
Abstract
Although the benefits of physical activity for older adults are well established, the prevalence of insufficient physical activity remains the highest among individuals over 60. This quasi-experimental study was intended to analyze the physical and psychological effects of older adults’ participation for 15 weeks in a light-intensity, group-based, multicomponent program designed to be long-term, inclusive, and low-cost. A total of 143 community-dwelling older adults were included in the final analysis. On average, participants attended 76.5% of the sessions (SD = 15.8%), and the median time of previous participation in the program was 15 (IQR: 4–37) months. Significant improvements were observed in executive functioning and selected physical outcomes with lower baseline performance; furthermore, overall well-being was maintained. This program promotes prevention by maintaining or enhancing physical and psychological health, in addition to addressing barriers to long-term participation in community-based physical exercise, especially for those with poorer health status.
Keywords
• This light-intensity, multicomponent group exercise improved older adults’ endurance, upper-limb strength, and cognitive functioning while maintaining lower-limb function, handgrip strength, quality of life, short-term memory, and emotional well-being. • The light-intensity design fosters self-efficacy and offers meaningful opportunities for community engagement and socialization, even for older adults managing health conditions.
• The efficacy of the Adapted Physical Activity (AFA Over 65) program, implemented across 77 cities over 10 years, supports policy-level promotion aimed at fostering healthy aging and reducing sedentary behavior in a heterogeneous population. • The attendance observed in the AFA Over 65 program provides an ongoing, sustainable model that supports long-term maintenance. • The cognitive improvements observed in participants without baseline impairment highlight a preventive window of opportunity: Incorporating light-intensity, multicomponent programs into routine aging care could help delay cognitive decline in a cost-effective manner.What This Paper Adds
Applications of Study Findings
Introduction
As the population ages, frailty becomes an increasing concern. The majority of existing research focuses on older adults with age-related diseases that limit self-sufficiency (Morganti, 2024). The prevalence of physical frailty in community dwellers aged over 50 worldwide is 12–24% (O’Caoimh et al., 2021). Although interventional studies are crucial for frail older adults, a significant portion of the aging population remains free from frailty and can be defined as healthy aging individuals. Studying this group is equally important for promoting healthy longevity and implementing effective strategies for frailty prevention.
The risk of developing frailty can be mitigated by the adoption of a healthy lifestyle throughout one’s life course (Morganti, 2024), including in later life (Wang et al., 2023). A recent study on the influence of lifelong habits on aging has shown that higher levels of physical activity are a factor influencing longevity (Argentieri et al., 2025). However, data from 197 countries indicate that insufficient physical activity remains most prevalent among individuals over the age of 60 (Strain et al., 2024). Although systematic reviews have demonstrated that structured exercise programs effectively reduce fall risk (Ng et al., 2019), improve psychological and social aspects (Kong et al., 2024) as well as global cognition, executive functioning, and memory (Zhang et al., 2023), longitudinal research indicates that older adults rarely maintain these activity levels beyond 12 months after completing such programs (Audsley et al., 2021).
Community-based group exercise programs play a promising role in older adults’ sustained adherence to an active lifestyle, with long-term adherence rates of nearly 70% (Farrance et al., 2016). These programs improve mobility and physical functional outcomes (Ng et al., 2019), can reverse prefrailty to a healthy state (Lim et al., 2024) and represent an opportunity for social connectedness (Farrance et al., 2016). Evidence also indicates improvements in cognitive function, even though this is largely focused on individuals with mild cognitive impairment or dementia (Lewis et al., 2017; Yan et al., 2023).
However, such programs may be perceived as having low accessibility (Wells et al., 2024) and affordability (Fien et al., 2022). In addition, existing research on community group programs has largely focused on either older adults who are relatively younger, excluding those using walking devices (Kuo et al., 2024) or populations with a significant risk of falling (Ng et al., 2019). This emphasis on either end of the health spectrum overlooks a common barrier faced by individuals living with health conditions that may not identify with either group. Therefore, to overcome initial barriers, interventions should be flexible, safe and adapted to the disabilities that older adults may face (Garmendia et al., 2013).
The Adapted Physical Activity (AFA Over 65) program is promoted among senior communities by the Sports Center of the University of Bergamo, and in the last 10 years, it has been implemented across 77 municipalities in northern Italy, encompassing both urban and rural settings. This multicomponent group program promotes group-tailored, light-intensity exercise and is designed to be adjustable, inclusive, and low-cost. Given the potential of community-based group exercise to support sustained adherence to an active lifestyle and considering that this program appears to address key barriers identified in the literature
Methods
Trial Design
This was a quasi-experimental study with a within-subject design. This research adhered to the ethical principles outlined in the Declaration of Helsinki and received approval from the Ethics Committee of the University of Bergamo (Approval Number 2024_04_02).
Participants
Overall, approximately 2,000 older adults were active in the AFA Over 65 program across all 77 municipalities in the Bergamo province. A total of 339 community-dwelling individuals from eight municipalities were considered for the study. Eligibility criteria for inclusion were: (1) being enrolled in the AFA Over 65 program in one of these municipalities and (2) had medical clearance to engage in an exercise program. The exclusion criterion was: (1) the presence of a pacemaker. Recruitment was carried out using a convenience sampling method. A member of the research team visited each participating municipality and introduced the study during one of the scheduled group sessions, during which all enrolled individuals were invited to participate.
All participants were thoroughly informed in both written and verbal forms about the study purpose and procedures as well as any potential risks involved. Prior to their involvement in the study, the participants were briefed on the protocol for data collection, and written informed consent was obtained from them.
Intervention
The AFA Over 65 program follows a structured protocol of light-intensity group exercise, conducted twice a week under the supervision of a licensed sports trainer. The program generally runs each year from the first week of October to the second week of June; it is paused during the summer, and there are breaks during holiday periods, such as Christmas and Easter.
Each municipality had a different number of active AFA Over 65 groups, with each group consisting of a maximum of 20 participants with varying levels of physical function. The sessions include 20 min of warm-up, 30 min of workout, and 10 min of cool-down exercises.
The warm-up phase consisted of whole-body activation and walking. It included a combination of mobility, flexibility, and joint-activation exercises for the upper and lower body. These exercises were performed either seated or standing, depending on individual capabilities. The cool-down phase focused on relaxation and breathing, in addition to the stretching of the most contracted muscle areas.
The workout phase was designed to target specific goals, including the maintenance or improvement of strength, balance, aerobic capacity, and range of motion. Strength exercises, both isometric and isotonic, targeted the upper and lower body using dumbbells, resistance bands, and soft balls. These exercises included shoulder raises, internal and external shoulder rotations, bicep curls, arm extensions, elastic band pulls, leg extensions, adductions, and abductions. Balance training involved the use of obstacles, balance pods, steps, and cones to create circuits that included, for example, obstacle clearance, changes in direction and sense, weight-shifting, one-leg standing, and wavy courses between objects. In range-of-motion exercises, wooden sticks, resistance bands, soft balls, and tennis balls were utilized to perform shoulder lifts, arm flexions, rotations, extensions, and pelvic retroversion and anteversion against a wall, while ball rolling was used for ankle mobility. Aerobic capacity was addressed through dynamic circuits involving different sets of specific movements and gait patterns, as well as continuous on-the-spot exercises.
The progression of each session was recalculated monthly, with each mesocycle focusing on developing specific objectives related to strength, balance, mobility, and aerobic capacity. As a result, activities alternated, and the complexity of execution gradually evolved. The progression of the training load followed a structured approach: starting exercises from a seated position across all three phases of a single session, gradually alternating between seated and standing exercises, and eventually performing most of the training session in a standing position. The execution progression involved increasing the duration of exercises, raising the number of repetitions, enhancing the load while reducing repetitions, progressively increasing repetitions with the new load, and slightly reducing the recovery time between repetitions.
Outcome Measurements
At the beginning of the AFA Over 65 program, the participants’ demographic data, anthropometric measurements, medical history, and time of participation in the program were recorded. The frequency of participation was collected using a diary. The Borg Rating of Perceived Exertion Scale (Morishita et al., 2019) was used to measure the intensity of the exercise intervention for each training session.
Participants were assessed before and after 15 weeks of intervention. Prior to this period, they had already been exposed to the program for approximately 12 weeks, from October to December. The 15-week study period corresponds to the continuous participation phase from January to May, following the 2-week holiday break in late December and early January. A physiotherapist conducted all motor assessments, while a psychologist performed all psychological assessments; both were licensed professionals with over 5 years of experience. For a more comprehensive overview of the assessment procedure, please refer to the following publication (Benincá et al., 2024).
The motor assessments included the Timed Up and Go (TUG) test (Bohannon, 2006), which assessed mobility. Upper-limb strength and function were evaluated using the 30-Second Arm Curl (30AC; Parkatti et al., 2012) and Handgrip Strength (HGS; Patrizio et al., 2020) tests, while the Short Physical Performance Battery (SPPB; Silva et al., 2021) was used to assess lower-limb function. The Two-Minute Step Test (2MST; Bohannon & Crouch, 2019; Rikli & Jones, 1999) was used to measure endurance, with the heart rate collected during the test execution. In particular, the resting heart rate was measured in the sitting position prior to the commencement of the motor and psychological assessments, using a Polar RS800CX training computer (Polar Electro Oy, Kempele, Finland). The maximum heart rate was recorded at the end of the 2MST, and the participants then sat down to rest. The recovery heart rate was measured 1 min later while they remained seated.
The psychological assessments included the Frontal Assessment Battery (FAB15; Ilardi et al., 2022) for evaluating executive functioning, the WAIS Digit Span Test (Orsini et al., 1987) for assessing short-term memory, the 15-item Geriatric Depression Scale (GDS; Shin et al., 2019) for identifying depressive symptoms, and the 26-question World Health Organization Quality of Life Brief Version (WHOQOL-BREF; De Girolamo et al., 2000) for assessing quality of life.
Sample Size
G*Power software Version 3.1.9.7 was employed for sample size calculation. The sample size was determined through an a priori analysis using the F-test family for repeated measurements, within factor, considering a power of 80% and an alpha of 5% to detect a small effect size (f = 0.1). Based on the calculations, the minimum sample size required to include all nine measurements was 125. A larger number of individuals were enrolled considering a discontinuation rate.
Statistical Analysis
Before conducting the analysis, the scores of the FAB15 and the WAIS Digit Span Test were adjusted as recommended (Ilardi et al., 2022; Orsini et al., 1987), while the WHOQOL-BREF raw scores were converted into a 4–20 scale for each domain (De Girolamo et al., 2000). All analyses were performed using the software R 4.3.3 (R Foundation for Statistical Computing, Vienna, Austria; Team R Core, 2021).
Physical capacity, psychological well-being, physiological, and demographic data were summarized using descriptive statistics, and the normality of data distribution was assessed using the Shapiro–Wilk test. Physiological and anthropometric data was compared using two-tailed paired t test or the Wilcoxon signed-rank test. As the assumption of multivariate normality was not met, a semi-parametric repeated measurements multivariate analysis of variance (MANOVA) was conducted using the MANOVA.RM package (Friedrich et al., 2023); the model included time (pre-test and post-test) as the within-subject factor and 2MST, TUG, 30AC, HGS, SPPB, FAB15, WAIS Digit Span Test, GDS, and WHOQOL-BREF four domains (physical health, psychological, social relationships, and environment) as dependent variables. When significant, the MANOVA was followed by a one-tailed paired t test for normally distributed variables, while the Wilcoxon signed-rank test was applied to non-normally distributed variables.
The effect sizes for parametric tests were computed using Cohen’s d (< 0.2: negligible; < 0.5: small; < 0.8: medium; and otherwise large), whereas those for nonparametric tests were determined using the Wilcoxon effect size (r; 0.10 to < 0.3: small effect; 0.30 to < 0.5: moderate effect; and ≥ 0.5: large effect). To control for multiple testing, p values were adjusted using Holm’s method. All results are reported with the corresponding effect sizes and corrected p values where applicable. Statistical significance was set at p < .05 for uncorrected values.
An additional exploratory analysis was conducted to assess whether the number of months already spent in the program before the 15-week study period was associated with the magnitude of change in outcomes.
Results
Of the 339 older adults eligible to participate, 202 volunteered to enroll in the study. Among them, 55 were lost to follow-up, resulting in a final sample of 143 adults (25 males) with a mean age of 74.3 years (SD = 6.6) were included in the final analysis (Figure 1). On average, participants attended 76.5% (SD = 15.8%) of the sessions during the 15-week study period, and the intensity of the exercise intervention was 10.4 (SD = 1.8) on the 6–20 Borg Rating of Perceived Exertion Scale. The median time of previous participation in the AFA Over 65 program, before the 15-week study period, was 15 months (IQR: 4–37). Correlation analyses revealed very weak correlations (|r| < 0.10) between the number of months already spent in the program and changes in all outcomes, suggesting that prior participation did not affect the observed improvements. Flow of participants from the eight included municipalities (Municipality A–H, connected by dotted lines)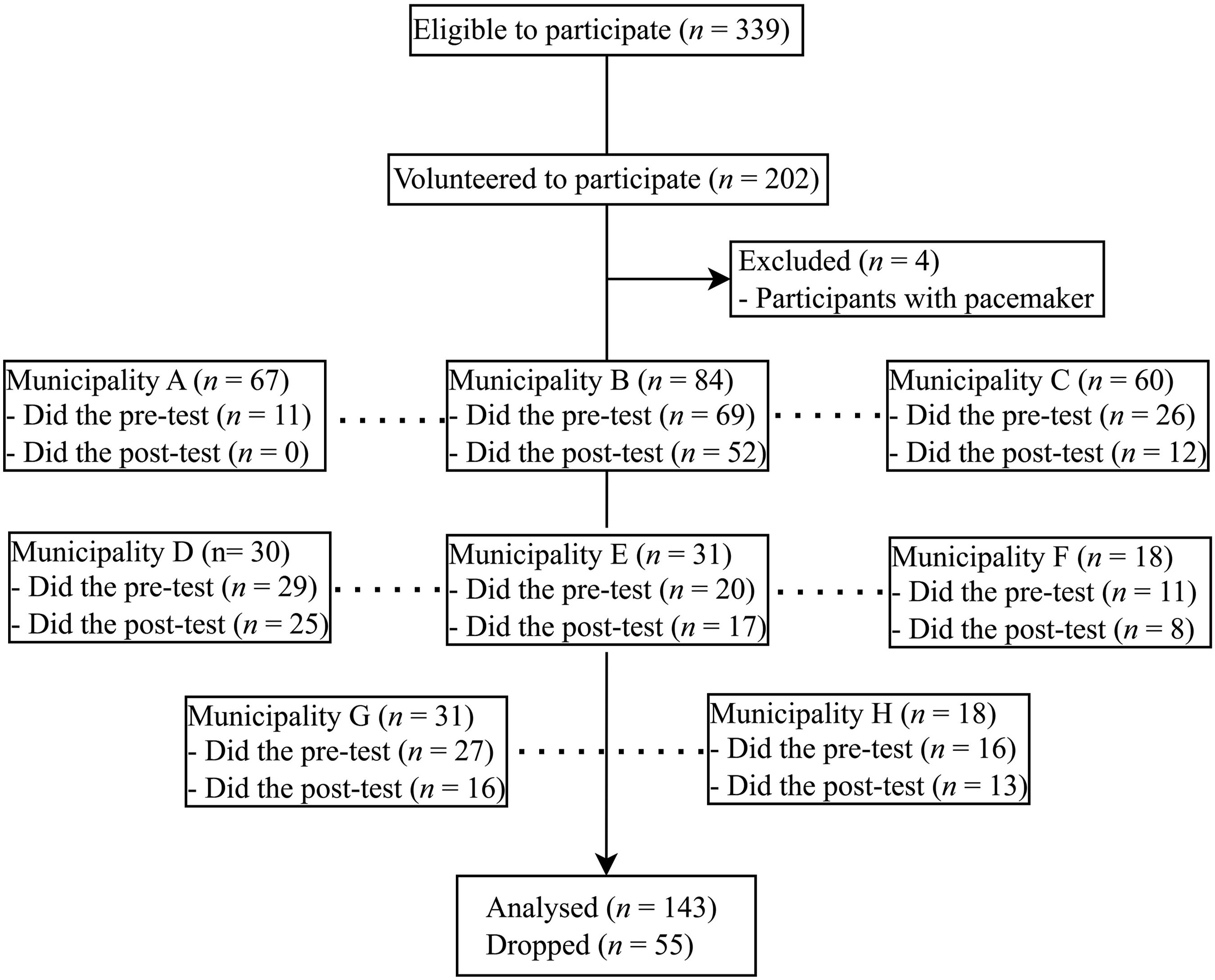
The Participants’ Physiological and Anthropometric Measures at Pre-test and Post-test in Mean ± SD; Median (IQR)
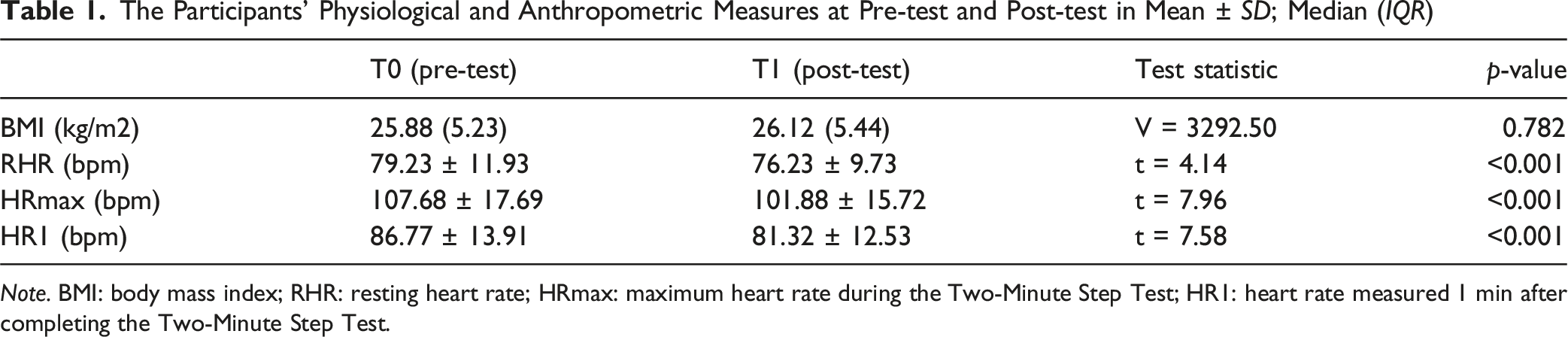
Note. BMI: body mass index; RHR: resting heart rate; HRmax: maximum heart rate during the Two-Minute Step Test; HR1: heart rate measured 1 min after completing the Two-Minute Step Test.
In the baseline, the proportion of participants who did not reach normative values in the motor tests was 75% for 2MST (Rikli & Jones, 2013), 68% for TUG (Bohannon, 2006), 71% for 30AC (Rikli & Jones, 1999), and 22% for HGS (Landi et al., 2020). For the SPPB, 77% of the participants scored > 9, indicating high physical performance (Veronese et al., 2014). With regard to the psychological tests, 17% of the participants were below the cut-off score of the FAB15, indicating cognitive dysfunction (Ilardi et al., 2022), and 21% were above the cut-off point of the GDS, indicating a depressive state (Shin et al., 2019). In the evaluation of short-term memory, 82% of the participants attained the highest score: between 5.25 and 9. Finally, 36% of the participants attained more than 70% of the WHOQOL-BREF maximum score (Chen et al., 2017), with a pre-test mean of 58.9 (SD = 4.4) and post-test of 58.3 (SD = 4.6).
Post-Hoc Univariate Analysis for Motor and Psychological Variables (Pre-test vs. Post-test) in Mean ± SD; Median (IQR)
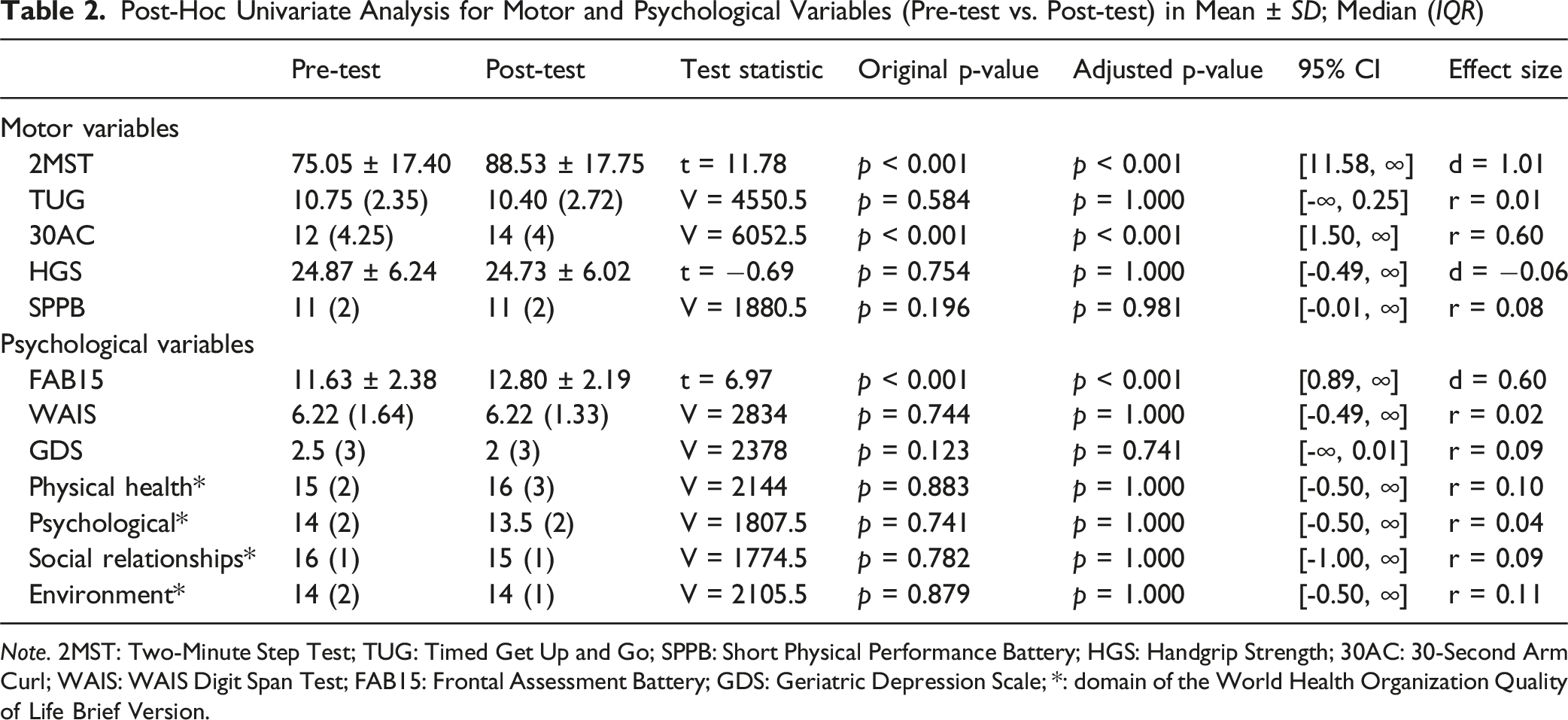
Note. 2MST: Two-Minute Step Test; TUG: Timed Get Up and Go; SPPB: Short Physical Performance Battery; HGS: Handgrip Strength; 30AC: 30-Second Arm Curl; WAIS: WAIS Digit Span Test; FAB15: Frontal Assessment Battery; GDS: Geriatric Depression Scale; *: domain of the World Health Organization Quality of Life Brief Version.
Discussion
This study was intended to evaluate the outcomes of a 15-week community participation program for older adults, characterized by light-intensity exercise and a multicomponent approach, with an emphasis on community engagement. Concerning physical outcomes, the findings revealed significant improvements in endurance and upper-limb strength, accompanied by a reduction in the resting heart rate and the maximum heart rate. In addition, mobility, lower-limb function, and handgrip strength were maintained. Regarding psychological outcomes, a significant enhancement in executive function was observed, while short-term memory, depressive symptoms, and quality of life were maintained.
Notably, even light-intensity exercise led to improvements in motor outcomes. The variables that showed improvement were those in which most of the participants had baseline values below normative standards, except for the TUG test. Light-intensity physical activity is often seen as an opportunity to break up sedentary behavior or as an alternative for individuals who cannot perform higher-intensity activities (Delaire et al., 2023; Gardner et al., 2022). To date, light-intensity exercise protocols have been investigated less frequently. The current findings contribute to the growing body of evidence suggesting that even this level of intensity can lead to meaningful gains in strength and endurance, as indicated by large effect sizes—an area still debated in the literature (Stojanović et al., 2021; Thomas et al., 2004). Although light-intensity exercise has demonstrated beneficial effects, a Cochrane review reported that higher-intensity exercise tends to produce more pronounced improvements in highly supervised, gym-based programs. However, it remains unclear which approach is more beneficial for less fit or healthy older adults in other settings (Christie, 2011).
As regression to the mean (RTM) is a relevant concern in pre-post study designs, we evaluated this possibility and concluded that the improvements observed in motor performance are best interpreted as genuine gains rather than statistical artifacts. Our rationale aligns with the framework proposed by Morton and Torgerson (2005), who emphasize that RTM effects are most pronounced when measurement error is high and test-retest correlation is low—neither of which applies to our data.
The absence of improvements in tests in which the participants’ performance was already within normative ranges suggests that this protocol may help maintain function but does not necessarily confer additional protective effects through increased intensity. The low normative values observed in the TUG test appear inconsistent with the SPPB findings, as both assessments are related to balance, mobility, and lower-limb strength. However, when applying a 12-s cut-off for fall risk prediction, only 30% of the study sample would be classified as at risk (Ambrose et al., 2015).
Regarding psychological outcomes, approximately 80% of the participants exhibited optimal levels of executive functioning, short-term memory, and emotional well-being. However, fewer than half scored above 70% of the maximum quality of life score at baseline, indicating substantial room for improvement—yet this proportion remained unchanged post-intervention. Although overall WHOQOL-BREF scores slightly declined, subdomain analyses revealed no significant changes in physical health, psychological well-being, social relationships, or environmental quality of life.
These findings may reflect the complexity of health-related quality of life, which encompasses not only subjective perceptions of health but also external and contextual factors (Ramji et al., 2023). Moreover, 75% of participants had already attended the program for more than 4 months, suggesting that the benefits of participation may have reached a plateau. It is noteworthy that nearly half of the participants lived alone, which may have contributed to lower quality of life scores, as living alone is associated with health challenges such as social isolation, reduced social support, and limited access to emergency assistance (Kuo et al., 2024). Overall, this finding supports the importance of a holistic approach that extends beyond physical training to promote active aging.
The modest, though statistically significant, improvement in executive functioning suggests that this domain may be more responsive to light-intensity exercise than the other psychological outcomes measured. The integration of various exercise components may require coordination and control over different movement patterns, potentially contributing to this effect. Notably, most participants already had high FAB15 scores at baseline, which raises the possibility of a ceiling effect. However, less than 15% reached the maximum score at post-test (Terwee et al., 2007), suggesting the measure retained sensitivity to change. This result was accompanied by a medium effect size (d = 0.60), which could indicate a noticeable change. However, this interpretation should be made with caution, as the clinical relevance of this finding remains unclear due to the lack of an established minimal clinically important difference (MCID) for the FAB15. These findings are in line with those of Sanders et al. (2019), who reported small but positive effects of exercise on executive function (d = 0.27).
Although previous studies have found that memory is the cognitive domain least improved by exercise interventions, some research suggests that the benefits of physical activity on memory are independent of intensity. In contrast, a recent meta-analysis reported a moderate and significant effect directly linked to intensity (Zhang et al., 2023). The current study’s findings contribute to this discussion by demonstrating that memory function can be preserved through light-intensity exercise. However, group dynamics and the multicomponent nature of the intervention may have played a moderating role in this outcome.
In this study, it was found that adherence to the program was maintained, even though there was no substantial progression in exercise intensity. This finding seems to contradict an umbrella review that highlighted that tailored exercise plays a crucial role in enhancing adherence, whereas longer exercise interventions tend to be associated with lower adherence rates (Collado-Mateo et al., 2021). This presents a challenge because discontinuing exercise leads to a partial or complete loss of training-induced adaptations (Cassemiliano et al., 2024). A possible explanation for the high attendance and long-term adherence observed in the AFA Over 65 program is that, although it allows for some degree of progression, its primary focus lies elsewhere. Specifically, its light-intensity design, combined with its widespread availability across multiple neighborhoods at a low cost, facilitates self-efficacy, provides a valuable opportunity for socialization within the community, and supports integration into daily life.
The current study has certain limitations, some of which are inherent in its design. First, the absence of a control group is a notable shortcoming, as it limits the ability to attribute observed effects solely to the intervention. In addition, although short-term improvements were observed, it remains unclear whether these benefits persist beyond the 15-week period. Future studies should incorporate longer-term follow-up assessments, such as at six or 12 months, to evaluate the sustainability of the intervention’s effects. Besides, while our exploratory analysis found a very weak association between prior participation and outcome changes, the variability in participants’ prior exposure to the program may still have influenced baseline function and the potential for improvement. The use of convenience sampling led to a sample that was predominantly female. As a result, the generalizability of the findings may be limited. Finally, the use of self-reported measures rather than objective quantification of intensity is also a limitation. Furthermore, there is a possibility of selection bias, as frailer or less motivated individuals may have been less inclined to participate in the assessment. The resolution of these limitations is a primary objective in forthcoming research endeavors.
Conclusions
This study shows that a real-world, light-intensity, community-based exercise program for older adults significantly improves executive functioning and selected physical outcomes with lower baseline performance while maintaining overall well-being.
The program is designed to address common barriers to participation in physical exercise in the community: it offers a valid option for older adults with or without health problems, as it is safe, flexible, and adaptable thanks to its light intensity and multicomponent structure. It is available across many municipalities, ensuring geographical accessibility, and it is affordable, given its symbolic cost. Considering the potential functional decline that can result from the cessation of physical activity, programs like this have the potential to support the integration of physical exercise into daily life in a sustainable manner and, in doing so, serve as a tool for promoting healthy longevity.
The light-intensity design of the AFA Over 65 program presents both advantages and limitations. With regard to advantages, the program’s focus on accessibility, social engagement, and continuity likely contributed to the high attendance observed. Besides, this program is adaptable and versatile, making it suitable not only for healthy older adults but also for those with chronic conditions, undiagnosed motor weakness, or transitioning from rehabilitation. Regarding limitations, the program is designed to be adaptable and inclusive, and allows for progression only up to a certain point, which may be insufficient to provide benefits other than maintenance for older adults in optimal health.
Subsequent research will assess the efficacy of light-intensity motor activities as a preventative measure against cognitive decline, in line with the enhanced executive function benefits observed. This will involve developing community-based programs, such as AFA Over 65, that also include cognitive strategies. The protocol is expected to integrate specific motor exercises designed to promote executive function and other cognitive functions. Implementing this approach could facilitate the structuring of mind–motor activity, thereby mitigating the risk of decline, encompassing both physical and cognitive domains.
Footnotes
Acknowledgments
We would like to thank the University Sport Centre (CUS) for their collaboration, as well as the volunteers and sport trainers of the AFA over-65 program.
Ethical Considerations
The study received ethics approval from the Ethics Committee of the University of Bergamo (Approval number 2024_04_02).
Consent to Participate
Written informed consent for inclusion in this research was obtained from the patients prior to participation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: I.L.B., M.G., S.B. and F.M. were partially granted by Unione Europea—Next Generation EU (grant number PRIN2022RAESSJ).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.