
Abstract
Providing home and community-based services (HCBS) is critical for active and healthy aging. However, in China, the positive factors for improving HCBS provision are unclear, limiting its contribution to improving older adults’ quality of life and promoting active and healthy aging. Therefore, this study examines the configurations that produce differences in HCBS and identifies multiple pathways for improving them and narrowing regional disparities. Using data from multiple datasets comprising 23 cases, we performed configuration analysis using fuzzy-set qualitative comparative analysis. Four pathways producing high HCBS provision and three pathways producing low HCBS provision were found. Different combinations of the aging population, economic development, institutional support, financial support, and development of multiple stakeholders influence HCBS provision. Thus, measures based on the main factor characteristics should be implemented to improve the HCBS provision level.
Keywords
• The development of multiple stakeholders, institutional support, economic development, financial support, and the aging population affect HCBS provision in China. • Policies and measures related to these factors can improve HCBS provision in China.
• fuzzy-set qualitative comparative analysis is suitable for exploring improvement pathways for the provision of HCBS. • The study findings can provide a reference for improving policies on HCBS.What this paper adds
Applications of study findings
Introduction
Population aging is increasing worldwide and critically requires aging care services. Home and community-based services (HCBS) can improve aging care services and are preferred by many older adults (above 60 years) (Yan, 2019; Yu et al., 2021). HCBS can match the preference of most older adults to receive aging care services at home or in the community through targeted services (Feng et al., 2020). Furthermore, compared with other aging care services, HCBS is a closer-to-home and lower-cost alternative to institutional aging care for older adults (Yan, 2019). HCBS can fulfill the diverse needs of older adults through providing assisted living, healthcare services, and social support (Yan, 2019; Yu et al., 2021), and improve their quality of life (Pepin et al., 2016). Therefore, providing HCBS is essential for active and healthy aging, and reduces inequalities in aging care among regions.
HCBS provision is a complicated indicator, including input and output considerations, which can reflect HCBS development as influenced by economic status, older adults’ needs, financial subsidies, and policy support (Yan, 2019). HCBS is widely utilized in some Western countries such as Denmark and the United States. China has made some progress in expanding HCBS. The Chinese government has implemented several HCBS-related policies since 2000 (including Opinions on Comprehensively Promoting the Work of Home Care Services (2008), Opinions on Carrying out Pilots for the Reform of Home and Community-based Services (2016)), with the number of centrally issued HCBS-related policies rising from 3 in 2000 to 80 in 2020 (Ministry of Civil, 2020). Government subsidies encouraged the spread of HCBS centers, which rose by 8.96 times between 2016 (26 HCBS pilots) and 2020 (203 HCBS pilots) (Ministry of Civil, 2021). In addition, HCBS provision per capita (number of older adults with HCBS offered/total number of older adults) has risen from 0.58 in 2008 to 1.86 in 2018 (Yu et al., 2021).
Although HCBS provision in China is improving in many specific aspects, no study exists on the provision and regional disparities of HCBS in China. HCBS provision relates to HCBS input and output levels in a region (Shao et al., 2021; Zhou et al., 2022). However, overall HCBS provision in China remains lower than expected (Feng et al., 2020). Some studies contend that HCBS coverage is narrow, and some of the services are insufficient in content and accessibility and cannot effectively meet older adults’ needs (Feng et al., 2020; Yan, 2019), which is contrary to the equity and efficiency principle emphasized by the safety net. Research data have shown that only 14.1% of older adults are provided with assisted living services (Zhang et al., 2022), while 69.18% of older adults need assisted living services (CLHLS, 2018). Furthermore, the number of HCBS beneficiaries in China has remained relatively small; of 264 million older adults in 2020, 31.04 million older adults above 80 years of age enjoyed an allowance, and only 5.35 million received an aging care service subsidy (including cash payment to older adults, and an actual service provided by the government). Additionally, disparities in HCBS provision across regions remain significant (Weaver & Roberto, 2020), limiting its impact on improving older adults’ quality of life. Therefore, understanding pathways to improve HCBS provision and narrow the disparities across regions is necessary.
Extant literature on factors influencing HCBS provision remains relatively scarce; only single factors such as state economic status, financial subsidies, policy support, or volunteers have been investigated (Muramatsu et al., 2010; Yan, 2019; Yu et al., 2021; Zhou et al., 2022). HCBS emerged not through a single factor but as a combination of many factors, such as economic development and financial support. However, while existing studies on HCBS and its provision cannot explain the configurations of different HCBS provisions, fuzzy-set qualitative comparative analysis (fsQCA) can detect combinations of causal conditions that lead to outcomes.
Therefore, using fsQCA, this study aimed to (1) explore the configurations that lead to different levels of HCBS provision and analyze the reasons for these configurations, (2) identify multiple pathways for narrowing disparities in HCBS provision among regions and provide suggestions to help improve this provision.
Conceptual Framework
The fsQCA requires a theoretical framework as the basis for conditions selection (Ragin, 1987). The first step in fsQCA is to establish a theoretical model and select appropriate conditions and outcome variables according to the research problem (Ragin, 1987; Ragin, 2008b).
In the following section, we draw on welfare pluralism, new public management, social development impetus, and social needs theories, which are typically considered in the field of public service provision, to guide the theoretical development of factors influencing HCBS provision.
Welfare pluralism theory contends that rules, financing, and the provision of welfare need to be jointly undertaken and implemented by different departments, rather than restricted to a single government department (Weisbrod, 1986). The provision of welfare products can derive from many sources: the government, families, profit organizations, nonprofit organizations, and voluntary institutions. HCBS is a type of social welfare. Thus, it is universally acknowledged that a “welfare mix,” including the government, nonprofit organizations, volunteers, private provisions, and families, must be considered when providing HCBS. Older adults in need are the primary beneficiaries of HCBS. At the same time, older adults in good health could become one of the main providers of HCBS in terms of supporting other older adults as volunteers or in other ways. The government, as the service provider, is responsible for formulating the corresponding rules and policies of HCBS, with a grasp of the macro development direction.
New public management theory holds that, in public service provision, the government should act in terms of “steering rather than rowing” (Ferlie, 2017), implying that the government must guide the provision and future direction of public services. Additionally, new public management theory advocates a competition mechanism, allowing more private sector agencies to participate in the provision of public services (Willis et al., 2018). HCBS emphasizes the role of political design in practice. The government can guide subordinate departments and service providers to provide services by formulating relevant policies in the practice process of HCBS.
Social development impetus theory proposes that institutional factors are vital for the development of society (Bob, 1990). Institutional factors refer to the forms and mechanisms adopted by political organizations and society to integrate and standardize the behavior of individuals to achieve social goals. Furthermore, it holds that the economy is the fundamental cause and core driver of social development (Bob, 1990). As a public service, HCBS provision usually needs financial support for development. Researchers have illustrated that economic development can affect the provision of public and aging care services (Beauregard & Miller, 2021), and that the government should provide subsidies and investments to both providers.
Social needs theory refers to the physical, psychological, economic, and cultural requirements of human beings for survival and well-being, as well as the collective needs of society (Adalbert, 2005). Social needs for older adults concern basic needs that should not be ignored (Millar, 2005). In terms of HCBS, social need refers to older adults’ need for HCBS in the aging care process (Feng et al., 2012). HCBS service providers should accurately provide targeted services by focusing on the needs of older adults (Yan, 2019).
Integrating the above theories and literature, we identified factors that could explain the causal complexity involved in HCBS provision (see Figure 1). Two conditions—development of multiple stakeholders and financial support—were chosen for this study based on welfare pluralism theory. We selected the development of multiple stakeholders, institutional support, and the aging population as conditions in accordance with new public management theory. Economic development, institutional support, and financial support were selected as research conditions based on social development impetus theory. The aging population was chosen as one of the factors for HCBS provision based on social needs theory. This framework indicated that the development of multiple stakeholders, institutional support, economic development, financial support, and the aging population is critical to HCBS provision. Among them, the aging population and economic development are external environmental factors, which are difficult to change within a short period, whereas institutional and financial support and the development of multiple stakeholders are internal factors that can be improved through measures in a shorter timeframe. Conceptual framework of HCBS provision.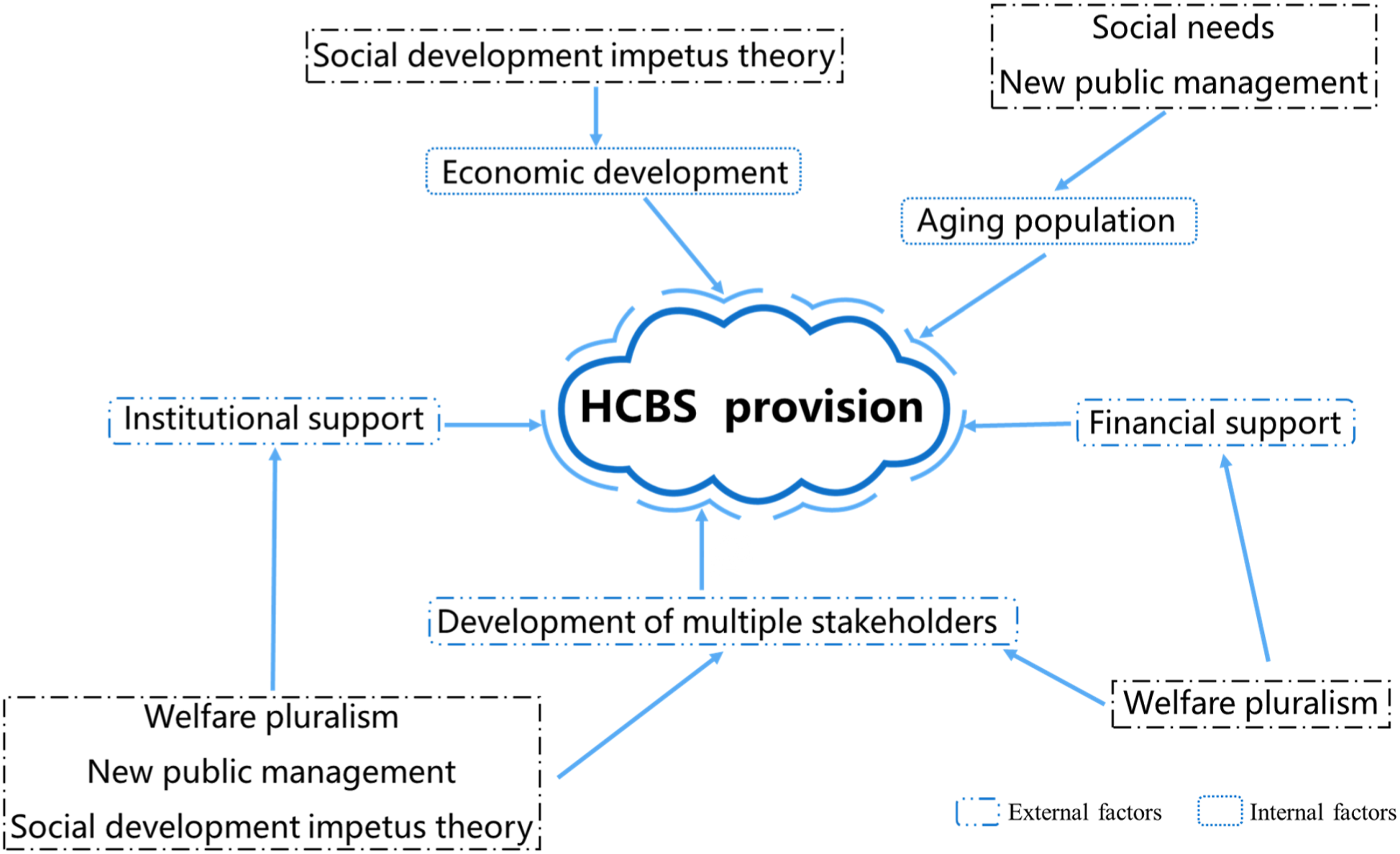
Fuzzy-Set Qualitative Comparative Analysis
The fsQCA was created as a type of qualitative comparative analysis (Ragin, 1987). Based on Boolean algebra minimization algorithms, fsQCA was designed to help researchers analyze and understand complex causal relationships (Ragin, 1987; Ragin, 2000). With the core idea of “all roads lead to Rome,” fsQCA can describe all the possible solutions and configurations that explain the outcome (Ragin, 2008a). However, fsQCA has not been applied to HCBS. Thus, in this study as noted, we used fsQCA to explore the pathways to improve HCBS provision and narrow disparities in HCBS provision among regions.
Method
Data Source and Case Selection
As a single dataset contains limited variables, we used multiple datasets to better depict HCBS provision and its impacting factors, namely, the Chinese Longitudinal Healthy Longevity Survey (CLHLS), China Civil Affairs Statistical Yearbook (2021), China Statistical Yearbook (2021), National Bureau of Statistics, and China Market Index Database. Along with the CLHLS, other datasets included in our study covered all the provinces in China. Therefore, we chose 23 provinces from the CLHLS as our cases, based on the breadth of data.
Outcome and Causal Conditions
As our primary interest was to identify the configurations that lead to different levels of HCBS provision, HCBS provision was chosen as our outcome variable. Based on previous studies (Rouyendegh et al., 2019; Shao et al., 2021; Zhou et al., 2022), we explored HCBS provision in terms of input and output in this study. As the quality of HCBS provision is difficult to measure, we chose only the quantity of HCBS provision. It is generally agreed that the input dimension of HCBS provision includes human resources, hardware facilities (e.g., the number of beds and aging care centers), and financial and service management (Rouyendegh et al., 2019; Vongxaiburana et al., 2011). Prior studies have calculated the service provided and coverage for older adults as the output dimension of HCBS provision (Meyer et al., 2021).
Five causal conditions were selected in this study: the aging population, institutional support, economic development, financial support, and development of multiple stakeholders.
The outcome and five causal conditions consisted of several sub-indicators, and we used the entropy weight method to calculate the corresponding variables. Finally, each variable was assigned a score. See Supplementary files 1 and 2 for specific indicators, weight, and data sources.
Analysis
The fsQCA was conducted using fsQCA 3.0 software, which contains calibration and truth tables for necessary and sufficiency analyses.
Calibration
Calibration is an essential step in fsQCA, which involves assigning a value to a variable from 0 to 1 and defining if and in what amount a case belongs to this group (Pappas & Woodside, 2021). A score of 1 means that the case is completely in the set, 0 means that it is completely out of the set, and 0.50 means that it is at the mid-point in the set; these three anchors are called full membership, full non-membership, and the cross-over point, respectively (Ragin, 2018). Depending on different data types, researchers can choose different thresholds for calibration. As this study’s data were not normally distributed and were skewed left, we finally decided on 80%, 50%, and 20% as full membership, the cross-over point, and full non-membership, respectively. We added 0.001 in all the casual conditions after the calibration, ensuring that no case assigned 0.50 was deleted.
Truth Table Analysis
A truth table was used to list all possible combinations of the causal conditions. Truth table algorithm analysis was based on only relevant combinations. As per previous studies, we selected 1 as the frequency cut-off. Following recent fsQCA research and guidelines, we set the raw consistency threshold as 0.80 and the proportional reduction in inconsistency (PRI) as 0.70.
Necessary Analysis
Necessary analysis examines if a condition is necessary for an outcome. We analyzed the necessity of the presence and absence of each condition for the two opposite results (high and low HCBS provision).
Sufficient Analysis
Sufficiency analysis is also called configuration analysis. It is used for analyzing the configurations that lead to the outcomes. We conducted a sufficiency analysis for both high and low provision of HCBS.
Sensitivity Analysis
Sensitivity analysis is critical for examining results’ stability. Many optional robustness analysis methods for fsQCA can be used for sensitivity analysis, such as changing the calibration (Fiss, 2011), changing the consistency levels (White et al., 2021), and dropping or adding cases (Park et al., 2020). In this study, we conducted several sensitivity analyses. First, we changed the PRI consistency from 0.70 to 0.75 and 0.80. Second, we tested for various raw consistency thresholds in accordance with prior research (White et al., 2021), specifically, 0.72, 0.75, 0.76, and 0.85. Third, we altered the calibration to 15%, 50%, and 85% for testing.
Results
Results of Descriptive and Calibration Analysis
Descriptive Statistics and Calibration of the Conditions.
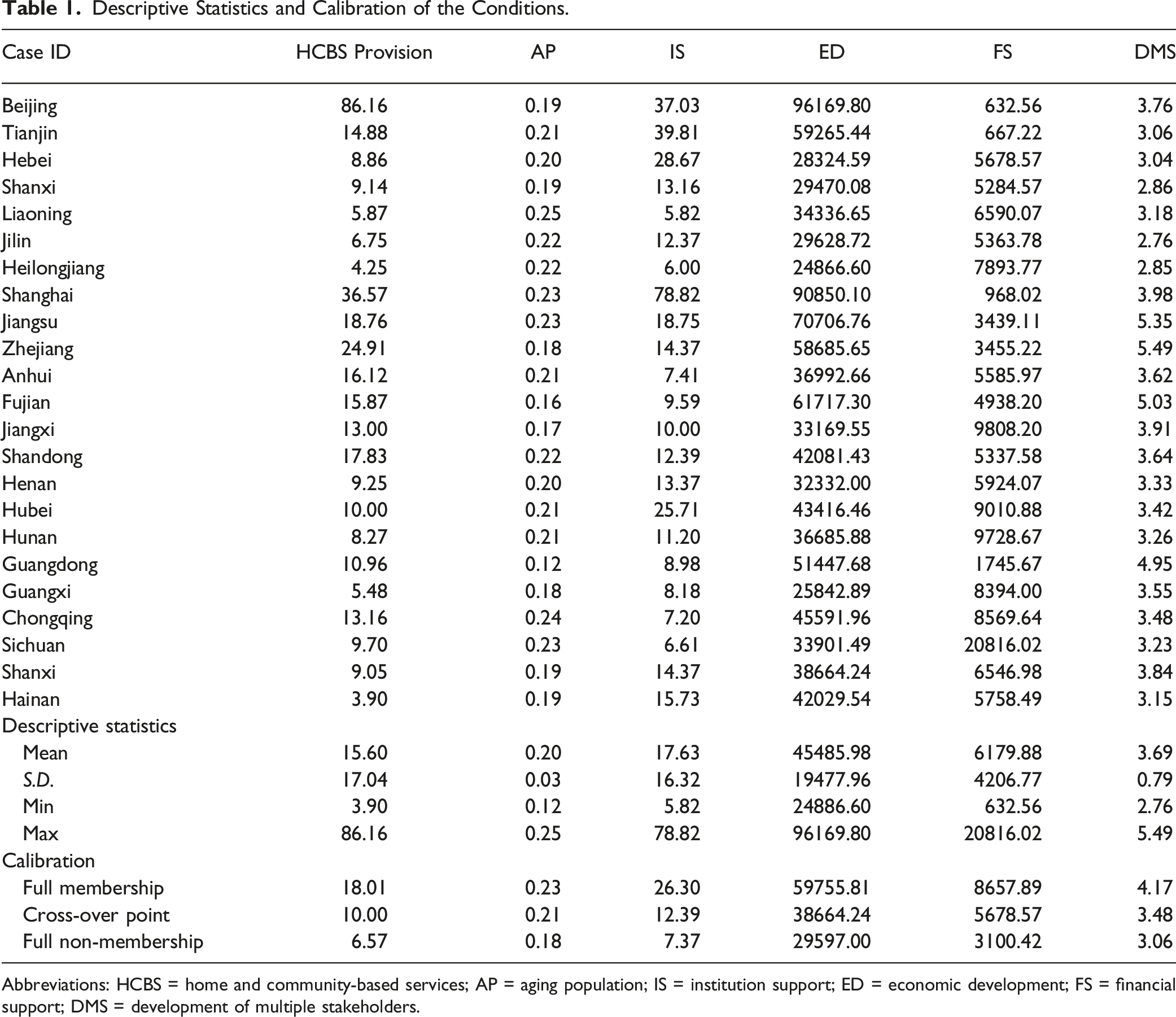
Abbreviations: HCBS = home and community-based services; AP = aging population; IS = institution support; ED = economic development; FS = financial support; DMS = development of multiple stakeholders.
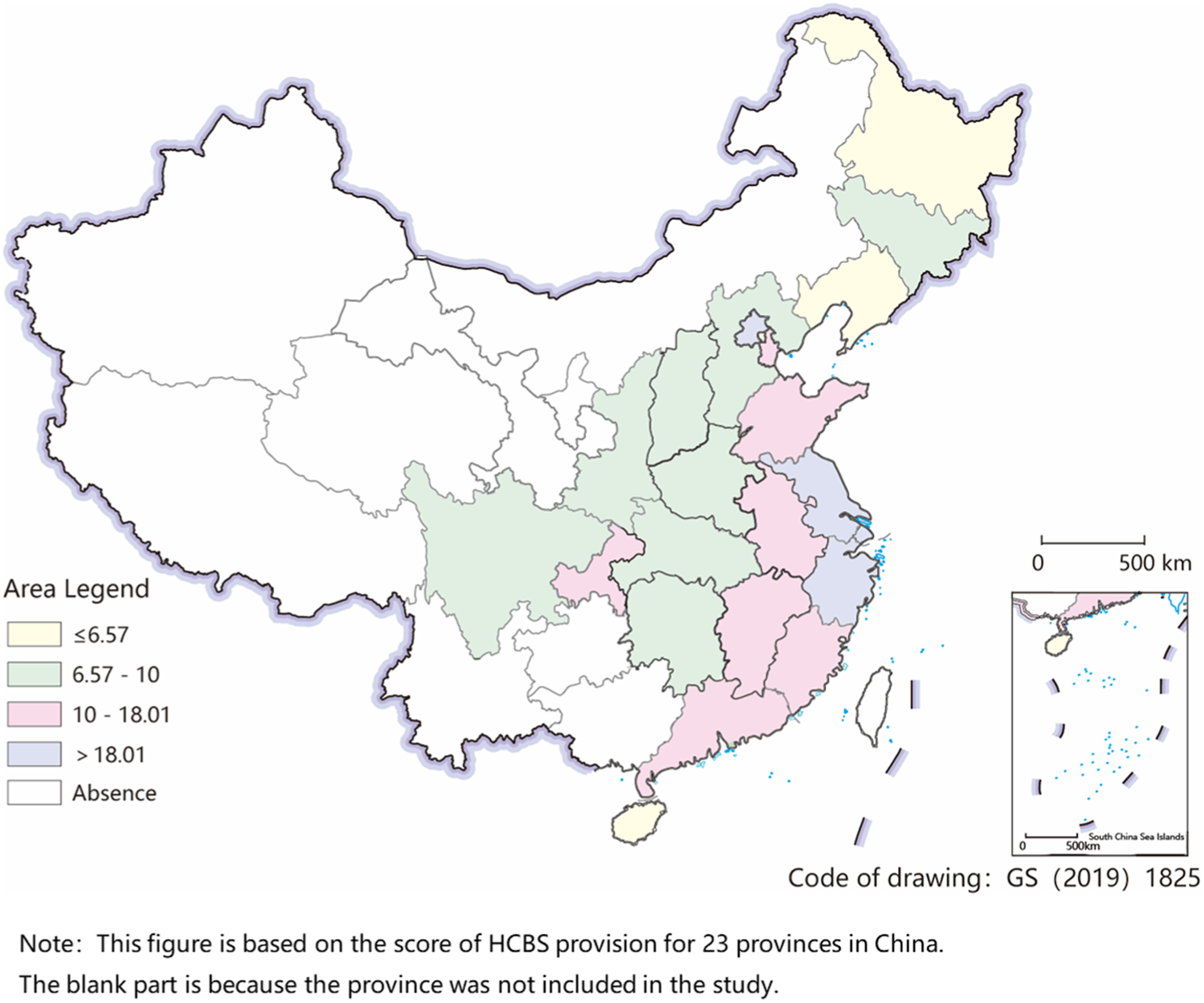
HCBS provision in 23 provinces in China.
Results of the Truth Table
We first obtained 25 rows reflecting all possible combinations of causal conditions. The 1s and 0s indicated full membership and zero membership for each condition, respectively. After selecting the threshold, we finally obtained 14 rows for the following analysis.
Results of the Necessary Analysis
Analysis of Necessary Analysis.
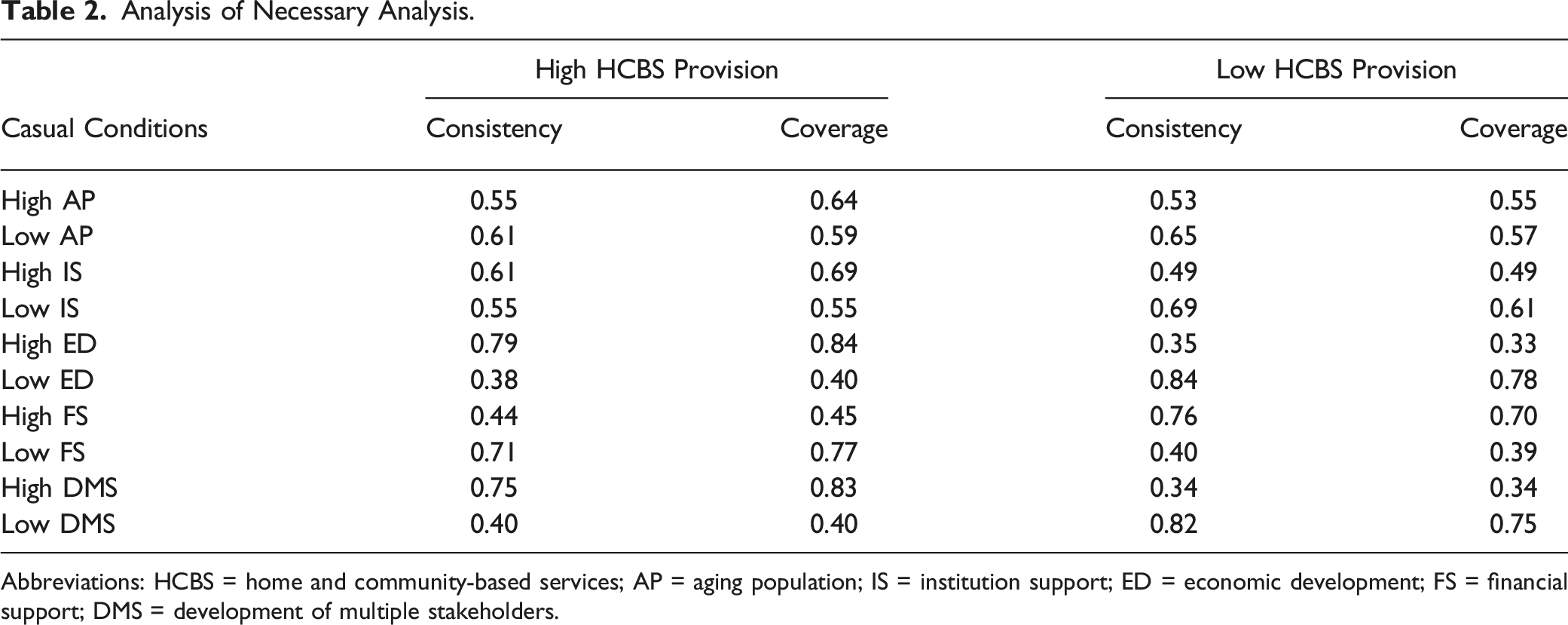
Abbreviations: HCBS = home and community-based services; AP = aging population; IS = institution support; ED = economic development; FS = financial support; DMS = development of multiple stakeholders.
Results of the Sufficiency Analysis
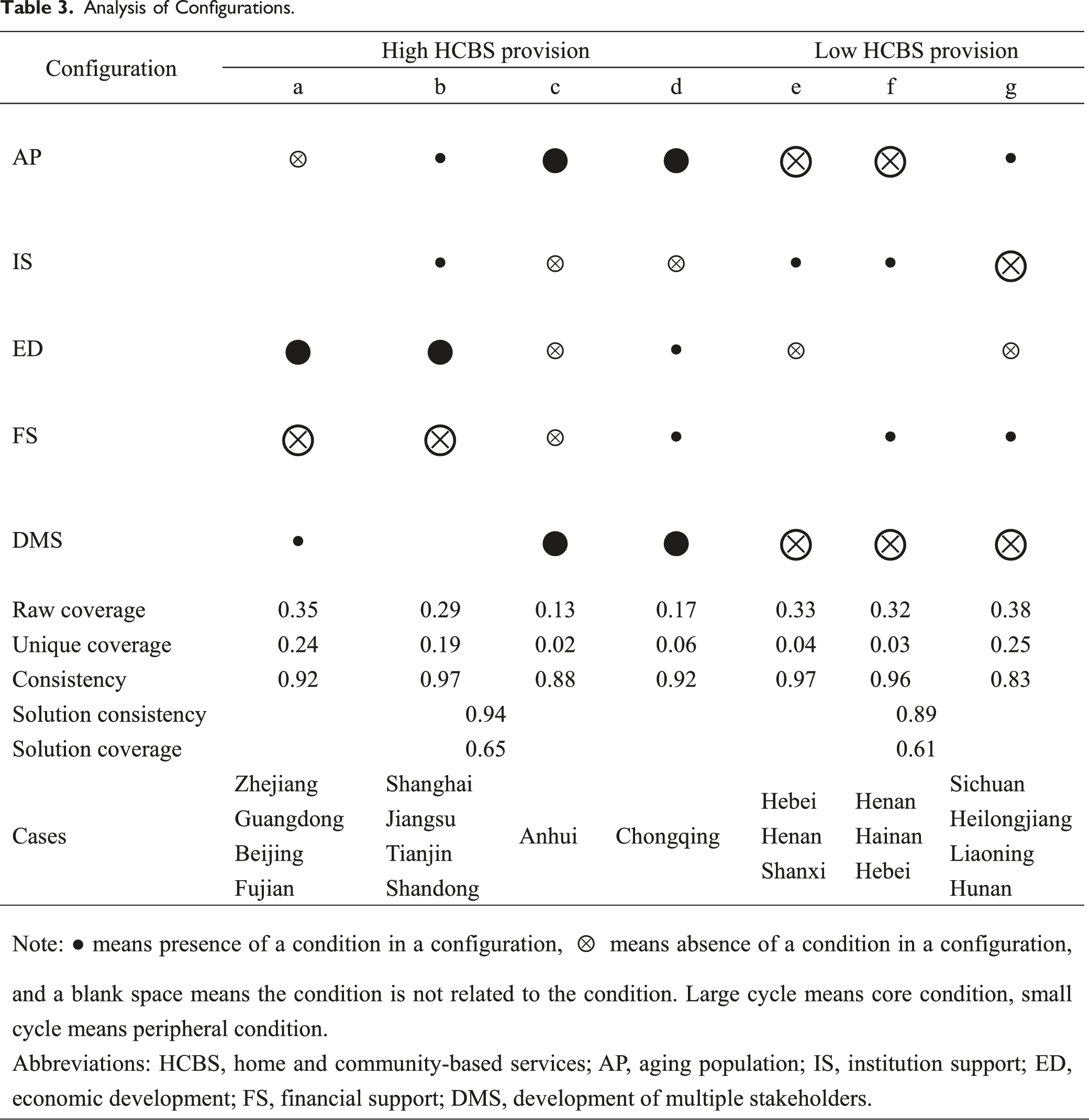
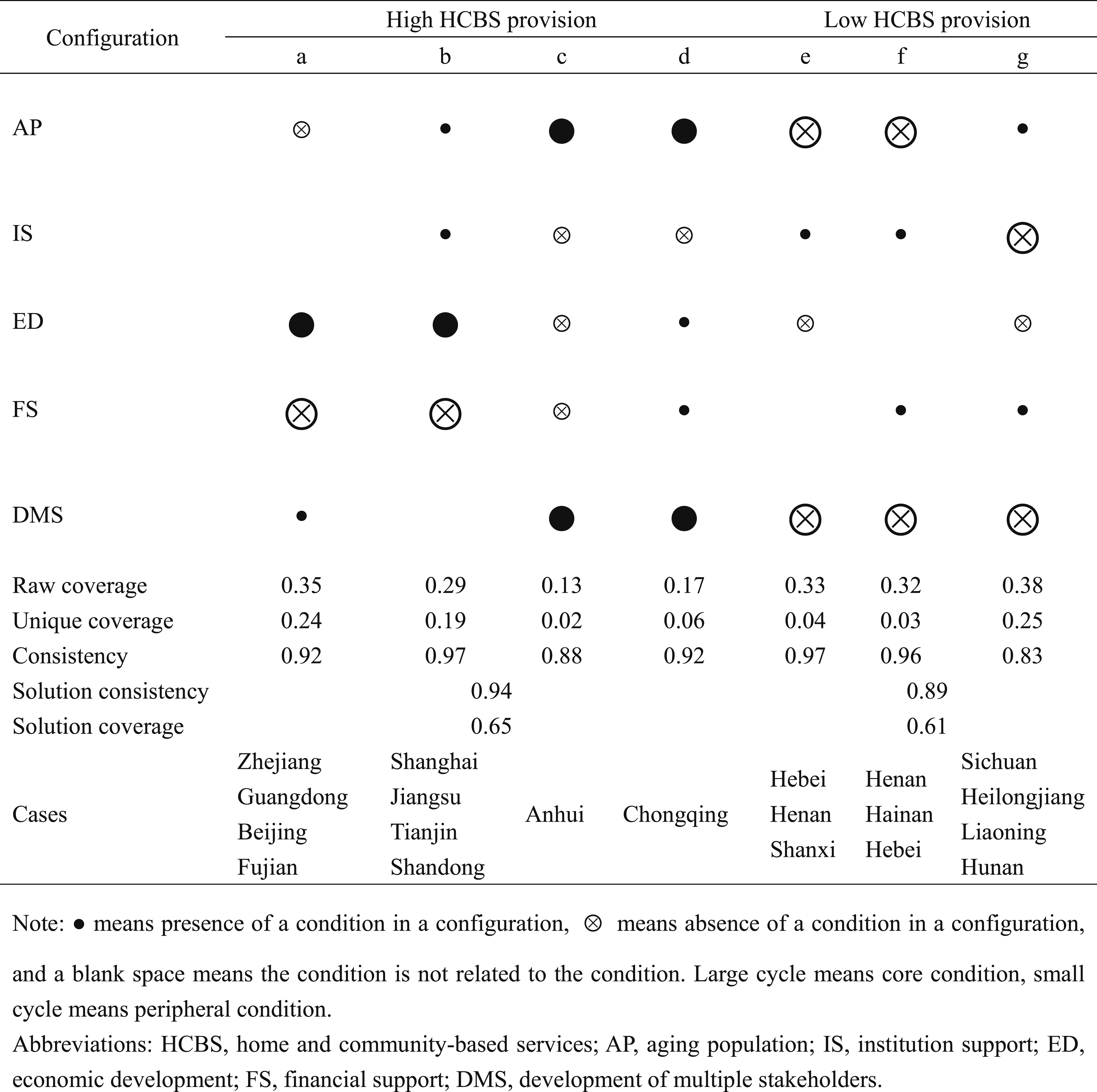
Analysis of Configurations.
Configurations for High HCBS Provision
The results showed four configurations leading to a high HCBS provision, which can explain 65% of cases in this study, with a high overall solution consistency of 0.94. Because of the same core conditions, configurations a and b and configurations c and d constituted second-order equivalent configurations.
Economic Factor-Oriented Type
Configurations a and b showed the same combination of core conditions. Economic development was the present core condition for both, and financial support was the absent core condition. Furthermore, for configuration a, the aging population was the absent peripheral condition, and the development of multiple stakeholders was the present peripheral condition. The raw coverage of configuration a was 0.35, with a high consistency of 0.92, covering 24% of provinces that had high HCBS provision. The cases included in configuration a were Zhejiang, Guangdong, Beijing, and Fujian. For configuration b, both the aging and institutional support were the present peripheral conditions for high HCBS provision. Configuration b covered 19% of cases among high HCBS provision provinces, including Shanghai, Jiangsu, Tianjin, and Shandong, with a raw coverage of 0.29 and a very high consistency of 0.97.
Multiple Stakeholder-Oriented Type
Configuration c and configuration d showed the same core present and absent peripheral conditions for a high HCBS provision. The aging population and development of multiple stakeholders were present core conditions, and institutional support was an absent peripheral condition in configurations c and d. Economic development level and financial support were absent peripheral conditions in configuration c but present peripheral conditions in configuration d. Configuration c covered only Anhui among the provinces with high HCBS provision, with a consistency of 0.88 and raw coverage of 0.19. Additionally, configuration d contained only Chongqing, with a raw coverage of 0.17 and consistency of 0.92.
Configurations for Low HCBS Provision
The results indicated that three configurations led to a low HCBS provision, which could explain 61% of cases comprising the outcome with an overall solution consistency of 0.89. Configurations e and f were conducted with a second-order equivalent configuration due to the same core conditions.
Multiple Stakeholder-Absence Type
Configurations e and f presented the same core absent conditions for low HCBS provision, specifically, aging and development of multiple stakeholders. Furthermore, institutional support was the present peripheral condition in both solutions. Economic development was the absent peripheral condition in configuration e, and financial support was the present peripheral condition in configuration f. Both configurations e and f had high consistency at 0.97 and 0.96, respectively. The raw coverage of configurations e and f was 0.33 and 0.32, respectively. Configuration e covered 4% of cases that had low HCBS provision, namely, Hebei, Henan, and Shanxi. Additionally, configuration f included Henan, Hainan, and Hebei, covering 3% of cases among low HCBS provision.
Institutional-Absence Type
Configuration g indicated that institutional support and development of multiple stakeholders were absent core conditions for low HCBS provision. In contrast, the aging population and financial support were present peripheral conditions, and economic development was an absent peripheral condition. The raw coverage of configuration g was 0.38, with a consistency of 0.83, covering 25% of cases; the cases were Sichuan, Heilongjiang, Liaoning, and Hunan.
Results of Sensitivity Analysis
Three methods were chosen for sensitivity analysis. All results remained substantively unchanged, and all solutions were logically substitutable (see Supplementary file 3). There were four pathways for high HCBS provision and two pathways for low HCBS provision in sensitivity analysis A (PRI = 0.75/raw consistency threshold = 0.85). The solution consistency for high and low HCBS provisions was .94 and 0.97, respectively. The solution coverage for high and low HCBS provisions was 0.65 and 0.36, respectively. Three pathways and two pathways for high and low HCBS provisions, respectively, were shown in sensitivity analysis B (PRI = 0.80). The results revealed a solution consistency of 0.94 and 0.97 for high and low HCBS provision, respectively. The results of sensitivity analyses A and B were subsets of the main results, indicating that this study’s results were robust. Sensitivity analysis C (raw consistency thresholds = 0.72/0.75/0.76) and D (calibration = 15%, 50%, 85%) showed the same results, namely, four pathways and three pathways for high and low HCBS provisions, respectively, with 0.94 and 0.65 for the solution consistency for high HCBS provision and the solution coverage, respectively. The same results were observed among sensitivity analyses C and D, and in the main results of our study, indicating that this study’s results are robust.
Discussion
This study’s results showed that: (1) high economic development could contribute to a high HCBS provision; (2) the combination of the aging population and development of multiple stakeholders could lead to changes in the HCBS provision; and (3) the absence of institutional support could generate low HCBS provision. The aging population and economic development are external environmental factors that affect HCBS provision. Nevertheless, they are not the focus of HCBS policies and are difficult to substantially alter in the short term. Institutional support and the development of multiple stakeholders are internal factors significantly affecting HCBS provision and can be changed substantially by implementing adequate measures over a short period.
High Economic Development Can Contribute to a High HCBS Provision
Social development impetus theory proposes that the higher the regional economic development level, the more available resources for HCBS are, and the more HCBS can be promoted. Beijing, the capital of China, has abundant resources and opportunities, making it a leading area in terms of socio-economic development and HCBS. In this study, Beijing had the highest economic development (1/23) and the highest degree of HCBS provision (1/23). Furthermore, increased economic development can lead to a higher level of HCBS management, which can improve the distribution of resources and quality of supervision, gradually improving HCBS provision (Yan, 2019).
Meanwhile, the development and expansion of HCBS may put more pressure on the government budget, which depends mostly on economic development. According to the Organization for Economic Co-operation and Development (OECD) database, Luxembourg, Ireland, and the United States rank high in GDP per capita (OECD, 2022a), and the development of HCBS in these countries is better than it is in other countries.
Combination of an Aging Population and the Development of Multiple Stakeholders Can Lead to Changes in HCBS Provision
Population aging is an objective tendency in population growth that is difficult to change and normally has to be accepted. However, it is possible to proactively address the increased need for HCBS caused by aging populations. Based on the match of supply and need, it is vital to consider both the needs of older adults and multiple providers. HCBS provision requires older adults’ needs to be the motivating reason for supplying HCBS, under the value of “person-centered” services. Escalating population aging increases the demand for diversified, multi-level, and individualized aging care services, prompting providers to invest resources to improve HCBS provision. Thus, population aging is an essential factor that should be considered during HCBS provision (Meinow et al., 2005).
Moreover, according to welfare pluralism theory, multiple stakeholders represent a crucial factor that cannot be ignored in promoting HCBS provision. High-welfare states, such as Demark, Sweden, and Norway, have a high aging population (OECD, 2022c). Concurrently, the development of social organizations and the organization of volunteers are more advanced in those countries than in most Asian and African countries. In America and England, multiple stakeholders are also in a more highly developed state (OECD, 2022d, OECD, 2022b, OECD, 2022e). The combination of a high aging population and high development of multiple stakeholders in these countries generates the high HCBS provision, mainly in terms of HCBS coverage.
With the ability to plan and implement an extensive program, efficient achievement of required deliverables and HCBS objectives become possible (Callens et al., 2021). However, what governments can do for public services is limited (Davis et al., 2019), and HCBS is not the only public service they must provide. Therefore, it is important to invite more stakeholders to engage with the provision and development of HCBS. Multiple stakeholders would enable improvement in the availability of human and infrastructure resources for HCBS (Callens et al., 2021), along with the range of services furnished, which in turn would improve HCBS provision.
Absence of Institutional Support Can Generate a Low Provision of HCBS
As a type of public service, HCBS is primarily policy-driven and institutional path-dependent (Andrews et al., 2019). Institutional and policy support can guide and promote HCBS in terms of financial incentives, basic service standards, facilities operations, equipment, and service management and supervision (Feng et al., 2020; Mu et al., 2022). The OECD countries have developed policies to encourage HCBS (Feng et al., 2020). Accordingly, Canada, Ireland, Sweden, and Poland have expanded HCBS for older adults living in their homes and communities (Feng et al., 2020). Casady (2021) pointed out that spending on public services and infrastructure depends on a country’s supportive policies. The support of leadership and a favorable policy environment are critical to the success of public projects (Casady, 2021). Using financial incentives, such as increasing public funding, insurance coverage, and cash benefits, Sweden, Austria, the United Kingdom, and other OECD countries have expanded HCBS and improved its utilization (Francesca et al., 2011). By raising eligibility criteria, Finland and Hungary have promoted the quality of HCBS (Francesca et al., 2011). Without strong policy inducements like those described above, it is difficult for HCBS to expand (Feng et al., 2020).
China has major regional differences, and it is difficult for the central government to introduce policies that suit every province; the government can only provide guidance in policy formulation. Therefore, the provinces in China must introduce more detailed policies to assist in HCBS policy implementation, based on local conditions (Feng et al., 2012). While policies on operational advice are relatively sparse and unspecific, HCBS may face operational hurdles and challenges (Feng et al., 2020). Although the Chinese government has implemented policies for promoting HCBS, provision across provinces remains sporadic, with a shallow provision of benefits (Feng et al., 2012). Current policies are derived mainly from a national level and have not been implemented successfully because of a lack of information and suitable supporting policies, such as determining the appropriate type and quantity of HCBS that must be provided, as well as the sufficient level of financial subsidies required for HCBS. In some provinces, such as Sichuan, Heilongjiang, Liaoning, and Hunan, HCBS provision remains below expectations, owing to insufficient institutional support and a lack of resources and infrastructure, similar to that reported in African countries. Because of institutional and policy flaws, it is difficult to develop HCBS adequately.
Contributions and Limitations
To the best of the authors’ knowledge, this is the first study to examine the configurations leading to different HCBS provisions using fsQCA. This study provides a new perspective showing that different pathways can improve HCBS provision. Furthermore, the findings can help policymakers and practitioners to gain confidence in taking incremental steps toward greater access to HCBS, especially from the perspective of internal factors, including institutional support and the development of multiple stakeholders. Moreover, this study’s results can also provide a reference for other countries and territories that aim to push or promote HCBS internally.
However, our study has certain limitations. First, this study only researched the configuration effect of factors that lead to different HCBS provisions in China. Further studies should include more countries for international comparisons. Second, owing to sampling limitations in the CLHLS, this study could only cover 23 Chinese provinces. Further studies should include more provinces based on data availability. Owing to the limited sample size, the conditions were also limited. In the future, more cases should be included in relevant studies to enrich research results and provide further possible pathways to improve HCBS provision. Furthermore, this study included only the quantity of HCBS provision because of the difficulty in measuring its quality. Future studies should consider the quality of HCBS provision, using accessible data.
Conclusion
This study showed that different combinations of an aging population, institutional support, economic development, financial support, and the development of multiple stakeholders can influence HCBS provision. Policies and measures related to these factors can improve HCBS provision in China.
Based on this study’s results, we propose the following strategies. More possibilities for the development of HCBS should be explored. As the main factors that influence HCBS provision are both internal and external, targeted measures should be implemented based on the influencing factors’ characteristics. Concerning internal factors such as institutional support and the development of multiple stakeholders, some intervening actions could be promoted to improve HCBS provision in the provinces considered in this study. First, the government should develop more policies concerning HCBS at a granular level, especially supportive policies, including types, prices, hours, beds, infrastructure, and supervision of HCBS. Second, more stakeholders should be encouraged to involve themselves in the construction of HCBS. Concerning external environmental factors, although the current situation cannot be changed easily, positive measures could be taken to improve HCBS provision. For provinces with higher rates of population aging, older adults’ specific needs should be considered, using evaluation tools such as questionnaires and interviews. This can help address the perceived gap between rising demand and limited provision of HCBS, promote the overall provision of HCBS, and gradually narrow the gaps in HCBS provision among regions.
Supplemental Material
Supplemental Material - Pathways to Improve Provision of Home and Community-Based Services—A Configurational Approach Based on a Fuzzy-Set Qualitative Comparative Analysis From China
Supplemental Material for Pathways to Improve Provision of Home and Community-Based Services—A Configurational Approach Based on a Fuzzy-Set Qualitative Comparative Analysis From China by Yunyun Huang, Rujia Zhang, Qianru Zhao, Xiaoyi Wang, Lizheng Ge, Songjia Zhang, Qingren Yang, Chenkai Zhang, Xiangyang Zhang, and Chun Chen in Journal of Applied Gerontology.
Footnotes
Author Contributions
YYH and RJZ drafted the manuscript, designed the study, and conducted the literature review. QRZ, XYW, and SJZ collected the literature. QRY and CKZ collected the data. XYZ and CC designed the original version of plans. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Natural Science Foundation of China [72274141], Zhejiang Provincial Natural Science Foundation [LY22G030006], Key Project of Science and Technology Department of State Administration of Traditional Chinese Medicine - Zhejiang Administration of Traditional Chinese Medicine [GZY-ZJ-KJ-23084], Zhejiang Office of Philosophy and Social Science, China [22NDJC104YB].
Data Availability Statement
The authors confirm that all data is contained within the manuscript and its ![]() .
.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.