
Abstract
Research on mandated occupational role change focuses on jurisdictional conflict to explain change failure. The authors’ study of the English National Health Service highlights the role of occupational dispositions in shaping how mandated role change is implemented by members of multiple occupational groups. The authors find that tension stemming from misaligned dispositions may emerge as members of different occupations interact during their role change implementation efforts. Depending on dispositional responses to tension, change may fail as members of the different occupations avoid interactions. This suggests that effective role change can be elusive even in the initial absence of conflicting occupational interests.
In professionalized settings, tasks and associated responsibilities are formally distributed across occupational groups. However, this distribution is not stable, as the highly professionalized healthcare field (Freidson, 2001) has witnessed over the past decades (Nancarrow & Borthwick, 2005). For instance, quality-focused policies led to the creation of new quality-focused roles (Menchik & Meltzer, 2010; Timmermans, 2003; Wiener, 2000), while attempts to increase community-based care led to the establishment of new advanced practice nursing and allied health roles (Chreim et al., 2007; Reay et al., 2006). Such changes in occupational roles in healthcare are often an outcome of policy mandates (Allen, 2000; Kellogg, 2014; Nancarrow & Borthwick, 2005; Wiener, 2000).
As emphasized by Abbott (1988), the implementation of policies designed to change occupational roles is not uniform. Occupations can resist, contest, or negotiate mandated role changes at a field level, shaping how they might be implemented (Anteby et al., 2016; Starr, 1984). In addition, interactions within and across occupations in the workplace can impact whether and how mandated changes are actually put into practice on the front line (Allen, 2000; Givan, 2016; Kitchener, 2000; Wiedner et al., 2017). Dynamics in the workplace can ultimately prevent effective policy implementation (Givan, 2016; Kellogg, 2011).
Prior research primarily focuses attention on jurisdictional conflict (Abbott, 1988)—that is, conflict between professions for control over work tasks—as the mechanism that might explain whether policy initiatives and other field-level pressures results in changes in workplace-level occupational mandates and roles. For example, Allen (2000) demonstrates how jurisdictional conflict between nurses and doctors shaped the redefinition of occupational role relations in response to a range of policy initiatives in a hospital in the English National Health Service (NHS). She highlights the importance of jurisdictional conflict by showing that nursing managers proactively defined new nursing roles to prevent medics from imposing them on nurses. Others similarly point to jurisdictional conflict as a mechanism shaping how roles are renegotiated in practice in response to policy initiatives (Kellogg, 2014; Nancarrow & Borthwick, 2005; Weinberg, 2004).
Although these studies provide valuable insights, they risk simplistically portraying individuals as rational actors whose actions and interactions are motivated by their jurisdictional interests. A broad range of research, however, suggests that the negotiation of occupational mandates, and roles in the workplace are shaped by a wide range of factors, including local work demands (Nancarrow, 2015; Xyrichis et al., 2017) and work ethos (Fayard et al., 2017; Nelsen & Barley, 1997). By moving beyond jurisdictional conflict, scholars have focused attention on dispositions—the categories of perception and appreciation, gained through lived experience (Bourdieu & Wacquant, 1992, p. 11)—in shaping how members of an occupation think and act. As an important driver of how members of occupations interact (e.g., Oborn & Dawson, 2010), dispositions may be critical in shaping how mandated role changes are negotiated between members of different occupations in the workplace. All of this suggests that a focus on jurisdictional conflict alone may not fully explain why a mandated role change may or may not succeed. In particular, we still lack knowledge concerning how dynamics that are shaped by occupational dispositions rather than jurisdictional conflict can affect mandated role change implementation.
In this article, we present an inductive analysis of local responses to a policy designed to shift regional public healthcare budgeting responsibilities from public healthcare system administrators (known as ‘commissioners’) to local primary care physicians (known as ‘General Practitioners’ (GPs)) in the NHS to further knowledge on how occupational dispositions can inhibit mandated role change implementation. The policy initiative, known as ‘Liberating the NHS,’ was described as the most fundamental restructuring in the organization’s 60-year history (BBC News Online, 2012). Initiated with the rationale that financial decisions should be guided by a clinical perspective (Department of Health, 2010, p. 1), the initiative mandated that primary care physicians across the country manage more than 60% (approximately £60bn) of the total NHS budget.
We find that differences in disposition across occupations can inhibit effective policy implementation even when members of the relevant occupational groups are initially eager to alter their roles. Our analysis suggests that the lack of effective policy implementation results from misaligned occupational dispositions as members of each group engage in actions that are interpreted negatively by members of the other occupational group. Dependent on their dispositions, these negative interpretations and judgments can lead members of each group to attempt to limit further interoccupational interactions, inhibiting the implementation of the mandated role change. We extend prior research by highlighting the importance of occupational dispositions in shaping how mandated occupational role changes are negotiated on the ground.
Theoretical Context
Jurisdictional Conflict and Changes in Occupational Roles
The overwhelming focus of prior research on the implementation of mandated role changes in the workplace is on the role of jurisdictional conflict in shaping whether or how role changes are implemented. Policy mandates can trigger both field-level jurisdictional conflict and workplace-level conflict over the renegotiation of local occupational mandates and associated occupational roles. An occupational role is a set of expectations about who does what work, how work should be performed, and how someone in one occupational role will interact with others (Abbott, 1988; Freidson, 1988; Okhuysen & Bechky, 2009). An organization’s work is constituted through a role system that is comprised of multiple, interdependent and interacting occupational roles (Abbott, 1988; Bechky, 2003). Due to the interdependent nature of roles, mandated change in one occupational role necessarily involves changes to other roles and thereby to the role system (Abbott, 1988; Eisenstadt et al., 1967; Turner, 1990). Given that different occupational groups in a role system are constantly competing for jurisdictional control over valuable or high-status tasks, changes in roles can trigger jurisdictional conflict.
Extant research has highlighted the importance of jurisdictional conflict in contributing to diverse outcomes related to policy implementation (Ferlie et al., 2005; Kellogg, 2014; McDermott et al., 2013; Nigam et al., 2016). Moreover, jurisdictional concerns, or the effective ability to reduce status hierarchies across well-established jurisdictional boundaries, are also important in shaping the potential for coordination and conflict in multiprofessional teams (Edmondson, 2003; Huq et al., 2017; Nancarrow et al., 2013; Xyrichis et al., 2017).
Consistent with this broader body of research, studies on how mandated role changes are implemented in the workplace focus on the importance of jurisdictional conflict in shaping how policy implementation unfolds (Anteby et al., 2016). This work presupposes that members of the higher status occupation within a particular role structure make a judgment about a policy initiative’s impact on their jurisdictional interests and, based on that judgment, either engage with implementing the policy or resist it (e.g., Kellogg, 2011; McNulty & Ferlie, 2004). For example, Currie et al. (2010) show that physicians resisted a policy initiative that aimed to bring cancer genetics care into community-based settings by enhancing the nursing-genetics role. Physicians continued to have expectations of a more traditional doctor–nurse working relationship and subverted the policy by limiting the autonomy of the individuals who assumed the new nursing roles. Similarly, in a study of reforms related to the Affordable Care Act, Kellogg shows that members of high-status occupations resisted performing new tasks that they interpreted as requiring the acquisition of “information unrelated to their professional expertise” (2014, p. 912) and/or as involving work practices that conflicted with their professional identity and interests. They were able to subvert the policy by not engaging with the mandated role changes. Alternatively, Chreim et al. (2007) demonstrate that primary care physicians judged that a policy initiative to move care toward an interdisciplinary team model would advance their occupation-specific goals and hence cooperated with the initiative to introduce new occupational roles within the primary care setting. In sum, research shows that concerns about jurisdictional interests can shape occupation members’ actions in a broad range of settings, including implementation of mandated role changes in the workplace.
An exclusive focus on jurisdictional concerns, however, may be incomplete. Although professions and professionals can and do act in ways that are interest-driven, this behavior is layered onto a more complex set of motivations and rationales that shape action. This may matter in shaping how members of an occupation act and interact in the workplace generally and how they respond to mandated role change specifically.
The Role of Occupational Dispositions in Implementing Mandated Role Change
Potentially complementing a focus on jurisdictional conflict, a large but disparate body of research suggests that occupational dispositions—which structure or guide members’ interpretations and habitual actions (Bourdieu, 1985)—shape how professions act and interact (Anteby et al., 2016; Bosk, 2003; DiBenigno, 2018; Hughes, 1981). According to Hughes (1981), [l]iterature and common sense … have given us stereotyped pictures of persons engaged in various occupations: the old-maid school teacher, the parson, the village blacksmith, the farmer, the professor, the politician, the financier. All these and many other types so created are expected to react to the situations of life in a characteristic manner. (p. 24)
Occupational dispositions become an engrained and habitual way of interpreting the world. For example, engineers routinely view organizations as machines (Morgan, 2006). According to Lawrence and Lorsch (1967), distinct work patterns manifest themselves in different goal and temporal orientations within organizations, such as between sales representatives and members of R&D teams. Dougherty (1992) encapsulates the idea of occupational dispositions in noting that members of differing occupations, even when forming part of the same organization, inhabit different “thought worlds.”
In shaping worldviews, occupational dispositions can structure how members of an occupation behave as part of their routine work and beyond. For instance, in a study of clinicians’ practices at a mental health clinic, Kirschner and Lachicotte (2001) observed supervision meetings in which matters were often left unresolved, mirroring the open-endedness of “the structure of psychodynamic therapy itself” (p. 448).
Moreover, occupational dispositions might shape how members of different occupational groups interact with one another. For example, Currie et al. (2010) show that nurses who are formally in charge of designing and implementing change may struggle when an initiative involves physicians, in part because their dispositions may prevent them from challenging higher status medical professionals. Wiedner et al. (2017) witnessed similar dynamics with regard to primary care physicians struggling to implement changes to local healthcare services due to being deferential to higher status hospital consultants. By contrast, Pouthier (2017) suggests that shared dispositions, exemplified by shared identification rituals involving joking and griping, can enable coordination in cross-professional teams delivering palliative care to cancer patients. In this case, shared dispositions develop across occupations within a specialty area (palliative care) and differ from the dispositions in other specialty areas (e.g., acute care).
As an important driver of how members of an occupational group will behave and, specifically, interact with others, occupational dispositions are likely to play a role in how mandated role changes are negotiated. A dispositional focus, then, may complement the focus on jurisdictional concerns that predominates prior research. Given the lack of research examining dispositions in processes of implementing mandated role change, we thus address the research question: How do occupational dispositions impact interactions between members of different occupational groups in the process of mandated role implementation?
Methods
This article is based on an ethnographically informed, in-depth single case study, which is appropriate to gain insights concerning a phenomenon that has remained undertheorized (Ozcan et al., 2017; Yin, 2003). Our qualitative study concerning mandated occupational role change in the NHS started in 2010 in response to the government’s announcement of a policy to radically restructure how the public healthcare system was managed. The policy involved shifting responsibilities for managing local public healthcare budgets from administrators to GPs.
This was not the first effort to engage GPs in managing public healthcare budgets. Around twenty years earlier, GPs across the country had been given opportunities to make certain budget allocation decisions, which were initially restricted to nonurgent elective and community care. However, “GP fundholding” was abolished after only 6 years. Subsequent attempts to engage GPs in healthcare systems management included the national “practice-based commissioning” policy (in 2004) that allowed GPs to advise local healthcare management agencies on budget allocations. Yet, these agencies, which were largely staffed by nonmedically trained administrators, maintained responsibility for healthcare management decisions.
Studying responses to a policy designed to radically change administrators’ and physicians’ responsibilities provides an extreme case with high revelatory potential (Siggelkow, 2007) for understanding dynamics that may occur following attempts to change an established multioccupational role structure. Unlike other cases of expanding physicians’ roles by increasing managerial duties (e.g., Kitchener, 2000), successfully implementing this radical change appeared to require the transfer of a complex and highly specialized body of knowledge from those who had been performing relevant tasks to those who were assuming responsibilities for them. It therefore required interoccupational collaboration.
We began by collecting data to help us understand public healthcare systems management (“commissioning”) and how stakeholders reacted to the change policy. With regard to the former, we primarily reviewed academic literature (e.g., Flynn & Williams, 1997) and reports published by the U.K. government and relevant think tanks (e.g., Cohen & Light, 2003; Department of Health, 2005; Woodin & Wade, 2007) and also interviewed a small number of administrators and clinicians across the country. Through interviews, along with articles from the media and trade journals (e.g., Dixon & Ham, 2010; West, 2011), we sought to gauge responses to the policy.
Our objective at this stage was to identify a relevant research site that would allow us to observe efforts to implement mandated role change. Given uncertainty about whether the policy would be implemented at all, we decided to focus on healthcare management agencies where administrators had started preparing for change and where local GPs appeared keen to assume commissioning responsibilities.
Having gained access to one such site, the first author received permission to conduct further interviews and attend management-related meetings. This was followed by two 3-month periods of observations, in which the first author shadowed administrators (Czarniawska, 2007) for 3 to 4 full days a week to gain an in-depth understanding of how they were adjusting to the new policy and whether and how GPs were becoming more involved in commissioning-related work. In total, the study involved 3 years in the field, from the initial interviews to identify a research site to interviews conducted after the two periods of observation. In this time, we had conducted more than 700 hours of direct observation, reviewed 20 Gb of confidential documents, and completed a total of 66 semistructured interviews with administrators in the region (42), local GPs (9—all of whom initially expressed a desire in becoming involved in aspects of commissioning), and other stakeholders with some involvement in aspects of public healthcare management (15). In addition to semistructured interviews, the first author also asked questions during periods of observation while attempting to minimize interference and disruption for participants. In this respect, informal chats with administrators and GPs before and directly after commissioning-related meetings were especially valuable. As the study progressed, we became intrigued by our observation that knowledge sharing was limited despite initial enthusiasm and focused our analysis on understanding why.
Our ongoing data collection and analysis proceeded iteratively, with emerging questions generating provisional answers, further data collection, and further questions (Alvesson & Kärreman, 2007; Wiedner & Ansari, 2017). Through this process, we identified interoccupational tension, and the negative judgments that both administrators and GPs formed of the other group in the course of negotiating new roles, as important. We then focused our efforts on identifying the specific sources of tension and actors’ responses. Repeatedly comparing our emerging interpretations of the empirical data with theory (Mantere & Ketokivi, 2013), specifically an emergent focus on occupational dispositions, we progressively abstracted from our particular case to develop a theoretical model specifying how misaligned occupational dispositions may inhibit mandated role change implementation in practice. Examples of data for each of the themes that comprise our model are presented in Table 1 of the online appendix.
Findings
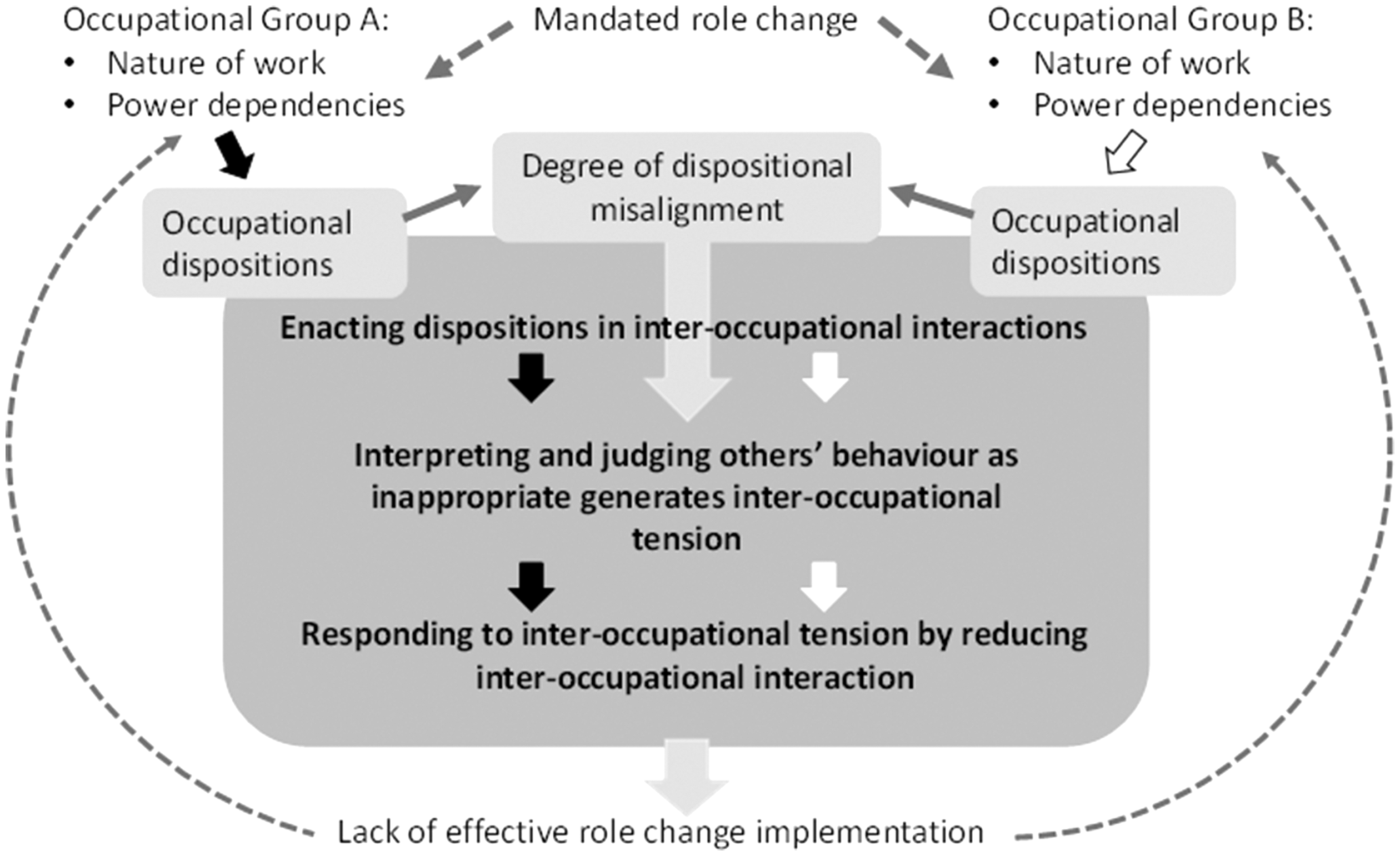
We found that implementing mandated role change involved members of the occupations whose roles were being altered interacting with one another to negotiate their new roles. These interactions were substantially influenced by the dispositions of the different occupational groups, which ultimately inhibited successful policy implementation. Figure 1 presents our model of relevant dynamics. It shows that the nature of GPs’ and administrators’ work and power relations shaped their occupational dispositions. Although dispositions were principally shaped by long-standing work practices and established power relations, the latter were somewhat impacted by the mandated role change itself. These dispositions, in turn, shaped how members of each group interacted in their efforts to negotiate their new roles. The same dispositions, along with the degree of misalignment between them, influenced how members of each group interpreted and judged each other’s actions. High misalignment between GPs’ and administrators’ dispositions generated tension in interoccupational interactions, leading to negative judgments and interpretations. Both groups, in accordance with their dispositions, responded to emerging tension in ways that reduced further interoccupational interaction. This contributed to a lack of transfer of commissioning-related activities to GPs, thereby inhibiting the implementation of the mandated role change and ultimately reinforcing the existing role system. We unpack these dynamics later.
The Role of Occupational Dispositions in Inhibiting Mandated Role Change Implementation.
Occupational Dispositions
In the following, we contrast each occupational group’s primary focus of interest, typical decision-making speed and routine enactment of discretion with one another. We also consider the immediate impact of the announcement of the mandated role change.
GPs’ Dispositions
GPs’ primary focus of interest at work concerns diagnosing individual patients, prescribing medicine and referring patients to relevant specialists. As a result, diseases, treatment methods, patients’ responses to them, and individual specialists are more meaningful for GPs than governance arrangements in the NHS. As one GP noted: Even if you have been working in the service like I was for all those years, it is amazing how you don’t really care [about formal organizational structures]. Because you are focused on your insular little GP surgery world with one patient. (GP #1, interview)
GPs’ routine work also affects their temporal orientations: GPs typically diagnose, decide on appropriate treatment methods, and write up a summary of their consultation in less than 10 minutes (Carr-Hill et al., 1998). GPs therefore necessarily employ heuristics (Gabbay & Le May, 2004).
Finally, GPs’ relative power vis-à-vis other occupations, specifically their possession of valued medical knowledge and status as independent contractors who own their practices, allow them to enact a relatively high degree of discretion. GPs exercise their professional judgment when diagnosing patients and suggesting treatment options, arguing that their personal experiences with patients, medications, and local specialist services enable them to provide nuanced treatment methods. As is the case with most professionalized occupations, GPs regularly resist attempts to limit their discretion: “GPs don’t like being managed … and we don’t like being told. So [if someone] wants to change general practice, we say ‘bugger off!’ (GP #6, interview).”
The U.K. government’s announcement that GPs were going to assume responsibilities for managing regional healthcare budgets (Department of Health, 2010, p. 27), in addition to previous reforms designed to encourage GPs’ input in commissioning, further signaled that GPs were trusted to make healthcare management-related decisions, reinforcing beliefs that GPs’ high level of discretion is appropriate. In giving them freedom to shape regional healthcare services, the mandated role change appeared to confirm GPs’ abilities to enact a high degree of discretion beyond their traditional professional role as clinicians.
Administrators’ Dispositions
In contrast to GPs’ attention to individual patients and treatment pathways, administrators focused their attention on the organizational structures and financial flows across the regional healthcare system. Much of their work involved monitoring expenditure, reviewing performance indicators and examining contracts negotiated with public and private organizations. During meetings, administrators routinely presented expenditure figures and interorganizational disputes. The focus on these issues stemmed from the central role of contracts and financial pressures on administrators’ work. A particularly telling moment occurred when an administrator delivered an improvised leaving speech to her colleagues. After beginning to cry, she stated: “I do hope that I was able to get some money out of those contracts” (Administrator #22, observation notes).
Unlike GPs, who engaged in rapid, heuristic-based decision making, administrators were used to being involved in several months-long decision-making processes. The need to follow national policies and regulations, coupled with lack of expertise concerning specialized healthcare services, resulted in decisions routinely requiring the input from a number of stakeholders across several hours-long meetings. This resulted in decisions, such as awarding or terminating a contract, taking up to a year. For instance, referring to an initiative to save money by no longer paying for an underutilized ward in a hospital, one administrator noted: “We’ve got to go around the scrutiny committee and all the politicians, the local involvement network, all sorts of other things … you can’t just say this is what [we will do]” (Administrator #6, interview).
Similarly, local healthcare needs assessments required inputs from several stakeholders and could take longer than 6 months. Administrators did not consider this slow. Rather, they were to be expected given “statutory obligations” (Administrator #5, interview).
Finally, administrators’ lack of power limited their ability to enact discretion. Despite having formal responsibilities for managing budgets and thereby altering local services, administrators’ abilities to make decisions to shape the healthcare system were constrained. This was because their lack of clinical expertise limited their ability to evaluate local services and suggest changes. Furthermore, the existence of monopoly providers inhibited their ability to threaten the withdrawal of funding. Large hospitals, in particular, could rely on the media and politicians to come to their aid if they faced financial difficulties and to pressure local commissioners to continue to fund services even if they were unsustainable. As one administrator noted, “if the [commissioning organization] is ever in the media, then it’s negative: … ‘you’re a bunch of swines because you’re cutting [services]’” (Administrator #8, interview). In addition, the increasing use of standard treatment episode charges reduced commissioners’ ability to negotiate prices. Most of the evaluation criteria were also set at a national level, limiting monitoring activities to performance indicators and targets that administrators could not influence.
Administrators consequently saw their roles as following procedures, implementing policies and trying to prevent the financially strained local healthcare system from collapsing by asking local providers for ways of increasing efficiency. As one administrator noted: What you’re doing is, you’ve got to deliver these centrally set targets, which actually cost more than the resources that you’ve got anyway … We don’t have the capacity or skills or leverage to make … major changes. [We have] very little influence … Most of our work is in terms of working with people to plan or tweak the service models that we have and the pathways and how do we do that to save money, basically. (Administrator #3, interview)
Shifting commissioning responsibilities from administrators to GPs meant that the former were now officially assuming a supporting role for the latter. This shaped dispositions by reinforcing administrators’ deference to GPs because the latter were no longer only associated with high-status medical knowledge but also with directly affecting their careers.
Dispositional Misalignment Leads to Negative Interpretations
Occupational dispositions can shape actors’ actions and interpretations in settings beyond their everyday work. These settings include interoccupational interactions in which details concerning policy implementation are negotiated and role transfer is initiated (see dark-shaded area in Figure 1). Dispositional misalignment leads certain actions to be interpreted as inappropriate, generating interoccupational tension.
The implementation of the mandated role change began with a group of administrators and GPs who were initially predisposed to making the initiative a success. Administrators invited GPs to join them at internal commissioning meetings and meetings with external stakeholders. The GPs who chose to participate in the first implementation efforts were regarded as “evangelists” (Administrator #6, interview) who wanted to play an active role in transforming the local care system. However, through their interactions, administrators progressively developed a view of GPs as being ignorant and selfish, and GPs judged administrators as being slow and inefficient.
Differences between members of the two occupational groups became evident during commissioning meetings. For instance, in stark contrast to the norm of starting a meeting about 5 minutes past the official starting time to allow attendees to prepare themselves, we observed that occasionally GPs pushed for meetings to begin early to save time. Also, GPs at times interrupted and argued with administrators, checked their emails on their phones (“started playing with their blackberries” according to Administrator #3), or simply left if they felt that their presence was not required. As one administrator noted: “I had a meeting the other day … where, after half an hour … a GP [suddenly] said, ‘I don’t see what I’m doing here’ … and off he walked” (Administrator #37, interview).
GPs also did not hesitate to voice their opinions and propose solutions to what administrators perceived as highly complex problems that required extensive analysis and negotiation. As one administrator noticed, as costs concerning the redesign of a local service were being discussed, one GP remarked: “by the time this is implemented it will be down to us to do the commissioning and we’ll just spend the money intuitively” (Administrator #14, interview). Using intuition contrasted sharply with administrators’ adherence to formal procedures. In addition, in contrast to administrators’ focus on numbers that represented total volumes or averages to evaluate provider organizations, GPs at times discussed issues that their registered patients were experiencing. Moreover, recognizing potential conflicts of interest did not deter GPs from making local healthcare management-related suggestions from which they appeared to personally benefit: “I’m still at a loss as to why we don’t integrate more [secondary health services] into general practice; yes, I am biased; I am a GP, but what the hell!” (GP, observation notes).
In summary, GPs adopted a very direct and personal style, which was at odds with the diplomatic approaches characteristic of administrators.
Despite a lack of visible conflict, administrators experienced tension. This tension arose “based on experience” of interacting with GPs, “not simply blind prejudice” about them (Administrator #5, interview). Furthermore, this tension did not appear to stem from jurisdictional battles as administrators we interviewed largely approved of GPs having to take “ownership” (Administrator #12) for unpopular decisions.
Notably, administrators interpreted GPs’ behaviors in commissioning-related activities as potentially disruptive to their everyday work and the local healthcare system. Administrators especially complained about GPs’ inability to recognize their ignorance about the complexities involved in commissioning. For instance, referring to the aforementioned GP’s comment on intuition, an administrator noted: You can’t really have a GP come out of a ten minute consultation and in five minutes, before the next one, get the facts and intuitively spend £200 million of tax payers’ money … They can’t be doing that. I think where this comes from is a remarkable arrogance. (Administrator #14, interview) A GP … told me the other day: “We run our own businesses, so of course we know how this works.” Well, it’s very different running a very small GP practice of four or five GPs, as opposed to a [multi-]million pound business! (Administrator #32, interview)
I specifically remember a meeting in which one GP started by talking about “let’s think about the analogy of the kitchen. I want the kitchen, this is the budget I’ve got for it. You want to sell me this kitchen which has these units, these things and these things, but I don’t like the color of these units” … and we [an administrator and I] were looking at each other and thinking, “oh God!” (Clinical Director #1).
Administrators and other stakeholders also confided in interviews their worry about GPs’ apparent focus on their own practices rather than thinking about implications of commissioning decisions for the entire region. One administrator (#5) commented that GPs’ general approach to commissioning amounted to stating “I have this skill and I’ll [provide this service] for this amount of money, so give me this money to do it”; [which indicated that they] “don’t seem able to separate their two roles: provider and commissioner.”
Administrators deduced from their observations of GPs’ behavior that GPs were transferring their habitual ways of working to a setting where they were out of place, thereby “not bringing out the best in them” (Administrator #42, interview), which, in turn, generated interoccupational tension. As one administrator (#11) commented in an interview, “we are talking of two organizations with completely different styles; GPs coming in and working in a certain way that we are not accustomed to.”
In line with their acceptance of highly limited discretion based on their routine work, as well as the reinforcement of unequal power relations via the mandated change of commissioning responsibilities, administrators did not challenge GPs in meetings. As one administrator (#36) noted in an interview, “managers become reserved when you are around a dominant GP because there is a sense of hierarchy and you are not meant to argue with your clinical lead.” A provider representative who witnessed such behavior referred to administrators as “bloody sycophants” (Clinical Director #1, interview).
Administrators’ deference to GPs contributed to situations in which the former refused to be seen as guiding the latter, even when they evidently held relevant knowledge. For instance, at one meeting about organizational structures concerning community care provision, GPs asked the community care commissioner which option he would recommend. In response, the commissioner said he did “not want to influence” them and that “my view doesn’t matter here. It’s your decision” (observation notes). Similarly, administrators did not intervene when GPs agreed in a meeting to amend a contract with a local provider by adding a clause that was not legally enforceable (observation notes). Regarding administrators’ general lack of intervention, one administrator (#36) commented in an interview that “you have to suck up to the clinicians, really. But it is frustrating when you can see that something is being done that isn’t right.”
Meanwhile, when asked in interviews to assess their meetings with administrators, several GPs used terms such as “a waste of time” and “pointless.” One commented about administrators’ adherence to standard procedures: “they have crap management … they were really the old-school contract management” (GP#6). One GP (#8) noted that administrators, due to their lack of clinical experience, “have never seen [a] service [they commission] work and they don’t know what the pitfalls of it are,” adding that their routine and rigid “segregation” of tasks related to “finance, contracting, and [designing, as well as monitoring] clinical services” did not make sense. With regard to administrators’ inflexibility about rescheduling meetings, one GP commented:
I asked [the administrators] to change them to Mondays, because I thought for the managers it doesn’t really make much difference to them. And that caused some hoo-ha, as you heard, at the last meeting: “Oh, then we can’t get the papers to you [on time]. and …” And I was thinking, “well why? You just release them the day before, as you do with any meeting.” (GP #2, interview).
In interactions with one another, GPs and administrators largely enacted their traditional roles: GPs, who were used to high levels of discretion and making relatively quick decisions, displayed dominance and impatience. Given their traditional focus of attention on their registered patients, they also brought up issues that might only affect a small number of individuals or from which they could personally benefit. Meanwhile administrators—who were used to analyzing contracts and multimillion pound budgets, reaching decisions only after months of negotiation and deliberation, as well as implementing orders from those hierarchically above them—largely remained silent or referred to standard procedures. Interpreting each other’s behavior as inappropriate, members of both occupations experienced tension.
Responding to Interoccupational Tension by Reducing Interoccupational Interaction
In addition to contributing to potential interoccupational tension, occupational dispositions also shape responses to tension. Administrators avoided tension by being deferential to GPs in public while also limiting GP involvement in their administrative work. GPs, in turn, responded by avoiding extensive involvement in activities with administrators who they came to perceive as wasting their time. Taken together, these responses had the effect of reducing interoccupational interaction, as shown in our model.
Responding to GPs’ apparent ignorance concerning commissioning, administrators could have attempted to educate them by exposing them to the complexity of commissioning tasks. However, given their interpretations of GPs as impatient, aggressive, and unwilling to listen, in conjunction with their own deference to higher status GPs and their dependence on GPs for keeping local commissioning jobs, administrators generally concluded that “clearly you can’t just tell GPs” how they ought to perform their new role (Administrator #32, interview).
Reluctant to directly challenge GPs, administrators adopted other methods of dealing with tension. In particular, they restricted GPs’ involvement in commissioning by directing them to particular types of meetings and splitting existing meetings into “operational” (to which administrators occupying lower pay band positions were invited) and “strategic” meetings (to which GPs and senior administrators were invited). Administrators justified this on the grounds of maximizing efficiency: A GP [said to me]: “I need to know everything you know!” And I said …, “you don’t need to know everything I know … Your career is as a GP. You have a huge skill set … You set the vision.” (Administrator #42, interview)
Administrators were especially keen for GPs to make use of their available time by attending public “scrutiny committee” meetings in which politicians tended to ask difficult questions concerning how the local healthcare system was being managed. As one administrator (#3) commented, GPs were in a position to dismiss any criticism by stating “this [system] is better for the patients; what do you know about it?” Although such meetings arguably provided learning opportunities for GPs about the political nature of budget allocation decisions, they did little in terms of increasing their understanding of the day-to-day work underlying them.
Some administrators recognized that separating commissioning-related work into separate tasks, undertaken by different groups of individuals who rarely met each other, was ineffective. In fact, one administrator had made efforts to combine a few existing work streams. Nevertheless, the same administrator (#6) also argued in an interview that GPs “are not going to sit in three hour contract meetings” and would not want to “deal with basic service issues … and all of that … because it takes longer than seven minutes, actually.”
Finally, administrators persuaded GPs to use their valuable time as effectively as possible by focusing on a few “strategic priorities” (Administrator #13, ethnographic interview). As a result, GPs had to provide written justifications for any time spent on commissioning-related activities to their respective representatives. GPs who recognized that certain issues, such as redesigning community-based mental healthcare services, were complex and required lengthy negotiations with stakeholders were unhappy with this arrangement. As a result, one GP (#5), who had been very active initially, withdrew from all commissioning-related activities after complaining about this attempt to limit his involvement.
Administrators’ responses to tension by reducing interaction were consistent with their habitual ways of dealing with conflict. Notably, one administrator (#3) commented that instead of directly confronting issues, such as underperforming colleagues, “we just work around them and everybody knows that.”
Unlike administrators, GPs did not appear to be afraid of offending others (apart from higher status medical doctors) in interoccupational meetings by being confrontational. However, they seemed to favor avoiding interoccupational engagement as they became increasingly frustrated about their lack of perceived progress—or, in their own words, “got pissed off with the whole thing” (GP#7, interview). Rather than seeing interactions with administrators as opportunities for learning about commissioning, GPs increasingly seemed to think that “going to meetings” meant they had less time to “save lives” (GP #2, informal conversation). Their disposition to maximize efficiency via quick interventions left little time for finding ways of developing interoccupational collaboration.
Reduced Interoccupational Interaction Inhibits Effective Role Change Implementation
Finally, our model highlights that reducing interoccupational interaction inhibits effective role change implementation. This is because shared understandings of how the new roles should be enacted are not developed. Consequently, the nature of work and power dependencies of the occupations involved may remain largely unchanged.
In our case, GPs’ exposure to everyday commissioning activities remained limited as their involvement was directed to attendance at “strategic meetings.” As a result, 4 years after they had first been approached by administrators, GPs appeared to still have a rather limited understanding of the commissioning role. During interviews, GPs confessed they had difficulties interpreting certain management documents, not least due to the heavy use of acronyms that they were unable to decipher. One GP (#9) noted more than 4 years after the policy announcement that she still did not “know the details of contracting” in the NHS and wondered why it was so difficult compared with contracting in the private sector.
GPs’ limited attendance of commissioning-related meetings contrasted with those of several administrators, who typically spent several days a week in back-to-back meetings. Asked whether going to so many meetings was a productive use of their time, one administrator (#37) noted that every meeting typically provided “a nugget of information” that resulted in learning something new and potentially consequential. Starved of these “nuggets of information,” GPs reinforced their views of administrators’ work as largely useless.
In addition, because most of the administrative work was performed outside of the few meetings that GPs attended, GPs began having doubts about their ability to influence decisions. One GP (#8, interview) complained about an “illusion of choice” that administrators presented to GPs, when in fact they had decided beforehand how to proceed. Meanwhile, administrators’ views of GPs as simply being unable to understand their work were also reinforced due to GPs’ limited learning, with one noting, “they understand their world [but] trying to get them to understand a different world is really quite difficult” (Administrator #29, interview).
In summary, by directing GPs to a very limited number of specific types of commissioning-related activities, administrators inhibited GPs’ ability to understand and perform certain tasks that comprised their extended roles. This was reinforced by GPs’ withdrawal due to frustration concerning administrators’ apparent lack of guidance and flexibility. GPs’ existing roles, including their role-specific worldviews, were thereby left largely unchanged. Administrators consequently predicted that public healthcare commissioning would “go on much as before” (Administrator #3, interview).
These findings are consistent with other studies that have sought to evaluate GP-led commissioning across the UK. In particular, they support McDermott et al.’s (2017) claim that GPs can only “add value” to healthcare commissioning if extensive “time and effort” has been invested “in preparing those involved” to ensure “that they systematically gather evidence about service gaps and problems” (p.10). They also support the observation made by the same researchers that GPs have limited their engagement in certain commissioning-related activities based on perceptions that they “are not a good use of GP time” (2017, p. 8). Importantly, this article adds insights into how this preparation and engagement may fail to emerge by foregrounding the role of misaligned occupational dispositions in shaping interoccupational interactions.
Departures From the Model
The narrative above may give the impression that occupational dispositions created strong misalignment between every GP and every administrator, triggering universal resentment and a complete unwillingness to collaborate. Although our model reflects the predominant themes emanating from our analysis, we did witness a few outliers that suggest that occupational misalignment varies in practice and that interventions designed to change the above described dynamics could succeed.
With regard to occupational misalignment, we noticed that a small number of semiretired GPs appeared to be more accepting of administrators’ work style, including lengthy meetings and rigid procedures. These few GPs continued to attend commissioning-related meetings until we stopped collecting data. Apart from these individuals simply having more time to engage in nonclinical work, as well as their desire to reduce their routine clinical work by “learning new skills” (GP #1, interview), their continued interoccupational interaction may be attributable to their previous work in GP fundholding and engagement with administrators in relation to earlier reforms. In other words, their experiences may have reduced the occupational misalignment between themselves and administrators.
With regard to possible interventions, GPs’ reflections on their experiences in interviews are potentially instructive. For instance, one GP (#7) commented that due to GPs being used to having a high degree of autonomy, “they are always able to speak their minds. So, that is a strength … but it also means that if they are not self-disciplined and sensitive enough, you can end up with dysfunctional meetings.” Another GP (#9) concurred that her colleagues could be quite aggressive, stating, “that is very true. I have seen that … and they might not really know what they are talking about.” Yet another GP (#6) admitted that her own behavior had been problematic (or had made her look “like a complete idiot” in her words), as she later, when taking part in a leadership training program, came to realize. These comments suggest that increased awareness of how one’s behaviors may be interpreted by members of another occupation may help in preventing the buildup of interoccupational tension. At the same time, the interviews also highlight how difficult it may be to change strongly internalized occupational dispositions, with GP#6 noting that despite increased self-awareness, “it is too late [for me] to change, sorry … If I had done it [leadership training] ten years ago, I might ’ve been able to modify my behavior. By then it was too late.”
Discussion
We examined how occupational dispositions may contribute to inhibiting mandated role change implementation. Our findings suggest that misaligned occupational dispositions may lead to the emergence of interoccupational tension, which actors address by reducing interoccupational interaction, thereby undermining actors’ abilities to effectively alter their roles. In demonstrating the importance of misaligned dispositions in inhibiting mandated role change implementation, our findings provide an alternative to the predominant view that role change is primarily dependent on the outcomes of jurisdictional battles between occupational groups (Abbott, 1988).
Attributing change implementation dynamics to occupational dispositions departs from a model of human motivation and action that is grounded in rationality and protection of self- and/or group interests (Coleman, 2009). This rational actor model is either implicit or explicit in accounts focused on jurisdictional conflict (Abbott, 1988) as well as much of the broader sociological literature on professions and professional work (Freidson, 1988; Starr, 1984) and has been a subject of some prior critique (Eyal, 2013). Although our findings do not deny the potential relevance of such interests, we argue that foregrounding nonreflective habitual behavior in interoccupational interactions adds important insights about mandated role change implementation that would otherwise remain hidden.
Conclusion
Given the broad importance of dispositions in shaping social interaction across a wide range of domains and contexts (Bourdieu, 1985), we anticipate that dispositions would play a complementary role to jurisdictional disputes in shaping the implementation of a broad range of mandated role changes. However, there are boundary conditions defining where dispositions might be more likely to feature prominently. Dispositions may be particularly useful for understanding the difficulty of effectively implementing change in situations where actors do not feel that their occupational interests are being threatened. This can include cases where mandated role changes give higher status occupations opportunities to hive off lower status scut work (Huising, 2015). In our case, the policy of granting healthcare systems management responsibilities to GPs appeared to trigger minimal jurisdictional conflict between them and administrators because the former were not losing control over their clinical domain and administrators had limited control over their local healthcare system anyway.
Dispositions and how they shape interactions may also be relatively more important when implementing mandated role change creates situations involving members of different occupational groups that do not habitually interact. Our article examines the role of nonprofessionals who normally interact infrequently with clinicians. In doing so, we develop a contrast to traditional depictions of professionals as being in a position to resist and subvert change (e.g., Givan, 2016; Kellogg, 2011) and administrators as mere implementers (Lipsky, 1983). Instead, we find that the latter may (perhaps unintentionally) play a role in inhibiting change. Yet, our focus on interactions involving administrators raises the question of whether this occupational group is in some ways unique or noncomparable to lower status clinical professionals. Would we expect the dynamics we identified to emerge in the context of mandated role change involving physicians and nurses? Arguably, due to somewhat shared educational experiences, the degree of dispositional misalignment between different types of clinicians is generally lower than between clinicians and nonclinicians, potentially reducing the number of situations in which actors judge each other’s behavior as inappropriate. Moreover, physicians’ and nurses’ experiences of working together in their day-to-day work is likely to contribute to shared understandings (Brown & Duguid, 1991) that may prevent the buildup of interoccupational tension.
In summary, while we argue that our model is transferable to other settings, the difference between GPs and administrators may represent an extreme case of dispositional misalignment that results in interoccupational tension becoming particularly salient. We call for more empirical studies of mandated role change implementation involving diverse occupational groups to assess the transferability of our model.
Our findings also have implications concerning the managerialization of professional work and professionals’ experiences of assuming increased administrative and managerial responsibilities (Waring & Currie, 2009). Much of this literature focuses on the individuals who experience transitions to managerial roles and the identity-related tension that results from adopting multiple, potentially conflicting roles (McGivern et al., 2015). In addition, the risk of clinicians being ostracized by members of their own occupational group once they assume managerial roles has been documented (Thorne, 1997). Our case instead highlights that challenges may arise even when professionals seem eager to assume aspects of nonprofessional work—and that success may depend on how interoccupational interactions evolve.
In addition, our analysis presents an interesting contrast to prevailing assumptions about the impact of change initiatives on dispositions. Specifically, mandated changes are often theorized as causing disruptions that call into question traditional behaviors (Kotter, 1995). In other words, actors may become aware of how their dispositions are no longer aligned with their environment, triggering adjustments. Alternatively, dispositions may simply fail to adapt to changing circumstances (Strand & Lizardo, 2017). Our analysis suggests a further possibility, namely that mandated changes may reinforce existing dispositions—such as a shift in responsibilities confirming GPs’, and denying administrators’, abilities to enact discretion. This finding has important implications for understanding unanticipated consequences of change initiatives (Balogun, 2006; McKinley & Scherer, 2000; Wiedner et al., 2017) and why supposedly radical change initiatives may represent continuity (Brunsson, 2009).
Finally, beyond its theoretical significance in terms of understanding mandated change implementation processes, our focus on the importance of disposition, and dispositional misalignment has important implications for policy design and implementation. As reflective comments from GPs in our findings show, actors’ increased awareness of (a) their own dispositions, (b) how their behavior may be interpreted negatively by others, and (c) how this may ultimately contribute to undermining desired change efforts and can support the suppression of actions that may generate interoccupational tension. This suggests that efforts to implement role changes may need to focus on supporting actors’ self-awareness, empathy, and reflexivity so as to minimize the potential for interoccupational tension to develop, as well as to help actors constructively deal with tension once it has emerged.
Via our analysis of local responses to the policy of shifting healthcare systems management responsibilities from administrators to GPs in the NHS, we have shown that misaligned occupational dispositions may contribute to inhibiting mandated role change implementation due to the buildup of interoccupational tension. By highlighting the role of occupational dispositions in shaping the negotiation of mandated role change implementation between members of different occupations, we add important insights to role changes in professionalized settings in general, and healthcare systems management in particular.
Supplemental Material
sj-pdf-1-wox-10.1177_0730888420918643 - Supplemental material for General Practitioners Are From Mars, Administrators Are From Venus: The Role of Misaligned Occupational Dispositions in Inhibiting Mandated Role Change
Supplemental material, sj-pdf-1-wox-10.1177_0730888420918643 for General Practitioners Are From Mars, Administrators Are From Venus: The Role of Misaligned Occupational Dispositions in Inhibiting Mandated Role Change by Rene Wiedner, Amit Nigam and Jose Bento da Silva in Work and Occupations
Footnotes
Acknowledgments
We wish to thank Ariel Avgar, Dan Cornfield, and the anonymous reviewers for their valuable comments and guidance. We also thank the participants at the Consequences of Change in Healthcare for Organizations, Workers, and Patients Conference and at the Tenth International Symposium on Process Organization Studies for their insightful feedback and suggestions on earlier versions of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Rene Wiedner was funded by the U.K. National Institute for Health Research Collaborations for Leadership in Applied Health Research and Care Cambridgeshire and Peterborough. The views expressed in this article are solely those of the authors and not necessarily those of the National Health Service in England, the National Institute for Health Research, or the U.K. Government’s Department of Health.
Author Biographies
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.