
Abstract
Making home care a healthy workplace is a societal concern but research on specific interventions is still scarce. The aim of this systematic review was to provide an initial overview of interventions addressing home care workers’ health. All (quasi-) experimental studies, presenting any intervention among home care employees, and reporting any outcome related to occupational health, safety, or well-being were included. PsycArticles, Medline, PubMed, and Web of Science were searched from January 2000 to February 2022. From 16,345 publications, 18 studies with 2432 participants were included and assessed with the Joanna Briggs Institute Critical Appraisal Tools. Organizational and training/educational approaches were found in five studies each, a behavioral approach in one, and seven studies presented a combined approach. Due to methodological limitations and the heterogeneity of interventions, the existing studies are insufficient to inform new programs, but emphasize the need for tailored approaches, integrated concepts, and participatory intervention development.
• The small number and low-level evidence of existing studies indicate that research on interventions addressing home care workers’ health is still in its infancy. • The dominance of physical study endpoints shows that the biomedical perspective on health still prevails. • Currently, interventions only partially address the specific working conditions, demands, and resources of home care.
• The development of future interventions should be based on integrated concepts of occupational health, safety, and well-being. • Incorporating participatory and gender approaches can help to better target interventions and enhance their effectiveness.What this paper adds
Applications of study findings
Introduction
Population aging has been outpacing the growth of the long-term care supply in more than half of OECD countries (OECD, 2021). As part of this development, a trend toward increased demand for non-institutional care services can be observed in many Western countries. Currently home care is the fastest growing care branch (OECD, 2020) and it holds shares of up to 50% within the long-term care sector (European Commission & Social Protection Committee, 2021). As a result, the demand for home care workers in the labor market already exceeds the number of available workers (Gruber et al., 2021). The U.S. Bureau of Labor Statistics (2022) projects that this trend will continue in the coming decades. Nearly 600,000 new jobs openings are expected in the U.S. home care sector each year, and overall, the need for home care workers will increase by 33% until 2030. Thus, to attract and retain employees in the home care sector is one of the greatest future challenges (Möckli et al., 2020; OECD, 2020). In response to this situation, several countries such as Germany, the Czech Republic, and the Netherlands, have taken government measures for the long-term care sector, including home care (European Commission & Social Protection Committee, 2021). These political actions include higher staffing ratios, higher salaries, better access to training, and improved working conditions. As part of these initiatives, health insurers in Germany were legally required to fund workplace health promotion to enable care workers to remain healthy and thus in their profession for as long as possible (German Federal Ministry of Health, 2018).
The attention on the conditions under which care is provided raises the question of how home care can become a healthy workplace. This question needs to be addressed specifically for this care sector, as the unique working conditions require tailored intervention strategies (Otto et al., 2019; Schaller et al., 2021). Providing care in the private home of clients, transferring between clients’ homes, handling predetermined time budgets for every single task, and working alone within unpredictable environments represent working conditions that determine the daily working routine of home care workers (Cœugnet et al., 2016; Grasmo et al., 2021; Mojtahedzadeh et al., 2021b; Strandås et al., 2019). These characteristics appear to have a more adverse impact on caregivers' health compared to institutionalized care, as home care workers have significant worse general, physical
Recent studies have identified a wide range of health-damaging factors associated with home care work. Home care workers experience burdens most frequently related to work organization (Gebhard & Wimmer, 2022; Sjöberg et al., 2020), including staffing challenges, too tight schedules (Mojtahedzadeh et al., 2021a; Ruotsalainen et al., 2020), and the requirement to perform additional tasks on a daily basis (Karlsson et al., 2020). These conditions result in high workloads and time pressure (Fjørtoft et al., 2020; Grasmo et al., 2021; Otto et al., 2019; Sjöberg et al., 2020). Interaction
Research on health-promoting factors in home care is still in its infancy. Nevertheless, working autonomously, having varied tasks, and being able to positively impact clients' lives have already been identified as health resources in home care (de Groot et al., 2018; Kusmaul et al., 2020). Additionally, home care workers have a high level of resilience, a strong feeling of work-related meaningfulness, and experience a variety of joyful moments in their daily work live (Gebhard et al., 2022).
Health affecting factors in home care do not occur in isolation but are causally related and interact with each other (Gebhard & Wimmer, 2022). For example, time pressure is caused by organizational demands (Gebhard & Wimmer, 2022), presents a health risk in itself (Ruotsalainen et al., 2020; Sjöberg et al., 2020), increases risks for other work-related demands and injuries (Baron et al., 2022; Cœugnet et al., 2016), and leads to unhealthy behavior, such as an increased consumption of sweets and insufficient hydration (Mojtahedzadeh et al., 2021a). In addition, there are determinants of worker health that are external to, but interact with, the work context, such as socioeconomic variables or leisure time health behaviors (Sterling et al., 2021).
The diversity and complexity of factors affecting home care workers’ health require holistic intervention approaches that go beyond single intervention strategies addressing individual behavior modification or focusing solely on the prevention of work-related injuries (Syed, 2020). Integrated concepts of occupational health, safety, and well-being respond to these requirements by (1) systematically combining approaches that originate in occupational safety and health protection, and are therefore focused on risk/demand reduction and the prevention of health injuries, with health promotion strategies that aim to develop protective factors and promote well-being, (2) applying a holistic perspective on determinants of workplace health, and (3) promoting the participatory engagement of workers, particularly during intervention prioritization and planning (Motalebi et al., 2018; Punnett et al., 2020; WHO, 2010). Arguments for integrated programs range from increased effectiveness and efficient use of resources to improved sustainability of implementation (Cooklin et al., 2017; Punnett et al., 2020). The WHO Healthy Workplace framework (2010) and the U.S. National Institute of Occupational Safety's (NIOSH) Total Worker Health® program (Tamers et al., 2019) provide relevant foundations for integrated concepts.
However, research on specific interventions addressing the health of home care workers is still scarce (Neumann et al., 2021), indicating that targeted and holistic approaches to ensure and promote home care workers’ health effectively are urgently needed (Grasmo et al., 2021). Currently, it is unknown whether existing intervention studies provide evidence for the development of new programs; as to the best of the authors’ knowledge, there are no literature reviews on interventions addressing workplace health in home care. A growing body of literature reviews deals with interventions addressing care workers’ health but without specifying the work setting. Reviews focus on a variety of outcomes, such as low back pain (Van Hoof et al., 2018), obesity (Upadhyaya et al., 2020), mental health (Melnyk et al., 2020), occupational stress (Bischoff et al., 2019), burnout (de Oliveira et al., 2019), resilience (Kunzler et al., 2020), and happiness (Gray et al., 2019). Some reviews explore specific intervention approaches, such as mindfulness (Guillaumie et al., 2017), tai chi (Cocchiara et al., 2020), and physical activity interventions (Guillaumie et al., 2017). Recently, Otto et al. (2021) presented one of the few literature reviews that specifically address long-term care workers. Based on six randomized controlled trials, weak evidence that any type of intervention affects physical and mental health was found (Otto et al., 2021).
Study Aims
Since a synopsis of existing interventions is missing, a systematic review of programs and measures addressing the health of home care workers can serve as starting point for the development of targeted and holistic interventions. Consequently, the aim of this systematic review was to provide an initial overview of the literature on programs and measures focusing on home care workers’ health by determining (1) the number and regions of publications, (2) the characteristics of included participants, (3) the methodological quality of studies, (4) the participatory engagement of workers during intervention development, (5) the approaches and characteristics of interventions, (6) the study endpoints, and (7) the impact of conducted interventions.
Methods
This systematic review adhered to the updated recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement (Page et al., 2021) and was registered at the international prospective register of systematic reviews (PROSPERO 2020 CRD42020203919).
Eligibility Criteria
The elements of the PICOS framework (population, intervention, comparison, outcome, and study design) were used to define the eligibility criteria. (1) Employees of home care services, regardless of their profession or field of work were defined as the population. Studies on retired employees and employees in apprenticeships were excluded. (2) Any programs and measures focusing on occupational health, safety, or well-being were included, except those addressing clinical skills, hygiene, and infection control. (3) Any kind of control condition and studies without a control group design were included. (4) Studies reporting any outcome related to the interventions’ impact on employee’s health were included. Studies with a primary outcome among home care clients were excluded. (5) All types of quantitative experimental and quasi-experimental study designs with and without a group comparison were included.
Search Strategy
The databases APA PsycArticles, Medline, PubMed, and Web of Science were searched from January 1, 2000 to April 28, 2020. Reference lists of systematic reviews and other studies were examined for potentially eligible studies. Articles related to the study aim were used to identify appropriate keywords for the search strategy. The literature search was restricted to language (German/English), and document type (journal article). The complete search strategy used for each database is presented in Table S1_1–Table S1_3 in the Supplementary Material 1. Using the same methods, the search was updated on February 14, 2022. Titles and abstracts were transferred into the software Rayyan (Ouzzani et al., 2016). Duplicate records were identified, manually reviewed and then removed. Two researchers (DG and SB) independently reviewed all titles, abstracts and full-texts. Disagreements were resolved by discussion until consensus was obtained. If necessary, a third researcher (MH) was consulted.
Data Extraction
A data extraction form was developed, which the two review authors (DG and MH) used to extract data independently from all eligible studies. Disagreements were resolved by consensus-building discussion. The following variables were extracted: reference, country, design, participants’ characteristics, participatory intervention development, intervention approach (organizational, behavioral, training/education, combined; integrated or not integrated approach), focus of the intervention, intervention modalities, outcomes and measurements, and results. Meta-analyses could not be undertaken due to the heterogeneity of study designs, interventions, outcomes, and related measures. Thus, the evidence was synthesized narratively.
Risk of Bias Assessment
Risk of bias was assessed by two independent researchers (MH and JN) using the Joanna Briggs Institute Critical Appraisal Tools (Tufanaru et al., 2017). The 13-item checklist for randomized controlled trials assesses nine domains: randomization process, allocation concealment, similarity between groups, blinding of participants, treating groups identically, dropout, intention-to-treat analysis, reliability of outcome measures, and statistical analysis. The nine-item checklist for quasi-experimental studies includes seven domains: cause and effect, similarity between groups, control group, multiple measurements, dropout, reliability of outcome measures, and statistical analysis. Disagreements were resolved through a consensus-based discussion, or with a third reviewer (DG).
Results
A total of 16,345 publications were identified through the search, 7264 duplicates were removed. Thus, 9081 titles and abstracts were assessed for eligibility. Of those, 75 full-texts were included in further screening. Finally, 19 publications, reporting on 18 studies were included in the narrative literature synthesis. Figure 1 presents the PRISMA flowchart; the Supplementary Material 4 presents information on the excluded reports. PRISMA flowchart.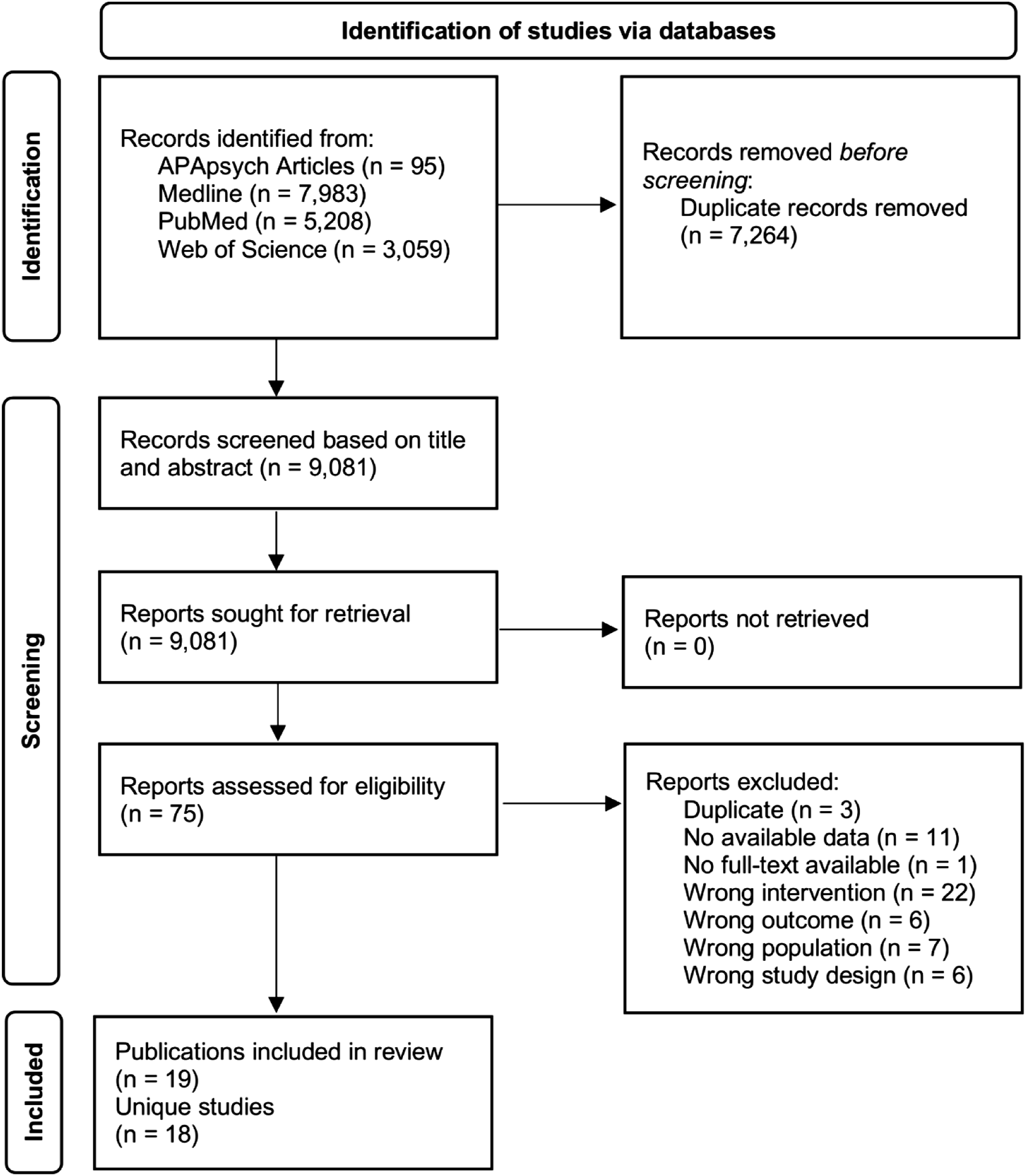
Study Characteristics
Organizational Approach.
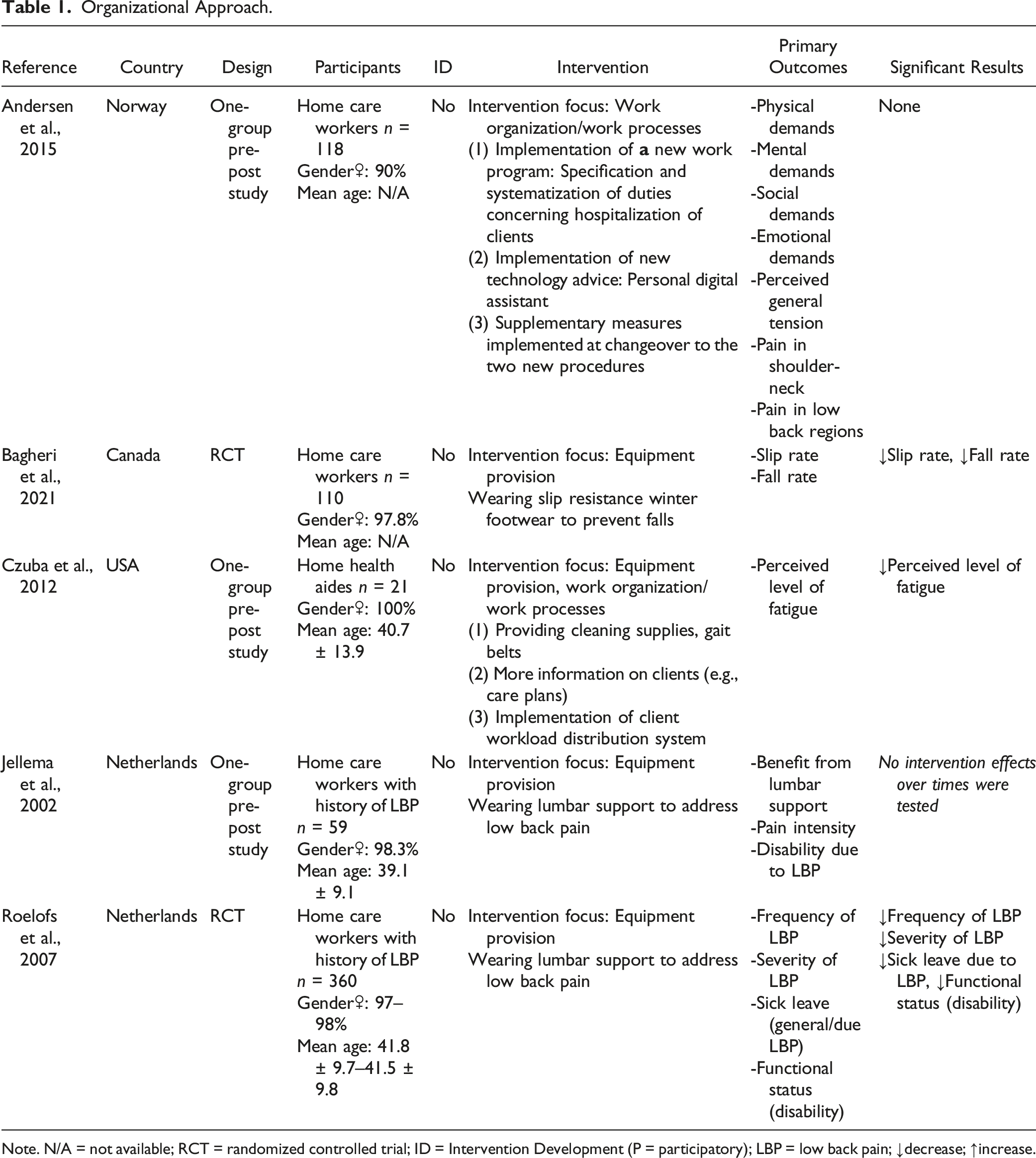
Note. N/A = not available; RCT = randomized controlled trial; ID = Intervention Development (P = participatory); LBP = low back pain; ↓decrease; ↑increase.
Behavioral Approach.
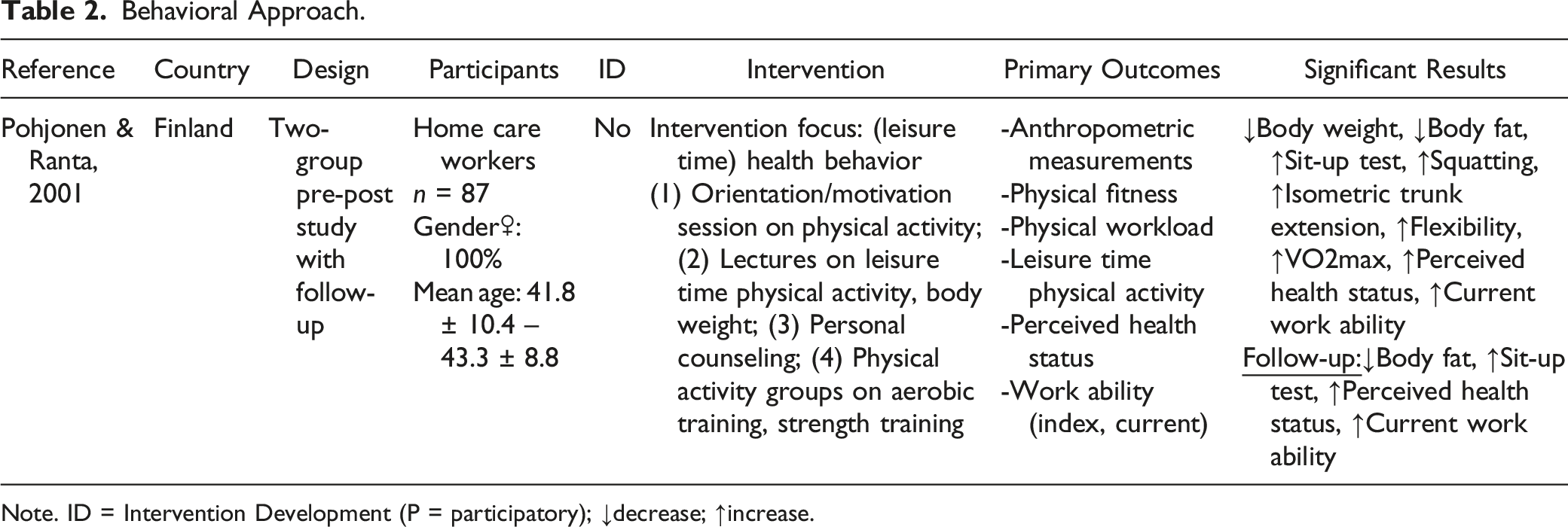
Note. ID = Intervention Development (P = participatory); ↓decrease; ↑increase.
Training/Educational Approach.
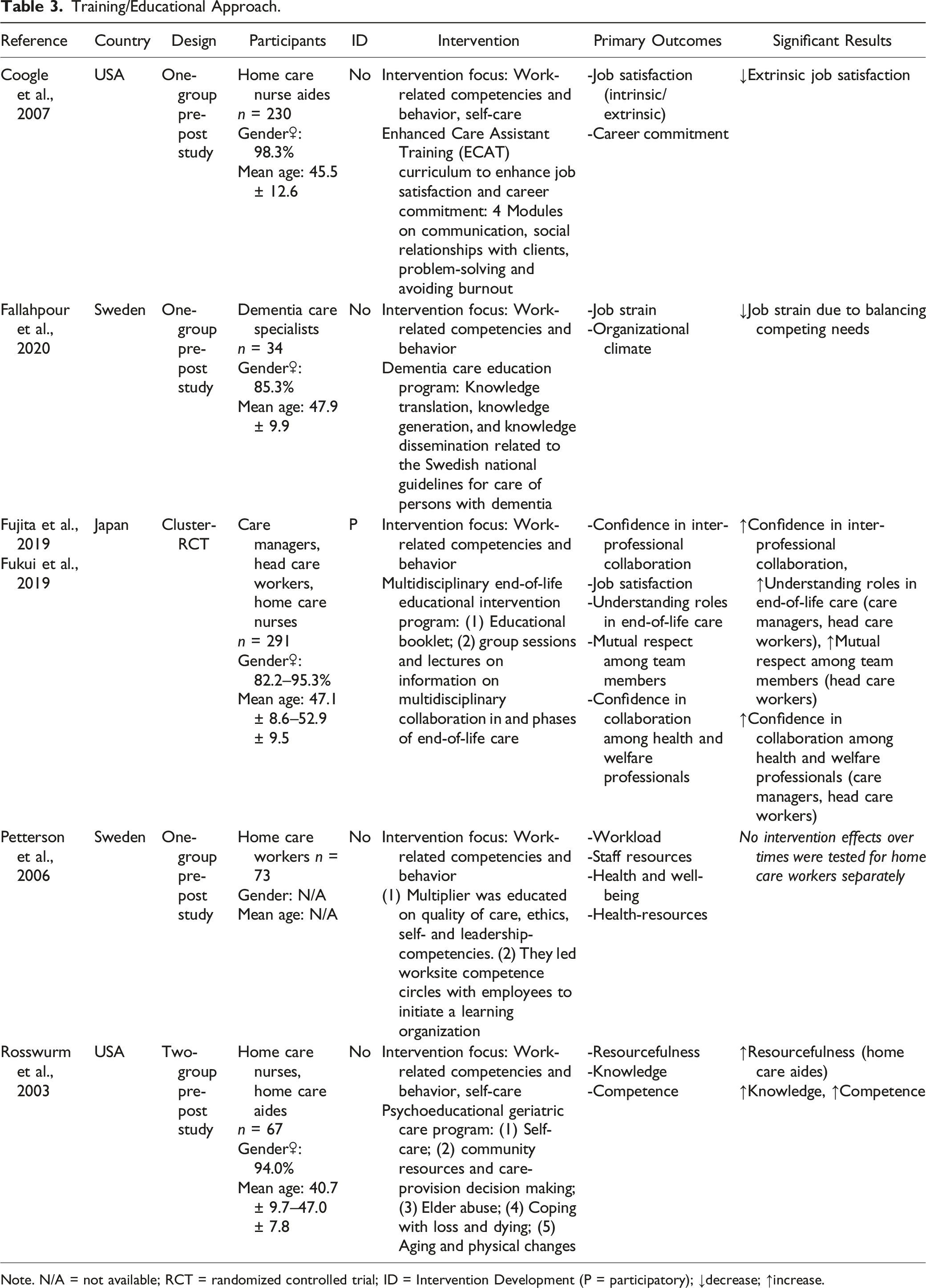
Note. N/A = not available; RCT = randomized controlled trial; ID = Intervention Development (P = participatory); ↓decrease; ↑increase.
Combined Approach.
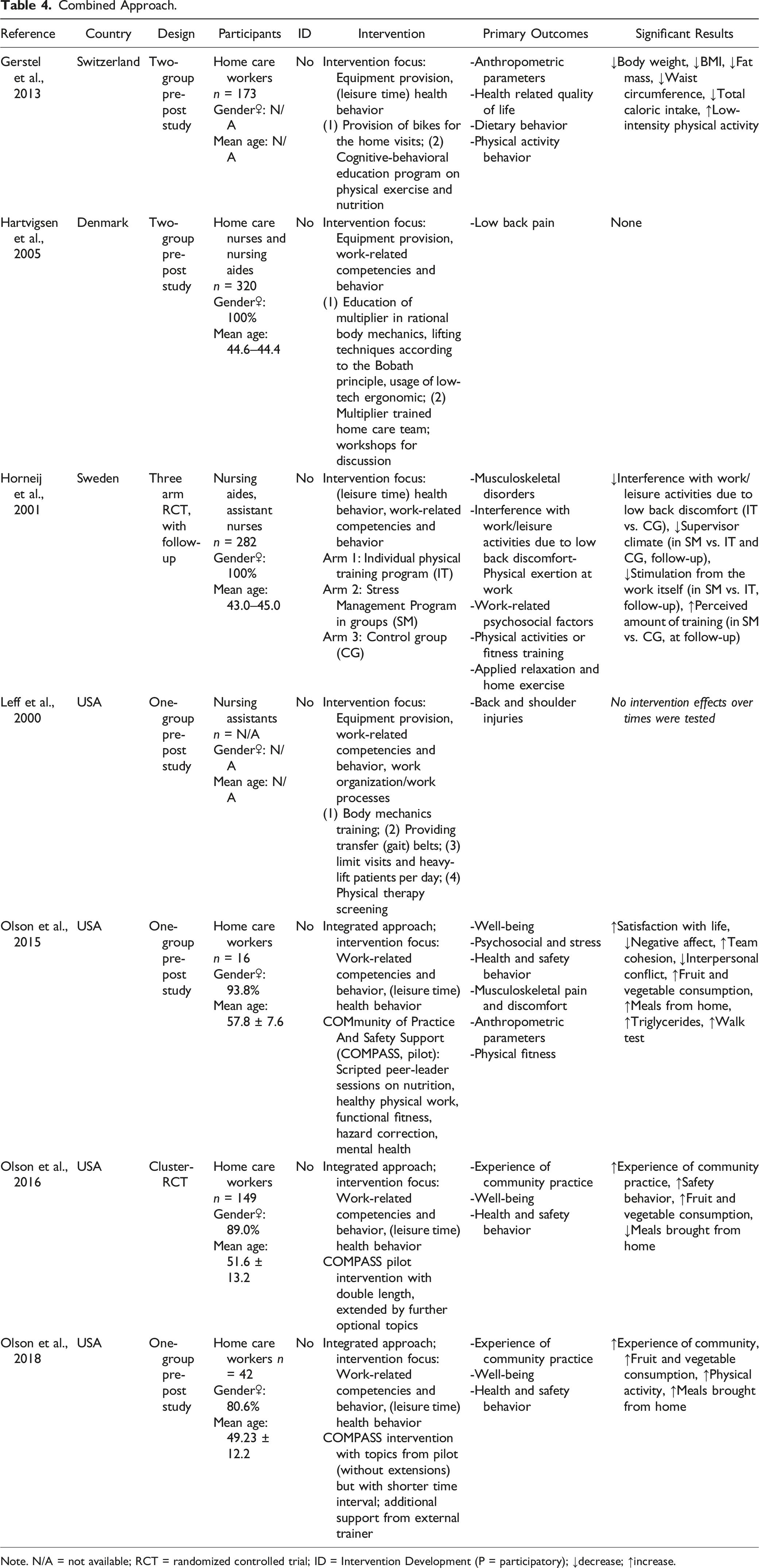
Note. N/A = not available; RCT = randomized controlled trial; ID = Intervention Development (P = participatory); ↓decrease; ↑increase.
Most of the included studies have a quasi-experimental design (n = 13). Of these, four studies conducted a control group comparison (Gerstel et al., 2013; Hartvigsen et al., 2005; Pohjonen & Ranta, 2001; Rosswurm et al., 2003), while nine studies examined the effectiveness of the intervention using a single-group pre-post design (Andersen et al., 2015; Coogle et al., 2007; Czuba et al., 2012; Fallahpour et al., 2020; Jellema et al., 2002; Leff et al., 2000; Olson et al., 2015, 2018; Petterson et al., 2006). Three studies conducted randomized controlled trials (Bagheri et al., 2021; Horneij et al., 2001; Roelofs et al., 2007); in two studies, a cluster randomization was executed (Fujita et al., 2019; Fukui et al., 2019; Olson et al., 2016). The results from the quality assessment are presented in the Supplementary Material 2 (for quasi-experimental studies in Table S2_1; for RCTs in Table S2_2).
Home care workers were most frequently targeted (n = 7) without specifying role, occupation, or pre-existing conditions. All studies, which reported on gender (n = 15) had a significantly higher proportion of female participants, with a range between 80.6% (Olson et al., 2018) and 100% (Czuba et al., 2012; Hartvigsen et al., 2005; Horneij et al., 2001; Pohjonen & Ranta, 2001). In 17 studies, the number of participants was reported with a total of 2432. The number of participants ranged from 16 (Olson et al., 2015) to 360 (Roelofs et al., 2007) with a mean of 143. Participants were on average between 39.1 years (Jellema et al., 2002) and 57.8 years (Olsen et al., 2015) old.
Interventions
One study was developed with the participation of home care workers (Fujita et al., 2019; Fukui et al., 2019), as the booklet used in the intervention was developed based on focus group interviews.
Five studies examined an organizational approach. One study addressed work organization/work processes (Andersen et al., 2015); in three studies, equipment to prevent injuries /reduce the risk of health hazards was provided (Bagheri et al., 2021; Jellema et al., 2002; Roelofs et al., 2007); and in one study, the provision of equipment was combined with changing work organization/work processes (Czuba et al., 2012).
Five studies conducted trainings/applied an educational approach. They all focused on work-related competencies and behaviors (Coogle et al., 2007; Fallahpour et al., 2020; Fujita et al., 2019; Fukui et al., 2019; Petterson et al., 2006; Rosswurm et al., 2003).
One study applied a behavioral approach (Pohjonen & Ranta, 2001) that focused on leisure time physical activity and used the worksite only as a venue for the program delivery.
Seven studies implemented a combined approach. Three studies (Olson et al., 2015, 2016, 2018) combined a behavioral approach, focusing on leisure time health behaviors with training/educational approaches, focusing on work-related competencies and behaviors. Two studies combined organizational and training/educational approaches (Hartvigsen et al., 2005; Leff et al., 2000). In both studies, equipment to prevent injuries/reduce the risk of health hazards was provided in combination with the training of lifting/transfer techniques. Gerstel et al. (2013) combined organizational and behavioral approaches, as they provided bicycles for home visits and implemented an exercise and nutrition program. Horneij et al. (2001) applied a behavioral approach, and training/education was conducted. However, the approaches were not directly combined in Horneij et al.’s (2001) intervention because they were conducted in different study arms.
An integrated concept of occupational health, safety, and well-being was only applied in the COMPASS program (Olson et al., 2015, 2016, 2018). The program targets safety and health behavior changes together and refers to the NIOSH Total Worker Health® program as its foundation. Brief descriptions of all interventions are provided in Tables 1–4, extended descriptions are presented in Supplementary Material 3 in Table S3_1.
Outcomes
Six studies defined general health/well-being/quality of life as main outcomes (Gerstel et al., 2013; Olson et al., 2015, 2016, 2018; Petterson et al., 2006; Pohjonen & Ranta, 2001). Across all studies, physical parameters were most commonly defined as primary outcomes (n = 11), with pain measured most frequently (n = 6; Andersen et al., 2015; Hartvigsen et al., 2005; Horneij et al., 2001; Jellema et al., 2002; Olson et al., 2015; Roelofs et al., 2007). Psychosocial and mental parameters were defined as primary outcomes in four studies (Andersen et al., 2015; Fallahpour et al., 2020; Olson et al., 2015; Petterson et al., 2006).
Occupation-related outcomes, such as job satisfaction, career commitment, and organizational climate were reported in four studies (Coogle et al., 2007; Fallahpour et al., 2020; Fujita et al., 2019; Fukui et al., 2019; Petterson et al., 2006). The same number of studies examined the impact of interventions on social support and cooperation (Fujita et al., 2019; Fukui et al., 2019; Olson et al., 2016, 2018; Petterson et al., 2006). One study reported on work ability (Pohjonen & Ranta, 2001) and one on sick leave (Roelofs et al., 2007).
Health and safety behavior were examined in six studies (Gerstel et al., 2013; Horneij et al., 2001; Olson et al., 2015, 2016, 2018; Pohjonen & Ranta, 2001). Two studies explicitly included (health) resource-oriented primary outcomes (Petterson et al., 2006; Rosswurm et al., 2003), such as self-esteem, self-control, and coping. All primary outcomes are presented in Tables 1–4. Further details on endpoints and their measurement are provided in the Supplementary Material 3, Table S3_1.
Effectiveness of Interventions
An improvement in general health/well-being/quality of life was only observed in one intervention that applied a behavioral approach (focusing on leisure time physical activity) (Pohjonen & Ranta, 2001). Although this result refers only to perceived health status measured by a single item, the effect appears to be stable over the 5-year follow-up period. All organizational interventions that provided equipment to prevent injuries/reduce the risk of health hazards showed a significant positive impact on (low back) pain, disability, or injury (Bagheri et al., 2021; Czuba et al., 2012; Roelofs et al., 2007). Only one study showed significant improvements in psychosocial and mental parameters (Fallahpour et al., 2020).
No intervention proved effective in terms of occupation-related outcomes. In contrast, all studies presenting results on social support or cooperation showed positive effects (Fujita et al., 2019; Fukui et al., 2019; Olson et al., 2016; 2018), but with the limitation that multidisciplinary cooperation interventions seemed to affect the management level rather than the direct care workers (Fujita et al., 2019; Fukui et al., 2019). A reduction in sick leave or an increase in the work ability index was not observed (Pohjonen & Ranta, 2001; Roelofs et al., 2007).
Health and safety behavior could be positively influenced by combined approaches. The combination of organizational and behavioral approaches (Gerstel et al., 2013) appears to be effective in positively influencing physical activity and dietary behaviors while improving anthropometric parameters. The COMPASS interventions (Olson et al., 2015, 2016, 2018), which use a combination of behavioral and training/educational approaches, also increased fruit and vegetable consumption, and in the latest version of the intervention even physical activity. The safety behavior was significantly increased by the first version of the COMPASS program (Olsen et al., 2016).
Studies exploring the impact on (health) resource-oriented primary outcomes showed mixed results. One intervention appears to positively affect home care aides but not home care nurses (Rosswurm et al., 2003), and the second intervention leads to improvements in self-esteem and coping but not in mastery (Petterson et al., 2006; significance of the change was not tested statistically).
All statistically significant results related to the primary endpoints are presented in Tables 1–4. Further results are presented in Supplementary Material 3, Table S3_1.
Discussion
The aim of this systematic review was to provide an initial overview of the literature on interventions addressing the health of home care workers. Over the last two decades, a relatively small number of 18 studies have been conducted, most of which used a one-group quasi-experimental study design and showed mixed results in assessing risk of bias. Thus, the need for high-quality studies on health interventions for care workers (e.g., Bischoff et al., 2019; Otto et al., 2021; Van Hoof et al., 2018) can also be confirmed for the home care sector. Because implementing experimental research designs in workplaces entails unique challenges, the use of cluster randomization and stepped-wedge designs is recommended as feasible and valid (Tamers et al., 2018) and appears to be well suited for investigating workplace interventions in home care.
Physical parameters dominate the endpoints of included studies, indicating a still predominant biomedical perspective on health. Since psychosocial and mental demands characterize everyday work in home care (Grasmo et al., 2021; Ruotsalainen et al., 2020) and are reported as burdening much more frequently than physical strains (Gebhard & Wimmer, 2022), interventions must broaden their approach to a biopsychosocial perspective. A review indicated that mindfulness trainings have a positive effect on the mental health of nurses (Guillaumie et al., 2017). Melnyk et al. (2020) showed that even brief mindfulness interventions focused on gratitude and deep breathing were beneficial, an approach that would be particularly suitable for home care workers without additional time expenditure while driving to clients. Nevertheless, this behavioral approach is not far-reaching enough to holistically address the mental health of home care workers, as the root cause of stress lies on organizational and structural levels (Fjørtoft et al., 2020; Grasmo et al., 2021; Otto et al., 2019; Sjöberg et al., 2020). However, interventions that improve home care workers' psychosocial or mental health through organizational/structural approaches could not be identified in this review, as the only intervention with this focus (Andersen et al., 2015) did not show significant results.
Independent of endpoints, this review shows that the majority of interventions provide individual oriented approaches focusing on work-related competencies and behavior and (leisure time) health behavior. This is in accordance with the intervention landscape across the entire field of occupational health (Faller, 2021). Nevertheless, two included RCTs (Bagheri et al., 2021; Roelofs et al., 2007) indicated that organizational interventions providing equipment, such as slip resistance winter footwear and lumbar support belts are effective in reducing (low back) pain, and preventing injury. These findings extend the range of interventions identified by Van Hoof et al. (2018) to reduce low back pain in nurses. The supply of equipment also proved beneficial related to other outcomes in this review, as the provision of bicycles for home visits in combination with a cognitive-behavioral education influenced physical activity and dietary behavior positively, and improved anthropometric parameters (Gerstel et al., 2013). Gerstel et al.’s (2013) study showed that integrating physical activity into existing processes/activities can be a feasible and effective approach, as lack of time has been shown to be the main barrier to health behavior change among nurses (Chong & Shorey, 2022). A similar approach can be found in the study from Muramatsu et al. (2017). In this study, home care workers delivered a physical activity intervention to their clients and experienced changes in physical activity behavior themselves (Muramatsu et al., 2017).
Such interventions, which are specifically tailored to the specific working conditions, demands, and resources of home care, are hardly found in the included studies. Additionally, the included studies were not tailored to the characteristics of the participants, who were predominately female and had a relatively high average age, as none of the included interventions addressed gender issues or took a life course approach. This result is in line with the findings of Jiménez-Mérida et al. (2021), which have shown that the proportion of publications on workplace health promotion measures aimed specifically at women is very low (1.9%). Gender-related interventions that address specific aspects of women’s health throughout working life, such as premenstrual syndrome and breastfeeding in younger ages, or menopause and reducing the risk of osteoporosis in older age, are urgently needed in the female-dominated work sector of home care (Crawford et al., 2016; Jiménez-Mérida et al., 2021). The inadequate tailoring of interventions may be related to the lack of participation of home care workers in the development of the interventions, as the present review identified only one study using a participatory approach. Participatory intervention development could not only promote tailoring of interventions, but also enhances their impact on health (Brand et al., 2017). Thus, in accordance with Otto et al. (2021) participatory approaches can strongly be recommended for future studies.
Only the COMPASS interventions (Olson et al., 2015, 2016, 2018) were based on an integrated concept of occupational health, safety, and well-being. This suggests that integrated approaches to worker health are not yet established in home care, which is consistent with the findings of Neumann et al. (2021), who examined the types of interventions offered to home care workers. However, Syed (2020) advocates for integrated approaches in long-term care that also improve social and material circumstances. Kotejoshyer et al. (2019) provide valuable insights into how an integrated intervention in long-term care can be developed and implemented, and what barriers need to be considered in the process. These pioneering studies can serve as a starting point for the development of interventions that have a holistic understanding of the determinants of health of home care workers.
Strengths and Limitations
The greatest strength of the study is that it is the first systematic review dealing with interventions addressing the health of home care workers. Thus, it provides a unique overview of the literature in this field. The main limitations of the study are related to the methodological shortcomings of the included studies, the heterogeneous characteristics of the interventions, and different endpoints and measures used, which restricts the identification of effects for any intervention or the preference for a particular intervention approach.
Conclusion
The literature currently includes 18 studies on interventions addressing the health of home care workers. The existing studies provide limited guidance for new programs, but point to some shortcomings from which recommendations for the development of future interventions can be derived. Future studies should (1) draw on the biopsychosocial understanding of health, (2) develop interventions with participation of home care workers, (3) incorporate age and gender-specific components, (4) consider working conditions, demands and resources specific to home care, (5) implement integrated concepts of occupational health, safety, and well-being, and (6) investigate the effect of interventions using feasible experimental research designs.
Supplemental Material
Supplemental Material - How to Address the Health of Home Care Workers: A Systematic Review of the Last Two Decades
Supplementary Material for How to Address the Health of Home Care Workers: A Systematic Review of the Last Two Decades by Doris Gebhard and Michael Herz in Journal of Applied Gerontology.
Footnotes
Acknowledgments
The authors would like to thank Sabina Bösl (SB) for screening the studies and Julia Neumann (JN) for assessing the risk of bias of the included studies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.