
Abstract
A social pension, regarded as a reliable source of income, has the potential to significantly influence the overall wellbeing of vulnerable older adults. This study aimed to extend the understanding of the effects of social pension expansion beyond its economic impacts to encompass recipients’ health status. Using three-wave data from a representative sample of older adults, we employed a quasi-experimental assessment model to evaluate the impact of a recent social pension expansion in Hong Kong on health-related consumption and health outcomes among older adults. The results of the triple difference estimations revealed that an increased social pension significantly enhanced older people’s engagement in entertainment activities, utilization of healthcare services, and expenditures on preventive health products. Furthermore, the increased social pension was found to have a significant positive effect on mitigating poor self-rated health and poor sleep quality. However, it did not have a significant impact on the prevalence of depression. These findings suggest that social pension expansion should be coordinated with other policy initiatives to comprehensively improve the physical and mental health of older adults.
Keywords
• This study provides compelling evidence of the impact of social pension expansion on health-related consumption and mental and physical health outcomes. • It presents a vivid narrative that illustrates the response of older adults in the personal health domain when a non-generous social pension benefit experiences a substantial increase.
• The findings suggest that expanding and strengthening social pension programs is a worthwhile endeavor, particularly in non-welfare economies that prioritize the health-related wellbeing of older adults. • Social pension expansion can be effectively combined with other policy interventions, forming a comprehensive multicomponent framework to promote the overall health and wellbeing of older adults.What this paper adds
Applications of study findings
Introduction
Social pension refers to a tax-funded scheme that provides regular monetary payments to older individuals, supporting their financial needs during retirement. The research framework surrounding social pension encompasses four dimensions: program design and features (Larsen & Munk, 2020), targeting mechanisms (Cruz-Martínez, 2019), financial sustainability (Mesa-Lago et al., 2022), and impact evaluation (Lee et al., 2019; Mostert et al., 2022). Impact evaluation is a crucial component, particularly for non-welfare economies that plan to significantly expand social pension programs in response to population aging and the need for financial security in old age. These expansions are driven by specific policy objectives, such as reducing poverty, improving income equality, promoting population health, enhancing social stability, or stimulating consumption. Impact evaluations play a vital role in determining whether social pension expansions achieve their intended policy objectives, thereby guiding future reforms of social pension schemes in these economies.
A review of the literature reveals that many impact evaluations focus on understanding the effects of social pension on economic and poverty indicators (Ferreira, 2006; Kang et al., 2022; Lee, 2022; Lee et al., 2019). Policymakers are particularly interested in exploring whether more generous social pension benefits lead to the undesirable “crowding-out” effect, where income of older adults from other sources, such as employment or family transfers, is reduced. However, global evidence from rigorous experimental designs provides reassurance that the crowding-out effect is minimal, and social pension expansions have been found to significantly improve household income, reduce poverty rates in old age, and increase household expenditures (Ebbinghaus, 2021; Ferreira, 2006; Kang et al., 2022; Lee, 2022; Lee et al., 2019; Long & Pfau, 2009).
In addition to economic and poverty indicators, recent research has also examined the effects of social pension expansion on various aspects of physical and mental health, showing encouragingly positive impacts. However, most of the available studies have focused on older populations in mainland China and South Korea (Cheng et al., 2018; Hwang & Lee, 2022; Pak, 2021; Pan et al., 2021; Yuan et al., 2022), highlighting the need for more evidence from the international community to better understand the impact of social pension expansion on the health status of older individuals. In response to this call, our study examined the effects of a social pension reform in Hong Kong, involving a substantial increase in monthly benefit amounts, on multiple health-related outcomes among older adults using a three-wave longitudinal observation. The experiences and findings from Hong Kong’s social pension reform can serve as a valuable reference for other no-welfare aging economies with similar plans to expand their social pension programs.
Social Pension Reform and Health of Older People: Theoretical Explanations of Social Pension Expansion and Health-relatedConsumption
The life cycle theory proposed by Ando and Modigliani (1963) provides a framework for understanding the link between social pension expansion and health-related consumption. According to this theory, individuals are rational consumers who plan their finances throughout different stages of life. In an ideal scenario, people actively manage their income and expenses, saving for retirement and ensuring financial security (Bodie et al., 2008). In old age, individuals can rely on their accumulated assets for consumption, leading to a relaxed and worry-free lifestyle. Social pension expansion in this context provides additional income beyond life-cycle financial planning. Older adults, already financially secure, are motivated to spend the additional income without concerns about future expenditures, as they perceive their finances to be well-managed until the end of their lives.
Even though older adults have not saved sufficiently during their working years, social pension expansion still has the potential to boost expenditures. Older individuals make consumption decisions based on accumulated wealth, current income, and expected income for the remainder of their lives (Holt, 1995). Social pensions, funded by taxes, are viewed by recipients as a sustainable and permanent income resource in old age. This restructuring of life-cycle financial planning leads to an increased social pension being interpreted as an asset yet to be fully utilized, with its value increasing as longevity is anticipated. Consequently, recipients of social pensions are motivated to increase spending, particularly in personal health investments, to prolong their lives and maximize the benefits of the pension scheme. This may include increased expenditures on entertainment activities, healthcare services, and preventive health products, such as fitness equipment, dietary supplements, and regular health check-ups.
Health-related Consumptions and Health Outcomes
Existing biomedical social science literature highlights the beneficial components of cultural and entertainment activities, including creative expression, aesthetic pleasure, sensory activation, emotional evocation, and social interaction (Dunphy et al., 2019). Engaging in these activities improves mental health by reducing inflammation and stress hormones, promoting positive mood, and enhancing self-esteem (Bone et al., 2022; Lu, 2011; Wion et al., 2021). Similarly, the use of healthcare services and consumption of preventive health products among older adults have been shown to have positive effects on physical health, such as improved lung function and memory (Aguila et al., 2015; Tse et al., 2014). Furthermore, social pensions may create economic incentives for older adults in lower social classes to leave risky and physically demanding work before retirement, resulting in improved health outcomes after escaping stressful work environments (Kuhn, 2018).
This Study
Given the potential path from social pension expansion to improved physical and mental health outcomes through health-related consumption, this research aimed to evaluate the impacts of a social pension reform on various outcome variables. Specifically, we examined the effects of the social pension reform on engagement in entertainment activities, utilization of healthcare services, and consumption of health products as indicators of health-related consumption. Additionally, we assessed three outcome variables related to physical and mental health: self-rated health, sleep quality, and depression. While recent studies have established the positive effects of social pension expansion on the health outcomes of older adults (Cheng et al., 2018; Hwang & Lee, 2022; Pak, 2021; Pan et al., 2021; Yuan et al., 2022), these investigations have not sufficiently explored the mechanisms through which social expansion promotes health status. This research incorporated health-related consumption as an outcome variable, shedding light on the potential role of health-related consumption in mediating the impact of social pension expansion on health outcomes among older people and indication a direction for future research.
Background of Social Pension Reform in Hong Kong
The poverty rates among older adults aged 65 and above in Hong Kong were alarmingly high, with 21.4% experiencing income-based poverty in 2017 (Cheung & Chou, 2019). This figure was much higher than the average income-based poverty rate of 12.5% among the Organization for Economic Co-operation and Development (OECD) countries in the same year (OECD, 2017). Recognizing the urgent need to alleviate poverty among the older population, the Hong Kong government prioritized strengthening social pension schemes.
Social pension schemes in Hong Kong consist of three main components: (1) Old Age Living Allowance (OALA), which is means-tested and targets individuals aged 65 and above; (2) comprehensive Social Security Assistance (CSSA), which is means-tested but has stricter household asset and income limits and provides higher benefits; and (3) the Old Age Allowance (OAA), which is provided universally to individuals aged 70 and above but offers the lowest allowance. Older people are eligible to participate in only one of these schemes.
The Eligibility and Benefit of Comprehensive Social Security Assistance, Old Age Allowance, Old Age Living Allowance and Higher Old Age Living Allowance.
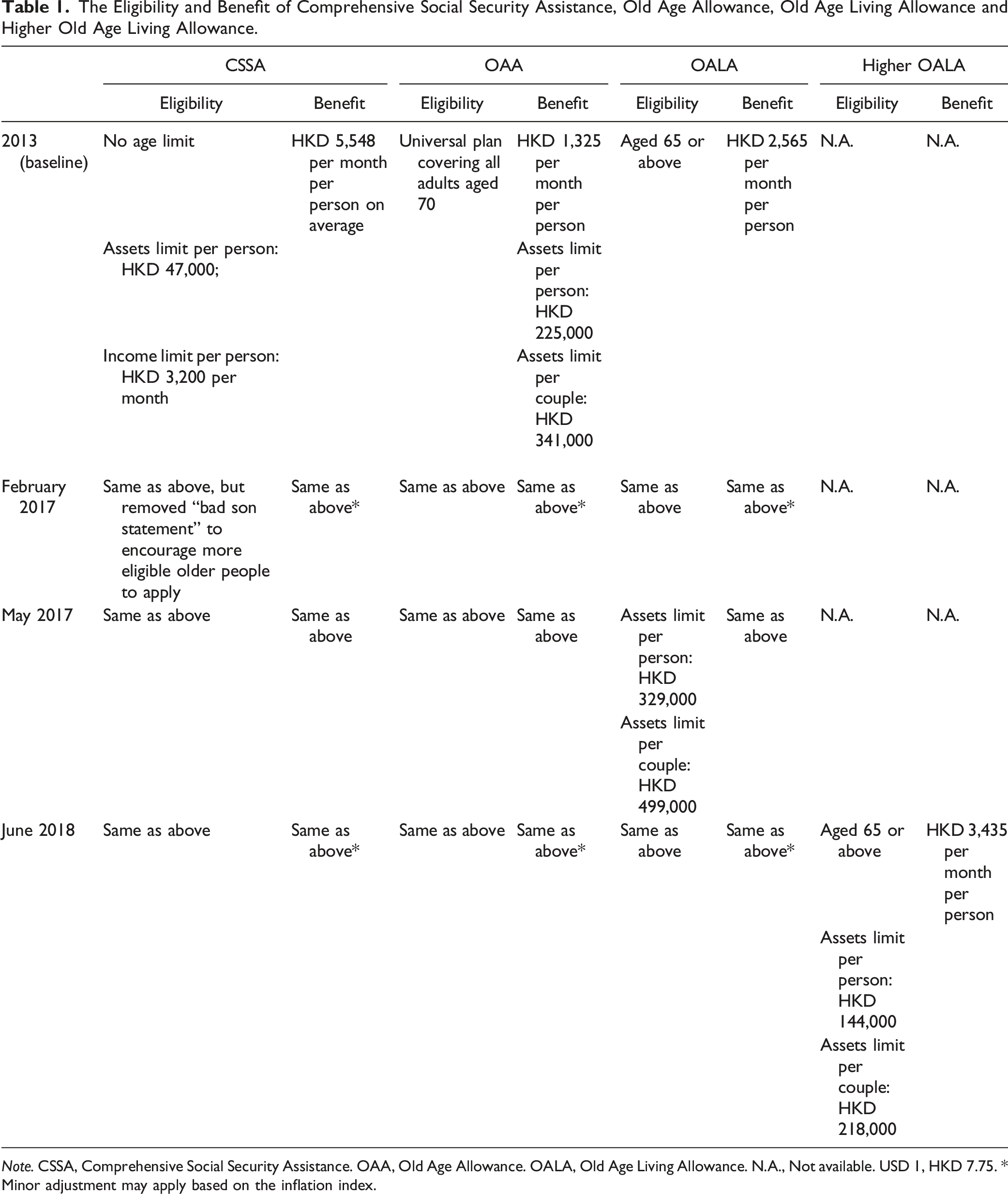
Note. CSSA, Comprehensive Social Security Assistance. OAA, Old Age Allowance. OALA, Old Age Living Allowance. N.A., Not available. USD 1, HKD 7.75. * Minor adjustment may apply based on the inflation index.
In February 2017, the government eliminated a requirement from CSSA that forced older individuals living apart from their children to submit a “bad son statement,” which was a declaration stating that their adult children were not providing financial support (see Table 1). This reform aimed to remove social stigmatization from the policy and encourage eligible older individuals to apply for CSSA benefits.
In May 2017, the government relaxed the asset limit for the OALA scheme (see Table 1), extending the coverage of OALA. Furthermore, starting from June 1, 2018, the government introduced a new tier to the existing OALA scheme, known as the higher OALA. This new tier offered a monthly allowance that was 50% higher than the previous one but imposed stricter asset limits (see Table 1). These reforms provided a natural experimental setting to assess the effects of expanding the social pension scheme on consumption patterns among older adults in Hong Kong.
This study focused on the implementation of the higher OALA in 2018 as the experimental condition and evaluated its impact on six outcome variables related to health-related consumption and health outcomes. These variables included engagement in entertainment activities, utilization of healthcare services, consumption of health products, self-rated health, sleep quality, and depression. By examining these outcomes, the study aimed to provide valuable insights into the effects of social pension expansion on the consumption behavior and health outcomes of older adults in Hong Kong.
Method
Procedure
The target population for this study consisted of Hong Kong residents aged 60 or above. In 2015, we obtained a large sample list of living quarters from the Census and Statistics Department based on their Register of Quarters and Register of Segments. Using a stratified sampling design based on geographical areas and types of quarters, we confirmed our target sample of living quarters (see Figure 1). This sampling framework provided a powerful approach to generate a sample that could be representative of the general population in Hong Kong. After excluding vacant households and households without an older member aged 60 or above, we successfully visited 2,817 households in 2015 and conducted face-to-face structured interviews. The older participants for the interviews were selected based on the last birthday rule. Ethical approval was obtained from The Education University of Hong Kong three months prior to data collection. Before the formal interview, a mini-test consisting of ten questions was conducted to assess the memory of the older participants. If an older participant failed to pass the memory test, a family member was invited to answer questions on their behalf after obtaining the participant’s approval. To ensure interrater reliability, a research assistant was appointed to supervise and monitor all face-to-face interviews. Cash coupons were provided to older participants as an incentive for completing the interviews. Sampling framework and sample.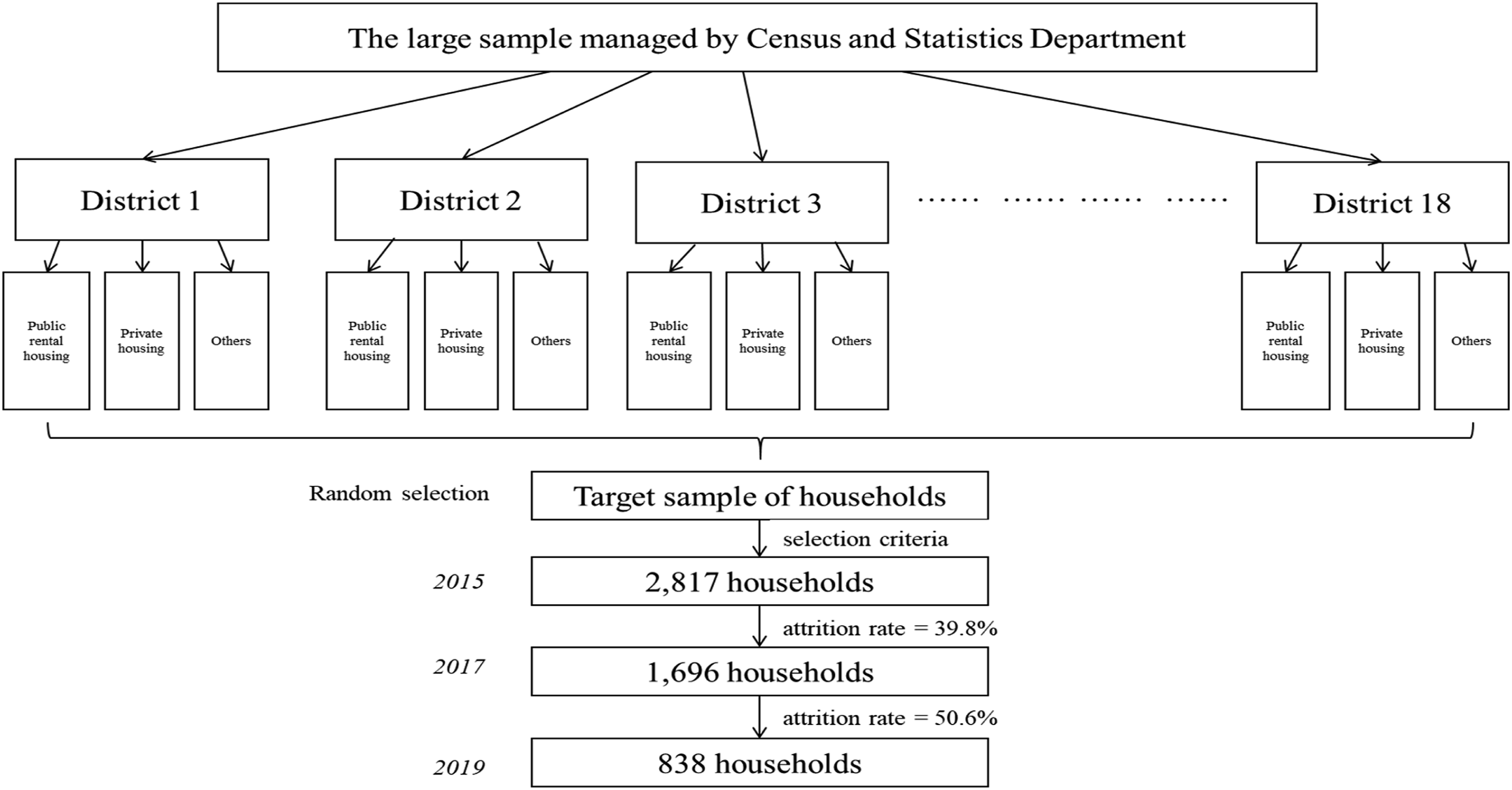
The second wave of data collection took place two years later, in 2017, with the aim of including the same participants interviewed in the first wave. A total of 1,696 participants were successfully interviewed for a second time. The third wave of data collection occurred in 2019, one year after the implementation of the higher OALA. We approached all the older participants who had been included in wave two and successfully interviewed 838 of them. These participants who were involved in all three waves of data collection (N = 838) constitute the three-wave sample used in this study.
Measures
Engagement in entertainment activities was measured using five items adapted from the English Longitudinal Study of Ageing (ELSA) (Barnes et al., 2006). The items included “going to the cinema,” “visiting an art gallery or museum,” “going to the theatre, concert or opera,” “going to a restaurant, café, or pub,” and “traveling in Mainland China or overseas.” Participants rated the frequency of their engagement on a 5-point scale, ranging from 1 (less than once a year) to 5 (equal to or more than twice per month). The Cronbach’s Alpha values across the five items in the three waves were .73, .73, and .67, respectively. The score for engagement in cultural and entertainment activities in each wave was calculated as the mean of the five items.
Utilization of healthcare services was assessed by asking participants to report the number of doctor visits they had in the last six months. This included general outpatient services, inpatient services, specialist services (e.g., Ophthalmology, Otolaryngology), Chinese medicine, dentist visits, and physiotherapy. Participants were also asked to report their total expenditures on preventive health products, including body checks, physical fitness equipment, and dietary supplements in the last month. The total amounts were adjusted for inflation and expressed in 2019 Hong Kong Dollars.
Poor sleep quality was assessed using a single item. Respondents were asked to report how often they felt refreshed after sleep on a four-point scale (1 = never; 4 = most of the time). The responses were reverse-coded to reflect poor sleep quality. Self-rated health was measured using a five-point scale, with older participants asked to describe their general health (1 = very good; 5 = very poor). Those reporting a score of “4” or “5” were identified as having poor health status.
Symptoms of depression were assessed using the 15-item Chinese Geriatric Depression Scale (GDS)-Short Form, a validated tool for measuring depression among older adults in Hong Kong (Yesavage et al., 1982). Each item on the scale reflected a specific depressive symptom. Participants were asked to indicate whether they experienced each of the 15 symptoms, with response options of 1 for “Yes” and zero for “No.” The depression scores were calculated as the sum of the 15 items.
To classify participants as either depressive or non-depressive, we used a cut-off value of 7, as suggested by Cheng et al. (2010) for identifying depressive older adults in Hong Kong. Participants in our sample were categorized as either depressive (coded as 1) if their depression score exceeded the cut-off, or non-depressive (coded as 0) if their score fell below the cut-off.
Data Analysis
The group assignment in this study required careful consideration. There are two viable options for defining an experimental group, as outlined by Lee et al. (2019). One approach is to assign older participants who meet the eligibility criteria for the treatment to the experimental group at the pretest stage. Alternatively, the group assignment can be conducted at the posttest stage by assigning older participants who have already benefited from the treatment to the experimental group.
Given the potential endogeneity of defining an experimental group at the posttest level, where individual choice may contaminate group selection (e.g., through false declaration when applying for the higher OALA), we opted for group assignment at the pretest stage. We assigned participants who were eligible for the higher OALA but not eligible for the CSSA based on their assets threshold in 2015 to the experimental group. Other participants in the sample were assigned to the control group. We chose assets as the criterion for group assignment instead of income because assets are a more stable economic indicator across the three waves of data collection.
The different economic status between the experimental group and the control group led us to consider the triple differences (DDD) approach instead of the classical difference in difference (DD) for our evaluation (Blundell & Dias, 2009; Lee et al., 2019). To implement the DDD approach, we created two higher-order years: ‘2015–2017’ and ‘2017–2019’. Within these higher-order years, we calculated the DDs. We designated 2015 as the first pretest time and 2017 as the first posttest time, representing the counterfactual situation without policy intervention, to define the first DD. Subsequently, we set 2017 as the second pretest time and 2019 as the second posttest time to define the second DD. The DDD was then determined as the difference between the two DDs, representing the deviation of the residual common trend between the two groups and indicating the effect of the policy intervention (i.e., the higher OALA).
In our analysis, we modeled the DDD as a triple interaction term in multiple linear regression estimations (or linear probability regression). This approach incorporated important covariates such as gender, age group, number of close adult children, household size, economic status (earning income or not), and housing type. The triple interaction term was calculated as the product of group status (experimental or control group), time (pretest or posttest), and higher-order year (2015–2017 or 2017–2019). The coefficient of the triple interaction in the regression model indicated the effect of the higher OALA.
Results
Based on our grouping strategy, which involved assigning eligible participants for the higher OALA but not eligible for the CSSA based on their assets threshold in 2015 to the experimental group, we excluded certain individuals from the analysis to ensure the accuracy of our estimates of DDDs. Specifically, we excluded those who received CSSA in 2017 and 2019 in the experimental group (N = 36 in 2017 and N = 24 in 2019), those who received OAA (N = 95) or ordinary OALA (N = 72) in both groups in 2019, and those who received the higher OALA in the control group in 2019 (N = 126). This was done to prevent their potential influence on the estimation of DDDs. The exclusion of these participants resulted in a final three-wave sample size of 489 participants.
Attrition Analysis.
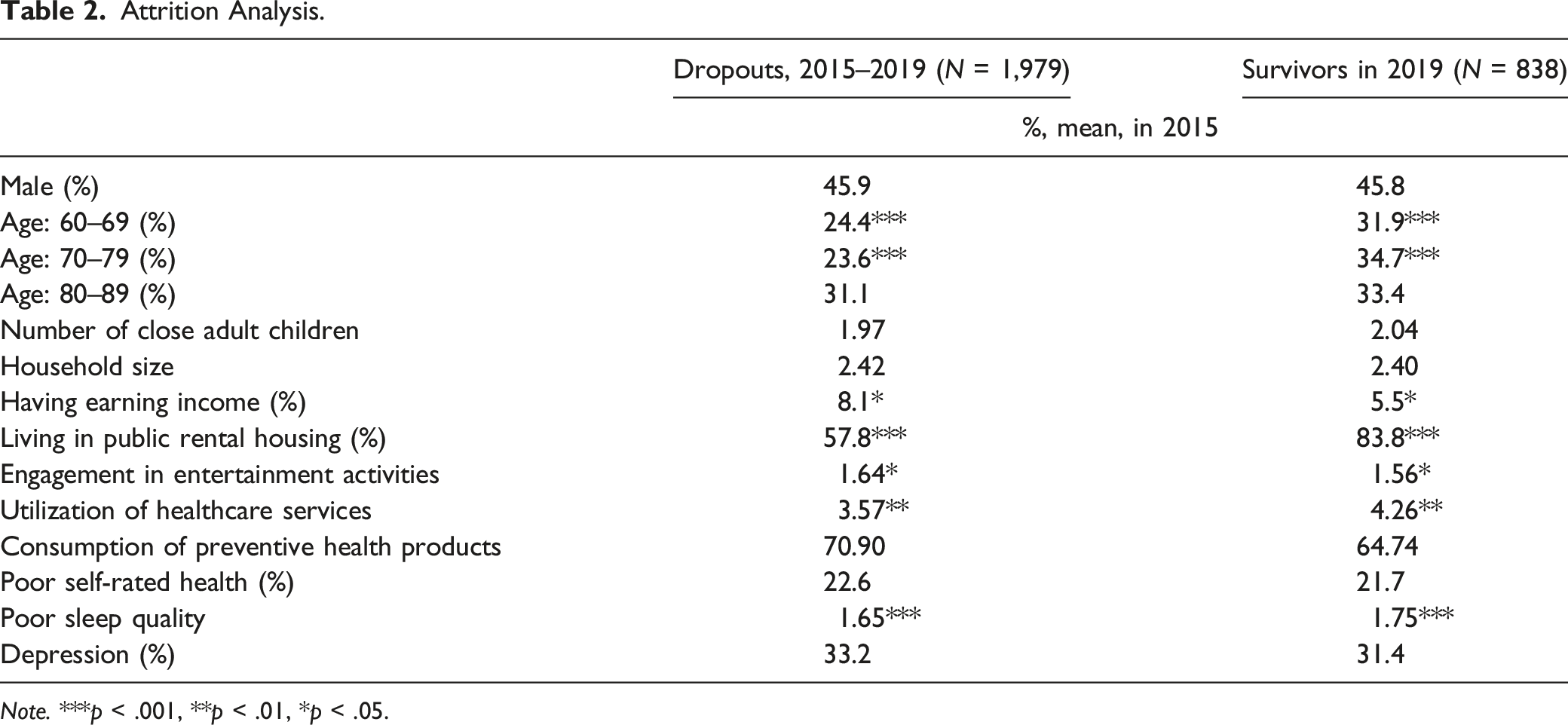
Note. ***p < .001, **p < .01, *p < .05.
Sample Descriptive Statistics of Two Groups (N = 489).
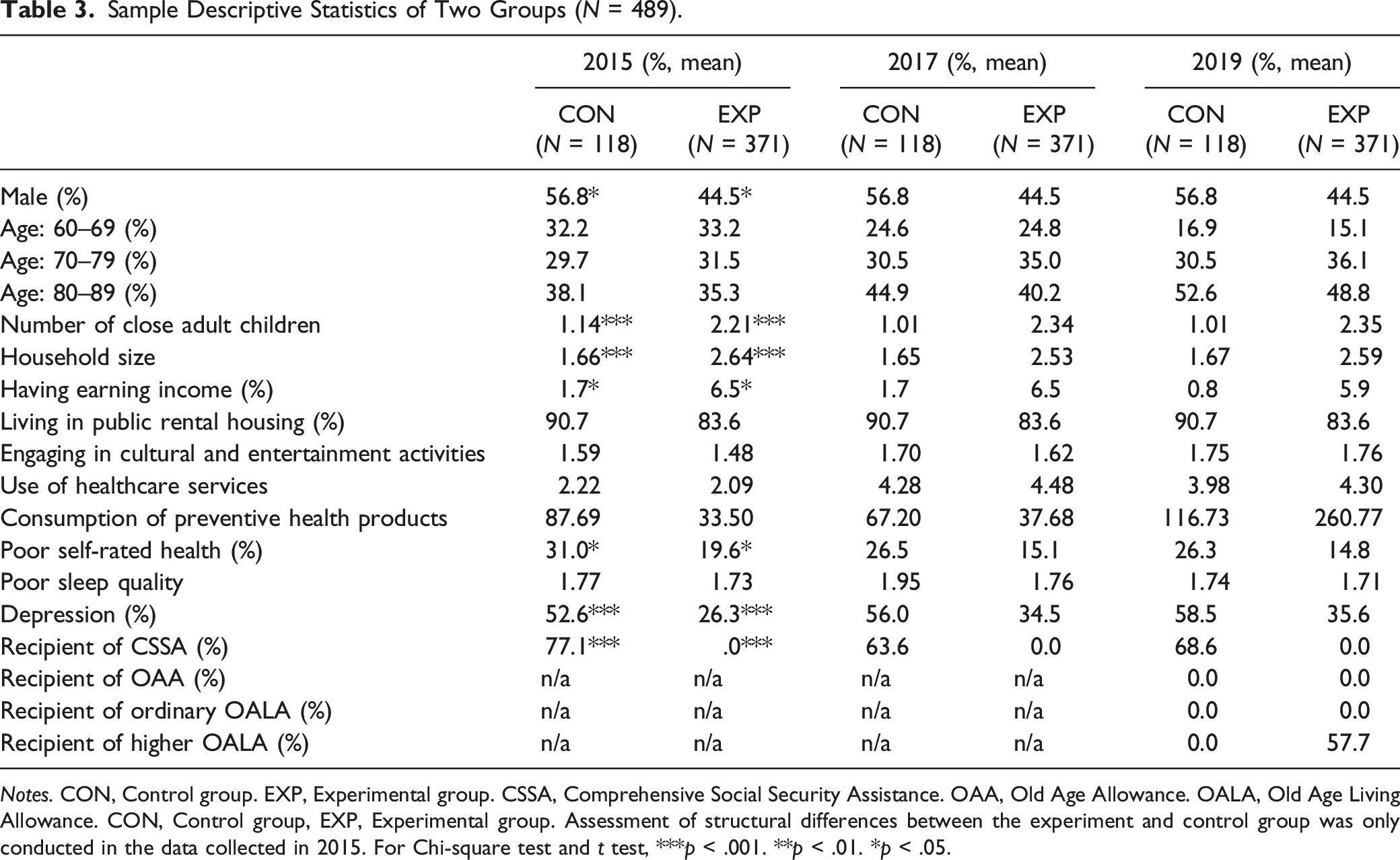
Notes. CON, Control group. EXP, Experimental group. CSSA, Comprehensive Social Security Assistance. OAA, Old Age Allowance. OALA, Old Age Living Allowance. CON, Control group, EXP, Experimental group. Assessment of structural differences between the experiment and control group was only conducted in the data collected in 2015. For Chi-square test and t test, ***p < .001. **p < .01. *p < .05.
Multiple Linear Regression and Linear Probability Regression Estimations on Health-Related Outcomes.
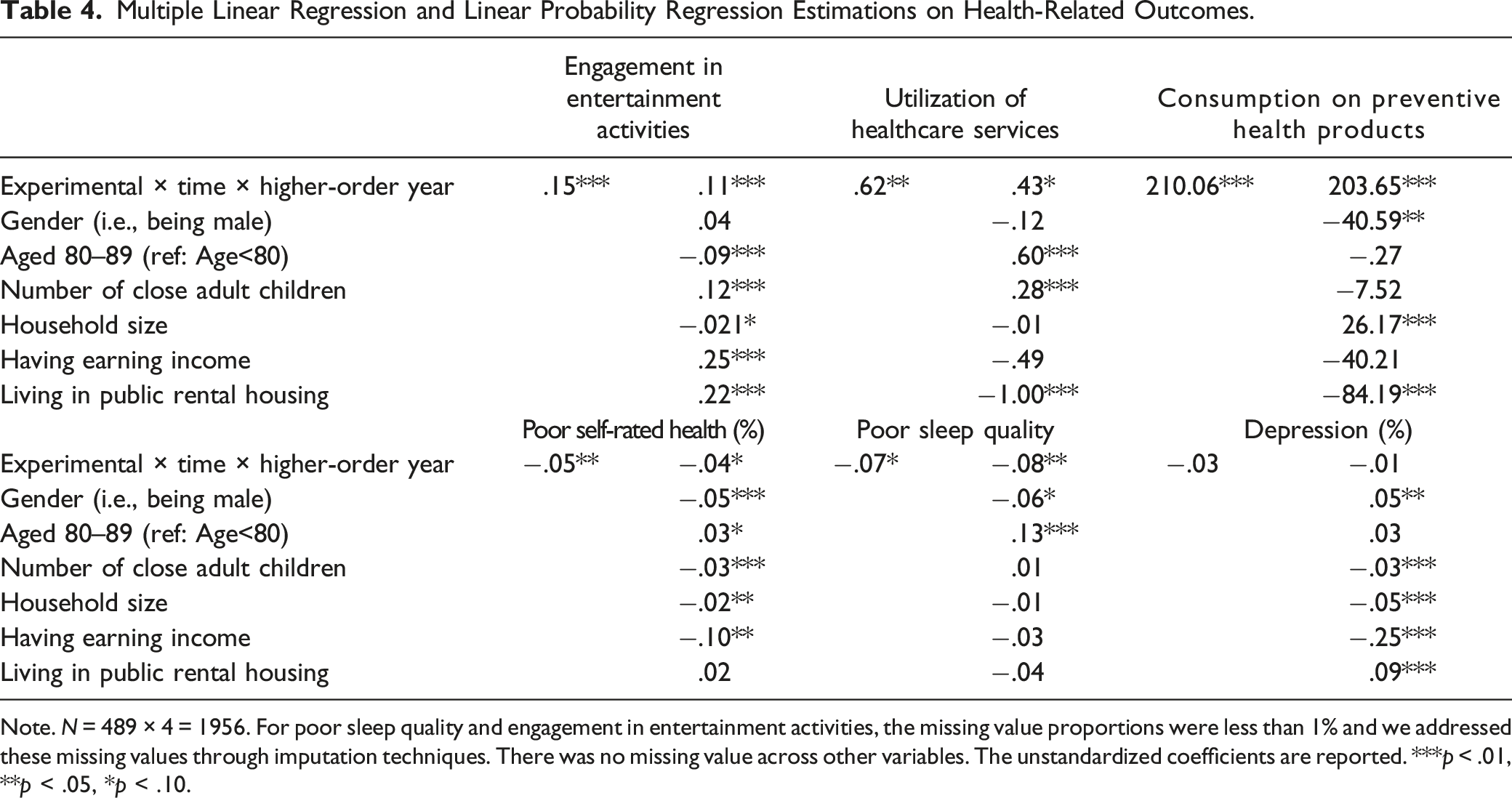
Note. N = 489 × 4 = 1956. For poor sleep quality and engagement in entertainment activities, the missing value proportions were less than 1% and we addressed these missing values through imputation techniques. There was no missing value across other variables. The unstandardized coefficients are reported. ***p < .01, **p < .05, *p < .10.
Discussion
The existing literature has established the positive economic impacts of social pension expansion, including increased disposable income and reduced poverty among older adults in various economies (Ebbinghaus, 2021; Ferreira, 2006; Kang et al., 2022; Lee, 2022; Lee et al., 2019; Long & Pfau, 2009). However, to gain a comprehensive understanding of the effects of social pension on overall wellbeing, it is crucial to examine the physical and mental health outcomes of older recipients following such expansions. Although recent studies have provided evidence of the positive impacts of social pension expansion on health outcomes, these studies have predominantly focused on samples from mainland China and South Korea. In this research context, our study responds to the call in the literature by investigating the positive effects of social pension expansion on personal health indicators in old age.
The main findings from our triple difference estimations partially align with existing research, indicating that the introduction of the higher OALA significantly improved certain physical health indicators such as sleep quality and self-rated health (Cheng et al., 2018; Hwang & Lee, 2022; Pak, 2021; Pan et al., 2021; Yuan et al., 2022). However, the higher OALA did not have a significant effect on the prevalence of depression among older adults in Hong Kong. Upon reviewing the estimated coefficients of covariates, we observed that factors such as gender, number of close adult children, household size, earning income, and housing type appeared to be more influential predictors of depression compared to the higher OALA. To address depression among older adults, interventions that focus on increasing social support through closer family ties and promoting labor market participation may be more effective solutions compared to relying solely on receiving the OALA.
Considering that the higher OALA did not comprehensively promote health-related consumption and health outcomes, including depression, we hesitate to solely recommend strengthening social pension schemes as a means to improve the health status of older adults in Hong Kong. Upon reviewing the effects of covariates on health-related consumption and health outcomes in Table 4, we observed that factors such as number of close children, household size, and earning income were powerful predictors, but like the higher OALA, none of them comprehensively affected all six outcome indicators. Therefore, in addition to strengthening social pension schemes, other aging policies such as aging-in-place (e.g., living with family members to improve household size and the number of close children) and labor policies that encourage employment among older adults (e.g., improving the prevalence of earning income) should also be implemented to comprehensively improve health-related consumption and outcomes.
Considering the current aging policy landscape in Hong Kong, we note that the government has allocated resources to support aging-in-place (e.g., issuing Community Care Service Vouchers), promote employment of older adults (e.g., providing on-the-job training allowances to employers who hire older employees), and expand social pensions (e.g., implementing the higher OALA). Future research should explore how these three policy interventions interact and influence the physical and mental health of older adults. We suggest that future studies identify effective combinations of these policy interventions, which will require the optimal utilization of public financial resources and maximize their effects on the physical and mental health outcomes of older individuals.
Limitations
While this study has important theoretical and practical implications, there are several limitations to the analytical design that should be acknowledged. First, the measurement of physical and mental health was limited to only three indicators, which implies that the overall picture we present may be incomplete. However, considering the scarcity of research examining the effects of social pension expansion on health outcomes, the contribution of this study is significant. Another limitation is that we did not investigate the causes of attrition among the dropouts in the last wave of the study. This lack of follow-up to understand the reasons for attrition (e.g., inability to locate participants, relocation, refusal to participate, illness, or death) raises uncertainty about whether the dropouts possess critical features that may impact the estimation of the model.
Furthermore, while the triple difference analysis allows us to comment on the effects of social pension expansion on changes in the health status of older adults, the evidence presented so far does not illustrate the specific mechanisms through which social pension affects the health status of older individuals. In other words, the impacts of social pension reform on health outcome variables have been analyzed in this paper, but gerontologists might be more interested in understanding the intricate relationships underlying these effects. Unfortunately, the present data are insufficient to further address this objective. The three-wave data used in this study have been employed to fit the triple difference model for the impact evaluation, leaving us without additional waves of data to construct a mediational model that examines how social pension affects the health status of older people. Another challenge is that the outbreak of COVID-19 at the end of 2019 has made it difficult to connect the follow-up assessments after 2019 (if we have) with the three-wave data collected on or before 2019. Consequently, investigating the mediational model that opens the black box of social pension reform becomes unlikely. To address this limitation, we suggest that future research replicate the design of this paper with at least 4–5 waves of data collected after 2023 (i.e., after the end of the COVID-19 pandemic). This approach will ensure that the evaluation is not affected by pandemic-related economic shocks. Specifically, 3–4 waves of data can be used to test the triple difference model, while an additional 1–2 waves of follow-up tests can be used to examine the mediational model. The triple difference estimations presented in this paper provide a solid foundation for future studies to build upon. For instance, since we found that social pension expansion improved three health-related consumptions (engagement in entertainment activities, utilization of healthcare services, and consumption of preventive health products) and reduced the prevalence of physical health problems (poor self-rated health and poor sleep quality), future research can investigate whether social pension expansion decreases the occurrence of poor self-rated health and poor sleep quality through the mediating effects of improving engagement in entertainment activities, utilization of healthcare services, and consumption of preventive health products, respectively.
Despite these limitations, this study fills an important research gap and provides valuable evidence on the relationship between social pension expansion and health outcomes. It serves as a foundation for future investigations to delve deeper into the topic and consider additional factors that may influence the effects of social pension on the health of older adults.
Footnotes
Author Contributions
All authors contributed to the study conception, design, material preparation, data collection and analysis, and the draft of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work described in this paper was fully supported by a grant from the Research Grants Council of the Hong Kong Special Administrative Region, China (Project No. EdUHK 18612718).
Ethics Approval
The ethical approval was obtained from the Human Research Ethics Committee (HREC) of The Education University of Hong Kong before the data collection.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent to Publish
The authors affirm that human research participants provided informed consent for publication.