
Abstract
Retention of the home care (HC) aide workforce is essential to meet the needs of our aging population. Some studies suggest that improving HC safety could increase job retention. This study objective was to explore qualitatively the connection between aide and client safety and factors impacting this care relationship. Data consisted of audio-recorded, verbatim responses to open-ended questions of two focus groups with aides (n = 10), two in-person interviews with HC agency managers, and 37 phone interviews with those working in (aides, n = 16; managers, n = 12) and receiving (clients, n = 9) HC. Clients reported home layout and accessibility as safety concerns. Aides and managers reported that client family members can make the care job more challenging. The aide-client connection was affected by communication style, family and HC agency support, allotted care time, and job task boundaries. Interventions that address the safety of both clients and aides can influence HC job satisfaction and retention.
Keywords
• Illustrates through qualitative inquiry the connection and overlap between (a) home care (HC) aide and client relationship, and (b) HC aide and client safety and well-being, and how these contribute to aide job satisfaction and client security. • Provides nuanced perspectives from key HC stakeholders—aides, clients, and agency managers—on the role of safety in improving care work conditions and job satisfaction. • Reports verbatim voices on strengths and challenges of working in or receiving HC through the lens of safety and its role in the development of trusting, professional relationships that improve care services for both clients and aides.
• These qualitative findings suggest specific HC workforce retention attributes upon which stakeholders can affect practice and policy changes that can improve the safe delivery of care services for clients and aides alike.What this paper adds
Applications of study findings
Background
Home care (HC) is an essential part of the health care and social assistance sector for older adults, people with chronic illnesses, and those with disabilities (Markkanen et al., 2014; Quinn et al., 2016, 2021). Home care aides assist clients with activities of daily living, including dressing, bathing, toileting, mobilization, meal preparation, and homemaking. In 2020, there were over 3.4 million home health and personal care aides employed in the USA (Bureau of Labor Statistics, 2021). Demand for HC is increasing in the USA, with predicted growth of 33% between 2020–2030 in the HC sector (Bureau of Labor Statistics, 2021). A recent analysis estimates there will be 7.4 million total direct care employment openings between 2019–2029—over 4.5 million specific HC jobs (McCall, 2021). Availability and quality of essential care services are affected by turnover and caregiver shortage within the HC aide workforce (Galewitz, 2021; Scales, 2022).
Many researchers have characterized occupational safety and health (OSH) hazards among HC workers (Quinn et al., 2021). Recently published HC OSH research includes, but not limited to, musculoskeletal injuries (Sun et al., 2018), exposure to cleaning and disinfecting chemicals (Lindberg et al., 2021), injuries from sharp medical devices (Brouillette, Quinn, & Kriebel, 2017; Brouillette, Quinn, & Kriebel, et al., 2017) and other blood or biological exposures (Agbonifo et al., 2017), occupational stress (Grasmo et al., 2021; Muramatsu et al., 2019), burnout (Mockli et al., 2020), and verbal abuse (Byon et al., 2020; Karlsson et al., 2019). Noted gaps in existing literature include limited published data on how safety of each stakeholder in HC affects others, as well as limited findings from first-person reports by different stakeholders regarding safety climate in HC. Studies have shown that HC work safety can predict both job satisfaction and workforce retention (Sherman et al., 2008) and the relationship between job satisfaction and worker retention (Boone, 2021; Gleason & Miller, 2021; Jang et al., 2017).
Prior qualitative studies from authors suggest that HC aide and client safety are connected and need further investigation (Karlsson et al., 2020; Markkanen et al., 2014, 2021). This synergy is not as well recognized in HC compared to other healthcare settings, where strong evidence shows that patient safety cannot exist without healthcare worker safety (Grime, 2021; Riehle et al., 2013; Shaw et al., 2020). In response to the COVID-19 pandemic, the World Health Organization published a report identifying various action points for ensuring healthcare worker safety as it affects patient safety (World Health Organization, 2020).
The objectives of this paper are to: (a) explore the connection and overlap—through qualitative inquiry—between the HC aide and client safety and well-being through self-reported lived experiences and perspectives of key stakeholders, namely, aides, clients, and managers, and (b) build upon prior research regarding safety strengths and challenges in HC. The focus of this paper is safety while working in or receiving HC. Qualitative inquiry is well-suited for this study’s exploration: in-depth interview and focus group data can reflect “real life” occurrences among aides, managers and clients, therefore, offer a rich and solid understanding on their lived experiences as they happen in their social and professional worlds (Miles et al., 2020).
In this study, we explore HC safety from both aides’ and clients’ perspectives, including both physical and psychological aspects. Physical safety may include risk of acute injury or pain, physical violence, and risk of endangerment. Psychological safety may refer to factors such as autonomy, degree of control over self or job, or may refer to issues like verbal abuse, workplace stress, interpersonal relationships (e.g., dealing with challenging family members), being asked to complete tasks outside the job description.
Methods
This study—conducted in Massachusetts (USA) in 2020—was part of a formative grounded theory qualitative phase of the larger Safe Home Care Project intervention study (2019–2023) (University of Massachusetts Lowell, 2020) to improve the safety of HC aides and clients. Study methods and materials, including the informed consent procedures, were approved by the University of Massachusetts Lowell Institutional Review Board (IRB, Protocol number: 19–112-QUI-XPD). All study participants provided a signed consent.
Participants were recruited by (a) mailing recruitment materials to partnering HC agencies (aides), (b) utilizing an agency liaison to deliver recruitment materials (clients), or (c) directly contacting participants via email (HC managers). The senior mixed methods investigator (PM) conducted all interviews and moderated two in-person focus groups according to the question guides. Sample focus group and interview questions are available in Online Appendix 1. All focus group and interview sessions were audio-recorded and transcribed verbatim. The interview research team revised in-person methods (i.e., focus groups, in-depth interviews) to remote phone in-depth interviews in March 2020 due to the pandemic.
The dataset comprised transcribed, open-ended responses from (a) two in-person focus groups with HC aides (n = 10) during February–March 2020, (b) two in-person interviews with HC agency managers (n = 2) during February 2020, and (c) 37 phone interviews with HC aides (n = 16) and HC agency managers (n = 12), and clients (n = 9) receiving HC services, during April–November 2020. The dataset was previously coded according to the grounded theory approach (Charmaz, 2014; Patton, 2015) by three research team members (PM, NB, NK) using NVivo 12 software (QSR International). For the current analysis, a team member trained in qualitative methods (NB) reviewed open-ended responses and existing hierarchy for relevant themes and cross-referenced by the senior investigator (PM). The coding process was an integrated approach, utilizing both deductive and inductive coding strategies (Miles et al., 2020). The prominent themes were determined deductively and based on the focus group and interview guide questions. The supporting themes were derived inductively through grounded theory from the participants’ narratives.
Study participants were also invited to complete a voluntary, anonymous demographics survey as described in Markkanen et al. (2021). Study data are confidential and not publicly available to protect participant anonymity; further information may be requested from the corresponding author.
Further detailed methods—including the purposive sampling strategy, study population recruitment, data collection and analysis, and triangulation of findings between different participant groups (i.e., clients, aides, and managers)—are described elsewhere (Markkanen et al., 2021). This prior study focused solely on analyzing COVID-19 pandemic impacts on key HC stakeholders. Online Appendix 2 includes the completed Criteria for Reporting Qualitative Research (COREQ) (Tong et al., 2007) checklist for this study.
Results
Demographics of Study Population
Characteristics of Study Participants Who Responded to the Demographics Survey: Home Care Aides (n = 14), Managers (n = 9), Clients (n = 6).
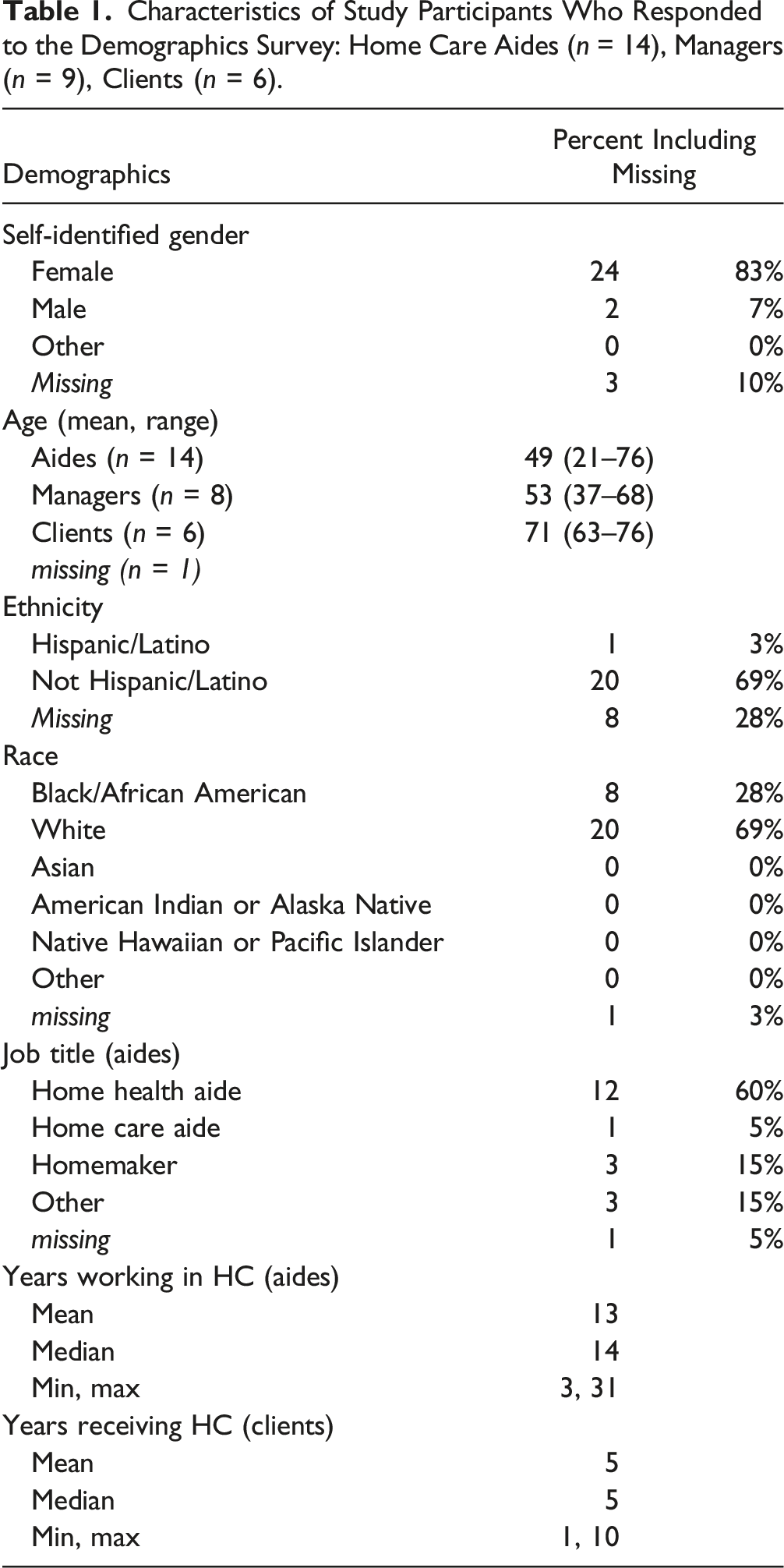
Of the 14 aides who returned the survey, respondents were Black (n = 8) or White (n = 5) and one aide did not respond. All managers (n = 9) and clients (n = 6) reported their race as White. Most participants (aides, managers, clients) identified as Not Hispanic/Latino (n = 20, 69%) and one aide identified as Hispanic/Latino (4%). There were significant missing values for this ethnicity question (n = 8, 28%).
Clients received HC for 1–10 years (mean 5 years). Aides reported working in HC for an average of 13 years, ranging from 3 to 31 years. Most aides reported their occupational titles as home health aide (n = 12, 60%), followed by homemaker (n = 3, 15%). Some aides reported multiple job titles, such as “home health aide” and “hospice aide” (n = 1) or “Certified Nursing Assistant” (n = 1). Among managers, half were executive directors while half held care manager or clinical services director/manager positions at their agencies/organizations.
Meaning of Safety in the Home
Three prominent themes were determined through deductive coding: (a) client-aide relationship, (b) aide job safety, and (c) client home safety (Figure 1). These contribute to: (a) aide job satisfaction or (b) client security. Aides described job satisfaction as a career goal, while clients sought security as a focal point or life goal. In our dataset, aide job satisfaction is described as compensated work that is meaningful and rewarding, and aides strive to have a career they enjoy, and one that provides a sense of accomplishment and pride while helping others live more independently. For clients, security is described as feeling confident and trusting regarding personal safety and well-being, having technology to assist during safety or medical incidents (e.g., Life Alert, Lifeline), and consistency regarding HC providers, including adequate allotted visit time and turnover rates among HC aides. There was considerable overlap among aide and client safety themes; aides and clients described similar physical and psychological safety concerns, as depicted in Figure 1. Additionally, both the client-aide relationship and the safety of both aides and clients were impacted by several factors: communication style, client’s family cooperation, and the extent to which the HC agency acts as a bridge between aides and clients and offers support to both groups. The client-aide relationship and safety in home care as reported by aides, clients, and managers in Safe Home Care Project focus groups and interviews. The bolded themes were derived deductively from parent codes based on the focus group and interview guide questions. The bulleted supporting themes were derived inductively from the verbatim narratives of participants.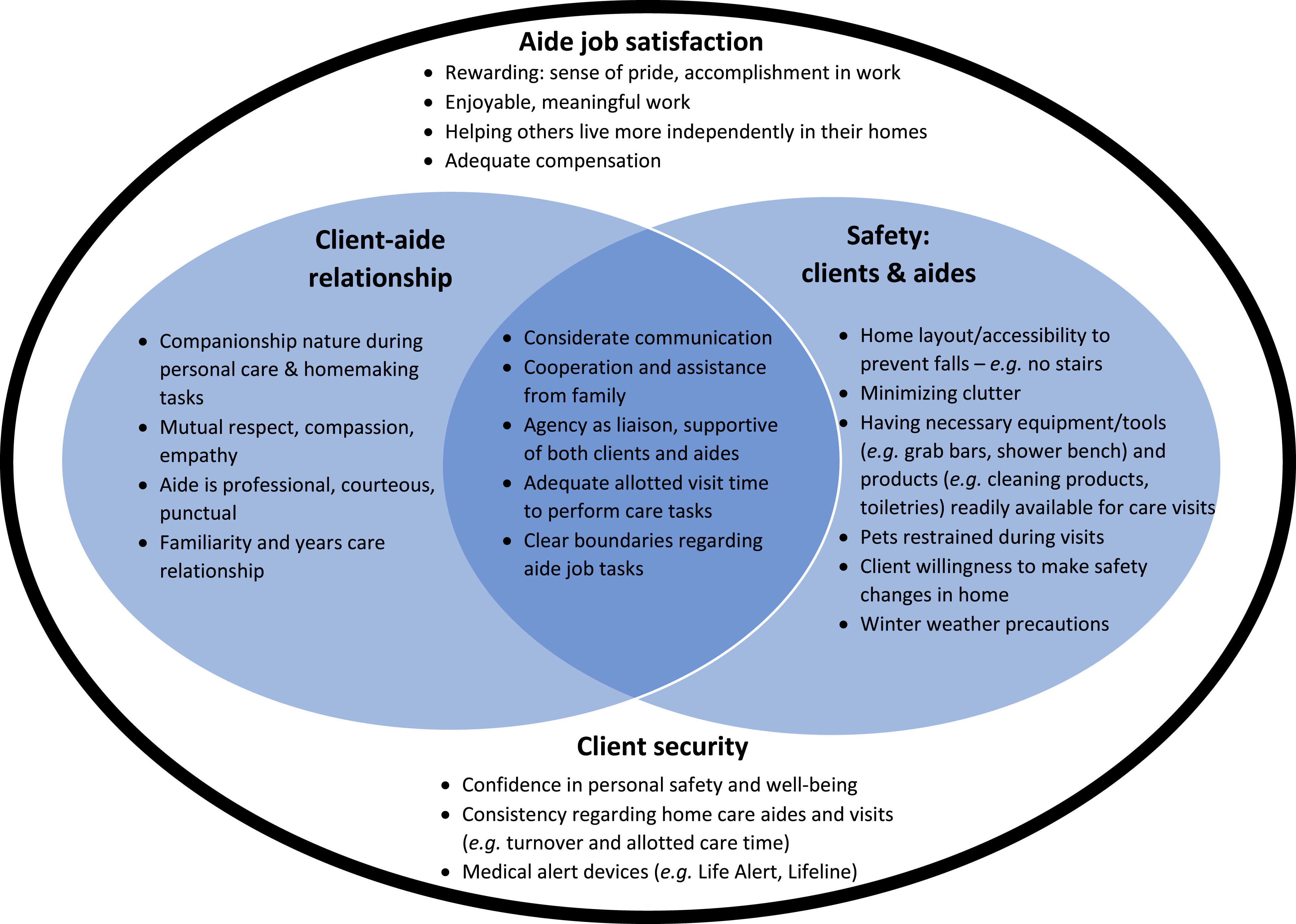
When asked what safety means, one client replied, “mainly being safe, and feeling secure. Safety and security go hand in hand.” (HC client interview #6) Risk of falling was a widely reported safety concern among clients. Many interviewed clients had fallen in their homes (6 out of 9) and reported accessibility concerns throughout their homes. For example, a client specifically identified stairs as a safety hazard: “My fear is falling. That’s my biggest fear in life is to fall … No stairs … I just can’t be any more blunt than that.” – HC client interview #4
When asked what hazards or challenges should be communicated to clients and their families at the start of receiving HC services, nearly half (7 of 16) of aides requested information about risk of falls to be included in a future safety intervention. 1 Four aides said rugs are slip, trip, and fall hazards. Aides also reported that organized, decluttered spaces within the home can make the job easier, and four aides addressed clutter in the home as it contributes to fall risk among clients.
Managers explained that fall risk is evaluated during the initial home visit. Usually, there are quick fixes related to fall prevention that can be addressed during the initial meeting with the client (e.g., remove throw rugs), or safety tools and equipment can be requested from housing authority or family, for example.
Technology may also be helpful; one client identified the sense of security provided by using a medical alert device (e.g., Life Alert, Lifeline). “The other thing is a blessing is I have a Lifeline medallion around my neck … I fell and I hit the alarm and I said, you’re not going to believe this, but I’ve fallen and I can’t get up. We chuckled together and she got me help. So, I wear it all the time. I go to bed with it. So, I have it on [me] constantly.” – HC client interview #3
Physical and Psychosocial Challenges for Aides Working in Home Care
When asked what is challenging while working in HC, nearly half (7 of 16) of aides reported performing care tasks while client’s family was present. These aides reported that a client’s family can become physically or verbally assaultive toward the aide, or not view the aide as a care professional, often instructing the aide how to perform their job or otherwise make the care visit more challenging. “… sometimes it’s family members. They kind of get into the details of the work and give you certain ideas and how to do things, and what to do.” – HC aide interview #1 “Well, the only thing that I have a problem or situation with is some of the client’s homes where the family members are there and they’re basically in my way, [not] allowing me to do my job. I have to wait for someone to get done using the bathroom. I have to wait for someone to get done using the microwave, or I have to wait for someone to finish talking to [the client] and that makes it a little bit difficult for me.” – HC aide interview #4
One aide did highlight the potential to work as a team with client family members, with the common goal of providing safe care for the client. “Sometimes it’s harder when there’s a relative that has a routine. There can be pros and cons. Pros, because if you guys work as a team, it’s going to help the client. Cons because if they’re doing shortcuts that we are not allowed to do, then it becomes a little bit of a problem …” – HC aide interview #12
Other challenges and safety concerns reported by aides included client disposition or declining mobility or health status (n = 5), allotted care time restraints (n = 4), winter weather issues (e.g., ice, snow) (n = 4), and clutter in client homes (n = 3). Two aides specifically mentioned low wages when asked what could be changed to improve the HC job.
According to managers, the most concerning safety hazards in clients’ homes were uncooperative or aggressive client family members (n = 9), clutter or hoarding (n = 8), unsafe conditions (e.g., pest infestation, syringes lying around, exposure to drug paraphernalia, no access to running water, indoor smoking, weapons in the home) (n = 8), and unrestrained pets (n = 8). Client disposition, and cognitive or behavioral issues were mentioned by six managers. Aides being asked to do tasks not part of their job was also considered a safety concern by managers (n = 5).
What Makes the Aide’s Job Easier?
Most clients (6 of 9) reported the installation of low-tech safety tools or durable medical equipment designed to aid in mobility as the most helpful changes in the home for improving safety (e.g., grab bars, bed rails, ramps and stair lifts, shower chairs, non-slip mats, toilet lifts); managers (n = 5) and aides (n = 5) reported that these make aides’ jobs easier. Clients (n = 2) and managers (n = 5) reported having toiletries and personal care supplies readily available (e.g., linens, soaps, cleaning products) and easily accessible for aides to be an important consideration that affects both the client and aide and five aides said readily accessible client care supplies can make it easier to perform their jobs.
Safety Communication and Clients’ Willingness to Make Changes
Communication about Safety
A manager explained that positive aide-client working relationships can allow aides to advocate for safety changes themselves, but was also supportive of aides discussing directly with management if the client is not cooperative (n = 1). Aides (n = 11) often described their clients as willing to make safety changes in the home, and several clients (n = 4) self-reported as being open or receptive to making changes to improve safety. Characteristics of clients that indicated greater likelihood to make changes include client’s health status and physical/mental capability, as well as access to support persons such as family. “I think what makes it safe is an open attitude on the part of the consumer … They have to really be willing to accept the help which is not always easy, especially for older people who are used to doing it themselves. So, an open attitude, the willingness to partner towards a goal … The fact that the consumer no matter what level of care they’re needing, appropriately identifies what they can do to make it safe for the aide …Someone coming in and not knowing your home, you got to be very careful about what you’re inviting people into.” – HC client interview #2
Both aides and managers discussed various strategies used when speaking with clients about necessary or suggested safety changes. Aides reported helpful communication strategies such as direct yet respectful communication with clients, and utilizing other resources such as speaking with managers or client families. Similarly, managers reported a variety of positive communication styles, including open communication, economics discussions, providing choices and opportunity to maintain client autonomy, and involving community, church, or family. Regardless of communication strategy employed, both aides and managers highlighted the importance of a positive working relationship with clients as an indicator of client willingness. Developing a good working relationship built on trust can also make safety discussions easier. “… I usually will encourage whatever the safest option is, but I always let people know that they have a right to make their own decisions about their lives. So I will usually preface it by saying, now, I know you’ve been doing this this way for so long. But I would hate for you to go into the hospital again, so I think it’s a good idea for you to have some grab bars, and here’s how we could get those installed for you. So usually I kind of identify and relate with a client …trying to support as much as possible, but then kind of give my expertise or my opinion on what could be done to prevent any further issues down the line. And usually with me and a good rapport with my clients, and they respect my opinion … get people to kind of come around just by relating to them and speaking openly with them.” – HC manager interview #13 “I think it comes back to the consistency in caregivers. I know that myself being able to make a trusting working relationship with patients allows me some leverage … when I eventually maybe need to make a hard recommendation that I think they may not like or appreciate. They’d be more likely to hear me out and maybe give it a try as opposed to if you have multiple caregivers in the home saying different things and not really able to make a trusting relationship with them.” – HC manager interview #9
A manager discussed the need to work together with aides and clients to accomplish a shared goal of delivering care in a safe environment: “I think a lot of the clients are willing to do what’s necessary within reason, to accommodate what will make the worker safely be able to deliver the services that they need … So for the most part the consumer is open to figuring out, how do we secure the dog, or figure out a way for that grandson to be out of the home for the one hour when the worker goes in from nine to 10, or whatever the case may be, to figure out a solution to make it a safer situation, or more comfortable situation for the aide to go in and be able to deliver the service.” – HC manager interview #3
When asked what can make it easier for an aide to provide safe care to clients, most clients (n = 8) described things they do for their own safety (e.g., limited stairs, having an open attitude), discussed keeping supplies stocked nearby, or misunderstood the question to be about their own personal safety.
Care Relationship between Aides and Clients
Aides reported that respectful relationships with clients (n = 2) and familiarity from years of experience in long-term working relationships with clients (n = 1) make their jobs easier. Eight clients described consistency—receiving care from the same aide—as fundamental to building a trusting relationship. Four clients specifically mentioned punctuality and professionalism as aspects of a positive working relationship. Respectful communication was an underlying theme mentioned by all stakeholder groups. “And also by ensuring privacy with a client … [y]ou have to establish good communication with your clients … it’s going to make the work more easier for you.” – HC aide interview #16
According to most aides (10 of 16), working in HC was rewarding and they enjoyed the satisfaction from helping others, as well as the companionship aspect of the work. Clients often appreciated the relationship with aides. Nearly all (8 of 9) clients reported companionship as one of the best aspects of HC. “… she’ll talk every once in a while and I’ll talk a little while … so that kind of makes the atmosphere very happy, very relaxing and it makes me feel good knowing that someone cares enough to come and help me do the things I can’t do …” – HC client interview #8
An aide described the importance of the companionship aspect of HC, providing clients with a supportive outlet outside of family: “because you become like family … become close … [clients] kind of look forward to seeing us girls. They vent with us about a lot of things. They probably can’t with their own families … I just would like the families to understand how important that moment is for their loved one to have that person that they can confide in, that’s looking out for best interest number one.” – HC aide interview #4
Two managers described the association between aide and client safety. Often, the focus is safety for the client; however, the aide-client relationship is interconnected due to the nature of care tasks. Additionally, making safety changes in client homes affects not only the client and aide but also others in the home. “I think that people just are looking at it from the client’s safety, but it’s the caregiver’s safety that is uber important … I believe they should go hand in hand.” – HC manager interview #1 “… it should [come] from the perspective of the consumer, the client in that whatever the [intervention] recommends is for their safety as well as for the safety of the HC worker. And for the safety of the family members, anybody in the household because if it’s going to impact the HC aide, it’s also going to impact everybody that’s living there.” – HC manager interview #5
Discussion
This study has qualitatively explored the connection between (1) HC aide and client relationship, and (2) aide and client safety (Figure 1). The findings show that both physical (e.g., fall prevention, decluttering) and psychological (e.g., considerate communication, family cooperation) safety in the home-work environment supports the improved job satisfaction of aides. However, not having necessary products and safety tools available for care visits, aggressive family members, unclear job task boundaries, and inadequate care visit times affect aides negatively by making it difficult to provide consistent and safe care to clients, which then triggers the client’s distrust in the care relationship and anxiety about the care continuity.
Physical and psychological hazards affect both HC client and aide safety. Falls were considered the most concerning safety hazard among clients in our study: the risk of falling due to stairs, rugs, and clutter. Both aides and managers felt that challenging family members may hinder safe and effective client care. Aides being asked to do more than is allowed in their HC role were also mentioned by managers. Previous qualitative and quantitative research on HC OSH highlighted these concerns (Markkanen et al., 2014; Quinn et al., 2016), and a recent publication identifies the association between aides being asked to do tasks outside their HC role and risk of experiencing workplace abuse or experiencing pain/injury resulting in lost work time (Karlsson et al., 2020). Educating clients on the impacts of safety for not only their own well-being but also others in the home is needed.
Due to the personal nature of HC tasks, aides often develop a unique working relationship—a care bond—with their clients, based on closeness and trust (Okyere, 2016). A positive aide-client care bond was helpful in conveying safety concerns and influencing client willingness to make safety changes. Evidence suggests that the aide-client care bond can be compromised by variables such as not having the necessary client mobility devices, the presence of uncontrolled pets, exposure to slip, trip, fall hazards, mopping floors, and exposure to feces (Okyere, 2016). Because of the close nature of HC work, aides are often empathetic to client suffering. Additionally, the COVID-19 pandemic highlighted the essential care provided by aides (Guerrero et al., 2020; Markkanen et al., 2021; Osei-Poku et al., 2021; Sama et al., 2021). A noted challenge is the difficulty in expressing compassion due to social distancing practices (Markkanen et al., 2021). The aide-client relationship may be an indicator of job satisfaction and retention (Boone, 2021). Maintaining a positive working relationship is important for opening and maintaining lines of communication of HC safety topics.
Care workers—including homeless shelter workers, school food workers, HC aides, and household cleaners—engage in critical functions that maintain and support societal growth, yet often go without well-deserved recognition (Tsui et al., 2021) while also experiencing impacts to their health (Baron et al., 2022; Sterling et al., 2021). Nationally, direct care workers make efforts to provide quality care yet feel they do not receive adequate recognition for their work (Institute of Medicine (US) Committee on the Future Health Care Workforce for Older Americans, 2008). In our study, many aides reported such challenges with client family members, or were asked to do tasks that were not part of their jobs. A mixed methods assessment of HC aides (n = 1249) highlighted the nuanced client-aide dynamics and blurred boundaries, including an agency manager’s description of an accusation of theft against an aide who went to the bank upon a client’s request (Karlsson et al., 2020). A prior study of this population (n = 1249 aides) found that 40% (n = 502) were asked to do things outside the scope of their job (Quinn et al., 2016). This group also reportedly felt respected (85%, n = 1064) and cited schedule flexibility (63%, n = 781) and independent working structure (60%, n = 747), as well as enjoying the nature of care work (86%, n = 1069), as reasons for continuing to work in their HC jobs (Quinn et al., 2016).
Among 512 home health aides, greater job satisfaction was reported in conjunction with higher degree of control on the job and perceived support from supervisors and the HC agency (Gleason & Miller, 2021). One way to promote a degree of control and sense of management support is to consult and include HC aides in care-related communication, as they are integral parts of the care team with valuable first-hand observations during client care (Paraprofessional Healthcare Institute, 2021). While aides generally report high job satisfaction, they face economic strains, including low wages and high turnover (Quinn et al., 2021). It is challenging for HC workers to financially support themselves and their families with low wages combined with part-time working hours—median hourly wages were $13.02 in 2020, and annual median earnings were $27,080 (Bureau of Labor Statistics, 2021; Paraprofessional Healthcare Institute, 2020). Urgent focus is needed on improving job quality to fulfill the demand for HC caregivers in the coming years (McCall, 2021).
Results from this Massachusetts-based study may not be generalizable nationwide to populations of HC workers and recipients. The researchers were not minorities, nor were they employed in HC.
Conclusions
Safety education of clients and their families could improve HC aide safety and job satisfaction and serve as a strategy to promote aide workforce retention. To promote HC aide job satisfaction, stakeholders must consider improving and promoting both (a) client-aide relationships, and (b) safety of both clients and aides.
Supplemental Material
Supplemental Material - Aide and Client Safety “Should go Hand-In-Hand”: Qualitative Findings From Home Care Aides, Clients, and Agency Leaders
Supplemental Material for Aide and Client Safety “Should go Hand-In-Hand”: Qualitative Findings From Home Care Aides, Clients, and Agency Leaders by Natalie M. Brouillette, Pia K. Markkanen, Margaret M. Quinn, Catherine J. Galligan, Susan R. Sama, John E. Lindberg, and Nicole D. Karlsson in Journal of Applied Gerontology
Supplemental Material
Supplemental Material - Aide and Client Safety “Should Go Hand-In-Hand”: Qualitative Findings From Home Care Aides, Clients, and Agency Leaders
Supplemental Material for Aide and Client Safety “Should Go Hand-In-Hand”: Qualitative Findings From Home Care Aides, Clients, and Agency Leaders by Natalie M. Brouillette, Pia K. Markkanen, Margaret M. Quinn, Catherine J. Galligan, Susan R. Sama, John E. Lindberg, and Nicole D. Karlsson in Journal of Applied Gerontology
Footnotes
Acknowledgments
This publication was funded by the National Institute for Occupational Safety and Health of the Centers for Disease Control and Prevention grant number R01 OH008229. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention. The Safe Home Care Project research team members appreciate the time and effort of the participating provider agencies and elder services agencies that collaborated to recruit home care aides and clients to the study. The authors express their gratitude to all home care aides who enrich many lives throughout the USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute for Occupational Safety and Health/Centers for Disease Control and Prevention [grant number R01 OH008229].
Research Ethics
The University of Massachusetts Lowell Institutional Review Board (IRB) approved all study protocols and materials: approval number 19–112-QUI-XPD. All study procedures were followed in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. In addition to the IRB, the Massachusetts Elder Rights Review Committee reviewed and approved all client phone interview methods and materials. All study participants provided signed informed consent to participate prior to in-person focus group or interview participation. Electronic or verbal consent procedures were applied to phone interviews. All of these informed consent procedures were approved by the same University of Massachusetts Lowell IRB that approved the entire study.
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.