
Abstract
Symptoms of dementia can impact the nutritional status and quality of life of people with dementia, but there is limited research exploring the dietitian’s role in post-diagnostic care. This study aims to explore the role of a dietitian in a multidisciplinary dementia program for people living in the community. Participants in a twelve-week multicomponent, multidisciplinary post-diagnostic intervention for people with dementia and care partners were offered three consultations with a dietitian to receive dietary assessment, education and advice. Key clinical findings from dietetics case notes of 40 people with dementia were analyzed using a composite case series approach. Of these, 39 required ongoing nutrition support and intervention. Common issues identified include insufficient energy and/or nutrient intake, unintentional weight loss, poor management of comorbidities and difficulties with coordination of care. Dietitians are an integral part of a multicomponent intervention for dementia. Future work is needed to optimize dietetic care models. Running headline. Dietetics in an early intervention for dementia.
• This research provides insights into the role and impact of dietitians within a multidisciplinary early intervention program for people with dementia and their care partners through composite case studies. • Demonstrates common nutrition-related challenges faced by people with dementia and their care partners living in the community, including insufficient energy intake, altered food preferences, and difficulties managing comorbidities. • Highlights unique nutritional support needs for different care partner dynamics (e.g., spouse vs. adult-child care partners) and the importance of tailored dietetic interventions and advice.
• Supports inclusion of dietitians as essential members of multidisciplinary dementia rehabilitation teams to address complex nutritional needs and maintenance of health. • Identifies need for specialized training for dietitians and other healthcare professionals to optimize care for people with dementia and their care partners living in the community. • Informs development of dietetic care models and interventions that consider both the person with dementia and their care partner’s needs to improve the effectiveness and sustainability of nutritional support.What this paper adds
Applications of study findings
Introduction
Dementia is a group of neurodegenerative diseases that contribute to a decline in cognitive functions including memory, judgment, and problem-solving, and can impact a person’s ability to perform daily tasks (Jansen et al., 2015; WHO, 2023). The progressive symptoms and incurable nature of dementia results in challenges for people with dementia as well as their family and care partners (Andrews et al., 2015; Labyak et al., 2024; WHO, 2023). While there is currently no cure for dementia, steps can be taken to maintain the health and quality of life of a person with dementia (Dominguez et al., 2021; Suominen et al., 2015; WHO, 2023). This includes addressing lifestyle factors such as diet, exercise, and stress reduction that have been shown to impact progression of dementia symptoms (Dominguez et al., 2021; Labyak et al., 2024).
Healthy dietary patterns, such as those high in fruits, vegetables, wholegrains, legumes, and omega-3-fatty acids, are associated with a decreased risk of dementia and slow the progression of cognitive decline (Grant & Blake, 2023; Xu Lou et al., 2023). Malnutrition, unintentional weight loss, dysphagia, altered taste and smell, loss of cooking and eating skills, loss of food recognition, and loss of hunger and fullness cues are common in dementia (Dominguez et al., 2021; Jansen et al., 2015; Labyak et al., 2024). These nutrition complications are associated with decreased quality of life and health outcomes for people with dementia through worsening cognition, as well as increasing risk of sarcopenia, frailty and subsequent risk of falls (Labyak et al., 2024; Pacifico et al., 2020; Roque et al., 2013). Furthermore, unintentional weight loss and malnutrition in people with dementia are associated with an increased risk of mortality (de Sousa et al., 2020).
For people with dementia living in the community, poor nutrition status can exacerbate symptoms of dementia and the impact of caring on care partners (Ball et al., 2015; Roque et al., 2013). Ball et al. (2015) identified nutrition-related challenges as one of the largest factors affecting care partners who reported feeling unsupported and uninformed on the topic of nutrition-related care for people with dementia (Ball et al., 2015). Caring for a person with dementia has also been found to impact the nutritional status of care partners due to prioritizing the person with dementia before themselves, increased stress, and lack of time and energy (Labyak et al., 2024; Volkert et al., 2024).
The number of multidisciplinary post-diagnostic support services for people with dementia living in the community in Australia is limited, and existing services are typically poorly coordinated, resulting in gaps in care (NHMRC, 2021). The number of people with dementia in Australia is projected to increase in the coming years, resulting in further challenges to the efficiency and sustainability of many services within the Australian healthcare system (AIHW, 2024; Standfield et al., 2018). This has led to an increased interest in improving support services to assist people with dementia living in their own home (Clemson et al., 2021). Approximately two-thirds of people with dementia in Australia are currently living in the community (AIHW, 2024), and supporting them to remain at home could reduce financial and emotional impacts, and potentially improve health and nutrition outcomes (Clemson et al., 2021; You et al., 2014).
Multidisciplinary interventions for people with dementia and their care partners have the potential to be more effective with the inclusion of a dietitian within the healthcare team (Jones, 2019; Lahiouel et al., 2023; Marshall et al., 2017). Interventions involving dietetic support have resulted in improved nutritional status of people with dementia in both community and residential care settings (Bellantonio et al., 2008; Keller et al., 2003; Rivière et al., 2001; Shatenstein et al., 2017). Dietitians have also been involved in interventions shown to improve quality of life indicators for people with dementia, including their ability to independently complete activities of daily living (Bellantonio et al., 2008; Rivière et al., 2001; Salva et al., 2011). However, there remains limited evidence exploring dietetic-focused interventions for community-dwelling people with dementia and their care partners (Marshall et al., 2017).
There is a recognized need for growth in the size and capacity of the dietetic workforce to support the nutrition of older people, as well as a need for dietitians to be included as part of multidisciplinary teams (Dietitians Association of Australia, 2019). The present study focuses on the role of a dietitian working in the Sustainable Personalised Interventions for Cognition, Care and Engagement (SPICE) program. The program is an innovative twelve-week multidisciplinary, multicomponent post-diagnostic program for people with dementia and their care partners living in the community (D’Cunha et al., 2023). This study examines the value of the dietitian in the multicomponent intervention, identifies common nutrition issues faced by this population and documents the strategies employed by the dietitian in response to these challenges.
Method
Study Design
The study employs a composite case series approach to describe the common concerns of people with dementia and their care partners regarding nutrition and the strategies provided by the dietitian within an innovative multicomponent, multidisciplinary post-diagnostic intervention for people with dementia and their care partners. The composite case studies were developed based on key themes that emerged from qualitative analysis of clinical case material for each participant. Composite case studies illustrate central findings by presenting multiple perspectives as one lived experience (Duffy, 2010). Each composite case study encapsulates an array of complex clinical accounts to build an accessible and nuanced perspective. Composite case series protect participant anonymity and capture shared experiences to highlight common patterns across the experience of multiple participants (Duffy, 2010; McElhinney & Kennedy, 2022). Composite case studies are increasingly valued in medical and clinical literature to present findings in an accessible format, presenting authentic descriptions of participant’s experiences without further burden of data collection, particularly for vulnerable populations such as people with dementia (McElhinney & Kennedy, 2022).
Setting and Context
The study was based at the University of Canberra Hospital Specialist Centre for Rehabilitation, Recovery and Research. The hospital is a public health purpose-built rehabilitation center in the Australian Capital Territory (ACT). The SPICE program aims to address a gap in dementia-specific services in the ACT for people with dementia and their care partners. The program was developed through a collaboration between Canberra Health Services and the University of Canberra, drawing on best available evidence in the design, development, implementation and evaluation stages. Dementia Australia Advocates were consulted in the design and development phases.
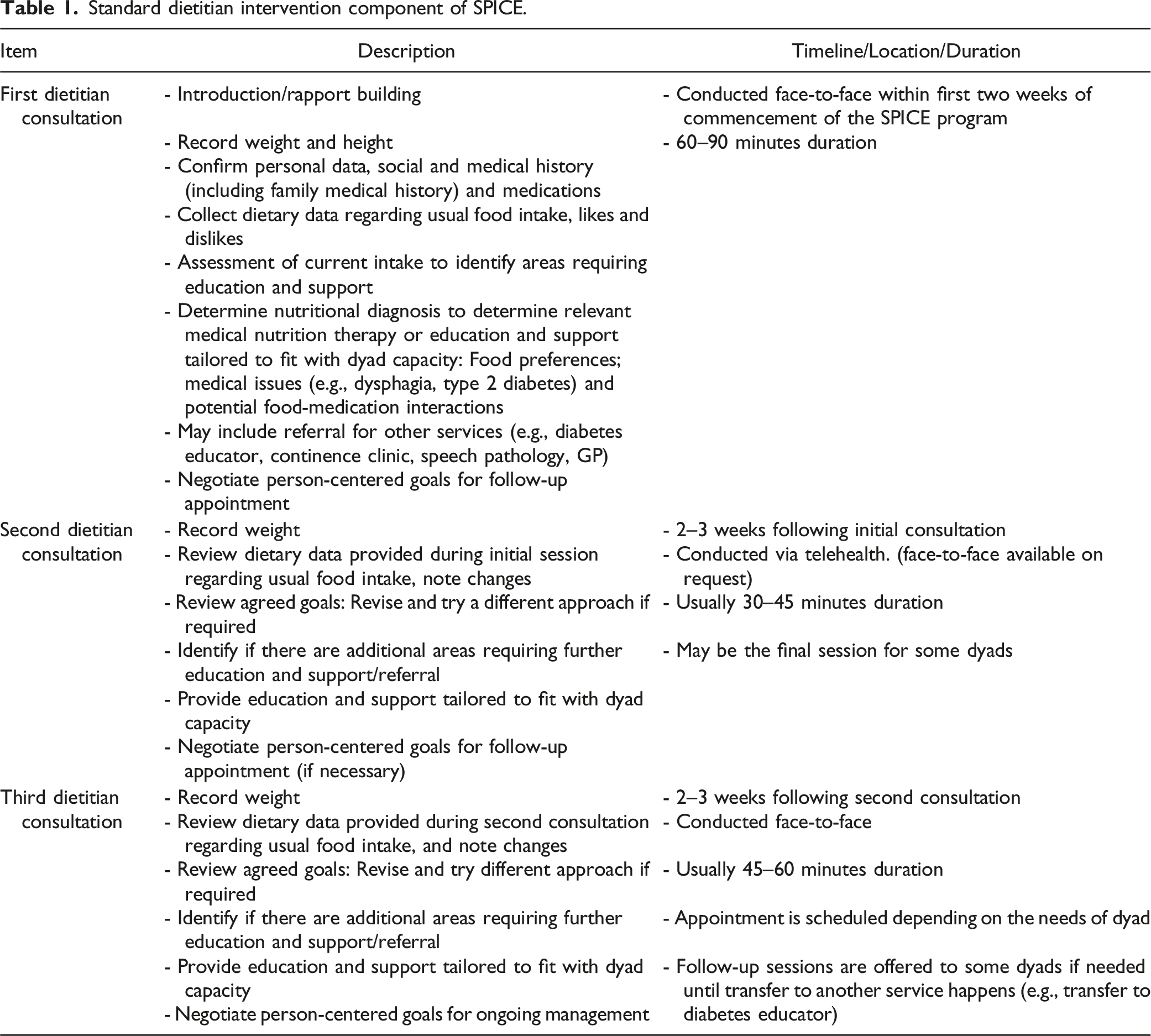
The SPICE program is a twelve-week multicomponent, multidisciplinary post-diagnostic intervention for people with dementia and care partners which has been previously described (D’Cunha et al., 2023). Up to seven people with dementia and their seven care partners participate in each group. To be eligible, people with dementia had to have a dementia diagnosis, a Clinical Dementia Rating (CDR) score of between 0.5 and 2 (Berg, 1984), be an ACT resident, and be English-speaking. The SPICE program aims to delay progression of dementia and improve quality of life through participation in a combination of evidence-based psychosocial and rehabilitation interventions completed in small groups and as a dyad: 1) Cognitive Stimulation Therapy (CST) (Desai et al., 2024); 2) Carer Social, Emotional, and Resilience Education and Capacity Building (Parkinson et al., 2017; Pierse et al., 2022); 3) Physical activity; 4) Care of People with dementia in their Environments (COPE) program (Clemson et al., 2021); and 5) Dietary assessment, education, and advice (Table 1). Standard dietitian intervention component of SPICE.
The overall program design of SPICE equates to a complex intervention with a mix of group and dyadic-based activities across the different dimensions of health. This means participants likely experience a synergistic effect from exposure to the multiple components, and social influences may enhance their adherence and motivation for lifestyle changes (D’Cunha et al., 2025). The SPICE program is primarily funded through the public health system; however, the dietetics component is funded by the University of Canberra. The present study is a sub-sample of all clients to complete the SPICE program through August 2024.
Dietary Assessment and Advice Component
At the start of the SPICE program, participants are offered three appointments with a dietitian. When the program commenced, participants attended a dietetics clinic. As the program evolved, a single Accredited Practicing Dietitian with extensive experience working with older people was assigned to see all participants. The dietitian holds a Master of Nutrition and Dietetics, is a current doctoral student investigating the diet quality of older people living independently in the community, and has lived experience as a care partner.
Appointments with the dietitian are separate from program group components and based on person-centered care principles focused on the nutrition and diet of the person with dementia. Care partners have varying input depending on the cognitive function of the person with dementia. At the beginning of each consultation, people with dementia and care partners are encouraged to identify issues of concern, including discussing strategies for dealing with potential future issues with dietary intake. Appointments commenced with an assessment and review of current dietary intake of the person with dementia. Advice and education are provided, as well as interventions to address specific issues and needs as appropriate. The standard consultation pattern is presented in Table 1. Participants are required to attend at least one dietitian session during the program. Two sessions were offered face-to-face, and one session conducted via telehealth. However, depending on preference, they could elect to have the telehealth appointment face-to-face. A fourth consultation was permitted as needed at the discretion of the dietitian. When necessary, the dietitian reports back to the Canberra Health Services SPICE team to enhance the clinical care of the clients and recommends referrals to adjunct services as necessary.
Data Sources
People with dementia and their care partners who attended appointments with the dietitian (n = 40 dyads) had their data included in the study. Client case notes of the dietetics appointments and letters to clients were analyzed. Participant ratings of the dietetics appointments are drawn from post-SPICE program satisfaction interviews and reported using a five-point Likert scale (1 = Not at all useful; 5 = Very useful).
Data Analysis
Clinical focuses were established for each composite case through analysis of all documented case notes and letters, and discussions within the research team, including with the dietitian, regarding key themes and features of the dietetic consultations undertaken by the participants. Individual client cases with relevant themes were systematically identified and synthesized into four composite cases representing the most common clinical presentations in the sample. To generate themes, the lead author (a dietetics Masters student), who was not involved in the SPICE program, and the dietitian, conducted independent data review and code generation. They then met with two other members of the research team (both dementia researchers with doctoral qualifications) with knowledge of the participants to discuss, cross-check, and develop themes. Cases were discussed during team consensus meetings to form the composite case series.
Although the presented composite cases represent multiple perspectives and disguise the identifiable features, each case is a representation of the events described by the documented case notes and letters. The most illustrative clinical material was extracted from each individual case to best represent and blend the clinical focus of each composite case (Duffy, 2010). Participant characteristics, demographics, and clinical presentations included in each composite case represent the average of the individual cases incorporated. Each composite case was written in adherence of the CAse REport (CARE) Guidelines (Gagnier et al., 2013).
Participant ratings for the dietetics component of the SPICE program are presented as median (interquartile range [IQR] 1st, 3rd).
Results
Participant Characteristics
Characteristics of People With Dementia.
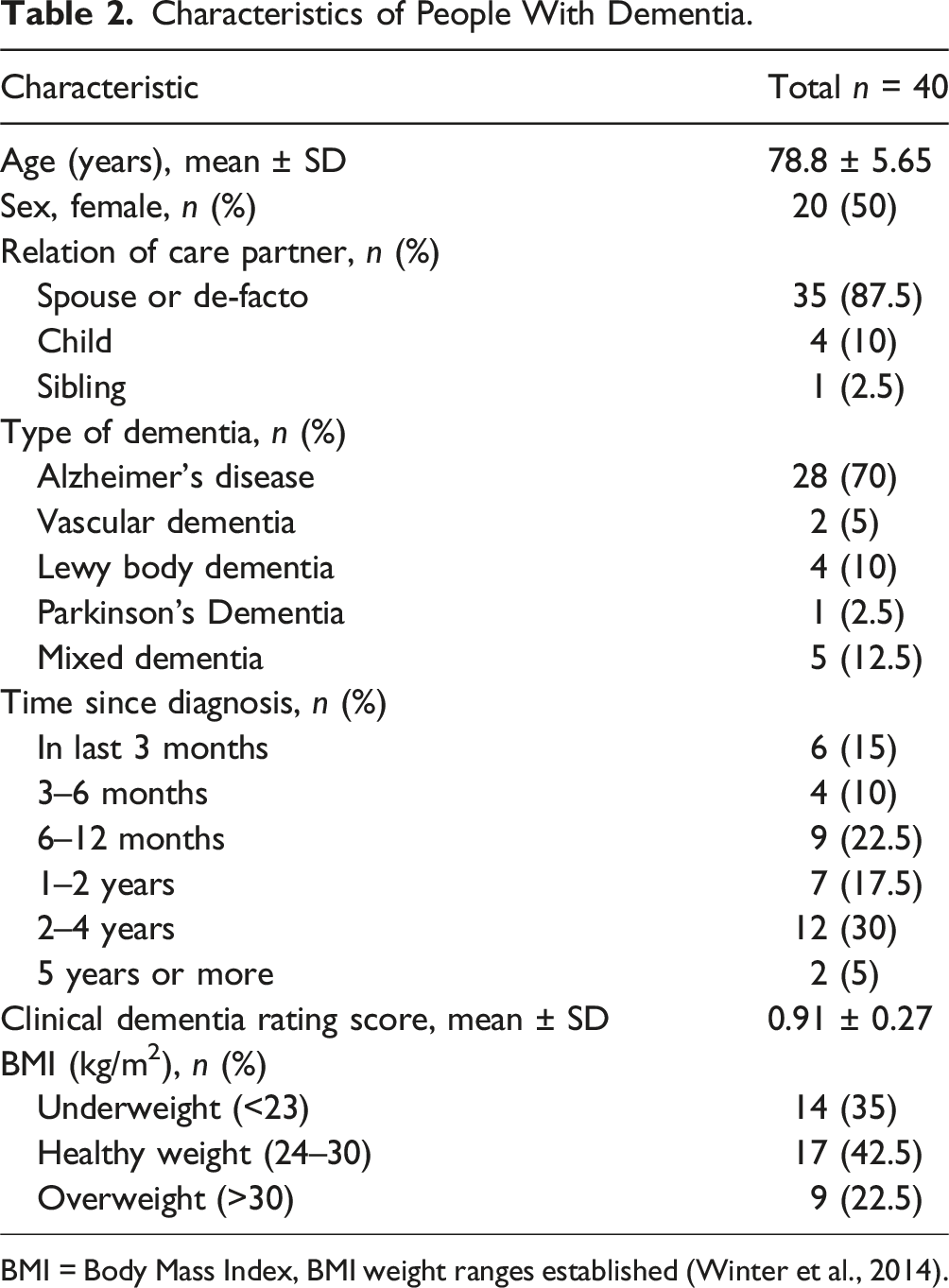
BMI = Body Mass Index, BMI weight ranges established (Winter et al., 2014).
Dietetic Consultations
The self-reported dietary behaviors of participants varied. Some participants were maintaining a reasonably healthy diet, while others required more support and intervention as well as referrals to other health professionals. Common issues identified include insufficient energy and/or nutrient intake, altered food preferences, unintentional weight loss, poor management of comorbidities (e.g., Parkinson’s disease, type 2 diabetes, Gastro-Oesophageal Reflux Disease (GORD)) and difficulties with communication and coordination of care. Male care partners (n = 11) often had limited knowledge of nutritional requirements and/or skills in meal planning, preparation and cooking, and were provided support accordingly.
The focus of appointments was to deliver realistic and achievable evidence-based dietary education and advice. Goals were negotiated through working with the person with dementia and their care partner and reviewed at follow-up appointments. The dietitian employed a range of techniques informed by clinical practice guidelines such as the updated ESPEN on nutrition and hydration in dementia (Volkert et al., 2024), motivational interviewing techniques, Dementia Support Australia resources, and drew upon clinical and lived experience. The most common approach taken by the dietitian included provision of individualized advice on how people with dementia could meet their intake requirements per the Australian Guide to Healthy Eating (AGHE) (NHMRC, 2013). The dietitian provided referrals and reports to other health professionals and services, including a general practitioner (GP), speech pathologist, continence physiotherapist, Canberra Health Services Diabetes Service, and a geriatrician. Dietary goals were targeted to benefit people with dementia with support from the care partner scaffolded across multiple consultations when required. All food and meal suggestions provided by the dietitian considered food preferences, allergies and/or intolerances and cooking skills of the dyad. Comorbidities of people with dementia were also considered in provision of all dietary advice. Another strategy implemented was education aimed at the care partner regarding the importance of nutritional adequacy and appropriate monitoring strategies for malnutrition including monthly weighing, observing changes in fitting of clothes, and noting changes in food intake and preferences. At the final dietary session, weight maintenance, healthy weight gain and increased weight monitoring were observed following education on weight and energy intake in earlier sessions.
Composite Case Series
Five recurrent clinical themes emerged from the qualitative analysis of clinical materials relating to the forty dyads included in this study. They were suboptimal energy and nutrient intake, poor management of nutrition-related comorbidities, limited cooking skills and nutrition knowledge of care partners, unintentional weight loss and challenges with communication and coordination of care. The following four composite cases illustrate some of the common nutrition issues experienced by dyads and key strategies the dietitian employed to provide support.
Composite Case Study 1: Support for Suboptimal Energy Intake
Arthur, an 80-year-old man, was diagnosed with Alzheimer’s disease three years ago. Arthur attended his first dietitian consultation with Dorothy, his 78-year-old wife. Arthur’s self-reported diet included a wide variety of homemade foods prepared by Dorothy. However, following a major fall, which resulted in a brief hospitalization, Dorothy reported Arthur’s cognition had declined further, leading to increased difficulties remembering to eat and tolerating foods. Arthur reports his brain now “stops him” from eating the foods he previously enjoyed. Arthur’s BMI was 20.7, slightly lower than the recommended protective BMI range of 24–30 for older people.
The dietitian estimated Arthur’s current energy intake was suboptimal for weight maintenance, increasing his risk of falls and sarcopenia. The dietitian provided education on Arthur’s energy needs and set a goal to increase energy intake to maintain/slightly increase his weight. Dorothy was recommended to monitor Arthur’s weight periodically for weight loss. Through comparing his dietary intake against the recommendations of the AGHE, the dietitian identified several other areas for improvement. This included increasing his dairy intake, increasing intake of protein-rich food, and drinking more water. Agreed goals were to have a glass of water with each cup of tea during the day, eat more than an apple at lunch, replace one coffee with a hot chocolate made with milk, add cheese to his steamed vegetables with dinner and to have eggs with breakfast three times each week.
Arthur and Dorothy attended the second consultation together via telehealth two weeks later. Dorothy reported Arthur was consuming more fluid throughout the day and adding sources of dairy, including cheese, to breakfast and lunch. She also reported trying to incorporate protein-rich foods, including occasionally having eggs with breakfast and eating a handful of almonds as a snack. The dietitian encouraged them to continue implementing these initial strategies and recommended including more sources of calcium (e.g., calcium-fortified tuna) to ensure Arthur continued to meet his nutrient requirements for optimal bone health. Dorothy was advised to continue monitoring Arthur’s fluid intake and weight.
Three weeks later, Arthur and Dorothy attended the final consultation face-to-face. Dorothy reported implementing each recommendation from the previous consultations, including making a more substantial lunch (e.g., sandwich with tuna, and cheese with an apple), having eggs more regularly at breakfast and keeping better track of Arthur’s fluid intake, and encouraging him to drink more. Arthur’s weight increased by 2.8 kg since the initial consultation. Dorothy enquired about future dietary issues she and Arthur might be confronted with as dementia progresses. The dietitian provided education on common challenges, including further decreases in appetite and increases in food aversions. Education and resources were provided on oral nutrition supplements, including when they are needed, how to use them to fortify foods, what products are available, and where to find them.
Composite Case Study 2: Managing Comorbidities
Peter, a 78-year-old man, diagnosed with Lewy Body Dementia six months ago. Peter attended the first dietitian consultation with Eleanor, his 72-year-old wife. Peter reported experiencing constant tremors in his right hand, and more recently being diagnosed with GORD. Peter reported having difficulties swallowing, resulting in requiring fluids while eating and cutting his food into smaller pieces. Peter also reported experiencing fecal incontinence approximately four times daily. Eleanor reported Peter had lost weight over the last three months. Eleanor shops, prepares and cooks meals for Peter, primarily a traditional English diet.
The dietitian provided initial education on the AGHE including how to meet Peter’s recommended daily food and nutrient requirements. Minor adjustments to Peter’s oral intake were required, including increasing his protein and fluid intake. Peter often disagreed with the advice. Further education was provided on the importance of increasing his energy intake due to his tremors and reassuring that this change from his normal intake would not result in weight gain. Given Peter’s preference for milk and milk-based drinks and associated gastrointestinal symptoms, the dietitian suspected lactose intolerance and provided suggestions on testing tolerance. The dietitian suggested enquiring with Peter’s GP about a referral to a gastroenterologist to explore other causes, and the dietitian also referred to a speech pathologist for a swallowing assessment and provided resources on GORD management.
Two weeks later, Peter and Eleanor attended the second dietitian consultation together face-to-face (on request). Peter reported trialing a lactose-free diet, and Eleanor had been encouraging him to eat more regularly. Peter’s fecal incontinence continued to occur sporadically, but he reported his bowel movements had reduced to two each day since commencing a lactose-free diet. The dietitian recommended to continue a lactose-free diet until the next session. Eleanor reported they were still trying to increase Peter’s fluid intake as well as experiencing difficulty reaching his recommended energy requirements. The dietitian provided recipes and strategies to improve energy intake and recommended Eleanor monitor Peter’s weight.
Peter and Eleanor attended the final consultation three weeks later, face-to-face. They reported continuing to try recommendations from previous sessions and were happy with how things were progressing. Peter reported waking most nights needing to go to the bathroom. The dietitian recommended Peter try having his heavier meal at lunch and a lighter meal at dinner. Eleanor was concerned about her own cholesterol levels following a recent blood test and resources were provided to support her.
Composite Case Study 3: Upskilling Male Care Partners
John, a 79-year-old man, is the sole carer for his wife Carmel, a 78-year-old woman who was diagnosed with Alzheimer’s disease three years ago. John reported having limited nutrition knowledge, with Carmel previously taking sole responsibility for all shopping and cooking in their household. Carmel’s short-term memory had recently deteriorated further, making activities of daily living more challenging. John is now taking sole responsibility for shopping and cooking. He reported feeling “unsure” of how to take on the role of the “cook.” He viewed cooking as a chore and found it challenging to encourage Carmel to eat. Carmel was eating two meals daily, struggling with early satiety since the dementia diagnosis, and reported frequent constipation. John reported frequently taking Carmel to eat at their local shopping center food court, with minimal cooking being done at home. The dietitian provided initial education on the AGHE including how to meet their recommended daily food and nutrient requirements. Further education was given on increasing Carmel’s energy intake and regularity of eating, increasing her fluid intake and how to plan and prepare meals. Initial goals set were to try to eat according to serve recommendations and increasing Carmel’s daily energy intake so she can maintain her current weight to prevent risk of falls, trial “Lite and Easy” Senior Meals ready-made meal service, and to monitor Carmel’s weight and fluid intake.
The second consultation was conducted via telehealth two weeks later. John and Carmel noted they were both enjoying the recommended ready-made meals suggested at the last consultation and trialing having a supper. Carmel’s weight remained stable. The dietitian estimated Carmel was still not eating enough throughout the day to meet her daily energy requirements; however, her intake improved slightly since the last consultation. The dietitian provided a range of higher-protein, higher-energy snack options for John and Carmel to try, including cheese and biscuits, milk with Milo or swapping plain Greek yoghurt for a protein-enriched variety (e.g., “YoPro”). Carmel was encouraged to continuing trying to drink more water.
The final consultation was conducted two weeks later, face-to-face. Carmel’s bowel movements and subsequent comfort had improved. John reported feeling more confident in the kitchen and aware of how to “eat better.” He also reported an increased interest in nutrition and brain health, having recently borrowed two books from the local library discussing micronutrients and cognition. He continues to refer to the AGHE to keep on track. The dietitian provided another resource on snacking as well as further recipes that suited both taste preferences.
Composite Case Study 4: The Adult-Child Care Partner Dynamic
Clare, an 80-year-old woman, was diagnosed with mixed dementia six months ago. Clare lives alone in the community but is cared for by Alice, her 60-year-old daughter. Clare has early-stage Alzheimer’s disease and is very independent. She reported being reluctant to ask for help despite a loss of self-confidence. Clare struggled to recall her dietary intake, and frequently commented on being “overweight” and needing to eat less. Alice was unsure if the dietary intake Clare was reporting was accurate. Clare reported difficulty sleeping and ongoing constipation. The dietitian provided initial education on the nutritional challenges associated with aging including early satiety. Further education was provided on the importance of nutrition, weight maintenance, planning meals and the AGHE recommendations. The dietitian estimated Clare was unlikely meeting the recommendations. Initial goals were to increase sources of dairy, grains, protein and fluids, to maintain or slightly increase Clare’s weight. Meal timing suggestions, recipes and pre-prepared meal options were provided to help Clare, especially when she did not want to cook. Alice was also encouraged to periodically monitor Clare’s weight.
Clare and Alice attended the second consultation together via telehealth two weeks later. Clare reported trying to drink more water throughout the day. She also trialed eating freezer-stored “Lite and Easy” Senior Meals when she did not want to cook as recommended. Clare reported occasionally skipping breakfast so she does not put on any more weight. Her overall dietary intake since the previous appointment was difficult to gauge as Clare had difficulty recalling exact details. A food diary was not recommended, as Clare couldn’t reliably complete it. She reported having regular headaches. The dietitian estimated she was still not meeting her energy requirements for weight maintenance. Further education was provided on the importance of weight maintenance for reducing risk of falls and sarcopenia. Alice agreed to date Clare’s frozen meals to track consumption. Clare had the opinion grains are “bad for you”; therefore, education on the important role of grains and fiber in the diet was provided. Alice displayed similar restrictive views on eating to Clare, reporting feeling conflicted regarding advice on introducing higher-energy snacks to Clare’s diet, as they are “sugary.”
The third and final consultation was conducted three weeks later, face-to-face. Overall, there were minimal reported changes to Clare’s diet. Clare reported continuing to focus on increasing her fluid intake. She also started drinking her coffee with milk to increase her dairy intake. The dietitian provided more strategies and recipes for making a clearer food routine to meet her requirements within her lifestyle. Clare continued to express concerns related to her body image. Together, a goal was made for Alice and her husband to come over and eat with Clare once per month. Ongoing weight monitoring was also recommended. Alice reported challenges balancing work demands with her role as care partner as well as experiencing new nutrition challenges of her own related to onset of menopause. The dietitian provided support and a take-home resource on nutrition for menopause.
Ratings of Dietetics Component
People with dementia found the dietetics component to be “Quite useful” with a median value of 4 out of 5 (IQR 4–5). Care partners found the appointments to be “Very useful” with a median value of 5 (IQR 4–5).
Discussion
This composite case series highlights the positive impact a dietitian can have on the health and quality of life outcomes of people with dementia and their care partners. The study design allowed multiple perspectives to be included to best represent central findings which included common nutrition issues experienced by people with dementia and their care partners such as insufficient energy and/or nutrient intake, altered food preferences, unintentional weight loss, poor management of comorbidities and difficulties with communication and coordination of care. The common approaches employed by the dietitian to support each dyad included education on the AGHE, malnutrition risk and monitoring strategies, and referrals and reports to other health professionals and services.
A key clinical concern among participants was insufficient energy intake, resulting in unintentional weight loss. Jansen et al. (2015) identified early satiety and unintentional weight loss as a nutrition-related challenge can be faced at all stages of dementia, starting from initial deterioration of memory. Weight maintenance, healthy weight gain and increased weight monitoring were often seen following education on weight and energy intake in earlier sessions, suggesting the positive impact of early intervention from a dietitian. These findings are supported by Rivière et al. (2001) who found a 12-week dementia care intervention involving a dietitian resulted in mean weight of the intervention group increasing compared the control group. Keller et al. (2003) supported these findings in a nine-month nutrition intervention resulting in a higher proportion of weight maintenance and healthy weight gain in residents of a dementia special care unit.
Family care partners require support on how to monitor for malnutrition and prevent nutritional decline (Mole et al., 2018). The composite case series provides further evidence that ongoing support from a dietitian may be an effective strategy for healthy weight maintenance and increased care partner awareness of appropriate monitoring strategies to decrease malnutrition risk for people with dementia. Resistance to weight gain was an apparent barrier faced in the consultations, suggesting ongoing, long-term dietetic support is needed for adequate counseling on weight management.
Changes in food preferences resulting in decreased oral intake was another key clinical concern identified. Kouzuki et al. (2020) found people with Alzheimer’s disease exhibited signs of gustatory impairment, which subsequently decreased their interest in meals. Care partners of people with dementia have also reported gustatory decline is a barrier to providing a healthy diet (Lahiouel et al., 2023). Early intervention may improve dietary interest and quality of life (Kouzuki et al., 2020), particularly as people with dementia often lose interest in foods they previously enjoyed. Improvements in nutritional adequacy and healthy weight gain were seen following dietetic intervention, further supporting the importance of early intervention and ongoing support from a dietitian.
An individualized approach to nutrition care, as well as interprofessional collaboration, was required due to the complexity of presenting comorbidities. Across the composite case series, the dietitian referred the dyads to a range of health professionals including a speech pathologist and an incontinence physiotherapist. The dietitian also advised the dyad on when contacting their GP or geriatrician may be beneficial to further investigate health concerns. Benefits of effective interprofessional collaboration for people with dementia include more holistic support, improved disease management, and continuity of care (Egan et al., 2023). To achieve these outcomes, specialized standardized training should be provided to healthcare professionals, including dietitians, to deliver quality, individualized, collaborative care to people with dementia living in the community (Egan et al., 2023).
The findings highlight the unique experiences and challenges faced by care partners of people with dementia in the community. Male care partners often lacked nutrition knowledge and cooking skills, feeling unprepared for domestic roles previously managed by their spouses (Milligan & Morbey, 2016). Male care partners are proposed to both provide support to others and seek support for themselves differently to females (Poisson et al., 2023). In most cases, engaging with a dietitian improved confidence and nutrition-related symptom management. Children caring for parents with dementia living independently faced challenges in care coordination and communication (Evans et al., 2016; Rigby et al., 2019), leading to difficulties in assessing nutritional intake. In both scenarios, tailored strategies and support resulted in positive dietary changes. These findings underscore the importance of specialized, person-centered nutrition interventions to adequately inform and support various care partner dynamics for people with dementia.
Care partner engagement has been associated with increased success in outcomes, with dyadic reablement interventions being suggested as beneficial for both people with dementia and care partners (Clemson et al., 2021). For people with dementia and their care partners living in the community, interventions targeting the needs of the dyad will increase the likelihood of successful outcomes (Parkinson et al., 2017; Van’t Leven et al., 2013). Several care partners in the present study sought advice regarding their nutritional needs including nutritional management of a range of conditions including hypercholesterolemia, menopause, and hemochromatosis, and planning and preparing meals ahead of time. Support received from the dietitian could increase ability to manage their role as a care partner long-term, subsequently improving health and quality of life outcomes for the person with dementia they support.
Dementia is commonly feared due to the associated loss of self-sufficiency and increased reliance on the support of others (Dominguez et al., 2021). This loss of independence, self-sufficiency, and autonomy contributed to some people with dementia disagreeing with advice. These emotions were associated with experiences with fecal incontinence, which resulted in increased need for support to assist with the loss of control of bodily functions and often a reluctance to ask for help. Advice on optimal nutrition from a dietitian has the potential to promote independence, dignity, and quality of life through reducing symptoms and risk of falls (Suominen et al., 2015). The care partner’s fear of future issues that would arise as the dementia progresses was also addressed. Providing education on potential future nutrition challenges and appropriate strategies has been demonstrated to be important to care partners (Lahiouel et al., 2023) and was a focus during the consultations with the aim of reducing any overwhelming uncertainties. The positive impact of seeing a dietitian in the SPICE program is supported by the findings of Mole et al. (2018) who found family care partners feel unsupported and uninformed of nutrition risk and care and would like more input from professionals.
Limitations
While the chosen study design provides insight into lived experiences of participants, generalizations cannot be made as these observations are not representative of the larger population. Notably, older people in the ACT generally enjoy higher socioeconomic status compared to other states and territories in Australia (Australian Bureau of Statistics, 2023), and all but four participants in the sample were Caucasian. Composite case series have methodological limitations similar to other qualitative research methods, including selection bias, potential researcher bias, and risk of over-simplification (Crowe et al., 2011). The dietitian consultations were also not run in isolation but as part of a multicomponent program. This context should be considered in the interpretation of the composite case studies presented due to the likely synergistic effect from exposure to the multiple components and social influences may enhance the perceived effectiveness of the dietetic intervention. Moreover, only a single dietitian was used. However, in Australia, there are limited dietitians with dementia-specific training (Bartrim et al., 2024), which impacts the scalability of programs such as the SPICE program. As all people with dementia and care partners experience the dementia pathway in different ways, the cases only represent a small proportion of possible outcomes of dietetic consultations. Additionally, this is a preliminary analysis of the first ten groups to complete the SPICE program and not representative of the entire sample that will complete the study. As longer-term outcomes of the entire program will be presented separately, the current study represents an interim report of the dietetics component only.
Future Directions
Research is needed to inform optimal dietetic care models for managing nutritional concerns of dementia (van Buuren et al., 2023), particularly for groups with lower socioeconomic status and those from diverse cultural backgrounds. Further work is also necessary to inform how multicomponent, multidisciplinary interventions can be funded sustainably given multiple priorities in health services in Australia and internationally and funding limitations. The SPICE program has been funded primarily through public health funding and in-kind resourcing in response to increased recognition of the need for rehabilitation for people with dementia and the healthcare needs of care partners. This was possible as it was developed and implemented in collaboration with a university, and the dietetics component is funded by the university independently of research grant funding. Partnerships between health services and universities are vital, leading to improved client health outcomes, lower mortality rates, and greater adherence to clinical guidelines (Nott et al., 2024). Collaborations enable health services to harness research expertise while allowing universities to access clinical settings and populations, creating mutual benefits that enhance the development and evaluation of health interventions through shared resources, knowledge, and infrastructure. The SPICE program collaboration has been a successful example with funding available through to 2028.
Conclusion
This study highlights the positive impact a dietitian can have on the nutrition, health and quality of life outcomes for a person with dementia and their care partner. These include decreasing the risk of malnutrition through weight maintenance and monitoring, increasing care partner skills and confidence and supporting dyads to manage complex nutrition-related comorbidities. The highlighted prevalence of nutrition-related complications of dementia supports the dietitian as an essential component of a multidisciplinary team. The involvement of a dietitian in both early-stage and longer-term interventions could be beneficial to health outcomes for dyads living in the community. Further dietetic intervention trials are needed to better inform an optimal dietetic care model in a real-world context. Future research is still needed to evaluate dietetic interventions and training models in detail, considering both the feasibility and sustainability of proposed models of care in a community setting.
Footnotes
Acknowledgments
The authors want to acknowledge and thank the participants, the Canberra Health Services SPICE team, and the SPICE External Advisory Group and Steering Group.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Canberra Health Services, the Dementia Australia Research Foundation - Hazel Hawke Alzheimer’s Research Award, and the University of Canberra Faculty of Health.
Ethical Statement
Data Availability Statement
The data is not publicly available due to privacy and ethical considerations.