
Abstract
This study investigated among older Europeans how physical function limitations lead to depressive symptoms and reductions in quality of life and well-being, and vice-versa. Further examined was how years of education moderate these relationships. These objectives were pursued using a sample of Europeans aged 50+ years (N = 46,492) within waves 5 (2013) and 6 (2015) of the Survey of Health, Ageing and Retirement in Europe. The analyses employed conditional change multilevel mixed-effects linear regressions. Mental health was found to affect physical function limitations, and vice-versa. More education significantly reduced only how earlier mental health problems lead to later physical function limitations, plausibly because of the former’s higher controllability. Thus highlighted are education-linked psychosocial resources’ protective effects.
• A longitudinal investigation showing the significant relationships between changes in mental and physical health through time, specifically among older Europeans. • The finding that education buffers how mental health problems lead to physical function limitations, but not vice-versa. • The examination of two important measures of mental health, one negative and one positive.
• Older adults’ health problems should be addressed early on, to prevent them from leading to additional health concerns. • The identification of more vulnerable older populations, including those with less education or more generally fewer psychosocial resources, who should be a focus of societal and clinical health efforts, and of health research. For those with less education, alternative means should be found and employed for bolstering problem-solving abilities and sentiments of personal control, learned effectiveness, and confidence.What this paper adds
Applications of study findings
Introduction
Older persons show physical and mental health vulnerabilities. Concerning physical health, and especially pertinent as populations worldwide age (Olsen et al., 2019), advancing age raises physical disability and functional limitations (Olsen et al., 2019; Rueda-Salazar et al., 2022; Venturini et al., 2022). In most European nations, 35%–40% of adults aged 50+ years have functional limitations (Rueda-Salazar et al., 2022). These functional limitations incur substantial societal costs in healthcare expenses (Sicsic et al., 2020) and economic productivity (Cylus & Al Tayara, 2021), including through earlier retirements (Phua & McNally, 2008). While more evenly distributed throughout the lifespan, mental health concerns also threaten older persons’ well-being. The World Health Organization (WHO) reports that among persons aged 60+ years, 15% have a mental illness, while mental-based problems account for 6.6% of disabilities (WHO, 2017). Older persons’ mental health is particularly threatened by loneliness concomitant to life course changes, such as retirement, widowhood, loss of close contacts, and physical health problems (Coyle & Dugan, 2012). More generally, the social roles losses common in later life can compromise life meaning and purpose (Sherman et al., 2011). Therefore, research and policy must address how advancing age accentuates both physical and mental health concerns’ importance.
Notably, physical and mental health are causally related, as problems potentially spread throughout a person’s life. Among older adults, having multiple chronic health conditions increases risk of depression and anxiety (Graham et al., 2024), and functional limitations mediate between chronic illnesses and depression (Han, 2018). Additionally, depressed older adults are prone to morbidity, worse consequences of physical health conditions, compromised social, physical, and cognitive functioning, inadequate self-care, and mortality (Blazer, 2003; Fiske et al., 2009; Rodda et al., 2011). A study of older adults found that over time, physical and mental health are mutually influential, with intensity of physical activity (daily life sports or other activities involving considerable energy expenditure) substantially mediating both causal directions (Ohrnberger et al., 2017). This study is among the minority of such investigations having employed longitudinal designs to infer causality, beyond cross-sectional associations. The present study also helps fill this gap.
Prominent within discussions of older persons’ health are the protective effects of resources and beneficial life circumstances, including those linked with education (see Axon & Chien, 2021). Though typically completed early in life, greater education initiates advantaged and health-beneficial life course trajectories, the benefits of which accumulate with advancing age (see Ross & Wu, 1996). Beyond economic and workforce outcomes, these health benefits occur through diverse psychosocial resources (see below).
Relatedly, an unanswered question is how education moderates older persons’ spreads of health problems between the physical and mental domains. These spreads’ moderators are generally understudied, a further gap this study helps fill. By fostering personal control, learned effectiveness, confidence, and problem-solving skills (Mirowsky & Ross, 2005a, 2005b), education plausibly stymies these health problems’ spreads (see below). These topics are highly relevant to older populations because of their heightened vulnerability to physical function limitations (Olsen et al., 2019; Rueda-Salazar et al., 2022; Venturini et al., 2022).
Accordingly, this study of older persons asks: (1) Do earlier physical function limitations lead to later mental health problems? (2) Do earlier mental health problems lead to later physical function limitations?
This study makes a further original contribution through its longitudinal assessment of how education moderates both directions of effect. Thusly, this study of older adults asks: does education help prevent (3) earlier physical function limitations from leading to later mental health problems? (4) earlier mental health problems from leading to later physical function limitations?
A further novel contribution is the investigation of two mental health measures, one negative (depressive symptoms) and one positive (an index of quality of life and well-being), permitting broader analyses of these questions.
This knowledge is of scholarly interest, as it reveals interdependencies between physical and mental health and personal characteristics that are thus protective. More pragmatically, it identifies means of limiting health problems’ spreads. This study proposes that education, because of its provided psychosocial resources, helps prevent the spread of health concerns across the physical and mental domains.
Theoretical Perspectives
The Stress Process
The stress process model is this study’s orienting theoretical framework. This model emphasizes that life circumstances can generate stressors that negatively affect physical and mental health (Pearlin et al., 1981). Furthermore, it postulates mediators and moderators of these impacts, including psychosocial resources (Pearlin et al., 1981), such as personal control, learned effectiveness, confidence, and problems-solving skills. Stressors thus proliferate across one’s interconnected life domains (Pearlin et al., 1997).
While most stress process scholarship studies features of health as outcomes of stressful circumstances, this model’s scope permits considering one health dimension as a condition that creates stressors that impact other health dimensions. In fact, some stress process scholarship concords with this claim. For example, physical function limitations constrain work, social, and leisure activities, while making daily living and personal upkeep both physically and mentally straining (see Han et al., 2021). These constraints and strains constitute stressors leading to demoralization and mental health problems (see Han et al., 2021). Mental health problems can restrain motivation for active living, including mental, physical, and social activities (see Stults-Kolehmainen & Sinha, 2014), which potently predict physical health (Cockerham, 2022; Qin & Guo, 2023). Furthermore, this inactivity is itself stressful, and attempting to live actively while undergoing mental health problems might constitute a potent stressor. All this can cause physical function limitations.
Further concordant with this model, psychosocial resources might moderate how one health concern’s resultant stressors affect other health outcomes. For example, through increasing mastery, personal control (Chesters et al., 2019; Mirowsky & Ross, 2005a), learned effectiveness, confidence, self-esteem, and problem-solving skills (Mirowsky & Ross, 2005a, 2005b; Thomas Tobin et al., 2021), education might limit stressors’ spread across intertwined life domains (see Pearlin et al., 1997), thus preventing one health problem from leading to additional health concerns (see the next section).
Accordingly, this study hypothesizes that among older persons: (1) Earlier physical function limitations lead to later mental health problems. (2) Earlier mental health problems lead to later physical function limitations.
Education-Fostered Psychosocial Resources
The stress process model highlights various moderating resources (see Pearlin et al., 1981) and their associated socioeconomic circumstances, including education. Beyond occupational and financial outcomes (Mirowsky & Ross, 2005a, 2005b), education benefits health and well-being through behaviors, including diet and exercise, and even physiological processes (Mirowsky & Ross, 2005a).
Education furthermore fosters the psychosocial resources of control over one’s life (Chesters et al., 2019; Mirowsky & Ross, 2005a), problem-solving skills, and the learned effectiveness and confidence concomitant to having effectively addressed past challenges (Mirowsky & Ross, 2005a, 2005b). Accordingly, education benefits management of aging’s challenges, including those based in health (Mitchell et al., 2018). More broadly, when faced with mental and/or physical health difficulties, more educated persons might proactively find solutions that they might confidently and effectively implement to maintain and improve their well-being. This success bolsters sentiments of personal control and optimism (Mitchell et al., 2018). These concomitants to education are mutually influential (Mirowsky & Ross, 2005a). For example, fewer sentiments of personal control and learned effectiveness and less confidence in one’s problem-solving skills could stifle actions to improve one’s life, creating worse circumstances that further decrease these psychosocial resources. The reduced control over one’s life commonly associated with aging (Morgan & Brazda, 2013) might accentuate education’s value.
Since education-linked psychosocial resources might bolster effective management of difficult and constraining life circumstances, including those based on physical and mental health (see Mirowsky & Ross, 2005b), this study of older adults hypothesizes: more years of education help prevent (3) earlier physical function limitations from leading to later mental health problems. (4) earlier mental health problems from leading to later physical function limitations.
Methods
Dataset and Sample
This study is focused on the fifth (2013) and sixth (2015) (Börsch-Supan, 2022a, 2022b) waves of the Survey of Health, Ageing and Retirement in Europe (SHARE), a longitudinal panel survey of adults aged 50+ years within many European countries and Israel. The SHARE includes extensive variables concerning employment and retirement, health, socioeconomic status, and living circumstances. The first wave (2004) involved over 22,000 interviews and spanned 11 European countries. Later rounds took place approximately once every 2 years and included further European nations. Börsch-Supan et al. (2013) explain many of the SHARE’s facets. Bergmann et al. (2019) discuss SHARE response and retention rates.
Data constraints necessitated use of waves 5 and 6. Wave 7 (2017) included the SHARELIFE module for all respondents not included in this module during wave 3 (2008–2009). This module addressed only past circumstances, producing too much missing data for some of this study’s key variables. The COVID-19 pandemic interrupted the eighth wave (beginning in October 2019). The subsequent pandemic-era interviews involved health determinants extraneous to this study’s concerns, while being discordant with the pre-pandemic interviews. Waves 5 and 6 were thus the two most recent consecutive waves that could be here employed. Longitudinal data were required to assess the mutual influences through time between physical and mental health. Employing further waves would create additional concerns with selective attrition and sample weighting (see below).
Marital status, parental status, and years of education (discussed below) were obtained from the easySHARE’s (Börsch-Supan & Gruber, 2022) fifth wave. This simplified generated dataset includes key variables for all respondents throughout all waves within a single file (see Gruber et al., 2014). This dataset was ideal for these variables since all their values were recorded during all waves, instead of being recorded only if a change occurred since the previous wave, which pertains to some variables within the regular SHARE datasets.
Respondents were included if they were involved in both waves 5 and 6 and were aged 50+ years during wave 5. The sample size was 46,492 respondents, from 14 nations: Austria, Belgium, Czech Republic, Denmark, Estonia, France, Germany, Israel, Italy, Luxembourg, Slovenia, Spain, Sweden, and Switzerland.
Variables
Dependent Variables
This study’s dependent variables were wave 6 health-related measures. First was an index of physical function limitations, computed through adding together the numbers of reported limitations in activities of daily living (0–6), instrumental activities of daily living (0–9), and mobility (0–10). This addition of these three variables that are conceptually congruent as difficulties with physical actions and activities thus produced a “physical function limitations” index (values ranging 0–25). Activities of daily living denote management of basic physical requirements, including ability to walk or move around, eat, toilet, dress, and maintain personal hygiene. Instrumental activities of daily living involve more complex tasks, including accessing transportation, telephone calls, laundry, preparing food, and cleaning one’s residence. The mobility limitations concern actions involving strength, stamina, arm function, and fine motor function. At wave 6, all three components showed statistically significant correlations (p < .0001) spanning 0.617–0.755. These considerable intercorrelations suggest that these measures denote overlapping features of a broader aspect of physical health based on difficulties with physical functions, thus supporting their inclusion in one index. These strong intercorrelations are unsurprising given these variables’ conceptual overlap and similarity. In fact, previous scholarship has combined these variables into indices (Connolly et al., 2017; Døhl et al., 2016, 2020; Hsueh et al., 2004; Tian et al., 2021).
This study’s first mental health outcome was a negative measure, the EURO-D (European depression scale). This index (0–12) denotes the number of positive reports of 12 symptoms of depression in the previous month, including feelings of being depressed, pessimism, guilt, irritability, concentration difficulties, and tearfulness.
The second, a positive and more general measure, was the CASP Index for Quality of Life and Well-Being (12–48). It includes four dimensions: control, autonomy, self-realization, and pleasure. Among the 12 items, three per dimension, are how often do you feel/think -left out of things? (control) -that shortage of money stops you from doing the things you want to do? (autonomy) -full of energy these days? (self-realization) -that your life has meaning? (pleasure)
Respondents answered all items from 1 = never to 4 = often (negative statements reverse coded). These responses (1–4) were added across all 12 items.
Independent Variables
The independent variables were the dependent variables’ wave 5 counterparts. Concerning the physical function limitations index, at wave 5 all three components showed statistically significant correlations (p < .0001) spanning 0.583–0.707, supporting their inclusion in one index. Since the independent variables were continuous interactants, they were mean centered to aid their main effects’ interpretability. Through mean centering, each one’s main effect denotes its coefficient based on the other interactant being at its mean, instead of zero, which is a less logical value.
Moderating Variable
This study’s moderating variable was years of education (constant between both waves). This continuous interactant was mean centered.
Control Variables
Some potentially confounding wave 5 demographic variables were controlled, including gender (men = reference category (ref.)) and age (in years). Marital/relationship status included married, living together with spouse (ref.); registered partnership; married, living separated from spouse; never married; divorced; and widowed. Parental status included no children (ref.), one child, two children, and three or more children. Employment status included retired (ref.), employed/self-employed, unemployed, permanently sick or disabled, homemaker, and other.
Each model further controlled for the outcome’s wave 5 counterpart (see conditional change modelling below), without mean centering.
Household income was not controlled because a substantial proportion of the sample were retired, lessening this variable’s value. Furthermore, education fosters personal control and learned effectiveness partly through improving household finances. The latter thus lie on the postulated causal pathways between this study’s interaction terms and its health outcomes.
Analysis
This study’s central analyses were four multilevel mixed-effects linear regressions, including random intercepts for each country of residence to account for the data’s nested structure, adjust for unobserved heterogeneity at this contextual level, and account for within-country correlations between respondents. Importantly, each model controlled for the dependent variable’s wave 5 counterpart. This conditional change modelling implied that each wave 6 outcome designated change in this variable between the fifth and sixth waves, lessening concerns with reverse causation, while adjusting for floor and ceiling effects. Furthermore, studying predictors of changes in an outcome permits stronger causal inferences.
The first model focused on how wave 5 physical function limitations affected wave 6 depressive symptoms and moderation by education. The second model repeated this analysis with the CASP Index as the outcome. The third model assessed how wave 5 depressive symptoms affected wave 6 physical function limitations and moderation by education. The fourth model repeated this analysis with the wave 5 CASP Index as the central predictor.
Only Models 3 and 4 showed statistically significant interactions (see below). For these models, figures graphically display the central associations’ magnitudes. While the x-axes denote the independent variables, the y-axes designate the dependent variable. Two lines are displayed (with 95% confidence intervals (CIs)), one indicating 5 years of education (10th percentile) and the other indicating 17 years of education (90th percentile). In creating these figures, no variables were mean centered. These figures were developed via predictive margins, computed through Stata’s “margins” command.
All models were weighted with the SHARE calibrated longitudinal individual weights for waves 5 to 6, which adjusted for differing likelihoods of selection into the sample, nonresponse, and selective attrition, helping prevent biases. Inclusion of further waves would have precluded use of effective longitudinal weights.
This study’s moderate amounts of missing data did not require multiple imputation. After exclusion of missing data in the dependent variable (the imputed values of which would not have been used in the final analyses if a multiple imputation procedure were conducted, see Von Hippel (2007)), only Model 4 had a proportion of missing data of 10% or more (10.71%). Accordingly, missing data were dealt with through listwise deletion.
Further analyses repeated these regressions separately among respondents aged 50–64 years and 65+ years (online supplemental appendix). These analyses were motivated by these groups’ health differences and discrepancies in activity levels based on the latter’s higher likelihoods of being retired.
All analyses employed the Stata 18 statistical software package.
Results
Descriptive Statistics (N = 46,492).
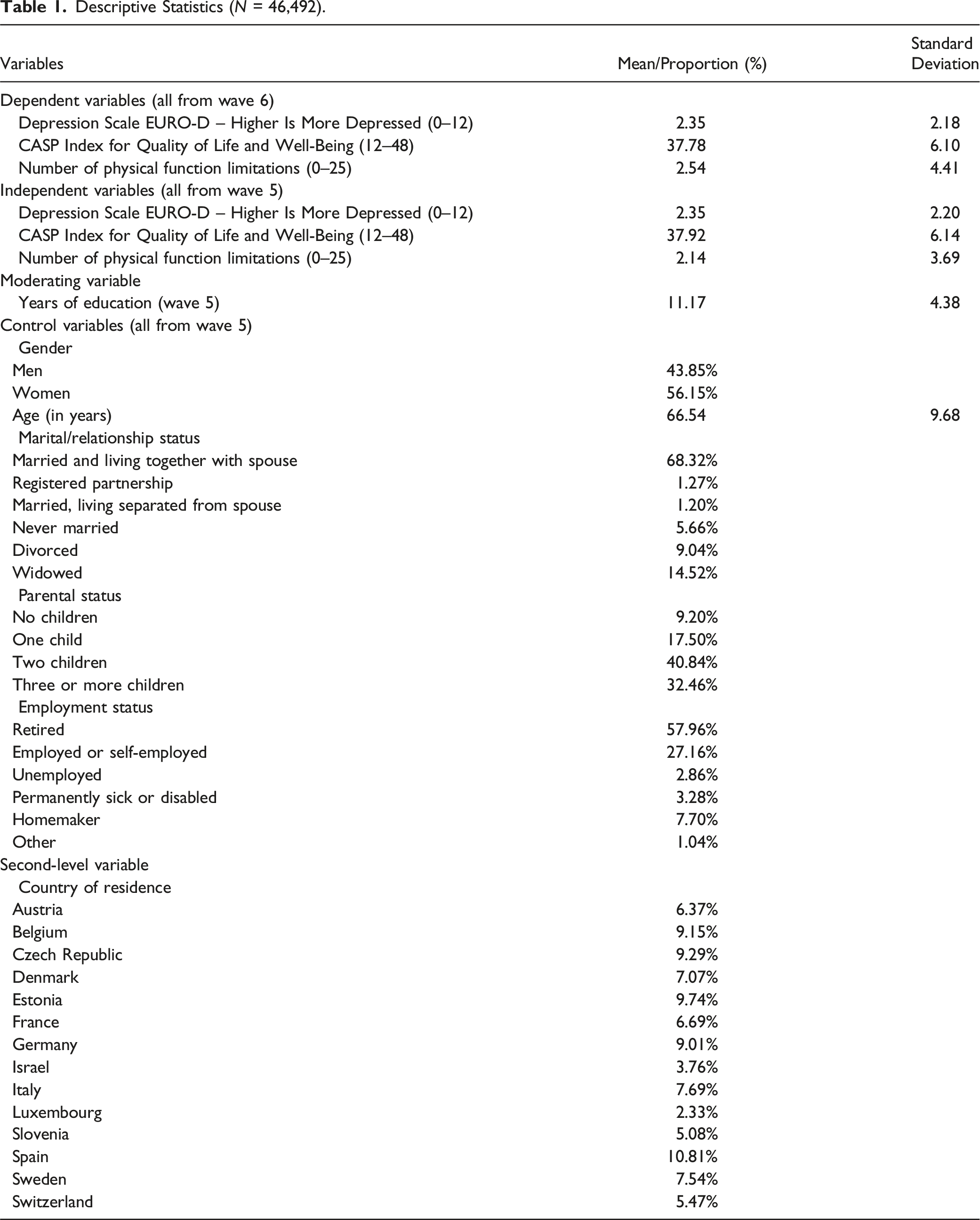
The majority of the sample were women (56.15%). The average wave 5 age was 66.54 years. The majority of the sample were married, living together with spouse (68.32%). The modal parental status category was two children (40.84%). While 57.96% of the sample were retired, 27.16% were employed/self-employed. Respondents were broadly spread across the countries, the modal country being Spain (10.81%).
Multilevel Mixed-Effects Linear Regression Analyses of Physical Function Limitations and Mental Health Coefficients.
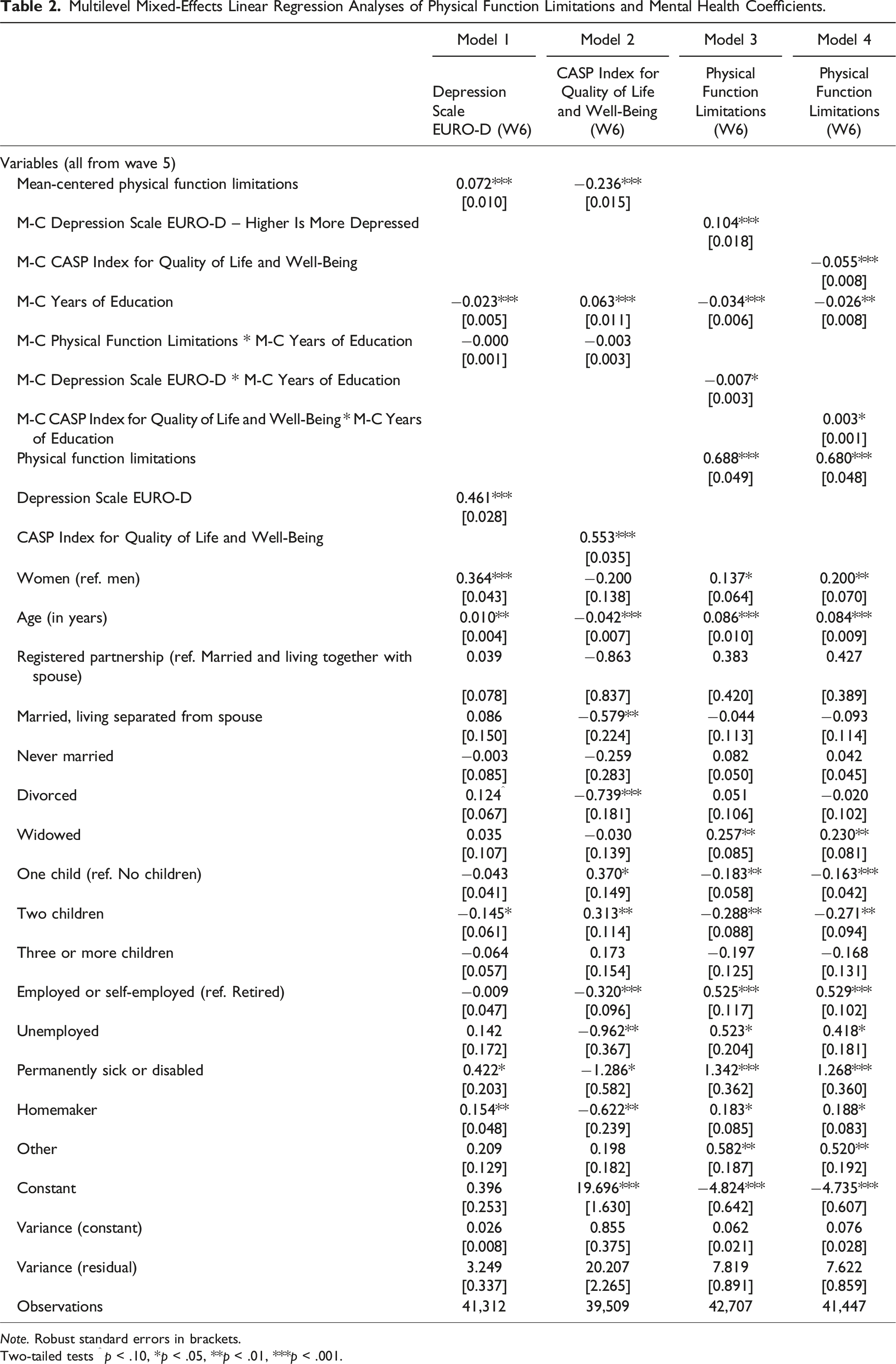
Note. Robust standard errors in brackets.
Two-tailed tests ^ p < .10, *p < .05, **p < .01, ***p < .001.
Within each model, at the average amount of education, the focal independent variable was significantly associated with the outcome in the expected direction. Each additional physical function limitation increased one’s depressive symptoms by 0.072 (p < .001) (Model 1) and decreased one’s CASP Index by 0.236 (p < .001) (Model 2). Each additional depressive symptom increased one’s physical function limitations by 0.104 (p < .001) (Model 3), and each additional CASP Index point reduced one’s physical function limitations by 0.055 (p < .001) (Model 4). Thus evidenced are health concerns spreading bidirectionally across the physical and mental domains, confirming hypotheses 1 and 2.
In predicting depressive symptoms (Model 1) and the CASP Index (Model 2), physical function limitations insignificantly interacted with education. However, in predicting physical function limitations, education significantly downwardly moderated the effect of depressive symptoms (interaction coefficient (coeff.): −0.007, p < .05) (Model 3) while significantly reducing the value of higher CASP Index scores (interaction coeff.: 0.003, p < .05) (Model 4). Accordingly, education significantly buffered only the effects of mental health upon physical function limitations (confirming hypothesis 4, disconfirming hypothesis 3).
Figures 1 and 2 graphically display the magnitudes of the central associations within Models 3 and 4, respectively. Both figures reveal more education implying fewer physical function limitations. Figure 1 shows that at both 5 and 17 years of education, more wave 5 depressive symptoms predicted worse wave 6 physical function limitations. However, this increase was steeper at 5 years of education. As of approximately two depressive symptoms, the two lines’ 95% CIs do not overlap. Predicted Number of Physical Function Limitations based on Depressive Symptoms Moderated by Years of Education, with 95% Confidence Intervals. Predicted Number of Physical Function Limitations based on the CASP Index for Quality of Life and Well-Being Moderated by Years of Education, with 95% Confidence Intervals.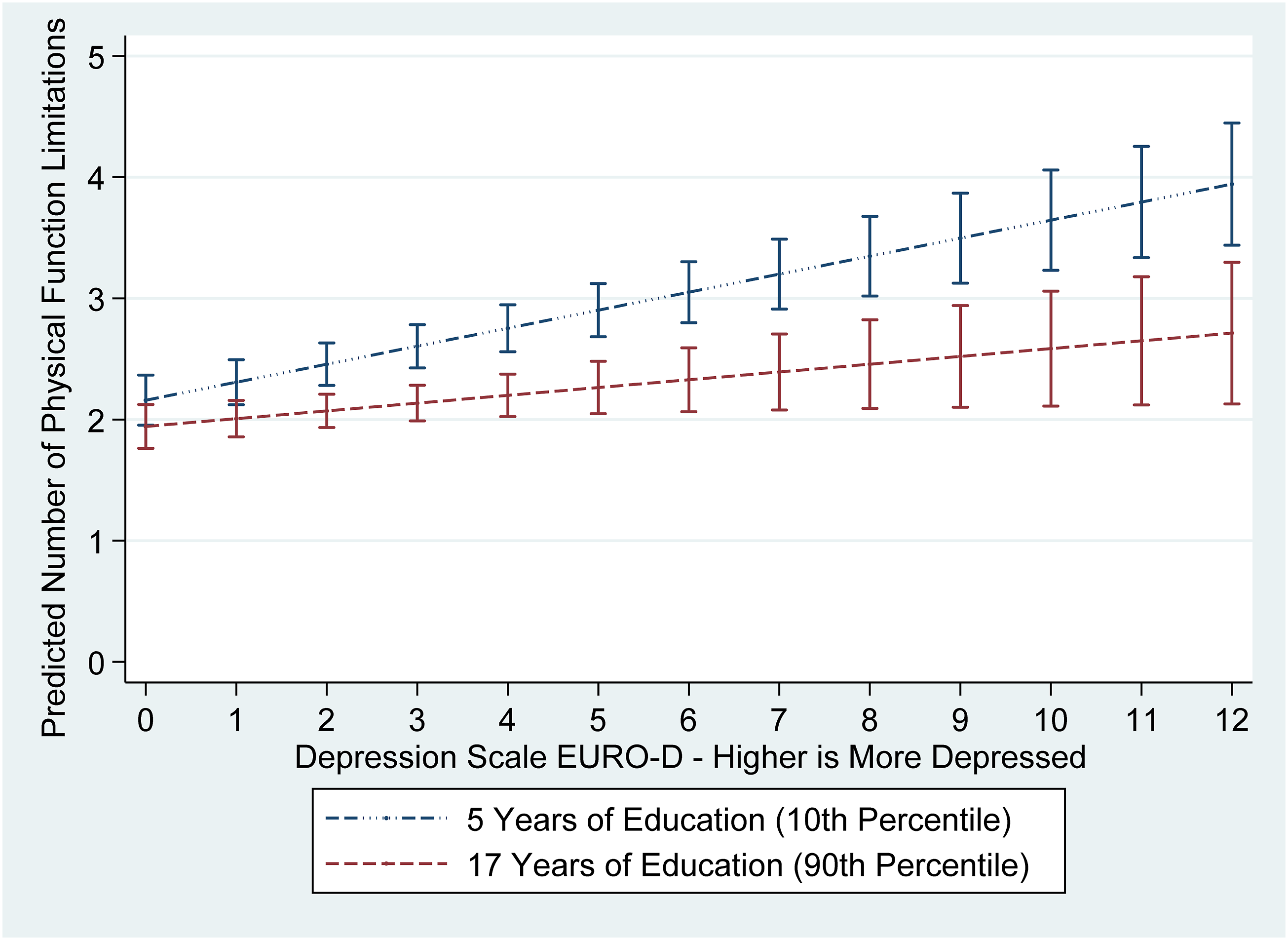
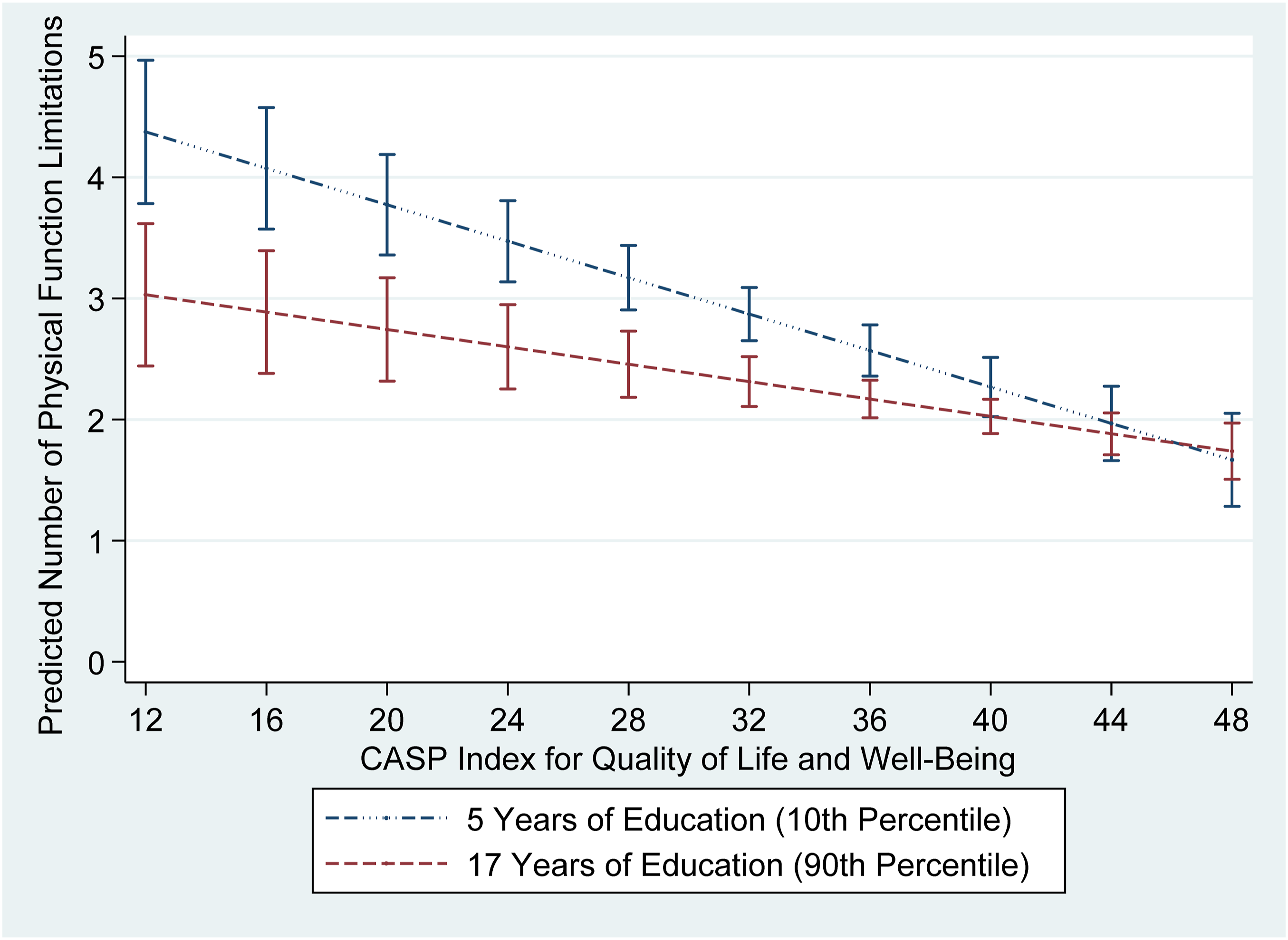
Figure 2 shows that at both amounts of education, a higher wave 5 CASP Index score led to fewer wave 6 physical function limitations. However, this decrease was steeper for those with 5 years of education. Until a CASP Index score of approximately 37, the two lines’ 95% CIs do not overlap.
The age-stratified analyses mostly concur with the main analyses. Notably, the smaller sample sizes prevented the interaction terms from reaching statistical significance. This is unsurprising since to have the same statistical power as a main effect, an interaction term requires 16 times the sample size (Gelman, 2018).
There are only a few notable differences between these two age groups’ results. The wave 5 CASP Index shows a stronger association with wave 6 physical function limitations among the older respondents (coeff.: −0.064, p < .001; younger respondents coeff.: −0.044, p < .001). Similarly, the interaction between education and the wave 5 CASP Index is more strongly associated with wave 6 physical function limitations within the older sample (interaction coeff.: 0.003; younger sample interaction coeff.: 0.002). Accordingly, regarding the CASP Index, hypotheses 2 and 4 are more strongly supported within the older sample. Also notably, wave 5 physical function limitations more strongly predicted wave 6 depressive symptoms among the younger respondents (coeff.: 0.086, p < .001; older respondents coeff.: 0.059, p < .001). Accordingly, regarding depressive symptoms, hypothesis 1 is more strongly supported within the younger sample.
Discussion
This study of older Europeans found physical function limitations leading to mental health problems, and vice-versa. Education helps prevent earlier mental health problems from leading to later physical function limitations, but not vice-versa. The findings’ moderate (yet noteworthy) magnitudes were expected given the 2-year timeframe and the fact that all life characteristics conceivably affect health.
Concordant with the stress process model (see Pearlin et al., 1981, 1997), one health circumstance can generate stressors that affect other health domains. Physical function limitations can cause daily pains and efforts; hamper personal and home upkeep; restrain one’s help provided to close contacts; and hinder physical, social, cognitive, and work activities, all of which can affect depressive symptoms and well-being.
In turn, mental health problems can cause fatigue and lethargy, and physical (Lindwall et al., 2011) and more general inactivity (Morrow-Howell et al., 2014). Furthermore, depression raises risk of health-damaging behaviors, including overeating and smoking (Lindwall et al., 2011), which affect physical functioning (Capodaglio et al., 2010). Conversely, happiness and well-being improve physical functioning (Lyubomirsky et al., 2005). Mental health problems can thus create stressors that impact one’s body and activities in manners that increase physical function limitations. Thus evidenced is the proliferation of stressors across interlinked life domains (see Pearlin et al., 1997).
This study postulates that education’s protective effect is largely due to its fostering of personal control, learned effectiveness, confidence, and problem-solving skills (Chesters et al., 2019; Mirowsky & Ross, 2005a). Mental health problems might be more controllable than physical function limitations, which constitute more concrete and unmalleable restraints on daily actions, less amenable to efforts of will. This might explain why education and its associated psychosocial resources only moderated mental health problems’ effects upon physical function limitations. Well-educated older persons undergoing mental health problems might feel empowered to sustain their physical, social, and cognitive activities, and generally favorable life circumstances, protecting their physical functioning. They might develop and enact effective plans for managing their mental health concerns and reducing their consequences.
The age-stratified analyses’ results mostly confirmed the main analyses’ answers to the research questions. Pertaining to the second and fourth research questions, the findings that the wave 5 CASP Index and its interaction with education more strongly predicted wave 6 physical function limitations among the older respondents are plausibly due to their more fragile physical health, which is more vulnerable to lower quality of life, thus also increasing education’s protective value. With relevance to the first research question, wave 5 physical function limitations’ stronger prediction of wave 6 depressive symptoms among the younger respondents is possibly because among them, worse physical function limitations are less normative and expected, thus constituting bigger shocks and/or sources of self-blame.
Conclusion
This study makes some notable theoretical contributions. These include adding to the limited stress process scholarship (e.g., Cockerham, 2022; Han et al., 2021; Qin & Guo, 2023; Stults-Kolehmainen & Sinha, 2014) addressing how health problems of one type can affect health concerns of another type. This study also extends scholarship emphasizing that psychosocial resources are especially effective at buffering the effects of more controllable stressful conditions (e.g., Gaylord-Harden et al., 2018; Holzer et al., 2024; Kubzansky et al., 2018). Accordingly, “control” pertains to both people and their stressors. A person profiting from personal control while facing more controllable stressors will be especially protected. This study further suggests that education is a socioeconomic characteristic that promotes a multitude of psychosocial resources (concurring with Mirowsky and Ross (2005a, 2005b)) that operate in unison in preventing more controllable health problems from leading to subsequent health concerns. Accordingly, while a life circumstance (including poorer health of one kind) can generate diverse stressors, a socioeconomic or demographic characteristic (including extent of education) can produce multiple protective psychosocial resources.
Some policy recommendations are suggested. First, older adults’ health problems should be addressed early on, before they accumulate into further health concerns. Second, some populations, including older persons, those with less education, and those more generally lacking psychosocial resources, are more susceptible to the accumulation of health concerns. They should be foci of societal and clinical efforts to limit health problems and of health research. Beyond improving older persons’ lives, such measures will help contain healthcare costs and maintain economies’ strength within circumstances of population aging.
Further noteworthy are this study’s limitations and recommended future research paths. These analyses should be repeated within younger samples, whose results might differ due to contrasts in mental and physical health, psychosocial resources, workforce involvements, etc. Additional health measures should be studied, including chronic health conditions, biomarkers, anxiety, and stress levels. Future research might also examine social connectedness, employment, and financial circumstances as moderators.
Future research should also investigate cross-national differences. One relevant variable is ageism. Less ageist nations might be more sympathetic to older residents’ health problems, reducing stigma and increasing support. Among this study’s nations, the Czech Republic, France, and Slovenia are more ageist, while Denmark, Germany, and Sweden evince lower ageism (Rychtařiková, 2019). Further relevant is collectivistic versus individualistic cultural orientation. More collectivistic cultures might show more willingness to help older residents undergoing health concerns. While Slovenia is especially collectivistic, Belgium, Denmark, and Italy are notably individualistic (Ilies & Zahid, 2019). Also pertinent are national governments’ expenditures to support those with physical and mental disabilities. While the Czech Republic and Slovenia have low percentages of their GDPs dedicated to such protections, the converse applies to Belgium, Denmark, and Germany (European Court of Auditors, 2023). Among other contextual characteristics, these variables plausibly affect older persons’ spreads of health problems between the physical and mental domains, and the importance of education and its associated psychosocial resources.
This study found that among older adults, physical and mental health are mutually influential. Furthermore, education protects against mental health concerns resulting in physical function limitations. Education’s insignificant moderation of physical function limitations’ effects upon mental health suggests that psychosocial resources might be more protective against more controllable stressful circumstances. Accordingly, this study makes notable contributions to stress process scholarship.
Supplemental Material
Supplemental Material - Shielded by Education? The Buffering Role of Education in the Relationships Between Changes in Mental Health and Physical Functioning Through Time Among Older Europeans
Supplemental Material for Shielded by Education? The Buffering Role of Education in the Relationships Between Changes in Mental Health and Physical Functioning Through Time Among Older Europeans by Jason Settels in Journal of Applied Gerontology
Footnotes
Acknowledgements
This paper uses data from SHARE waves 5 and 6 (DOIs: 10.6103/SHARE.w5.800, 10.6103/SHARE.w6.800) (see Börsch-Supan et al. (2013) for methodological details). The SHARE data collection has been funded by the European Commission, DG RTD through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982, DASISH: GA N°283646) and Horizon 2020 (SHARE-DEV3: GA N°676536, SHARE-COHESION: GA N°870628, SERISS: GA N°654221, SSHOC: GA N°823782, SHARE-COVID19: GA N°101015924) and by DG Employment, Social Affairs & Inclusion through VS 2015/0195, VS 2016/0135, VS 2018/0285, VS 2019/0332, and VS 2020/0313. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C, RAG052527A) and from various national funding sources is gratefully acknowledged (see ![]() ).
).
Author Contributions
The sole and corresponding author made all contributions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the 2020 Research Block Grant Allocation Scheme–Merit Based Funding Scheme: Incentive B, Faculty of Humanities, Education and Social Sciences, University of Luxembourg. This funding source had no involvement in study design; in the collection, analysis, and interpretation of data; in the writing of the article; and in the decision to submit it for publication.
Ethical Statement
Data Availability Statement
One must apply for access to Survey of Health, Ageing and Retirement in Europe (SHARE) data, see https://share-eric.eu/. This paper uses data from the generated easySHARE data set (DOI: 10.6103/SHARE.easy.800), see ![]() for methodological details. The easySHARE release 8.0.0 is based on SHARE waves 1, 2, 3, 4, 5, 6, 7, and 8 (DOIs: 10.6103/SHARE.w1.800, 10.6103/SHARE.w2.800, 10.6103/SHARE.w3.800, 10.6103/SHARE.w4.800, 10.6103/SHARE.w5.800, 10.6103/SHARE.w6.800, 10.6103/SHARE.w7.800, 10.6103/SHARE.w8.800).(1)
for methodological details. The easySHARE release 8.0.0 is based on SHARE waves 1, 2, 3, 4, 5, 6, 7, and 8 (DOIs: 10.6103/SHARE.w1.800, 10.6103/SHARE.w2.800, 10.6103/SHARE.w3.800, 10.6103/SHARE.w4.800, 10.6103/SHARE.w5.800, 10.6103/SHARE.w6.800, 10.6103/SHARE.w7.800, 10.6103/SHARE.w8.800).(1)
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.