
Abstract
We aimed to develop and test the psychometric properties of a new instrument to assess long-term care (LTC) home residents’ social connection. We developed a conceptual model and then used literature review and qualitative interviews to identify candidate items for the Social Connection in Long-Term Care Residents (SONNET) scale, which we refined following pilot and field testing and with patient and public involvement. We evaluated the final instrument’s feasibility, acceptability, reliability, and validity in 52 LTC resident-staff dyads in the UK and Canada. The 12-item SONNET scale comprises subdomains assessing social engagement and social connectedness, with versions to be rated by a resident or proxy (staff) informant. The SONNET scale is feasible and acceptable, and preliminary testing indicates its reliability and validity. It is available for use to examine social connection in LTC residents. Further testing in diverse samples and confirmation of psychometric properties is needed.
Keywords
• We developed a new instrument to measure social connection for LTC residents, guided by gold-standard psychometric methods and with methodological considerations for people with dementia. • Through two-stage testing, we established its feasibility and acceptability, content and construct validity (structural validity and hypothesis testing), and reliability (internal consistency, test–retest, and inter-rater reliability).
• Our new measure is freely available for researchers and LTC settings to test the effects of interventions at the individual, home, and system levels. • Addressing social connection has the potential to advance care and improve the health and quality of life of LTC residents.What This Paper Adds
Applications of Study Findings
Introduction
Social connection is an umbrella term encompassing the structure, functions, and quality of social relationships (Holt-Lunstad, 2021). Social connection is a core element of human experience, a basic need, and a key determinant of health (Thoits, 2011). Poor social connection has been linked to adverse health outcomes, including increased risk of mortality (Holt-Lunstad et al., 2015) and dementia (Sommerlad et al., 2023). Social connection may be particularly important for long-term care (LTC) home residents, most of whom have dementia (Stewart et al., 2014) and live apart from their previous social networks. In this setting, social connection is an important determinant of quality of life (O’rourke et al., 2015) and a marker of quality of care (Sion et al., 2020). Supporting social connection is a dementia care practice recommendation (Calkins, 2018) and important concept for person-centered care (Corazzini et al., 2019).
Evidence on effective interventions for improving social connection in LTC residents is sparse (Brimelow & Wollin, 2017), partly due to conceptual ambiguities (Liougas et al., 2024) and measurement difficulties (Chapman et al., 2024). LTC residents and homes have distinct considerations that must be reflected in a measure of social connection. Most residents are older adults with complex health needs, including cognitive, sensory, or mobility impairments. Within LTC homes, residents share space, take part in congregate activities, and receive daily care from staff. LTC homes are often separated from community activities, although families, volunteers, and other service providers may have important roles. Although over 30 measures of social connection have been tested with LTC residents, when evaluated against established criteria for evidence of psychometric properties, none are currently recommended for use because of lack of evidence of content validity, due to failing to demonstrate the relevance, comprehensiveness, and comprehensibility of measure items (Dewan et al., 2024).
We, therefore, aimed to develop a psychometrically robust, person-centered measure of social connection for residents in LTC homes, applicable to residents across the spectrum of cognitive impairment and assessing key domains of social connection. A measure of social connection in LTC residents, with acceptable validity and reliability, would facilitate rigorous study of determinants of social connection as well as the evaluation of interventions to improve social connection.
Methods
We used gold-standard psychometric methods (Streiner et al., 2024) and methodological considerations for people with dementia (Smith et al., 2005) to design a measure that could be used in settings that align with the international definition of nursing home (Sanford et al., 2015) and with all residents, irrespective of cognitive impairment (Hughes et al., 2021). We used the COnsensus-based Standards for the selection of health Measurement Instruments (COSMIN) guidelines (Mokkink et al., 2010) and the Person-Centered Measure Evaluation Tool (PC-MET) (Zimmerman et al., 2023) to guide our work. We followed a six-step process outlined by De Vet et al. (de Vet, 2011), adapted for concept elicitation, and which we summarize in Figure 1. Overview of six-step study process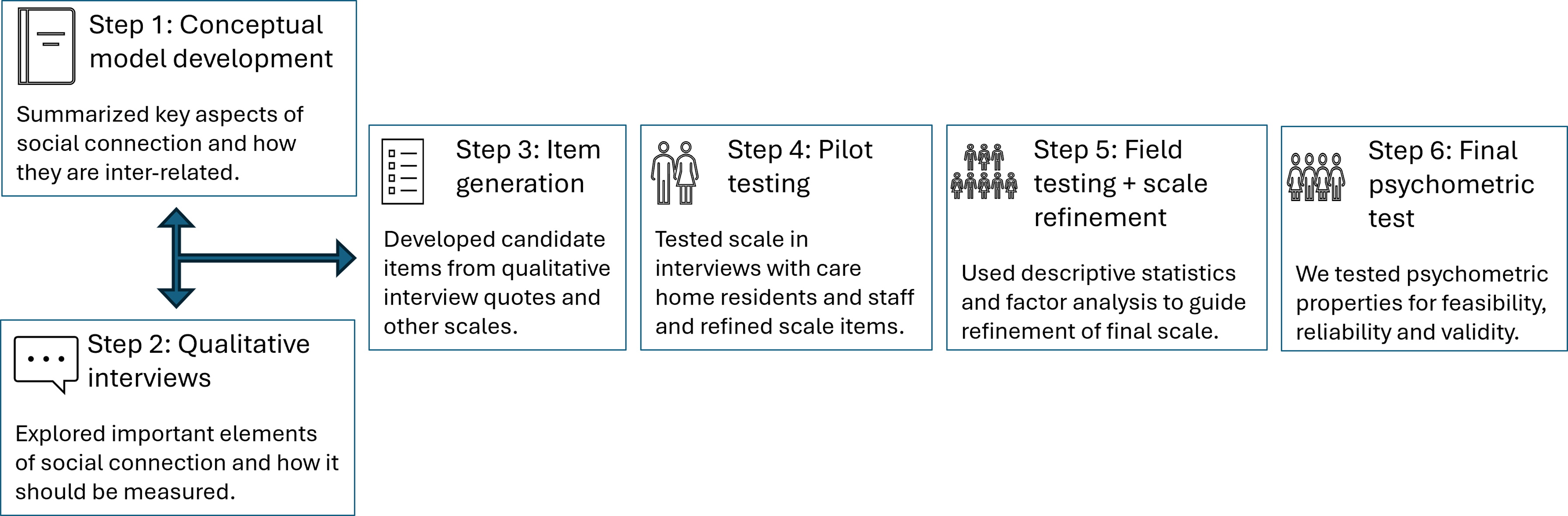
Conceptual Model
Social connection is acknowledged to comprise multiple concepts (Holt-Lunstad, 2021) and thus presents implications for a multidimensional measurement. Yet, the inter-relationships between the aspects of social connection have not, to our knowledge, been articulated in a unifying conceptual model. Hence, we developed a conceptual model to summarize key aspects of social connection, and how they are related to each other, including along gradients as observable and experienced characteristics (Supplemental Material 1.1). We did this to also guide the development of our measure to focus on the most important aspects of social connection for LTC homes as identified by LTC residents and their relatives. We adapted a model (Berkman et al., 2000) by incorporating aspects of social connection highlighted for LTC home research (Leedahl et al., 2018) and iteratively refining it based on our literature review, qualitative interviews, patient and public involvement (PPI) input, and discussions with our multidisciplinary team.
Qualitative Interviews
Participants and Setting
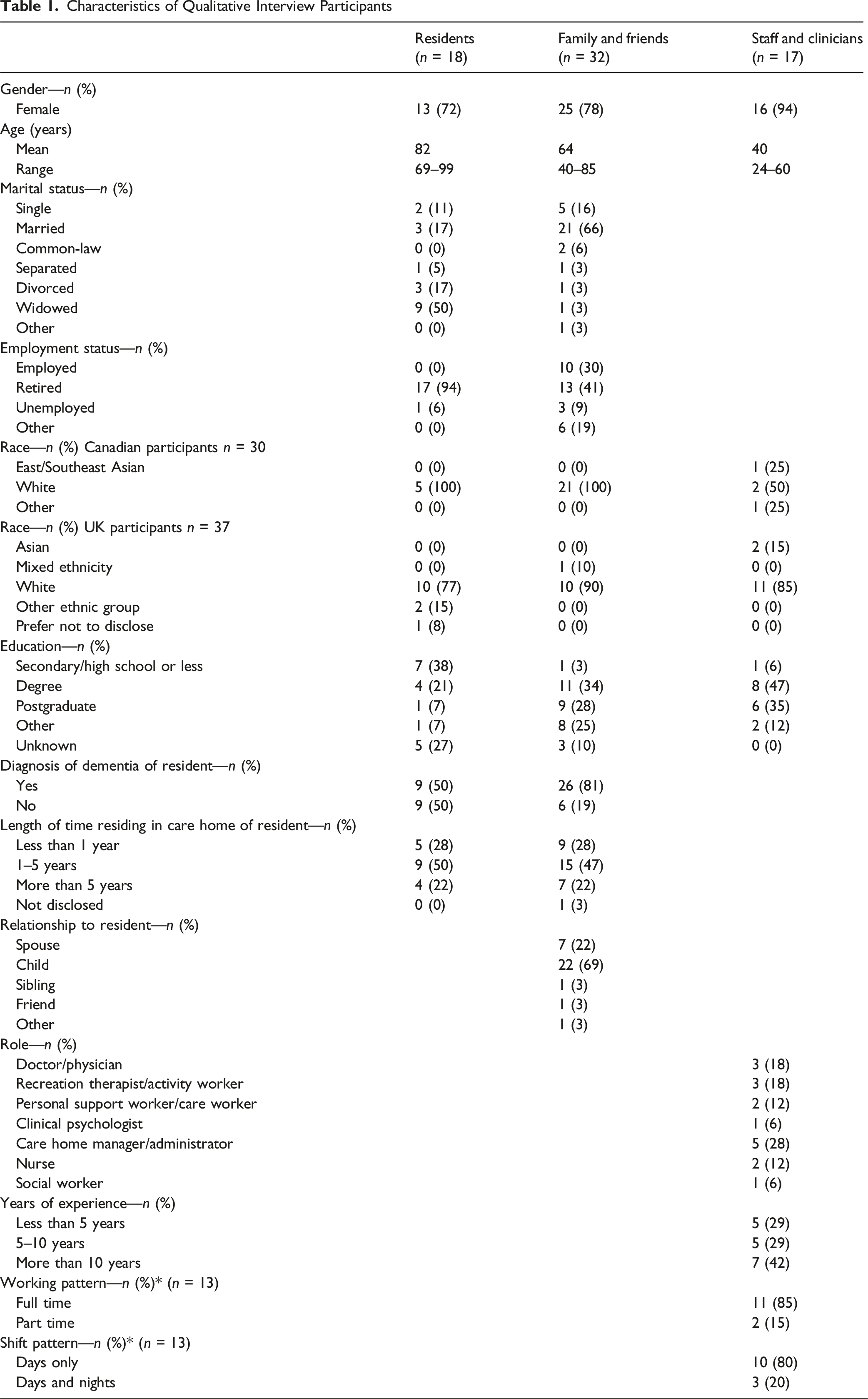
We completed interviews, in Canada and the UK, with LTC residents, staff and clinicians, and family and friends of residents. We purposively sampled using the following criteria: - LTC residents: aged 65+, had no active severe mental illness, and had mental capacity to consent to participation. - Staff and clinicians: aged 18+ and who worked at an LTC home or had during the previous 2 years. - Family and friends: aged 18+ and who visited an LTC resident at least monthly.
In the UK, we recruited participants from National Health Service (NHS) care home in-reach mental health teams from three NHS trusts, via newsletters from ENRICH, the national care home research network, and from LTC homes directly. In Canada, we recruited participants through organizations from across Ontario representing LTC residents, families, and staff and through LTC homes.
Procedures
We obtained informed consent from prospective participants and then conducted individual or dyadic interviews (for residents, family, and friends) and individual or dyadic interviews or focus groups (for staff and clinicians), in person or remotely, between May 2022 and June 2023. We followed pre-piloted interview guides (Supplemental Material 1.2a & b) derived from our conceptual model, previous study findings, and existing measures of social connection to explore views on the most important elements of social connection and how it should be measured. We audio-recorded and transcribed interviews/focus groups using MS Teams for both in-person and remote interviews and then anonymized and checked them for accuracy. We stopped recruitment when we judged that we had reached theoretical sufficiency (Saunders et al., 2018). We compensated participants with a gift voucher (£20 in the UK and $35 in Canada).
Analysis
Our analytic method, based on thematic analysis (Braun & Clarke, 2006), is described in detail elsewhere (Chapman et al., 2024). Using Dedoose 9.0.90 software (SocioCultural Research Consultants, 2023), five team members developed a codebook from a subsample of five interview transcripts. We then applied the codebook to four previously unread interviews whereby two members of the research team independently coded each transcript. We discussed the code book throughout and once inter-rater reliability was moderate or higher (Cohen’s kappa >0.60), one researcher coded all subsequent transcripts with regular research team meetings to discuss uncertainties in interview content or meaning thereby ensuring consistency throughout the coding process.
Item Generation
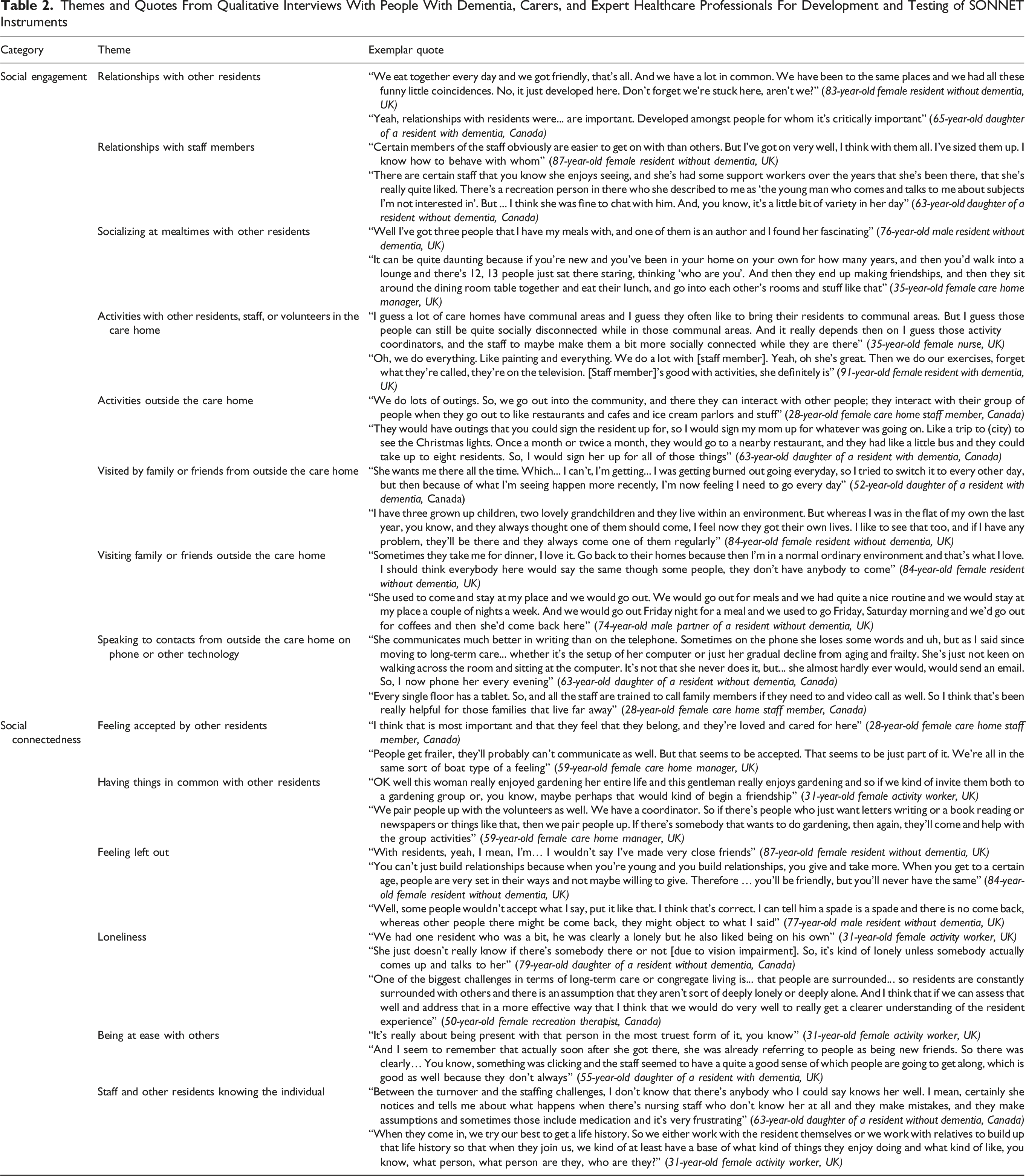
We used two approaches to generate candidate items. First, we extracted quotes from our qualitative interviews indicating positive and negative aspects of social connection, aligned with our conceptual model, and developed them into items. Second, we selected candidate items from a subset of scales with high or sufficient evidence of content validity and at least two measurement properties categorized as having adequately low risk of bias (Dewan et al., 2024): Laurens Well-Being Inventory for Gerontopsychiatry (van der Wolf et al., 2018), Lubben Social Network Scale Revised (Munn et al., 2018), QUALIDEM (Ettema et al., 2007), and the Revised Index of Social Engagement (Gerritsen et al., 2008). We further considered the UCLA three-item Loneliness Scale’s items (Russell, 1996), as the most widely used loneliness scale.
We shared the draft items as a survey with the study team (comprising nursing, psychiatry, epidemiology, rehabilitation, and psychology expertise), asking for them to indicate whether each item should be retained, rejected, or modified based on its relevance, comprehensibility, and contribution to a comprehensive measure and to nominate other items not covered by the long list. The survey also allowed for feedback, either on the content or form of the items, including any suggestions for modified wording. We then shared our preliminary version with our PPI groups in Canada and the UK for their feedback.
Pilot Testing
We purposively recruited residents and staff from the same settings as stage 2 for cognitive interviews. We followed recommendations for conducting cognitive interviews to ensure comprehension and comprehensiveness (Patrick et al., 2011), and we developed an interview guide (Supplemental Material 1.3a & b) to explore how respondents understood instructions, recall period, candidate items, and response options using the “verbal probing” method. We audio-recorded and transcribed interviews using MS Teams and then anonymized and checked them for accuracy. The two lead researchers and two research assistants iteratively amended the instructions, items, and response options as interviews were conducted, enabling us to pilot test the refined SONNET scale in subsequent interviews.
Initial Field Testing and Scale Refinement
Participants and Setting
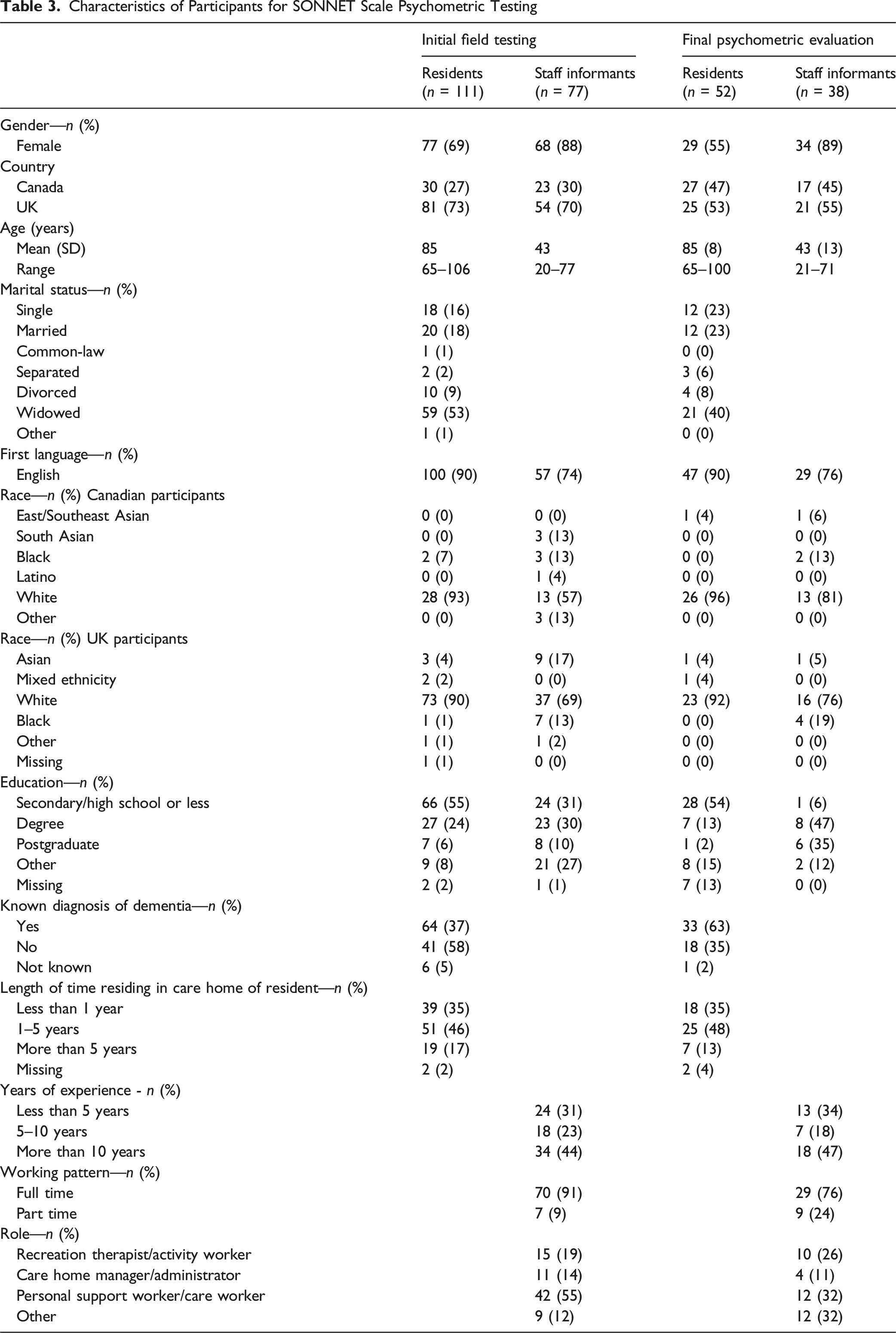
We tested the scale with LTC resident–staff proxy dyads. We recruited dyads to test both the resident- and proxy-report versions and because staff provided some additional data about residents. Eligibility criteria for LTC were being aged 65+ and having adequate English language proficiency. Staff members were required to be aged 18+, have adequate English language proficiency, and have cared for the dyadic resident at least once weekly over the past month.
In Canada, we recruited participants from five LTC homes in Ontario, each with over 100 residents and located within 150 km of Toronto. In the UK, we recruited residents from the same sources as stage 2 and from four additional NHS research networks.
Procedures
We posted the research opportunity through an advert whereby potential participants could contact the study team directly. We also approached LTC home managers to identify potentially eligible resident participants. In the UK, we also used electronic health records to identify eligible resident participants who had previously consented to being contacted about research. For each resident, LTC homes identified potential staff participants. A trained member of the research team assessed mental capacity to consent against UK Mental Capacity Legislation or, in Canada, with an evaluation to sign consent (Resnick et al., 2007). Resident participants either gave informed consent for themselves, or, for those who lacked capacity, we sought to discuss the research study with the nearest relative or a nominated consultee. Once the consultee provided consent, the study was discussed with the LTC resident and assent obtained before administering questionnaires.
We interviewed LTC residents and staff separately, in-person. They were first asked for personal and demographic information (e.g., age, sex, and length of time living or working in an LTC, and whether the resident had a recorded diagnosis of dementia). Questions from the SONNET scale were then administered. A prompt sheet was provided to facilitate ordinal response options. Instructions to record binary (yes/no) responses or lack of response were also included. For residents with severe cognitive impairment, we corroborated personal and demographic information with staff.
Analysis
We aimed to recruit 100 dyads, estimated as five dyads per scale item (Rouquette & Falissard, 2011). Using Stata 16.1 (StataCorp LLC, 2020), we described the participants and their SONNET item responses using descriptive statistics (e.g., frequencies, proportions, ranges, and missingness)—as there was little missing data, we used complete case analysis in these descriptive analyses and full information maximum likelihood in the factor analyses. We examined dimensionality by conducting an exploratory factor analysis which used the principal factors method without rotation applied to the polychoric correlation matrix of ordinal item responses from the data. Items with low loadings below 0.3 on the general social connection factor or cross-loadings outside of domains were noted. We examined internal consistency by calculating inter-item and item-total correlations as well as Cronbach’s alpha. We conducted Horn’s Parallel Analysis (Dinno, 2009), using Stata’s paran command which implements Horn’s technique to contrast eigenvalues produced through a factor analysis on a random dataset with the same number of variables and observations as the observational dataset. We then reduced the items based on Horn’s Parallel Analysis results, missingness, response range, factor loading, and in consultation with the study team and PPI collaborators.
Final Psychometric Evaluation
Participants and Setting
We recruited participants from the same settings and with the same eligibility criteria as Stage 5. We purposively sampled participants aiming for two-thirds of residents with dementia and a range of demographic characteristics for both residents and staff.
Procedures
We followed the same procedures as stage 5, but using the final SONNET scale version and recording the time taken to complete the scale. At the same time as we collected the SONNET scale ratings, we also collected additional data from staff about the resident, namely: (1) Revised Index of Social Engagement (RISE) (Gerritsen et al., 2008); (2) Modified Clinical Dementia Rating (CDR) scale; this version has been tested and validated in people without dementia, those with mild cognitive impairment, and those with dementia (Duara et al., 2010). We used the total CDR score in our analyses and the “community affairs” subscale; (3) Katz Index of Independence in activities of Daily Living (Katz et al., 1963); (4) Neuropsychiatric Inventory (NPI) (Kaufer et al., 2000); (5) Quality of Life in Alzheimer’s Disease scale, Nursing Home Version (QOL-AD-NH) (Dichter et al., 2018). A social subscale has previously been used, comprising four questions (i.e., living situation and relationships with each of family members, staff, and friends).
When available, a second researcher administered the SONNET scale (i.e., evaluating inter-rater reliability). When feasible, the researcher returned to participants 2 weeks later (+/− 1 week) to repeat the SONNET scale (i.e., evaluating test–retest reliability). All participants were provided with a £20/$35 gift voucher.
Analysis
We aimed to recruit 50 dyads (de Vet, 2011), providing 90% power at a significance level of 5% to find correlation of 0.42 between the SONNET and other measures, and adhering to the commonly used rule of thumb for factor analysis sample size calculation (Rouquette & Falissard, 2011). We used Stata 16.1 for statistical analysis. We first described the participant characteristics and their responses to the SONNET scale using descriptive statistics (e.g., frequencies, proportions, ranges, and missingness). We described feasibility (i.e., whether or not respondents are able to complete the scale) and acceptability (i.e., whether or not respondents are willing to complete the scale) with completion rates, item missingness, and mean time for completion. We conducted subsequent analyses using complete cases.
We assessed measurement properties for the SONNET resident- and proxy-report versions, namely: • Construct validity (structural validity): We performed a confirmatory factor analysis, using full information maximum likelihood. To test the scale against our hypothesized bifactor structure, we used the comparative fit index, χ2 statistic (with non-significant p-values indicating exact fit), coefficient of determination (CD, with values 0.08 or smaller indicating close fit), and Root Mean Square Error of Approximation (RMSEA, with values 0.06 or smaller indicating close fit) (Hu & Bentler, 1999). All subsequent analyses were based on the emergent subscales whereby we calculated subscale scores (as the sum of the items within the subscale). • Construct validity (hypothesis testing): We calculated the Pearson’s correlation coefficient to estimate and characterize (Evans, 1996) the relationship between the SONNET subscales and SONNET summary question 12 and other measures (i.e., RISE; CDR total and community affairs domain; Katz index; NPI; and QOL-AD NH total and social subscale). We hypothesized that the SONNET subscales would be positively correlated with the SONNET question 12, RISE, QOL-AD NH, and Katz scores and inversely correlated with CDR and NPI. • Reliability (internal consistency): We calculated and described (Morera & Stokes, 2016) Cronbach’s alpha for the subscales. • Reliability (test–retest and inter-rater): We calculated Pearson’s correlation coefficients to estimate the association between the SONNET subscale totals from the two time points and from the two researchers (Cicchetti & Sparrow, 1981), respectively.
In sensitivity analyses, for the resident-report version, we categorized residents by level of cognitive impairment (based on the median CDR score) and examined measurement properties in stratified analyses.
Patient and Public Involvement/Engagement
We worked with PPI groups in Canada (Engagement of People with Lived Experience of Dementia (EPLED)) (Snowball et al., 2022) and the UK (Alzheimer’s Society Research Network), which included people with lived experience of dementia and LTC. The PPI group members provided feedback on and piloted the qualitative interview guide (step 2), assisted with interpreting findings to focus scale development on social engagement and social connectedness, refined and reduced the items (step 3), and offered insights on the measure (e.g., wording and format) (steps 4–6). We consulted PPI collaborators via online meetings, whereby members from Canada and the UK joined together, and email for ongoing input.
Results
Conceptual Model
Our conceptual model (Supplemental Material 1.1) includes components described along a continuum from more directly observable (e.g., social networks, social engagement and their converse, and social isolation) to constructs which reflect individuals’ experiences (e.g., social connectedness and its converse loneliness).
Qualitative Interviews
Characteristics of Qualitative Interview Participants
Themes and Quotes From Qualitative Interviews With People With Dementia, Carers, and Expert Healthcare Professionals For Development and Testing of SONNET Instruments
Item Generation
We developed 58 items (44 from our qualitative interviews and 14 from existing measures). We edited and reduced this to 30 items based on study team feedback and then to 20 items based on PPI group feedback.
Pilot Testing
We pilot tested the 20-item SONNET scale with five LTC residents and four staff (Supplemental Material 1.4). We refined the instructions, items, and response options based on input into the relevance and comprehensibility of items, and the comprehensiveness of the scale.
Initial Field Testing and Scale Refinement
Characteristics of Participants for SONNET Scale Psychometric Testing
Final Psychometric Evaluation
We evaluated the 12-item SONNET scale with 52 resident–staff dyads, whereby 14 staff acted as proxy for more than one resident (Table 3).
Feasibility and Acceptability
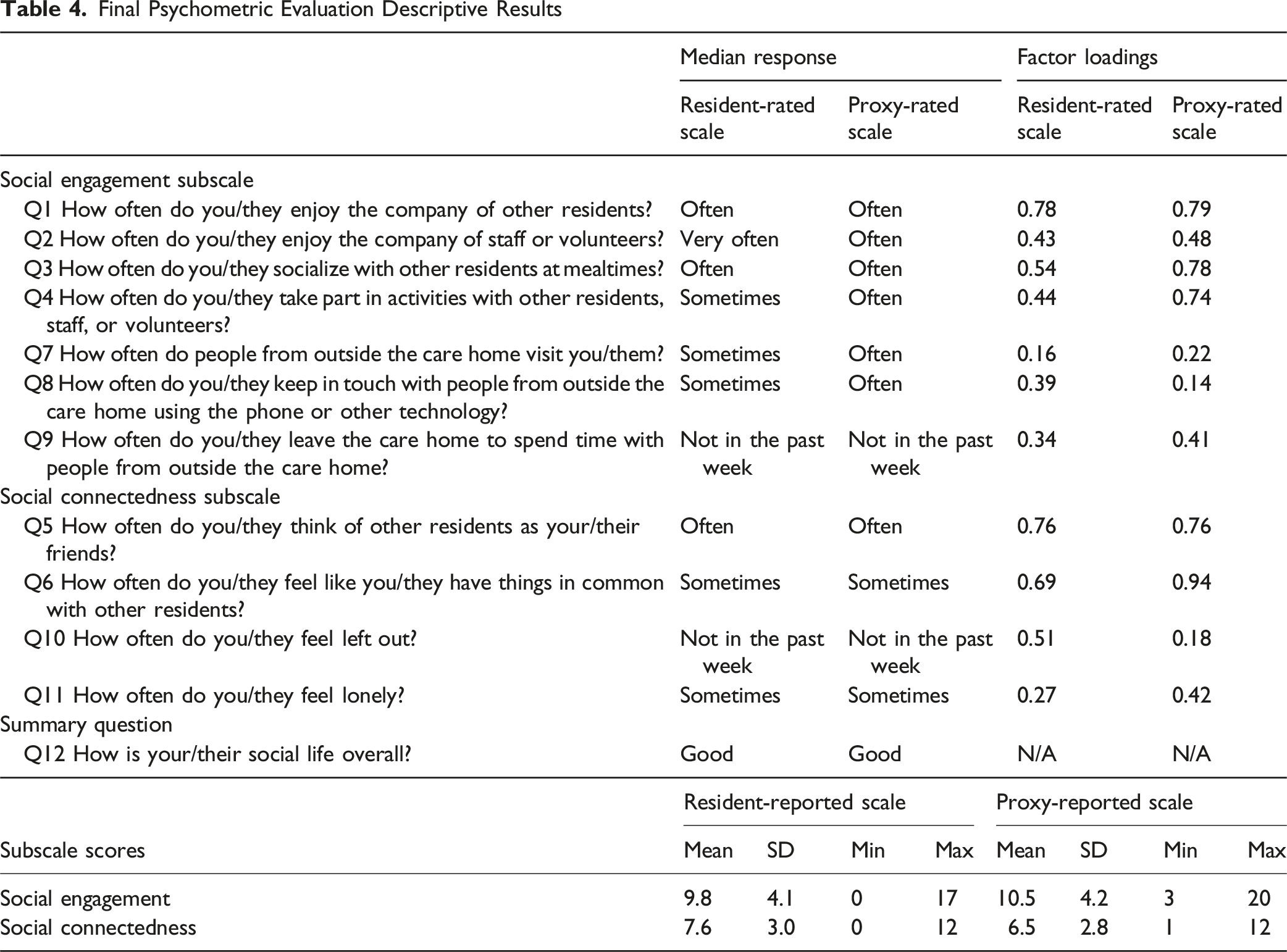
Residents took a mean of 8.1 minutes (SD 3.6, range 3–16) and staff took a mean of 4.7 minutes (SD 3.0, range 2–15) to complete the resident- and proxy-reported versions. There were 53 (8.5%) and 10 (1.6%) missing responses for the resident and proxy-reported versions, respectively, but most residents (n = 44; 84.6%) and proxies (n = 45; 86.5%) had no missing data.
Construct Validity (Structural Validity)
Final Psychometric Evaluation Descriptive Results
Construct Validity (Hypothesis Testing)
Validity of Social Connection in Long-term Care Home Residents (SONNET) scale
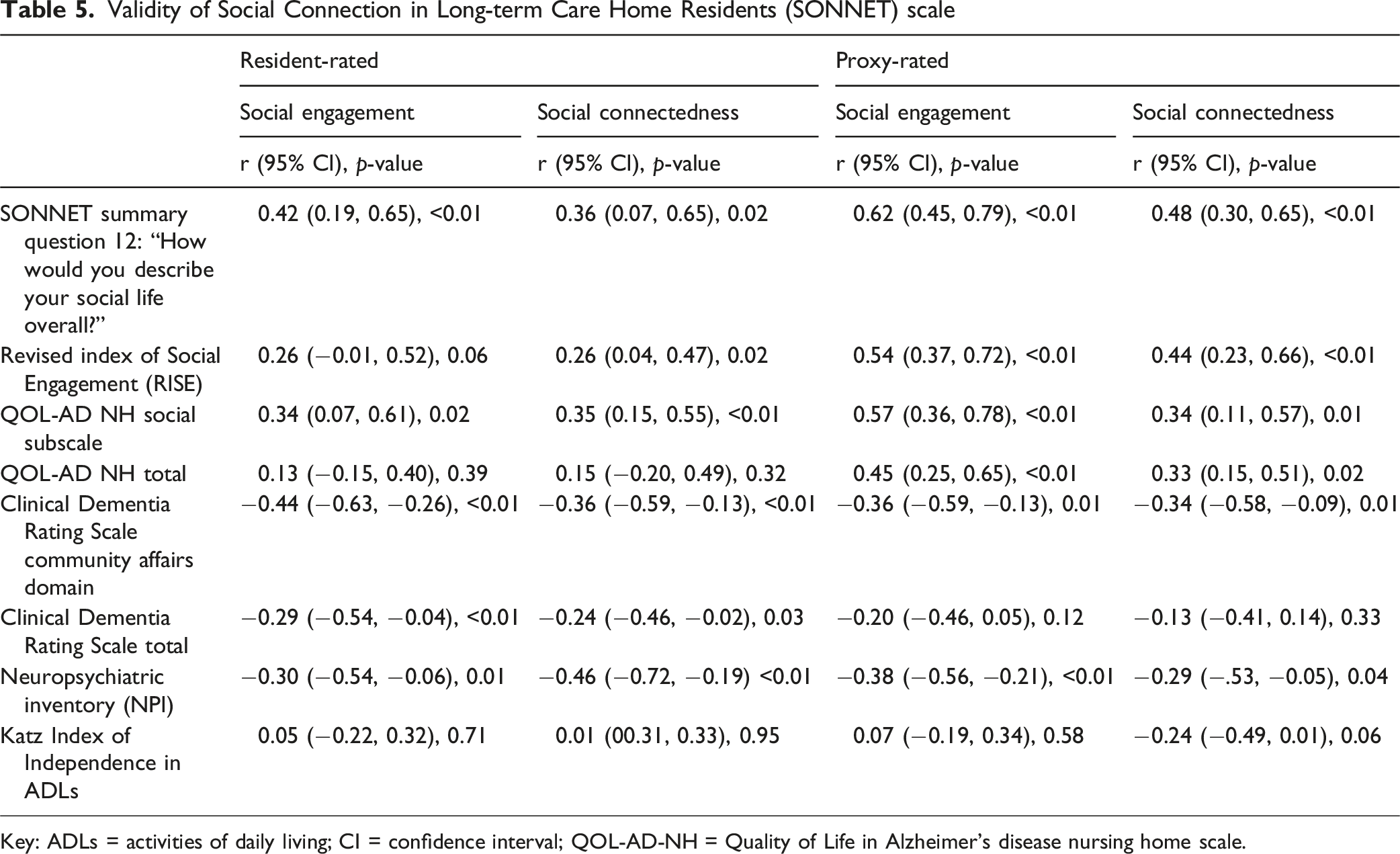
Key: ADLs = activities of daily living; CI = confidence interval; QOL-AD-NH = Quality of Life in Alzheimer’s disease nursing home scale.
The proxy-reported social engagement subscale had strong correlation with SONNET summary question 12, moderate correlation with the RISE, QOL-AD NH total, and QOL-AD NH social subscale, and weak correlation with the NPI, CDR total, and CDR community affairs domain. The social connectedness subscale had moderate correlation with SONNET summary question 12 and the RISE, and weak correlation with the QOL-AD NH social subscale and QOL-AD NH total, CDR community affairs domain, NPI, and Katz index. There was moderate correlation between the resident-reported and proxy-reported social engagement scale (r = 0.35, p = 0.01) and weak correlation between the resident-reported and proxy-reported social connectedness subscale (r = 0.26, p = 0.08).
Reliability (Internal Consistency)
The internal consistency was acceptable; Cronbach’s alpha for the resident-reported scale was 0.64 for social engagement, 0.72 for the social connectedness, and 0.71 for both proxy-reported subscales.
Reliability (Test–Retest and Inter-rater)
Reliability of Social Connection in Long-term Care Home Residents (SONNET) scale
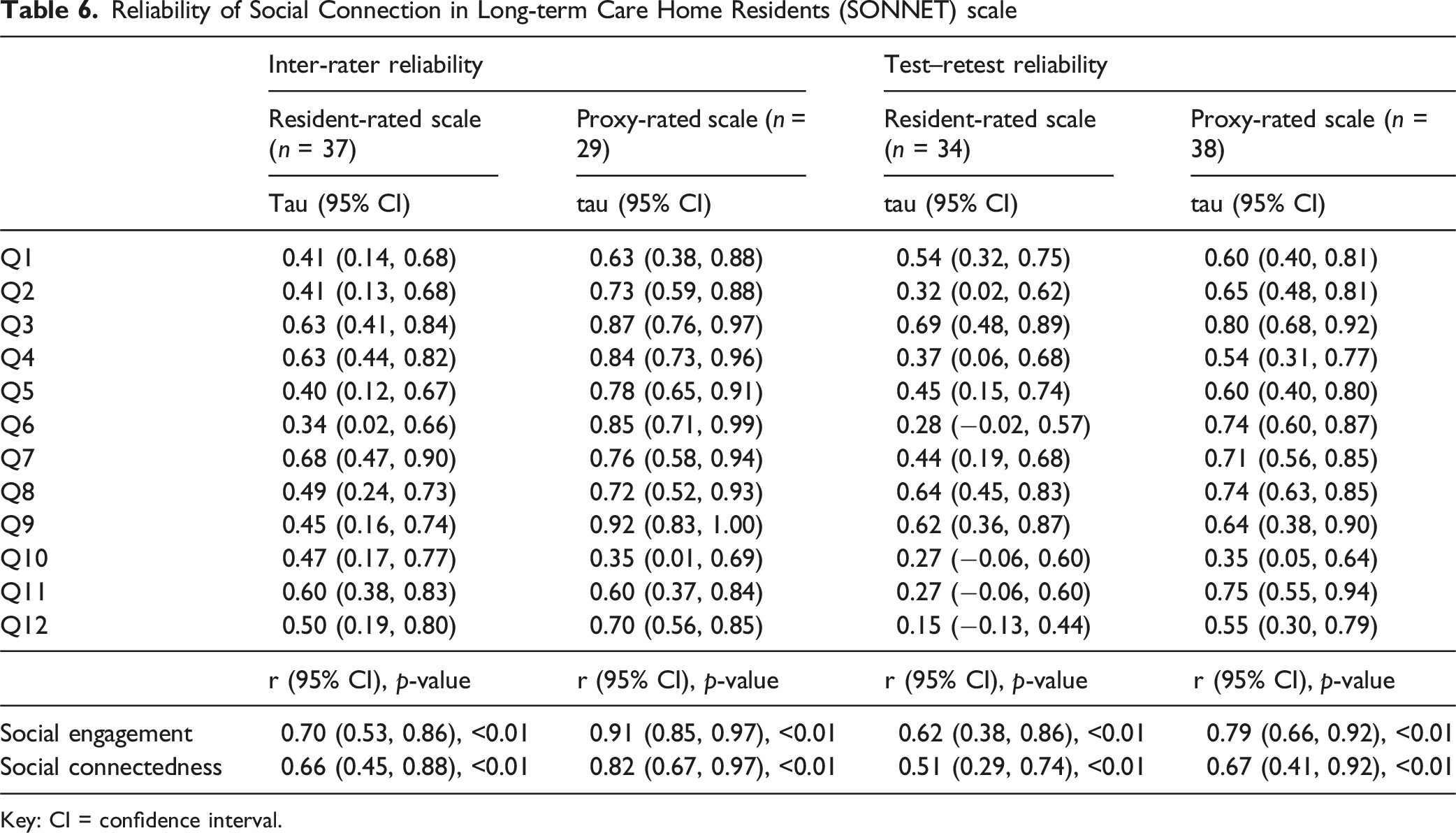
Key: CI = confidence interval.
Sensitivity Analyses
In sensitivity analyses (Supplemental Material 1.7), inter-rater reliability for the social engagement subscale was higher for residents with less cognitive impairment (r = 0.86 (p < 0.01) and r = 0.55 (p = 0.02), respectively), which was similarly observed for the subscale’s test–retest reliability (r = 0.74 (p < 0.01) and r = 0.50 (p = 0.08), respectively). For the social connectedness subscale, inter-rater reliability was similar and, unlike social engagement, the test–retest reliability was higher among those who were more cognitively impaired (r = 0.63 (p = 04) and r = 0.33 (p = 0.14), respectively). There was no consistent difference in correlation of the SONNET subscales with hypothesized related constructs (Supplemental Material 1.8).
Discussion
We developed a new measure for assessing social connection with LTC residents. We followed key methodological approaches and used a conceptual model of social connection for LTC residents to align the development and content with principles of person-centeredness and ensure the content validity of the measure. We demonstrated feasibility and acceptability for both self-reported and staff proxy-reported versions, and provided evidence of their reliability and validity in UK and Canadian settings.
The structural validity of the scale was evidenced by our hypothesized scale structure, with two domains of social connection (i.e., social engagement and social connectedness) supported in confirmatory factor analysis. However, test–retest and inter-rater reliability was lower for both of these subscales in the resident-reported version when compared to the proxy-reported subscales; sensitivity analyses suggest a differential for both the subscale (observed social engagement vs. experienced social connectedness) as well as the resident’s level of cognitive impairment. No previously tested measures have reported high test–retest reliability indicating the challenge of establishing this domain (Dewan et al., 2024), and this finding extends to measures of deficit in social connectedness (loneliness) used across populations and settings (Maes et al., 2022).
In our analysis of construct validity, findings supported our hypotheses that the SONNET scale would be positively correlated with other measures of social connection and inversely correlated with neuropsychiatric symptoms. However, we did not find any association with independence in activities of daily living and only weak associations with dementia severity. This finding may be explained by the support provided from care staff to all residents, particularly to enable those who are most impaired, as well as preservation of some aspects of social functioning despite increasing dementia severity (Budgett et al., 2019). We also did not find any association between the resident-reported SONNET subscales and staff-reported overall quality of life, suggesting that social connection may differ from quality of life (Budgett et al., 2019) or reflecting a mismatch between residents and staff in quality of life ratings (Spector & Orrell, 2006). Similarly, independence in activities of daily living was not correlated with either resident-reported SONNET subscale. Despite the potential negative impact of disability on social connection, it is possible that it can also ensure social contact as staff or family help for ADLs is provided in LTC settings. Others have also recently reported no association between independence in activities of daily living and loneliness in this setting (Pavlovski et al., 2025).
We found stronger correlation between resident and staff ratings for the social engagement (vs. social connectedness) subscale. This suggests that social engagement items, which can be directly observed (e.g., participation in activities or visits from family and friends), are more readily assessed by staff or residents. The lower correlation for resident and staff ratings of social connectedness may reflect residents’ impairment of memory about social connection (Sommerlad et al., 2024) or the difficulty faced by a proxy-rater in accurately assessing other’s experiences (Albrecht & Devlieger, 1999). Taken together, this highlights the benefits of self- and proxy-reported versions of the SONNET scale. Although our study was not designed to specifically assess psychometric properties according to cognitive impairment, our sensitivity analyses suggest further testing is warranted for best approaches to assess social connection in people with severe cognitive impairment. However, we reiterate previous researchers’ caution (Hughes et al., 2021) against developing one measure for people with dementia and another for people without dementia.
Strengths of our study include the methodical and detailed development and psychometric evaluation processes, all underpinned by principles of person-centeredness (Zimmerman et al., 2023). The SONNET scale offers a measure of social connection that can be used by researchers and LTC settings to test the effects of interventions at the individual, home, and system levels. Given the broader movement to address social connection as a public health priority (Holt-Lunstad et al., 2017) and the distinct importance for LTC homes (Estabrooks et al., 2020), integrating robust measures of social connection with mechanisms for ongoing data collection could offer new opportunities for research and health surveillance. A formal analysis of the current study methods and results, as a mechanism to compare SONNET with other existing measures (Dewan et al., 2024), is beyond the scope of the current study. However, we highlight some key limitations and areas for building the evidence for the SONNET measure. First, generalizability is limited by our study design and sample. Participants were required to speak English, and there was a lack of racial diversity in the resident participants. Further, our approach to recruitment likely selected higher-quality homes and residents who were more socially active. Second, to minimize burden on residents, we did not administer other resident-rated scales and this limited our analysis of construct validity. Our findings also highlight areas for development, including longitudinal data to test responsiveness and predictive validity, translation and testing in other diverse settings as well as testing of a self-completed version. Third, testing of a proxy-reported version that could be completed by family may be useful in some settings, given staff and family can have differing views on quality of life in LTC residents with severe dementia (Clare et al., 2014; Robertson et al., 2017). Fourth, our confirmatory factor analysis sample size was small which may lead to unstable factor loadings, so further evaluation in larger samples is warranted. Finally, we did not define a threshold or cut-off point as a binary (e.g., high or low social engagement), despite the potential utility for both research and practice, but highlight this as an area for future investigation to generate normative data in a representative sample of LTC residents.
Conclusion
The SONNET scale is feasible and acceptable for use in measuring LTC resident’s social connection. It is freely available through our website: https://www.sonnetstudy.com/measure. The self- and proxy-reported versions each yield two scores, social engagement and social connectedness, intended to be treated separately. Our study provides initial data; however, further study is needed to adapt and establish psychometric properties for diverse uses and settings. Research using high-quality measurement instruments would improve our understanding of LTC system, home, and resident-level factors which facilitate social connection and, in turn, develop evidence-based approaches to improve social connection.
Supplemental Material
Supplemental Material - Development and Testing of the Social Connection in Long-Term Care Home Residents (SONNET) Scale
Supplemental Material for Development and Testing of the Social Connection in Long-Term Care Home Residents (SONNET) Scale by Andrew Sommerlad, Steven Stewart, Hannah Chapman, Neha Dewan, Gill Livingston, Katherine S. McGilton, Sube Banerjee, Kirsten Corazzini, David Edvardsson, Madalena P. Liougas, Hannah M. O’Rourke, and Jennifer Bethell in Journal of Applied Gerontology
Footnotes
Acknowledgments
We are grateful for the participation of the long-term care home residents, families, and staff who took part in our study. Our thanks to the Camden and Islington National Health Service (NHS) Foundation Trust; Oxford Health NHS Foundation Trust; Northumbria Healthcare NHS Foundation Trust; Devon Partnership NHS Trust; South London & Maudsley NHS Foundation Trust; Solent NHS Trust; Clinical Research Network (CRN) West Midlands; and CRN East of England. And special thanks to Mary Connell at Jarlette Health Services; Stacey Januszewski at Alexander Place (Waterdown, ON); Teresa Figliuzzi at Roberta Place (Barrie, ON); Denise Simpson at Avalon Care Centre (Orangeville, ON); Monica Bolger at Royal Rose Place (Welland, ON); Cristina de Santis at Responsive Group Inc.; Nicole Fisher at Cooksville Care Centre (Mississauga, ON); and Laura Petta at the Alzheimer Society of Toronto. We would like to thank Michal Misiak from University College London; Deborah Moll and Anouska Pearson from Oxford Health NHS Foundation Trust; Debera Drew and Louise Jones from Northumbria NHS Trust; Emma Searle and Amie Zolanver from Solent NHS Trust; Humberto Matos, Anna Percival, and Humberto from Devon Partnership NHS Trust; Roselyn Enesi, Yin Fan, Lisa Farrell, Susan Frost, Kathryn Howlett, and Adam Peel from CRN East of England for support in data collection.
ORCID iDs
Ethical Considerations
Consent to Participate
Consent was obtained from participants, or, for those residents lacking capacity, consent was obtained from a consultee decision maker.
Author Contributions
All authors contributed to the conception or design of the study. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canada Brain Research Fund (CBRF), an innovative arrangement between the Government of Canada (through Health Canada) and Brain Canada Foundation, and the Alzheimer’s Association (grant number: ARCOM-22-875327). To date, Health Canada has invested over $130 million through the CBRF which has been matched by Brain Canada Foundation and its donors and partners. Ce projet a été rendu possible grâce au soutien financier de Santé Canada, par le biais du Fonds canadien de recherche sur le cerveau, un partenariat novateur entre le gouvernement du Canada (via Santé Canada) et Brain Canada, et d’Alzheimer’s Association (Re: ARCOM-22-875327). Andrew Sommerlad is funded by the Wellcome Trust (grant number 222932/Z/21/Z). Andrew Sommerlad, Hannah Chapman, and Gill Livingston are supported by the University College London Hospitals’ National Institute for Health Research Biomedical Research Centre. Jennifer Bethell and Katherine McGilton are supported by the Walter & Maria Schroeder Institute for Brain Innovation and Recovery. Sube Banerjee is supported by a National Institute of Health and Care Research (NIHR) Senior Investigator Award.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data cannot be made publicly available as a condition of our ethical approvals.
Supplemental Material
Supplemental material for this article is available online.