Mireille Gagnon-Roy, Didier Mailhot-Bisson, Sarah Rahimaly, Monia D’Amours, Solange Nkulikiyinka, Nathalie Delli-Colli, Bessam Abdulrazak, Chantal Viscogliosi, and Véronique Provencher in Journal of Applied Gerontology
Ethical approval and informed consent statements
Footnotes
Acknowledgments
We want to thank all the stakeholders who took part in the co-development and evaluation process of the VCS approach of care, especially the management team of the SR and the home care services. We would like to acknowledge the precious contributions of family caregivers and residents who generously shared their time and experiences in support of this research.
ORCID iDs
Ethical Considerations
The study was approved by the Ethical Board of the CIUSSS de l’Estrie – CHUS (2023-4741).
Consent to Participate
All participants provided their informed consent to participate to this study. Caregivers had to check a box stating that they read the consent form and accepted to participate before completing the survey. A verbal consent was obtained before the interviews with the caregivers. Older adults signed a consent form.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was jointly funded by the Canadian Institutes of Health Research (492219) and the Fonds de recherche du Québec - Santé (339238), as well as the Vitae Foundation and the Research Center on Aging. MGR was supported by a postdoctoral scholarship from AGE-WELL and the Réseau Québécois de recherche sur le vieillissement (RQRV).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during the current study are not publicly available due confidentiality.
Supplemental Material
Supplemental material for this article is available online.