
Abstract
Chronic pain is prevalent among older people and significantly impacts daily life. Effective communication between healthcare providers and patients is essential for proper pain management, yet existing assessments frequently fail to capture the full complexity of chronic pain, especially in older populations. This study aimed to explore the lived experiences of chronic pain in older people to inform the development of more comprehensive pain assessment. Semi-structured interviews with 20 participants aged 60+ with chronic pain were thematically analyzed and mapped to the International Classification of Functioning, Disability, and Health framework. Chronic pain significantly impacted participants’ mobility, social interactions, and emotional well-being. Participants highlighted the need for a holistic pain assessment that includes psychological and social dimensions alongside physical symptoms. Holistic pain assessments addressing the multidimensional impacts of chronic pain are needed to enhance clinical care and improve older people’s quality of life.
• Provides qualitative insights into lived experiences of chronic pain • Identifies gaps in current pain assessment for older people • Advocates for a multidimensional, patient-centered approach to pain assessment
• Supports developing tools that include psychosocial and functional dimensions • Highlights the importance of training healthcare professionals in holistic assessmentsWhat this paper adds
Applications to Practice, Policy, and Research
Introduction
According to the American Chronic Pain Association (2016), chronic pain, defined as pain lasting more than 3 to 6 months, is prevalent among older people, significantly affecting their mobility and quality of life. Research suggests that up to 80% of people aged 65+ experience acute or chronic pain (Schofield, 2007). Older people are particularly vulnerable to chronic pain due to a higher incidence of musculoskeletal conditions such as arthritis and coexisting chronic diseases, with 50% to 70% experiencing two or more chronic illnesses (Dionne et al., 2006; Stevenson et al., 1992). Multisite pain also becomes more common (Rundell et al., 2019) and is linked to reduced mobility, impaired balance, increased risk of falling, and overall disability (Butera et al., 2019). The consequences of chronic pain extend beyond physical discomfort. Pain negatively influences emotional well-being, leading to anxiety, depressive symptoms, and social isolation (Butera et al., 2019; Reid et al., 2003). It correlates with lower levels of physical activity (Stubbs et al., 2013), challenges during daily activities (Leveille et al., 2001), trouble sleeping (Chen et al., 2011), a higher risk of falls (Leveille et al., 2002), and a reduced quality of life (Sivertsen et al., 2015). It is, therefore, important to manage pain in older people appropriately.
Current policies in Australia encourage practitioners to collaborate closely with older people to ensure that their needs and preferences form the basis for early intervention, assessment, and management of chronic pain (Australia, 2019). Despite the recognition of pain’s complexity, healthcare professionals often face barriers to assessing and managing chronic pain in older people effectively (Weiner et al., 2005). These include limited training in geriatric pain management, reliance on standardized tools that focus predominantly on pain intensity (Froud et al., 2014), and systemic challenges such as time constraints and inadequate resources (Reid et al., 2015). In Australia, the National Strategic Action Plan for pain management emphasizes the significance of a coordinated care strategy, which focuses on self-management and best-practice pain management to improve the quality of life for people suffering from chronic pain (Australia, 2019). This collaborative approach emphasizes the importance of actively listening to older people’s perspectives about their experiences with chronic pain and encourages a more patient-centered approach to care. Developing such collaborative approaches requires a thorough understanding of older people’s pain perception.
Traditional pain assessment tools, such as the Visual Analog Scale (VAS) and Numerical Rating Scale (NRS), primarily measure pain intensity but fail to capture its broader physiological, social, and functional effects (Dalal & Bruera, 2013). More comprehensive tools, like the Geriatrics Pain Measure (GPM) and the Brief Pain Inventory (BPI), assess additional dimensions such as pain’s impact on daily activities and psychological well-being (Cleeland & Ryan, 1991; Ferrell et al., 2000). However, these tools still have some limitations. The BPI focuses on pain intensity and its impact on general activities and mood (Cleeland & Ryan, 1991), but lacks relevance for older people by omitting walking speed, mobility, or the nuanced effects of pain on hobbies and social participation, and its wording may challenge patients of low literacy (Grimmer-Somers et al., 2009). Furthermore, the activities it assesses, such as work, do not always apply to older populations, limiting its relevance. Despite being designed with older people in mind, the GPM also has limitations (Ferrell et al., 2000). While it includes emotional aspects like sadness and depression, it does not adequately cover the functional impact of pain, such as volunteer jobs or caregiving responsibilities. Both tools overlook key aspects like fear of pain, activity avoidance, and communication barriers, which are particularly significant in chronic pain management for older people.
The International Classification of Functioning, Disability, and Health (ICF) framework provides a valuable lens for understanding the impacts of chronic pain (McDougall et al., 2010). By considering the dynamic interaction between a person’s health condition, body functions, activities, participation, and contextual factors, the ICF framework highlights the need for a holistic approach to pain assessment and management. A more robust and individualized approach to pain assessment and management can improve therapeutic outcomes, minimize the risks of under- or over-treatment, and help older people maintain a better quality of life as they age.
Given the gaps in current research, this study aims to explore the lived experiences of chronic pain in older people, focusing on how healthcare professionals assess and address their pain. By applying the ICF framework, this study seeks to understand the relationship between pain, functioning, and the contextual factors that shape the pain experience in older people to provide key domains for clinical discussion and the development of a holistic pain assessment tailored to this group.
Methodology
Participants
The study used a qualitative methodology with one-on-one semi-structured interviews. We aimed to recruit 20 participants to achieve data saturation and capture diverse perspectives on pain’s effect on daily life. Saturation was confirmed since no new themes emerged after interview 17, indicating sufficient data had been collected. No prior relationship existed between the researchers and the participants. Participants were recruited through the Neuroscience Research Australia (NeuRA) volunteer databases. Each participant met the following criteria for inclusion: (i) aged 60 years or older, (ii) experienced chronic pain, as defined as pain lasting three months or more, within the last three months, (iii) cognitively intact, and (iv) able to read, write and communicate in English. Cognition was screened with the “Short Portable Mental Status Questionnaire” (SPMSQ), with a minimum score of eight for inclusion (Boustani et al., 2010). The study received ethical approval from the University of New South Wales (UNSW) Research Ethics Committee, and eligible participants provided verbal consent. A total of 32 participants were initially contacted for the study. Of the 32 individuals initially contacted, eight did not respond, and four missed scheduled interviews, resulting in a final sample of 20 participants.
Data Collection
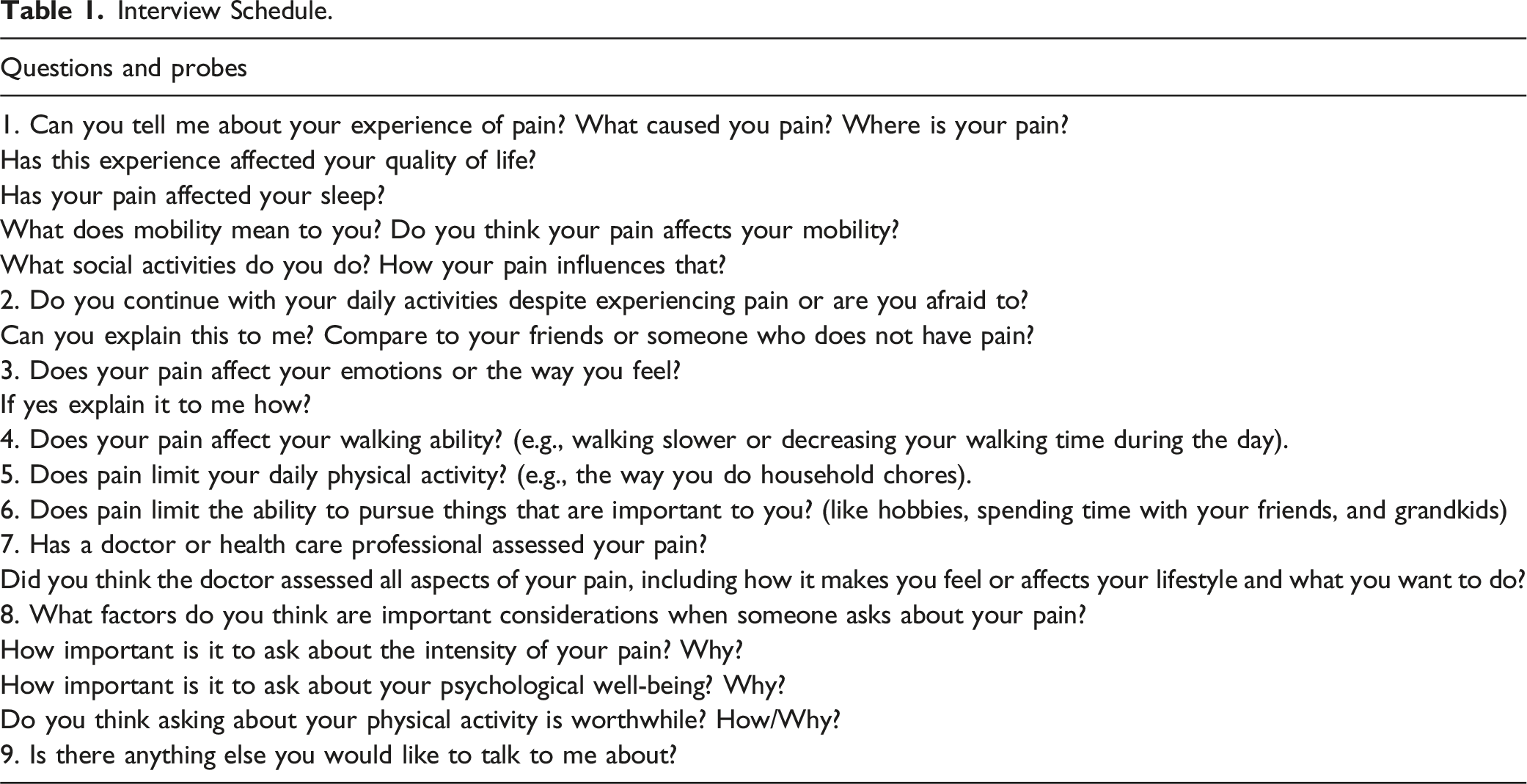
Interview Schedule.
Data Analysis
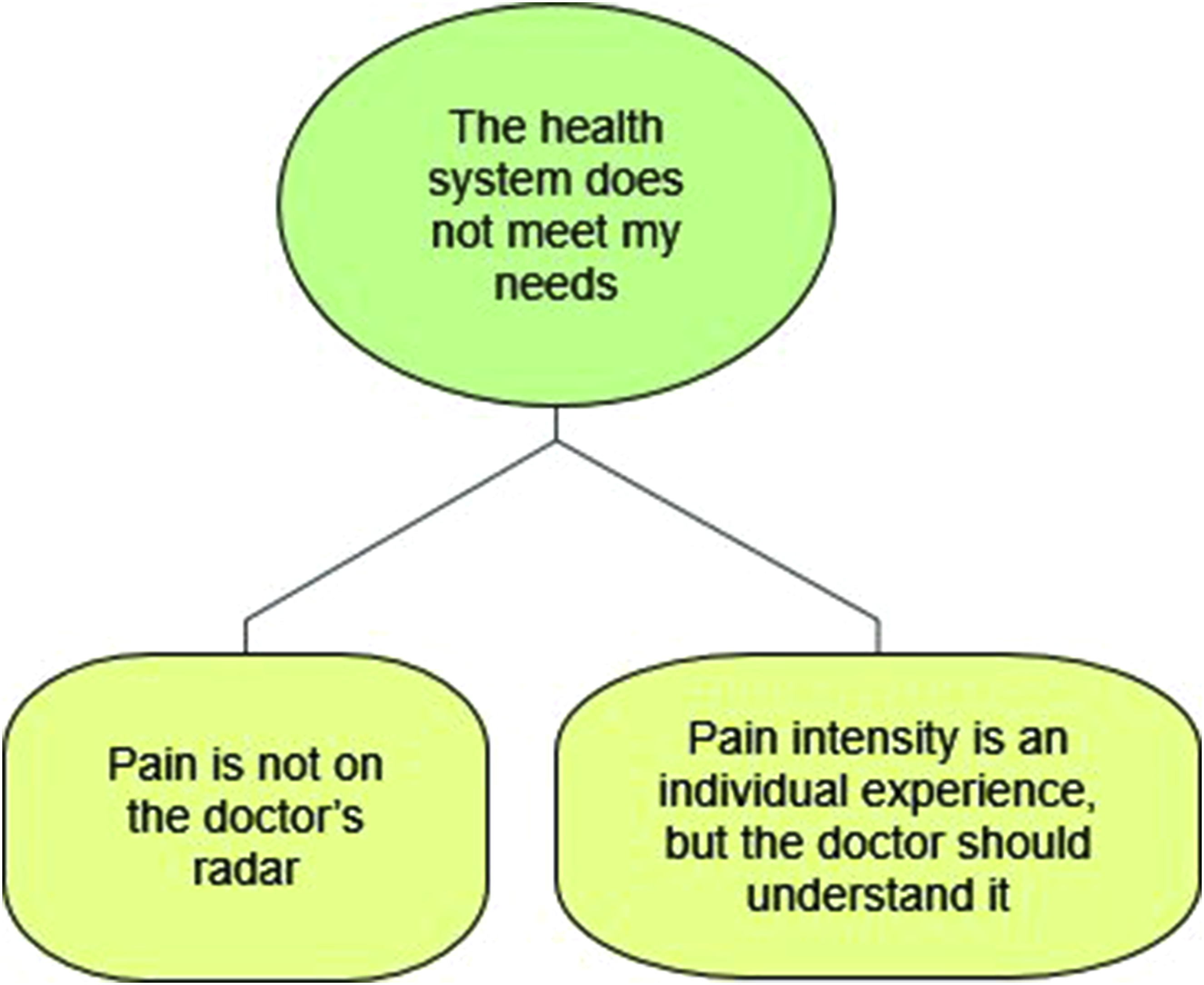
Data were analyzed thematically using the NVivo 12 (Castleberry, 2014), employing both inductive and deductive coding strategies. The analysis followed these steps: familiarization with the raw data, identifying key meaningful text segments, labeling segments of text with a descriptive code, reviewing first-level codes with the co-authors, aggregating first-level codes into higher-level codes by combining similar codes into broader categories, finalizing the codes into themes, and creating a data structure (i.e., a coding tree) to summarize the data-aggregation process. The ICF framework guided the coding process and ensuring themes were mapped to relevant domains of functioning, including body functions, activities, participation, and environmental and personal factors (McDougall et al., 2010). This approach provided a structured framework to comprehensively understand the multidimensional impact of chronic pain. Emerging codes and categories were reviewed with the field expert, MA, who provided guidance and confirmation. Figures 1 and 2 provide the coding tree, while Figure 3 illustrates how the study results were mapped onto the relevant ICF domains. Coding tree for Theme 1: “Pain Impacts All Aspects of My Life” showing its sub-themes and nodes. Coding tree for Theme 2: “The Health System Does Not Meet My Needs” showing its sub-themes and nodes. Mapping with ICF farmework.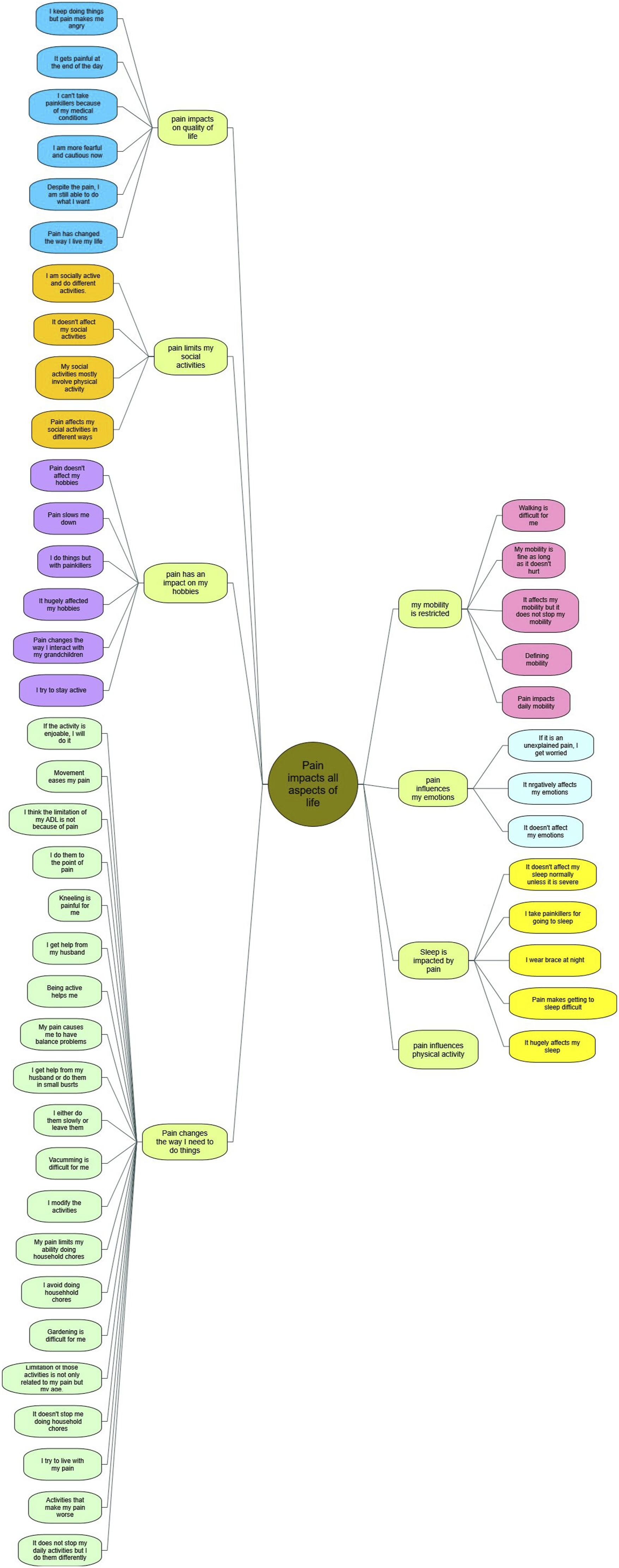

Results
Participant Demographics
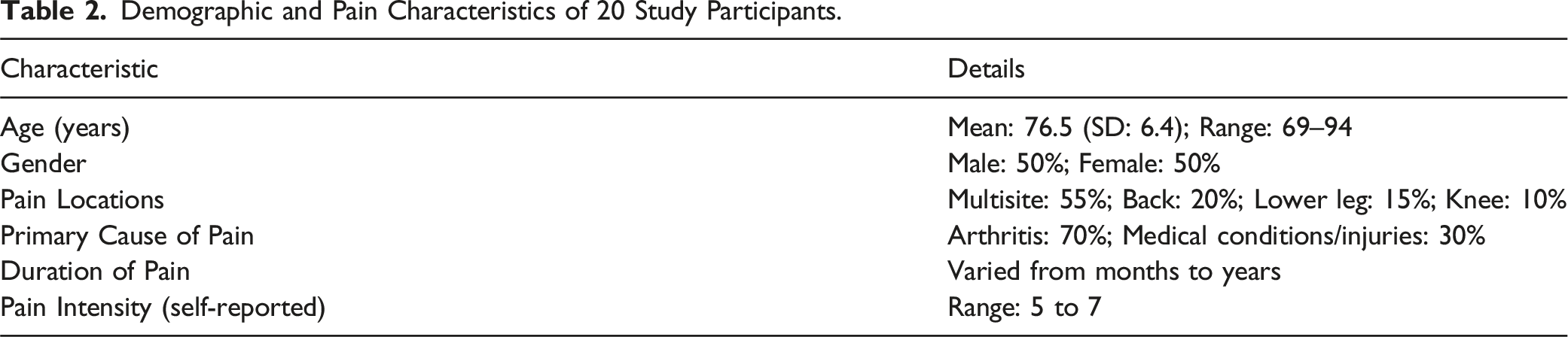
Twenty people between the ages of 69 and 94 participated in the study (mean 76.5 years, standard deviation: 6.4). There was an equal representation of men and women, and most participants reported experiencing multisite pain (55%), followed by lower leg limb pain (25%), and low back pain (20%). Arthritis was the primary cause of pain for 70% of participants, while medical conditions or injuries accounted for the remaining 30%.
Demographic and Pain Characteristics of 20 Study Participants.
The results summarize study participants’ experiences and perspectives on pain, capturing the multifaceted nature of chronic pain experienced by people aged 60 and over. This study identified two key themes: 1. Pain impacts all aspects of my life; and 2. The health system does not meet my needs. Each theme is accompanied by several sub-themes, which illustrate the participants' experiences and perspectives on pain.
Theme 1: Pain Impacts All Aspects of My Life
Sub-Theme: Pain Impacts on My Quality of Life
The impact of pain on quality of life (QOL) manifested in heightened fear and caution for many participants, who shared experiences like: “It’s made me more cautious in what I can do, what I choose to do, and things that I use to enjoy” (female, 73 years) or “I’m much more reluctant to, well, walking downstairs, I don’t mind upstairs, but walking downstairs, I’m really quite nervous if I can’t hold on” (female, 77 years). For participants, pain can also be attributed to changes in lifestyle and the way they live their lives: “I can no longer ride the car. I cannot pursue my hobby, it’s playing piano in the jazz band. I am in constant pain. There are very few movements that don’t cause me pain because they’re all intricately involved with your back, as you probably know” (male, 94 years). However, despite their pain, participants indicated they are still trying to participate in life: “I can tolerate the pain. So, I’m trying to get on with life” (male, 76 years).
Sub-Theme: Pain Limits My Social Activities and Hobbies
The effect pain has on social activities varied between individuals. For participants, pain limits their social activities: “If I’m in a lot of pain. I don’t go basically. So yeah, it’s certainly limited my social activities” (female, 74 years). Others described how pain impacts their hobbies and other activities: “Pain slows me down” (female, 70 years), and the need to “do things with painkillers” (male, 76 years). Despite their pain, participants were still socially active and remained able to do different activities: “I like to be with people, so I’m happy to look at someone to walk with and I swim when I can” (female, 73 years).
Sub-Theme: Pain Influences My Emotions
Pain affects older people’s emotions and psychological well-being. Participants discussed feeling frustrated and depressed because of their pain: “I keep doing things, but pain makes me angry” (female, 70 years). One participant talked about how their pain invokes fear: “If it is an unexplained pain, I get worried” (female, 77 years).
Sub-Theme: Pain Influences My Physical Activity
When asked about physical activity, participants believe it is important to manage their pain: “Exercise helps me to control my pain” (male, 76 years). Given the positive effect exercise has on pain, participants commented that medical professionals should consider exercise’s role in their pain treatment: “I think doctors should not only prescribe medications but also exercise” (female, 77 years). Further, exercise may aid in the treatment of pain through its use as a measure of (dis)ability and coping: “It would give the clinician a much better understanding of not necessarily the degree of pain, but where it comes from, what causes it, when it happens, when it’s not happening” (male, 76 years) and “Because if they [doctors] know how your life is, it’s more likely to be useful to find out what they need to help you with, or I mean, if you can’t do what you normally would like to do, then life isn’t so enjoyable, is it? And then it can affect your emotional health and psychological health” (female, 77 years). Despite agreeing on exercise’s importance, participants still needed help to be more physically active: “I need motivation to do exercise” (female, 71 years). One participant identified that “Movement eases my pain” (female, 77 years).
Sub-Theme: Pain Restricts My Mobility
Mobility is a significant concern for participants. Participants defined mobility as “Freedom” (female, 73 years) and “Being able to do what I used to do” (male, 76 years). While participants stated that pain affects their mobility, it does not stop them: “I limp a bit. But apart from that, I can do the things that I want to do” (female, 77 years). Participants also reported that pain significantly impacts their mobility: “I can’t run. I can’t even run across the street anymore. So, it affects me to that extent. Yeah” (male, 69 years).
Walking, an important form of physical activity, was greatly impacted by pain. Participants stated that walking is difficult and painful for them. One participant said: “I walk more slowly, and sometimes I’m limping, because the knees are painful” (female, 73 years). Others spoke about how pain impacts how long they can walk: “I just can’t walk for more than I would say 100 meters” (male, 75 years). Participants also told us their pain influenced other important predictors of mobility and physical activity, such as balance: “My balance is not good” (female, 70 years).
Sub-Theme: Pain Impacts My Sleep
Pain also affects participants’ sleep. Participants talked about how pain makes staying asleep difficult: “I have a lot of nerve pain in my legs, so I have to get up several times at night walk around, and warm them up” (female, 74 years). Participants discussed that they take painkillers to help them manage their sleep: “It was waking me up, but I’ve now got fairly strong painkillers” (female, 77 years).
Sub-Theme: Pain Changes the Way I Need to do Things
As for activities of daily living, most participants mentioned pain does not stop their daily activities but causes them to modify how they do them: “I do whatever it is that I need to do. I just maybe do it a bit more slowly, or maybe do it a little differently” (male, 76 years).
Theme 2: The Health System Does Not Meet My Needs
Sub-Theme: Pain is Not on the Doctor’s Radar
Participants revealed a gap in the assessment of their pain by healthcare professionals. Participants spoke about how medical doctors rarely inquire about their pain, and when they do, it is to prescribe medications: “The doctors prescribed [a medication] for me and they [doctors] have not been that interested in how I feel about it, or how it’s stopped me doing things” (female, 77 years). Further, participants told us they do not understand how a doctor can help them manage their pain, stating, “A lot of their [the doctors] assessment has been based around the physical aspects and whatever remedies they’re suggesting to help or assist” (male, 87 years).
Participants further mentioned that asking about their psychological well-being during the pain assessment is essential and noted, “I think it is important because, when you feel pain, it does affect your outlook, it does affect your daily life, it does affect your way how to organise your life. You know, daily life, you know whether you can go for a walk, whether you should stay home or whatever. No, I think it is even more than pain you get all this. Yeah, it is important” (male, 75 years), and “Yeah, I was like, like I feel like it can give me the opportunity to talk about my feelings, and maybe he [the doctor] can help with that” (female, 70 years). However, some participants were less eager to share their feelings with the doctor: “Whether they ask or not, I wouldn’t do that” (male, 76 years). For instance, one mentioned: “If I told him [the doctor] that that’s what I was struggling with. I know he would do something to help, but then he might say, well, if it’s something that you have feelings or thoughts. Maybe you need to go and talk to a psychologist, which I don’t think would be the answer. I think that that they will come to a point when I really need. I really want to be assessed, and have some sort of regime, of what medication might be helpful for daily activities or sleeping at night if the pain is keeping me awake. Probably more specific things” (female, 73 years).
Sub-Theme: Pain Intensity is an Individual Experience; One the Doctor Should Understand
As for the importance of asking about the intensity of pain, some participants believe it is very important: “I think the trouble is that doctors don’t ask about intensity. If you say you’ve got pain, they prescribe medication and because I’m incredibly sensitive to medication, and I’ve learned to deal with pain with as little medication as possible, if I say no, I don’t want it, they assume I don’t have much pain” (female, 77 years). One participant reflected, “It is important they should ask that question, but I’ve never seen a GP asking me that question” (male, 74 years).
In contrast, given pain intensity is individually subjective, some participants believe that asking about it is not important: “I always argue about it. That’s (about) level of tolerance and a level of tolerance depends on the context” (female, 74 years). This participant also discussed the limitations to how doctors inquire about and measure pain: “Well, it’s important if I understand that it’s a level of tolerance at the time. But that’s not how it’s presented by doctors. It’s presented as a kind of you know ‘If childbirth is worse, what would you call this?’ you know, it’s a bizarre kind of test” (female, 74 years). Some participants felt that it is more meaningful to understand pain intensity within the context of function: “I think more than intensity is how it affects what I do” (female, 71 years).
Discussion
The results of this qualitative study confirm the complex and multifaceted characteristics of chronic pain in older people. First, the findings highlight the broad impact of pain. Participants described significant emotional and psychological effects, such as increased fear, frustration, and depression, which they often felt were overlooked by healthcare professionals. These dimensions are rarely captured by widely used pain assessment tools, such as the BPI and GMP, which primarily focus on pain intensity and general interference but lack a detailed assessment of emotional or psychological burdens. Participants also reported social and functional limitations due to pain, even when using analgesics. While some could maintain social involvement, others described pain as a barrier to meaningful engagement in hobbies and relationships. Similar studies have reported that pain diminishes and restricts social life (Gillsjö et al., 2021; Makris et al., 2017; Rodriguez et al., 2019). These findings reflect the ICF framework’s emphasis on environmental factors (e.g., accessibility of social support and healthcare resources) and personal factors (e.g., attitudes toward medication and coping strategies) (McDougall et al., 2010). These interconnected factors shape pain experiences and highlight the need for interventions that address both medical and non-medical aspects of pain management. Participants often mentioned disrupted sleeping patterns, a finding consistent with previous research indicating that some older people rely on sleeping medications while others try different sleeping positions for pain relief (Makris et al., 2017; Rodriguez et al., 2019). While existing tools address sleep interference to some extent, they do not adequately capture the strategies older people adopt, such as changing sleeping positions or relying on sleep aids. Pain also adversely affected daily activities, disrupted sleep and exercise patterns, and contributed to mental health challenges, including anxiety, depression, and hopelessness. These findings support the importance of adopting a holistic, patient-centered approach that addresses both the physical and psychological dimensions of pain. Current tools overlook these broader psychosocial impacts, such as losing independence in performing specific daily tasks like gardening or volunteering. Previous studies in older people with low back pain also highlighted the value of integrating social and emotional support to mitigate these broader impacts and improve the overall quality of life (MacNeela et al., 2015; Makris et al., 2017).
Second, the findings highlight the multifactorial impact of chronic pain on mobility and daily activities, a dimension often overlooked in current pain assessment tools. Similar to previous studies, participants described difficulties performing basic tasks such as walking, gardening, shopping, or playing with grandkids (Stensland & Sanders, 2018), activities that provide a sense of purpose and connection. While the BPI includes items related to occupational functioning, this is often irrelevant to retired older people (Cleeland & Ryan, 1991). Similarly, the GPM asks for vigorous and moderate activities like running or lifting heavy objects, which may not reflect older people’s everyday realities or priorities (Ferrell et al., 2000). In contrast, participants in this study emphasized the importance of activities that support their independence and social roles, such as carrying grandchildren, maintaining their gardens, or doing household chores. Mobility, often described as freedom, was restricted by pain, yet participants made significant efforts to stay active within their limitations. These restrictions align with the ICF’s emphasis on the interaction between body functions, activities, and participation (McDougall et al., 2010). Addressing these functional impacts by integrating measures of mobility and daily activities should be inherent to any consultation or questionnaire guiding pain management in older people.
Third, this study reveals pain’s unpredictable and fluctuating nature and the central role of coping strategies in managing its impact. Participants described variations in pain intensity throughout the day and over time, with its effects often disproportionate to their medical diagnosis or physical symptoms. Despite these challenges, participants employed various coping strategies to navigate their daily lives, including modifying activities, using pain medication selectively, and engaging in physical activity when possible. Moreover, participants shared their reluctance to rely on prescription medications, often preferring non-pharmacological approaches like physical activity, relaxation techniques, or cognitive-behavioral strategies. This aligns with the ICF’s focus on personal factors, such as beliefs, attitudes and preferences, influencing how individuals experience and manage pain (McDougall et al., 2010). They expressed frustration at the limited discussion of such alternatives with healthcare professionals, who often prioritized medication as the primary solution. This underscores the importance of addressing beliefs, attitudes, and preferences in pain management plans to support older people in implementing sustainable coping strategies (Main et al., 2010). This is consistent with findings by Gillsjö et al. (2021), who observed that older people adopt adaptive processes, such as taking each day as it comes to manage their pain. Supporting these adaptive strategies is essential and underscores the necessity of personalized pain management plans. Such plans should emphasize non-pharmacological interventions, such as physical activity and cognitive-behavioral strategies, alongside medication (Knoerl et al., 2016; Sitthipornvorakul et al., 2018). Notably, the fluctuating nature of pain is not captured in existing tools like the GPM, which assesses pain primarily through fixed questions that do not account for daily or hourly variability (Ferrell et al., 2000). Similarly, coping strategies—an essential aspect of how older people manage pain—are overlooked in both the GPM and the BPI (Cleeland & Ryan, 1991; Ferrell et al., 2000).
Finally, participants spoke about feeling unheard by healthcare professionals, highlighting gaps in pain assessment and management. Similar to research by Makris et al. (2017), many participants expressed frustration over superficial assessments by healthcare professionals, who often focus on prescribing medications without exploring the broader impact of pain on mental health, daily life, or social participation. Participants shared that healthcare professionals rarely inquire about how pain affects their emotions, daily functioning, or social engagement. For some, this lack of engagement contributed to feelings of dismissal, while others felt their concerns were not taken seriously unless they accepted medication. Such communication deficits can hinder treatment adherence, as older people may struggle to follow prescribed regimens without fully understanding their purpose or perceiving them as relevant to their personal experiences. Such communication deficit contributes to poor adherence to prescribed regimens, with studies showing that up to 70% of older people do not comprehend their medication instructions, underscoring the critical need for healthcare professionals to actively involve patients in decision-making processes (Rosenbloom, 1988). Building stronger patient-provider communication ensures that older people feel heard and involved in decision-making processes. By integrating patient-centered assessments and personalized care plans, healthcare providers can better address the complex needs of this population. Addressing this gap requires a paradigm shift in pain assessment and management for older people, moving beyond conventional pain scales and adopting tools that consider the emotional, social, and functional dimensions of pain.
This study has several limitations that should be considered when interpreting the findings. First, the recruitment of participants from Australia may limit the generalizability of results to other cultural, geographic, and socioeconomic contexts. Second, the study focused on older people willing and able to participate in interviews, which introduces the potential for self-selection bias. Additionally, recall bias could have influenced participants’ recollection of their pain experiences. Finally, the findings may not fully apply to people receiving care from specialized pain clinics, who often experience more severe or debilitating pain compared to those managed in primary care settings. Future research should refine existing pain assessment tools to better capture the multidimensional nature of pain in older populations. There is a need for longitudinal studies examining the long-term impact of personalized, multidimensional pain management strategies, as well as interventions that address systemic barriers, such as time constraints and communication gaps in clinical practice.
In conclusion, this study advances the understanding of chronic pain in older people by highlighting its multifaceted nature and profound impact on emotional, social, and physical well-being. Current pain assessments are insufficient to capture the full scope of these experiences, underscoring the need for more inclusive and patient-centered approaches. Healthcare providers should be trained to use multidimensional assessment tools that extend beyond pain intensity and encompass emotional, social, and functional dimensions. Training should emphasize patient-centered communication and shared decision-making, incorporating non-pharmacological interventions such as tailored exercise programs and psychological therapies into personalized care plans (Hassett & Williams, 2011). By bridging these gaps, healthcare systems can move toward a more compassionate, holistic model of care that truly addresses the diverse needs of this population.
Footnotes
Acknowledgments
We sincerely thank all the participants who generously shared their time and experiences, which were invaluable to the success of this study.
Author Contributions
MS, MA, KS, and KD conceptualized the study and designed the methodology. MS and MA collected and analyzed the data, as well as the data interpretation. The original draft was prepared by MS, with all authors contributing to manuscript review and editing. Supervision was provided by KD and KS. All authors approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the UIPA PhD scholarship from the University of New South Wales (UNSW) and the Pearl PhD program from Neuroscience Research Australia (NeuRA). Additional support was provided by the NHMRC Investigator Grant (APP1193766).
Declaration of Generative AI
During the preparation of this work, the author (MS) used ChatGPT, a generative AI tool by OpenAI, to improve the language. After using this tool, all authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Ethical Statement
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon request.