
Abstract
Telecare promises support for older adults aging in place and helps alleviate the burden on informal caregivers. However, research on informal caregivers’ perceptions of telecare is limited, particularly in the context of unique challenges of dementia. This study addresses this gap by examining the differences between informal caregivers of older adults with and without dementia in terms of the care burden, acceptability of different telecare functionalities, and perceived psychosocial outcomes of telecare use. Conducted in Slovenia with 612 informal caregivers aged 40 and above, the study determined that dementia caregivers experienced higher care burden and perceived greater acceptability of mobility-related telecare devices. Both groups reported similar perceived psychosocial outcomes of telecare use, including reassurance and reduced anxiety. The findings highlight the need to tailor telecare functionalities to informal caregivers’ specific circumstances, particularly in supporting people with dementia, to enhance telecare’s effectiveness and the well-being of informal caregivers and care recipients.
Provides the first comprehensive national data comparing telecare perceptions among Slovenian informal caregivers of older adults with and without dementia. Reveals that informal caregivers of older adults with dementia favor mobility-related technologies and emphasize context-specific needs.
Highlights the importance of tailoring telecare to dementia-related needs, such as wandering, to improve informal caregiver support and the well-being of older adults. Encourages integration of user-centered design principles in telecare development to ensure usability for both informal caregivers and cognitively impaired older adults.What This Paper Adds
Applications of Study Findings
Introduction
The global population is aging rapidly, with people aged 65 or older projected to comprise 30.7% of the global population by 2050 (Population Reference Bureau, 2024). Aging in place, which enables older adults to remain at home rather than moving to long-term care facilities (Grimmer et al., 2015), is being widely promoted but remains inaccessible for many due to care poverty—that is, a lack of necessary care resulting from the limited availability, accessibility, or affordability of formal and informal support (Kröger et al., 2019, 2022). Addressing care poverty has thus become crucial, particularly as demographic changes threaten the availability of informal caregivers, 1 unpaid individuals providing ongoing care outside formal structures, which has prompted the European Commission to emphasize their support and to promote their empowerment (Zigante, 2018). Another pressing challenge is the growing prevalence of dementia, which is expected to affect significantly more people as the population ages. Currently, approximately 57.4 million people globally live with dementia, which is projected to increase by 166% by 2050 (GBD 2019 Dementia Forecasting Collaborators, 2022; World Health Organization, 2025). Because dementia progressively limits independence and increases the need for continuous supervision and support, its rising prevalence poses an additional barrier to aging in place and further increased reliance on informal caregivers (Alzheimer’s Association, 2022).
Care Burden
In response to the rising need for support for long-term care, many European countries, including Slovenia, have shifted their care models toward aging in place, thus further increasing reliance on informal caregivers (Spasova et al., 2018). In Slovenia, 33.1% of people aged 40 and over now provide at least four hours of unpaid care weekly to someone aged 65 or older (Dolničar et al., 2021). This extensive caregiving role requires ongoing engagement in daily personal care, household tasks and financial management, medication oversight, and continuous attention to safety (Winblad et al., 2016), placing multifaceted demands on informal caregivers. These responsibilities contribute to cumulative strain, encompassing disruptions to professional and social life (Raiber et al., 2023), strained family relationships (Yusri & Khairudin, 2024), and a range of physical and mental health issues, including stress, depression, burnout, and reduced quality of life (Akgun-Citak et al., 2020; Tatangelo et al., 2018). Such responsibilities are typically more time and emotionally intensive for dementia caregivers than for those assisting older adults without dementia (Karg et al., 2018), with consistently higher care burden observed internationally (Boogaard et al., 2019; Givens et al., 2012). Despite such global evidence, data on the care burden in Slovenia is still limited. Nearly half of Slovenian informal caregivers report a mild-to-moderate burden, and a quarter report a moderate-to-high burden (Nagode et al., 2021), but no study has yet systematically compared informal caregivers of older adults with and without dementia in the Slovenian context; this study addresses that gap.
Telecare
Telecare is increasingly recognized as a tool that supports aging in place, reduces the care burden, and promotes the well-being of older adults (Eurocarers, 2018). It entails the use of digital technologies to deliver health and social support remotely, enabling older adults to remain at home with greater safety and independence (Oxford English Dictionary, n.d.). Telecare includes devices such as personal alarms, fall detectors, environmental monitors, GPS trackers, and medication reminders (Karlsen et al., 2019; Roberts et al., 2012), supporting both sensory and cognitive needs (Cook et al., 2017).
Acceptability of Telecare
Understanding how informal caregivers perceive telecare technologies before using them is crucial. Acceptability—distinct from post-use acceptance—captures users’ anticipated cognitive and emotional responses to a technology they have yet to experience (Sekhon et al., 2017). A scoping study (Hvalič-Touzery et al., 2022c) found that post-use acceptance of telecare among informal caregivers was more nuanced than acceptability before use, while also highlighting a lack of research on acceptance and particularly on the acceptability of telecare in informal care. Furthermore, research suggests that acceptability can vary depending on the care recipient’s level of dependency and the specific functionalities offered (Hvalič-Touzery & Dolničar, 2022; Smole Orehek et al., 2020). However, existing studies have rarely considered the variety of telecare functionalities or examined the unique needs of informal caregivers supporting older adults with dementia. This is significant because informal caregivers of highly dependent older adults with cognitive impairments may rely more heavily on specific technologies to alleviate anxiety, provide peace of mind, and reduce the care burden (Sriram et al., 2019). Poor acceptability of telecare would therefore undermine such benefits, which highlights the need to explore informal caregivers’ perspectives further.
Perceived Psychosocial Outcomes of Telecare use
It is also important to consider the perceived psychosocial outcomes of telecare use, which relate to its impact on informal caregivers’ emotional well-being, social interactions, and overall quality of life (Martikainen et al., 2002; Vizzotto et al., 2020). Telecare does not operate in isolation; rather, it is embedded in a broader socio-technical environment that can affect informal caregivers’ psychological and social functioning, feelings, behaviors, relationships, interactions, and cognitive processes (Abda et al., 2019). While much existing research has focused on benefits for care recipients (Hvalič-Touzery et al., 2022d; Verloo et al., 2020), there is growing evidence that informal caregivers themselves can enjoy increased reassurance and peace of mind (Guisado-Fernández et al., 2019; Hvalič-Touzery et al., 2022a, 2022b; Karlsen et al., 2019), decreased commuting time from being able to monitor the care recipient remotely (Gaugler et al., 2019), and greater personal freedom (Sriram et al., 2019). These benefits are especially relevant in dementia care, in which constant supervision is often necessary and for which technology may offer some relief.
Aim of the Study
Despite recognition of the importance of informal caregivers’ views, little research has examined their perceptions of telecare prior to use. Furthermore, there is limited evidence on how these perceptions differ between informal caregivers of older adults with and without dementia, including in the Slovenian context. To address this gap, the present study explores the first-hand perspectives of informal caregivers of older adults with and without dementia. Specifically, it seeks to answer the following research questions: (1) How do the two groups differ in perceived care burden? (2) How do they differ in telecare acceptability? (3) How do they differ in perceived psychosocial outcomes of telecare use?
Methods
Procedures
Participants were recruited through Valicon, a market research firm, and data were collected using the online survey tool 1KA, an open-source platform for web surveys. The average completion time for the entire survey was 20 min. The first part of the survey (approximately 3%) served as a screening tool, covering weekly caregiving hours, types of caregiving tasks (e.g., basic and instrumental activities of daily living and emotional support), and the kinship and age of the older adult. Eligible participants continued directly in the main survey, which had to be completed in a single session. Of the 3,284 individuals invited, only those meeting the inclusion criteria—individuals aged 40 or older providing at least four hours of care per week to family member(s) aged 65 or above—proceeded, while others were excluded. This resulted in a final sample of 612 participants (18.6% response rate).
Data were collected using a structured online questionnaire in April and May 2021. Participation was voluntary and based on informed consent. Participants accessed the survey via a unique invitation link distributed by Valicon. Before starting the survey, participants received information about the study’s aims, data use, survey length, and contact details, and consent was indicated by proceeding with the survey. Data quality was ensured through rigorous screening, removal of incomplete or inconsistent responses, and exclusion of cases with implausibly fast completion times. Quota sampling based on gender, age, and region, guided by official data from the Statistical Office of the Republic of Slovenia, ensured diversity, and responses were weighted using data from the Slovenian Public Opinion Survey (Hafner-Fink et al., 2021) to enhance representativeness.
Measures
Care burden was measured using the Self-Rated Burden Scale (van Exel et al., 2004), a self-assessment tool in which respondents rate their perceived burden on a single scale from 0 (“not at all straining”) to 10 (“much too straining”), with higher scores indicating greater burden.
Telecare acceptability was measured using four items, each corresponding to specific functionality: (1) an emergency call system activated by the older person, (2) a fall detection device that sends automatic alerts, (3) home sensors that notify caregivers of unusual activities, and (4) a wearable device for location tracking. The participants were asked how likely they would be to use each telecare service using a five-point scale from 1 (“certainly would not want to”) to 5 (“certainly would want to”). The four items showed high internal consistency (Cronbach’s α = 0.878). Two-item combinations also demonstrated excellent reliability, with Spearman-Brown coefficient of 0.898 for personal alarm systems and 0.883 for mobility-related devices.
Perceived psychosocial outcomes of telecare use were measured using five outcome types, identified in a prior scoping study (Hvalič-Touzery et al., 2022c), focusing either on informal caregivers or care recipients. Caregiver-focused outcomes included reassurance, reduced worry, and increased feelings of safety, while care recipient-focused outcomes addressed perceived independence and security. Responses were rated on a five-point scale from 1 (“strongly disagree”) to 5 (“strongly agree”). The four items demonstrated high internal consistency (Cronbach’s α = 0.906).
Data Analysis
The statistical analyses focused primarily on comparing informal caregivers of older adults with and without dementia. Descriptive statistics summarized the participant characteristics, and group differences were examined using chi-square tests for binary variables and independent-samples t-tests for continuous measures such as care burden, acceptability of telecare functionalities, and the perceived psychosocial outcomes of telecare use. All analyses were performed using SPSS version 27. We used the STROBE cross sectional checklist when writing our report (von Elm et al., 2008).
Results
Participant Characteristics
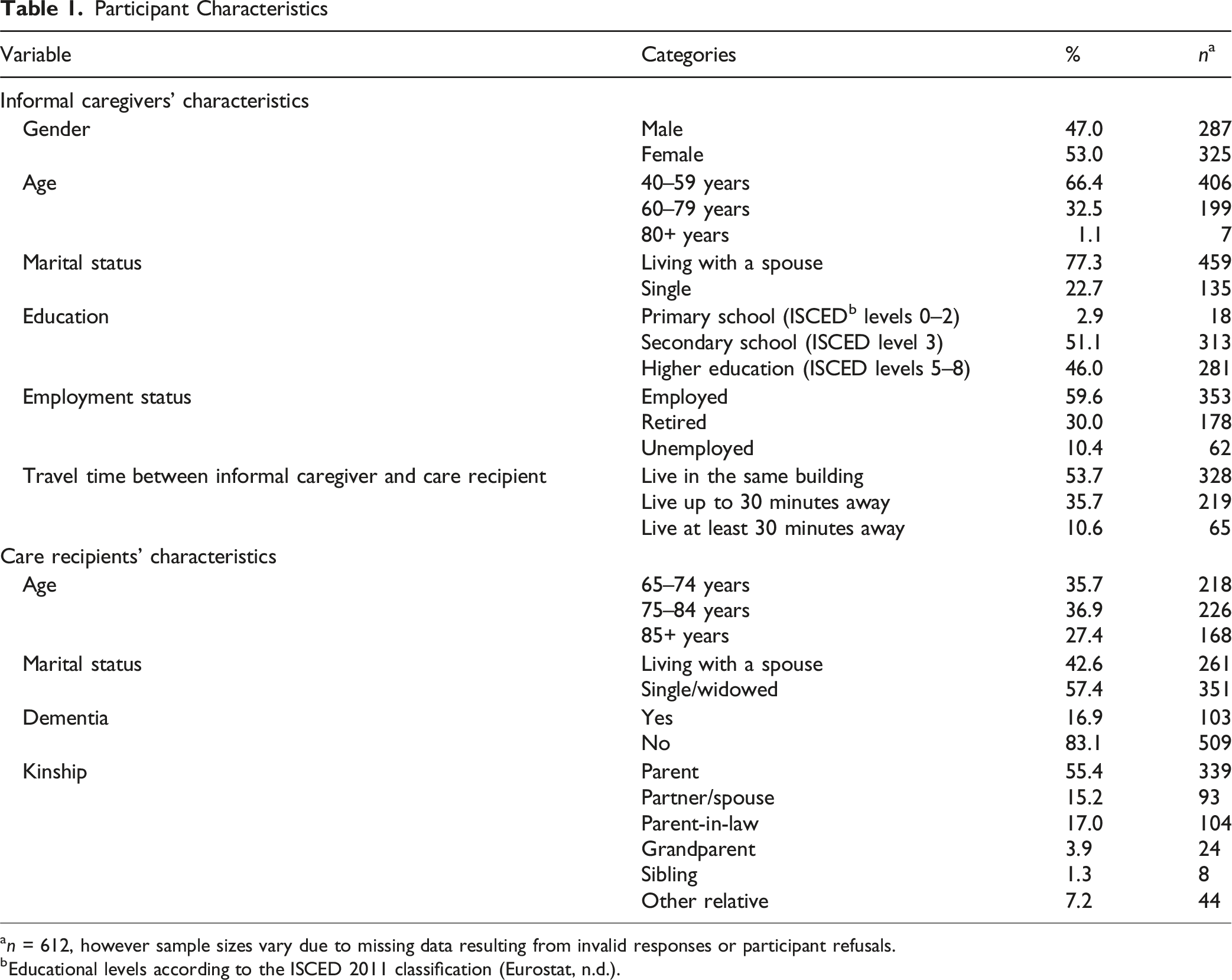
an = 612, however sample sizes vary due to missing data resulting from invalid responses or participant refusals.
bEducational levels according to the ISCED 2011 classification (Eurostat, n.d.).
Comparative Sample Characteristics: Older Adults With and Without Dementia
Characteristics of Older Adult Care Recipients
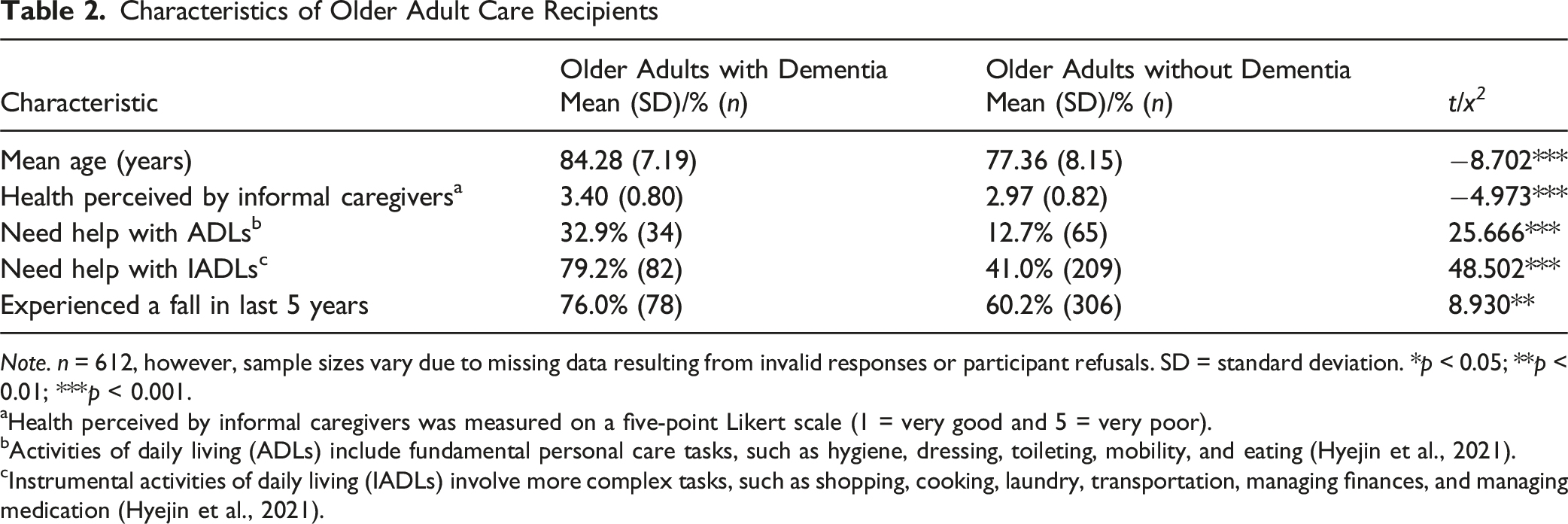
Note. n = 612, however, sample sizes vary due to missing data resulting from invalid responses or participant refusals. SD = standard deviation. *p < 0.05; **p < 0.01; ***p < 0.001.
aHealth perceived by informal caregivers was measured on a five-point Likert scale (1 = very good and 5 = very poor).
bActivities of daily living (ADLs) include fundamental personal care tasks, such as hygiene, dressing, toileting, mobility, and eating (Hyejin et al., 2021).
cInstrumental activities of daily living (IADLs) involve more complex tasks, such as shopping, cooking, laundry, transportation, managing finances, and managing medication (Hyejin et al., 2021).
All following analyses comparing both groups of informal caregivers were conducted using independent-samples t-tests.
Care Burden
Primary Outcome Measures
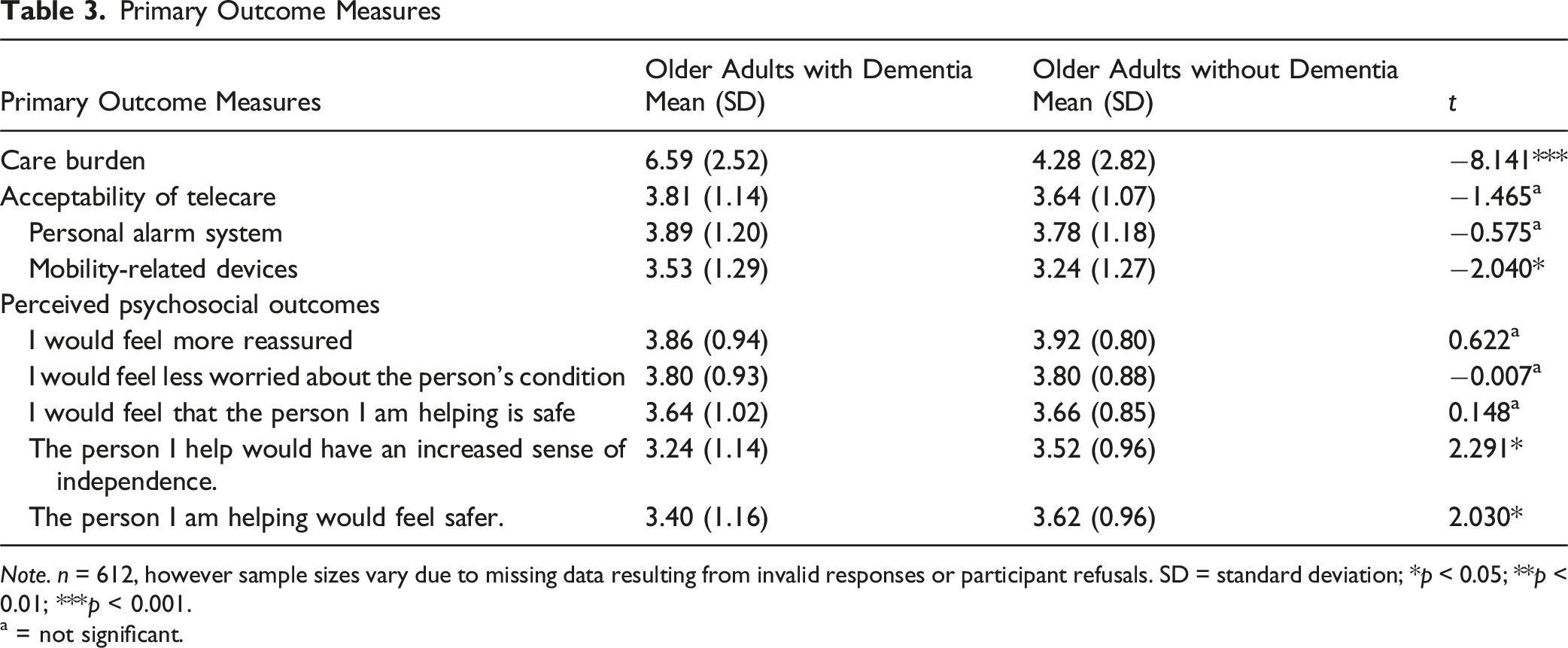
Note. n = 612, however sample sizes vary due to missing data resulting from invalid responses or participant refusals. SD = standard deviation; *p < 0.05; **p < 0.01; ***p < 0.001.
a = not significant.
Acceptability of Telecare
Informal caregivers of older adults with dementia rated mobility-related telecare technologies more favorably than informal caregivers of those without dementia (mean = 3.53 vs. 3.24, p < 0.05). Overall telecare acceptability was relatively high in both groups, with mean score of 3.81 for informal caregivers of older adults with dementia and 3.64 for those without, though this difference was not statistically significant (p > 0.05). No significant differences were observed for personal alarm systems or fall detectors (p > 0.05).
Perceived Psychosocial Outcomes
Informal caregivers of older adults without dementia rated care recipient-focused outcomes, such as increased independence and safety, significantly higher than informal caregivers of those with dementia (p < 0.05). By contrast, caregiver-focused outcomes did not differ significantly between the two groups. Both groups rated these outcomes positively, with the highest scores for increased reassurance and reduced worry (see Table 3).
Discussion
This study explored the differences between Slovenian informal caregivers of older adults with dementia and those without dementia, focusing on care burden, acceptability of various telecare services, and perceived psychosocial outcomes of telecare use. It found significant differences in the care burden experienced, consistent with Steinsheim et al. (2023), who argued that more severe dementia is associated with higher care burden due to increased neuropsychiatric dementia symptoms and the simple need for more care and assistance. While numerous studies from other countries have similarly emphasized the detrimental effects of caregiving on both physical and mental health (Brini et al., 2021; Gérain & Zech, 2019), no such research has been conducted in Slovenia. These findings further highlight how caring for an older adult with cognitive impairment places a significantly greater burden on informal caregivers simply due to the complex and demanding nature of such care (Budnick et al., 2021).
While the overall acceptability of telecare was high, informal caregivers of older adults with dementia expressed a stronger preference for mobility-related technologies, such as motion sensors and GPS tracking. These technologies are particularly relevant for addressing dementia-related risks, including wandering (Bartlett & Brannelly, 2019; McMaster et al., 2018), which can pose significant safety risks and increase the care burden for informal caregivers (Lindeza et al., 2020). This finding aligns with previous studies showing that informal caregivers often value mobility-related devices for their potential to reduce supervision demand and enhance safety (Ehn et al., 2021; Firouraghi et al., 2022). Earlier research has also noted that such devices are most useful in the early stages of dementia, when individuals can still engage with them
In contrast, no significant differences were found in the acceptability of personal alarm systems. This may reflect that these devices address broad safety needs, such as fall risk and emergency response, that are common across caregiving situations and not specific to dementia, and that practical issues like inconsistent device use, forgetfulness, or false alerts are frequently reported in both dementia and non-dementia caregiving (Stokke, 2016).
These findings help to explain the mixed results in previous research on telecare acceptability. While some studies have emphasized the importance of care recipients’ level of dependency—particularly in relation to dementia (Hvalič Touzery et al., 2022c; Thordardottir et al., 2019)—others suggest that dementia does not influence acceptability (Dolničar & Hvalič-Touzery, 2024). Our results suggest that, while there are no statistically significant differences in the overall acceptability of personal alarm systems or telecare in general, significant differences emerge for mobility-related devices. This underscores the importance of distinguishing between the different types of telecare services when investigating their acceptability.
Perceived psychosocial outcomes of telecare use were evaluated across two categories: caregiver-focused outcomes and care recipient-focused outcomes. The average scores for both categories were above average, suggesting that informal caregivers generally perceive telecare as likely to provide meaningful emotional and psychological benefits while also emphasizing caregiver-focused outcomes such as increased reassurance and decreased anxiety.
Previous empirical studies have reported similar positive psychosocial outcomes from actual use of telecare by informal caregivers; for example, Dolničar et al. (2017) concluded that telecare can reduce anxiety and worry and provide a greater sense of security and reassurance because informal caregivers can monitor their care recipients’ well-being remotely. Similarly, Cook et al. (2017) and Karlsen et al. (2019) emphasized that telecare provides peace of mind and increases safety, particularly when there is a risk of falling or wandering.
Interestingly, while the caregiver-focused psychosocial outcomes did not differ significantly between the two groups, informal caregivers of those without dementia reported higher perceived benefits in terms of the care recipient’s independence and safety. This may be because informal caregivers of those with dementia are aware that cognitive decline can limit the care recipient’s ability to interact with or benefit from such telecare technologies. As dementia progresses, individuals may struggle to use devices like pendant alarms or even to understand their purpose, lowering caregivers’ expectations of their effectiveness (Hvalič-Touzery, 2022d; Smole Orehek, 2022; White et al., 2020). Overall, our findings align with this literature, while also indicating that expectations of care recipient outcomes may be more modest in dementia caregiving contexts.
Implications
Our findings also hold practical relevance in that they may contribute to the development of more effective telecare solutions that support both informal caregivers and care recipients. Telecare solutions that address dementia-specific risks, such as wandering, may reduce care burden and help mitigate care poverty. Importantly, our findings support international evidence that highlights the need to design telecare systems that can be tailored to the severity and progression of dementia. Factors such as the size of a device and its complexity, reliability, ease of use (Nasrun et al., 2024; Sriram et al., 2019), and greater flexibility in design and implementation should also be considered (Gibson et al., 2019; Guisado-Fernández et al., 2019). As Chien et al. (2024) argue, for technology to be both accepted and effectively used, it must go beyond user-friendliness and be thoughtfully designed to meet the distinct challenges of different dementia trajectories.
Strengths and Limitations
A key strength of this study is that it is the first comprehensive national research in Slovenia to explore how the unique demands and stressors of dementia care produce differences in informal caregivers’ preferences for telecare devices and their perceived psychosocial outcomes. However, several limitations should be noted. While the sample was sufficient for group comparisons, the use of quota sampling and online surveys may limit generalizability due to potential self-selection bias. Self-reported data also creates the possibility of recall or social desirability biases. Because dementia status was caregiver-reported rather than clinically validated, some misclassification is possible, and results should be interpreted with appropriate caution. This study also did not control for potential confounds, such as dementia severity, caregiving duration, or previous experience with telecare, which may all shape informal caregivers’ perceptions. Additionally, while telecare functionalities were analyzed separately for acceptability, the psychosocial outcomes were considered in aggregate, limiting insights into which technologies might offer specific emotional or psychological benefits.
Future Research
Future studies should seek larger, more diverse samples, especially among dementia caregivers, and account for variations within this group. A study exclusively targeting this population could provide deeper insights into the patterns observed and better contextualize the current study’s findings. Future research should also expand upon distinctions between telecare functionalities and psychosocial outcomes and explore possible complex relationships using multivariate or longitudinal methods. Our results indicate that future work should also examine acceptability in relation to specific types of telecare rather than as a single category and consider the stage of dementia when interpreting caregivers’ responses. Moreover, connecting caregiver-focused and care recipient-focused psychosocial outcomes more explicitly to individual telecare functionalities (e.g., GPS trackers to caregiver reassurance and care recipient safety, or motion sensors to fall prevention and reassurance) would substantially strengthen the practical implications of this line of research. Finally, evaluating the real-world use and effectiveness of tailored telecare solutions would support the design of user-centered technologies that truly benefit informal caregivers and care recipients alike.
Conclusion
This study contributes new evidence from under-researched Slovenian context, where the uptake of digital healthcare is increasing, but the use of telecare in dementia care remains limited. Our findings reveal distinct differences between informal caregivers of older adults with and without dementia, particularly in terms of care burden and telecare perceptions. Informal caregivers of people with dementia reported a greater burden and showed a stronger preference for mobility-related technologies, while both groups recognized psychosocial benefits—especially increased reassurance and reduced worry. However, informal caregivers of those without dementia perceived greater positive impacts on the care recipients’ independence and safety. These findings underscore the importance of personalized telecare approaches that align with the caregivers’ specific contexts. As aging in place becomes a central policy goal, investing in tailored, effective telecare solutions will be essential for supporting both informal caregivers and the older adults for whom they care.
Footnotes
Ethical Considerations
The study received ethical approval from the Ethics Committee on Research at the Faculty of Social Sciences (ECRFSS) on 12 March 2021 (Reference: 801-2021-020/JG).
Consent to Participate
Prior to participation, all respondents were presented with an informed consent statement at the beginning of the survey. By proceeding with the survey, participants indicated their informed consent to participate in the study.
Author Contributions
All authors contributed to the study conceptualization, methodology, formal analysis, investigation, and the draft of the manuscript. All authors read and approved of the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Slovenian Research and Innovation Agency (ARIS) under research grants J5-1785 and J5-4578. Additionally, the study was conducted as part of the doctoral training of the first author, who is funded through the “Young Researchers” program within the research program Internet Research (P5-0399), also supported by the ARIS.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available in the PsychArchives repository, https://doi.org/10.23668/psycharchives.14686.