
Abstract
California’s In-Home Supportive Services (IHSS) program provides vital home care to low-income consumers, some of whom live with Alzheimer’s disease or related dementias (ADRD). Yet, most IHSS caregivers receive little or no training in dementia care. We present preliminary descriptive results of the IHSS + ADRD Training Project, a 10-week, competency-based, dementia training program, delivered online, for IHSS caregivers, in Alameda County. Increase in dementia knowledge and self-efficacy at training completion supports the importance of continuing and expanding this work.
• This paper adds to existing literature that new educational training models that use online and remote strategies can enhance IHSS caregivers’ dementia knowledge and skills to work with consumers living with ADRD. • Our findings have implications for increased funding and training opportunities to bolster the roles and capacity of IHSS caregivers, especially as the prevalence of ADRD and the need for dementia-trained home care workers increases locally and statewide.What this paper adds
Applications of study findings
Successfully supporting people with Alzheimer’s disease and related dementias (ADRD) to live safely at home requires assistance from home care workers. In-Home Supportive Services (IHSS) caregivers are a type of home care worker directly hired by consumers of California’s Medi-Cal-funded IHSS program. Approximately, 550,000 IHSS caregivers provide custodial care and/or paramedical services to 650,000 IHSS consumers, the majority of whom are older adults (California Department of Social Services, n.d.). With ADRD prevalence among Californians age 55+ projected to increase 127% by 2040, reaching over 1.5 million people (Ross et al., 2021), the IHSS consumer population with ADRD will likely increase at a similar rate, amplifying the need for dementia-trained home care workers.
Since IHSS caregivers spend intimate time with consumers, they have the opportunity to observe changes in their consumer’s cognition, health, or behaviors to report to other family members or care team members. Caring for a consumer with ADRD is complex and can be physically and emotionally taxing. In-Home Supportive Services caregivers may be under-equipped to help consumers cope with environmental challenges (e.g., prevent wandering), manage comorbidities (e.g., diabetes), and may feel distress if/when expected to act as surrogate decision-makers (Parker et al., 2022; Sheehan et al., 2021). In-Home Supportive Services caregivers were essential workers during the Coronavirus Disease (COVID-19) pandemic (Espinoza, 2022), providing extended support during shelter-in-place, helping consumers prevent viral spread (e.g., masking and handwashing), and likely missing respite when their consumer would have been at an adult day program.
In-home supportive services caregivers have immense capacity to influence their consumer’s quality of care and reduce healthcare utilization (Newcomer et al., 2018). Without home care, many people with ADRD would have to live in costly institutions, such as nursing homes (Cook, 2017). Yet, IHSS caregivers remain an underutilized and undervalued resource in our long-term care system—most are hired family members (70%), they constitute a marginalized workforce composed of women (81%) and people of color (72%), receive minimal training or supportive supervision, and earn approximately US$16/h (California Department of Social Services, n.d.). Little is known about whether and how training could better support IHSS caregivers to thrive in their roles. Burgeoning research suggests that training programs are urgently needed, especially as the number of Californians with ADRD is projected to double by 2040 (Guerrero et al., 2020; Polacsek et al., 2020; Ross et al., 2021).
Methods
The goal of the IHSS + ADRD Training Project is to implement and evaluate a 10-week dementia training program for 600 IHSS caregivers in Alameda County, California, by 2024. The curriculum contains 35-hours of content developed by the Center for Caregiver Advancement (CCA), a non-profit organization founded by home care workers (Guerrero et al., 2020). The project aims to increase IHSS caregivers’ dementia knowledge and self-efficacy to maximize care they provide to consumers.
Project funding and implementation began just prior to the onset of the COVID-19 pandemic. Consequently, the training launch was delayed by 6 months. In-person training pivoted to online training via Zoom, a video-conferencing platform, to comply with social distancing mandates.
This brief report presents preliminary results from the first cohort of IHSS caregivers who participated in the online training from September 2020 to March 2021. We used a quasi-experimental, longitudinal design.
Participants
The Center for Caregiver Advancement recruited eligible IHSS caregivers through mailers, phone, text, internet, and social media outreach. Eligibility for IHSS caregivers included: age 18+, English-speaking, and hired by an IHSS consumer who is age 50+, has a score of 2+ on the Washington University Dementia Screening Test (AD8), and is a member of Alameda Alliance for Health (a local Medi-Cal managed care plan).
Consent was obtained from IHSS caregivers and consumers or a designated power of attorney. Among 187 IHSS caregivers who initially enrolled, 95 withdrew or deferred participation and 92 completed the training when it relaunched as an online program 6 months later due to COVID-19 (Figure 1). Reasons for withdrawal or deferral included pandemic uncertainties; fraud, scam, or privacy concerns; technology barriers; illness; or the enrolled IHSS consumer died or no longer lived at home (e.g., placed in a facility), thereby disqualifying the caregiver. IHSS caregiver participant flow diagram.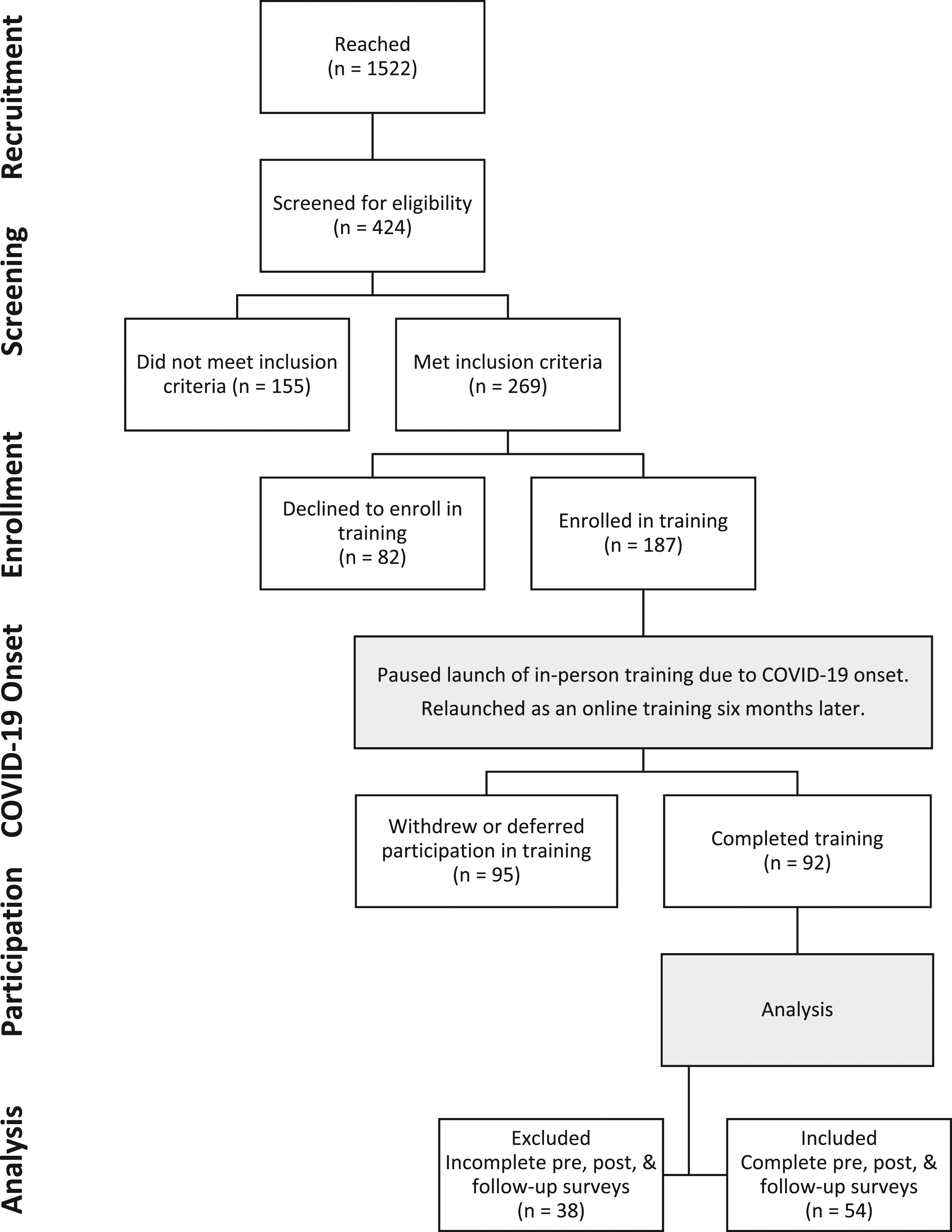
Data Collection
Overall Number and Percentage of Mail-and-Return Versus Qualtrics Surveys Received.

Measures
The Washington University Dementia Screening Test (AD8) is a valid screening measure that differentiates between signs of normal cognition and mild dementia, which is completed by an informant (e.g., caregiver), the preferred administration method. It includes eight statements with response options of Yes/No/Don’t Know or N/A. Two or more “Yes” responses indicate cognitive impairment is likely present. The
The Dementia Knowledge Assessment Tool 2 (DKAT2) is a valid self-assessment of dementia knowledge and includes 21 statements, with response options of Yes/No/Don’t Know. The more statements correctly answered indicates better dementia knowledge. The DKAT2 has a reliability coefficient of α = 0.79 (Toye et al., 2014).
The Caregiver Self-Efficacy Scale includes 10 statements, with a 1–10 rating scale, clustered into two domains: “Symptom Management” (5 statements; 5–50 score range) and “Community Support Service Use” (4 statements; 4–40 score range). One statement—“find ways to pay for services”—did not load into either domain. The domains have reliability coefficients of α = 0.77 and α = 0.78, respectively (Fortinsky et al., 2002).
The Caregiver Self-Assessment Questionnaire (CSAQ) is a valid self-report screening measure sensitive for detecting distress and includes 18 statements. The first 16 statements have Yes/No response options followed by two statements with a 1–10 rating scale. Chances of experiencing high distress are true if any of these criteria are met—(a) “Yes” is answered to either or both statements #4 and #11, (b) total “Yes” response is 10 or more, or (c) statements #17 or #18 score 6 or higher. The CSAQ has a reliability coefficient of α = 0.82 (Epstein-Lubow et al., 2010).
The Patient Health Questionnaire-2 (PHQ-2) is a valid self-report depression screener and includes two questions, with a 0–3 rating scale (Kroenke et al., 2003). The possible score range is 0–6, and a score 3+ has sensitivity for depressed mood over the past 2 week. The PHQ-2 had a reliability coefficient of α = 0.76 in an earlier study (Maroufizadeh et al., 2019).
Analysis
Quantitative data were analyzed in Stata/SE 17. To compare demographics between the groups included and excluded for analysis, we performed chi-square tests. To compare changes in dementia knowledge and self-efficacy, we performed repeated measures univariate Analysis of Variance (ANOVA), with post-hoc comparisons adjusted by the Bonferroni test. An alpha value of 0.05 was used to consider differences statistically significant. Demographics, distress, depression, and training satisfaction were summarized with descriptive statistics.
Results
IHSS Caregiver Characteristics.
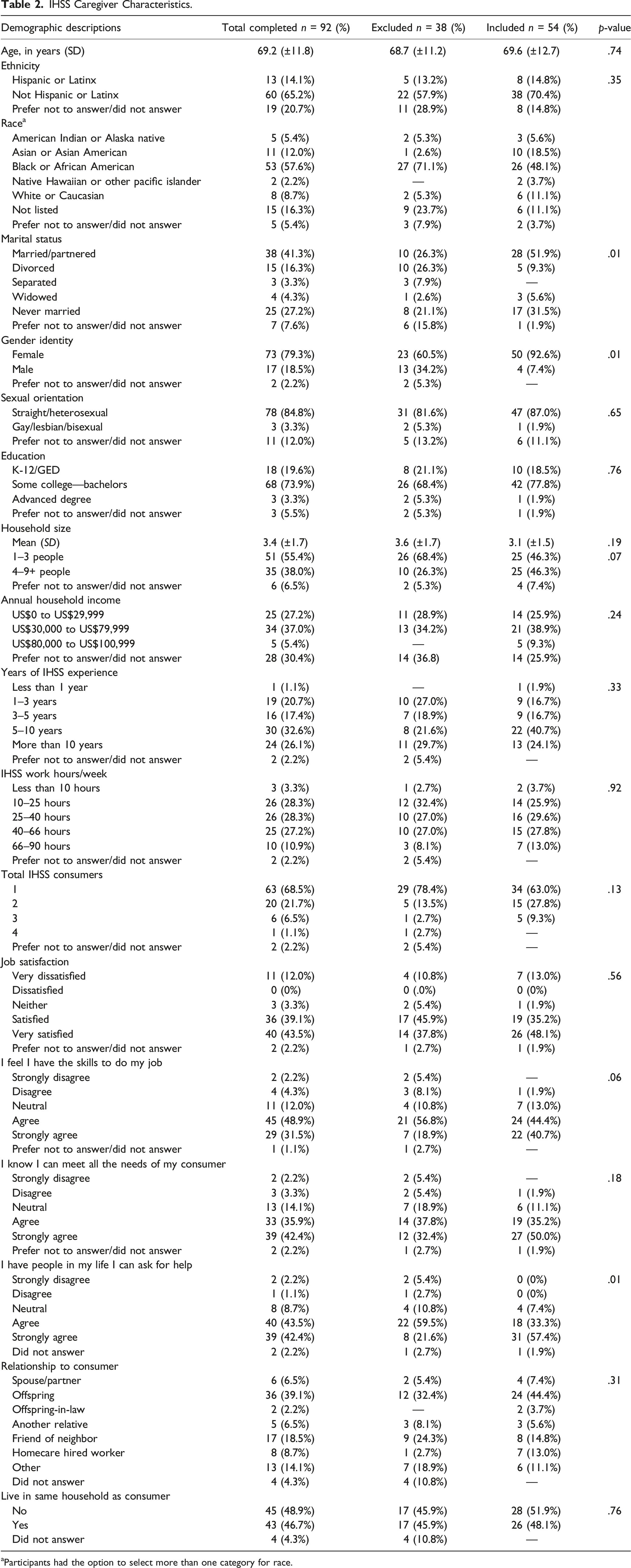
aParticipants had the option to select more than one category for race.
Among the 54 IHSS caregivers included for analysis, 70% were not Hispanic/Latinx, 48% Black/African American, 52% married/partnered, 93% female, and 87% straight/heterosexual. Average age was 69 (±12.7). Most had 5–10 years of IHSS experience (41%), worked for IHSS 25–40 hours/week (30%), cared for one IHSS consumer (63%), were very satisfied with their job (48%), agreed they have skills to do their job (44%), strongly agreed they know how to meet their consumer’s needs (50%) and have people in their life they can ask for help (57%). Most were the offspring of (44%) and did not live in the same household as their consumer enrolled in this program (52%).
Knowledge
Mean and Standard Deviation of the Dementia Knowledge Assessment Tool (DKAT2) and Caregiver Self-Efficacy Scale Scores.
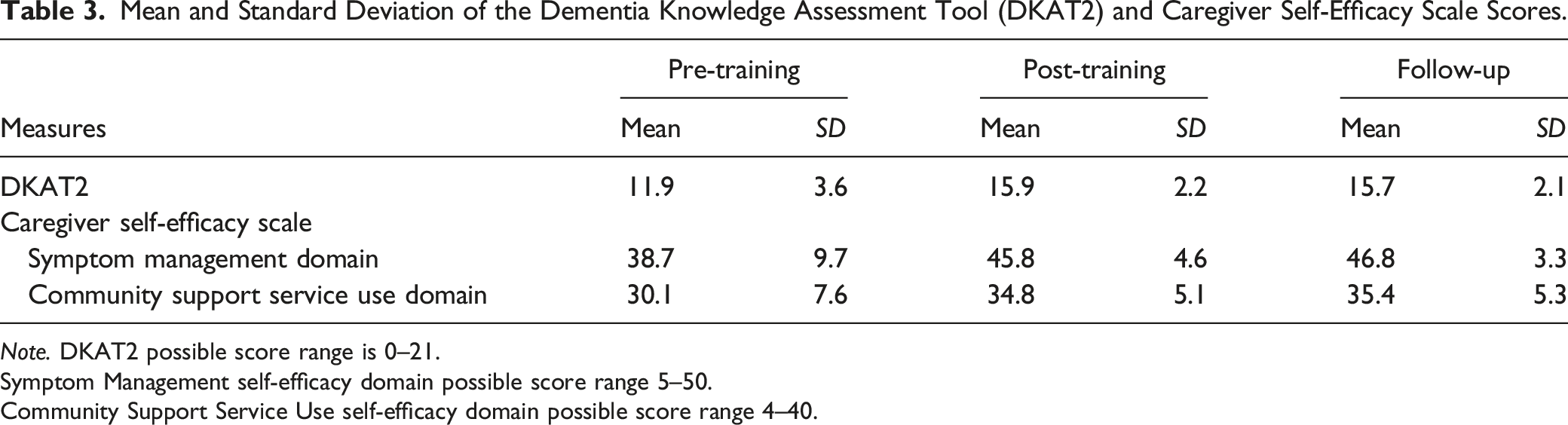
Note. DKAT2 possible score range is 0–21.
Symptom Management self-efficacy domain possible score range 5–50.
Community Support Service Use self-efficacy domain possible score range 4–40.
Repeated Measure Univariate Analysis of Variance (ANOVA) Results of the Dementia Knowledge Assessment Tool (DKAT2) Scores.

Abbreviation: DF, Degrees of freedom; G–G, Greenhouse–Geisser epsilon; H–F, Huynh–Feldt epsilon.
Pairwise Comparisons of Marginal Linear Predictions of the Dementia Knowledge Assessment Tool (DKAT2) Scores.

Self-Efficacy
Repeated Measure Univariate Analysis of Variance (ANOVA) Results of the Caregiver Self-Efficacy Scale Symptom Management Domain Scores.

Abbreviation: DF, Degrees of freedom; G–G, Greenhouse–Geisser epsilon; H–F, Huynh–Feldt epsilon.
Pairwise Comparisons of Marginal Linear Predictions of the Caregiver Self-Efficacy Scale Symptom Management Domain Scores.

Repeated Measure Univariate Analysis of Variance (ANOVA) Results of the Caregiver Self-Efficacy Scale Community Support Service Use Domain Scores.

Abbreviation: DF, Degrees of freedom; G–G, Greenhouse–Geisser epsilon; H–F, Huynh–Feldt epsilon.
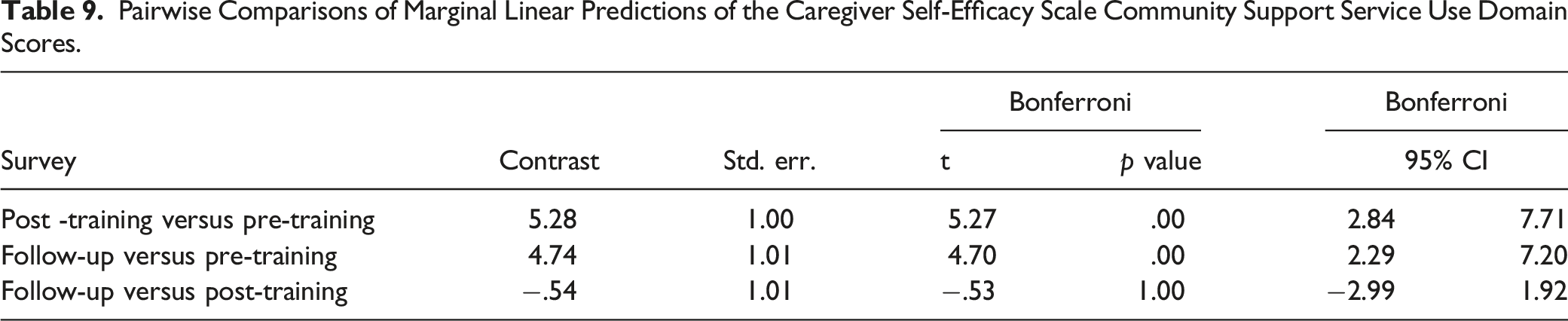
Pairwise Comparisons of Marginal Linear Predictions of the Caregiver Self-Efficacy Scale Community Support Service Use Domain Scores.
Distress
IHSS Caregivers Who Screened Positively for Distress on the Caregiver Self-Assessment Questionnaire (CSAQ) and Depression on the Patient Health Questionnaire-2 (PHQ-2), n = 54.

Note. Significance testing was not conducted.
Depression
PHQ-2 scores indicated that 7% of IHSS caregivers were experiencing depressed mood at pre-training, compared to 11% at post-training and 6% at follow-up (Table 10). Significance testing was not conducted.
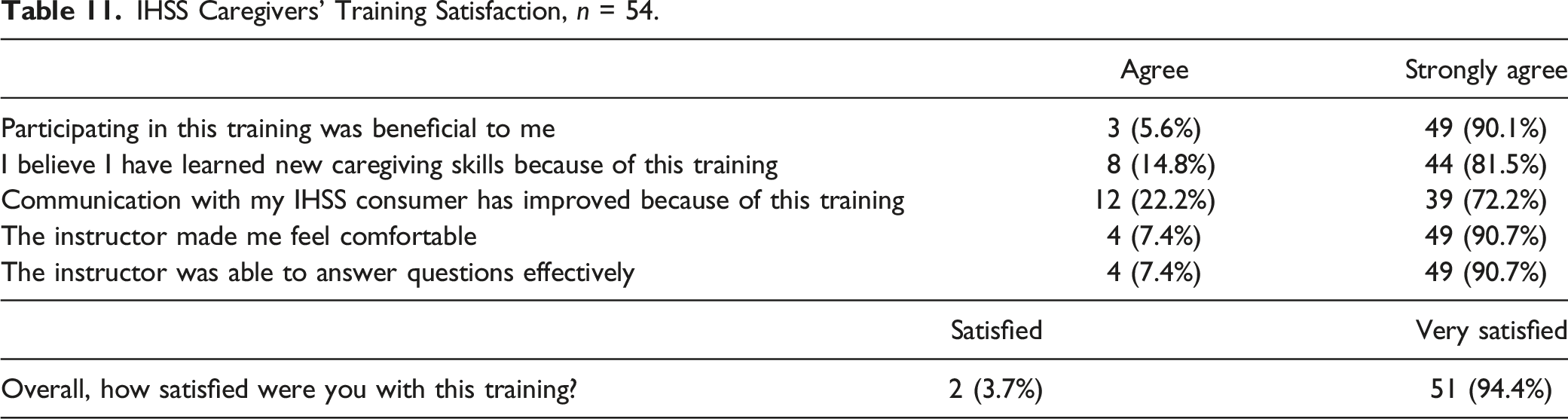
Satisfaction
IHSS Caregivers’ Training Satisfaction, n = 54.
Discussion
Our preliminary results revealed promising signs that online training can bolster the capacity of IHSS caregivers to better support their consumers living with ADRD or cognitive impairment. Dementia knowledge and self-efficacy significantly increased at post-training, with trends suggesting retention at 3-month follow-up. These results are consistent with positive outcomes found in the growing research on online dementia training efforts for caregivers (Pleasant et al., 2020), and supports the importance of continuing and expanding this work with home care workers (Guerrero et al., 2020; Polacsek et al., 2020).
This study had several limitations. Those who opt-in for eligibility screening may be more aware of ADRD and cognition changes in their consumer, which is potential selection bias. Switching to online and remote strategies introduced new processes and adaptations. Tracking and receiving complete data from IHSS caregivers through mail-and-return surveys was resource-intensive and not always reliable. Some IHSS caregivers were ambivalent about sharing personal information online due to heightened fears of fraud and scams. We did begin receiving more Qualtrics surveys at post-training and follow-up, suggesting growing comfort with using Qualtrics (Table 1). Those who responded to surveys may have also been influenced by selection bias. It was difficult to interpret if distress and depression measures captured or reflected fluctuating effects from the COVID-19 pandemic occurring concurrently. Self-reported data by IHSS caregivers were subject to recall and desirability biases. Finally, this study had no control group comparison.
Future analyses will include multivariate regression models to establish relationships between sociodemographic variables and caregiver outcomes, and compare healthcare utilization patterns of IHSS consumers before and after their caregiver’s participation in the training. Additional cohorts with classes in English, Spanish, and Cantonese are already underway. This work has implications for expansion to other California counties beyond Alameda as prevalence of ADRD and demand for dementia-trained home care workers rise statewide.
Footnotes
Acknowledgements
We acknowledge the labor of IHSS caregivers who are often unsung heroes. We are grateful for partnership with the Center for Caregiver Advancement and Alameda Alliance for Health. Special appreciation to Vanessa Beltran, Blanca Lopez, Martha Davila, Moraima Castaneda, Marlene Miranda-Saavedra, Kenneth Stollenwerk, Leah Harden, Zachary Paul, Susie Yu, Tiffany Cheang, Annie Wong, Scott Coffin, Cynthia Mercado-Scott, Echo Rowe, Brooke Hollister, and the reviewers for their insightful comments to strengthen this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication is supported by the California Department of Public Health Alzheimer’s Disease Program funding from the 2018 California Budget Act. The grant number is #18-10612. The views and opinions expressed in this publication are those of the authors and do not necessarily reflect the official policy or position of the State of California.
IRB Protocol/Human Subjects Approval Number
This study was approved by the University of California, San Francisco, Institutional Review Board (#19-28395).