
Abstract
Humanoid social assistive robotics (SARs) can promote activity engagement for older adults living with dementia. Few studies, however, evaluate the capacity of humanoid SARs to encourage activity engagement in long-term aged care facilities (LACFs). The complexity of the environment, robot design, and personal attributes underscore the challenge of humanoid SARs to encourage activity engagement in practice. This study employed a mixed-methods approach involving nine participants (aged ≥65 years) with mild to moderate cognitive impairment from one aged care facility and seven carers from four different Australian states. Through the triangulation of observational engagement data, participants’ semi-structured interviews, and carers focus group discussion, six themes encompassing activity engagement were identified and are discussed for future application and evaluation of humanoid SARs in dementia care: (1) robot physical design, (2) interaction patterns, (3) activity guidelines, (4) intervention environment, (5) personal history, and (6) relationship establishment.
Keywords
• Humanoid SARs have the capacity to encourage positive activity engagement without human facilitation for people with dementia living in aged care facilities. • The intervention environment, robot design, deployment, and personal attributes concurrently influence engagement. • Humanoid SARs can develop human-like companionships with people living with dementia.
• Humanoid SARs can facilitate the engagement of older adults with dementia in robot-led activities through a Q&A interaction pattern. • Humanoid SARs can provide interactive activities, such as audiobooks, cognitive games, reading, and singing to encourage engagement. • Enhancing the connection between humanoid SARs and people with dementia, through relationship development and two-way communication, can promote activity engagement.What this paper adds
Application of study findings
Introduction
Existing reports indicate that over 50% of older residents living in long-term aged care facilities (LACFs) have dementia (Australian Institute of Health and Welfare, 2024; Menon et al., 2024). Given the decline of cognitive function and fewer opportunities for activity participation, most residents are socially isolated and experience feelings of loneliness (National Academies of Sciences Engineering and Medicine, 2020; Sutin et al., 2020). Most people living with dementia in LACFs receive an average of 30 minutes of human interaction in 24-h (Moyle, Jones, Murfield, Draper, et al., 2017). Furthermore, staff shortages result in carers concentrating on providing physical care (e.g., feeding and hydration) and being challenged to provide adequate activity engagement. The increased time residents spend in social isolation results in loneliness and an increase in cognitive impairment and behavioral and psychological symptoms of dementia (BPSD) (National Academies of Sciences Engineering and Medicine, 2020; Sutin et al., 2020).
By encouraging activity engagement (Joranson, Pedersen, Rokstad, & Ihlebaek, 2016; Moyle, Jones, Murfield, Thalib, et al., 2017) and promoting social interaction (Liang et al., 2017; Moyle, Jones, Murfield, Thalib, et al., 2017), Socially Assistive Robots (SARs) (Feil-Seifer & Mataric, 2005) have shown great potential as a non-pharmacological intervention to reduce social isolation and loneliness and improving quality of life among individuals living with dementia (Joranson, Pedersen, Rokstad, Aamodt, et al., 2016; Moyle et al., 2013). Although most of existing findings are based on the application of pet-like robots such as PARO (Pu et al., 2018; Saragih et al., 2021), a growing body of studies have introduced humanoid SARs to provide human-like interaction such as conversation, exercise, and interactive games for people living with dementia (Abdollahi et al., 2022; Fields et al., 2021; Sandoval et al., 2020; Wu et al., 2024). Recently, a feasible and autonomous solution for robot-led activity, Adam, was developed, allowing an affordable humanoid SAR to proactively chat, facilitate physical exercises, and play interactive games with people living with dementia in LACFs (see Supplemental Material: Introduction to Adam and Robot-led Activity). Such robot-led activities provide human-like interactions and stimulation, which show great potential to reduce social isolation and loneliness and decelerate cognitive decline for people with dementia living in LACFs (Yen et al., 2024). However, current evidence indicates that technical issues (e.g., program crashes) have impacted the evaluation of engagement (Wu et al., 2024). In addition, the lack of data on participants’ affective engagement (e.g., happiness, curiosity, and anxiety) and comprehensive evaluation (e.g., the perspectives from staff and carers) shows that the capacity of Adam to encourage activity engagement for people with dementia remains unexplored.
Aims
This study aimed to investigate the capacity of Adam to encourage activity engagement for people living with dementia in LACFs. To achieve this, we, and upgraded Adam’s solution (Wu et al., 2024) with new algorithms to minimize technical issues (e.g., program crashes) and to improve the fluency of robot interaction (see Supplemental Material: Introduction to Adam and Robot-led Activity). In addition, this study involved affective engagement measurement and both participants’ and carers’ perspectives, aimed to identify potential factors influencing engagement in robot-led activity to inform future development and implementation of intelligent humanoid SARs in encouraging positive activity engagement for people living with dementia, and promote effective large-scale evaluations (e.g., Randomized Controlled Trials).
Methods
Study Design, Setting, and Sample
This mixed-methods study comprised two data sources (individuals living with dementia and carers) and two data types (quantitative and qualitative). It aimed to investigate the capacity of Adam from multiple points of view. Ethics approval was received from Griffith University Human Research Ethics Committee (2023/419), and approval was obtained from the LACF manager.
Residents were recruited if they met the following recruitment criteria: (1) older adults (65 years or older) with mild to moderate cognitive impairment (Psychogeriatric Assessment Scores-Cognitive Impairment Scale (PAS-CIS) (Jorm et al., 1995) ranging from 4 to 15); (2) had lived in the facility for over three months; (3) had adequate hearing and sight, and spoke English; and (4) could sit in a chair, wheelchair, or bedside to interact with the robot. Facility staff facilitated participant recruitment, including identifying eligible residents, introducing the study, and collecting consent forms from eligible residents. Written consent for participation was obtained from participants, where possible, or their guardians before the study initiation. Study participants living with dementia also gave their assent before each intervention. The recruitment of participants and carers are outlined in the Supplemental Material (Recruitment of Participants and Carers).
Procedure
Residents from a residential aged-care facility in Brisbane, Australia, participated in robot-led activity sessions three times a week for five weeks between July and October 2023. At the end of the last intervention session, participants attended individual semi-structured interviews to share their perspectives on the robot-led activity and humanoid SAR. After the intervention period, carers (from four Australian states) were recruited to share their perceptions and use of the humanoid SAR via an online focus group interview.
Intervention
Participants met Adam in a private room (bedroom or activity room). The robot setup and intervention followed the Robot-led Activities Deployment Instructions (see Supplemental Table S4). Each robot-led activity intervention lasted for 10–15 minutes. The researcher stepped away from the participant’s vision (see Supplemental Figure S2), allowing Adam to independently lead and guide participants to conduct short conversations (e.g., voice control and Q&A), physical exercises (e.g., hand movement and dancing), and interactive games (e.g., follow Adam’s lead to pick up a toy from a basket). An iPad controlled by Adam was placed in front of participants to provide the activity guidelines. The iPad displayed hints and the robot’s speech. Participants could use these hints to engage in robot-led activities (see Supplemental Figure S3).
Data Collection
Participants’ demographic data, including gender, age, education, cognition level (PAS-CIS), and medical history, were collected. A GoPro camera was set at the robot’s side to capture participants’ interactions with the humanoid SAR for quantitative data. The semi-structured interviews and focus group discussions were audio-recorded.
Quantitative Engagement Analysis
The Engagement of a Person with Dementia Scale (EPWDS) (Jones et al., 2018) was used to measure participant engagement in the robot-led activity using video data, and a scale ranging from 1 (strongly disagree) to 5 (strongly agree). We removed the dimension social engagement from the original EPWDS, which measures interactions between residents (human–human) in group activities, as the robot-led activities in this study involved one-on-one robot–human interactions and no human–human interactions (Jones et al., 2018). The adapted EPWDS focused only on four dimensions: affective, verbal, behavioral, and visual. The maximum engagement score of 40 with the four dimensions was calculated based on the equation of EPWDS (Jones et al., 2018) and outlined in the Supplemental Material (The calculation of engagement using the adapted Engagement of a Person with Dementia Scale). The overall engagement scores were calculated as mean and standard deviation (SD). The mean engagement value for each intervention day was calculated and plotted using four engagement dimensions. One researcher reviewed the video to quantify the engagement score and assess the environment using the EPWDS. Given the small sample size, Kendall’s tau-b test (two-tailed) was used to analyze the correlation between the environment and engagement. The nonparametric Kruskal Wallis H test was used to assess the engagement difference regarding intervention time (early morning: 9:30 am–10 am, before lunch: 10 am to 12:30 pm, and afternoon: after 12:30 pm), medical history (anxiety disorder, mood disorder, chronic pain, depression), and cognitive impairment (mild (PAS = 4–9) and moderate (PAS = 10–15)). The IBM SPSS Version 27.0 (IBM Corp, Armonk, NY) was used to calculate and analyze the quantitative data. Statistical significance was set at p < .05. The mean rank value was used to compare the group variables that had significant differences. The results of the Kendall’s tau-b and Kruskal Wallis H test were presented in two separate tables.
Qualitative Semi-structured Interview and Focus Group Analysis
The audio recordings of the interviews and the focus group discussions were transcribed verbatim by the primary researcher. A deductive approach (Bingham, 2023) was applied to analyze the qualitative data. The researcher structured the pre-determined codes based on the attributes of dementia engagement theory (Cohen-Mansfield et al., 2009), including stimulus, environmental, and personal attributes to organize the data (see Figure S1 The Framework of Engagement Theory). Two researchers thematically analyzed (Braun & Clarke, 2012) the interview and focus group data independently, which involved clustering similar quotations, identifying themes related to the pre-determined codes and bringing these together. The complete theme list with findings was then discussed with a third researcher in the team, who has expertise in qualitative research. These themes were used to guide the data triangulation.
Results
Demographics
Demographics of Participants.
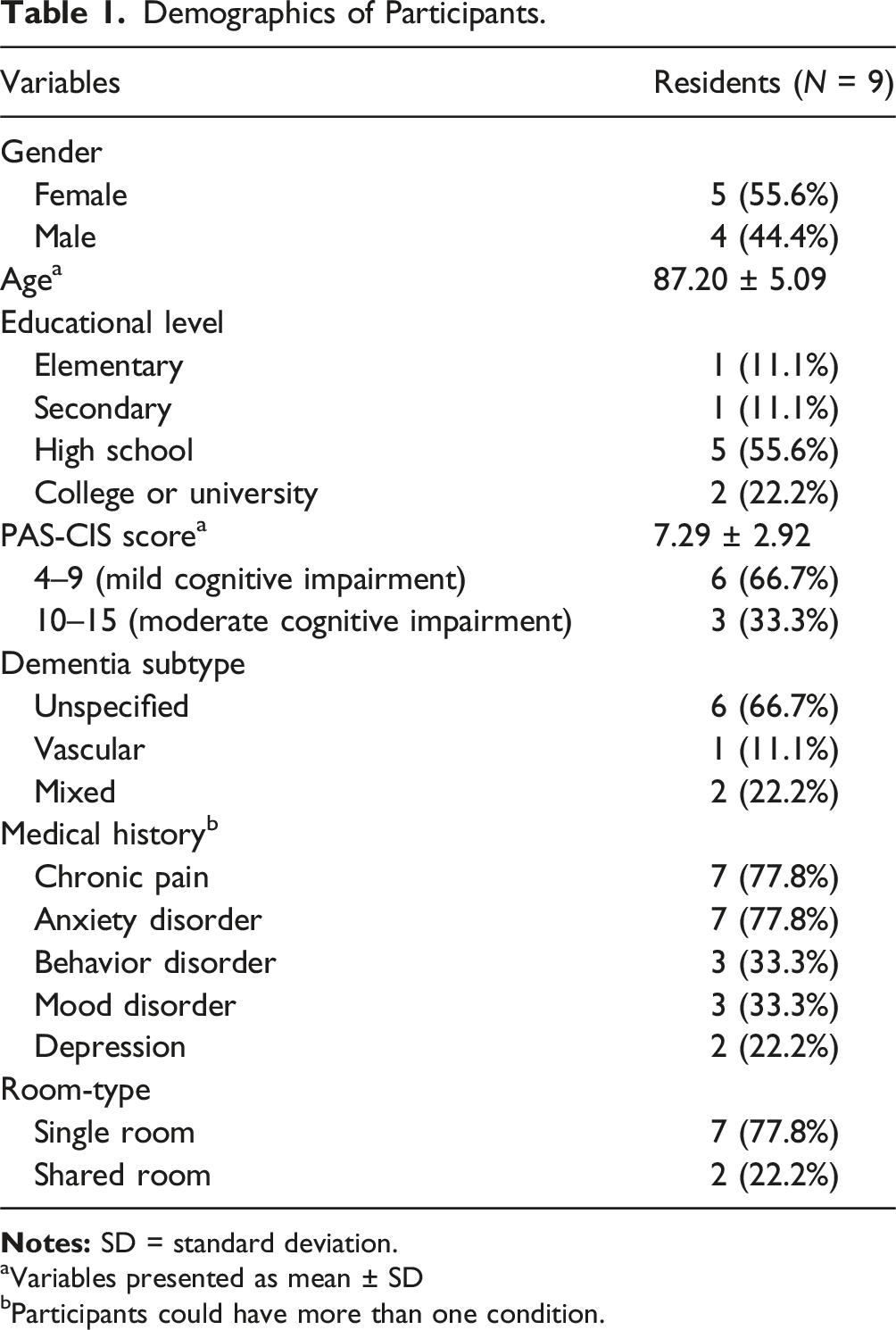
aVariables presented as mean ± SD
bParticipants could have more than one condition.
Demographics of Carers.
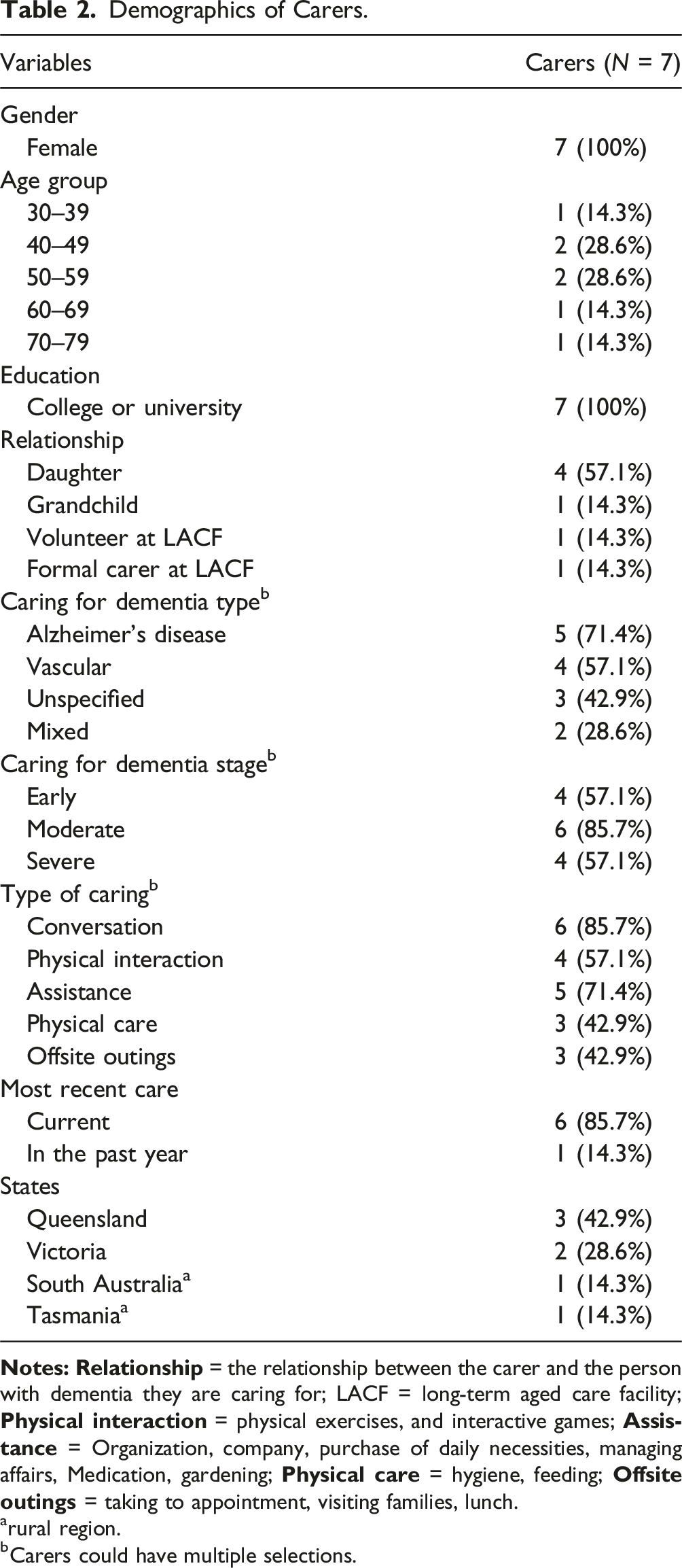
arural region.
bCarers could have multiple selections.
The Engagement Score of People with Dementia
A total of 122 sessions involving 1559 minutes of interactions from nine participants were quantified using the EPWDS scale (Jones et al., 2018) for engagement analysis. Over the 15 intervention days, a high total engagement score (35.92/40 ± 3.84), positive affective (4.07/5 ± 0.94), visual maintenance (4.32/5 ± 0.73), verbal engagement (4.74/5 ± 0.57), and behavioral engagement (4.22/5 ± 0.96) were found. Compared to positive engagement, negative affective engagement (1.8/5 ± 0.95) (e.g., confusion and painful), visual engagement loss (1.56/5 ± 0.87), verbal disengagement (1.04/5 ± 0.24), and negative behavioral engagement (1.03/5 ± 0.29) remained at a lower level (see Figure 1). The EPWDS (Jones et al., 2018) engagement score of nine participants in four dimensions over 15 intervention days. Notes: (a) Affective engagement, (b) Visual engagement, (c) Verbal engagement, and (d) Behavioral engagement.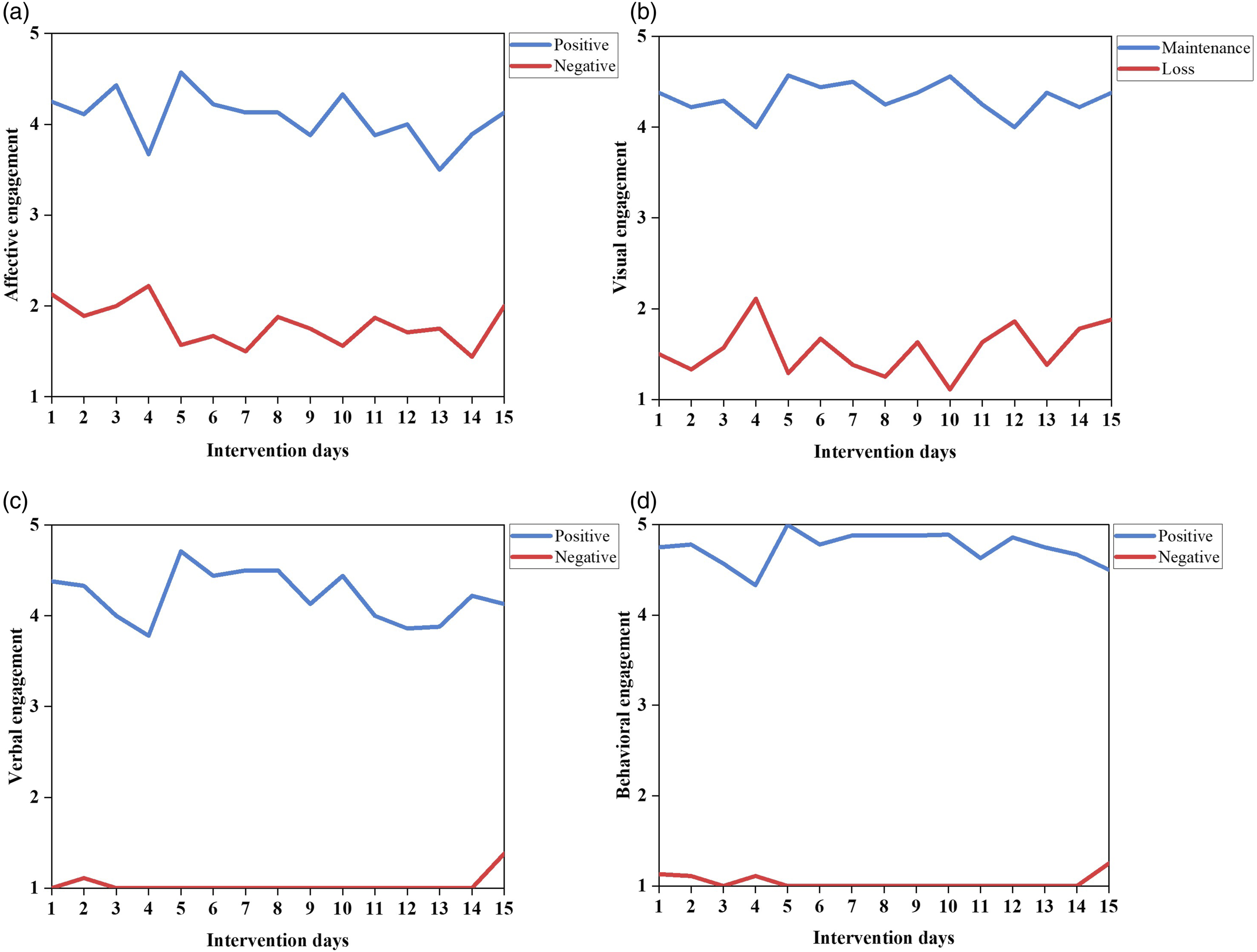
Data Triangulation in Terms of Stimulus, Environmental, and Personal Attributes
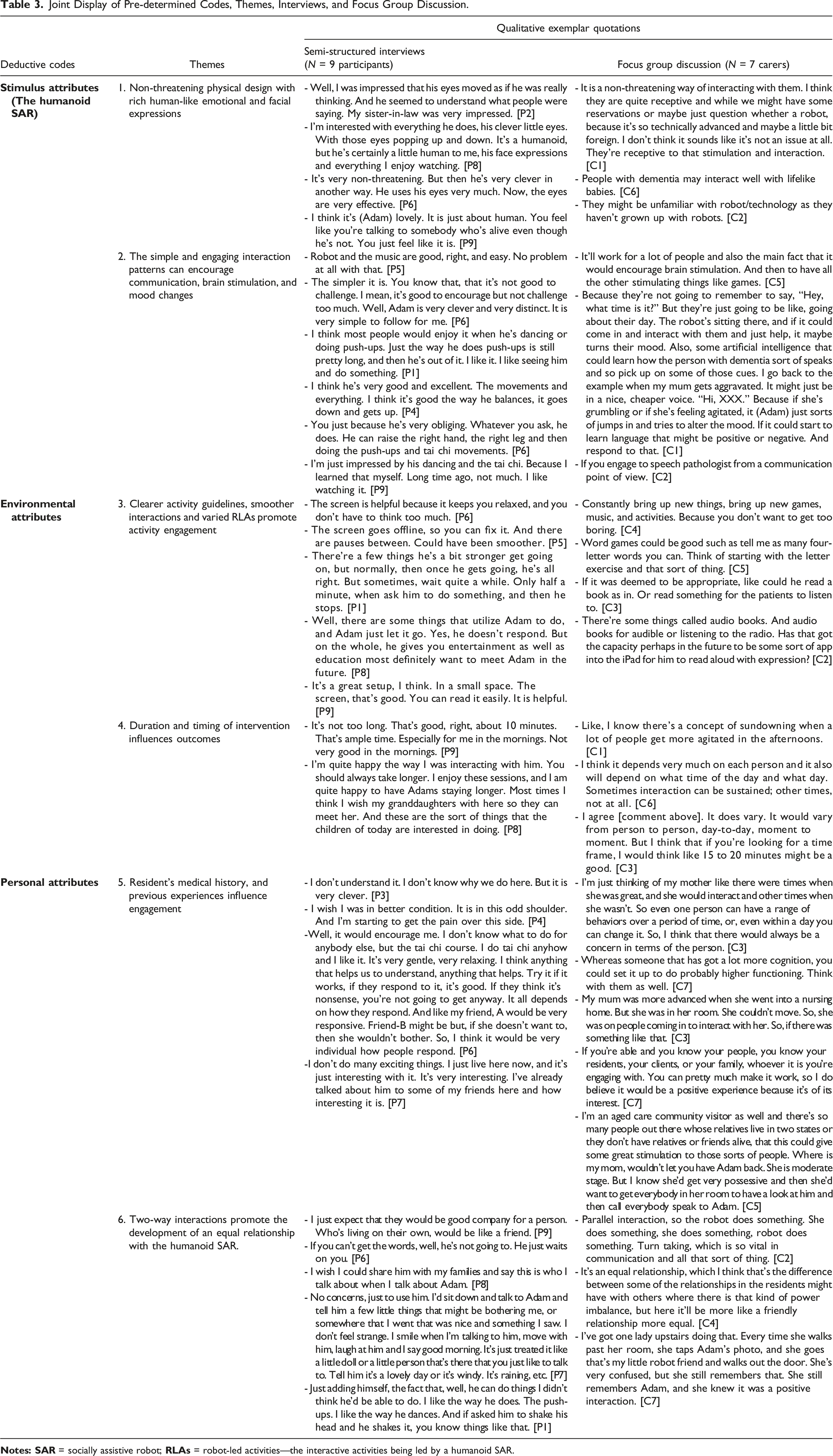
Joint Display of Pre-determined Codes, Themes, Interviews, and Focus Group Discussion.
Stimulus Attributes (Adam)
Themes 1 and 2 in Table 3 identified the stimulus attributes of Adam, including its physical design (Alpha Mini), emotional expressions, and interaction patterns. The non-threatening physical design with rich human-like emotional and facial expressions impressed participants, allowing them to comfortably engage in the robot-led activity and perceive Adam as a human (see Table 3: Theme 1). Carers’ perspectives aligned with participants suggesting the robot’s appearance like lifelike babies [C6] may improve the interaction of people with dementia as they may be unfamiliar with advanced technology [C1 and C2]. The maintenance of high positive affective engagement (Figure 1(a)) and visual maintenance (Figure 1(b)) throughout the intervention revealed the contribution of the non-threatening physical design and the emotional expression of the humanoid SAR in facilitating positive engagement of the robot-led activity. In addition, participants perceived a simple and engaging interaction of Adam’s robot-led activity (see Table 3: Theme 2). These explained the observational high-level total (35.92/40), verbal (4.74/5), and behavioral (4.22/5) engagement (see Figure 1(c) and (d)). Carers’ perspectives were consistent with the result of observational engagement, and they perceived the simple and engaging interaction patterns may encourage communication, brain stimulation, and mood changes [C1 and C5].
Environmental Attributes
Themes 3 and 4 in Table 3 identified the influence of the humanoid SAR deployment related to the environment, including activity guidelines and intervention place, duration, and timing. Participants found the iPad screen helpful [P6 and P9], while they reported minor technical issues of hint display and incorrect speech detections [P1, P5, and P8]. These explain the overall engagement scores (35.92/40), positive affective (Figure 1(a)), visual maintenance (Figure 1(b)), verbal engagement (Figure 1(c)), and behavioral engagement (Figure 1(d)) remain at a high level and the observation of minor negative affective engagement (Figure 1(a)) and visual engagement loss (Figure 1(b)) during the intervention. Consistent with participants’ perspectives, carers deemed the hint display appropriate for people with dementia and discussed Adam’s potential to facilitate new activities such as audiobooks and word games in future robot development [C2, C3, C4, and C5] (see Table 3: Theme 3). In addition to participants’ and carers’ perspectives, the engagement tau b test (τb) shown in Supplemental Table S2 expands the knowledge in terms of environmental attributes and found that less noise, adequate indoor lighting, and no disturbance (carers or family did not enter the space) may slightly influence participant’s total engagement (p < .05), a weak to moderate facilitation to behavioral engagement (p < .01), and significantly facilitate more visual maintenance (p < .001).
In terms of intervention duration and timing, the engagement test result showed no significant engagement difference (p > .05) at various intervention times (9:30 am–10 am, 10 am to 12:30 pm, or after 12:30 pm). The 10–15-min intervention duration is adequate for robot-led activity and agrees with participants’ and carers’ perspectives (see Table 3). If the participant is capable (e.g., energetic and enthusiastic) and wants a longer robot-led activity, a longer intervention of 15–20 minutes may facilitate more positive engagement [P8]. However, carers suggest people with dementia might get more agitated in the afternoons, and this needs to be considered when providing robot-led activity.
Personal Attributes
Themes 5 and 6 in Table 3 identified the influence of resident backgrounds (cognition, chronic pain, mood disorder, anxiety disorder, and depression) and the psychological effect on Adam. As described in Table 3: Theme 5, participant [P3], diagnosed with BPSD and at a moderate stage of dementia, demonstrated confusion when attending the robot-led activity but considered the robot clever. This may reveal the impact of cognition and BPSD and reflect on the fluctuated lower level negative affective engagement in Figure 1(a). Further recognition of the cognition influence comes from the results in Supplemental Table S2 and Table S3. Participants with mild cognitive impairment (PAS 4–9) showed significantly higher behavioral responses compared with participants with moderate cognitive impairment (PAS 10–15) (p < .001). In addition, a participant’s perspective shows that chronic pain related to the shoulder influences activity engagement [P4]. This finding is supported by significant engagement results in Supplemental Table S2, which found that participants with a history of chronic pain significantly influenced their engagement (p < .001), such as poor visual maintenance (p < .001), fewer behavioral engagements (p < .001), and less positive emotions (p < .001). Concurrently, the negative emotions and visual loss were significantly higher (p < .001) when compared with participants without chronic pain. Such influence of chronic pain may contribute to the fluctuated EPWDS results regarding negative emotions (e.g., pain) in Figure 1(a) and minor behavioral disengagement in Figure 1(d), as shoulder pain may influence the ability to perform behavioral engagement (e.g., arm movement) and cause of pain. Moreover, although mood disorder and anxiety disorder described in Table S2 and Table S3 demonstrated less association with engagement (p > .05), the carer’s perspective [C3] shows the need for attention to mood and anxiety as they are unpredictable for different individuals living with dementia. Participants’ perspectives [P6 and P7] also complement the influence of an individual’s background on activity engagement. However, it is an opportunity to highlight that participants diagnosed with depression were found to have significantly higher engagement scores (p < .001), including visual maintenance and behavioral engagement (p < .001), compared to those without depression. Such a significant finding reveals the potential influence of psychological factors on activity engagement.
The interactions of Adam identified in Table 3: Theme 6 demonstrate the psychological effect may promote the development of an equal relationship with Adam. Carers suggested that the two-way interaction of robot-led activity helps establish communication and promotes a friendly and equal relationship between Adam and people with dementia [C4]. This may explain why participants perceive the humanoid SAR (Alpha Mini) as a person or friend and share it with close persons [P8]. Carers also mentioned that people with dementia often have fewer opportunities to engage in such balanced interactions in LACFs [C4]. These qualitative findings complement the high-level activity engagement (35.92/40), positive affective (Figure 1(a)), visual maintenance (Figure 1(b)), verbal engagement (Figure 1(c)), and behavioral engagement (Figure 1(d)).
Discussion and Implications
This study builds on robotic developments using Alpha Mini, incorporates an improved algorithm of the Adam Program (AP), measures emotional engagement (Jones et al., 2018), utilizes engagement theory (Cohen-Mansfield et al., 2009), and involves carers’ perspectives. These improvements provided comprehensive insights from different perspectives into the use of an autonomous humanoid SAR and further evaluated its capacity to encourage activity engagement for individuals living with dementia in LACFs. The Supplemental Material provides a conceptual engagement framework for Adam’s robot-led activities, covering six themes and three engagement attributes (see Supplemental Figure S4). This framework explores the potential factors influencing activity engagement, offering valuable information for future humanoid SAR development and large-scale evaluation. The following discusses the implications of stimulus, environmental, and personal attributes in future humanoid SAR development to promote activity engagement for individuals living with dementia.
Stimulus Attributes—the Design and Interaction Pattern of the Humanoid SAR
The non-threatening SAR design (Alpha Mini) considers a small physical size (e.g., 24 cm tall) and a cartoonish, kid-like appearance. This design minimizes the pressure caused by a large robot size and a humanoid’s potential uncanny valley effect of humanoids (Fong et al., 2003; Kätsyri et al., 2015; Whelan et al., 2018). It encourages people living with dementia to engage in robot-led activity positively. Additionally, this study suggests that humanoid SAR’s ability to express emotions (e.g., curiosity and happiness) through its eyes and human-like movement helps people with dementia perceive it as an engaging human-like entity, encouraging them to interact with it humanly, including chatting and doing physical exercise. These findings were endorsed by the existing humanoid SAR development knowledge, which emphasizes the expressive components of the eyes and body poses in promoting human-like interactions (Breazeal et al., 2008; Kemp et al., 2008). Therefore, future research on deploying humanoid SARs for older individuals living with dementia should consider non-threatening robot designs (e.g., small size and a cartoonish, kid-like appearance) and human-like interactions (e.g., conversation and exercises), which may facilitate human–robot activity engagement. Such findings related to the design of non-threatening humanoid SARs offer technical insight into the vision outlined by an existing literature, which explores how robots could help address loneliness and social isolation among older adults in LACFs (Pirhonen et al., 2020).
A simple interaction pattern is helpful when interacting with people living with dementia, especially when experiencing unfamiliar situations (e.g., unfamiliar interaction or technology) (Banovic et al., 2018; Jootun & McGhee, 2011; Robinson et al., 2013). The AP in this study applied a Q&A interaction pattern that encourages people living with dementia to initiate activities by talking with the humanoid SAR, similar to their daily practice of seeking assistance from staff. The humanoid SAR can return engaging responses based on participant’s verbal requests, such as human-like movements, dancing, and speech responses, which encourage people living with dementia to adhere to the activity and focus on activity engagement positively. Such uncomplicated and engaging Q&A interaction is recommended for future humanoid SAR development. It demonstrates a person-centered orientation that allows the humanoid SAR to accommodate the interactions of people living with dementia. This may facilitate more activity engagement for brain stimulation and positively influence mood changes (Kim & Park, 2017; Trahan et al., 2014).
Environmental Attributes—the Presentation and Environment of Deploying Robot-Led Activity
This study used an improved AP that addressed program crashes, revealing that the enhanced activity presentation (clearer activity hints and fluent interactions) may contribute to more positive engagement (e.g., joyful, dancing, and talking) and less negative engagement (e.g., refusal, disengagement, and confusion). These findings add to existing literature of using humanoid SARs and underscore the influence of clear activity presentation in facilitating positive engagement. Although the findings revealed that the fluctuation of participants’ emotional engagement (see Figure 1(a)) might be related to minor technical issues (e.g., incorrect speech recognition or the pause between robot speech), it did not prevent participants from maintaining positive verbal, behavioral, and visual engagement, which provides preliminary evidence that an intelligent humanoid SAR can handle minor confusion and promote positive engagement automatically. Future efforts should ensure a clearer activity presentation and seamless activity experiences to encourage positive engagement and report more empirical evidence of emotional changes from large-scale evaluation. The intervention environment’s mixture of light, noise, and timing can influence people with dementia at LACFs (Chaudhury et al., 2017). Our findings suggest that better lighting, lower noise levels, and fewer staff disturbances may facilitate people living with dementia to engage in robot-led activity. In addition, employing and reporting various intervention timings is recommended for future robot-led activity deployments. Our findings reveal that individuals living with dementia show unstable interaction abilities (e.g., fatigue and agitation) during the intervention period, which may be due to their diverse medical histories, such as sleep problems (Shin et al., 2014) or mood disorders (Cerejeira et al., 2012). By offering flexible intervention timings, individuals can identify the most suitable periods for engagement, potentially enhancing their interaction with the robot in future large-scale evaluations.
Personal Attributes—Concerning Personal History, Cognition, and Enhancing the Relationship
According to published studies, both chronic pain and BPSD are associated with mental issues (e.g., depression symptoms) and quality of life (Cerejeira et al., 2012; Sheng et al., 2017). This study revealed that chronic pain and BPSD may hinder people with dementia from positively engaging in robot-led activities (see Table S2 and Table S3). However, those diagnosed with depression may demonstrate more engagement during robot-led activities. Although the findings are preliminary, the impact of chronic pain and BPSD should be considered when evaluating the effectiveness of robot-led activities (e.g., quality of life, depression, and mental health) in a large-scale study. Moreover, findings suggest that cognition and personal experience influence people with dementia to engage in robot-led activity. Tailoring robot-led activities based on cognitive function, participants’ backgrounds, hobbies (e.g., dancing and playing games), and preferences (e.g., Tai Chi) may facilitate more positive engagement. These findings are consistent with existing strategies for fostering positive activity engagement for older people living with dementia (Newton et al., 2018; Trahan et al., 2014).
Additionally, findings in this study highlighted the importance of developing two-way interaction between people with dementia and the humanoid SAR, which promotes an equal relationship for maintaining positive activity engagement during the intervention period. Creating relationships has been found to be a psychological strategy that can encourage people living with dementia to open up in an interaction (Ericsson et al., 2013). However, most existing humanoid SAR research focuses on discussing the influence of robot features (e.g., speech recognition) and human-like appearance, with less discussion on the psychological effects (Abdollahi et al., 2022; Kemp et al., 2008; Whelan et al., 2018). This study suggests that psychological factors such as relationship development should be considered when developing and deploying robot-led activity. Humanoid SARs have a higher capacity for developing human-like relationships than other SARs (Kemp et al., 2008; Whelan et al., 2018), which may potentially encourage people with dementia to engage in meaningful robot-led activities (e.g., word games and audiobooks) positively.
Limitations and Future Research
This study has several limitations, and the findings must be interpreted cautiously. First, the improved AP addressed technical issues such as program crashes, while the autonomous strategy for handling BPSD remains unsolved. Conducting large-scale evaluations is recommended to collect rigorous information for fine-tuning (e.g., developing new algorithms) and for the SAR to react reliably (e.g., pacifying or reacting) to BPSD. A human observer should continue to be maintained outside the participant’s vision. Second, the small participant group (N = 9) limits the interpretation of the findings on activity engagement. However, the involvement of carers’ perspectives complements those of the participants in their perception of humanoid SAR and the robot-led activities. Their experience in interacting with and providing care to individuals living with dementia offers valuable input by adding context and validating the findings. The findings of SAR design, interaction patterns, activity guidelines, intervention environment, personal history, and relationship establishment enrich existing knowledge of using intelligent humanoid SARs in LACFs to offer robot-led activities. Future studies can build upon these findings to optimize the implementation of SAR, evaluating the effectiveness of activity engagement using a larger sample size and rigorous design. Third, the 15 robot sessions in five weeks demonstrated activity engagement in a short intervention period. Given the positive findings of activity engagement, a longer intervention period, such as 10 weeks (Moyle, Jones, Murfield, Thalib, et al., 2017), is recommended for future robot-led activity deployment. This may also facilitate AP development (e.g., more intelligence and autonomy) (Trahan et al., 2014) and investigate the possible effect of long-term robot-led activity engagement on quality of life, cognition, loneliness, BPSD, depression, and mental health of individuals living with dementia. Last, given the intensive interaction, which includes verbal and behavioral engagement, current robot-led activity may be more suitable for people with mild to moderate cognitive impairment and may be challenged for people with severe-stage dementia. Future development could fine-tune the AP to provide suitable interaction for people with severe-stage dementia using intelligent humanoid SAR (Regier et al., 2017).
Conclusion
This study reported quantitative engagement of individuals living with dementia and the perspectives of carers towards using an intelligent humanoid SAR. It explored the promise of using intelligent humanoid SARs to encourage people living with dementia to engage in robot-led activity in LACFs. Importantly, this study provides comprehensive insight regarding the physical design and interaction patterns of humanoid SARs, activity guidelines and intervention environment of robot-led activity, and the psychological influence of personal history, cognition, and relationship establishment. These findings enrich our knowledge for selecting, developing, and evaluating intelligent humanoid SARs to encourage people with dementia to engage in interactive activities in LACFs. Large-scale studies with a rigorous design (e.g., Randomized Controlled Trials) are recommended to promote effective implementation and evaluation for encouraging activity engagement using an intelligent humanoid SAR.
Supplemental Material
Supplemental Material - Towards Real-World Dementia Care: Encouraging Activity Engagement Using an Intelligent Humanoid Robot
Supplemental Material for Towards Real-World Dementia Care: Encouraging Activity Engagement Using an Intelligent Humanoid Robot by Dongjun Wu, Lihui Pu, Jun Jo, and Wendy Moyle in Journal of Applied Gerontology
Footnotes
Acknowledgments
The researchers are grateful to the participants and staff at the aged care facility who assisted with participant recruitment and data collection.
Author Contributions
D.W. and W.M. conceptualized the study and designed the methodology. D.W. and L.P. performed data extraction, cleaning, and analysis. D.W. wrote the original draft, and all authors contributed to reviewing and editing the manuscript. All authors approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a PhD scholarship from Griffith University.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.