
Abstract
Using a national survey of assisted living administrators (n = 2,084) and interviews with residents’ bereaved next of kin (n = 30), we describe policies administrators reported complying with at the worst of the COVID-19 pandemic and explore relationships between COVID-19-related policies and bereaved next-of-kin’s perceptions of end-of-life care quality, integrating findings to develop a comprehensive examination of end-of-life care in assisted living. During the pandemic, most administrators reported allowing compassionate care visits and hospice services. Next of kin described limited visitation and external care services and declines in residents’ physical, mental, and social well-being, emphasizing the difficulty of missing precious time together. This study examines next-of-kin experiences of residents who died during the COVID-19 pandemic, providing evidence to inform future infection control policies.
Keywords
This study provides national evidence comparing administrator-reported policies and the experiences of bereaved next of kin. While most assisted living administrators reported permitting end-of-life care services and visitation during the “worst” of the pandemic, bereaved next of kin expressed significant barriers, underscoring the possible disconnect between policies and residents’ experiences. Our mixed-methods design yielded rich, detailed insights integrating administrator data on hospice and visitation policies with narratives from bereaved next of kin, illustrating the value of mixed-methods research in revealing different interpretations of policies and protocols. Previous research on end-of-life care in long-term care settings has primarily focused on nursing homes, relied on smaller, less diverse qualitative samples, or featured less nationally representative survey designs. Our findings offer new evidence of how assisted living residents and their next of kin experienced end-of-life care during the COVID-19 pandemic.
State agencies revising emergency preparedness and infection control policies should consider residents at the end of life in assisted living, balancing resident safety while promoting meaningful interactions with next of kin and access to essential services like allied health professionals, including audiologists and dentists. Although supplies were limited early in the pandemic, ensuring that evidence-based resources—such as personal protective equipment and improved ventilation—are prioritized and maintained in sufficient stockpiles could help state agencies and assisted living communities support safe in-person visits for residents nearing the end of life during future outbreaks.What This Paper Adds
Applications of Study Findings
Introduction
Approximately 30,600 U.S. assisted living (AL) communities provide care to over one million residents (National Center for Assisted Living, 2024). A longitudinal study of Medicare beneficiaries in large AL communities between 2017 and 2019 found that over one-third died within 3 years; nearly half (49.5%) of dying residents experienced a care transition in their last 30 days of life (Belanger, Rosendaal, Wang, et al., 2024). Such transitions are considered burdensome by most families (Makaroun et al., 2018) and may reflect AL staff training variability (Dobbs et al., 2006), resident characteristics (Ball et al., 2014), organizational factors, and end-of-life care policies (Travis et al., 2021).
State agencies regulate AL services, with over 100 license types nationally contributing to state variability in residents’ end-of-life care outcomes (Belanger et al., 2022; Thomas et al., 2020). An inventory showed that 31 states had explicit regulations allowing hospice in AL communities, 10 lacked such regulations, and others varied by license type (Thomas, Cornell, et al., 2021). Residents in states with supportive hospice regulations had slightly higher hospice utilization (Belanger et al., 2022), providing residents and their families crucial end-of-life and bereavement services (Cartwright et al., 2009). Yet, most qualitative AL end-of-life studies remain geographically limited (Ball et al., 2014; Bennett et al., 2021; Davis-Berman, 2011; Flock and Terrien, 2011). More geographically diverse research is essential, given the varied AL requirements across states.
States mandated varying AL infection prevention measures, including admission and discharge policies, personal protective equipment (PPE), and testing, with frequent policy changes, even in compassionate care or imminent death cases (Centers for Medicare and Medicaid Services, 2020). Most evidence about end-of-life services during COVID-19 focuses on nursing homes (Eriksson & Hjelm, 2022; Feder et al., 2021) or quantitative data (DeYoreo et al., 2024; Temkin-Greener et al., 2020; Thomas, Zhang, et al., 2021). More end-of-life care quality evidence across states with differing COVID-19 policies is needed to inform future high-mortality infectious disease responses. This mixed-methods study investigated national variation in administrator-reported COVID-19-related policies, and bereaved next-of-kin’s perceptions of how policies shaped end-of-life care quality.
Methods
Study Design
We employed a convergent, parallel mixed-methods study design (Figure 1) (Creswell & Plano Clark, 2017) to characterize administrator-reported COVID-19 policies and bereaved next-of-kin’s accounts of relevant end-of-life experiences. As an exploratory, descriptive study, no hypotheses were prespecified. Reporting followed COREQ and STROBE guidelines (Tong et al., 2007; von Elm et al., 2007). The study was approved by the Brown University Institutional Review Board (Protocol #2599), and an exempt determination was made for the administrator survey as it did not collect identifying information. Interview and survey instruments are provided in the Supplemental Materials. Sequential, parallel mixed-methods research design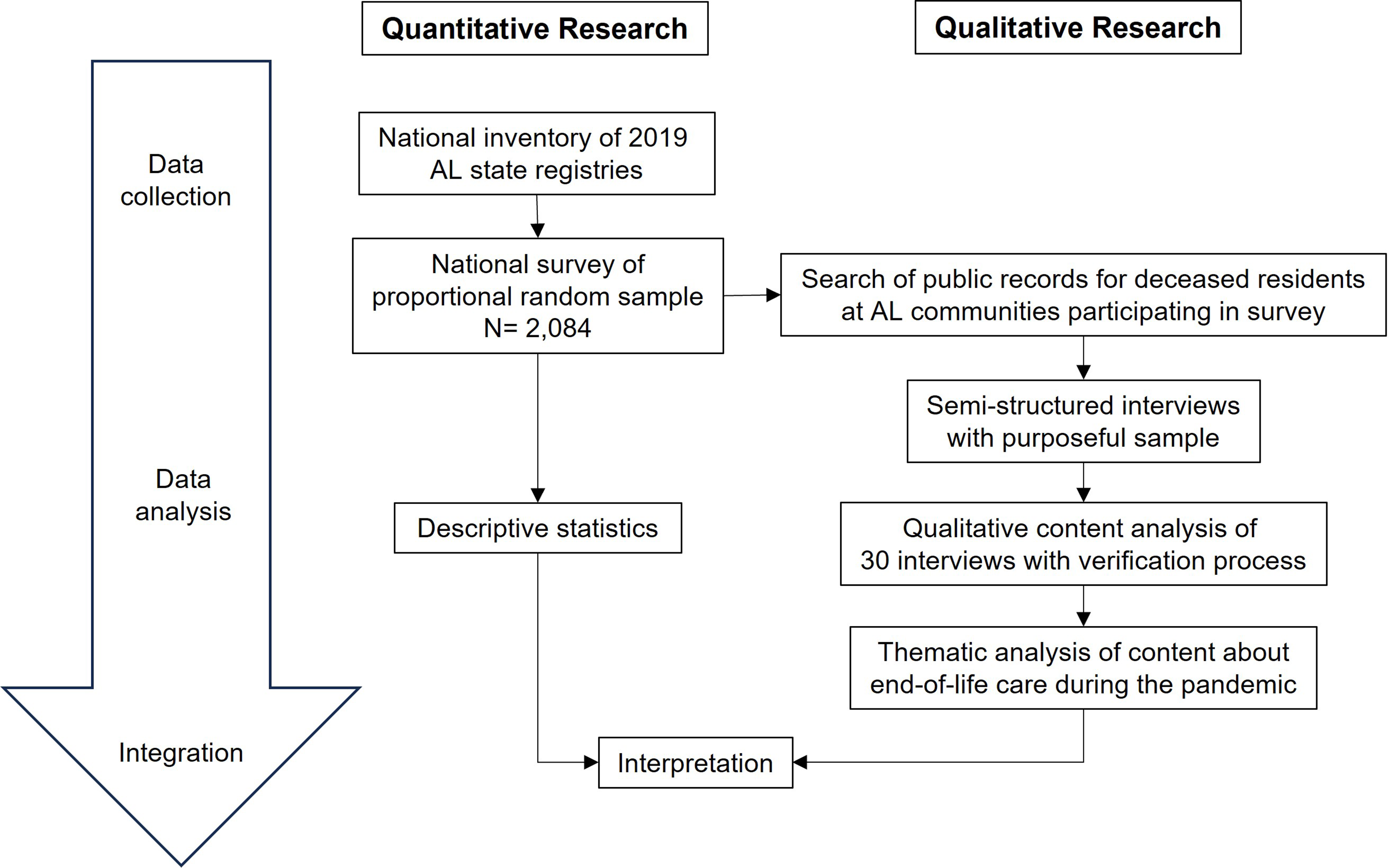
Quantitative Data Collection and Analysis
We contacted a proportional random sample of 4,082 administrators across all U.S. states and licenses, excluding Connecticut and Minnesota because of licensing differences (Belanger, Rosendaal, Rogers, et al., 2024). Between 2021 and 2023, administrators received mailed questionnaires with an online completion option, followed by mailed postcards and phone call reminders. Surveys took 20–30 min, depending on question applicability. Administrators received a $25 gift card.
AL Communities Descriptive Statistics, National Administrator Survey
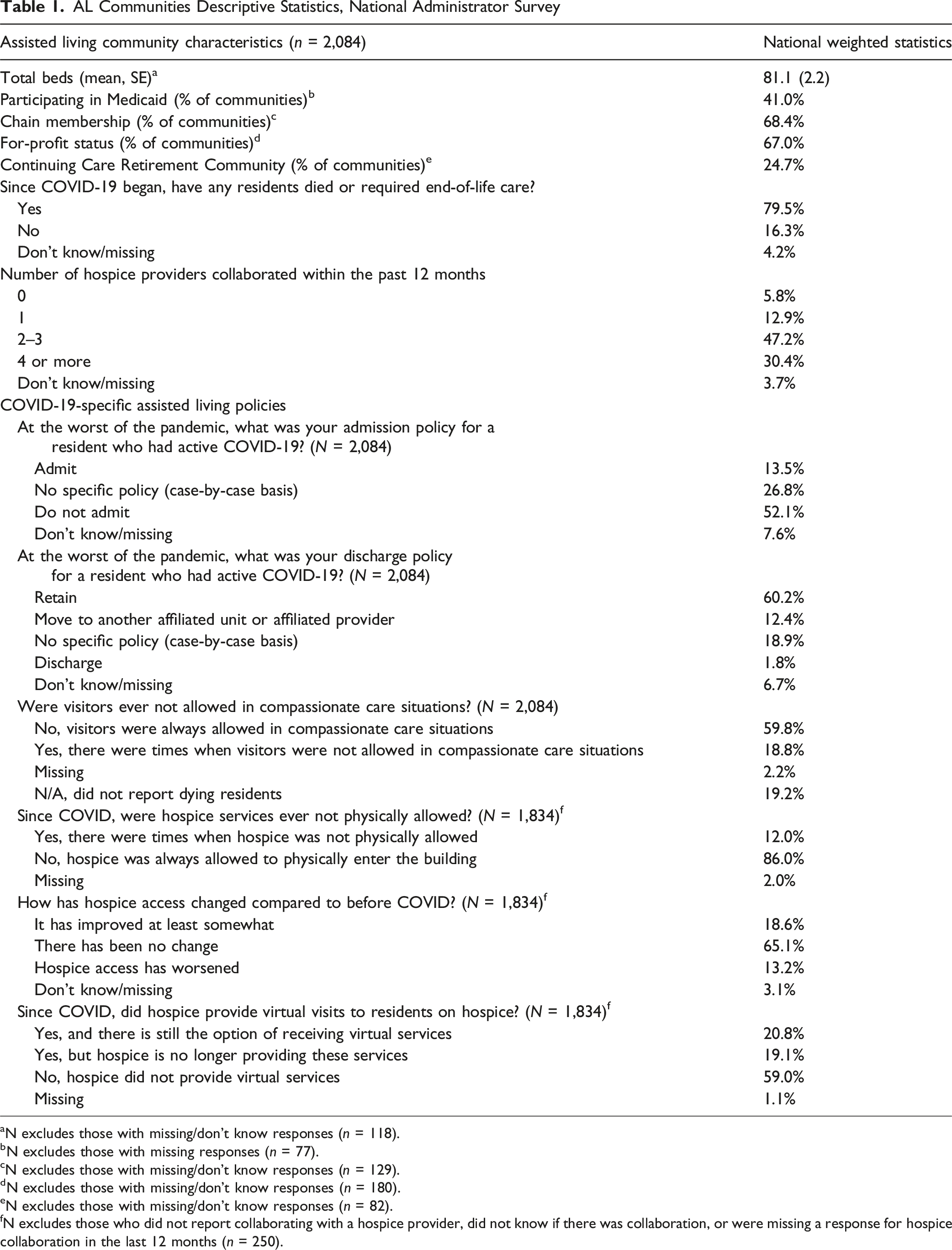
aN excludes those with missing/don’t know responses (n = 118).
bN excludes those with missing responses (n = 77).
cN excludes those with missing/don’t know responses (n = 129).
dN excludes those with missing/don’t know responses (n = 180).
eN excludes those with missing/don’t know responses (n = 82).
fN excludes those who did not report collaborating with a hospice provider, did not know if there was collaboration, or were missing a response for hospice collaboration in the last 12 months (n = 250).
The primary author analyzed survey data in Stata 18.0 using descriptive statistics. Two binary indicators reflected admission (admit, case-by-case, do not admit) and discharge (retain, case-by-case, move to affiliated unit, discharge) policies during the administrator-defined “worst” of the pandemic. When policies differed between memory care and general AL services, the least restrictive policy is reported. Sampling weights adjusted by license type, state, and nonresponse bias to represent large AL communities ( ≥ 25 beds) across state registries nationwide. Survey-weighted Wald F-tests estimated differences in reported resident deaths by discharge policies and compared policies by reported hospice access.
Qualitative Data Collection and Analysis
We used purposeful sampling to recruit diverse next of kin of AL community decedents who died between 2020 and 2022, sourcing from communities whose administrators completed the survey. Sampling ensured variation by hospice regulations, census region, and racial/ethnic composition. To oversample racial and ethnic minorities, we prioritized AL communities with higher proportions of these populations based on Medicare claims. A master’s-level analyst identified deceased residents whose public obituary named the AL as their place of residence or death. We obtained an IRB waiver and contacted next of kin using information from public records ≥ 3 months after their relative’s death was reported, consistent with participant identification methods in other bereavement studies (Neal et al., 1996). Recruitment involved mailing study information followed by phone calls. Research assistants explained the study, obtained informed consent, permission to record, and provided a $50 gift card for a one-hour interview.
Semi-structured interview questions, adapted from Shield et al. (2010), included open-ended questions on the decedent’s last year of life, hospitalizations or transfers, hospice use and quality, and how the COVID-19 pandemic shaped end-of-life experiences. No non-participants were present. Interviewers included faculty researchers, a doctoral candidate researcher, and trained qualitative staff, who conducted interviews between 2022 and 2023. All interviewers were female, except one, and all had prior qualitative interviewing and research training. Interviewers had no prior relationships with participants. Recruitment and interviewing occurred from October 2022 to September 2023. Of all individuals contacted, 12% were reached; among those reached, 5% were lost to follow-up, 15% were ineligible, 31% declined, and 49% participated.
Transcripts were generated using Otter.ai, reviewed against audio recordings for accuracy, emotional cues, and de-identification. Interviewers maintained an audit trail and discussed details and reflexive considerations at weekly meetings throughout data collection (Creswell & Plano Clark, 2017). We used NVivo 12 Plus software to organize transcripts, manually code them, compare coding across team members, link AL community survey data, and generate detailed reports of how manual codes intersected with each other and with survey data. The research team developed a codebook through inductive content analysis of 10 interviews, with some a priori research-based codes. Four researchers coded the remaining interviews in pairs, applying refined inclusion/exclusion criteria to promote consistency and meeting regularly to reconcile discrepancies through consensus. The codebook contained parent codes on AL communities' end-of-life care during COVID-19 and subcodes for visitation restrictions, communication, and miscellaneous COVID-19-related data. Codes selected for further thematic analysis pertain to the study’s research question (Braun & Clarke, 2006). Team discussions drove coding decisions and highlighted themes (Miles et al., 2020). We stopped data analysis once we reached saturation after 30 interviews. Saturation was defined as the point at which additional data yield no new information or themes (Fusch & Ness, 2015). Illustrative quotes that support major themes are labeled with participant ID, decedent’s age, and chronic conditions reported by next of kin.
Integration and Mixing of Quantitative and Qualitative Data
Quantitative and qualitative data were analyzed separately before mixing during interpretation. Using the NVivo query function, we stratified next-of-kin interview excerpts by administrator-reported admission, discharge, visitation, and hospice policies during COVID-19. The resulting matrices aligned thematic findings with policy data, providing structure when analyzing and interpreting integrated data. These comparisons added depth and nuance to our findings.
Results
Quantitative Findings: Administrator Survey of COVID-19 Policies and Processes
Proportion of AL Communities Reporting Dying Residents and their Admission/Discharge Policies

Nearly all administrator surveys (94.6%) were completed between 2022 and 2023, after managing the pandemic for over a year. During the worst of the pandemic, most (59.8%) reported following policies allowing compassionate care visits; 18.8% reported restricting them; 2.2% were missing a response; and 19.2% reported no dying residents since the pandemic began. Hospice-related responses are included for communities with completed questionnaires and at least one reported hospice partnership in the prior year (N = 1,834). Most of these administrators (86.0%) reported unrestricted on-site hospice access, while 12.0% imposed restrictions. One-fifth (20.8%) of all communities offered virtual hospice services that remained available; 19.1% offered them but discontinued them; and 59.0% never offered them during the pandemic. Responses indicated hospice access improved in 18.6% of communities, remained unchanged in 65.1%, and worsened in 13.2%. Administrators noting worsened hospice access were more likely to report resident deaths in the past year (91.0% vs. 84.7%; F (1,158) = 9.2, p = .003). During the worst of the pandemic, these administrators also more frequently reported restricting on-site hospice services (14.8 vs. 11.7%; F (1,158) = 1.6, p = .2) and compassionate care visitation (28.5% vs. 22.9%; F (1,149) = 2.7, p = .1), although these differences were not statistically significant.
Qualitative Findings: Bereaved Next-of-Kin Perceptions of Quality of Dying
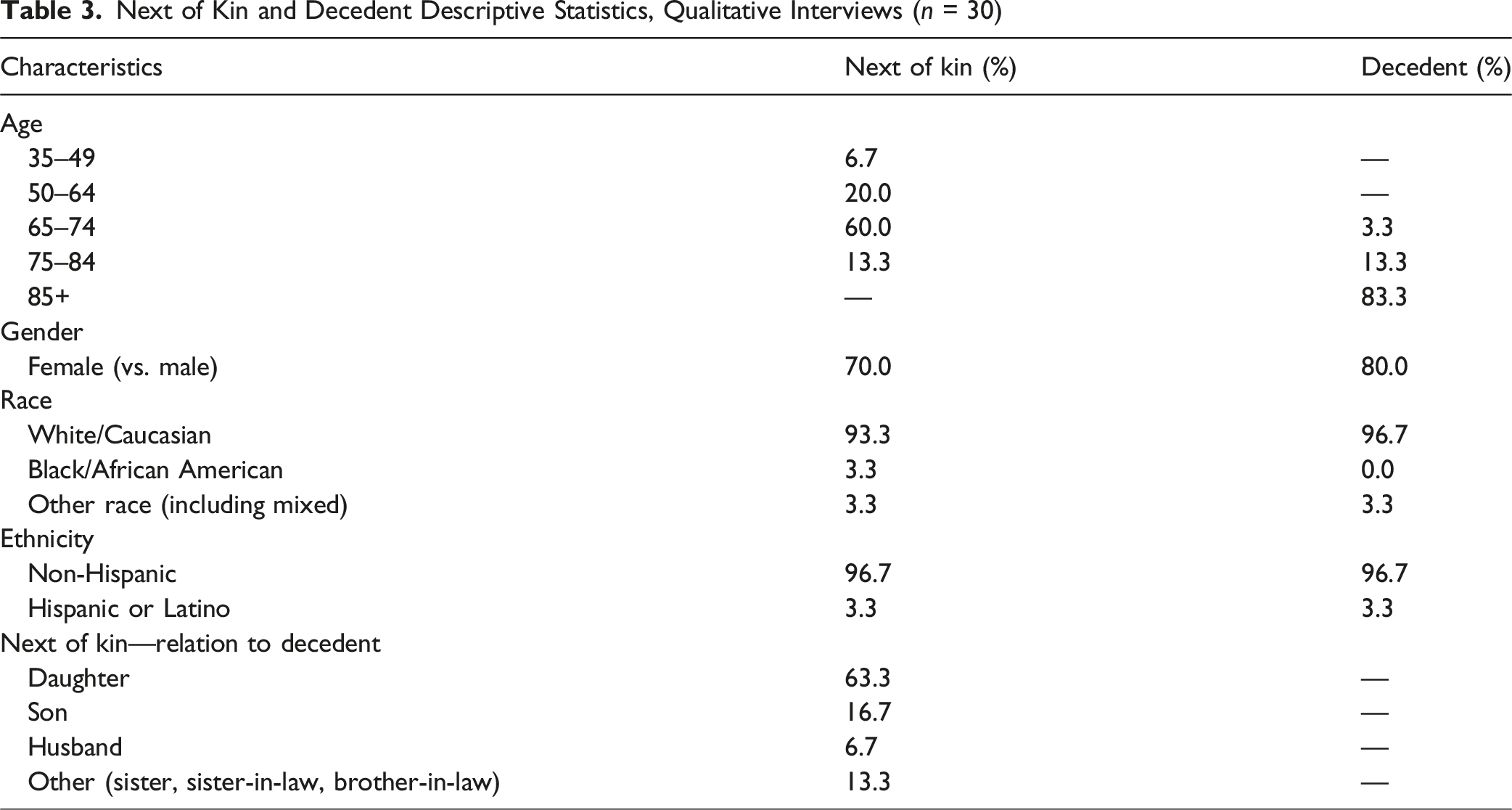
Next of Kin and Decedent Descriptive Statistics, Qualitative Interviews (n = 30)
Theme 1: Quarantine, Service Restrictions, and Limited Socialization Shaped End-of-Life Quality
Next of kin noted that social activities and visitation were essential for residents’ quality of life, but both were restricted during the pandemic. Outbreaks often prevented visitation during the residents’ final months. [For the year before] he died… […] Every other week or every other month, there was a-you know, reopening [and] closing again. Outside only [visitation], maybe inside. You know, it changed. Often. (Participant 173; decedent age 85–94, dementia and vision loss)
COVID-19-related restrictions on visitation, communal activities, and supportive services curtailed shared experiences between dying residents and next of kin. One participant described COVID-19-specific dining policies: “Nobody was allowed in the dining room unless you were a staff or a resident. You know, there was a time when I could have eaten with her, but the last [few] years of her life, no” (Participant 311; decedent age 95+, dementia, vision and hearing loss). Volunteer-led activities, including music, therapy animals, and other entertainment, were halted or modified during outbreaks. As a result, most participants reported no or modified social events during outbreaks, although some reported hallway programming or one-on-one interactions with staff when capacity allowed. Participants reported declines in residents’ physical, mental, and social well-being during disruptions to visitation and healthcare access. Couldn’t transport them […] Consequently, his hearing aids had an issue. I couldn’t do anything with them. You know, they are hearing aids that have to be tested by an audiologist, and so he ended up without hearing aids, you know, for 6 months […] his bottom teeth started falling out, but I couldn’t take him because the dentist wasn’t taking anybody. (Participant 1; decedent age 85–94, dementia, hearing loss)
Visitor and external-provider restrictions posed challenges in maintaining hearing and other assistive devices. Though experiences varied, several participants described missed or delayed specialty care, particularly dental and hearing services. [Dying during] COVID meant I couldn’t go in to see her. The things that I used to do for her […] No one at the facility knew how to change the batteries […] or the wax filters. So, she would call crying because she didn’t understand why her hearing aids weren’t working. And she was afraid. And she just didn’t remember that it was a question of changing the battery. This was in the last year, year and a half of her life. (Participant 42; decedent age 95+, dementia, heart/lung disease, hearing loss)
Nearly all next of kin reported being fully restricted from entering the AL at some point during the pandemic; only a few reported otherwise. Participants described the emotional toll of prolonged isolation at the end of life. The cost was pretty high, in terms of the lack of socialization. I mean, you couldn’t put a price on that […] Mom would say, often, “This was not how I planned to spend my last years, you know, being isolated like this.” (Participant 315; decedent age 85–94, no chronic conditions reported)
Theme 2: Restricted and Challenging Social Interactions Improved After Electing Hospice
During more restricted visitation, video and phone calls were vital for communication. One participant recalled the 9 months before her mother died in early 2022: They had a notebook or a tablet that we could Zoom with her, and they would set it up in her apartment, and contact us, and so we would visit with her […] Given the obstacles that COVID presented us, you know, we were pleased with the communication. (Participant 146; decedent age 95+, liver/kidney disease)
Next of kin appreciated Zoom and phone calls but some found them difficult, particularly for residents with hearing loss or dementia. One participant recalled: I can’t remember how many weeks all I could do is talk to her on the phone. And of course, talking to a person with dementia on the phone - how does that work? You know, she sort of knows and sort of doesn’t. […] probably harder on the family, on me. (Participant 239; decedent age 85–94, dementia)
Another described seeing their mother after 3 years of visitation restrictions; her hearing and vision loss made calls difficult, and when visitation resumed, distancing and PPE shaped experiences: As all of those things were failing, to make her sit six feet from us with a mask and try to visit with her- it was screaming. It was terrible […] they had her visitors talking into a […] megaphone […] It was humiliating […] and some of that lasted through- I would say to the end. (Participant 311; decedent age 95+, dementia, vision and hearing loss)
Participants noted limitations on the number of visitors, screening and distancing procedures, and challenges following safety protocols. Certain families and residents reported emotional difficulties after prolonged lockdowns. I couldn’t go in for several months [before her death]. […] And what was hard is, with the dementia, when we did get to go see her […] they’d open the window and would talk through the screen all masked […] She really lost us during COVID. She was, like, afraid of us at first, when we started visiting her again. Because she- she didn’t know us. (Participant 39; decedent age 95+, dementia)
In some instances, COVID-19-related policies shaped their final visit. One participant and her spouse described their final visit: They did allow us to gown up and wear our mask and go see him [outside his window] […] No one was allowed to go in there […] It was a very hard way to, you know, let him go. He was very emotional. He was having a hard time breathing. […] He was getting ready to go. And you know, of course, as his family, we were real emotional about it and-and wanted to encourage him and support him and hug him and [Husband: We couldn’t be there.] (Participant 2; decedent age 85–94, heart/lung disease)
Visitation restrictions notably eased with hospice involvement. One described his wife’s care improving: “[...] got more services […] I was allowed to go see her and feed her” (Participant 174; decedent 75–84, with dementia). Another contrasted general policies against more lenient hospice visitation: We only got to go inside and visit her three times. […] When hospice took over, the last month of her life, of course they had to let me in. And so I got to go in as much as I wanted to, at least at least two, maybe sometimes three times a week. (Participant 19; decedent age 65–74, dementia)
Most decedents received some hospice services, while a few did not because the decedent’s health decline happened more quickly than anticipated.
Theme 3: The COVID-19 Pandemic Exacerbated Staffing Shortages; Hospice Improved Resident Support and Communication
Next of kin discussed how pandemic staffing shortages shaped care delivery and communication, often delaying resident routines when employees were out sick. For the last year of her life, and you gotta keep in mind, it was COVID time […] [Workers] would be out sick […] They couldn’t always replace the care. There were times when I would be frustrated if she was still in bed [after breakfast] cause she couldn’t get out of bed by herself. (Participant 247; decedent age 85–94, heart/lung disease, liver/kidney disease)
One participant noted that staffing shortages, a common issue before the pandemic, worsened afterward: “[Staffing problems] got worse after COVID because they […] found out they could do with less staff, so they didn’t refill uh, positions” (Participant 311; decedent age 95+, dementia, vision and hearing loss). Only a small set of participants noted that staff were consistently available when residents needed them. Participants often described understaffing, especially at night. Reports included residents falling at night, not being discovered until morning, and participants not being notified. Several days prior to me talking to her on the phone and realizing that she didn’t sound well […] she admitted, well, it might have all started when she spent the night on the bathroom floor. […] Staff didn’t find her until they went to check, you know, the next morning […] I got [the AL] to send her to the hospital […] She had COVID […] There wasn’t a coming back from it. (Participant 315; decedent age 85–94, no chronic conditions reported)
Many participants described hospice services as supplementing AL staffing by providing more consistent status updates and closer oversight than AL staff, thereby increasing confidence in the resident’s care during lockdowns. “They have fewer patients, they’re able to focus on them more. They just were there [more than the AL nurses]. They called me all the time, giving me updates on his condition” (Participant 29; decedent age 75–84, dementia, liver/kidney disease).
Theme 4: End-of-Life Hospitalization-Related Challenges Included Difficulty Advocating for Decedents, Communication Failures, and COVID-19 Risk
Most next of kin discussed at least one end-of-life hospitalization and difficulties advocating for residents during lockdowns. One described their mother falling multiple times in an afternoon while AL staff disagreed on whether hospitalization was necessary: I couldn’t go in there […] [The nurse] said, “She probably needs to go to the hospital.” […] [The executive director] said, “I don’t think she needs to go.” […] It’s COVID. What-What am I supposed to do? […] She spent four days in the hospital. You know, [the executive director] didn’t think she needed to go. He didn’t know her very well. […] I took her to the emergency room three times in 4 days, in the last few days of her life, because she kept slipping out of her chair. (Participant 42; decedent age: 95+, dementia, heart/lung disease)
Participants reported that hospital settings increased COVID-19 risk and described limited communication from hospitals about the decedents’ test results and health status. One participant described their mother’s COVID-19 diagnosis: Through all that COVID, I had kept my mother very protected. And she did not get COVID […] She told me that they had put a COVID-positive patient in the room with her [at the hospital] […] I never got a call [about her test results after requesting them]. […] I got a phone call from her insurance company saying she's COVID positive […] [she] was in isolation for two weeks, had a stroke, and never really came out of that. (Participant 304; decedent age 75–84, liver/kidney disease, vision loss)
Participants said decedents often preferred to die in place. However, some experienced end-of-life hospitalizations: She [fell and] was sent to the hospital […] This was a DNR patient. And she was in their hospice care. So they should have left her at [the AL] and let things take its course. […] like less than a week, or like four or five days, she gradually went down [and passed away]. (Participant 174; decedent age 75–84, dementia)
Participants attributed transfers to provider recommendations, limited AL services, and care needs better addressed in nursing homes or inpatient hospices.
Mixing Quantitative and Qualitative Data: The COVID-19 Pandemic Made the End-of-Life Period More Challenging
The AL administrator survey highlights variation in admission and discharge policies for COVID-19 cases and whether hospice services were maintained on-site or virtually. Bereaved next of kin shared struggles with understaffing, restricted visitation, and infection prevention policies that limited dying residents’ quality of life. Interviewees expressed that hospice services often helped mitigate staffing issues. Most administrators reported allowing compassionate care visits for dying residents throughout the pandemic; yet interviewees described prolonged visitation limits during outbreaks. Administrators reported hospice services were largely maintained, but next of kin noted issues accessing other services including audiology, vision, dentistry, and daily care usually provided by loved ones.
Discussion
This study demonstrates that COVID-19 infection control policies deeply shaped dying residents’ and families’ experiences. Few studies have examined AL communities' COVID-19 policies beyond the pandemic’s onset (Chen et al., 2020; Zimmerman et al., 2020). Administrators reported varied admission and retention for COVID-19 cases during the worst of the pandemic, while next-of-kin interviews across 25 states highlighted consistent challenges tied to ever-changing infection control measures, particularly visitation and distancing. Although most administrators reported permitting end-of-life visitation, next of kin described restrictions limiting meaningful connection, emphasizing the need for resident-centered policies. These findings raise ethical concerns and underscore the importance of holistic, dignity-, and safety-focused policies (Kemp et al., 2022).
Healthcare services were reportedly limited at times during the pandemic, including audiology, vision, and dental. Before restrictions, next of kin and other visitors provided routine care, including hearing aid maintenance and daily assistance. The loss of this support is not well understood, as little research has examined AL resident outcomes during the pandemic. Two studies reported greater antipsychotic use, functional decline, and depression in AL communities and nursing homes during the pandemic (Barnett et al., 2022; Hoben et al., 2023). Further research should explore how healthcare access disruptions impacted residents and strategies to maintain essential services during outbreaks.
Virtual tools like Zoom reduced isolation during lockdowns, but some residents with dementia or hearing impairments struggled with technology, PPE, and distancing. Non-AL dementia and audiology studies acknowledge these difficulties (Talbot & Briggs, 2022; Ten Hulzen & Fabry, 2020). Residents with dementia face greater risks of depression and isolation (Boamah et al., 2021). State agencies should align visitation restrictions with residents’ diagnoses and prognoses, allowing for personalized communication plans. Although supplies were limited early in the pandemic, ensuring access to evidence-based resources—such as personal protective equipment and improved ventilation (National Center for Immunization and Respiratory Diseases, 2023)—could help state agencies and assisted living communities support safe, in-person end-of-life visitation during future outbreaks.
Visitation restrictions challenged the next of kin in advocating for residents’ well-being. Next-of-kin engagement may shape residents’ well-being (Kemp et al., 2021). Expanded telehealth could enhance advocacy during lockdowns. During the worst of the pandemic, many AL communities retained but did not admit COVID-19-positive patients. Next of kin noted residents often contracted COVID-19 during hospitalizations. Future preparedness efforts should include reintegration protocols for hospitalized residents with tiered quarantining based on vaccinations, exposure, and prognosis (Centers for Disease Control and Prevention, 2024).
Next of kin described end-of-life hospitalizations stemming from AL service and staffing limitations, with shortages leading to communication issues and care lapses. Studies highlight critical AL staffing challenges during the pandemic (Bahr et al., 2023; Kyler-Yano et al., 2022). Hospice helped mitigate staffing issues, and most administrators reported consistently allowing on-site hospice services. Training and resources to manage medical needs onsite may help reduce late-life transitions and support dying in place. During future outbreaks, state agencies should prioritize hospice in AL communities to potentially reduce the impacts of staffing shortages on dying residents.
This study’s strengths include a larger, more geographically diverse sample of AL residents’ end-of-life experiences than previous qualitative studies (Ball et al., 2014; Dobbs et al., 2006; Munn et al., 2008). However, several limitations are notable. Frequent changes in federal and state COVID-19 guidance complicated accurate assessment, and administrators’ responses may reflect social desirability. Repeated periods of staffing shortages, outbreaks, and mortality may have made it challenging for administrators to identify the “worst” period.
We did not track each AL community’s precise policies implemented over the project duration, because this was beyond the study’s scope and considered impossible to do accurately using a cross-sectional survey administered over 2 years. The qualitative sample included next of kin of residents who died between 2020 and 2022, though individual exposure to reported policies is unknown. Regional variation in infection rates, a significant contextual factor potentially influencing perspectives and policy implementation, was also not captured, as our focus was on administrator-reported policies during what they perceived to be the “worst” of the pandemic.
Despite rigorous qualitative methods, including recruiting geographically diverse participants, double-coding, and a detailed audit trail, the transferability of the findings may be limited by pandemic-related circumstances, as the “worst” period reported by administrators may have differed. Additional perspectives, including hospice staff and other AL employees, may further contextualize AL end-of-life experiences. We included large communities ( ≥ 25 beds) to ensure comparable licensing and regulations. Future research should examine how COVID-19 policies shaped end-of-life care in smaller communities facing distinct regulatory and care challenges. A consensus study could help develop evidence-based recommendations for state regulatory agencies regarding AL end-of-life care policies during high-mortality outbreaks. We did not conduct participant checking of transcripts or our findings, a COREQ-recommended practice; however, iterative, team-based coding helped improve the rigor of analysis.
Conclusions
Our findings indicate COVID-19 policies shaped AL residents’ end-of-life experiences. Bereaved next of kin noted that visitation, socialization, and service restrictions diminished the quality of dying. Future research should identify infection control practices that preserve connection while balancing safety concerns. To support high-quality care during outbreaks, state agencies and AL administrators should consider broader compassionate care policies to promote meaningful interactions and quality time with loved ones.
Supplemental Material
Supplemental Material - A Mixed-Methods Study of End-of-Life Care in Assisted Living During the COVID-19 Pandemic: National Survey of Administrators and In-Depth Interviews With Bereaved Next of Kin
Supplemental Material for A Mixed-Methods Study of End-of-Life Care in Assisted Living During the COVID-19 Pandemic: National Survey of Administrators and In-Depth Interviews With Bereaved Next of Kin by Jacy Weems, Grace Reed, Emily A. Gadbois, Elyse Couch, Joan M. Teno, Kali S. Thomas, Melissa A. Clark, and Emmanuelle Belanger in Journal of Applied Gerontology.
Footnotes
Acknowledgements
We would like to thank all of the next of kin who participated in our interviews for their time and for sharing their experiences, as well as the administrators who voluntarily completed our survey. We would also like to acknowledge members of the qualitative research team, including Cindy Williams for her administrative support, Nikki Dagen for her assistance with coding verification, and Jeffrey Turner and Joan Brazier who helped perform interviews and provided additional administrative support.
ORCID iDs
Ethical Considerations
This study was approved by the Brown University Institutional Review Board (IRB protocol/Human Subjects Approval Number: 2599) on November 22, 2022. An exempt determination was made for the administrator survey on December 20, 2019, as the survey did not ask for personal identifiable information. The survey distributed to assisted living administrators included information on how their responses would be used.
Consent to Participate
Informed consent was obtained verbally from next of kin before their participation in the audio-recorded interviews.
Author Contributions
Conceptualization: J. Weems, G. Reed, E.A. Gadbois, E. Couch, K.S. Thomas, J. Teno, M.A. Clark, and E. Belanger. Data Curation: J. Weems, G. Reed, E.A. Gadbois, E. Couch, K.S. Thomas, M.A. Clark, and E. Belanger. Formal Analysis: J. Weems, G. Reed, E.A. Gadbois, E. Couch, K.S. Thomas, J. Teno, M.A. Clark, and E. Belanger. Funding Acquisition: K.S. Thomas, M.A. Clark, J. Teno, and E. Belanger. Investigation: J. Weems, G. Reed, M.A. Clark, and E. Belanger. Methodology: J. Weems, K.S. Thomas, J. Teno, M.A. Clark, and E. Belanger. Project Administration: J. Weems, G. Reed, and E. Belanger. Supervision: E. Belanger. Writing—original draft: J. Weems, G. Reed, and E. Belanger. Writing—review and editing: J. Weems, G. Reed, E.A. Gadbois, E. Couch, K.S. Thomas, M.A. Clark, J. Teno, and E. Belanger.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under Award Number R01AG066902. The funders played no part in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. JW was funded as a predoctoral fellow through NIA T32AG023482-18 while developing this manuscript and presented preliminary findings at the 2024 AcademyHealth Annual Research Conference, Baltimore, MD.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
In accordance with resource sharing guidelines published by the National Institutes on Aging, the survey data will be made available in an aggregated, anonymized fashion at the end of the study period. Additional study documentation is available: ![]() . In-depth interviews will not be made available to ensure protection of participant anonymity and to not inadvertently reveal identifiable information.
. In-depth interviews will not be made available to ensure protection of participant anonymity and to not inadvertently reveal identifiable information.
Supplemental Material
Supplemental material for this article is available online.