
Abstract
The importance of giving a voice to groups considered hard-to-reach for research purposes is becoming increasingly apparent, with insights into their experience having the potential to improve research participation. Fall-prone older adults are a cohort underrepresented in research, often excluded in large-scale research and considered difficult to recruit. This study aims to explore older fallers’ experiences of being fall-prone and participating in research. Seven older fallers (4 males, aged 69–88) participated in semi-structured telephone interviews following participation in an experimental research project. Interviews explored participants’ personal experience of being fall-prone and participating in research. The resulting data was analyzed using thematic analysis. Three primary themes emerged: “Research through the eyes of older fallers”, “Living with falls”, and “It’s all in the mind is it?”. Our study gives voice to older fallers who have recently participated in experimental research to learn of their personal views on research participation.
• The current study identifies motivating factors and obstacles to fall-prone older adults’ participation in research via direct consultation with fallers. • We gain an insight into how some fallers may conceptualize their falls as unpreventable, a factor which may explain poor uptake for falls prevention initiatives.
• Future research aiming to recruit fall-prone older adults should include opportunities for social interaction with the research team to maximize uptake and benefit for fallers. • Future efforts to engage older fallers in community falls initiatives or research would benefit from co-design of projects to maximize engagement and retention of participants.What this paper adds
Applications of study findings
Introduction
Falls represents a major public health challenge, with our global population progressively aging and falls in older adults being one of the leading causes of hospitalization and mortality. A fall can have debilitating effects for an older individual with physical injury and the associated psychological distress affecting quality of life (Moore & Ellis, 2008).
The causes of falls amongst older adults remain something of an enigma. Primary factors are considered to be physical frailty, environmental hazards, sensory decline, and psychological factors, primarily fear of falls (Voermans et al., 2007). However, it is estimated 1 in 5 falls remain unexplained (Bhangu et al., 2016). Furthermore, existing falls prevention and intervention strategies enjoy limited success, despite falls costing the Irish health service (HSE) over €160 million every year (Nolan et al., 2016). Extensive research has focused on the causes of falls, yet much of this work is quantitative in nature, with little existing research on fallers’ own insights into falls.
Giving voice to older fallers’ experience of research participation serves several purposes. Firstly, fallers are considered a hard-to-reach population for research participation with recruitment amongst this population difficult (Mody et al., 2008). A qualitative investigation into fallers’ perception of research participation would provide insights into barriers and facilitators to participation. Furthermore, randomized control trials (RCTs) tend to exclude frail older individuals as confounds to a clean sample (Bourgeois et al., 2016). Including this often excluded patient group is important to begin to engage this population in the research process. There is a growing realization amongst the research world that giving voice to hard-to-reach participant groups could provide insights into how to increase research participation (Baczynska et al., 2017). Of the fallers that do participate in research, what motivates them to do so and how do they experience the process of participating in research?
Berge and Colleagues (2020) explored frail older peoples’ views on research participation. Participants identified feeling they are contributing to society and the social interaction with the research team as motivations for participating. Challenging aspects of research involvement identified by the frail individuals included doubting their ability to meaningfully contribute to research and feeling like an outsider in research activities (Berge et al., 2020). The overall theme of challenging oneself on the threshold to the world of research captures frail older adults’ cautious interest in contributing to research despite doubts and challenges associated with participating due to their frailty.
Given the similarities and sometimes overlap between frailty status and being fall-prone, we expect some parallels in older fallers’ experiences of research. Both frail individuals and fallers are often excluded from clinical trials, are considered hard-to-reach populations, and consequently, warrant research exploring their insights and experiences of research. The aim of this study is to explore older fallers’ experiences of participating in research.
Methods
Participants
Participant Characteristics.
Note. SD = standard deviation, n = number.
Procedure
Purposive sampling was used. Older adults who had recently engaged in an experimental research study were contacted via telephone and invited to participate in this study about their experience of the research (the experimental research focused on exploring outcomes following a Physiotherapy-run Falls Prevention Programme [see Online Appendix A]). Nine participants were contacted and invited to interview, with seven consenting to participation and two declining due to hospitalization/ill-health.
Data Collection
Telephone interviews were conducted in September 2020 during the global COVID-19 pandemic, when a national lockdown was in effect in Ireland (i.e., movement restricted to 2 km from home, closure of all non-essential businesses, and no visitors allowed to people’s homes). Telephone interviews were the chosen method of data collection given the inability to collect data in person during the pandemic. Telephone contact was chosen over video calls for ease of access. Both interviewers (JOB and MD) were previously known to participants from the experimental research project 6–12 months prior.
Thematic analysis was used to analyze the data, providing a means to gain insights into our research question (Braun & Clarke, 2021) by identifying patterns of lived experience of research and falls. Two researchers (JOB and MD) coded the data simultaneously and reached a consensus on the definition and naming of themes. The interview was semi-structured, with participants given the opportunity to respond to each of the questions on the interview schedule (see Online Appendix B) as well as allowing the researchers to explore other avenues of interest to the research questions.
The interviews lasted between 10 and 30 minutes approximately. The length of the interview was based on how much participants wished to share their experiences as a faller and a research participant. Field notes were taken by interviewers during and immediately after the interview. Following the principle of diminishing returns (Creswell & Creswell, 2003), data saturation was considered when no novel themes were found in subsequent interview data. This point was reached following seven interviews. All interviews were audio-recorded and transcribed verbatim using Microsoft Word. No repeat interviews were necessary, and participants were not contacted further following interviews.
Data Analysis
NVIVO Pro 12 software was used to code transcripts. The steps of analysis progressed in accordance with Braun and Clarke’s (2006) guidelines for thematic analysis. Firstly, two researchers involved in the coding of the data, read and re-read the transcripts along with listening to the interview recordings. Initial coding was data-driven and completed on a line-by-line basis. Focused coding was then conducted, with initial codes revisited and refined following coding of all transcripts. Next, codes were grouped into categories based on their similarities in terms of addressing the research questions. Categories were refined into themes and sub-themes, with a theme being a pattern of responses saying something meaningful about the research questions (Coding Tree in Online Appendix C).
Researcher Reflexivity
Both interviewers took time to reflect on their position as researchers in this study and were aware of their outsider role, considering age and physical health. Both interviewers are young female healthcare professionals while our participants are aged 69+ and classified as frail individuals. Both interviewers were also consciously aware of the possible power dynamics at play, given participants’ unfamiliarity with research activities and the fact the research was conducted under the auspices of the hospital which participants attend as outpatients. This research formed part of JOB’s PhD Research. MD is a Physiotherapist in the Research Department of the Hospital where participants receive outpatient care.
Ethics
This study was approved by the ethics boards in both the research institution and Hospital involved in the project. All participants had previously engaged with the interviewers during their involvement in an experimental study of 6 weeks duration, for which written informed consent was provided. For the present study, verbal informed consent was established with participants at the start of the telephone interview (as approved by ethics committees). Participants’ verbal consent was audio-recorded and subsequently confirmed by a second member of the research team. Participants were advised of their right to withdraw from the phone interview at any time without repercussion. Participants were all outpatients of a public hospital, and it was made clear to each participant that their participation or non-participation in the research would not affect their access to healthcare at the hospital in any way. At the time of interview, all but one participant was living independently in the community and were deemed capable of giving consent. One individual was residing in a residential home and was also deemed to have the capacity to self-consent to participation. Researchers who conducted the interviews were both skilled in conducting research with older adults, including previous experience of qualitative data collection. All participants were assigned participant numbers for write-up to preserve confidentiality.
Results
Three interconnected narratives emerged from the interviews whereby participants spoke about their experience of life as a faller, of participating in falls-based research and how they individually make sense of their falls. These narratives are captured in our three primary themes: Research through the eyes of frail older fallers, Living with falls, and “It’s all in the mind, is it?”. Figure 1 depicts the themes and sub-themes captured in the interview data. Themes and sub-themes.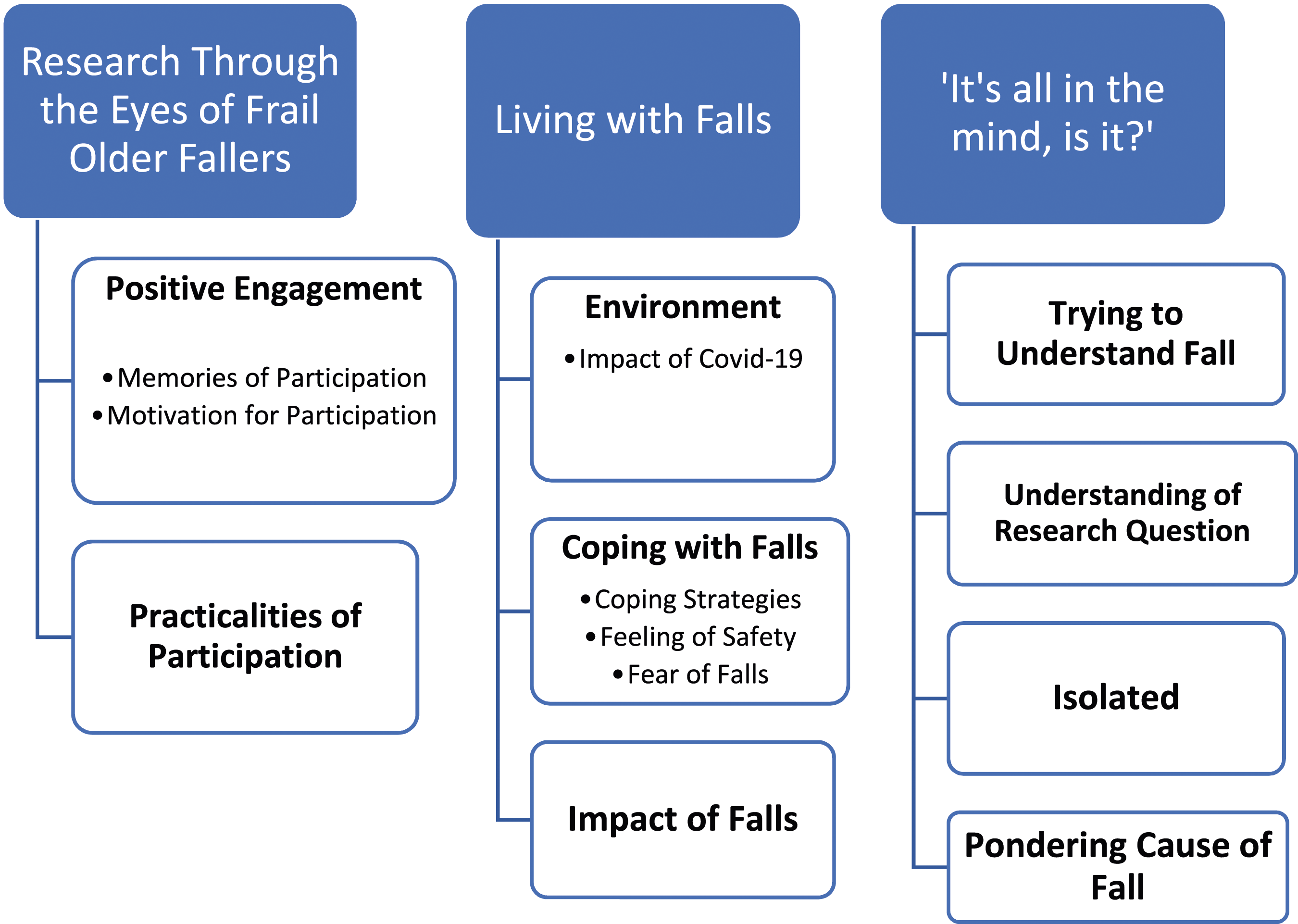
Research Through the Eyes of Frail Older Fallers
Fall-prone older adults are faced with unique challenges with respect to research participation. Mobility difficulties and falls risk can restrict their movements and their opportunities for partaking in a range of activities, including research. When speaking about their experience of being a participant, older fallers mentioned two core aspects: their positive experiences and their thoughts on the practical aspects of participation.
Positive Engagement
The subtheme of positive engagement comprises two categories related to participants’ experiences: their memories of, and motivation for, participation in the experimental research study.
Memories of Participation
During interview discussions, the majority of participants made reference to their limited memory of the specific events in the research sessions. It should be noted there was a considerable gap between research sessions and the post-research interviews, with between 6 and 16 months elapsed in between. It is understandable incomplete memory of the research sessions was mentioned during interviews, as participants reflected on their experience of the sessions. The following quote captures participants’ incomplete recall of the sessions; “I didn’t think I did so well with them flashes [experimental stimuli], I don’t know. I don’t remember how I did or the specific details really” [P4].
However, all participants commented on the fact that what they do remember is that they enjoyed the research sessions. Every participant referred to the social element of research participation, with most noting that social engagement with the research team was a positive experience and memorable. Participants made reference to the research team being “lovely people” [P2] and many stated their enjoyment of conversations with the team, “we had a bit of a laugh there” [P1]. A statement from one participant captures this enjoyment of the social element of being a participant: Ah it was ahm a trip out I guess. It was no trouble and I- as I said earlier it was nice to get out of the house and talk to you girls y’know. It was good for me [P4].
This is linked with the next theme, as the opportunity for social interaction during research participation was highlighted by participants as an aspect of the experience they valued. When reflecting back on their role as a participant, many fallers saw the social exchange during the research sessions as personally beneficial.
Motivation for Participation
Participants’ motivation stemmed from self-interest (personal enjoyment and seeking answers to questions), collective group interest (feeling of representing “fallers”), and/or for the common good. In terms of their motivation for volunteering, some fallers mentioned the feeling that they were contributing something important that would help somebody else. One faller mentioned she felt that by participating in this research, she was giving back to society, referring to a previous fall incident where passersby assisted her and healthcare professionals supported her recovery: I suppose if I thought it would help other people or something, I don’t really know. I think it’s because I felt like I was doing something to make payback for all the help and attention I got when I broke my hip [P5].
Participants had a sense that they were helping others out by attending the research sessions, which contributed to their enjoyment; “…the people who did it were lovely people. I felt I was helping people. It was nice, I enjoyed it” [P5].
Others noted their experience of being a faller as a source of motivation for them to contribute to research exploring falls: The fact, I was having the occasional fall like you know maybe spurred me to do it like you know [P2].
There was a sense that as they were fallers themselves, contributing to this research project was on behalf of their group. Few participants made reference to the fact they were interested in the end result of research, hoping it would answer some of their questions around falls. One male participant hoped participating would eventually lead to a personal benefit for him in terms of dealing with a fall, stating “I just want to know how to get up if I fall, that’s all” [P1].
Practicalities of Participation
As participants reflected on their experiences, they were prompted for feedback for improving future older fallers’ experiences of contributing to this experimental project. Feedback centered around the practicalities of research participation, with some participants suggesting their desire and need for more instrumental support to facilitate their participation (e.g., improving the transport to and from the experimental sessions). The awkwardness and general dislike of the conductive gel used during electroencephalogram (EEG) testing (participants wore an EEG cap during testing which involved the use of conductive gel) was mentioned by several participants as something to be improved or changed for future research of this nature. Many participants suggested that having a hairdresser would be an improvement, while others speculated at alternatives to the gel: Oh that’s horrible, it’s hard to get it out. Had to wash my hair to get it out. If you could find some way of am doing it without putting that kind of gel on it, something else, oil or something that would come out easy [P4].
When it came to receiving feedback or results from the research, participants presented different views on this, with some expressing a keen interest in being provided with a summary of the study results and other participants stating they had no interest in being contacted or sent such information.
Living With Falls
Living with falls is composed of narrative threads which emerged around participants’ status as fall-prone individuals and how they live their lives as fallers. The role of environments, coping with falls, and impact of falls were all topics discussed by participants in relation to their physical status as a faller.
Environment
During the interviews, many participants provided descriptions of recent falls they experienced, in particular focusing on the environments where they fell or felt likely to experience a fall. There was a general consensus amongst participants that being outdoors, navigating footpaths and steps, and moving location were scenarios identified as uncomfortable or “tricky” for them as fall-prone individuals. Each participants’ fall experience was spoken about extensively during interviews, highlighting how memorable a fall event is for them. For older fallers, feeling safe was dependent on a person’s environment, with familiar environments bestowing a sense of safety. “Anywhere not that familiar” or most outdoor spaces were avoided by participants due to the perceived risk of falling.
Interestingly, participants picked out specific aspects of an environment that they considered “safe” or “comforting”, and this was quite individual to each person. For example, one participant in residential care found that having a bell to press was comforting for her, while another participant spoke about his own garden when asked about a place he feels comfortable in or safe (i.e., low falls-risk). Yet another participant pinpointed their own bed as the space they feel most safe in respect to risk of falling.
Coping With Falls
Throughout the interviews, participants gave accounts of their lived experience of coping with being a fall-prone individual, at times providing tips as to how they manage and other times, explaining how falls have shaped aspects of their lives. Taking the collective experiences of our participants, two ways of coping emerge in their discourse: one being the use of physical supports and the other being mental strategies or approaches participants have adopted in their day-today lives to manage their falls risk.
In terms of physical coping strategies, a number of different aspects were highlighted as important for supporting independence. For some, this comprised the use of a walking stick or walker or pieces of technology (e.g., help bell on wrist) or access to healthcare (i.e., medical card). For others, people-based support was highlighted, including the support of a caring family, spouse, or nursing staff. People were seen as providing both emotional support and physical support with managing their falls. Fallers highlighted the necessity of these forms of support to allow them to live a meaningful and safe life despite their falls-risk. Oh I’d be lost without it [walking stick]….I can’t go very far at all without it [P2]. Yeah, I’m fine with her [cousin who is retired nurse]. I don’t stumble or anything with her [P5].
The second strategy mentioned by participants was centered around a mindset or approach used to either minimize the risk of falls (avoidance strategies) or preserve their quality of life (involvement/active strategies). Such strategies were identified by participants as ways to help them feel more in control of their falls and their lives. Almost all participants described the need for them to “be careful”, reflecting a cautiousness and vigilance around their falls-risk. One participant described it as “I have to watch myself” [P6]. Perhaps stemming from this cautiousness, some participants spoke of avoiding outings or occasions due to the perceived risk of falling: Like I don’t go anywhere really y’know, I- I try and avoid going someplace now, because I don’t go to funerals or weddings or ANYthing, y’know (P4).
While participants were not asked directly about their means of managing their falls, each participant spoke of ways they cope with being fall-prone during their discussions about living with falls. Participants’ coping mechanisms for living with falls varied but generally fell within the categories of having a positive mindset, keeping active and exercising caution in day-to-day life. Participants spoke about how “you have to keep going like” [P1], and many fallers spoke about keeping active and moving as much as they could, representing an active approach, that is, facing a falls-risk situation as opposed to avoiding exercise/movement; “I don’t vegetate” [P6].
An interesting aspect around coping with falls emerged, whereby a number of participants spoke about the need to get on with their lives and not dwell on their falls. This appeared to represent an internal coping strategy. Many participants gave a sense of accepting their fall-prone status and that falls will happen. For many, future falls were seen as a foregone conclusion. One participant spoke of her belief that the government or healthcare providers could do little to help. What can they do for goodness sake?....I mean it’s just one of these things isn’t it [P2].
The phrase “it’s just one of these things” was stated by another participant and many others echoed this sentiment throughout the interview discussions. The sense that falls are an inevitable part of life for these individuals was a narrative that emerged in the interviews and it appeared for some, adopting an acceptance of falls represents a means of coping with falls. If you fall, you fall like, that’s sort of it really, nothing can be done, I don’t think [P6].
Impact of Falls
The knock-on effects of having a fall was something brought up by almost all participants. Many spoke of specific physical injuries as a result of a fall, such as “cracked three ribs”, “cuts on my hand”, and “banged my head.” One female participant’s advice for other fallers focused on sharing her strategy of being prepared for the potential physical health consequence of a fall (i.e., the need for urgent medical attention); “and always have a bag packed for the hospital, just in case” [P5].
Beyond the immediate impact of a fall, it was evident throughout the interviews that falls also have other consequences, namely, the pervasive impact on their day-to-day lives. While not framed as an impact by many participants, but mentioned as their ways of coping with being fall-prone, many of their coping strategies appear to impact their lives, particularly avoidance-based approaches used to cope with falls. For example, many participants spoke about avoiding outings or declining event invitations.
“It’s all in the mind is it?”
Fallers spoke of their own take on their falls, that is, their conceptualization of what being a faller means and what sets them apart as a fall-prone individual. A sense of lack of control emerged when participants were asked to reflect on the cause of falling. The essence of this theme is captured in a quote from one participant, with their statement of a rhetorical question during their interview; “it’s all in the mind is it?” [P4]. This line embodies the two elements of fallers’ response to what causes their falls; firstly, that the answer is elusive and the question is as such unanswered and secondly, fallers’ belief that psychological processes have a part to play. When describing accounts of their falls, each participant noted obstacles in the environment as possible external sources of their falls. Not having a walking stick, uneven surfaces, and slippery flooring were common culprits identified by participants as things in their environment that may account for falls. Yet, when asked directly to consider why they think falls happen to them, participants provided more psychological explanations for being fall-prone. The “mind,” “brain,” and “it’s all nerves” were identified by participants as possible root causes for their falls. This speaks to a potential conflict in the mind of the faller, where we get a sense they feel out of control physically, and when faced with no apparent reason for a fall, they identify aspects of their environment that could be at fault, possibly to normalize a fall. Yet, the conflict lies in the fact that fallers believe little can be done to prevent falls, and most frame their “habit” of falling as being an issue of the mind.
Many of the fallers in this study spoke to this psychological aspect of falls, showing they considered the mind had a role to play in causing and preventing falls. One participant framed this as a self-fulfilling prophecy: If you think you’re going to fall, you’re going to fall [P1].
This sentiment was echoed by other participants who spoke of the role of fear and anxiety in contributing to a fall. One participant (P4) captured this link when she voiced “I find if I get nervous, I fall.” This ties in with the psychological ramifications of being a faller captured under the theme of Living with Falls, where cautiousness emerged as a coping strategy. One female participant noted that nerves contribute to her falls-risk, describing it as “a feeling” to be managed. I was in town with friends and if I get nervous about falling… As sure as anything, I eh start slipping and and I’m eh taking baby steps then trying to overcome the feeling [P4].
Most Participants Eluded to the Evasive Nature of What Causes Falls. There must be something somewhere, yeah, but I can't put a finger on it [P3].
Falls are a multifaceted phenomenon with many potential causes and this fact was echoed throughout the interviews, with participants speaking of their exasperation at fruitless efforts to identify causes for their accidents, “I can’t find a reason,” “I really don’t understand why it would happen,” and most (five) participants referred to the sudden nature of a fall as something “that just comes over me.” Fallers’ search for reasoning may reflect a wish for control over their situation and their status as fall-prone. It just happened before I knew it like I… was falling before I knew it [P7].
There was a sense from participants that being a faller isolated one from others, participants in their language isolated themselves from friends and families when they described being fall-prone. One participant spoke of this feeling of difference: I don't know anybody who is like me. If a person falls, a friend now we’ll say. It’ll only be a once off thing, say. But I, I broke ribs twice [P4].
Considering the lack of clarity on what causes falls in older adults, as well as the role of psychological factors in contributing to falls, it is little wonder fallers frame themselves as distinct from their peers as their condition is difficult to conceptualize themselves, let alone explain to others. This theme “it’s all in the mind is it” captures the poignancy that surrounds fallers as they speak of their falls and living life while being fall-prone. Fallers’ accounts of their lives reference the inexplicable nature of falls and how to them, it remains an open question of “why me” and “how did that happen.”
Discussion
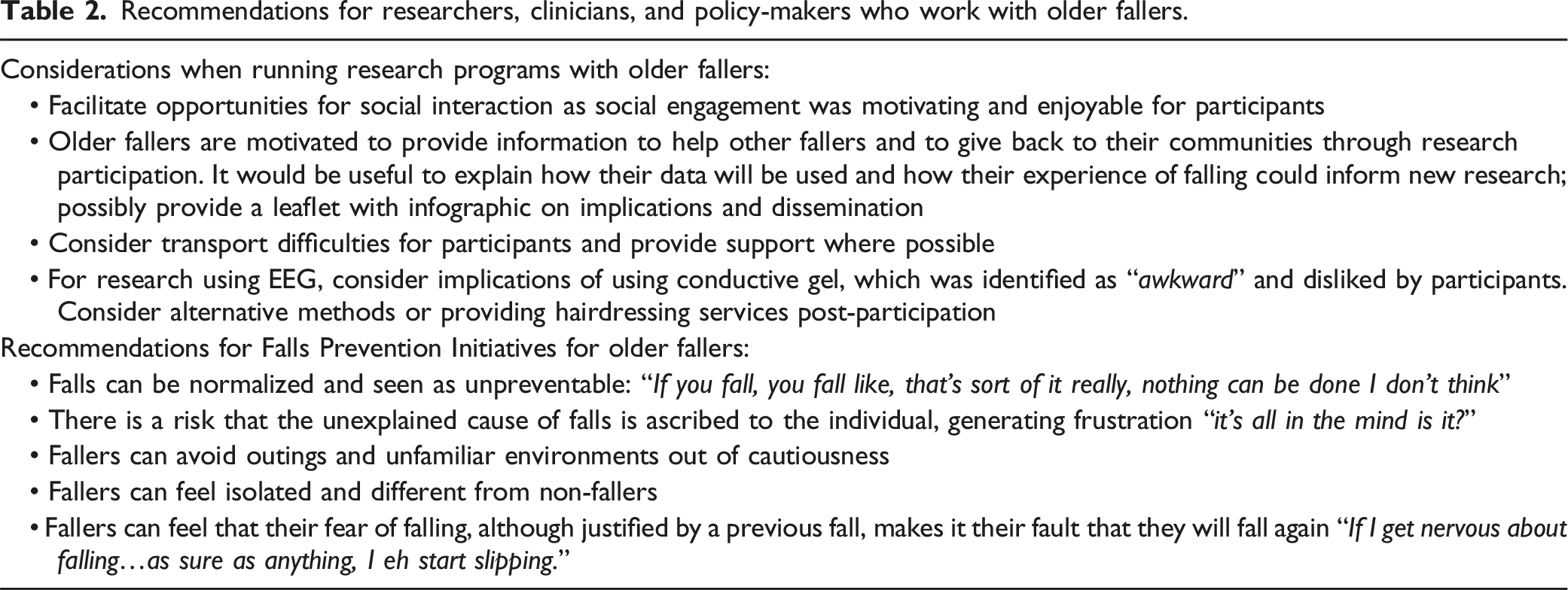
Recommendations for researchers, clinicians, and policy-makers who work with older fallers.
Through participants’ descriptions of their experience of research participation, this study provides a number of key insights into fallers’ mindsets and conceptualization of their falls. Firstly, participants emphasized the value of the social element of research participation as both motivating their participation and as a benefit they took from participating. Fallers spoke about research as a motivation to get out of the house, and the social interactions with research staff (“laughs” and “chats with the girls [research assistants]”) were described by fallers as good for them. This is important in light of the limitations to social activities expressed by most participants during interviews. One can infer that research participation is worthy of overcoming the tendency to avoid going places. All participants in this study referenced the social aspect of the study as positive and memorable. This ties in with recent findings from a study with frail older adults (Berge et al., 2020), where social interactions also emerged as motivating participation.
The current study also informs on some obstacles to participation, for example, travel to the research setting, the risk of falls when going to unfamiliar spaces, and the potential for this to impact on fallers’ ability to contribute to research. These findings have implications for future research studies in terms of appealing to fall-prone individuals to maximize participant engagement. It would be beneficial for future research studies to include opportunities for ample social interaction for fall-prone participants. Our findings also highlight the need for research into older people’s experiences of EEG, an under-researched area (Izdebski et al., 2016), as conductive gel was noted as challenging for most participants.
A second insight pertains to fallers’ conceptualization of their falls, specifically how fallers speak of falls as inevitable and “just one of these things.” This may partially account for the poor uptake in falls prevention programs. This may reflect a position where falls are seen as unpreventable and, therefore, participation in prevention initiatives may be seen as futile in the eyes of the fall-prone. Added to this is fallers’ descriptions of their cautiousness of new environments and their mobility in the community, which may represent a deciding factor in their participation in research/prevention programs. This opens the question of whether the co-design of research and falls prevention programs is required, whereby consulting fallers may maximize recruitment and retention, whilst also offering opportunities for social interaction in a low falls-risk space.
Finally, an interesting narrative thread emerged in the interviews, related to fallers’ perception of their falls. Participants’ rhetoric around falls represented a conflict, whereby fallers described their historic falls in terms of the environment they were in and all participants unprompted, identified potential external aspects that may have caused their falls. Yet, when asked directly about what they think causes their falls, participants spoke of the role of the mind and psychological factors in causing a fall. This belies fallers’ questioning of their falls as a possible psychological phenomenon and may reflect an internal coping strategy, whereby a fall is normalized through identifying external causes. This could reflect a struggle for control, whereby fallers may feel out of control physically (i.e., unable to prevent falls) and attempt to exert control mentally, by framing their falls in a certain light. We see through fallers’ language this normalization of their experience, with falls described as “just one of these things,” and the need to “get on with things”. Also probable, is that fallers seek internal causes for their fall (e.g., attention or anxiety), with the mentality of if you think you’ll fall, you will fall echoed across many interviews. Interestingly, fear of falling has become an area of research in its own right, capturing an individual’s specific anxiety around falls, and is debated as a consequence of having a history of falls (see Lavedán et al., 2018).
Limitations
It must be noted that participants in the current study are limited to fallers who access healthcare for their condition (i.e., current outpatients). Therefore, the voices of fallers who participate in research but who do not currently access healthcare are not represented. It is plausible that the experiences and views of other groups of fallers may differ to our participants. Secondly, our participants had engaged in an experimental project exploring a potential novel cause of falls (multisensory integration, that is, how our nervous system integrates information from different senses), perhaps reflecting their belief that the cause of falls is unclear. Multisensory integration may constitute a risk factor for falls (see O’Dowd et al., 2023; Zhang et al., 2020).
The time lapsed between completing the experimental study and participation in the interviews is noteworthy. Some participants participated in interviews over a year after being involved in the experimental research. We consider it a minor limitation as the focus of the interviews was on participants’ overall experience of research as opposed to the specifics of the research protocol. All participants were able to comment on their research experience, and it is unlikely partial memory of the experiment session/day affected the findings. Our inability to collect data in-person due to the effects of the COVID-19 pandemic also constitutes a limitation of this study.
Conclusion
The present study provides important insights into the mind of older fallers and, specifically, their view of research participation. Considering this population are difficult to engage in both research and falls-based initiatives, hearing the voices and perspectives of older fallers offers us an opportunity to adapt our efforts to support them to participate meaningfully and fully in community healthcare initiatives and research. This may hold benefit for them and scientific efforts to expand knowledge on falls and, by extension, intervention and prevention efforts to reduce the impact of falls on the lives of our older adults.
Supplemental Material
Supplemental Material - Experience of Being Fall-Prone and Participating in Research: Fallers’ Perspectives
Supplemental Material for Experience of Being Fall-Prone and Participating in Research: Fallers’ Perspectives by O’Brien Jessica, Marie Dollard, May Cleary, Anna Trace, Jason Chan, and Annalisa Setti in Journal of Applied Gerontology.
Footnotes
Acknowledgments
The authors would like to thank our participants, whose time and insights made this project possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JOB received funding for her doctoral research from the Irish Research Council (GOIPG/2018/3115).
Ethics Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.