
Abstract
This follow-up study investigated the associations of childhood learning disabilities (LDs) with adult-age anxiety, depression, and unemployment. Psychosocial problems in childhood and psychiatric diagnoses and lack of education in adolescence were studied as potential mediators, and gender and mother’s education were studied as potential moderators of these associations. Data on childhood clinical neuropsychological assessments and lifelong register data on individuals with childhood LD (n = 430; 301 [70%] males; 20–39 years of age) and matched controls (n = 2,149) were applied. Mediation analyses were performed using structural equation modeling. Childhood LDs exerted a significant, but relatively small effect on psychiatric diagnoses in adolescence, which predicted adult-age depression and anxiety. Learning disabilities were related to unemployment both directly and via psychiatric diagnoses in adolescence. Examination of differences in the effects on adult-age outcomes of subtypes of LDs revealed mathematical disability to be more strongly associated with psychosocial problems in childhood and psychiatric problems in adolescence and adulthood than reading disability. Our findings show that LD has small and mostly indirect effects on the risk for later well-being problems. The findings emphasize the importance of adolescence in predicting adult-age psychiatric and employment problems and call for more holistic support for individuals with LDs.
Developmental learning disabilities (LDs), such as reading disability (RD) or mathematical disability (MD), are likely to be persistent (e.g., Maughan et al., 2009; Morris et al., 2009; A. J. Wilson et al., 2015) and affect individuals’ learning both in the beginning of school and later in adolescence and adulthood. Thus, LDs are related not only to education, presenting a risk for dropping out or ending up with lower level of education (Hakkarainen et al., 2015; McLaughlin et al., 2014), but also to well-being, that is, employment, level of income (Caspi et al., 1998; McLaughlin et al., 2014; Parsons & Bynner, 2005), and psychiatric problems in adulthood (A. M. Wilson et al., 2009). Despite the reported risks, not all individuals with LDs have well-being problems in adulthood. Furthermore, most of the research has focused on RD and has seldom been longitudinal or examined individuals with psychiatric diagnoses. Our aim was to gain further understanding of the long-term associations of RD, MD, and comorbid reading and mathematical disability (RD + MD) with adult-age depression, anxiety, and unemployment in a large longitudinal sample of individuals who had been diagnosed with LD in childhood. The longitudinal data also enabled us to look at the possible effects of parental education, attained educational qualifications, gender, psychosocial problems in childhood, and psychiatric diagnoses in adolescence to the adult-age outcomes. Our data were drawn from childhood clinical assessments and combined with lifelong register data on benefits granted on the basis of diagnoses for depression and anxiety.
Despite growing research interest in the relationship of LDs to psychosocial well-being in both childhood (e.g., Maughan & Carroll, 2006; Nelson & Harwood, 2011a, 2011b) and adulthood (e.g., Klassen et al., 2013), longitudinal studies of LDs extending beyond early adulthood remain scarce. Moreover, because studies conducted on adults with the history of LDs have often been cross-sectional instead of longitudinal (e.g., Carroll & Iles, 2006; A. M. Wilson et al., 2009), less is known of the relation of the development during adolescence to adult-age outcomes. However, adolescence is a critical developmental period with rapid changes in physical and sexual maturation, brain development, and learning (Dahl et al., 2018). Adolescence is also known to be vital in terms of psychiatric problems: Among the population in general, psychiatric and social problems onsetting in adolescence predict adult-age psychosocial problems (e.g., Bardone et al., 1996; Fergusson et al., 2005; McLeod et al., 2016). Depression in adolescence has been linked with adult depression, anxiety, and social problems (Fergusson et al., 2005; McLeod et al., 2016), and conduct disorder in adolescence has been linked with several psychosocial well-being problems in adulthood (Bardone et al., 1996). These findings indicate that (a) psychiatric problems in adolescence tend to continue or reappear in adulthood, and (b) adolescents with psychiatric problems may be at a higher risk than their peers for having psychiatric and social problems as adults.
However, little empirical evidence exists on the effects of childhood LD on the association of psychosocial problems in childhood and adolescence with adult-age psychiatric and employment problems. Research has shown that children with LDs are more prone to anxiety (Nelson & Harwood, 2011a) and depression (Nelson & Harwood, 2011b) than their peers. Moreover, there is evidence of comorbidity between LDs and attention problems in children, although the rates vary depending on the diagnostic criteria and type of LD (DuPaul et al., 2013). Hence, by posing a higher risk for depression, anxiety, and attention problems in childhood, LDs may also have associations with psychiatric problems in adolescence that, according to the research on the general population, tend to continue into adulthood. To find out whether (a) childhood LD is directly associated with adult-age mental health or unemployment or (b) the association is mediated by factors in childhood or in adolescence is pivotal when considering the effect of LD on the individual’s life. If the influence from LDs in childhood on adult employment or mental health outcomes is direct, it indicates that better support should be provided at school for the LD itself to prevent negative well-being in adulthood. If the effects are indirect via childhood and adolescent mental health, then it is likely to be important to intervene for both learning difficulties and mental health problems in childhood and adolescence. Moreover, it is possible that the effects of LDs on adulthood differ in terms of different aspects of adult well-being, such as mental health problems or unemployment.
The associations of subtypes of LDs like RD or MD with adult-age well-being outcomes may differ. RD refers to a difficulty that primarily affects the skills involved in accurate and fluent word reading and spelling, whereas MD primarily affects basic arithmetic skills, such as manipulating numbers, performing calculations, and learning facts in mathematics. Secondary problems in, for example, reading comprehension or mathematical problems solving may occur, but they are not necessarily manifested along with the primary deficits. Most research has focused on RD, as it is the most prevalent specific LD (Shaywitz et al., 2008). The relationship of MD or comorbid RD and MD to adult-age outcomes has been less thoroughly explored, although the few existing findings indicate that there are differences among the subtypes of LDs. Hakkarainen and her colleagues (2015) discovered that MD has been found to be a stronger predictor than RD of postsecondary education dropout (Hakkarainen et al., 2015) and, among women, to predict adult-age unemployment and depression (Parsons & Bynner, 2005). However, it is still unclear whether childhood psychosocial problems and/or psychiatric problems in adolescence or postsecondary education have an effect on the association between MD and adult-age well-being.
Reading disability and MD are often comorbid, which has also been found to continue into adulthood (A. J. Wilson et al., 2015). Comorbid RD and MD have been shown to be particularly related to internalizing psychopathology in childhood (Willcutt et al., 2013). This may indicate that adolescents with the history of comorbid childhood LDs may be even more vulnerable to psychiatric and social problems than adolescents with a single LD and, hence, more prone to later adult-age problems as well. Indeed, there is some evidence that individuals with both RD and MD report more emotional symptoms, maladjustment, and school problems than do adolescents with a single LD (Martínez & Semrud-Clikeman, 2004) and also more unemployment and psychiatric problems as adults (Parsons & Bynner, 2005).
Adolescence is also a period of educational choices, and adolescents with LDs are more likely than their non-disabled peers to leave school after compulsory education or to drop out during their postsecondary education (e.g., Hakkarainen et al., 2015; McLaughlin et al., 2014). However, the association of low education with adult-age psychosocial well-being problems among individuals with LD is unclear. Some findings indicate that the lack of postsecondary education has no effect on the association of LD with adult-age depression and anxiety (see Klassen et al., 2013), while other findings suggest that distress, depression, and suicidal thoughts among adults with LDs are related to uncompleted secondary education (A. M. Wilson et al., 2009). However, studies on the linkages of different subtypes of LDs, low educational level, and well-being are, to our knowledge, non-existent.
One potential background factor that may be related to adult-age outcomes for children with LDs is their parents’ educational level. Despite the rise in educational levels over recent decades, children’s educational achievement continues to be predicted by their parents’ level of education (Organisation for Economic Co-Operation and Development [OECD], 2018). This may also indirectly affect adult psychosocial well-being outcomes (Dubow et al., 2009). Among Finnish students, a low level of parental education predicted learning difficulties (Hakkarainen et al., 2015). Moreover, high parental education has indirectly predicted successful completion of studies (Hakkarainen et al., 2015). In the present study, we examined parental educational level in childhood as a possible moderator of the association of LDs with adult-age well-being outcomes.
Gender may also be a moderator of the associations between LDs and adult outcomes. In the general population, women have been reported to be more prone to unemployment (OECD, 2018) and to adult-age depression or anxiety symptoms (Altemus et al., 2014; Kessler, 2003), and females with LDs to exhibit higher rates of depressive symptoms than females without LDs (e.g., Heath & Ross, 2000). However, gender-dependent differences in adult-age outcomes among individuals with LD are not clear. In their meta-analysis, Klassen and colleagues (2013) found no significant moderating effect of gender on the relationship between LD and adult-age depression and anxiety.
In the previous research, LD has often been defined on the basis of adult-age self-reports instead of an objective childhood diagnosis (e.g., Ghisi et al., 2016). Moreover, it has been common to rely on self-reports of psychosocial well-being. Thus, despite indications that individuals with LDs generally show lower mean levels of self-reported psychosocial well-being than do their non-LD peers, they may not show psychiatric disorders above the clinical threshold level (Maag & Reid, 2006). Owing to the scarcity of in-depth earlier research, we examined the associations of different subtypes of LDs (RD, MD, RD + MD) with adult-age well-being problems, studying them from a longitudinal perspective from childhood to adulthood and using medical diagnoses to define psychiatric problems in adolescence and in adulthood.
A previous study on the present longitudinal register data showed that psychiatric problems and extended periods of unemployment were more common among adults with LDs compared with controls (T. Aro et al., 2019). Also, MD was found to be particularly associated with depression and unemployment and to pose a higher risk than RD among women (T. Aro et al., 2019). In the present study, we aimed to continue these investigations of the associations between childhood LDs and adult-age well-being outcomes by examining the effect of psychosocial problems in childhood, psychiatric diagnoses in adolescence, lack of an educational qualification after comprehensive school, gender, and maternal educational level on these associations. As our register data included a population-based matched control group, we were able to examine which associations with adult-age outcomes appear to be specific to individuals with LDs and which would apply to the population in general. We addressed the following specific research questions:
Method
Procedure and Participants
The sample was drawn from the archival client database of the Clinic for Learning Disorders (CLD) kept by the Niilo Mäki Institute (NMI) and the Family Counseling Center of the city of Jyväskylä, Finland. This public clinic has offered neuropsychological assessment for children and counseling to parents and teachers of children with LDs in the Central Finland area since 1985. Children in the study (age range = 7–13 years) were typically referred by school psychologists due to considerable learning difficulties, for which they had received special educational services at school. The degree and type of learning difficulties detected at school were thoroughly examined in broad neuropsychological assessments at the clinic and confirmed as specific LDs. For purposes of this study, children referred to the clinical assessment ought not to have had primary psychosocial problems or global developmental delay, although no formal exclusionary criteria were used.
Individuals at least 20 years of age in 2014 (n = 517) were identified from the clinical database. The Population Register Centre of Finland (PRC) provided their current contact information. For eight individuals from the original sample, the requested data were unavailable either because the client had refused disclosure of such information or was living abroad. Thus, the final size of the LD group was 509. The PRC also provided a control group (we attempted to find five control group individuals for each participant with LD) matched for gender, age, and place of residence at the beginning of compulsory education. As it was derived from the registers, no information on the possible childhood learning or other problems of the control group was available. However, knowing that the control group was population-based and that the estimated prevalence of LDs in the population in general is 5% to 15% internationally (American Psychiatric Association [APA], 2013), it can be assumed that approximately the same percentage range of the control group members also had LDs of some kind.
It was not possible to identify five control group members for each participant with LD, and the final number of control group participants was 2,530. For the present study, we included only participants having an RD and/or MD diagnosis (see later) set at the CLD, and we excluded any person performing in both reading and math tests above the criterion set for RD/MD diagnosis. Number of participants with LD excluded was 79, and thus their control matches (n = 381) were excluded as well. Thus, the final number of participants was 430 in the LD group and 2,149 in the control group.
Statistics Finland and the National Social Insurance Institution of Finland (Kela) provided register data for both groups. Supervised by the Finnish parliament, Kela is a state institution that provides Finland’s residents with basic social security services (i.e., family and housing benefits; health insurance; financial aid for students; pensions; and unemployment, disability, and rehabilitation benefits; see www.kela.fi/web/en).
Due to regulations regarding the participant anonymity, we could not access any identifying information within the adult-age register data because we did not have a written informed consent for this from either the former clinical clients or control group members. Therefore, the clinical clients’ individual information from the childhood assessment could not be directly connected with their adult-age register data. Before being combined with the register data, the childhood data were converted into the categorical variables of gender, age, presence of psychosocial problems, and LD type (see later). This procedure allowed us to use information from the childhood assessment in the follow-up analyses even without identifying information available.
Measures
Age
The sample was classified into four categories based on the individual’s birth year: (a) 1991–1994 (ages 20–23 years in 2014), (b) 1986–1990 (24–28 years), (c) 1981–1985 (29–33 years), and (d) 1975–1980 (34–39 years). The age groups were used to construct the measures for psychiatric problems in adolescence and adulthood (see below).
Type of LD
The type of LD for the clinical group was classified into three subgroups: RD (n = 133), MD (n = 113), and RD + MD (n = 184). In the present study, a performance of at least −1.5 SDs below the standardization sample mean in the reading or mathematics tests was used as a definition of RD and MD, utilizing each child’s test scores that had been saved in the clinical data. As tests used at the CLD have varied over the years, the LD was defined according to the scores of the test in use at the time of the assessment (see below). At the time of the clinical data collection, few published measures with comprehensive psychometric data were available in Finland; therefore, reliability figures cannot be reported. However, each measure mentioned below, although not officially published, was in frequent use at the CLD at the time and had a standardization sample that provided standard scores to which the child’s performance could be referenced.
Reading measures
Two text-reading tasks and three word-list reading tasks described below, all developed and normed in Finland, were used as alternative reading measures, depending on which test the child had taken. Reading fluency (i.e., speed) was primarily used to define RD. In transparent orthographies like Finnish, in which accurate reading is typically achieved during the first grade, dysfluency is a better marker of reading difficulties than inaccuracy (M. Aro & Wimmer, 2003).
Misku-Text
Normed for 8- to 12-year-old children (NMI, 1985–2004), Misku-Text is a reading test in which the child reads aloud a one-page story as quickly and accurately as possible. In the present study, the time taken to complete the text was used as the result.
Äänekoski Reading Performance Scale (ÄRPS)
The ÄRPS (NMI, 1985–2004) is a reading test battery normed for Grades 2 to 4 that includes a text-reading task with a one-page story to be read aloud and a word/pseudoword-list reading task, 20 items each. In the present study, the number of words read per time unit in the text-reading task or the time taken to read the word list in the word/pseudoword task were compared with the reference group mean.
Markkinat Word List
Normed for 8- to 12-year-old children (NMI, 1985–2004), the Markkinat Word List consists of 13 words the child reads aloud. Here we used the time taken to read the words as the result.
Lukilasse
The Lukilasse (Häyrinen et al., 1999) is a test battery for reading, spelling, and mathematical skills normed for children in Grades 1 to 6. We used the Word Reading Subtest of the battery, in which the child reads aloud a list of gradually longer and more difficult words, and the number of correctly read words in 2 min was used as the fluency measure.
Mathematics measures
Three arithmetic tests used at the clinic over the years were alternatively used as measures of MD.
Kaufman Assessment Battery for children–Arithmetic Subtest (K-ABC)
The K-ABC (Kaufman & Kaufman, 1983) contains 38 items that measure the ability to identify numbers, understand mathematical concepts, count, and compute. Finnish norms for Grades 2 to 5 (NMI, 1985–2004) were used in the present study.
Räsänen Mathematical Ability Test (RMAT)
Normed for Grades 3 to 6, the RMAT (Räsänen, 1992) is a Finnish test in which the child performs as many basic arithmetical operations as possible in 10 min. The number of correct answers is compared with the reference group mean. Cronbach’s alpha for the test is reported to be .92 to .95 in a normative sample.
Lukilasse Arithmetics Subtest
The arithmetic subtest of the Lukilasse test battery (Häyrinen et al., 1999) consists of basic arithmetic operation tasks for Grades 1 to 6. The number of correct answers is compared with the norm for the child’s grade.
Mother’s educational level
Based on the information provided by Statistics Finland, the highest educational status of the participants’ mothers was classified into three categories: (a) comprehensive school, (b) vocational school or high school, and (c) university of applied sciences (polytechnic), university, or doctoral education. In the Finnish educational system, the comprehensive school, which children enter at the age of 7, comprises 9 years of compulsory education. At the end of the comprehensive school, adolescents can choose between high school and vocational school. High school is the more academically demanding option and is often followed by an application into a university or university of applied sciences. Vocational school provides its students with qualifications for a practical occupation (e.g., hairdresser, mechanic).
Psychosocial problems in childhood
Observations regarding childhood attention and internalizing or externalizing problems were requested from teachers and parents along with the clinical assessments. The problem scores were coded into dichotomous variables on the basis of everyday observations reported by teachers on the Teacher’s Report Form (TRF; Achenbach, 1991a) or by mothers on the Child Behavior Checklist (CBCL; Achenbach, 1991b), which were given during the clinical assessment process at the CLD. Each questionnaire contains 113 items on problem behavior rated on a 3-step response scale (0 = not true, 1 = somewhat or sometimes true, 2 = very true or often true). Eight syndrome scales and three larger sum scores (Internalizing, Externalizing, and Total Problems scores) can be formed from the items. We defined psychosocial problems in childhood using the Internalizing Problems scores (withdrawing, somatic complaints, and anxious/depressed symptoms), Externalizing Problems (delinquent and aggressive behavior) scores, and Attention Problems scale. The teacher’s ratings (TRF) were used as the primary source of information whenever available. As the present study focused on LDs, observations of the child in the school environment were considered more relevant than those at home. Owing to the lack of published normative data for Finnish children, the child was defined as having internalizing, externalizing, and/or attention problems if the raw scores were more than 1 SD from the mean of the North American reference data. The 1 SD cut-off criterion was used because Finnish teachers have been found to evaluate their students’ social and behavioral problems as relatively mild in relation to the reference data than do their counterparts in other countries (Rescorla, Achenbach, Ginzburg et al., 2007; Rescorla, Achenbach, Ivanova, et al., 2007).
In the present sample, the three problem scores correlated statistically significantly with each other. Moreover, the sample sizes of children having one of the psychosocial problems in different LD subgroups were rather small (20–75). Psychosocial problems in childhood were therefore defined broadly based on Internalizing, Externalizing, or Attention problems if one or more of the scores exceeded the 1 SD cut-off.
Psychiatric problems in adolescence
Psychiatric problems (depression, anxiety, and other) were defined using disability allowances, rehabilitation allowances, disability pensions, sickness allowances, and reimbursements for medicines subsidized by Kela on the basis of a psychiatric diagnosis (for detailed descriptions of these benefits, www.kela.fi/web/en; T. Aro et al., 2019). The benefits received between 12 and 19 years of age were used to define adolescent psychiatric problems. A person was defined as depressed in adolescence if they had received at least one form of the above-mentioned allowances on the basis of depressive mood disorder (International Classification of Diseases [ICD-10] codes F30–39) or reimbursement for antidepressants (WHOCC-ATC/DDD Index: N06A). Anxiety in adolescence was defined as having received allowances for anxiety and stress-related mental disorders (ICD-10 codes F40–48) or reimbursement for anxiolytics (WHOCC-ATC/DDD Index: N05B). Similarly, a person was defined as having other psychiatric problems if they had received at least one of the allowances on the basis of one of the following disorders: adult-age personality and behavior (F60–69), behavioral and emotional disorders (F90–98), mental and behavioral disorders due to psychoactive substance use (F10–19), eating disorder (F50), or for schizophrenic, delusional, or other non-mood psychotic disorders (F20–29); Also falling into this category were individuals who received reimbursements for the following medications: antipsychotics (WHOCC-ATC/DDD Index N03A–), sedatives (N05C–), psychostimulants (N06B–), or psycholeptics and psychoanaleptics (N06C–).
One categorical variable—“psychiatric problems in adolescence”—was formed by combining depression, anxiety, and other psychiatric problems in adolescence, owing to the small group sizes (from 2 to 22) in the three psychiatric problem categories, which would have diminished the statistical power in the analyses. Thus, psychiatric problems in adolescence were defined if any of the psychiatric problem category was present.
Educational level
Individuals’ educational level was defined using information provided by Statistics Finland on the highest educational attainment at the time of data gathering. In this study, education was classified into two categories: comprehensive school only and a post-compulsory education (i.e., after the ninth grade of comprehensive school).
Adult-age depression
Depression was defined on the basis of disability allowances, rehabilitation allowances, disability pensions, or sickness allowances received on the basis of depressive mood disorder (ICD-10 codes F30–39) or medicine reimbursements granted for antidepressants (WHOCC-ATC/DDD Index: N06A) after age 20.
Adult-age anxiety
Anxiety was defined on the basis of allowances for anxiety or stress-related mental disorders (ICD-10 codes F40–48) or reimbursement for anxiolytics (WHOCC-ATC/DDD Index: N05B) after age 20.
Unemployment
The data provided annual information on the number of days the individual had received the basic unemployment allowance from Kela. This allowance is paid for a maximum of 500 days from the beginning of unemployment for individuals who do not belong to any unemployment fund. For those belonging to a fund, the first 300 to 500 days are paid by the fund. This is followed by the 500-day maximum basic unemployment allowance paid by Kela. As information on possible payments by funds was not available, data on unemployment allowances paid by Kela were used. Unemployment was measured using the annual mean number of days the basic unemployment allowance was received, excluding years in formal education and years in which a disability pension/rehabilitation subsidy was received. If there was no post-comprehensive education, the mean annual unemployment was calculated starting from age 15. Participants were categorized as unemployed if their annual mean number of days of basic unemployment allowance paid by Kela exceeded 63, that is, 3 months or more per year during adulthood. Owing to the lack of information on the reimbursements paid by funds, this average was presumably below the true level of unemployment figures, although it was a good proxy for continuing and long-term unemployment.
Statistical Analyses
Differences between the LD subgroups in the proportions of childhood psychosocial problems, and differences between the LD group and the controls and between the LD subgroups in adolescence psychiatric problems, education after comprehensive school, and adult-age psychosocial well-being outcomes were examined with cross-tabulations and chi-square tests. Adjusted residuals were used to further analyze pairwise differences among the LD subgroups. An adjusted residual more than ±2.0 conventionally indicates that if the null hypothesis were true with a significance level of .05, the number of cases in that cell would be significantly larger or smaller than expected.
Two mediation analyses were performed using structural equation modeling (SEM) with Version 8 of the Mplus statistical package. All the mediators and outcome variables in the models were dichotomous. Hence, the models were estimated with the weighted least square mean and variance (WLSMV) method. Indirect effects were tested using bias-corrected bootstrapped confidence intervals (95%) with 1,000 replications. Possible moderator effects were tested with the Wald Test. The goodness-of-fit of the models was evaluated using the chi-square test of model fit, the root mean square error of approximation (RMSEA), and the comparative fit index (CFI) as indicators. A non-significant chi-square test value, RMSEA value lower than .06, and CFI greater than .95 indicate a well-fitted model (Muthén, 1998–2004).
Results
Table 1 presents the descriptive statistics on LD subgroups, childhood psychosocial problems, adolescent psychiatric problems, education after comprehensive school, and adult-age psychosocial well-being outcomes. The numbers and percentages of cases are shown in each problem domain in the LD and control groups and separately among the three LD subgroups. As the chi-square tests in Table 1 show, the LD group differed significantly from the control group in the percentage of individuals having psychiatric problems in adolescence, not having post-comprehensive education, having adult-age depression or anxiety, and being unemployed, with a higher proportion of problems in the LD group in each domain. Moreover, there were statistically significant differences among the three LD subgroups in childhood psychosocial problems in general, and in internalizing and attention problems when examined separately, the proportion of problems being higher than expected in the MD subgroup in each (adjusted residual, Adj.Res. = 2.3 for psychosocial problems in general, Adj.Res. = 2.6 for internalizing, and Adj.Res. = 2.6 for attention problems).
LD Group, LD Subgroup, and Control Group Numbers by Psychosocial Problems; Psychiatric Problems; Postsecondary Education; and Adulthood Depression, Anxiety, and Unemployment Categories.
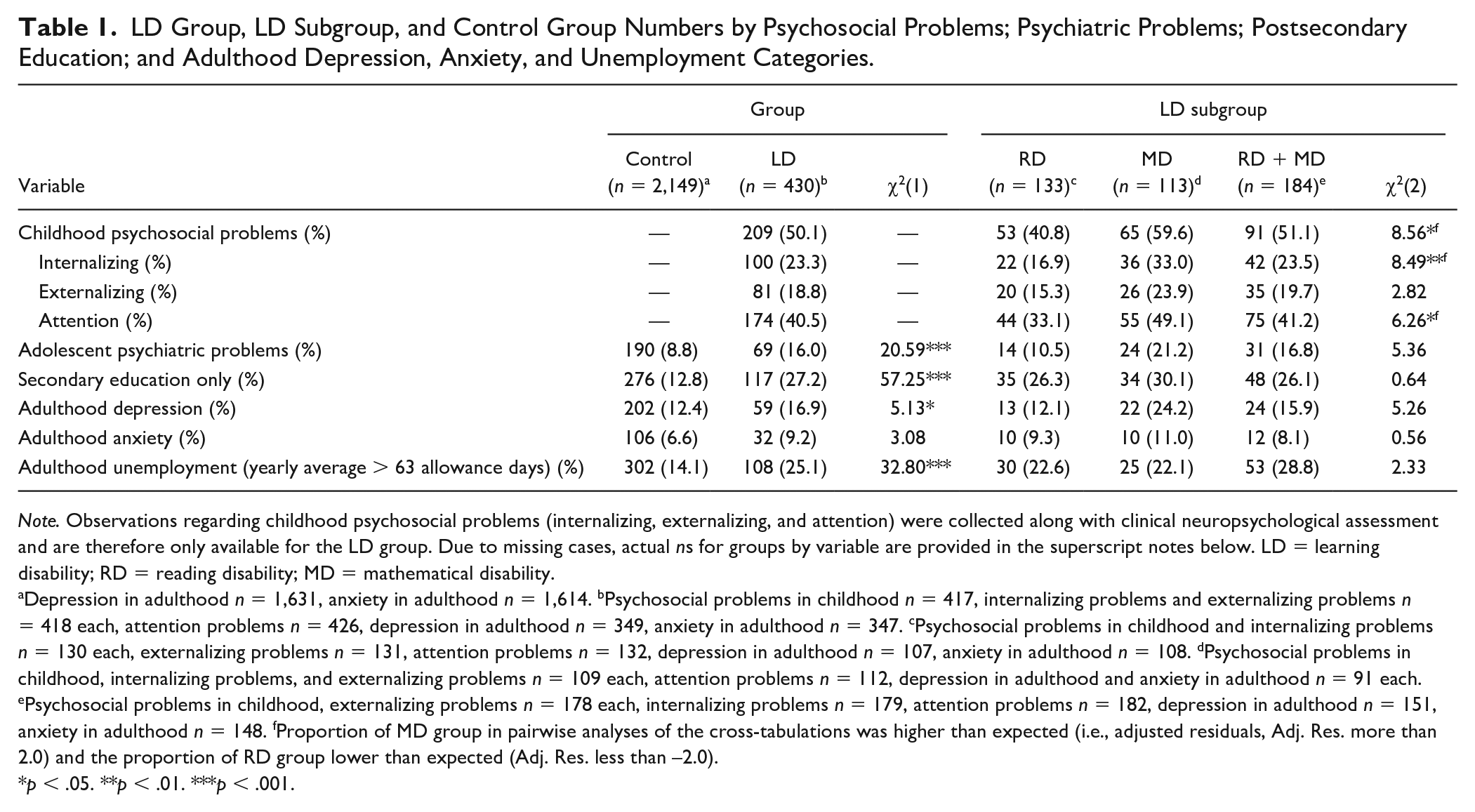
Note. Observations regarding childhood psychosocial problems (internalizing, externalizing, and attention) were collected along with clinical neuropsychological assessment and are therefore only available for the LD group. Due to missing cases, actual ns for groups by variable are provided in the superscript notes below. LD = learning disability; RD = reading disability; MD = mathematical disability.
Depression in adulthood n = 1,631, anxiety in adulthood n = 1,614. bPsychosocial problems in childhood n = 417, internalizing problems and externalizing problems n = 418 each, attention problems n = 426, depression in adulthood n = 349, anxiety in adulthood n = 347. cPsychosocial problems in childhood and internalizing problems n = 130 each, externalizing problems n = 131, attention problems n = 132, depression in adulthood n = 107, anxiety in adulthood n = 108. dPsychosocial problems in childhood, internalizing problems, and externalizing problems n = 109 each, attention problems n = 112, depression in adulthood and anxiety in adulthood n = 91 each. ePsychosocial problems in childhood, externalizing problems n = 178 each, internalizing problems n = 179, attention problems n = 182, depression in adulthood n = 151, anxiety in adulthood n = 148. fProportion of MD group in pairwise analyses of the cross-tabulations was higher than expected (i.e., adjusted residuals, Adj. Res. more than 2.0) and the proportion of RD group lower than expected (Adj. Res. less than −2.0).
p < .05. **p < .01. ***p < .001.
Table 2 presents the correlations among the variables in childhood, adolescence, and adulthood. As the table shows, childhood LD correlated significantly with mother’s education, psychiatric problems in adolescence, and secondary education, and with each of the three adult-age outcome variables. Psychosocial problems in childhood correlated significantly with each other. Moreover, psychiatric problems in adolescence correlated significantly with secondary education and with adult-age anxiety, depression, and unemployment, almost fully explaining depression in adulthood.
Intercorrelations Between Childhood and Adolescence Variables and Outcome Variables in Adulthood.
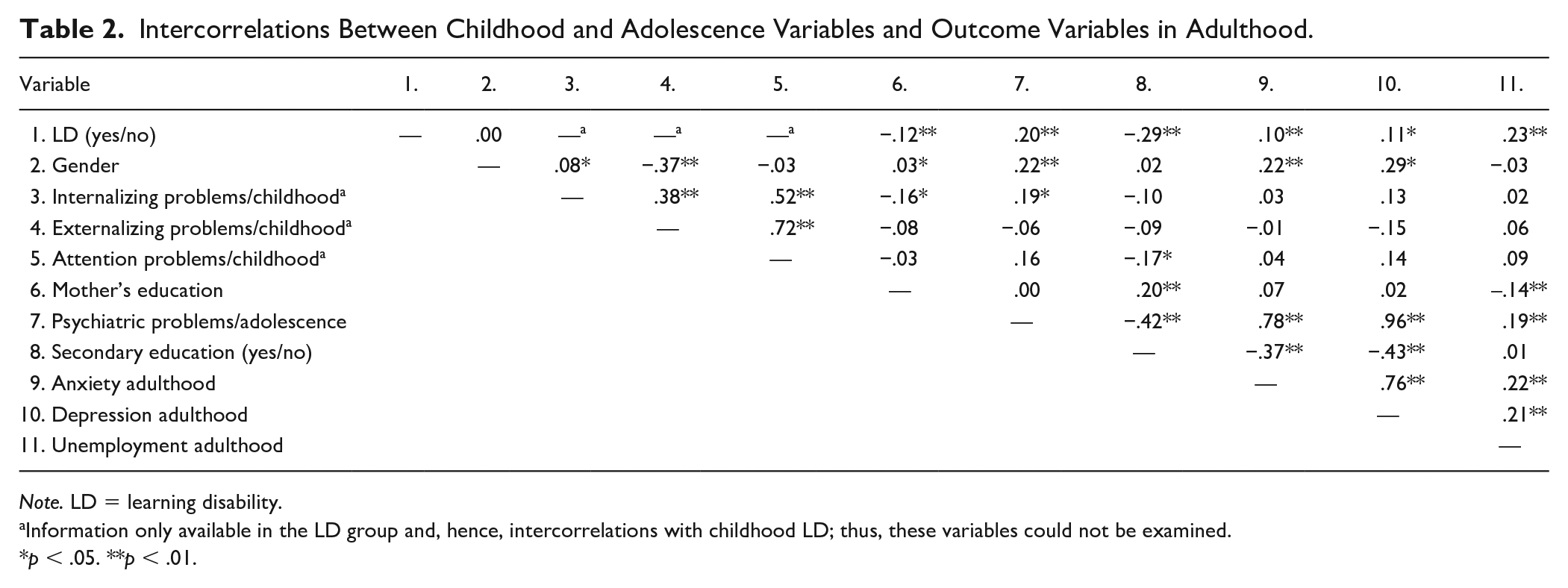
Note. LD = learning disability.
Information only available in the LD group and, hence, intercorrelations with childhood LD; thus, these variables could not be examined.
p < .05. **p < .01.
To answer the first research question, we tested the extent to which childhood LD explained adult-age depression, anxiety, and unemployment, and whether this association was mediated by the lack of post-comprehensive education or by psychiatric problems in adolescence. Moreover, we tested whether the possible mediation effects of the lack of education and of psychiatric problems in adolescence were moderated by gender and mother’s educational level. Psychiatric problems in adolescence almost fully predicted adult-age depression, showing a correlation between the variables of .96. Owing to this result and difficulties in further estimation, adult-age depression was dropped from the model.
The structural equation model pertaining to the first research question was estimated in two steps. In the first step, we tested if gender or mother’s education moderated some of the paths in the model. In the saturated model, adult-age anxiety and unemployment were regressed on post-comprehensive education, psychiatric problems in adolescence, and childhood LD. Post-comprehensive education and psychiatric problems in adolescence were regressed on childhood LD. Post-comprehensive education and psychiatric problems in adolescence were allowed to correlate. The model was tested separately for each of the two possible moderators, that is, gender and mother’s education. Neither gender, χ2(8) = 5.32, p = .723, nor mother’s education, χ2(17) = 13.31, p = .715, had moderation effects.
In the second step, the model was estimated with the single group analysis that set gender and mother’s education as independent variables in the model. Mother’s education had three categories, which were transformed into two dummy-coded variables. We started from a saturated model, dropping the statistically most non-significant paths one by one from the model, except the paths from childhood LD to adult-age anxiety and unemployment. The model fitted the data well: χ2(8) = 10.37, p = .240, RMSEA = .01, CFI = 1.0 (see Figure 1).
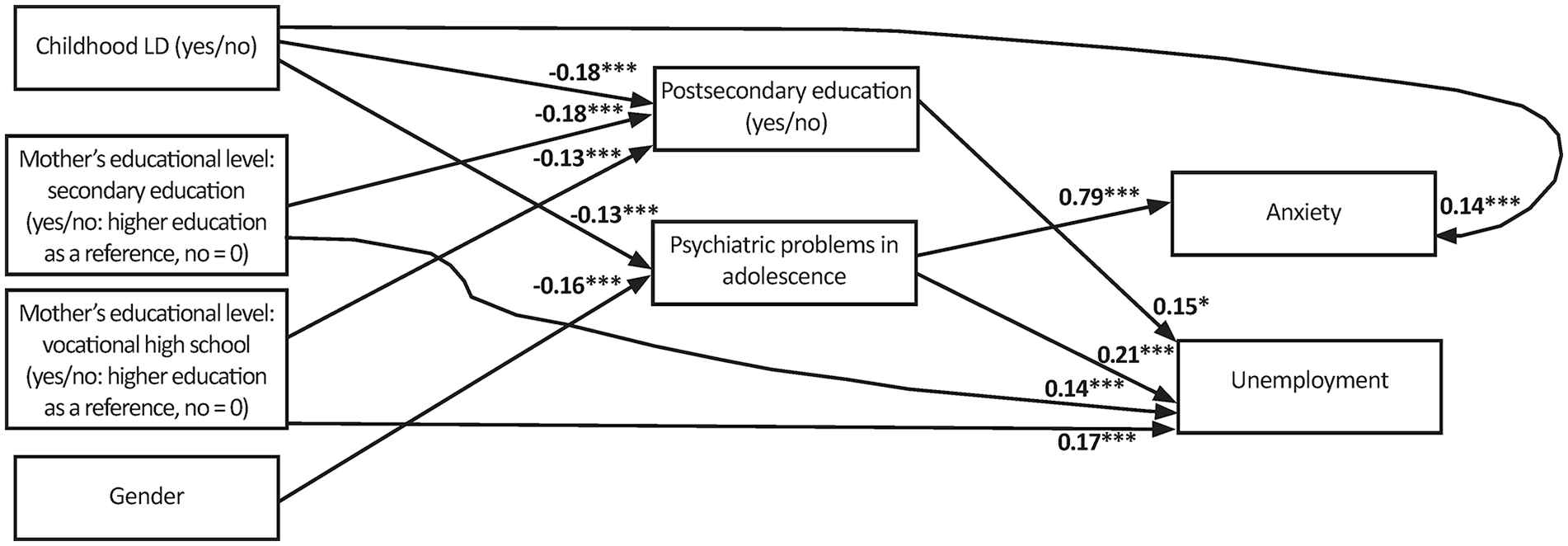
Mediation model depicting associations of childhood LD with adult-age anxiety and unemployment via postsecondary education and psychiatric problems in adolescence, controlling for gender and maternal education level.
As Figure 1 shows, the paths from childhood LD to psychiatric problems in adolescence and from psychiatric problems in adolescence to adult-age anxiety were both significant, and thus the indirect effect from childhood LD to adult-age anxiety via psychiatric problems in adolescence was small but significant (estimate = 0.28; 95% confidence interval [CI] [0.14, 0.41]; standardized estimate = 0.10). Moreover, the direct effect from childhood LD to adult-age anxiety was non-significant.
Childhood LD showed a significant total effect on unemployment in adulthood (estimate = 0.38; p < .001; standardized estimate = 0.14). Childhood LD predicted adult-age unemployment both directly (see Figure 1) and through having psychiatric problems in adolescence (estimate = 0.08; 95% CI [0.03, 0.14]; standardized estimate = 0.03). In addition, an unexpected effect of childhood LD on unemployment was found for those having post-comprehensive education (estimate = −0.07; 95 % CI [–0.15, −0.02]; standardized estimate = −0.03). Overall, all of the effects of LD on outcome variables were rather small.
To answer the second research question, we examined the associations between the subtype of childhood LD and adult-age anxiety and unemployment, and whether the associations would be mediated by childhood psychosocial problems, lack of education after comprehensive school, or psychiatric problems in adolescence. This was tested only in the group of individuals with childhood LD. The correlation between adult-age depression and psychiatric problems in adolescence varied between .96 and 1.0, depending on the subtype of childhood LD, and, as in the first model, we dropped adult-age depression from the model. Gender and mother’s educational level were first included in the model but as they showed no significant moderation effects, they were dropped from the final model. To compare the effects of the subtypes of LD, two dichotomous variables D1 (RD vs. MD) and D2 (RD + MD vs. MD) were coded using MD as a reference group in both D1 and D2 coded as 0, RD coded as 1 in D1, and RD + MD versus MD coded as 1 in D2. In addition, the effects of RD and RD + MD were compared by subtracting the comparison of D1 from D2.
The following paths were added successively in the model: the direct paths from the mediators in adolescence (i.e., having psychiatric problems in adolescence and not having education after comprehensive school) to adult-age anxiety and unemployment, the direct paths from psychosocial problems in childhood to the mediators in adolescence, the direct effects from the comparisons of the subtypes of childhood LD on psychosocial problems in childhood, and the direct effects from the comparisons of the subtypes of childhood LD on adult-age anxiety and unemployment (see Figure 2). This model fitted the data well: χ2(8, N = 430) = 10.04, p = .26; RMSEA = 0.02; CFI = 0.99.

Mediation model depicting associations of comparisons among subtypes of learning disability with adult-age anxiety and unemployment via psychosocial problems in childhood, postsecondary education, and psychiatric problems in adolescence.
For adult-age unemployment, no significant direct or indirect effects in the pairwise comparisons of the LD subtypes (RD vs. MD; RD + MD vs. MD; RD vs. RD + MD) were found. The LD group differences showed no significant direct effects on anxiety. However, a significant indirect path was found when the effects of RD and MD on anxiety mediated by psychosocial problems in childhood and psychiatric problems in adolescence were compared (estimate = −0.13; 95 % CI [–0.36; −0.07]; standardized estimate = −0.04), indicating that individuals with MD were more likely than individuals with RD to develop anxiety as adults if they had psychosocial problems as children and psychiatric problems as adolescents. The direct effect of the comparison between RD and MD on anxiety was non-significant.
When the effect of childhood LDs on psychiatric problems in adolescence was estimated in the model, no significant direct or indirect effects in the pairwise comparisons of the LD subtypes on adult-age anxiety or unemployment were found. The only significant total effect was found when comparing the effects of RD and MD on psychiatric problems in adolescence (estimate = −0.46; p < .05; standardized estimate = −0.21), suggesting that individuals with MD were more likely than individuals with RD to have had a psychiatric diagnosis in adolescence if they had had psychosocial problems in childhood. However, the direct and the indirect effects were not significant.
Discussion
In the present longitudinal study, we first examined the extent to which childhood LDs predicted the presence of adult-age depression, anxiety, and unemployment, and whether this association was mediated by a lack of education after comprehensive school or psychiatric problems in adolescence or was moderated by gender or mother’s educational level. Second, we examined the extent to which the subtype of childhood LD (RD, MD, or RD + MD) predicted adult-age depression, anxiety, and unemployment, and whether this association was mediated by childhood psychosocial problems, own educational qualification after comprehensive school, or psychiatric problems during adolescence. We defined RD as a deficit in word reading fluency and MD as a deficit in basic arithmetic skills like manipulating numbers and calculating. Possible secondary problems such as difficulties in reading comprehension or mathematical problem solving were not examined in the present study.
Association of LD and Adult-Age Mental Health Problems and Unemployment
Our findings showed that childhood LD as such exerted a statistically significant, but relatively small effect on depression, anxiety, and unemployment in adulthood. However, the findings emphasize the importance of mental health in adolescence in predicting adult-age psychiatric and employment problems. First, we found that childhood LD predicted adult-age anxiety indirectly via psychiatric diagnoses in adolescence, indicating that individuals with LD are more prone than their peers to have psychiatric problems as adolescents, which in turn puts them at risk for adult-age anxiety. Psychiatric problems in adolescence were found to explain adult-age depression almost fully, which suggests that via their proneness to psychiatric problems in adolescence, individuals with LDs are also prone to depression as adults. We also found that childhood LDs explained adult-age unemployment both directly and indirectly via psychiatric problems in adolescence. Unexpectedly, childhood LD was also found to have an indirect effect on the probability of later unemployment via having post-comprehensive education, not as might be expected via lack of further education. The association of childhood LDs with adult-age outcomes was underlined by the finding that neither gender nor maternal educational level had a moderation effect on this association.
Our research thus showed that childhood LDs per se do not necessarily have consequences on psychiatric problems in adult life. Our results indicate that problems in adolescence, in particular, are predictive of unfavorable adult-age outcomes.
Our finding on the association of childhood LDs with adult-age anxiety is in line with earlier research (e.g., Klassen et al., 2013). In addition, as this finding was based on psychiatric diagnoses, it extends the existing knowledge by indicating that besides being related to higher mean levels of self-reported psychological well-being problems (Maag & Reid, 2006), LDs also increase the risk for psychiatric disorders that exceed the clinical threshold (T. Aro et al., 2019). We deepened the earlier findings by revealing that psychiatric problems in adolescence are particularly critical when predicting adult-age psychiatric problems among individuals with LDs. We replicated the earlier findings that psychiatric and social problems in adolescence generally predict adult-age psychosocial problems (Fergusson et al., 2005; McLeod et al., 2016) but also showed that LDs in childhood increase the risk of psychiatric problems in adolescence. The psychiatric problems in adolescence were based on a medical assessment and psychiatric diagnoses. This emphasizes that the psychiatric problems related to childhood LDs can exceed the clinical threshold already in adolescence.
The findings on the direct association of LDs with unemployment in adulthood confirm the few earlier findings (Caspi et al., 1998; Parsons & Bynner, 2005). The finding that psychiatric problems in adolescence mediate the association of LDs with unemployment provides a novel contribution to the earlier findings as well as to the previous findings on the same longitudinal data (T. Aro et al., 2019). However, childhood LD also had an unexpected negative effect on employment even if the individual had postsecondary education. One explanation for this finding may be that after gaining a qualification, individuals with LDs may also need more support than peers in job seeking. However, the indirect effect of LD on unemployment via having postsecondary education was rather weak.
Association of LD Subtype With Adult-Age Outcomes
Our findings indicated that the significance of type of childhood LD on adult-age outcomes was minor. The only difference between the subtypes was found for RD, referring to a disability in fluent word reading, and MD, a disability in basic arithmetic skills: Individuals with MD were more prone than individuals with RD to have anxiety as adults if they had a history of psychosocial problems as children followed by psychiatric diagnoses as adolescents. However, this effect was not found when the RD group was compared with the RD + MD group or when the RD + MD group was compared with the MD group. We also estimated the direct effect of the different subtypes of childhood LDs on psychiatric problems in adolescence, but the results revealed no significant change in the effects of the LD subtypes on adult-age outcomes. The finding concerning a linkage of MD with adult-age anxiety is in line with previous findings from a study on same longitudinal register data in which adult-age psychiatric problems had been defined solely on the basis of medicine reimbursements (T. Aro et al., 2019).
Our finding extends the previous findings by showing that there is a significant path from MD to adult-age anxiety via psychosocial problems in childhood and psychiatric problems in adolescence. Moreover, in the MD group, the proportion of individuals receiving reimbursements for psychiatric problems in adolescence and that of those with reimbursements granted for adult-age depression were higher, although not statistically significant. With larger group sizes, a significant difference between the groups may have been found. This was shown more clearly by T. Aro and colleagues (2019), who found that individuals with MD, women in particular, were more prone than individuals with other LDs to depression and unemployment as adults. These findings suggest that MD may have some particular features that are more critical to psychosocial well-being problems in adulthood than features of RD. The appearance of MD (i.e., a problem in basic number and arithmetic skills) in childhood clinical assessment may also reflect a wider range of neuropsychological problems that may cause problems in coping in the information society, in social processing, and in adaptation and thereby hamper overall psychosocial well-being. However, present data do not enable further examination of the underlying factors, such as visual processing or social skills, and the relationship of MD to later problems. Further research with a special focus on the relationship of MD to problems in adult-age and underlying factors of this relationship is needed.
Study Strengths and Limitations
In the present study, the use of lifelong register-based data on psychiatric diagnoses and unemployment enabled more objective investigation than data based on individuals’ self-reports that are often used in studies of adults with LDs (Ghisi et al., 2016; Maag & Reid, 2006). One strength of the register-based data was the almost complete lack of attrition over the follow-up: Except for eight individuals from the original sample of 517, we accessed all the participants’ data in both adolescence and adulthood. In longitudinal research, attrition is typically considerable, unavoidable, and very often unexplained, which makes our results exceptionally comprehensive and reliable for a longitudinal study. However, one limitation of register-based data is the regulation of protection of participant anonymity. Hence, because we could not identify each individual in the follow-up and combine their childhood and adulthood information, studying different individual pathways from childhood to adulthood was not possible. Also, we were limited to the data that we were able to access. Unemployment allowances, for instance, only covered the allowances reimbursed by the Kela. This omits the reimbursements paid from unemployment funds, which a considerable number of Finnish workers subscribe to. Thus, the unemployment figures obtained for the present data are below the true level, although they can be assumed to represent both continuing and long-term unemployment. Another limitation related to the register data is that despite its comprehensiveness and objectivity, it only allows analysis of the variables at their level of classification in the registers. This meant that we could not further examine, for example, if a certain subtype of anxiety or depression in adult-age was especially linked to LDs and problems in adolescence.
In regard to childhood data, the use of clinical assessment data has a clear advantage in that it provides systematically collected assessment data for use in research. However, the use of the clinical sample is also problematic in terms of generalization of the results due to the referral bias. The children in the present data were typically referred by school psychologists, and the rationale for the referral may have varied according to factors such as personal preferences or school practices. Moreover, children with primarily socioemotional problems were advised not to be referred to the clinical assessment. It is presumable that a higher incidence of psychological problems would have been found if children with primarily socioemotional problems and co-occurring LD were also referred to the clinic. The possible bias due to the clinical sample is suggested by the notice that the incidence of internalizing and externalizing problems in children with LDs in our study was somewhat lower than the corresponding figures in a population-based study on LDs (Willcutt et al., 2013). Also, due to the clinical referral data, we could not control for factors such as IQ level, size of the LD subgroups, age, or gender distribution.
Another limitation of the childhood data was that we measured childhood psychosocial problems using a categorical variable that combined internalizing, externalizing, and attention problems. Owing to this decision, we may have lost relevant information concerning, for example, the effect of comorbid attention problems (attention deficit hyperactivity disorder [ADHD]) on adult outcomes in children with LDs. Hence, further research should be done to examine various psychosocial problems in childhood separately, particularly focusing on comorbid ADHD, to gain more in-depth knowledge of their long-term effects on individuals with LDs. Another limitation was that we used the teacher’s observations of childhood psychosocial problems as the primary information source. Because teachers have the best expertise in observing children in their learning environment, this selection was reasonable for a study focusing on LDs’ relationships to psychosocial well-being. However, parental observations along with teachers’ evaluations might have provided other aspects and a richer picture of the child’s psychosocial well-being. Yet another limitation regarding the childhood assessments was that most of the measures used to define LDs at the time the participants visited the clinic were unpublished and lacked psychometric data; hence, reliability of these measures cannot be reported. However, each test had unpublished norms based on comprehensive data and had been used on a routine basis at the clinic. Moreover, substantial learning difficulties were already identified at school and assessed by a school psychologist, followed by special educational support. If this support was not considered sufficient, the children would be referred to the clinic and difficulties would be confirmed as specific LDs at broad clinical assessments. Therefore, with these limitations, we consider the diagnosis of LDs reliable. Regarding the control group derived from the population registers, information on possible childhood learning problems was not available. However, a clear advantage of this control group was that it represented the population. Hence, it can be assumed that 5% to 15% of the control group members had LDs, considering that this is the estimated prevalence of LDs in the population in general internationally (APA, 2013).
Implications for Practice
As the children with LDs are at heightened risk for problems in adolescence, our findings indicate that (a) the development of children with LDs needs to be screened and monitored for the possible psychosocial problems and (b) continuous support provided. In educational and health care practices, psychosocial well-being should always be considered alongside cognitive deficit when planning support for individuals with LDs. Moreover, to support adolescents’ psychosocial well-being, possible learning problems should be considered in tandem with psychosocial problems instead of being treated separately in the same individual. Our findings indicate that individuals with LDs should be supported throughout the school years and adolescence, both academically and in their psychosocial well-being. Systematic educational support should not be withdrawn after the primary school years or after comprehensive school as is probably quite often the case.
Future Research
In the present study, the effects of LDs on adult-age outcomes, both direct and indirect, were generally rather small. This indicates that LDs are not necessarily linked to negative adult outcomes and that the majority of individuals with LDs cope well in life. However, it is still unknown as to which factors determine whether the individual is or is not affected by LDs that supposedly pose continual experiences of failure and major stress throughout school years. Some possible explanations for different adult outcomes were detected with individual assessments in a subsample of the present data: In a sample of individuals with RD, the continuity of the deficit into adult-age, not the initial childhood RD as such, was found to be related to unemployment (Eloranta, Närhi, Eklund, et al., 2019) and low psychosocial well-being in adulthood (Eloranta, Närhi, Ahonen, & Aro, 2019). Moreover, support experienced in adolescence was one of the predictors of improved RD in adulthood (Eloranta, Närhi, Eklund, et al., 2019). Earlier research on children has also shown that improving academic (reading) achievement decreases depressive symptoms as well as risk behaviors for later substance abuse and antisocial behavior (Ialongo et al., 1999; Kellam et al., 1994). In-depth knowledge of other possible protective factors in the lives of individuals with LDs is still needed, however.
This study did not examine whether the effect of LD on unemployment in adulthood was related to aging or societal era. Previous research has suggested that individuals with LDs may adjust to different life demands, such as entering working life, later than their peers. This means while elevated unemployment or having psychiatric problems differentiates them from peers in young adulthood, it no longer does so in their 30s (Werner, 1993). Moreover, differences in depression and anxiety between individuals with LD and controls have been found to diminish with age (see Klassen et al., 2013). Thus, it can be assumed that as graduating and being employed are related to psychosocial well-being and the individual with LD achieves these milestones later in life than peers, they also balance the general psychosocial well-being later in life. As employment is considered as one indicator of overall well-being, further research is needed to examine the association of employment with LDs in more detail and in relation to aging and societal era. Along with age, the general economic state in society may also be reflected in employment among individuals with LD.
By disentangling some factors mediating LDs and adult-age, we revealed that the association of childhood LDs with adult-age well-being outcomes is not simple or direct. Multiple factors intervene between LDs and adult-age and shape their relationship, and hence detecting these factors may enable us to find more effective means to support individuals with LDs. However, we were only able to scrutinize a limited number of potential mediators. This challenges further research to explore, for example, potential protective factors or attributes for success related to personal characteristics that may be crucial to how individuals with LDs cope in adulthood and that were beyond the scope of our study.
Footnotes
Acknowledgements
We are grateful to all the research assistants and staff at the Clinic for Learning Disabilities who contributed to the data collection, and to the study participants who generously gave their time to help with the research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research and authorship of his article has been financially supported by the Social Insurance Institution of Finland (Kela) and the Finnish Cultural Foundation.