
Abstract
This study examined the associations between cognition and depressive symptoms, function, and pain among hospitalized older patients with dementia. We utilized baseline data of 461 hospitalized older patients with dementia who participated in an intervention study implementing Family-centered Function-focused Care (Fam-FFC) and conducted stepwise linear regression. On average, the participants (males = 189; 41% and females = 272; 59%) were 81.64 years old (Standard Deviation, SD = 8.38). There was a statistically significant association of cognition with depressive symptoms (b = −0.184, p < .001), functional status (b = 1.324, p < .001), and pain (b = −0.045, p < .001) when controlling for covariates. This study utilized a large sample of a relatively underrepresented population, hospitalized older adults with dementia, and addressed a topic with great clinical significance. Specific focus on testing and implementing best practices or interventions to support the clinical outcomes, and the cognitive function of hospitalized older adults with dementia is warranted in both practice and research.
• Better cognition is associated with lower depressive symptoms, greater functional independence, and lower observed pain in hospitalized older adults with dementia • Interventions or activities are needed to support cognitive function of hospitalized older adults with dementia • Best practices or interventions are also needed to manage depressive symptoms, optimize function, and manage pain among hospitalized older adults with dementia
• Nurses caring for older adults in acute care settings need to remember to be sensitive to cognitive impairment and work collaboratively with patients and/or families to find best ways to improve mood, optimize function, and manage pain among hospitalized older patients with dementia • Continued efforts are needed in testing and implementing best practices or interventions to improve mood, optimize function, and manage pain among hospitalized older adults with dementia; and in reviewing policies and practices pertaining to availability and use of the interventionsWhat this paper adds
Applications of study findings
Background
An estimated 6.5 million Americans aged 65 and older are living with Alzheimer’s disease or a related dementia (ADRD) and this number has been continually on the rise (Alzheimer’s Association, 2022). Persons with ADRD are estimated to have twice the likelihood of hospitalizations compared to those without ADRD (Shepherd et al., 2019; Sommerlad et al., 2019). The combination of gradual physical and cognitive decline and the co-existing medical conditions such as hypertension, congestive heart failure, chronic obstructive pulmonary disease, and diabetes among the persons with ADRD often leads to falls, infection, or other acute issues which then contribute to hospitalization (Shepherd et al., 2019; Taylor et al., 2020).
Hospitalization among older adults with ADRD negatively impacts their cognitive functioning and could result in protracted cognitive decline (Fogg et al., 2018; Sprung et al., 2021). The cognitive decline during hospitalization is related to important clinical outcomes such as depressive symptoms, function, and pain among older adults. For example, prior research has noted a significant association between depression and cognitive impairment among older adults including hospitalized older adults (Brenowitz et al., 2021; Zou et al., 2018); higher depressive symptoms were associated with lower cognition, more cognitive deficits, and faster rate of cognitive decline (Brenowitz et al., 2021; Helvik et al., 2013). Similarly, evidence shows that older adults develop functional decline during hospitalization (Fogg et al., 2018; Hartley et al., 2017) and that cognitive impairment among older adults contributes to functional decline during hospitalization (Hartley et al., 2017; Pedone et al., 2005); a meta-analysis also reported that cognitive impairment is associated with greater risk of functional decline among hospitalized older adults (Hartley et al., 2017). Further, while the evidence is limited, some prior work has shown that hospitalized older adults with pain demonstrate low cognition (Corsi et al., 2018; Fogg et al., 2018) and that chronic pain is associated with cognitive decline (Corsi et al., 2018; Domenichiello & Ramsden, 2019).
Depressive symptoms, functional status, and pain are salient measures of quality of life of older adults with dementia, including hospitalized older adults with dementia. While there is some evidence to support the association between cognitive impairment and the clinical outcomes—depressive symptoms, functional status, and pain among hospitalized older adults, the association between cognitive impairment and these clinical outcomes among hospitalized older adults with dementia is particularly unclear. Therefore, the purpose of this study was to examine the association between cognition and depressive symptoms, function, and pain among hospitalized older patients living with dementia. It was hypothesized that cognitive impairment is associated with depressive symptoms, function, and pain among hospitalized older patients living with dementia while controlling for age, gender, race, and comorbidities. Patient demographics including age, gender, race, and comorbidities are commonly found to be associated with depression, function, and pain among older adults and as intrinsic factors with possible influence are used as covariates (Brenowitz et al., 2021; Corsi et al., 2018; Domenichiello & Ramsden, 2019; Hartley et al., 2017; Pedone et al., 2005; Zou et al., 2018). Findings from this study will advance our understanding of the association between cognitive impairment and depressive symptoms, function, and pain in hospitalized dementia population. It can also help to remind care staff about the need for greater attention to cognitive impairment, and the simultaneous change in the clinical outcomes during hospitalization of the older adults with dementia.
Methods
Study design and sample
This study was a secondary data analysis using baseline data of 461 hospitalized older patients with dementia who participated in a cluster randomized controlled trial; ClinicalTrials.gov identifier: NCT03046121 (Boltz et al., 2018). The purpose of the parent study was to examine the efficacy of Fam-FFC (Family-centered Function-focused Care), a nurse-family caregiver partnership model that aims to improve: 1) the physical and cognitive recovery in hospitalized patients living with ADRD during hospitalization and 60-day post-acute period and 2) caregiver preparedness and experiences. The protocol has received institutional review board approval (STUDY00006201) and has been previously published (Boltz et al., 2018).
The sample in this study was comprised of patients from six medical units of three large community teaching hospitals in central Pennsylvania for whom informed consent was obtained. In the parent study, patients were eligible to participate if they: were ≥65 years, spoke English or Spanish, lived in the community prior to hospital admission, screened positive for dementia on scales with well-established psychometrics including the Montreal Cognitive Assessment, MoCA ≤ 25 (Nasreddine et al., 2005) and the Eight-item Informant Interview to Differentiate Aging and Dementia, AD8 ≥ 2 (Galvin et al., 2005), and had a diagnosis of very mild to moderate stage dementia based on a score of 0.5–2.0 on the Clinical Dementia Rating Scale, CDR (Morris, 1997). Functional ability was assessed with the Pfeffer Functional Activities Questionnaire (FAQ) to discriminate mild cognitive impairment from dementia; a disability score of 9 or more (i.e., some combination of total dependence and/or requiring assistance with functional activities) was considered to classify as dementia (Pfeffer et al., 1982).
Data collection and measures
Data were collected through a combination of chart review, interview of the patient/care partner with input from staff, and observation by trained and experienced research evaluators. Baseline data were used in this analysis, collected within 48 hours of admission to the unit (Boltz et al., 2018).
The covariates comprised of descriptive measures including the patient’s age, race, gender (identify as male/female), and comorbidities (classified with the Charlson Comorbidity Index (Van Doorn et al., 2001)). Data on the descriptive measures were extracted by the research evaluators through chart review.
The independent variable, cognition, was assessed by research evaluators through interview of the patient using the Montreal Cognitive Assessment, MoCA (Nasreddine et al., 2005). The MoCA is a 10-minute, 30-point cognitive screener designed to assist clinicians with detecting mild cognitive impairment among patients. It evaluates cognition through the domains of executive functioning, orientation, memory, abstract thinking, visuospatial abilities, language, and attention. An MoCA score of less than 26 is suggestive of mild cognitive impairment, while less than 18 suggests moderate and less than 10 severe impairment (Nasreddine et al., 2005).
The dependent variables included patient measures of depressive symptoms, functional status, and pain. The assessment of depressive symptoms among the patients was done by research evaluators through interview of care partner using the Cornell Scale for Depression in Dementia (CSDD). CSDD is a 19-item questionnaire which assesses the severity of depressive symptoms in those with dementia and has/demonstrated evidence of inter-rater reliability (Kw = .67), internal consistency (coefficient alpha: .84), and sensitivity (Alexopoulos et al., 1988). The total CSDD scores range from 0 to 38 and higher scores indicate more depressive symptoms; more specifically, a CSDD score greater than 18 indicates definite major depression, a score greater than 10 indicates probable major depression, while a score below 6 indicates absence of significant depressive symptoms.
The functional status of the patient was assessed by research evaluators through interview of the patient’s family care partner using the Barthel Index which includes 10 items related to self-care, mobility, and bowel/bladder functions (Mahoney & Barthel, 1965). The total scores range between 0 and 100 and higher scores suggest greater independence in functional activities. Prior work confirmed the internal consistency of the Barthel Index and provided support for inter-rater reliability and construct validity (Mahoney & Barthel, 1965; Sainsbury et al., 2005).
The patient’s pain was assessed by research evaluators through observation of patient using the Pain Assessment in Advanced Dementia (PAINAD) Scale (Warden et al., 2003). PAINAD is an observational measure consisting of five domains—breathing, negative vocalizations, facial expression, body language, and consolability. Each of these five domains is scored from 0 (no pain) to 2 (severe pain). The total possible score ranges from 0 to 10 and higher scores indicate greater pain severity. Prior testing provided the evidence of internal reliability in persons with dementia (α = .90), and strong inter-rater agreement (kappa = .74, p < 0.000) and concurrent validity (Kendall’s τ = .73, p < 0.000) for PAINAD (Mosele et al., 2012).
Data analysis
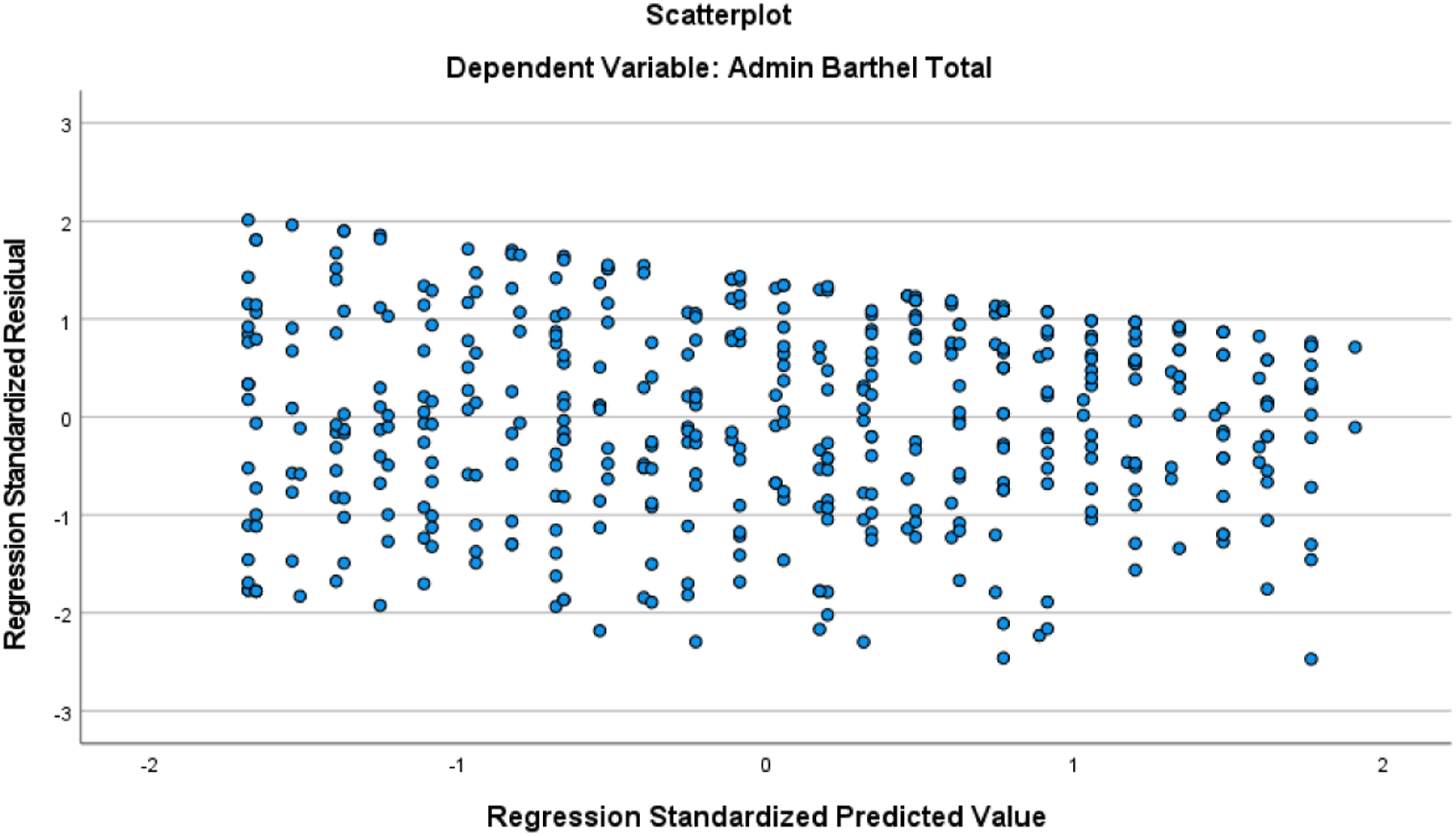
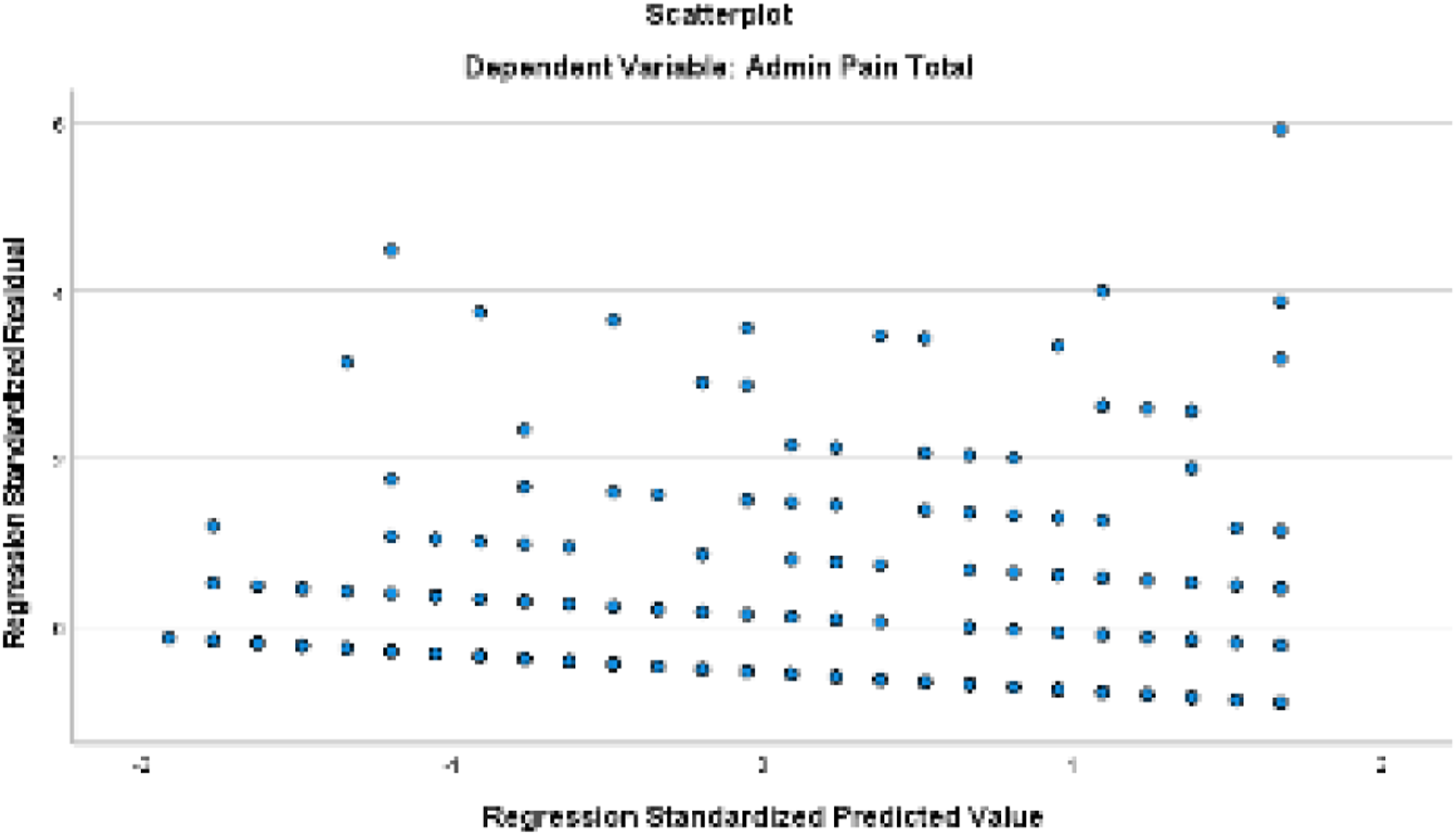
Data analyses were completed using the Statistical Package for the Social Sciences, SPSS version 28.0. We first explored the descriptive statistics to ascertain distributional characteristics, report participant characteristics, and to ensure that the assumptions associated with the planned statistical analyses were met. Following data check and descriptive reports, we conducted stepwise linear regression to test the proposed hypothesis. During stepwise regression, we used a step method of entry-level probability of F set at p = .05 and removal level at p = .10 for the predictor (cognition) and covariates (patient’s age, race, gender, and comorbidities); covariates were entered together as a block followed by the predictor. For regression analyses, we dichotomized race into White/Caucasian vs. African American/Black excluding the “Asian” and “more than one race” categories given there were only three participants in each of these excluded categories; our final sample included 455 participants. Three models were run separately to regress the same set of predictor (cognition) and covariates (patient’s age, race, gender, and comorbidities) on each outcome measure— depressive symptoms, function, and pain. Figures 1, 2, and 3 illustrate scatterplot of each model related to depressive symptoms, functional status, and pain, respectively. All analyses considered a p ≤ .05 level of significance. Scatterplot for model related to depressive symptoms. Scatterplot for model related to functional status. Scatterplot for model related to pain.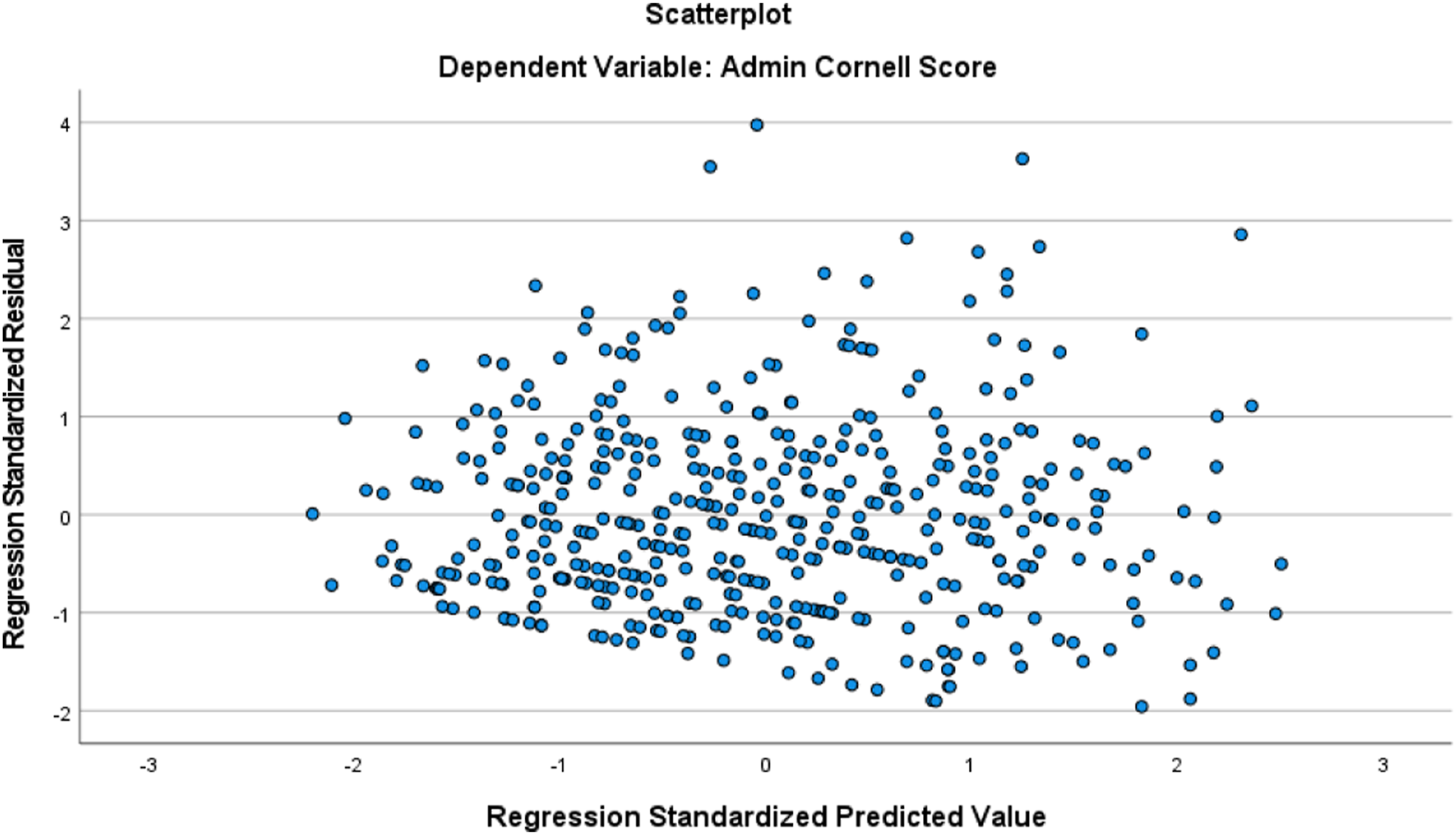
Results
Descriptive Characteristics of Study Participants.
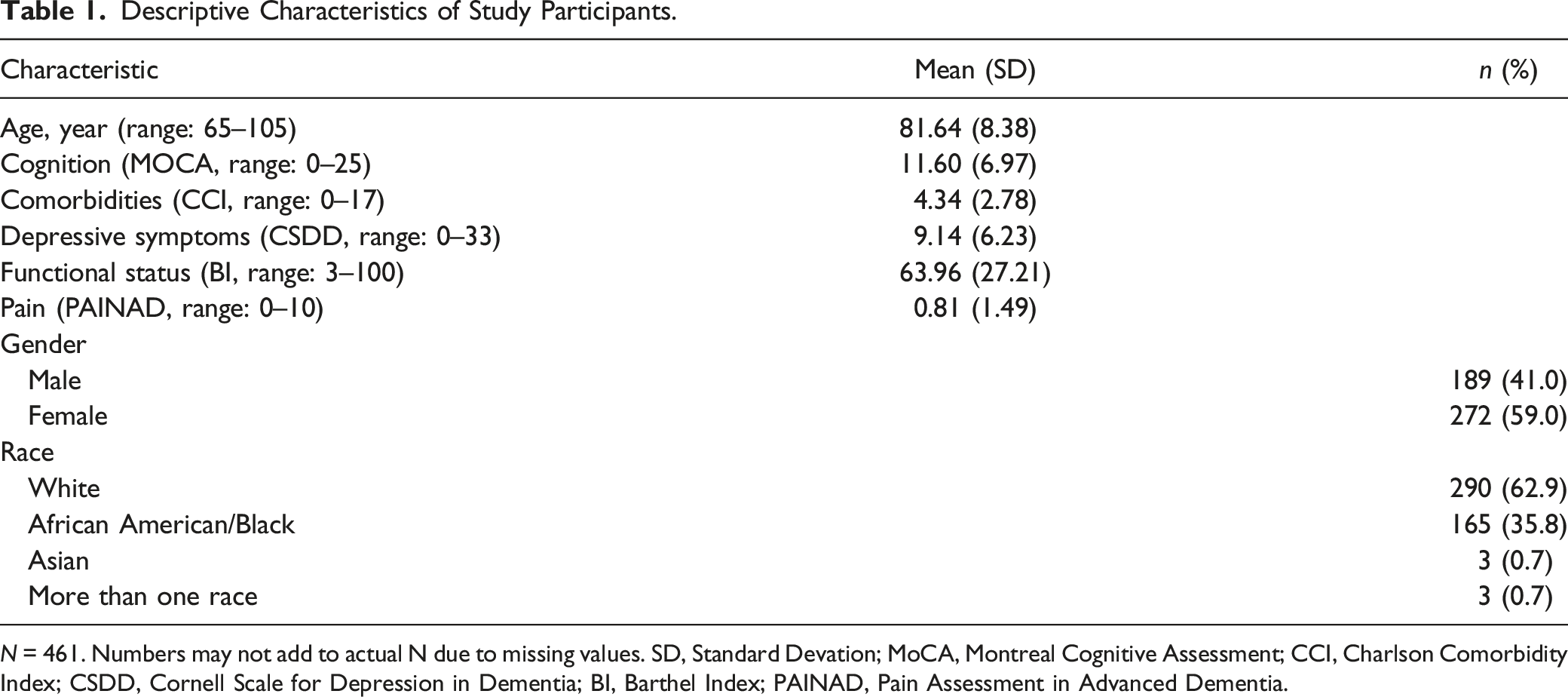
N = 461. Numbers may not add to actual N due to missing values. SD, Standard Devation; MoCA, Montreal Cognitive Assessment; CCI, Charlson Comorbidity Index; CSDD, Cornell Scale for Depression in Dementia; BI, Barthel Index; PAINAD, Pain Assessment in Advanced Dementia.
Results from Regression of Depressive Symptoms, Function, and Pain on Cognition.
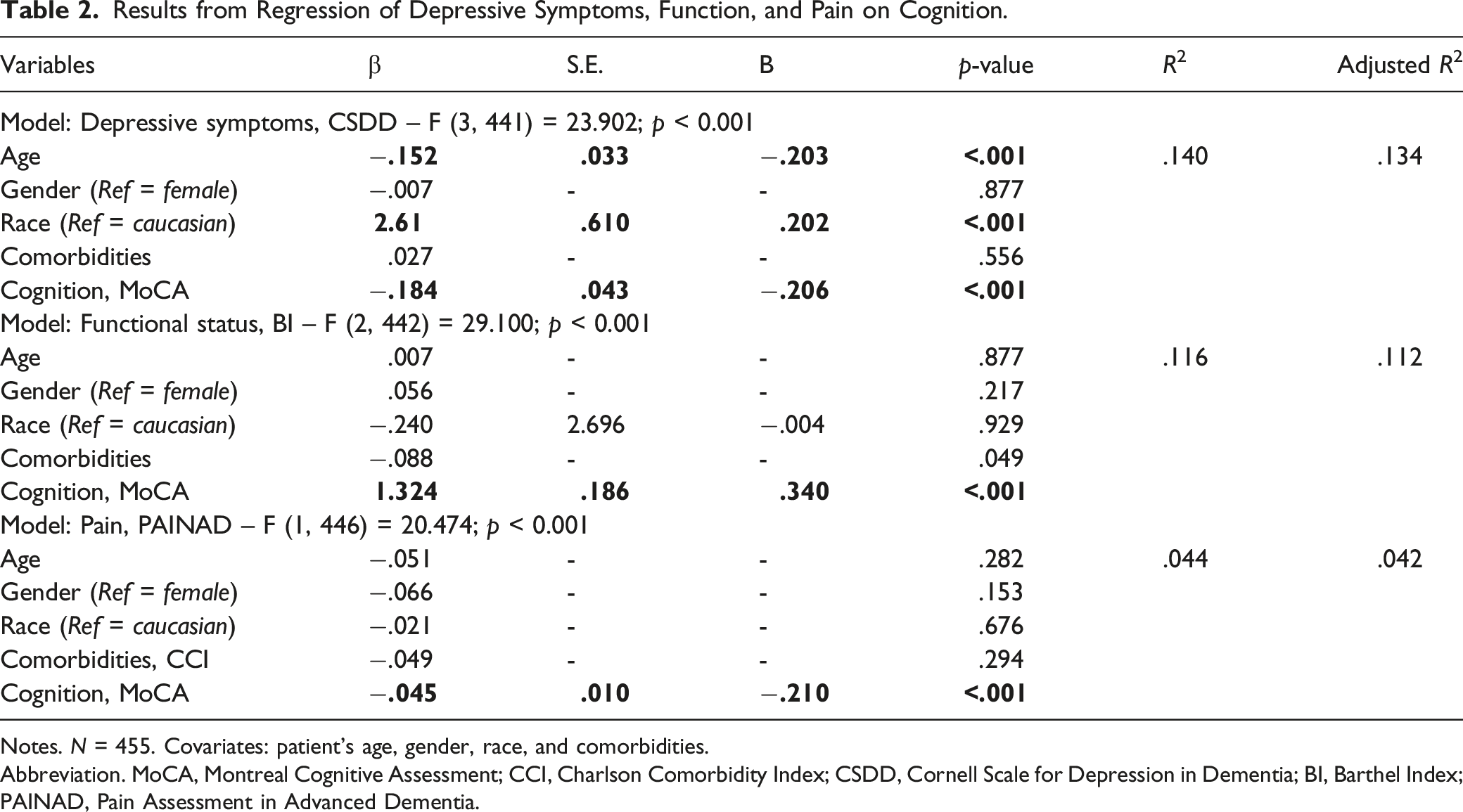
Notes. N = 455. Covariates: patient’s age, gender, race, and comorbidities.
Abbreviation. MoCA, Montreal Cognitive Assessment; CCI, Charlson Comorbidity Index; CSDD, Cornell Scale for Depression in Dementia; BI, Barthel Index; PAINAD, Pain Assessment in Advanced Dementia.
Discussion
The present study directly examined the association of cognitive impairment with depressive symptoms, functional status, and pain among hospitalized older patients with dementia. The hypothesis in this study was supported in that we found a significant association between cognitive impairment and depressive symptoms, functional status, and pain among hospitalized older patients with dementia when controlled for socio-demographic variables. Prior research also indicated the association between cognitive impairment and depressive symptoms, functional status, and pain among hospitalized older adults and these findings were replicated in hospitalized older patients with dementia in this study.
Consistent with prior research which indicated that cognitively impaired older adults have increased risk of depressive symptoms (Brenowitz et al., 2021; Helvik et al., 2013), we also found that lower cognitive functioning is associated with higher depressive symptoms among hospitalized older adults with dementia. Older adults with lower cognitive functioning might have lower social engagement and lack participation in self-care or other activities contributing to low and depressed mood. Hospitalization provides an opportunity to screen for depression and mobilize treatment to optimize health and quality of life. Treatment can include pharmacological interventions, non-pharmacological interventions, or some combination of both. Some non-pharmacological interventions reported to be effective in reducing depressive symptoms in older adults with dementia include music-based therapeutic interventions and psychological treatments such as the cognitive behavioral therapy (Kishita et al., 2020). Nurses caring for hospitalized older patients with dementia can also use approaches such as facilitating visits from friends and family, engaging patients in group activities (e.g., art or bingo), one-on-one interactions, providing quiet alone time as needed, and providing boardgames or other activity of choice to improve mood of hospitalized older adults with dementia.
Our findings indicated that lower cognition is associated with greater functional dependence among hospitalized older adults with dementia. This is in line with findings from prior work which indicated that cognitive impairment is associated with greater risk of functional decline among hospitalized older adults (Fogg et al., 2018; Hartley et al., 2017). Older adults with lower cognitive functioning might be more dependent or appear to be dependent on staff and engage less to none in self-care or other activities and thus the findings. Staff can incorporate routine walking schedules, stretching in bed, move of the day, or other creative activities in daily care routines to support functional ability of hospitalized older adults with dementia. More recent research has also emphasized function-promoting approaches (e.g., verbal and physical cueing) that are adapted to the specialized needs of persons with dementia, and promoting organizational capacity to meeting these needs (Boltz et al., 2015; Resnick et al., 2022). Continued efforts to test and implement such approaches are warranted in both practice and research.
Consistent with our findings, prior research has also noted that older adults with lower cognition tend to demonstrate more symptoms associated with pain (Corsi et al., 2018; Huang et al., 2022). Pain is a common and disabling experience among older adults (Corsi et al., 2018; Domenichiello & Ramsden, 2019) and therefore, care staff in hospital settings should be cognizant of pain among hospitalized older adults with dementia and provide appropriate pharmacological and/or non-pharmacological interventions to manage pain accordingly. This is particularly important because the progression of cognitive decline can affect the perception and the ability to verbalize/express the presence of pain among older adults with cognitive impairment or dementia, and thus, some older adults may perceive and verbalize/express pain less than others and vice versa (Cravello et al., 2019; Domenichiello & Ramsden, 2019). Non-pharmacological pain management approaches such as massages, exposure to heat or cold sources, vibratory therapy, music therapy, cognitive behavioral therapy, as well as alternative therapies like aromatherapy have been recommended for use independently or in combination to help reduce the intensity, duration, or frequency of pain symptoms in older adults with cognitive impairment (Cravello et al., 2019; Domenichiello & Ramsden, 2019). Nurses caring for hospitalized older patients with dementia can also develop a tailored pain intervention based on these non-pharmacological approaches.
Since cognitive impairment can significantly influence clinical outcomes such as depressive symptoms, function, and pain, future research should focus on testing and implementing best practices or interventions to support cognitive function of older adults, especially hospitalized older adults with dementia. For example, evidence suggests that physical activity and/or exercise could help to slow cognitive decline and thereby support cognitive function of older adults, particularly when combined with cognitive stimulation (Boltz, Chippendale, Resnick, & Galvin, 2015; Cui et al., 2018). Nurses or direct care staff in hospital settings could incorporate some form of physical activity and/or cognitive stimulation and engagement in daily care of older adults to optimize their cognitive functioning and thereby support clinical outcomes.
Strengths and Limitations
This study utilized a large sample of a relatively underrepresented population, hospitalized older adults with dementia, and provided useful information on a topic with limited direct attention, the association of cognitive impairment with important clinical outcomes in hospitalized older adults with dementia. Findings from this study are limited in that this secondary analysis utilized baseline data from a study conducted in hospitals of one state thus making the findings more specific to the sample and less generalizable to the overall older adult population or those with dementia. Future work can consider a more geographically diverse sample and confirm findings in the hospitalized dementia population. Additionally, this study included patient’s age, race, gender, and comorbidities as covariates and could have missed other important potential confounders including illness severity and reason for hospitalization. Future work can consider evaluating the discrete contribution of these and other potential confounders (e.g., acute illness and delirium). It should also be noted that the relationship between cognition and depressive symptoms, functional status, and pain is complex as these are not unidirectional variables, and causality cannot be established with the cross-sectional analysis. Longitudinal analysis is needed to assess change in the relationships over time. Furthermore, findings may also be biased due to social desirability during observations and recall bias during staff interviews for data collection.
Conclusion
This study provides valuable information, as well as important implications and directions for future work with regard to the relationship between cognitive impairment and multiple clinical outcomes including depressive symptoms, function, and pain among hospitalized older patients with dementia. Our findings can serve as a reminder that care staff need to be particularly sensitive to hospitalized older patients with cognitive impairment and work with the patients and their families to improve mood, optimize function, and manage pain in the hospitalized older patients with dementia. Continued evaluation of cognitive status of hospitalized older adults, and design and implementation of interventions to maintain cognitive function of hospitalized older adults with dementia is also important in both practice and research. From policy perspective, review of policies and practices pertaining to provision or use of interventions and activities to support cognitive function, as well as to improve mood, optimize function, and manage pain among older adults with dementia in hospital settings is both important and useful. Future research will be needed to identify the mechanisms of association between cognitive impairment and depressive symptoms, function, and pain in hospitalized older patients with dementia.
Footnotes
Author Note
IRB protocol/human subjects approval number The parent study was approved by the institutional review board at the Pennsylvania State University (STUDY00006201).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This secondary analysis utilized data from a randomized controlled trial supported by National Institutes of Health/National Institute on Aging under Grant R01AG054425 and R01AG054425-04S1.