
Abstract
Introduction
Sexually diverse adolescents report higher suicidality (ideation and attempts) than their heterosexual peers, but information on the onset and course of suicidality from early adolescence to young adulthood among contemporary sexually diverse individuals remains limited. This study traces suicidality trajectories across this critical developmental period, comparing sexually diverse and heterosexual adolescents both overall and by sex assigned at birth.
Methods
Data was drawn from the Quebec Longitudinal Study of Child Development, an ongoing population-based prospective birth cohort. This study included 1,505 participants who self-reported their sexual attraction at ages 15-17 (2013-2015) and past-year suicidal ideation and attempts using 3-items at ages 13, 15, 17 and 23 (2011-2021) from which a suicidality severity score was derived.
Results
11.5% of the sample (n = 173, 60.5% female) reported sexually diverse attraction. Growth curve modelling tested the random effect of sexually diverse (vs. heterosexual) attraction on suicidality severity intercept, linear and quadratic latent growth factors. Age-specific contrasts in suicidality severity between sexually diverse and heterosexual adolescents were also examined. Compared to heterosexual adolescents, sexually diverse adolescents showed a steeper increase in suicidality severity from ages 13 to 17, and declining yet persisting disparities from ages 17 to 23. Although developmental trajectories differed across sexually diverse males and females, both experienced greater suicidality severity during adolescence compared with heterosexual peers.
Discussion
Our findings point to a developmental trajectory in which sexually diverse adolescents, particularly females assigned at birth, experience elevated suicidality that persists into young adulthood. Targeted and timely interventions during this critical developmental period are essential for suicide prevention.
Introduction
Suicidality (i.e., suicide ideation and attempts) among sexually diverse adolescents is a pressing concern. 1 Sexually diverse adolescents represent a heterogeneous group of individuals who experience some degree of non-heterosexual attraction, including those who report attraction to same-sex individuals, to both same- and opposite-sex individuals, or no sexual attraction, among others. 2 Sexual identity formation typically occurs during adolescence and young adulthood, 3 and an increasing number of young people aged 10-24 in Canada are endorsing sexually diverse attraction, with rates of approximately 20% in 2019 compared to approximately 9% in 1998.4–6 Despite increasing recognition and acceptance of sexual diversity since the 1980s, 7 this growing minoritized group remains at heightened risk for suicidality, concurrently reporting 2 to 6 times more likelihood of suicidal ideation and attempts compared to heterosexual individuals,5,8–12 with greater vulnerability among sexually diverse individuals assigned female at birth compared to those assigned male.4,5,13
Developmentally, longitudinal population-based studies in the United States have shown that sexually diverse adolescents—particularly those assigned female at birth—experience higher rates of suicidality in mid-to-late adolescence (around age 16) compared to their heterosexual peers, followed by a decline into adulthood (ages 28-30).14–19 However, these American-based studies relied on data collected from adolescents surveyed in the late 1980s to early 2000s, which may not capture the evolving challenges in youth mental health today. 20 Furthermore, all but one 17 of these studies analyzed data from the National Longitudinal Study of Adolescent Health (Add Health), which employs a broad age range within study waves (12-19 years at baseline 21 ). As a result, these studies do not inform how suicidality emerges and evolves from early adolescence to young adulthood among today's sexually diverse individuals in an increasingly accepting sociopolitical climate in Canada. 7 Documenting trajectories among adolescents and young adults today is crucial for providing timely and targeted interventions.
This study examines suicidality trajectories over a decade—from early adolescence (ages 12/13 in 2011) to young adulthood (ages 22/23 in 2021)—among sexually diverse adolescents, comparing their trajectories to those of heterosexual peers and exploring differences by assigned sex at birth, using data from a contemporary, ongoing population-based cohort in the Canadian province of Quebec.
Method
Participants
Participants were drawn from the Quebec Longitudinal Study of Child Development, a population-based cohort study conducted by the Institut de la statistique du Québec (Quebec Statistics Institute). The cohort initially comprised 2120 babies born between October 1997 and July 1998 in the Canadian province of Quebec, followed annually or biennially to 2021. 22 Participants and their parents were recruited through stratified sampling from birth registries, covering all regions of the province, except for Cree and Inuit territories and Indigenous communities due to differences in institutional services and socio-cultural context. Families with mothers speaking neither French nor English, and babies born extremely pre-term (<24 weeks) or post-term (>42 weeks) were also excluded. The cohort aligned with Quebec's demographics in the late 1990s in terms of socioeconomic composition, race and ethnicity (90% self-identified as White). The cohort protocols were approved by the ethics committees of the Institut de la statistique du Québec, Sainte-Justine Hospital Research Centre, and the Montreal West Island Integrated University Health and Social Services Centre. Informed written consent, assent, or both were obtained at each wave of data collection. This study is reported according to the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines for cohort studies 23 (see Supplemental Table 1 for checklist).
Participants were included in present analyses if they reported their sexual attraction at age 15 and/or 17 (614 participants excluded for missing sexual attraction data) and provided information on suicidal ideation and attempts at least once between ages 13 and 23 (1 additional participant excluded without suicidality data). Thus, the analytic sample included 1,505 individuals (71% retention). Included participants were more likely to be female, White, live in a two-parent household, have higher family socioeconomic status, and have an older mother with fewer depressive symptoms (see Supplemental Table 2
Measures
Suicidality Severity
At ages 13, 15, 17 and 23 (in 2011, 2013, 2015 and 2021, respectively), participants reported their suicidal ideation and attempts in the past year using the following three items: In the past 12 months: (1) did you ever think about suicide (never/rarely/fairly often/very often, recoded as never = no/else = yes); (2) did you ever seriously consider taking your own life or killing yourself (no/yes); and (3) how many times did you attempt suicide (never/once/more than once, recoded as never = no/else = yes). Similarly to other suicidality questionnaires,24,25 a suicidality severity score (i.e., outcome variable) ranging from 0 to 3 was derived from these three items at each age, with scores reflecting the highest level of suicidality endorsed at each assessment. Specifically, a score of 0 represented no suicidal ideation or attempts (i.e., participants responded no on items 1 and 2); a score of 1 represented suicidal ideation considered as non-serious by participants and without suicide attempt (i.e., participants were coded yes on item 1 and no on items 2 and 3); a score of 2 represented suicidal ideation considered as serious by participants, without suicide attempt (i.e., participants were coded yes on items 1 and 2 and no on item 3); and where 3 represented suicidal ideation with at least one suicide attempt (i.e., participants endorsed yes to item 3). Participants were assured confidentiality, which is critical to improve the reliability of self-reports, 26 and were provided with a list of resources should they need assistance.
Sexually Diverse Attraction
At ages 15 and 17 (assessed in 2013 and 2015, respectively), participants reported whether they felt sexual attraction and desire for (1) people of the opposite sex, (2) people of the opposite sex and of the same sex, (3) people of the same sex, or (4) did not have any sexual attraction or desire for either sex. Participants were identified as sexually diverse (i.e., exposure; coded as 1) if they endorsed same-sex, same-and-opposite-sex, or no sexual attraction at either 15 or 17 years old. Participants were identified as heterosexual (i.e., reference; coded as 0) if they endorsed opposite-sex attraction at all available time points.
Sex
Assigned sex at birth was obtained from participant's medical chart and coded assigned-females=1 or assigned-males=0.
Statistical Analyses
Analyses were conducted with Mplus v.8.11 and SPSS v.28.0. Growth curve analyses 27 were used to model suicidality severity trajectories from ages 13 to 23. The Full Information Maximum Likelihood estimation method was used under the assumption that data was missing at random, allowing participants to contribute available suicidality data to analyses despite missingness 28 (see Supplemental Tables 3 and 4 for summary of available suicidality data and early-life predictors of missing suicidality data, respectively). Latent variables representing the intercept (i.e., baseline level of suicidality at age 13), slope (i.e., linear change), and quadratic (i.e., curvilinear or non-linear change) growth factors were specified from suicidality severity scores at ages 13, 15, 17, and 23. Analyses tested the random effect of sexually diverse attraction, dummy coded with heterosexual attraction as the reference group, on the latent intercept, slope, and quadratic growth factors. Analyses were tested both unadjusted and adjusted for sex assigned at birth (see eMethods 1 for justification of covariates). Unadjusted results stratified by assigned-sex were also tested to examine potential differences in trajectories across assigned-males and females. Post-hoc contrasts were computed to examine age-specific estimated mean differences in suicidality severity across groups at each time point. As sensitivity analyses, models were also estimated including participants who provided suicidality data at two or more time points (n = 1,453).
Consultation With Community Partners
Co-authors (RS and MCG) met with two sexually diverse community partners (included as co-authors) for consultation regarding interpretation of results and implications for practice and policy; summary points of this consultation are integrated in the discussion. They also provided feedback on the manuscript.
Results
A total of 173 adolescents, representing 11.5% of the sample, reported sexually diverse attraction, among whom the majority were assigned female at birth (n = 112; 60.5%). The heterosexual attraction group (n = 1,332) had an even sex distribution (47.5%, n = 632 assigned female). See Table 1 for assigned sex distribution across groups.
Assigned Sex Distribution Across Sexual Attraction Groups (Weighted).
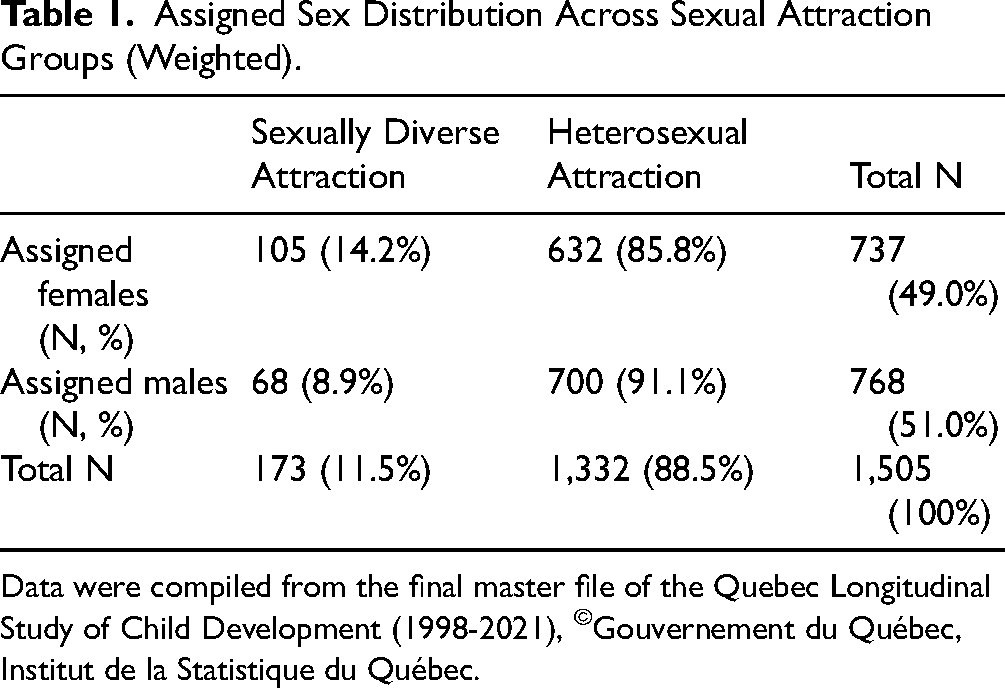
Data were compiled from the final master file of the Quebec Longitudinal Study of Child Development (1998-2021), ©Gouvernement du Québec, Institut de la Statistique du Québec.
Unconditional growth curve modelling estimates of variance related to the intercept (
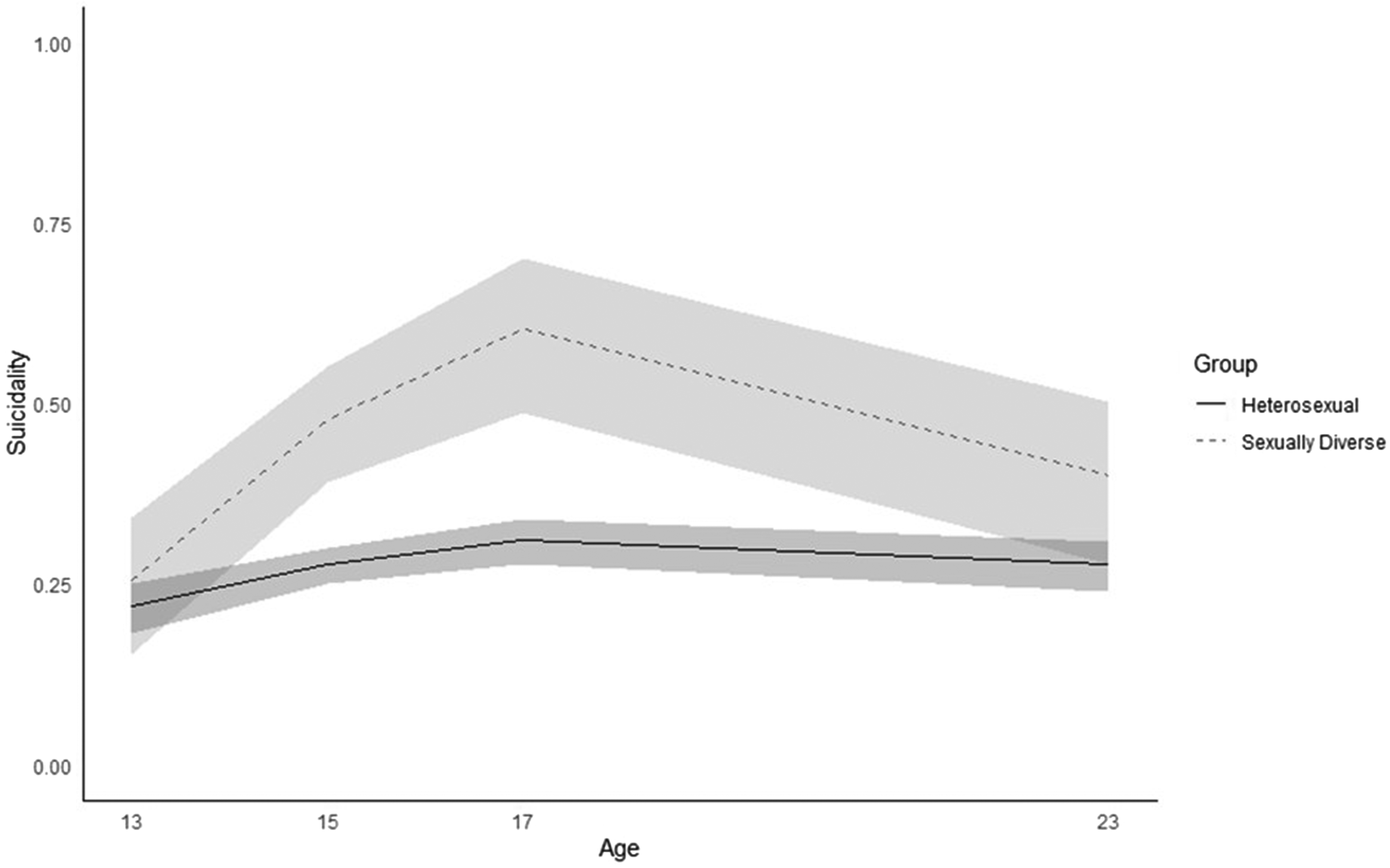
Suicidality trajectories from 13 to 23 years by sexual attraction groups (adjusted for assigned sex).
Growth Curve Modelling Suicidality From 13 to 23 Years of Sexually Diverse (Compared to Heterosexual) Adolescents.
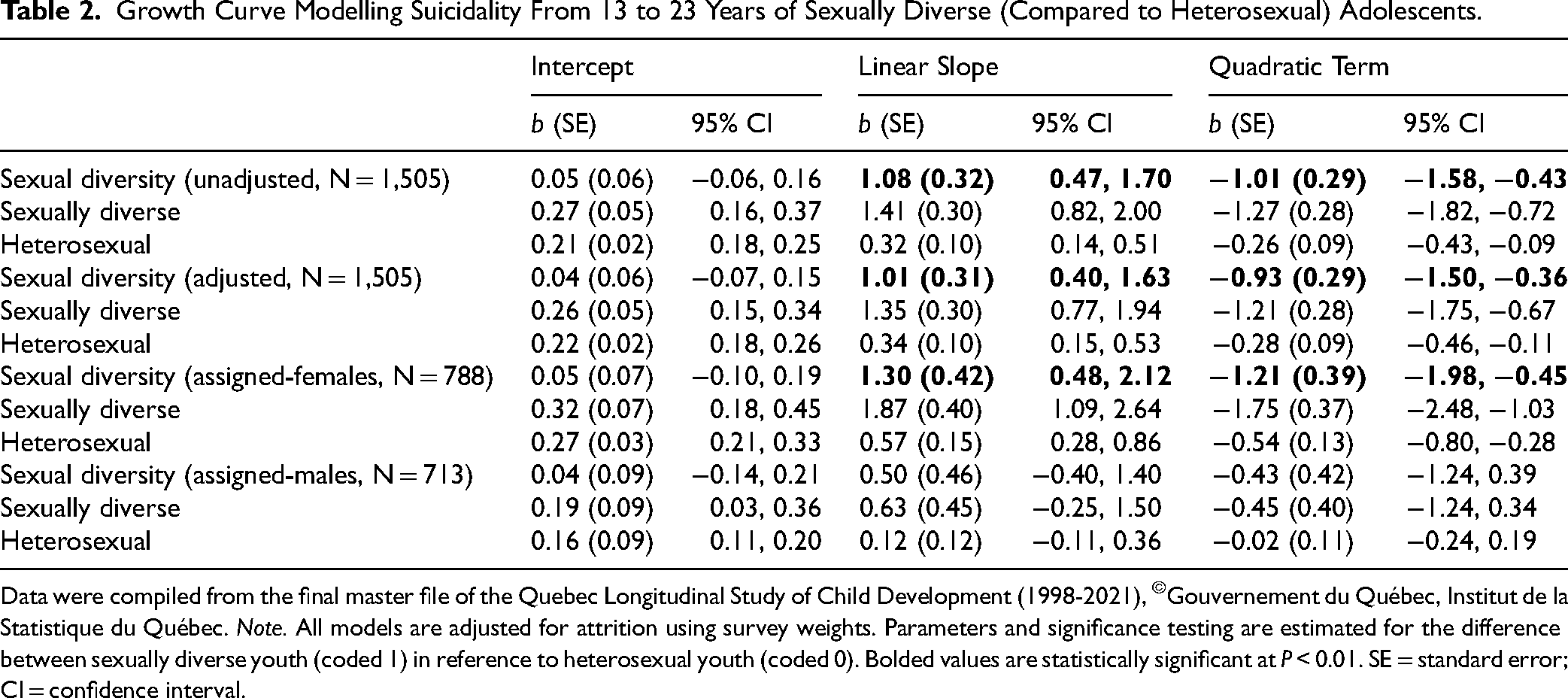
Data were compiled from the final master file of the Quebec Longitudinal Study of Child Development (1998-2021), ©Gouvernement du Québec, Institut de la Statistique du Québec. Note. All models are adjusted for attrition using survey weights. Parameters and significance testing are estimated for the difference between sexually diverse youth (coded 1) in reference to heterosexual youth (coded 0). Bolded values are statistically significant at P < 0.01. SE = standard error; CI = confidence interval.
Assigned sex-differences in suicidality severity trajectories were examined using group stratification, however, model fit indices for stratified results were poor: χ2(10) = 60.11, P < 0.001; χ2/df = 6.01; CFI = 0.73; RMSEA = 0.08. Instead, exploratory analyses were conducted to model suicidality severity trajectories among assigned-males and females separately 29 (Table 2, Figure 2). Among assigned females, fit indices were good: χ2(4) = 8.30, P = 0.08; χ2/df = 2.08; CFI = 0.96; RMSEA = 0.04. Sexually diverse and heterosexual females exhibited significant increases in suicidality severity from ages 13 to 17, followed by greater declines from ages 17 to 23, and this change over time was significantly steeper among sexually diverse assigned-females compared to their heterosexual counterparts. Among assigned males, fit indices suggested no evidence of global misfit: χ2(4) = 0.73, P = 0.95; χ2/df = 0.18; CFI = 1; RMSEA = 0. Neither sexually diverse nor heterosexual assigned-males exhibited significant change in suicidality severity over time, with no differences in trajectories. However, post-hoc estimated mean differences showed that both sexually diverse assigned-males and -females demonstrated greater suicidality severity at ages 15 and 17 compared to their respective heterosexual counterparts. Sensitivity analyses including only participants with two or more suicidality time points (n = 1,453) showed the same pattern of results (data not shown).
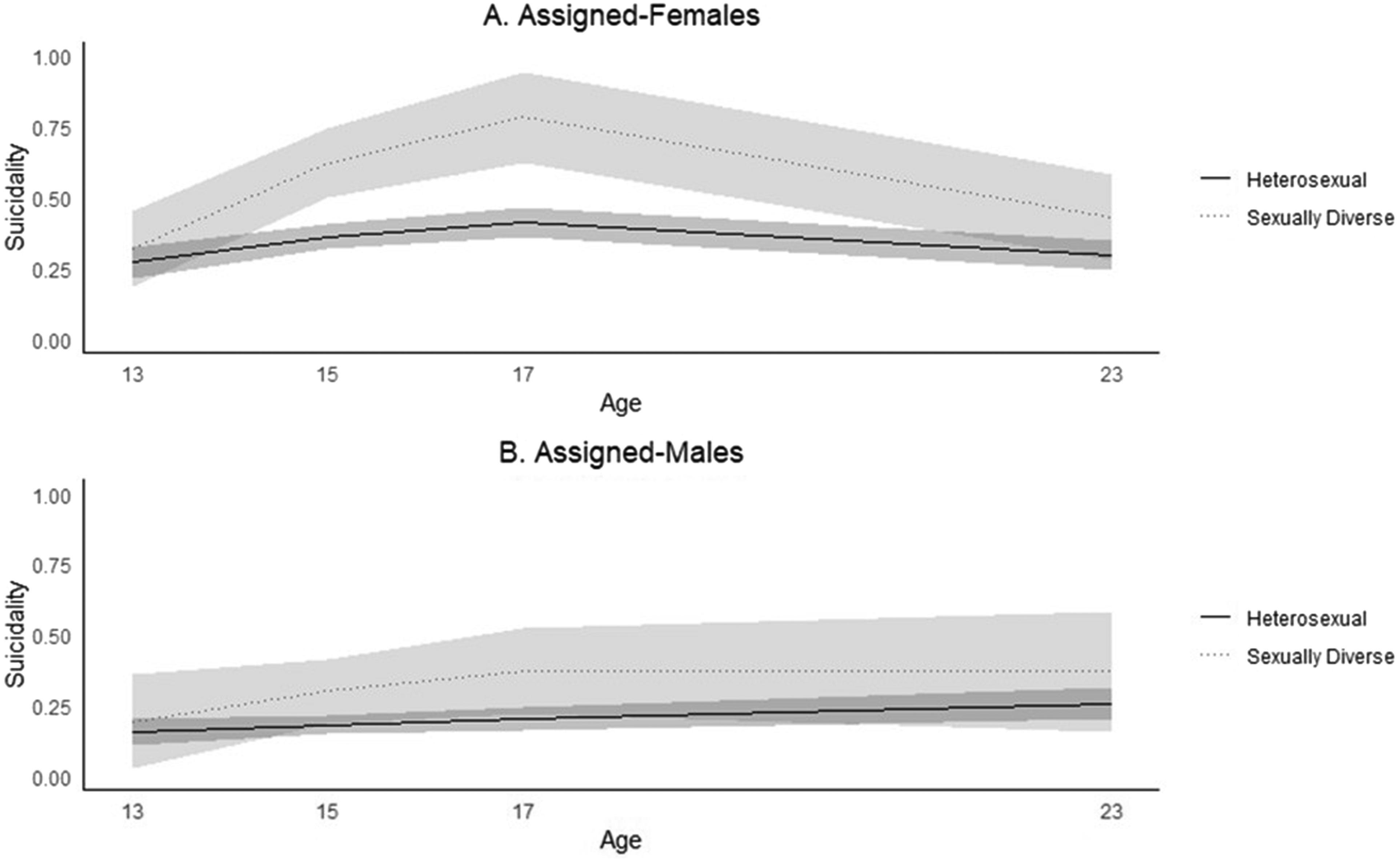
Suicidality trajectories from 13 to 23 years by sexual attraction groups for assigned-females and assigned-males.
Discussion
Within a contemporary population-based birth cohort from the Canadian province of Quebec, sexually diverse adolescents exhibited a trajectory of steeper increase in suicidality severity between ages 13 and 17 compared to their heterosexual peers. Specifically, no group differences in suicidality severity were observed at age 13, but sexually diverse adolescents experienced higher suicidality severity during mid-to-late adolescence (ages 15 and 17). Sexually diverse adolescents also demonstrated a steeper decline in suicidality severity into young adulthood (age 23), though remained at relatively elevated suicidality severity compared to heterosexual peers. This trajectory was also observed among assigned-female adolescents, but was not observed among assigned-males, who experienced stable suicidality severity over time similar to heterosexual males. Nevertheless, both sexually diverse assigned males and females reported greater suicidality severity during mid-adolescence, at ages 15 and 17, compared to their respective heterosexual counterparts.
These findings highlight a critical period from mid-adolescence to young adulthood during which sexually diverse individuals experience heightened suicidality severity. Longitudinal population-based studies among previous generations of adolescents have also identified mid-to-late adolescence, but not early adulthood, as a critical period for heightened suicidality among those identifying as sexually diverse.14–18 Adolescence is marked by significant changes in identity, social networks, cognition, physiology, and sexual identity development,3,30–32 and challenges or obstacles to navigating these developmental demands may contribute to enhanced risk for suicidality in adolescence. 33 Compared to heterosexual adolescents, sexually diverse adolescents must additionally navigate key milestones such as coming-out 3 and coping with minority status and stressors (e.g., risk of stigma, rejection and discrimination) tied to their sexual identity.34,35 Thus, it has been proposed that sexually diverse adolescents may experience a developmental collision whereby they must navigate these minority milestones and stressors concurrently with the typical changes of adolescence, potentially exacerbating mental health difficulties and suicidality during this period, and extending into young adulthood.34–37
Sexually diverse adolescents assigned female at birth exhibited greater increases in suicidality severity throughout adolescence than their heterosexual peers, followed by steeper decreases into adulthood. Among assigned-males, suicidality severity trajectories did not differ between sexually diverse and heterosexual adolescents and were generally stable from adolescence to young adulthood, though the number of sexually diverse males in the sample was relatively small. Nevertheless, age-specific comparisons indicated greater suicidality severity among sexually diverse assigned-male adolescents at ages 15 and 17. These findings align with prior longitudinal population-based studies reporting greater risk of self-reported suicidality16,17 and suicide-related service use 38 among sexually diverse assigned-females than males. Suicidality follows different developmental trajectories depending on sex assigned at birth. Among adolescents assigned female, suicidality tends to peak in mid-to-late adolescence and decline into early adulthood. In contrast, adolescents assigned male typically show a more gradual and linear increase in suicidality from mid adolescence to young adulthood.39–41 These developmental differences may reflect sex-specific timing of puberty and the emergence of distinct risk factors for suicidality. For instance, adolescents assigned female may experience earlier onset of emotional difficulties than assigned males, whereas assigned males may be more likely to exhibit behavioural problems and engage in substance use.13,42 Of note, sexually diverse adolescents assigned female report higher substance use compared to their heterosexual peers, whereas among adolescents assigned male, the difference in substance use between sexually diverse and heterosexual individuals is less pronounced.18,43 Therefore, sexually diverse adolescents assigned female may follow distinct developmental pathways characterized by greater exposure to both internalizing symptoms and substance use, potentially increasing their vulnerability to suicidality, although more research is needed to examine these distinctions.
Canada has shown increasing societal acceptance of sexual diversity since the 1990s and has ranked among the top five most accepting countries globally since 2017.7,44 Similarly, in Quebec, high school students reported growing comfort with lesbian, gay, and bisexual peers from 2001 to 2016, 45 a period coinciding with the high school years of the present sample. Thus, it is possible that sexually diverse adolescents in this sample were exposed to a generally accepting educational and societal environment. Exposure to more positive social climates and accepting attitudes has been associated with earlier age of coming-out,3,37 and better mental health outcomes, including reduced suicidality, among sexually diverse young people.46–49 However, recent concerning evidence suggests that high school students in Quebec have reported declining acceptance and comfort with sexual diversity between 2017 and 2024, 50 reversing prior progress. Similar trends are reported among adults in the United States, where decreasing acceptance has coincided with rising discrimination and worsening self-reported mental health among sexually and gender diverse adults. 51 These shifting societal attitudes underscore the urgent need for sustained and proactive efforts to foster inclusion and acceptance of sexually diverse individuals as a cornerstone of early and targeted suicide prevention strategies. Ongoing efforts to support acceptance of sexually diverse adolescents in schools, 52 and prioritizing organizational and community resources to promote positive development and mental health for sexually diverse young people (e.g., mental health services, supportive community and school resources)46,53,54 are imperative to address suicidality disparities for this group. Moreover, ongoing longitudinal research will be important to document mental health and suicidality among adolescents and young adults today.
Although the use of a contemporary prospective, population-based birth cohort is a strength of this study, almost 30% of the original sample was lost to attrition. Study weights were used to account for selective attrition, yet residual bias may remain. For example, although there is limited evidence that sexually diverse individuals are less likely to participate in health surveys and answer questions about sexual orientation,55–57 some non-responders excluded in the present study may have been reluctant to report or unsure of their sexual preferences 58 and at greater risk for minority stress and suicidality. 59 Thus, future research measuring sexual diversity among adolescents and young adults should consider response options reflecting uncertainty, fluidity, or a broader range of sexual orientation identities to promote inclusion. Likewise, young people experiencing suicidality may have exhibited greater non-response patterns and be under-represented in the current study. 60 Additionally, due to generally low base rates, fine-grained analyses of suicidality trajectories by sexual attraction and in interaction with assigned sex could not be conducted within this cohort. However, past research indicates particularly elevated risk of suicidality among assigned-female young people identifying as bisexual.38,61 Moreover, the current sample is predominantly White (90%), and gender identity was not assessed in adolescence, limiting the examination of intersectional patterns of risk. Given that one in four Canadians today identify with a racialized (non-White) group, 62 and that 8.1% of the sexually and gender diverse (2SLGBTQI+) population in Canada identify as gender nonbinary or transgender, 63 future longitudinal research should explicitly examine how intersecting social identities—including assigned sex, gender identity, sexual orientation, and ethnicity, among others—interact to shape cumulative minority stress experiences and suicidality among sexually diverse young people. Moreover, this study did not examine sexual developmental milestones, minority stressors, or other potential cascading factors that may contribute to these differential suicidality trajectories. However, evidence suggests that disparities in minority stress experiences and mental health problems contribute to heightened suicidality among sexually diverse young people.64,65 Future research should explore these mechanisms to better understand and address their impact.
These findings underscore the need for early, targeted suicide prevention strategies for sexually diverse adolescents and young adults. Promoting acceptance of sexual diversity 52 and expanding school-based, organizational, and community resources (e.g., mental health services, supportive school environments)46,53,54 may foster positive development and help reduce mental health and suicidality disparities in this group.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437261442420 - Supplemental material for Developmental Trajectories of Suicidality in Sexually Diverse and Heterosexual Adolescents: Findings From the Quebec Longitudinal Study of Child Development: Trajectoires développementales de suicidalité chez les adolescents hétérosexuels et de la diversité sexuelle : Résultats de l’Étude longitudinale sur le développement des enfants du Québec
Supplemental material, sj-docx-1-cpa-10.1177_07067437261442420 for Developmental Trajectories of Suicidality in Sexually Diverse and Heterosexual Adolescents: Findings From the Quebec Longitudinal Study of Child Development: Trajectoires développementales de suicidalité chez les adolescents hétérosexuels et de la diversité sexuelle : Résultats de l’Étude longitudinale sur le développement des enfants du Québec by Sasha MacNeil, Roxanne Sicotte, Camille Davisse-Paturet, Elise Chartrand, Em Alexander, Myriam Lecousy, Alain Girard, Massimiliano Orri, Nicholas Chadi, Isabelle Ouellet-Morin, Annie Pullen Sansfaçon, Srividya N. Iyer, Natalie Castellanos-Ryan, Ian Colman, Robert-Paul Juster and Marie-Claude Geoffroy in The Canadian Journal of Psychiatry
Footnotes
Acknowledgements
ChatGPT was used for editing purposes.
Author Contributions
Dr. Sasha MacNeil participated in study conceptualization, data preparation and analysis, writing, reviewing and revision of the manuscript. Drs. Roxanne Sicotte and Camille Davisse-Paturet participated in study conceptualization, data preparation, and critically reviewed and revised the manuscript. Mr. Alain Girard and Ms. Elise Chartrand participated in data preparation and analyses, and critically reviewed and revised the manuscript. Em Alexander, Myriam Lecousy, and Drs. Massimiliano Orri, Nicholas Chadi, Isabelle Ouellet-Morin, Annie Pullen Sansfaçon, Srividya N. Iyer and Natalie Castellanos-Ryan all critically reviewed and revised the manuscript. Dr. Marie-Claude Geoffroy participated in study conceptualization, data acquisition, and critically reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Consent to Participate
Informed written consent, assent, or both were obtained at each wave of data collection.
Data Availability
The data analyzed in this study was obtained from the Institut de la statistique du Québec and, as stipulated in the clauses 10 and 11 of the Institut de la statistique's Québec Act (Canada), the access to the data is restricted to the parties identified in the partnership agreement to ensure the conduct of the study and which describes the author's right. In the QLSCD cohort, the participants only consented to share their data with the study's financial partners and affiliated researchers and their collaborators. Those partners and researchers only have access to the data after signing a data sharing agreement. Requests to access these data can be directed to the Institut de la statistique du Québec's Research Data Access Services - Home (![]() ).
).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The cohort protocols were approved by the ethics committees of the Institut de la statistique du Québec, Sainte-Justine Hospital Research Centre, and the Montreal West Island Integrated University Health and Social Services Centre.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Quebec Longitudinal Study of Child Development was supported by funding from the Ministère de la Santé et des Services sociaux, Ministère de la Famille, Ministère de l’Éducation and Ministère de l’Enseignement supérieur (Québec ministries), the Lucie and André Chagnon Foundation, the Institut de recherche Robert-Sauvé en santé et en sécurité du travail, the Research Centre of the Sainte-Justine University Hospital, the Ministère de l’Emploi et de la Solidarité sociale, and the Institut de la statistique du Québec. Additional funding was received by the Fonds de Recherche du Québec - Santé (FRQS), the Fonds de Recherche du Québec - Société et Culture (FRQSC), the Social Science and Humanities Research Council of Canada (SSHRC), the Canadian Institutes of Health Research (CIHR). The funders had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; or decision to submit the manuscript for publication. Professors Orri, Ouellet-Morin, Iyer and Geoffroy reported holding a Canada Research Chair.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.