
Abstract
A primary objective of active aging policies is to promote health and optimize care for individuals. In aging societies, the maintenance of good physical and mental health and the management of risk factors are of utmost importance. Few research studies have analyzed active aging policies related to health and care from a multi-level governance perspective. The aim of this study was to determine what national and regional policies in these domains existed in Italy. We conducted an inductive thematic analysis of health- and care-related policies on active aging, selected through a systematic review in 2019–2021. The analysis uncovered three themes at both the national and regional levels (health promotion and disease prevention, health monitoring, and informal caregivers) and two additional themes at the regional level (access to health and social care services, and mental health and well-being). According to the findings, COVID-19 partially influenced the evolution of active aging policies.
• Review of health- and care-related policies on active aging in Italy; • Understanding the intersection between active aging and health and care policies; • Impact of the COVID-19 pandemic on health and care, as well as on active aging policies.
• Better understanding of health- and care-related policies on active aging for further research and policy-making; • Reflections on how theory, policy and practice of active aging deeply collided against the COVID-19 pandemic, its direct and indirect impacts, and the policy responses to manage the epidemiological, social and economic emergency; • Replicable study protocol for reviewing active aging policies in other countries or sectors.What this paper adds
Applications of study findings
Introduction
According to the World Health Organization (WHO, 2002, p. 12), active aging (AA) is the “process of optimizing opportunities for health, participation, and security in order to enhance quality of life as people age.” In many high-income countries, AA is typically framed in a positive policy discourse, where it (implicitly or explicitly) constitutes a new component of welfare states in times of aging populations (Walker & Maltby, 2012). The initial use of the AA concept by policymakers and researchers was predominantly based on a productivist interpretation that focused on work and other productive social activities such as volunteering (Foster & Walker, 2015; Zaidi & Howse, 2017). Rather, AA should be recognized as a multidimensional concept that encompasses various policy domains and social engagement activities (Walker, 2002). Consequently, AA may be formulated as a policy strategy, a coherent and harmonized policy framework, or a set of one or more sectorial policies targeting specific AA dimensions. These dimensions refer to a wide range of activities (e.g., labor market participation, volunteering, social relations, education and training, leisure, healthy lifestyles, and informal care) that contribute to individual well-being for all aging individuals, not just those with better health or more socio-economic resources (Foster & Walker, 2021).
“Health” represents one of the three pillars of WHO’s AA conceptual framework (the other two being “participation” and “security”), which is founded on the individual and societal benefits of maintaining and/or improving a satisfactory health status throughout the life course. For instance, this includes providing opportunities for healthy behaviors, physical activity, a healthy diet and nutrition, self-management of potential chronic diseases or disability conditions in daily life, etc., to aging individuals. Health-related policy on AA refers to broader public health objectives, which are to be attained through health promotion, education and disease prevention programs, awareness campaigns, and an adequate supply and organization of primary and secondary health and social care services.
Furthermore, the provision of informal care by aging individuals to significant others is a common occurrence in many societies (OECD, 2021; Schulz & Tompkins, 2010). According to the WHO (2002) framework (under the “health” pillar), being committed and capable of helping others, thereby supporting their health and quality of life, is an additional social engagement activity that is relevant for AA. Informal caregivers contribute directly to improving the AA of significant others, but they should also receive adequate support to prevent the negative effects of caregiving from impeding their individual AA pathways. Care-related policy on AA typically falls between long-term care (LTC) policies, which are intended to support the integration or complementarity of informal care with formal care; health policies that are designed to support informal caregivers by preventing and managing possible risks to their own health, such as burden, stress, and anxiety; and social welfare policies that are intended to mitigate the risk of income loss or social disadvantages for informal caregivers through monetary and work-care conciliation benefits.
The health and care components of AA, as well as the overall concept and purpose of AA, were challenged by the COVID-19 pandemic (Morrow-Howell, 2020; UNECE, 2020). The latter dramatically exposed the weaknesses of social protection systems and health and social care services, necessitating adaptations (Gorenko et al., 2021). Older people are most at risk and the primary victims of the pandemic, given their increased likelihood of contracting the disease, becoming seriously ill, and eventually passing away (Lupu & Tiganasu, 2022; Mueller et al., 2020; OECD & European Commission, 2020). In addition to health and epidemiological risks, older people also experienced (as did the general population) temporary restrictions in mobility and social life, with negative effects on their physical, mental, and social well-being (Cunningham & O’Sullivan, 2020; Landry et al., 2020; Weissberger et al., 2022).
In every country, the majority of AA programs and initiatives were stopped at the height of the epidemic. During this phase, policymakers focused on identifying new short-term priorities for the aging, health, and care sectors in order to manage the pandemic-related crisis. Among the key measures adopted by most countries were those designed to contain the spread of the novel coronavirus, organize massive vaccination campaigns, and adapt health and social care services to the new context. To date, few studies have investigated certain aspects of AA in pandemic times (Lucantoni, Principi, et al., 2022; Principi, Lucantoni, et al., 2022; Zingmark et al., 2022), with limited attention to the health and care components of AA.
In order to contribute to the knowledge on these topics, the purpose of this study was to determine, from a multi-level governance perspective, what health- and care-related policies on AA exist in Italy and whether or not COVID-19 influenced them.
Methods
Study Design and Conceptual Framework
The study was part of a large national initiative carried out in 2019–2022, which is now undergoing a 3-year follow-up project (2022–2024) with the objectives of developing, monitoring, and stimulating the progress of AA policies at both the national and regional levels, creating stakeholder networks, and increasing awareness of AA in Italian society (Barbabella et al., 2020; DPF 2022). The project was carried out by the National Institute of Health and Science on Aging (IRCCS INRCA) with funding from the Department for Family Policies (DFP), an office of the Italian Presidency of the Council of Ministers. Previous results on policy analysis (Barbabella, Cela, et al., 2022), policy implementation and recommendations (Lucantoni, Principi, et al., 2022), and the heterogeneity of AA across the country (Principi, Di Rosa, et al., 2022; Zannella et al., 2021) have been published elsewhere.
This study was conceived as an inductive thematic analysis of AA policies addressing the health and care domains. The goal was to determine what AA health- and care-related policies exist in Italy and what their purpose is, also in light of the social changes caused by the COVID-19 pandemic and the related revision of policy priorities.
In terms of selection criteria, AA policies were defined in accordance with the WHO’s (2002) multidimensional definition from a life course perspective. We therefore selected policies that directly or indirectly referred to the AA concept in relation to the promotion of labor, social, educational, leisure, health, and care activities performed by older people and aging individuals (Barbabella et al., 2020; 2022a). The unit of analysis was a single policy measure, not a single policy document.
Data Collection
List of National (Ministries, Departments, and Agencies) and Regional (Regions and Autonomous Provinces) Institutions Investigated in Each Wave of Data Collection.
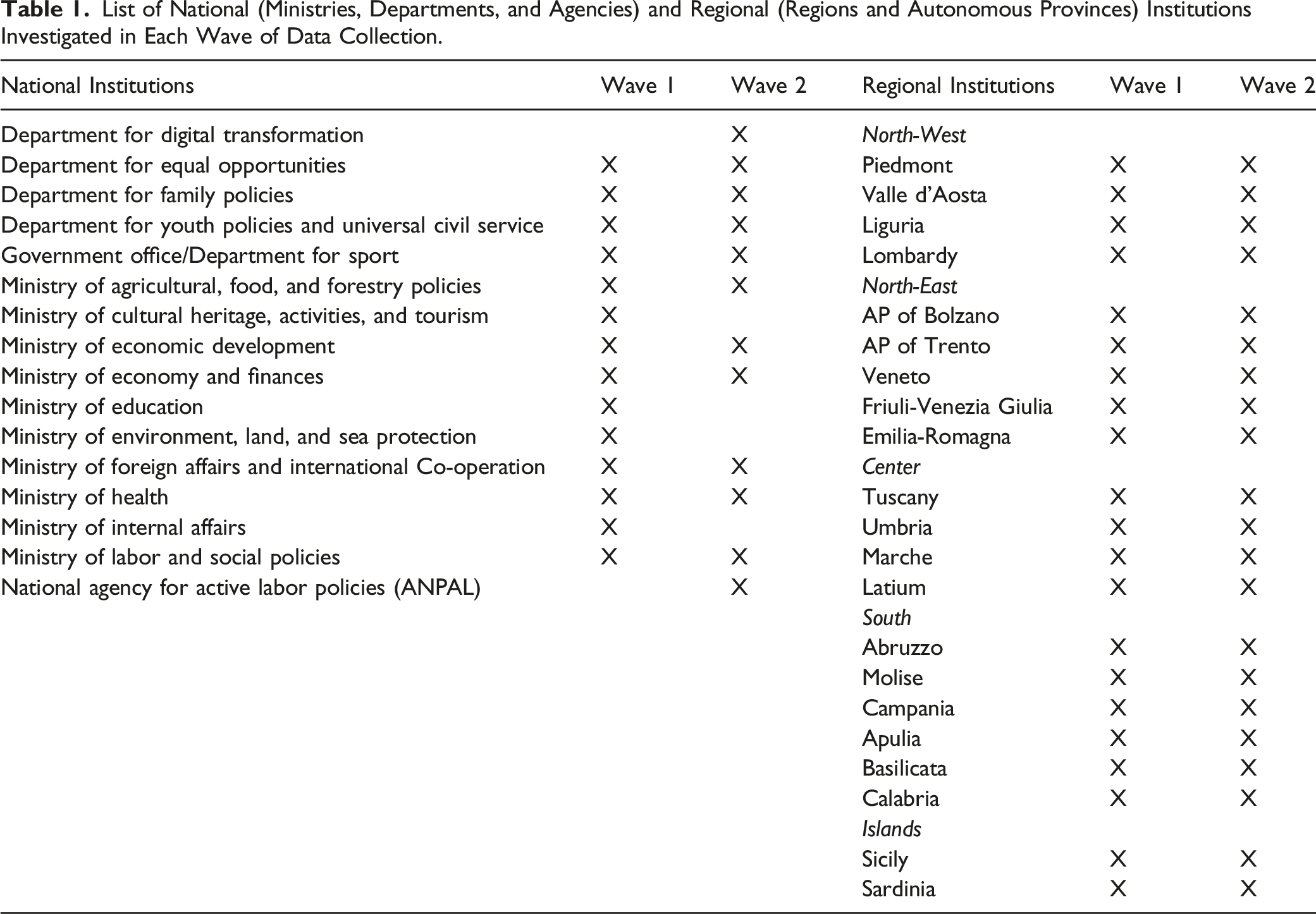
In 2020–2021, a further round of data collection (using the same methods as the first) was conducted during the first waves of the pandemic (Lucantoni, Principi, et al., 2022) involving representatives of the same national (n = 50) and regional institutions (n = 108) (with a few exceptions; see Table 1). This second round made it possible to update policy selection, also in consideration of recent societal changes in response to the pandemic.
The research team was composed of 16 trained members. Each member conducted desk and field work with one or more institutions. To maintain coherence, preliminary findings (including decisions regarding relevant materials) were discussed within the team and with one senior researcher.
Data Analysis
Researchers developed a case study report (in total, n = 68) for each national and regional 1 institution (one for the 2019 wave [see Barbabella & Principi, eds., 2020; Barbabella, Checcucci, et al., 2022] and another for the 2020–2021 wave [see Lucantoni & Principi, eds., 2022; Lucantoni et al., 2022b]), describing and analyzing the identified policies using the interview transcripts and notes and the document searches and review results.
All selected policies were grouped and organized under the nine domains of a conceptual framework 2 developed specifically to analyze the results of the overarching national project (Barbabella, Cela, et al., 2022). This conceptual framework was based on the WHO (2002) AA policy framework and incorporated elements from those international policy initiatives with direct or indirect links to AA and aging that were the most relevant for Italy: the European Regional Implementation Strategy (RIS) for the Madrid International Plan of Action on Aging (MIPAA) (UNECE, 2002), the Sustainable Development Goals (SDGs) of the Agenda 2030 (UN, 2015), and the European Pillar of Social Rights (EU 2017). The domains in our framework included “Ensuring quality of life, independent living, and health” and “Supporting informal care for older people and intergenerational solidarity.” The policies identified under these two domains were selected for this study.
On the basis of the 68 case study reports, we performed a qualitative, inductive thematic analysis of health- and care-related AA policies (as selected and described in the individual reports) in order to identify the main themes of national and regional policies (Schreier, 2012; Tonkiss, 2004; Weber, 1990). Each institution’s policies underwent an independent review by at least two researchers, who then independently assigned codes. The researchers then discussed the codes in order to reach a consensus and ensure reliability. On the basis of similarities and differences, codes and related policies were compared and grouped into themes.
Regarding the health domain, we adopted a broad definition in accordance with the WHO (2021). Health-related AA policies are those that promote health throughout the life course, with the ultimate aim of enabling better aging and maintaining satisfactory functional ability despite inevitable age-related changes.
In terms of care, we included policies designed to support the informal care provided by individuals over their life course. Care-related AA policies are therefore those that address informal care roles and activities for frail or dependent people, such as older people with LTC needs or people with disabilities. Our research did not consider policies targeting the basic health and care needs of care recipients (e.g., personal care services supporting activities of daily living and home help services).
The thematic analysis was structured on both the national and regional levels.
Results
The analysis revealed the presence of three themes at the national level and five at the regional level.
National Level
There is no national policy framework or strategy for AA or informal care in Italy. Health- and care-related policies on AA are sectorial and therefore refer to the administration of health and social care services. The public health care system is universal and based on a government-established list of well-defined health care services (latest version in the DPCM decree of January 12, 2017), which all citizens have the right to acquire through public regional health services. According to the legislative framework, the parliament and government are responsible for establishing the general guidelines and minimum levels of public services for citizens (e.g., setting national priorities and tax-funded resources for regional health care systems), while regions and APs are responsible for their organization and implementation with some autonomy (e.g., planning, organizing, and managing local health care providers and setting specific public health priorities).
National policies addressing the health and care domains within AA were grouped into the following three themes (themes 1–2 pertain to the health domain; theme 3 pertains to the care domain).
Theme 1: Health Promotion and Disease Prevention
The promotion of physical activity throughout the life course, education towards healthy behaviors and lifestyles, and empowerment for the self-management of chronic conditions are the key recurring aspects of national health promotion and disease prevention policies.
Every 5 years, the Ministry of Health prepares and issues a National Prevention Plan (Piano Nazionale della Prevenzione) to outline objectives and guidelines for implementing health promotion and disease prevention actions for the population’s benefit. A specific AA-related target was included in the National Prevention Plan 2020–2025s “active communities” program. One of its specific objectives was to implement integrated actions to increase physical activity and mitigate risk factors influencing AA and health in later life. Each region/AP incorporates the National Prevention Plan into their Regional Prevention Plans. The National Prevention Plan 2020–2025 was adopted at an early stage of the COVID-19 outbreak and includes specific actions targeting the containment of the epidemic and the strengthening of the connections between health care providers in order to create a resilient system.
“Gain Health” (Guadagnare Salute) is a national health promotion program that has been in operation since 2007 (Istituto Superiore di Sanità, 2022). Its objective is to reduce the burden of chronic conditions by addressing key health behavior determinants, such as improving diet and nutrition, promoting physical activity, advocating smoking cessation, and combating alcohol abuse. The program supports regions, APs, and stakeholders in promoting health education campaigns and activities.
Further existing initiatives to increase the participation of citizens in physical activity relate to a set of guidelines for different age groups and physiological conditions (Ministero della Salute, 2021). Moreover, the Italian National Olympic Committee (CONI) and the government office for sport issued calls for initiatives to support sport associations in attracting and involving people of all ages (including older people) in sports and group physical activity.
In Italy, national programs for disease prevention and physical activity were discontinued at the start of the pandemic.
Theme 2: Health Monitoring
In recent years, monitoring the health status of the general population and, in particular, the older age groups has been a key objective of national policies as a preparatory task to understand population health requirements and plan appropriate policy responses. The “Silver Steps” (Passi d’Argento) national surveillance program was implemented in 2016 to monitor health and behavioral risk factors associated with potential chronic diseases in the older population (65 years and older). The program supports regions/APs in collecting harmonized data and conducting periodic analyses against four risk group profiles in order to understand and address the health requirements and risk factors of older people. During the pandemic, this surveillance program was adapted to continue data collection and gather further insights on the health and social consequences of COVID-19 within the population.
Theme 3: Role and Recognition of Informal Caregivers
There is no comprehensive legislative framework for informal caregivers. Their recognition at the national level only occurred in recent years with a set of provisions incorporated into national budget laws (Law 205/2017, Art. 1, para. 254; Law 178/2020, Art. 1, para. 334). Family caregivers were defined as those who assist and care for a partner/spouse or close family member with LTC needs. The law established a National Fund for Informal Caregivers (similar to other national funds addressing other social welfare areas, such as poverty, LTC, or disability), with the intent of allocating resources for regions and APs to implement services and benefits. The National Fund has been allocated between 20 and 30 million euros annually since 2018 and was renewed and bolstered in 2020 to better support caregivers during the COVID-19 pandemic.
Law 104/1992, enacted in the early 1990s to recognize the rights of people with disabilities and their social integration, also established benefits for family caregivers, including the right to 3 days of paid leave per month for assisting a care recipient. Other, more general law proposals regarding informal caregivers were presented in parliament in recent years; however, none reached the stage of discussion or approval.
Other policy instruments, such as the National Prevention Plan or the National Plan for Chronic Diseases (Piano Nazionale della Cronicità) (Ministero della Salute, 2016), as well as calls for projects issued by various government offices (e.g., the Department for Public Administration [DFP] and the Department for Youth Policies and the Universal Civil Service) have also partially addressed the importance of the role of family caregivers. The initial initiatives fostered the involvement of caregivers and privately employed care assistants in the coordination of care by formal health and social care services. The second set of initiatives consists of funded local projects administered by public and non-profit organizations, which also support informal caregivers and work-family conciliation practices.
Regional Level
The 19 regions and 2 APs have considerable autonomy over health and social care sector policy decisions. They are able to coordinate services and benefits in accordance with the central state’s framework and guidelines. The latter also allocates financial resources to address regional population needs.
Health-and Care-Related AA Policies Adopted by the Regions and APs by Theme and Presence of General AA and Informal Care Policies.
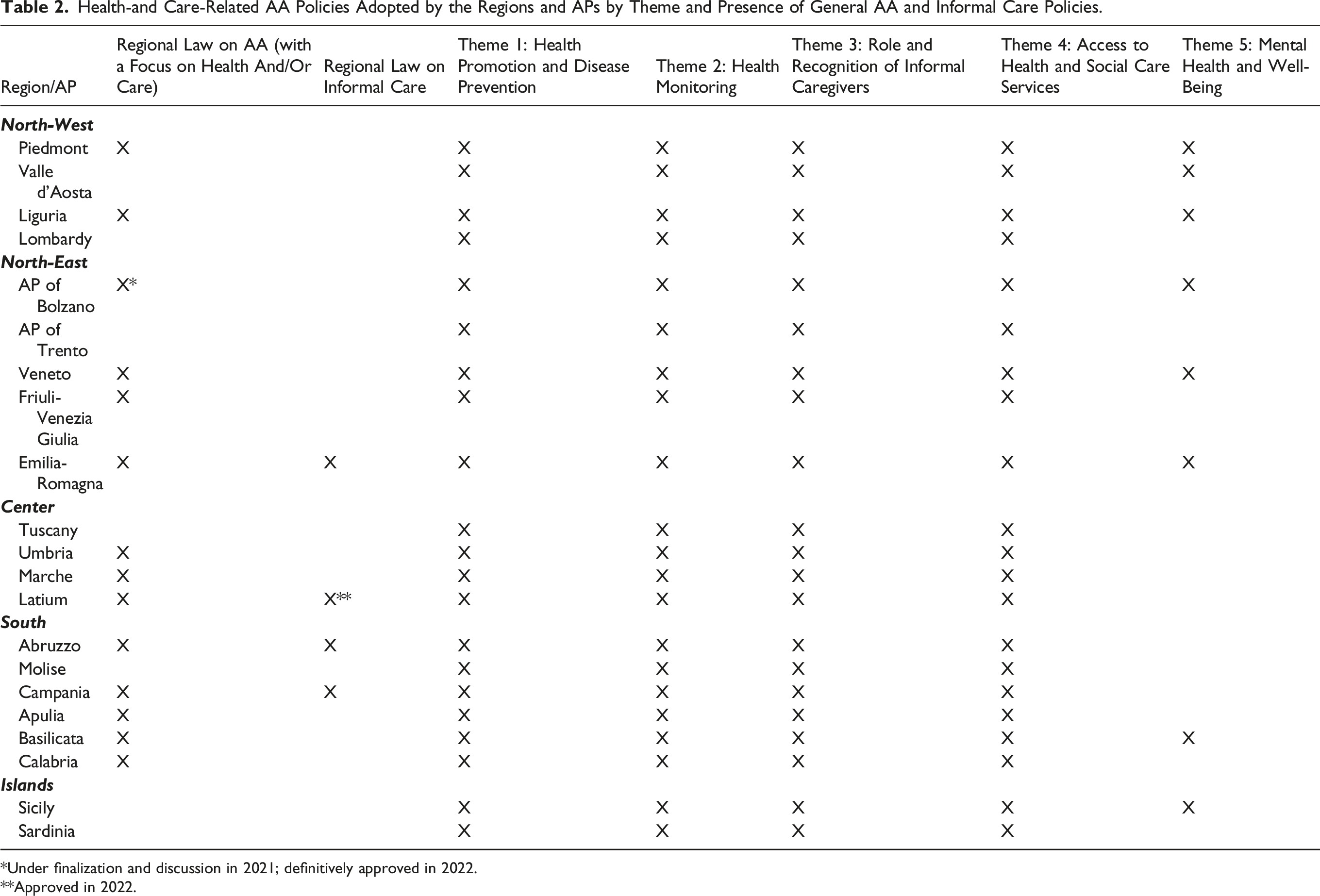
*Under finalization and discussion in 2021; definitively approved in 2022.
**Approved in 2022.
Theme 1: Health Promotion and Disease Prevention
Regional policies addressed health promotion and disease prevention in various ways. Firstly, all regions and APs adopted multiannual Regional Prevention Plans (Piani Regionali della Prevenzione), Regional Health Plans (Piani Sanitari Regionali), and Regional and Local Social Plans (Piani Sociali Regionali, Piani Sociali di Zona), 3 which are based on the priorities and guidelines set at the national level. These plans incorporated objectives, target groups, health and social care sector services, actions for promoting healthy behaviors, self-management of chronic conditions, and physical activity among the general population (throughout the life course) and within specific age groups and categories (including older people and individuals with chronic conditions). Their objectives were heavily revised since the onset of the pandemic in order to incorporate and prioritize epidemic emergency measures and a reorganization of health and social care services, for instance by reducing the number of prescribed, non-urgent examinations and increasing the availability of telehealth services.
Secondly, enhancing the quality and intensity of physical activity among the population (especially for older people and those with chronic diseases) is a key objective of a range of regional policies. In fact, certain regions (such as Tuscany, Marche, and Campania) have explicitly promoted adapted physical activity (attività fisica adattata, AFA), which is frequently provided by local health services in the form of a group activity.
Thirdly, beyond AFA, some regions and APs promoted physical activity as a recreational group activity with broader health and quality of life benefits. This could be accomplished by regions and APs either directly—for instance, by organizing walking and trekking groups for older people (such as the established programs of the Trento and Friuli-Venezia Giulia AP)—or indirectly, by financing social and recreational activities organized by local non-profit organizations.
AFA and physical activity programs were discontinued during the pandemic due to a shift in the health and social care sectors’ priorities and safety concerns in group activities.
Theme 2: Health Monitoring
All regions and APs regularly participate in the “Silver Steps” national program for monitoring the health and risk factors of the older population. Each region/AP is responsible for data collection and analysis, thus contributing to the national data pool.
During the COVID-19 outbreak, certain regions implemented additional mechanisms and technological or digital solutions to monitor the health status and needs of the older population. This was the case, for example, in the AP of Bolzano (where a proper social observatory open to local stakeholders was established), Friuli-Venezia Giulia, and Latium.
Theme 3 (Related to COVID-19): Access to Health and Social Care Services
The pandemic compelled regions and APs to adopt new tools for addressing the needs of the population to access health and social care services. All regions and APs provided new or enhanced services for the provision of health and service information by means of hotlines, mobile and online channels, and new information points in decentralized or rural areas.
In some cases, public services bolstered home help and home delivery services (e.g., for meals and drugs), although most initiatives were driven by private actors (e.g., non-profit or religious associations).
Finally, the pandemic accelerated the adoption of electronic services by public institutions, including the introduction of basic e-prescription procedures, enabling citizens to avoid in-person consultation with a general practitioner by receiving a prescription via email or text message.
Theme 4 (Related to COVID-19): Mental Health and Well-Being
The pandemic and the policy measures implemented to contain it also had a deleterious impact on the mental health and well-being of all age groups. Specific policy measures to combat this phenomenon included enhanced psychological support services in some regions (via hotlines or new physical sites in rural areas) aimed at those in greatest need, such as older people (who are typically less likely to access such services) and those suffering from physical or psychological abuse, regardless of the circumstances. Also, some regions and APs mitigated the increased risk of social isolation and related mental health issues among older people through helplines offering company, online group conversations, and other activities connecting individuals with local services and associations.
Theme 5: Role and Recognition of Informal Caregivers
After the initial formal recognition of informal caregivers at the national level (Law 205/2017) and the allocation of associated resources to regions and APs, the latter planned one or more benefits for this target group on an annual basis. At least one measure of a temporary care allowance, with amounts varying from less than 100 to 300–400 euros per month, was implemented in all regions and APs to support informal caregivers and their increased risk of income loss and social exclusion.
In the majority of cases, these care allowances were launched during the 2020-2021 pandemic to support individuals and families affected by limited mobility, restricted access to health and social services (including day and respite care), and reduced income (due to the cessation of most economic activities). During the onset of the pandemic, some regions’ local health authorities (Aziende Sanitarie Locali, ASL) and APs were able to provide caregivers with online information and training sessions, thereby ensuring a partial continuation of the service even during lockdowns or periods of restricted social contacts.
A few regions (Emilia-Romagna, Abruzzo, Campania, and Latium) adopted specific laws on informal caregivers, planning a more integrated and comprehensive set of benefits and support services for caregivers, including dedicated psychological support, recognition of professional skills as health or social care workers, information, education, and training initiatives, as well as measures to reconcile work and care commitments.
Discussion
The study provided an overview of AA health- and care-related policies and tools available in Italy, also in light of the developments during the first years of the pandemic. Three common policy themes were identified both at the national and regional levels: programs and actions for health promotion and disease prevention to sustain healthy aging throughout the life course; mechanisms for monitoring the population’s health status and risk factors, particularly in the older age groups; and measures to support informal caregivers in their role.
Health monitoring programs are crucial for understanding the health needs of a population and planning the most appropriate health promotion and disease prevention measures. Furthermore, prevention programs also have direct and indirect impacts on the level of informal caregiving required.
For regions and APs, two additional themes emerged in relation to the impact of the pandemic and related policy interventions: the realignment of health and social care services to enable access by users even in unusual circumstances, and the introduction of new or enhanced services for protecting the mental health and well-being of the population.
In Italy, AA is not considered a separate pillar within the national welfare model and is therefore subject to sectorial, non-harmonized interventions at both the national and regional levels (Barbabella, Cela, et al., 2022). Aging and older people have been prominent in policy discourse for a long time, primarily as target groups for social welfare programs providing, for instance, basic health services (such as LTC) or economic benefits (such as pensions). In recent years, policy awareness has evolved to increasingly recognize the active role and participation of older people in society (with positive benefits for both individuals and society as a whole) and the importance of tackling life-course issues for healthy AA.
Regional governments were faster to recognize this need, advancing good examples of AA policy-making either generally (e.g., regional laws on AA) or through sectorial policies. AA-related health- and care-related policies are increasingly integrated into the planning of health prevention, promotion, and monitoring programs.
Similar to what occurred in other countries and intervention areas, the pandemic affected the availability, accessibility, and quality of health and social care services. With the spread of COVID-19 and the concomitant increase in uncertainty, regional policies practically ceased programs for AA (e.g., physical activity) and initially focused on the frailest population groups. This situation progressively prompted regional governments to devise new ways for reaching users and addressing new emerging needs (Nanetti et al., 2020). Due to imposed distancing, lockdowns, quarantine measures, and meeting restrictions in general, the pandemic context exacerbated and created additional risks for the mental health and well-being of people with fewer social and economic resources, particularly older people living alone (Natilli et al., 2022; Pancani et al., 2021; Principi, Lucantoni, et al., 2022). The provision of adapted services for combating social isolation and managing mental health issues was part of a resilience mechanism implemented by regional governments, despite difficulties and delays in organizational change, implementation, and outreach to citizens (Maffeo et al., 2021; Palombi et al., 2020; Spadea et al., 2021).
The COVID-19 outbreak had a clear impact on public awareness regarding informal caregivers and their perceived relevance in society. Prior to the pandemic, only a few regions had approved policies that recognized and supported informal caregivers. The new context accentuated the frailty of the Italian welfare model and necessitated that families assume even more responsibilities and tasks due to the interruption of certain LTC services, lockdowns, and other restrictions. In 2020, all regions and APs had some form of budget available to immediately plan and organize support for informal caregivers, primarily through economic benefits and psychological services, as a result of a stimulus from the national government, which allocated resources to regions and APs specifically for informal caregivers. After a long-awaited recognition, informal caregivers are now an explicit target group of regional policies, although there is still much work to be done to develop comprehensive policies for them, as some regions (e.g., Emilia-Romagna) have begun to do.
In this context, the national project on coordinating a multi-level governance of AA policies (Barbabella et al., 2020), which was promoted by DFP and the IRCCS INRCA, was a key mechanism to continue monitoring and promoting AA even in times of health crises. AA will remain one of the key topics on the policy agenda for years to come, since a follow-up national project was launched in 2022 and a recent bill on reforming aging policies will be discussed by parliament in 2023 to enable more integrated policy interventions for LTC, AA, and informal caregivers. This reform is one of the policy milestones of the National Recovery and Resilience Plan (PNRR), which, with the support of the European Union, aims to implement massive public investments and reforms in the aftermath of the pandemic emergency.
Despite the novelty of the above findings, this study has some limitations that must be considered. First, the research team conducted primary (interviews) and secondary (document searches) data collection to identify AA policies. Despite the rigorousness of the study protocol, we cannot rule out the possibility that a few minor policies were missed during the process (due to gaps in interview data or searches). Furthermore, data collection was conducted in two phases: before the COVID-19 outbreak (2019–2020) and during the early pandemic phases (2020–2021). Therefore, AA policies or their evolution were not collected or considered after December 2021. In limited cases, the heterogeneity of data sources (individual or group interviews and document searches) and the varying quantity and quality of data available per institution may have affected the reliability of the researchers’ coding and analyses.
In spite of these limitations, this study provides a relevant contribution to knowledge on AA policies in Italy and elsewhere, as these policies are among the first to focus on the interrelationships between AA and health and care policy domains in the context of the COVID-19 pandemic. The new circumstances necessitate that researchers, practitioners, and policymakers examine how AA policies can better address the health and quality of life of aging individuals, taking into account the integration of activities and policy responses envisioned by the traditional AA framework based on the health, participation, and security pillars (WHO, 2002).
Findings from the Italian case can also be informative for other high-income countries and stakeholders interested in analyzing policies, recommending actions, and contributing to an evidence-based policy-making (EBPM) process (Davies & Nutley, 2000) for advancing AA (Barbabella, Cela, et al., 2022; Lucantoni, Principi, et al., 2022) in the context of demographic (population aging and decreasing availability of informal caregivers) and care-related trends (focus on home- and community-based services) shared by most high-income countries in Europe and North America (Chattopadhyay, 2020; Super, 2020). Our research questions and methods are transferable and adaptable for investigating the status and evolution of AA policies in other contexts from a multi-level governance perspective, thereby facilitating cross-national comparisons on these relevant issues and phenomena.
Footnotes
Acknowledgments
The authors thank the following colleagues, engaged directly in the relationships with national and regional policy makers and stakeholders during data collection: Alfredo Ferrante (DFP, Head of Unit “Family National Policies and International Relations”), Delia Amari (DFP), Maria Luisa Aversa (INAPP), Eralba Cela (IRCCS INRCA), Pietro Checcucci (INAPP), Luisa D’Agostino (INAPP), Giovanni Damiano (IRCCS INRCA), Claudia Di Matteo (IRCCS INRCA), Roberta Fefè (INAPP), Valeria Iadevaia (INAPP), Simona Rita Montagnino (DFP), Alessia Romito (INAPP), Giuliana Scarpetti (INAPP), Margherita Villa (IRCCS INRCA) and Marina Zannella (IRCCS INRCA). Furthermore, authors thank the main representative officers of national and regional institutions, as well as representatives of national and regional stakeholder organisations, involved in the data collection process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been supported by a grant of the Department for Family Policies (DFP) (1/2019 and 1/2022) at the Italian Presidency of the Council of Ministers and by Ricerca Corrente funding from the Italian Ministry of Health to the National Institute of Health and Science on Ageing (IRCCS INRCA).