
Abstract
Background
Mental health concerns are common among undergraduates and have been linked to lifestyle factors. This study examined the relationship between recreational screen time at university entry and mental health over the academic year, and the potential moderating role of self-esteem.
Methods
Data from the longitudinal Queen's U-Flourish Survey (2021/2022) included measures of screen time unrelated to academic work (leisure and social) and validated screening measures for anxiety (GAD-7), depression (PHQ-9), insomnia (SCI-8), disordered eating (SCOFF), and low well-being (SWEMWBS). Multivariable log-binomial regression was used to examine associations between screen time and mental health.
Results
At entry to university, a higher proportion of males (n = 394) than females (n = 1,135) reported averaging 4 + hours/day of leisure screen time (57.4% vs. 45.3%, P < 0.001), while a greater proportion of females reported 4 + hours of social screen time (32.2% vs. 25.2%, P = 0.01). Higher screen time was associated with increased risk of clinically significant levels of symptoms and reduced well-being at school entry, with greater effects for leisure compared to social screen time. Students reporting 7–9 and 10 + hours/day of leisure screen time were more likely to screen positive for anxiety (by 20% and 39%), depression (39%; 47%), insomnia (22%; 55%), and low well-being (45%; 68%) compared to students averaging ≤3 hours/day. Effects were comparable between males and females, except greater leisure screen time was associated with increased risk of disordered eating among females only. Associations between screen time and screening positive at the end of the academic year were largely attenuated. Leisure screen time ≥3 hours/day was most strongly associated with anxiety and depression among students with higher self-esteem.
Conclusions
Recreational screen time ≥3 hours/day is common among first-year undergraduates and associated with higher levels of anxiety and depressive symptoms and lower well-being. It should be considered in campus mental health promotion and prevention efforts.
Introduction
The transition to university is often a challenging time for young people, as they take on greater responsibility for managing their time, health, finances, and relationships while meeting the demands of higher education.1,2 Mental health concerns are common among undergraduates, with approximately one-third to one-half screening positive for anxiety and depression.3,4 The COVID-19 pandemic, marked by social restrictions and campus closures, exacerbated these problems among Canadian university students.4–7 Mental health challenges are, in turn, associated with academic difficulties such as school drop-out and lower GPA, as well as reduced quality of life8–10 and substance abuse. 11
Recreational screen time, which encompasses screen use unrelated to work or school, has averaged above 4 hours/day among undergraduates since the resolution of the COVID-19 pandemic.12,13 While screen time was already increasing, 14 pandemic-related restrictions necessitated increases in screen time for entertainment and socialization. During this period, averages reached as high as 7 hours/day in undergraduates 15 and have remained elevated compared to pre-pandemic levels. 16 Higher daily screen time has been correlated with lower quality of life and well-being, heightened stress, and increased symptoms of depression, anxiety, and insomnia among young adults.12,15,17–22 Specifically, exceeding 3 hours/day of recreational screen time has been associated with increased depression and anxiety, and in some studies females appear more vulnerable. 19 Other negative impacts include decreased physical activity/recreation, negative social comparison, reduced face-to-face connection, and increased risk of cyberbullying.23–25 While most studies have found negative associations between prolonged screen time and mental health, some report no impact or positive effects.19,24,26 Moderate screen use has been associated with better mental health, including higher self-esteem, resilience, and well-being. 24 Longitudinal studies indicate that frequent social media use and leisure screen time can predict future mental health problems, but effects are generally small. 24
While previous studies have largely focused on total recreational screen time and mental health it appears not all screen use is comparable.24,26–28 Unlike leisure screen time, social screen time involves active communication with others through video calling, texting, or messaging. While high levels of leisure screen time are largely seen as detrimental,19,24,26,27 moderate amounts of social screen time may be beneficial, allowing students to remain connected and feel supported. 29 The nature and strength of associations between screen time and mental health appear to depend on the type of screen activity, duration of use, and individual factors such as gender and self-esteem. 24
Few previous large-scale, longitudinal studies have examined recreational screen time and mental health in university students; few have considered differences by gender, and none to our knowledge have explored the moderating role of self-esteem. Examining these associations in first-year undergraduates is especially important, as they have less parental oversight and require more self-direction in screen time use. Further, they are often distanced from family and established friends and rely more on screens for academic commitments. For these reasons, university students may be particularly vulnerable to high levels of screen time use. Recreational screen time is often cited as a modifiable risk factor to address the risking rates of mental health concerns among university students, but its impact remains debated, requiring further investigation.
Utilizing longitudinal data from first-year undergraduates who began their studies after the peak of the COVID-19 pandemic (2021–2022 academic year), we examined associations between recreational screen time (leisure and social) at entry to university and mental health and well-being reported at the beginning and completion of the academic year, considering differences by gender. We also explored whether self-esteem influenced the associations between screen time and anxiety and depression. As a key psychological resource, self-esteem may affect recreational screen use and its impact on mental health, 30 thereby guiding interventions targeting at-risk students.
Methods
Data Source
Study data were from the biannual U-Flourish Student Well-Being Survey study, the protocol of which is previously published. 31 Briefly, since 2018, incoming first year students to Queen's University, Canada have been invited to complete an online survey in mid-September and again in mid-March, and biannually each year thereafter. The baseline survey collects data on students’ sociodemographic characteristics, daily behaviours, and mental and physical health. The U-Flourish student-led engagement team deploy a multifaceted strategy (e.g., booths on campus and at events, classroom talks, posters, and social media posts) to increase student participation.
This study included first-year students who completed a baseline survey in Fall 2021, after classes resumed in-person post COVID-19 pandemic, and some restrictions remained (e.g., mandatory masking and self-screening). The baseline survey, completed 2–3 weeks into the term, when students had settled into a routine, included supplemental items on daily social and leisure screen time. The fall baseline survey had a 34% response rate, and 41% of those respondents completed the spring follow-up. After reading a Letter of Information, students provided informed consent electronically and were given access to the survey hosted on Qualtrics. The U-Flourish Survey was reviewed for ethical compliance by the Queen's University Research Ethics Board (HSREB PSIY-609-18).
Study Variables
Exposure to Recreational Screen Time at School Entry
Leisure screen time was defined as time spent passively watching television or videos, or using an application or game, while social screen time was defined as time engaged in actively communicating with others through screens (e.g., FaceTime, text messaging), unrelated to academic studies. Average daily hours of each type of screen activity were reported using the following options: ≤3 hours, 4–6, 7–9, 10–12, and 13 + hours/day. Due to small cell sizes, the upper categories were collapsed into 10 + hours/day for leisure screen time and 7 + hours/day for social screen time.
Mental Health and Well-Being Outcomes at School Entry and Completion of the Academic Year
Symptoms of anxiety and depression over the past two weeks were measured using the 7-item Generalized Anxiety Disorder scale (GAD-7) 32 and 9-item Patient Health Questionnaire (PHQ-9), 33 respectively. On both scales a cut-off score of ≥10 indicates clinically significant symptoms.32,33 The eight-item Sleep Condition Indicator (SCI-8) measures past-month sleep quality, with scores of ≤16 indicating probable insomnia. 33 Well-being was assessed using the 7-item Warwick-Edinburgh Mental Wellbeing Scale (SWEMWBS), with a cut-off of ≤19 used to indicate low well-being. 34 Finally, the five-item SCOFF questionnaire was used to identify disordered eating behaviour. 35 Bulimia nervosa and anorexia symptoms are assessed with ≥2 “Yes” responses indicating disordered eating.
Demographic Characteristics
Age in years was self-reported at school entry. Gender was self-identified by selecting from the following: male, female, non-binary, prefer not to say, as well as an option to self-describe their gender identity. International student status was self-reported. Participants reported their ethnicity based on a standard set of options which were collapsed into the following categories: White, Asian, Black, Other, and Multiple. 36 Program of study was obtained by linking to the University administrative database.
Self-Esteem at School Entry (Effect Modifier)
Self-esteem was measured using the 10-item Rosenberg Self-Esteem Scale, 37 and categorized using approximate tertiles into low (0–14), moderate (15–19), or high (20–30).
Statistical Analysis
Analyses were conducted using SAS Version 9.4 (SAS Institute Inc., Cary, NC, USA). The sample was limited to students with complete data on age, gender, the screen time measures, and at least one mental health outcome, resulting in 1,562 of 1,943 students (80%) being retained for analysis. Analyses examining mental health outcomes at the end of the year included 678 students (43%). Recreational screen time and mental health concerns reported at baseline were not significantly different in those lost to follow-up compared to those who completed it (ꭓ2 P > 0.05).
Descriptive statistics were used to summarize the sample, average daily screen time, and the mental health outcomes. Spearman's correlation coefficient was used to assess the relationship between leisure and social screen time. 38 Multivariable log-binomial regression was employed to examine the relative risk (RR) of screening positive for a mental health concern based on students’ screen time, adjusting for age and gender (if not stratified by gender). The first series of log-binomial regression models examined associations between screen time and mental health outcomes reported at school entry. Potential effect modification by gender (male vs. female) was tested using interaction terms. Where significant gender differences were indicated (P < 0.15), the stratified results were presented.
A second series of log-binomial regression models examined associations between screen time at school entry and mental health outcomes at year-end, adjusting for baseline outcome status to assess whether screen time was associated with emergent mental health problems. The upper categories of leisure screen time were further collapsed into 7 + hours/day for these analyses due to small cell sizes. The regression analyses had 80% power (two-sided α=0.05) to detect RRs of 1.16–1.60 overall, with gender-stratified minimum detectable RRs of 1.68–2.06 (males) and 1.27–1.57 (females) for cross-sectional analyses, and 2.00–2.83 (males) and 1.34–1.71 (females) for the fully adjusted longitudinal models.
Effect modification by self-esteem of the associations between screen time and screening positive for anxiety and depression at university entry was explored by stratifying the models by levels of self-esteem.
Results
Description of the Sample
Most participants (n = 1,562) were 18 years old at school entry, identified as female, and either White (62%) or Asian (20%) ethnicity (Table 1). At university entry, the most common mental health screen-positives were for anxiety (45%) and depression (42%), followed by disordered eating (31%), probable insomnia (30%), and low well-being (28%) (Supplemental Table 1). Females more commonly screened positive than males (ꭓ2 P < 0.001), with the greatest differences observed for disordered eating (36% vs. 15%, ꭓ2 P < 0.001) and anxiety (50% vs. 29%, ꭓ2 P < 0.001). At school entry, average self-esteem was 17.1 out of 30 (SD = 5.7).
Description of the Study Sample (n = 1,562).
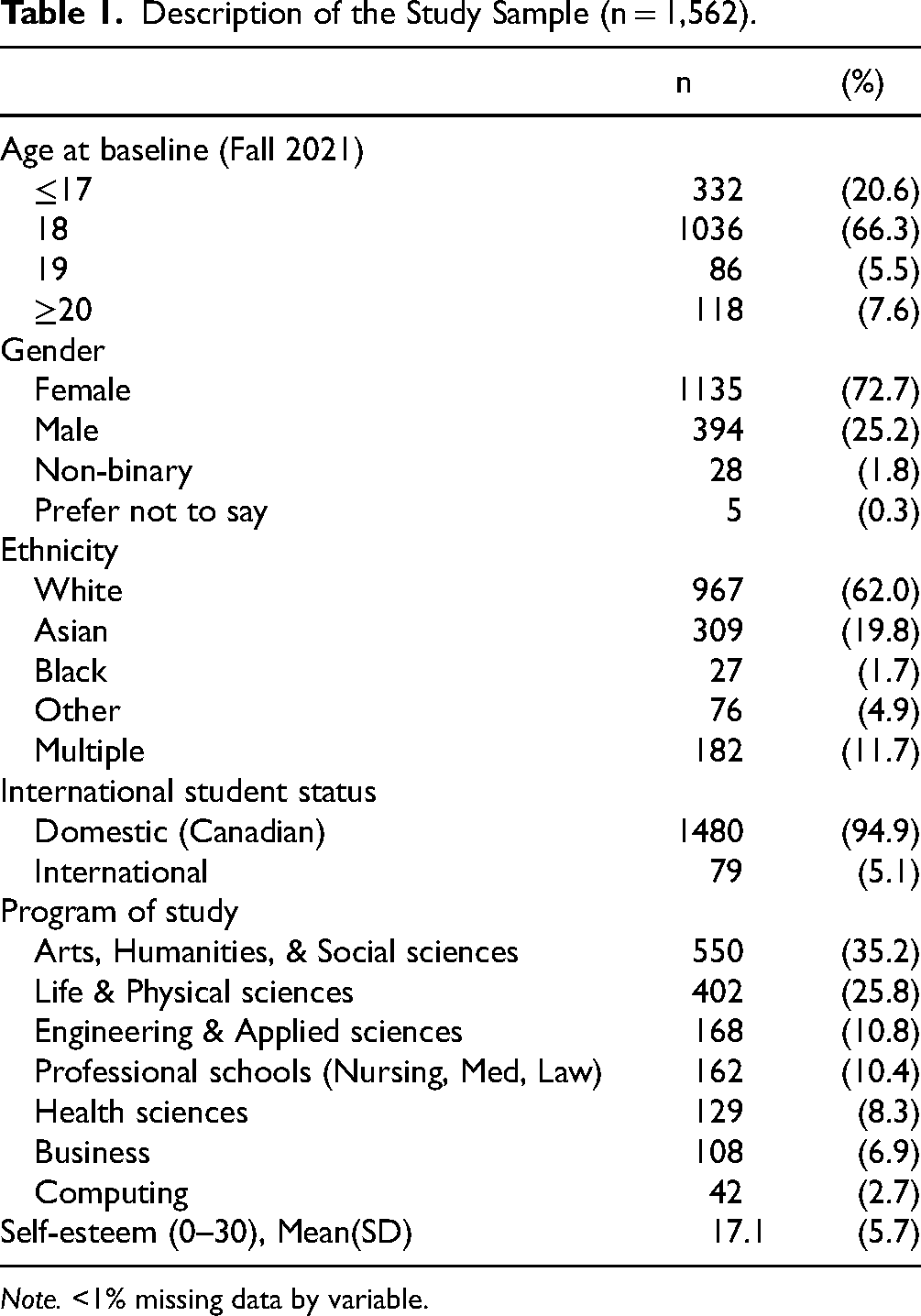
Note. <1% missing data by variable.
Recreational Screen Time at University Entry
Figure 1 illustrates leisure and social screen time reported at university entry, stratified by gender. For leisure screen time, a higher percentage of males than females reported averaging 4 + hours/day (57.4% vs. 45.3%, ꭓ2 P < 0.001), while for social screen time, a greater percentage of females reported 4 + hours/day (32.2% vs. 25.2%, ꭓ2 P = 0.01). In total, 15.5% and 5.6% of students reported averaging 7 + hours/day of leisure and social screen time, respectively. There was a weak correlation between leisure and social screen time (Spearman's rho = 0.22; 0.18 in males, 0.23 in females).
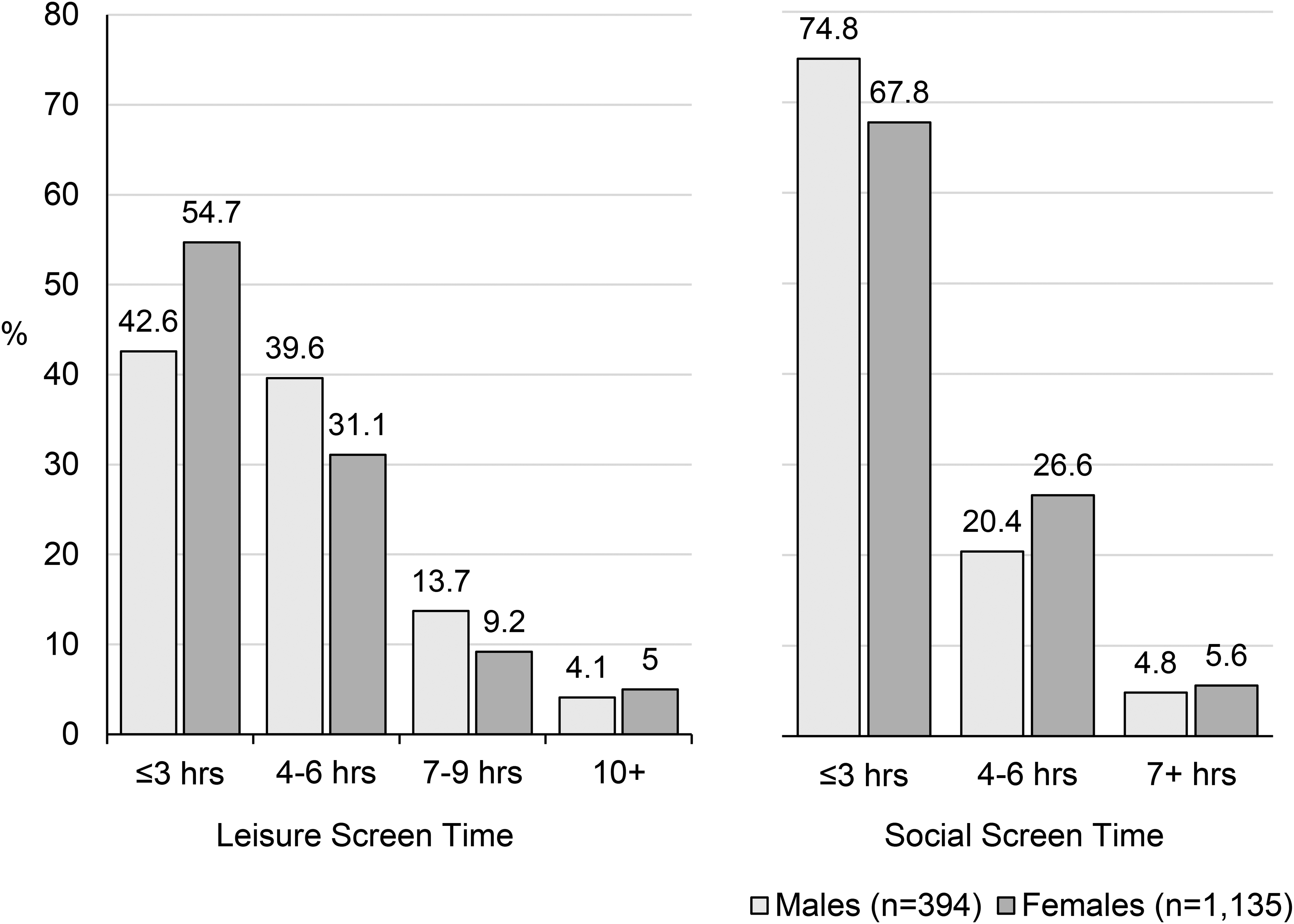
Average daily hours of leisure and social screen time reported by first-year undergraduates at school entry, by gender.
Associations Between Screen Time at University Entry and Mental Health at Entry and Completion of First Year
At school entry, longer duration of daily screen time was associated with a greater likelihood of screening positive for common mental health problems, with stronger effects observed for leisure compared to social screen time (Table 2). Students reporting 7–9 and 10 + hours/day of leisure screen time were 20–45% and 39–68% more likely to screen positive for anxiety, depression, insomnia, or low well-being than those averaging ≤3 hours/day (Table 2).
Multivariable Log-Binomial Regression Results Examining Associations Between Average Daily Recreational Screen Time (Leisure and Social) at Entry to University and Screening Positive for Common Mental Health Problems at School Entry (Fall 2021) and the End of the Academic Year (Spring 2022).
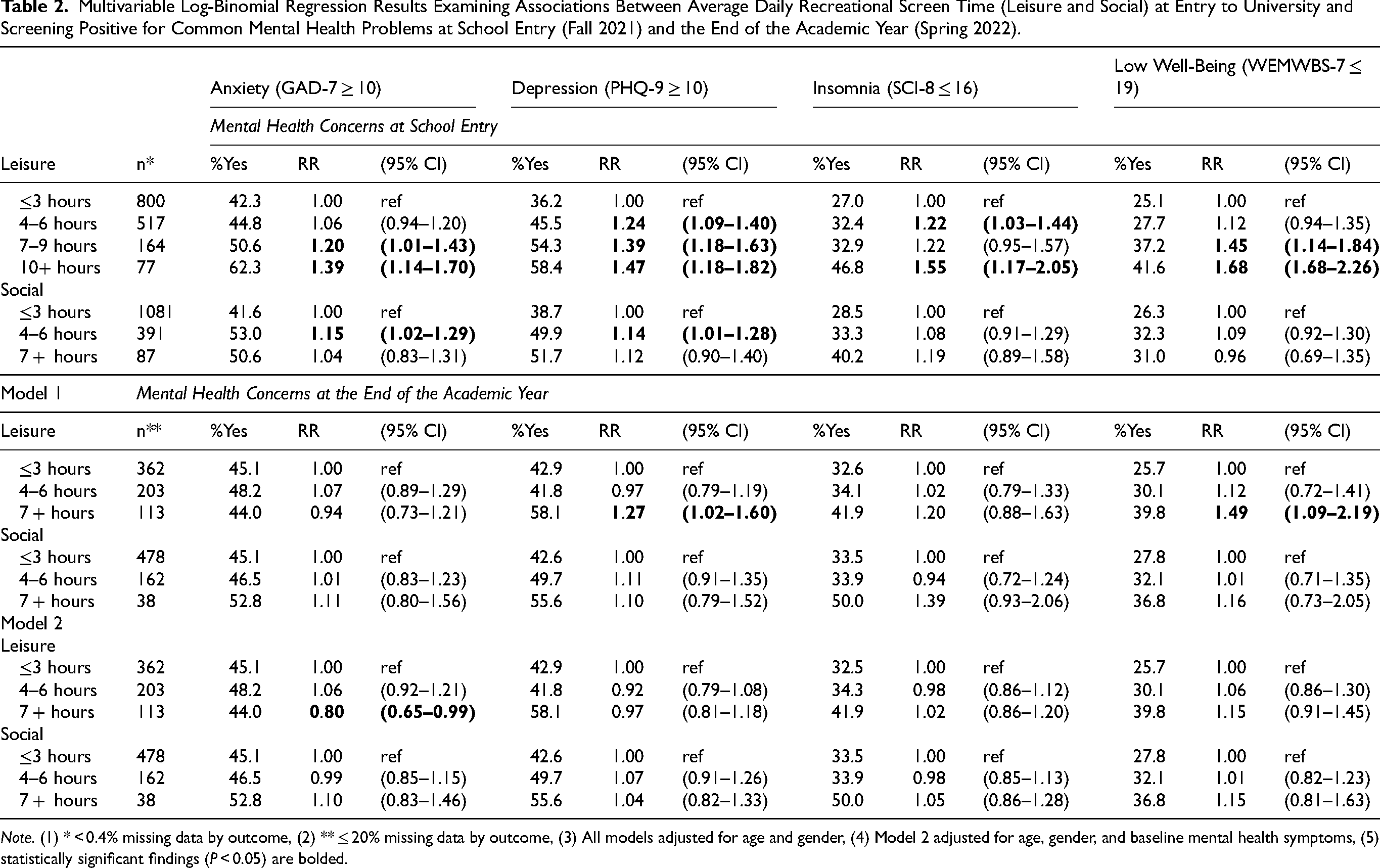
Note. (1) * < 0.4% missing data by outcome, (2) ** ≤ 20% missing data by outcome, (3) All models adjusted for age and gender, (4) Model 2 adjusted for age, gender, and baseline mental health symptoms, (5) statistically significant findings (P < 0.05) are bolded.
Associations between screen time and mental health outcomes were comparable between male and female students, except for disordered eating (Table 3). At school entry longer duration of leisure screen time was significantly associated with an increased risk of screening positive for disordered eating in females, but not males. However, 7 + hours of daily leisure screen time increased the risk of screening positive for disordered eating at the end of the academic year in both males and females. While 4 + hours/day of social screen time was associated with an increased risk of disordered eating at school entry, the effect was larger and statistically significant only in males (Table 3).
Multivariable Log-Binomial Regression Results Examining Associations Between Screen Time Reported at School Entry and Screening Positive for Disordered Eating (SCOFF ≥2) at the Beginning and End of the Academic Year, Stratified by Gender.
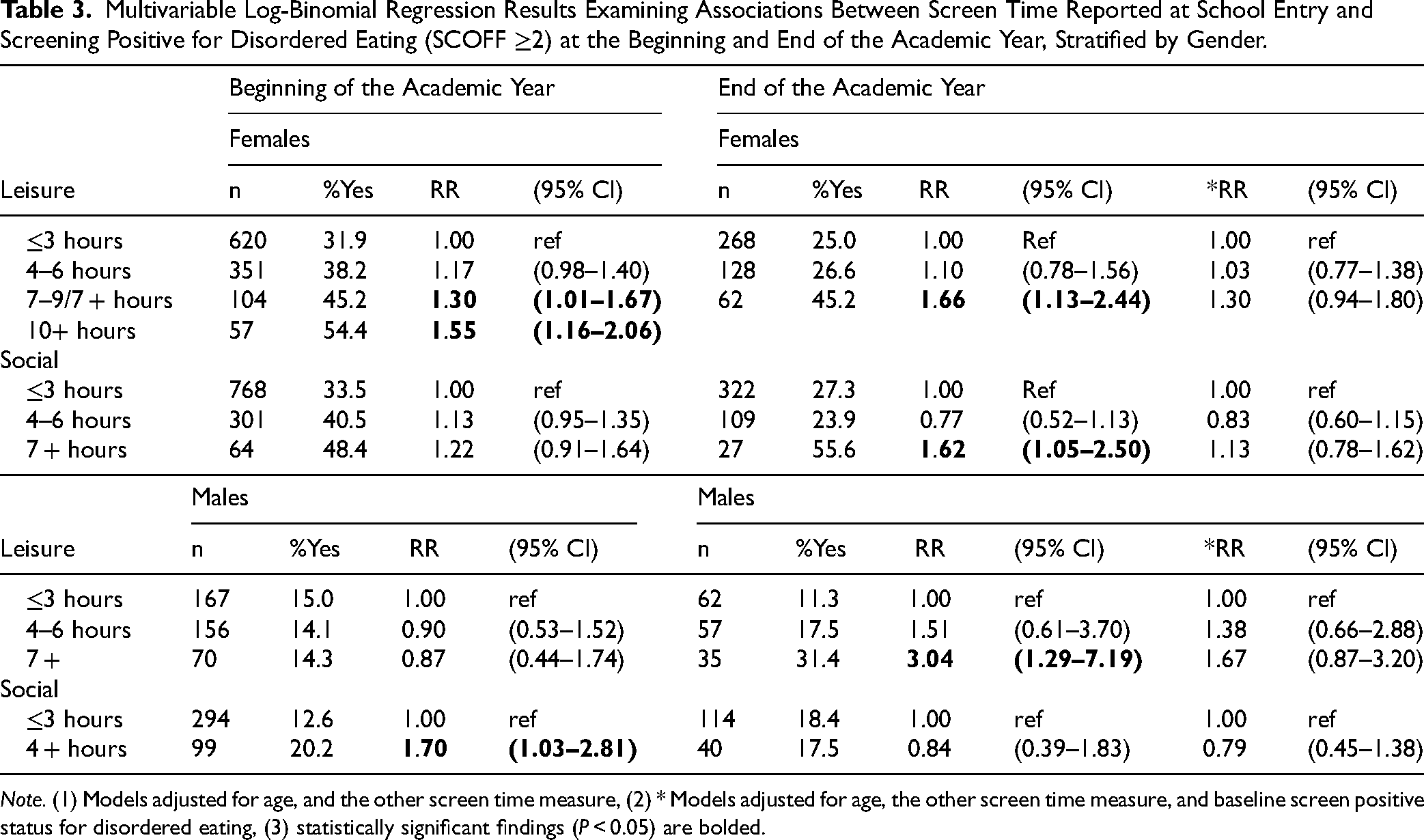
Note. (1) Models adjusted for age, and the other screen time measure, (2) * Models adjusted for age, the other screen time measure, and baseline screen positive status for disordered eating, (3) statistically significant findings (P < 0.05) are bolded.
Associations between screen time at school entry and mental health at the end of the year were generally consistent with the cross-sectional analysis, but smaller in magnitude (Table 2). However, only the associations between leisure screen time (≥7 hours/day) and increased risk of screening positive for depression and low well-being remained statistically significant; the association with anxiety was no longer evident (Tables 2 and 3). After adjustment for baseline symptoms, the associations were no longer statistically significant.
Self-Esteem as a Moderator of the Relationship Between Screen Time and Anxiety and Depression at University Entry
Students with low self-esteem were significantly more likely to screen positive for anxiety (72.5%) and depression (77.6%) at school entry than those with moderate (43.9% and 37.5%) and high (18.0% and 11.8%) self-esteem. However, the cross-sectional associations between longer duration of leisure screen time and clinically significant levels of anxiety and depressive symptoms were only observed in the high self-esteem group (Table 4). High self-esteem students who reported averaging 4–6 and 7 + hours/day of leisure screen time were 73% and 139% more likely to screen positive for anxiety and 118% and 172% more likely to screen positive for depression than those reporting ≤3 hours/day, respectively.
Multivariable Log-Binomial Regression Results Exploring Associations Between Average Daily Recreational Screen Time (Leisure and Social) and Screening Positive for Anxiety and Depression at University Entry (Fall 2021), Stratified by Level of Self-Esteem.
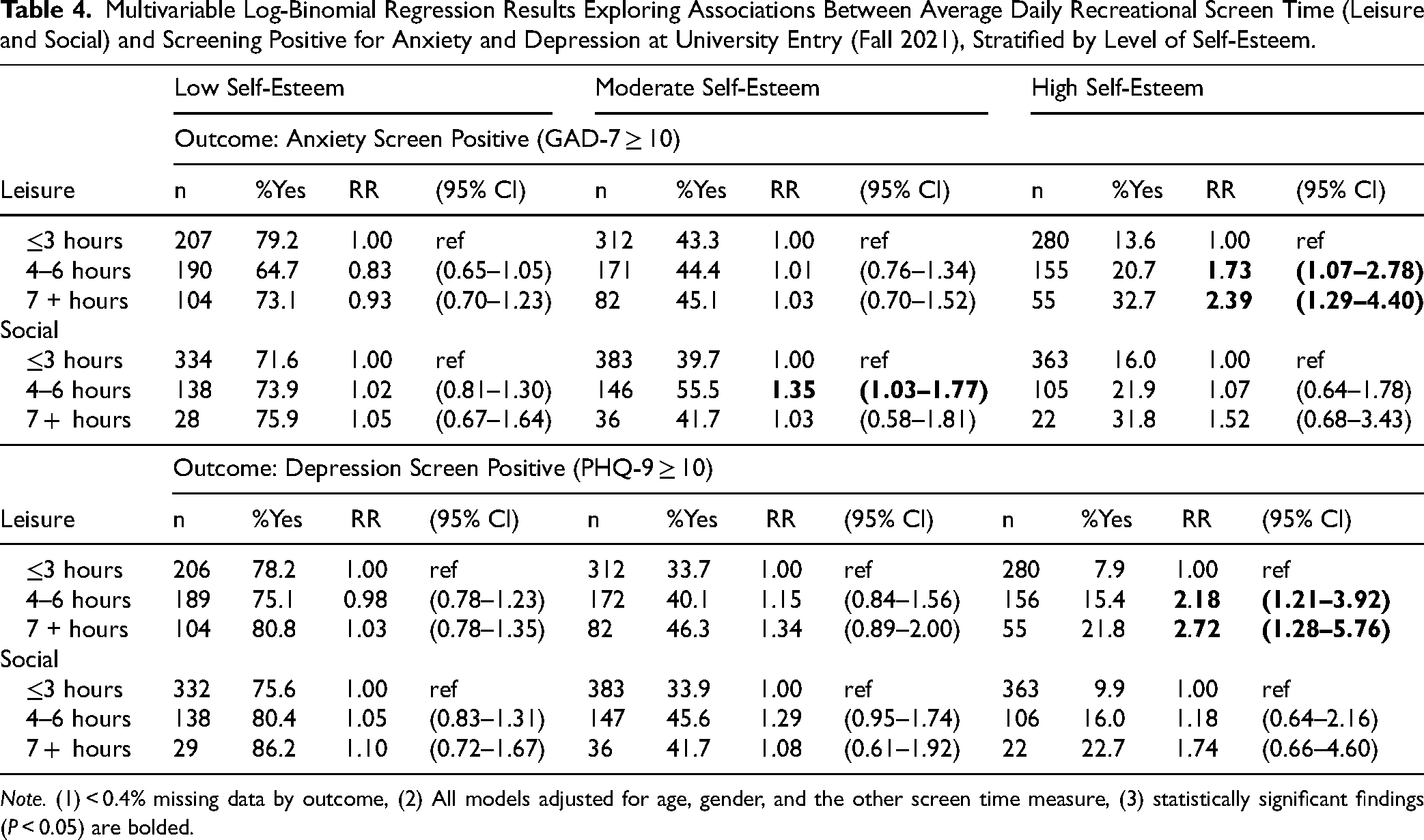
Note. (1) < 0.4% missing data by outcome, (2) All models adjusted for age, gender, and the other screen time measure, (3) statistically significant findings (P < 0.05) are bolded.
Discussion
This study examined the relationship between recreational screen time (leisure and social) and screening positive for common mental health concerns and low well-being in a large cohort of first-year undergraduates attending a major Canadian university. There was evidence of an association between averaging >3 hours/day of leisure screen time and screening positive for depression, anxiety, low well-being, and probable insomnia at university entry. Over half the students reported leisure screen time (4 + hours/day) associated with increased risk of significant mental health concerns. Similarly, there was evidence of an association between 7 + hours/day of leisure screen time and screening positive for depression and low well-being at the end of the academic year; however, the associations became non-significant after adjustment for baseline symptoms. Finally, the associations between increased daily leisure screen time (4 + hours) and screening positive for anxiety and depression at school entry were strongest in students reporting higher self-esteem.
Our main findings align with the extant literature. That is, while screen time has been associated with varying effects depending on individual differences, and the nature (passive vs. interactive; leisure vs. social), frequency, intensity, and duration of use, high levels of leisure screen time have consistently been linked with poor mental health.19,26,39 The positive relationship between duration of leisure screen time and increased risk of mental health problems identified is consistent with prior research on anxiety, depression, and insomnia.40–44 In this study, leisure screen time was associated with concurrent mental health status, but not with declines over the year, suggesting screen time may have a greater impact on current symptoms than the development of future problems. The observed cross-sectional association may be partly explained by reverse causality or shared underlying factors. Students experiencing poor mental health may use screens for emotional regulation, coping, or social connection, or because they lack the energy for non-screen activities.45,46 However, previous studies found limited evidence of a reverse association between psychopathology and subsequent screen time. 26 Our finding of minimal long-term effects of screen time on mental health aligns with previous studies showing inconsistent and largely attenuated longitudinal associations. 26
With the exception of disordered eating, screen time was positively correlated with mental health problems independent of gender, which differs from previous studies reporting more negative effects of high levels of screen time in females.19,24,26 However, these studies focused specifically on social media-based screen use.
The literature reports mixed findings regarding the effects of different types of screen time on mental health. While >3 hours/day of passive leisure screen time has consistently been linked to mood and anxiety disorders,19,27 some studies report no association or even positive effects on mental health.27,47 Similar to prior research, we found greater negative effects associated with leisure compared to active social screen time.19,24,26,27 Social media use has been negatively correlated with mental health, but few studies have examined the effects of time spent using screens specifically for interacting socially. In this study, social media-based screen time could have been captured as social (actively posting or messaging) or leisure (passively scrolling). Although not directly measured, our findings suggest passive social media use may have a greater negative mental health impact than active communication.
The passive use hypothesis posits that passive leisure screen time is associated with increased loneliness and negative affect, and that it increases upward social comparison more than active use. 48 In contrast, using screens to connect with others socially has been associated with increased social connectedness, subjective well-being, and participation in other health-promoting activities including physical recreation.29,49 Although online interactions pose barriers to understanding tone, mood and body language, and decrease the overall level of social connectedness compared to in-person interactions, 50 they may still alleviate feelings of loneliness. 51
Interestingly, leisure screen time was significantly associated with disordered eating in females, but not males. This aligns with prior findings and highlights the importance of considering the type of screen use young males and females engage in. Leisure screen time, as defined in this study, encompasses different activities such as watching television or videos, playing video games, or scrolling on social media. Males and females may differ in how they use screens, and what they are consuming. Male respondents may have spent more time playing video games, while females may have spent more time scrolling on social media. Among 13–15-year-olds, girls were found to average 3.28 hours/day on social media, compared to 2.05 hours for boys. 28 In contrast, boys spent significantly more time on video games (3.25 hours/day vs. 1.17). Importantly, social media use was more strongly associated with negative mental health outcomes than gaming. 28 Specifically, exposure to appearance-focused social media has been linked to body image concerns and thin-ideal internalization among young women. 52 Studies should further investigate how gendered patterns of screen use may influence disordered eating. 53
Self-Esteem at School Entry (Effect Modifier)
We found evidence that leisure screen time over 3 hours/day was most strongly associated with screening positive for anxiety and depression in students reporting higher self-esteem. This is a surprising finding, as higher self-esteem has been associated with more positive or protective effects on mental health and loneliness related to social media use,54,55 but there is little evidence to support a negative moderating effect on screen time and mental health. Previous research has also shown high self-esteem may only be protective up to a point, with effects diminishing at higher levels of screen time. 56 Further research is needed to elucidate the mechanisms underlying this finding given the cross-sectional nature of the data and reliance on self-report.
Implications and Future Directions
Recreational screen time greater than 3 hours/day was reported by over 50% of students in this study and represents a potentially modifiable target for health promotion and prevention initiatives in university students. While guidelines on screen time duration for young adults are unclear, and what constitutes “excessive” use remains debated, some recommend limiting recreational screen time to 3 hours daily. 57 This aligns with our finding that over 3 hours/day of leisure screen time is associated with increased risk of common mental health concerns. Previous studies have explored ways to limit screen time by self-nudging apps that monitor and remind users that they have extended beyond their set time limit. 58 Users of the app reported increased satisfaction with their use of screens and reduced time watching videos compared to controls. 59 Other strategies include choosing screen activities that are more cognitively engaging and avoiding screens before bedtime.
Future research is needed to understand mechanisms by which screen time affects mental health or vice versa, such as impacts on sleep quality/duration, emotional regulation, loneliness, and physical activity. The specific content being consumed may be increasing depressive and anxiety symptoms in this population, and/or screen time may take time away from positive mental health practices, or the actual light emissions could increase symptoms for example. 26 Understanding these mechanisms can help tailor university health promotion efforts to student behavioural patterns. Consideration of specific types of screen activities and applying objective measures 60 can be used to further increase understanding of these associations.
Strengths and Limitations
Strengths of our study include the use of a large broadly representative sample of first-year students, 61 with prospective follow-up data. Validated screening measures for assessing mental health problems and self-esteem were used, enhancing the reliability of the findings. Limitations of this study include a bias toward over-sampling female students and loss to follow-up, which may affect generalizability. The screen time measures lacked detail and are susceptible to recall bias and measurement error. Notably, the lowest category of daily screen time was ≤3 hours, which may have masked variability in risk. Additionally, the use of a single time-point measure of screen use may not have captured more habitual use. While we were able to examine leisure versus active social screen time, we did not have detailed or objective measures of either, and we did not specifically examine social media use. Furthermore, students may have had difficulty separating leisure and social screen time, which may not be mutually exclusive. Consequently, our ability to identify more nuanced associations between screen time and mental health was limited. Lastly, this study had limited power to detect some associations, particularly at higher levels of screen time and within gender-stratified analyses.
Conclusion
This study found evidence that leisure screen time of 4 + hours/day at entry to university is common and negatively associated with mental health among first-year undergraduates. Future research is needed on the mechanisms underlying the negative impact of screen time on university students’ mental health, and those most at risk. However, there appears to be sufficient evidence and rationale to include guidance on healthy and responsible recreational screen time for incoming university students as part of mental health prevention and health promotion initiatives.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437261428821 - Supplemental material for Recreational Screen Time at University Entry and Mental Health and Well-Being Over First Year: U-Flourish Student Well-Being Research
Supplemental material, sj-docx-1-cpa-10.1177_07067437261428821 for Recreational Screen Time at University Entry and Mental Health and Well-Being Over First Year: U-Flourish Student Well-Being Research by Simran Brar, MSc, Nathan King, PhD, Anna Park, BHSc, Kristen Kyone, BHSc, Emily Dephoure, BHSc, Daniel Rivera, MSc, Adeleine Lyon, MSc and Anne Duffy, MD, MSc, FRCPC in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
We thank the students who “had their say” and participated in this research and the student volunteers who helped develop and raise awareness contributing to the high participation rate.
Data Access
Access to de-identified data will be considered upon request to the corresponding author after study completion.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research (grant no. 165597) and the Rossy Family Foundation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.