
Abstract

People living with concurrent disorders are in urgent need of integrated healthcare research and investment, yet mental health and substance use health (MHSUH) systems and services remain deeply fragmented.1–9 In Canada, concurrent disorders are defined as the simultaneous presence of both a substance use disorder (SUD) and non-SUD mental disorder. These inherently heterogeneous clinical permutations are associated with greater risk of morbidity, premature mortality, socioeconomic inequities, heightened involvement in the criminal justice system, poorer treatment outcomes, and recurring harms associated with substance use than individuals with a single disorder.10–12 Moreover, the presence of a SUD or other mental disorder increases the likelihood of developing the other,10,11 with especially high prevalence of co-occurrence reported in treatment settings.12–15 Although concurrent disorders are the norm rather than the exception, the Canadian health system is not designed to serve this population, as it has historically separated MHSUH training and service delivery. Care providers are typically trained to specialize in either mental or substance use health,1,2 while responsibility for coordination and funding of these services varies among provincial and territorial ministries.1,3,4 Fragmentation between MHSUH services creates serious gaps in care for people with concurrent disorders by complicating system navigation and reducing service coordination, treatment efficacy, and continuity of care, ultimately leading to poor treatment outcomes, if care is received at all. For decades now, Canada has recognized the critical role of integrated care in bridging these gaps and improving health outcomes.1–9 In contrast to the progress in developing integrated models for the treatment of cancer, 16 MHSUH systems and services across Canada remain disjointed.5–9
Advancing integrated care for concurrent disorders requires multidisciplinary, national research to identify systemic barriers and facilitators to integration,1,5–9 though it is difficult to achieve progress in this area when research in Canada is just as siloed as our healthcare services and systems. As long as MH and SUH researchers continue to operate in isolation from each other and from other health system partners, there are limited opportunities to discern what is required to advance integrated care nationally. Novel mechanisms are thus needed to facilitate collaboration between the many sectors involved in understanding the complex needs of concurrent disorder populations and co-develop a national research agenda for care integration. Although research workshops, conferences, and similar events bring researchers and clinicians together to share knowledge related to concurrent disorders, they frequently neglect to include people with lived and living experience (PWLLE) from these conversations, though they are essential to creating a responsive and inclusive health system.17–19 Integrated, multidisciplinary research cannot wait any longer; action must be taken now to connect the research, healthcare, policy, and PWLLE sectors and identify national research priorities to advance integrated care, so that people with concurrent disorders can ultimately receive the healthcare that they need.
To bridge sectors together and identify research priorities for integrated care of concurrent disorders, we held a 1-day, in-person Concurrent Disorders Think Tank in December 2024. Through this event, we engaged 45 researchers, clinicians, PWLLE, policy makers, and organizational health partners representing not only MHSUH but also physical health and public health. A list of expert roles and geographic jurisdictions of participants is provided in Table 1. The event consisted of morning and afternoon panels on integrated care models and treatment modalities for concurrent disorders, respectively, followed by facilitated small group discussions. During group discussions, participants documented and shared their feedback and ideas for research, which were analysed by co-authors JL and RS using an inductive coding approach to identify key priority themes. Here, we share the five key priority areas that were most frequently identified by participants and suggest they help to inform the development of a high-level collaborative research agenda on integrated care for concurrent disorders in Canada.
List of Expert Roles and Geographic Jurisdictions of Think Tank Participants.
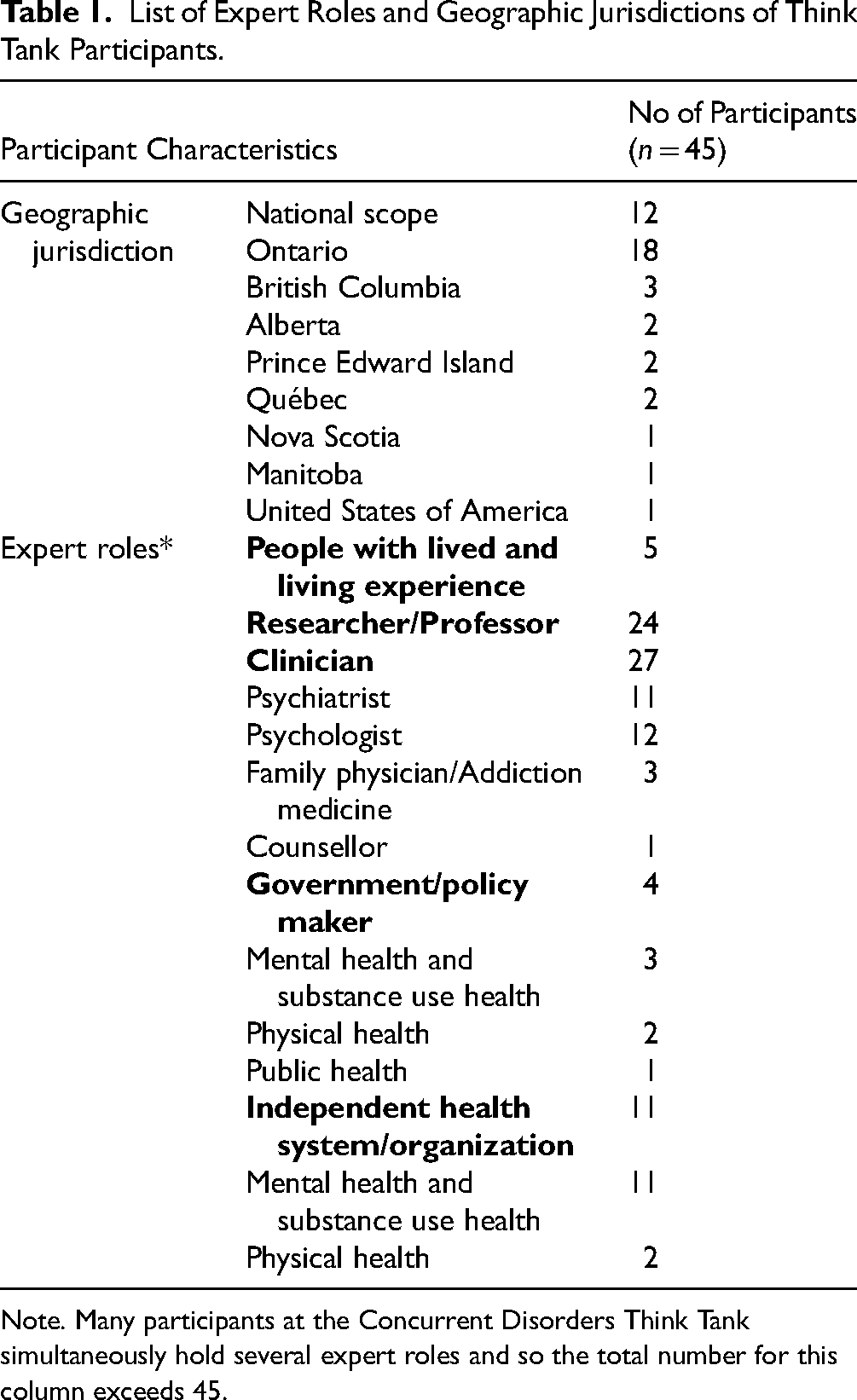
Note. Many participants at the Concurrent Disorders Think Tank simultaneously hold several expert roles and so the total number for this column exceeds 45.
Priority Area #1: Treatment Guidelines
Participants emphasized the need for research to inform concurrent disorders treatment guidelines that can be embedded within integrated care models, along with evidence-based recommendations for delivering new and emerging therapies. Developing treatment guidelines requires an iterative, stratified approach to address the numerous subtypes of concurrent disorder populations with distinct aetiologies, symptom profiles, and individual and cultural treatment preferences, each of which shapes care planning and treatment outcomes.1,3,5 Compiling evidence on interventions and providing recommendations that account for clinical and sociodemographic subgroups would be highly beneficial to clinicians and patients by reducing the need for extensive trial-and-error in treatment planning. Efforts to develop and maintain these guidelines should also include research on new and emerging treatment modalities, which may serve as adjunct or alternative therapies for individuals who did not respond to standard treatments. Overall, significant investment is needed to support the research that is vital to compiling and generating the evidence that is required for developing and maintaining treatment guidelines and standards, which are in turn essential for delivering integrated care to people with concurrent disorders.
Priority Area #2: Measurement-Based Care
Reliable, validated tools to measure patient health status are critical to the delivery of integrated care for concurrent disorders but their use across the Canadian healthcare system remains inconsistent. Measurement-based care (MBC) systems – built upon psychometrically rigorous tools to measure concurrent symptoms and other health indices – offer a strong framework that can leverage routinely collected health data to inform evidence-based treatment planning, research and policy evaluation. 20 While MBC is broadly associated with improvements in patient health outcomes and care satisfaction, 20 variations in selected measures and implementation can influence its effectiveness, feasibility and wide-scale adoption. To ensure that MBC provides consistent results across integrated care settings for concurrent disorders, multi-site research studies are needed to elucidate the core elements of MBC models and effective implementation strategies in these settings. These efforts must include dedicated equity-based analyses as a central research component, as instrument selection and clinical severity thresholds can vary significantly based on individual and cultural identities. Through multidisciplinary national research studies, strategies can subsequently be developed to address existing questions and concerns about implementing MBC, such as consensus on key measurement domains, flexibility in instrument selection, establishing data systems and governance policies, and integrating measurement into treatment planning and discharge processes. Investing in MBC implementation research across integrated care settings is vital to supporting people with concurrent disorders, as without consistent and appropriate measurement, we cannot know whether our efforts to improve healthcare outcomes are working.
Priority Area #3: Learning Health Systems
As with other fields of healthcare, 18 there is a substantial delay between generating research evidence on best practices for MHSUH treatment and applying results in practice, although this can be mitigated through investments in knowledge exchange and health system partnerships. The gap between research and practice often stems from fragmentation among healthcare users, clinicians, researchers, and policy makers.17,18 This gap is especially pronounced for concurrent disorders, as MHSUH organizations across Canada often operate in siloes and lack standard mechanisms to share information across institutions.4,8 One solution to bridge the divides between research and clinical practice is to implement a learning health systems (LHS) model within and across healthcare organizations, which provides an effective framework to accelerate knowledge exchange by embedding research and evaluation activities directly into everyday healthcare practice. 18 To advance LHS models, studies are required to identify the core components of these models within integrated care settings, develop strategies to adapt the framework to different geographic and cultural contexts, and determine the most effective methods for scaling LHS models across the Canadian health system. Beyond the healthcare organizational level, dedicated resources are needed to support the formation and maintenance of broader health system partnerships. Examples include national and local communities of practice, research networks, and government advisory committees, similar to those formed to promote integrated cancer care in Ontario. 16 Without adequate funding and incentives to support knowledge exchange, evidence-based practice cannot be realized in a timely manner and integrated care for concurrent disorders will consequently continue to crawl – rather than leap – forward.
Priority Area #4: Service Structure and Delivery
Given the growing evidence that integrated care improves outcomes for people with concurrent disorders,4–9 a critical research priority is to identify the level of service integration that achieves the optimal balance between clinical effectiveness and resource efficiency. 7 Equally important is understanding how these models can be tailored to reflect patients’ needs and preferences. Integration between MH and SUH services is possible at various levels – each with their own direct and indirect costs – and so implementation decisions must be guided by research evidence and feasibility. For instance, do individuals with concurrent disorders experience substantially different health outcomes and care satisfaction when a) mental and substance use health services are coordinated between different providers from separate organizations, b) services are coordinated between different providers who are located within the same organization or, c) when a single transdiagnostic intervention is delivered by one care provider? The level of care integration required to improve healthcare outcomes may depend on patients’ care needs and preferences, introducing additional complexity to consider. However, by applying a person-centred care framework, we can better understand how varying levels of care integration affect different patient-reported outcome measures, such as the effects of the therapeutic alliance and shared decision-making on changes to substance use health outcomes. 21 To provide guidance on selecting levels of care integration at the organizational level, we require investments in multi-site research and evaluation studies that align with person-centred care frameworks, which will enable comparisons of meaningful health outcomes across organizations that have implemented different integrated care models.
Priority Area #5: Co-Design
Engaging PWLLE as co-leaders in planning treatment programs, research agendas, and health policies is essential to ensure these efforts are comprehensive, engaging, and truly reflect the needs of the population being served. 19 While the Canadian health system is beginning to recognize the value of co-design, there are several barriers that health services and systems need to overcome to ensure that PWLLE have a variety of engagement opportunities that match their level of interest and capacity to contribute, and that they are appropriately supported, acknowledged, and compensated within their roles. 19 For instance, some individuals may prefer a relatively low level of participation in a survey or focus group, while others may want to participate as full members of the working team. Offering a spectrum of engagement opportunities ensures a comprehensive co-design approach and avoids tokenistic representation of PWLLE expertise, 19 because a ‘one-size-fits-all’ approach does not work.19,22 When assembling working teams, a true co-design approach also requires consideration of PWLLE team members’ individual skills and interests beyond their personal experience, 19 such as co-leading strategic planning, data analysis, knowledge mobilization, or other activities relevant to the work. Participants recognized that integrated care cannot proceed without adopting a co-design approach and that guidelines for appropriate and effective engagement strategies are required to accelerate this process across the Canadian health system. Thus, compiling existing best practices for engagement and supporting PWLLE advocates to lead implementation guidelines for co-design methods relevant to concurrent disorders treatment, research, and policy are immediate priorities, as these methods are applicable to all work conducted within a larger national research agenda.
A Call for Collaborative Research Across Five Priority Areas
Canadians cannot wait any longer; we need major system transformation to improve care delivery for people with concurrent disorders. 23 Applied research can help us identify existing gaps and solutions to address them; however, many of our current research efforts are just as siloed, disjointed and underfunded as the services they are meant to improve. Without mechanisms to share knowledge at the national level, research is too often duplicated or stalled past local implementation, ultimately wasting resources and hindering health system reformation. To facilitate a nationally coordinated approach to concurrent disorders healthcare, we urgently need to identify priorities underlying a collaborative research agenda that brings together the diverse perspectives of PWLLE, clinicians, researchers, policy makers, health system partners, and funders.
To support the priorities identified at this initial event and the subsequent development of a research agenda, we call on health system leaders and funders to make concurrent disorders research a priority, reduce siloes between MHSUH health care through targeted funding calls to support care integration and related training and education programs, offer parity of funding aligned with other serious health conditions, and invest in the following areas related to integrated care research for concurrent disorders:
Multi-site research groups to support the development and maintenance of treatment standards and guidelines for concurrent disorders. National research networks to create and advance implementation guidelines for MBC models in integrated care settings. Promote LHS models in healthcare settings and provide support for national and local partnerships with an explicit focus on knowledge exchange. Establish the optimal level of care integration for concurrent disorders treatment settings. Build infrastructure to enable co-design methods at all levels of the health system and offer resources on implementation and compensation for a variety of PWLLE engagement opportunities.
Given that resources and personnel capacity for research are not infinite, we believe that we can make the most efficient use of current resources by directing our attention to the five areas outlined above. Research in these areas will in turn drive the clinical service and system-level changes that are needed to fully realize these priorities, similar to how integrated care approaches to treating cancer have evolved over the previous decade in Canada. 16 However, these research efforts cannot be undertaken in isolation or without investments into the training and education programs needed to support successful implementation. During the Think Tank, participants shared provincial and national research initiatives that can be leveraged to address the gaps outlined in the key priority areas, allowing for a nationally coordinated approach that reduces the need for new pilot projects and accelerates adoption of practices that already have an evidence-base.
This Think Tank is just the first step in convening these experts and while the group represented several provinces from across the country, there was a higher concentration of experts located in Ontario. To engage more representatives from other provinces and territories, our next step is to hold a virtual meeting that can accommodate more participants, with a larger proportion of experts invited from outside of Ontario. At this meeting, we will begin to operationalize the priorities outlined here and determine strategies for moving them forward. As part of this larger effort, we recognize the 22nd Call to Action from the Truth and Reconciliation Commission of Canada, 24 which states that health system leaders must value Indigenous healing practices and support Indigenous healers and Elders to apply these practices in their communities. While one of our co-authors is an expert in Indigenous health, we recognize that perspectives of the many Indigenous and First Nations communities across Canada were not represented at the Think Tank and that to honour this call to action, we must develop strategies to engage more Indigenous community leaders, as well health advocates from other traditionally equity-denied groups, and illuminate how the Think Tank initiative may be adapted or leveraged to support leaders in advocating for the health of their communities.
Overall, the Concurrent Disorders Think Tank revealed that a collaborative and coordinated approach to health system reformation for concurrent disorders is not only needed but is possible, and the time to accomplish this is now.
Footnotes
Acknowledgements
We acknowledge the time and contributions of all those who participated in the Concurrent Disorders Think Tank; their input provided the basis for generating research themes and collaborative research priorities for concurrent disorders. We also thank Amy Estill from Collective Results for her role in planning and facilitating the event. Finally, we acknowledge the following HRI staff members involved in planning, organizing, and/or executing the event: Michelle Lawrence, Heather Froome, Kaili Hilkewich, and Rebecca Weston.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. SK has been a consultant for Boehringer-Ingelheim, Indivior Janssen, Lundbeck, and Otsuka. JM is a principal and senior scientist in Beam Diagnostics, Inc. No other authors have any conflicts of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for knowledge dissemination of the Concurrent Disorders Think Tank was provided by the Canadian Institutes for Health Research - Institute of Neurosciences, Mental Health and Addiction (INMHA) Planning and Dissemination Grant (FR# 197251). Financial support for the planning, implementation, and knowledge dissemination of the Concurrent Disorders Think Tank was provided by Cowan and Balsam Foundation. JM is supported by the Peter Boris Chair in Addictions Research and a Canada Research Chair in Translational Addiction Research (CRC-2020-00170).