
Abstract
Objective
Patients with intellectual and developmental disabilities (IDDs) and psychiatric disorders are at higher risk for prolonged hospitalisations. The aim of this study was to examine the prevalence of IDD among long-stay inpatients in Ontario psychiatric beds, and compare the demographic and clinical profiles of long-stay inpatients with and without IDD.
Methods
This Ontario population-based cross-sectional study used linked health administrative databases. All patients over 18 years of age occupying a non-forensic psychiatric inpatient bed in Ontario on September 30th, 2023 were included in the analysis. We examined prevalence of IDD among patients with a length of stay (LOS) ≥ 365 days (‘long-stay patients’). Standardised differences were used to compare demographic, clinical, functional, and health care utilisation characteristics between patients with and without IDD.
Results
Of the 1,466 long-stay patients in an Ontario non-forensic psychiatric inpatient bed, 22.0% had IDD. They were younger (mean age 44.3 vs. 47.6) and a higher proportion were male (64.3% vs. 50.1%). In the 2 years prior to admission, a higher proportion of long-stay patients with IDD had a psychotic disorder (73.3% vs. 54.0%), and they had a higher median number of ED visits (5 vs. 3). Long-stay inpatients with IDD were more likely to have difficulty with activities of daily living (39.8% vs. 15.0%), moderate/severe cognitive impairment (63.0% vs. 29.9%) and fewer social contacts in place to support discharge (59.3% vs. 48.6%). While in hospital, a greater proportion of long-stay patients with IDD were subject to restraints (12.4% vs. 8.0%) and seclusion (20.2% vs. 11.2%).
Conclusions
Adults with IDD account for more than one in five long-stay psychiatric inpatients and have unique needs including greater cognitive impairment and difficulty caring for themselves. Successful transitions out of hospital require specialised resources and cross-sectoral collaboration.
Plain Language Summary Title
A closer look at patients with and without developmental disabilities with lengthy hospitalisations
Plain Language Summary
Patients with intellectual and developmental disabilities (IDDs) and psychiatric disorders are at higher risk of having very long hospital stays. Long hospital stays can lead to negative outcomes for patients and cause treatment delays for other people who need inpatient care. The aim of this study was to learn how many long-stay inpatients in Ontario psychiatric beds have IDD and compare long-stay inpatients with and without IDD to see whether they might have different needs.
We did this using administrative health data. We started by identifying all patients over 18 years old who were in a psychiatric inpatient bed in Ontario on September 30th, 2023. Then we looked at how many of these patients had been in the hospital for at least 365 days. We learned that more than 1 in 5 of these long-stay patients had IDD. Long-stay patients with IDD had some similarities and also differences from long-stay patients without IDD. Some key differences include that long-stay patients with IDD were younger (mean age 44 vs. 48), and a higher proportion were male (64% vs. 50%). More long-stay patients with IDD had a psychotic disorder (73% vs. 54%), were subject to restraints (12% vs. 8%) and seclusion (20% vs. 11%), had moderate/severe cognitive impairment (63% vs. 30%), had difficulty with activities of daily living (40% vs. 15%) and lacked social support for discharge (59% vs. 49%). These differences mean that patients with IDD may need different types of care while in hospital and different supports to help them transition out of hospital. See Supplement A for an easy read version of this summary.
Background
Hospitals across Canada, including psychiatric hospitals, are experiencing an ongoing capacity crisis.1,2 One key contributor to this crisis is the large numbers of inpatients with long hospital stays, many of whom no longer require hospital-level care. 3 Cases where patients remain in hospital despite being ready for discharge are sometimes referred to as delayed discharges; in Canada, these patients are designated as alternate level of care (ALC). This designation signals that the patient no longer requires the intensity of services provided in a hospital but cannot yet be discharged, often due to a lack of appropriate community support options.
Lengthy hospitalisations, which are often ALC, can lead to negative outcomes for patients including deterioration of their physical health, mental health and social connections.3–6 They put pressure on hospital staff, who report increased frustration, guilt, burnout, and job dissatisfaction.3,4 At a system level, lengthy hospitalisations can lead to treatment delays and poor health outcomes for other patients who urgently require hospital care, as well as cascading challenges across hospital and community services.3,4,7 Typically, ALC initiatives focus on older adults in medical beds and little focus has been given to psychiatric inpatients.
As many as 40% to 45% of adults with IDD have a psychiatric diagnosis. 8 This group is more likely to become hospitalised and experience repeated hospitalisations compared with adults with IDD only or adults with a psychiatric diagnosis only.9,10 Some prior research has also indicated that adults with IDD are at higher risk of having lengthy or ALC hospital stays.9,11,12 Concerns have long been raised about barriers to transitioning patients with IDD out of hospital including the lack of community mental health services and housing options that are appropriate and equipped to meet the unique needs of this patient group.11,13 A better understanding is needed of the number of long-stay patients with IDD in hospital and their service needs in order to inform strategies to transition these patients out of hospital.
The aim of the present study was to examine the prevalence of IDD among long-stay inpatients in Ontario psychiatric beds, and compare the demographic and clinical profiles of long-stay inpatients with and without IDD.
Methods
Study Design, Population, and Setting
We conducted a population-based cross-sectional study including all patients aged 18 years and older occupying a psychiatric inpatient bed in Ontario, Canada as of September 30th, 2023 (the most recent available data at the time of analysis). This includes admissions to inpatient mental health beds located in general hospitals, provincial psychiatric facilities, and specialty psychiatric facilities. These patients would have been admitted to a psychiatric inpatient bed in Ontario prior to September 30th, 2023, with no record of being discharged from the setting (N = 5,735). We excluded patients with a death date prior to September 30th, 2023 (N = 233, 4.1%) or an invalid Ontario postal code upon their admission to hospital (N = 13, 0.2%). From this population of 5,489 psychiatric inpatients, we selected the 4,687 occupying non-forensic beds; those occupying forensic beds (due to involvement with the Ontario justice system) may have lengthy hospital stays for legal reasons.
Occupants of non-forensic psychiatric inpatient beds on September 30th, 2023 may have been previously transferred from other hospital institutions or units. In cases where patients were transferred between sites after their initial admission, we linked together consecutive inpatient records to form ‘episodes of care’. The earliest admission date within the hospital episode of care was used to determine the length of stay (LOS) as of September 30th, 2023 for our study population. We defined ‘long-stay’ as patients with a LOS ≥ 365 days. There was no reliable way within our dataset to identify which patients were formally designated as ALC.
Data Sources
We used linked health administrative databases from Ontario, which have been used previously to examine health service use among individuals with IDD in the province (e.g.,10,14,15). These databases were linked using encoded identifiers and analyzed at ICES, an independent, non-profit research institute. The use of data in this project was authorised under section 45 of Ontario's Personal Health Information Protection Act, which does not require review by a Research Ethics Board.
The Ontario Mental Health Reporting System (OMHRS), compiled by the Canadian Institute for Health Information (CIHI), contains administrative information on all admissions to adult psychiatric inpatient beds in the province and was used to create our study population. Additionally, the OMHRS holds clinical and functional information from the Resident Assessment Instrument for Mental Health (RAI-MH), 16 which is administered to psychiatric inpatients throughout their admission. Administrative and clinical information on emergency department (ED) visits, same-day surgery clinic procedures, or admissions to non-psychiatric inpatient beds were captured using CIHI's National Ambulatory Care System (NACRS), Same Day Surgery (SDS) Database, and Discharge Abstract Database (DAD), respectively. Physician visits were identified using the Ontario Health Insurance Plan (OHIP) billing claims database. Finally, the Registered Persons Database (RPDB) provided demographic information including age, sex, and date of death; it also included a yearly estimate of a patient's postal code, which was linked to census data using versions of the Postal CodeOM Conversion File Plus (PCCF+) to provide geographic-based measures.
Intellectual and Developmental Disabilities
The presence of an IDD was identified through a lifetime lookback in the administrative health databases from September 30th, 2023 using the following previously established case definition 17 : (1) One or more hospital visits recorded in the DAD or SDS with an IDD diagnosis in any diagnostic code field since database inception (DAD = April 1988; SDS = April 1991); (2) one or more hospital visits in OMHRS with an IDD diagnosis in any diagnostic code field since database inception (October 2005); (3) one or more ED visit in NACRS with an IDD diagnosis in any diagnostic code field since database inception (April 2002); or (4) two or more outpatient physician visits in OHIP with an IDD diagnosis since database inception (July 1991). Consistent with Ontario legislative definitions of IDD, diagnostic codes included terms such as mental retardation/intellectual disability, autism, other pervasive developmental disorders, fetal alcohol syndrome, and various chromosomal disorders. The same case definition was applied to health care interactions with a diagnosis of autism to measure its prevalence within the IDD cohort. 18 See Supplement B for more detail.
Sociodemographic Characteristics and Pre-Admission Diagnoses
Patient age, sex, neighbourhood income quintile, and rural residence (living in communities with <10,000 individuals) were captured using the RPDB. Information from the RAI-MH assessment upon admission to a psychiatric inpatient bed was used to identify patients living in group settings (e.g., boarding home, long-term care home, group home, jail) with non-relatives prior to admission. A previously validated definition 19 developed in Ontario was used to determine a past diagnosis of epilepsy. This consisted of a lifetime lookback in the administrative health databases from September 30th, 2023 for: (1) One or more hospital visits recorded in the DAD or SDS with an epilepsy diagnosis in any diagnostic code field, or (2) three or more outpatient physician visits in OHIP with an epilepsy diagnosis in any two-year period. To measure concurrent mental health and addiction conditions at the time of entry to a psychiatric inpatient bed, we looked back two years from admission date and flagged patients with any hospital-, ED-, or physician-based interactions for mood or anxiety disorders, psychotic disorders, or substance use disorders. 20
Health Care Utilisation Prior to Admission
We counted the number of health care interactions for each patient in the two years prior to a psychiatric inpatient admission. The OHIP claims database was used to determine the number of outpatient physician visits made by a patient to family/general practitioners and psychiatrists; only one visit per day per physician was included to avoid over-counting. We also counted the number of previous unique hospitalisation episodes (DAD and OMHRS) and unplanned ED visits (NACRS).
Clinical and Functional Characteristics During Hospital Admission
The RAI-MH completed upon admission was used to identify the reasons for admission. The RAI-MH completed closest to September 30th, 2023 was used to assess clinical and functional characteristics that may impact discharge planning: level of independence (Activities of Daily Living Hierarchy Scale), level of cognitive impairment (Cognitive Performance Scale), a flag for whether patients lacked appropriate social/familial connections to support discharge (Support Systems for Discharge Clinical Assessment Protocol), physical restraint use (measured as some restraint use in the three days prior to assessment), and seclusion (measured as confinement to hospital room at some point in the three days prior to assessment).
Analysis
Among long-stay patients occupying a non-forensic psychiatric inpatient bed, standardised differences were used to compare demographic, clinical/functional, and health care utilisation characteristics between patients with and without IDD. Standardised differences use effect size methods to assess meaningful differences in large, population-based studies where P values can be influenced by the large sample size. 21 Standardised differences > 0.1 were considered to be clinically meaningful. All analyses were conducted using SAS version 9.4.
Results
On September 30th 2023, there were 4,687 patients in Ontario non-forensic psychiatric inpatient beds (of which 19.9% had IDD). Of these patients, 1,466 had been in the hospital for at least one year, including 322 patients (22.0%) with IDD. Compared with other long-stay inpatients, long-stay patients with IDD were younger (mean age 44.3 vs. 47.6; standardised difference [StdDiff] = 0.195) and a higher proportion were male (64.3% vs. 50.1%; StdDiff = 0.290) (see Table 1). Within the IDD group, 125 patients (38.8%) were autistic (not shown). In the 2 years prior to admission, a higher proportion of patients with IDD had a psychotic disorder (73.3% vs. 54.0%; StdDiff = 0.409) and a similar proportion of both groups had a substance use disorder. Patients with IDD were more likely to have an epilepsy diagnosis (16.5% vs. 5.6%; StdDiff = 0.352) and to be living with non-relatives prior to admission (28.3% vs. 9.4%; StdDiff = 0.499).
Sociodemographic Characteristics and Pre-Admission Diagnoses of Long-Stay Patients With and Without IDD in Ontario Non-Forensic Psychiatric Beds (LOS ≥ 365 Days).
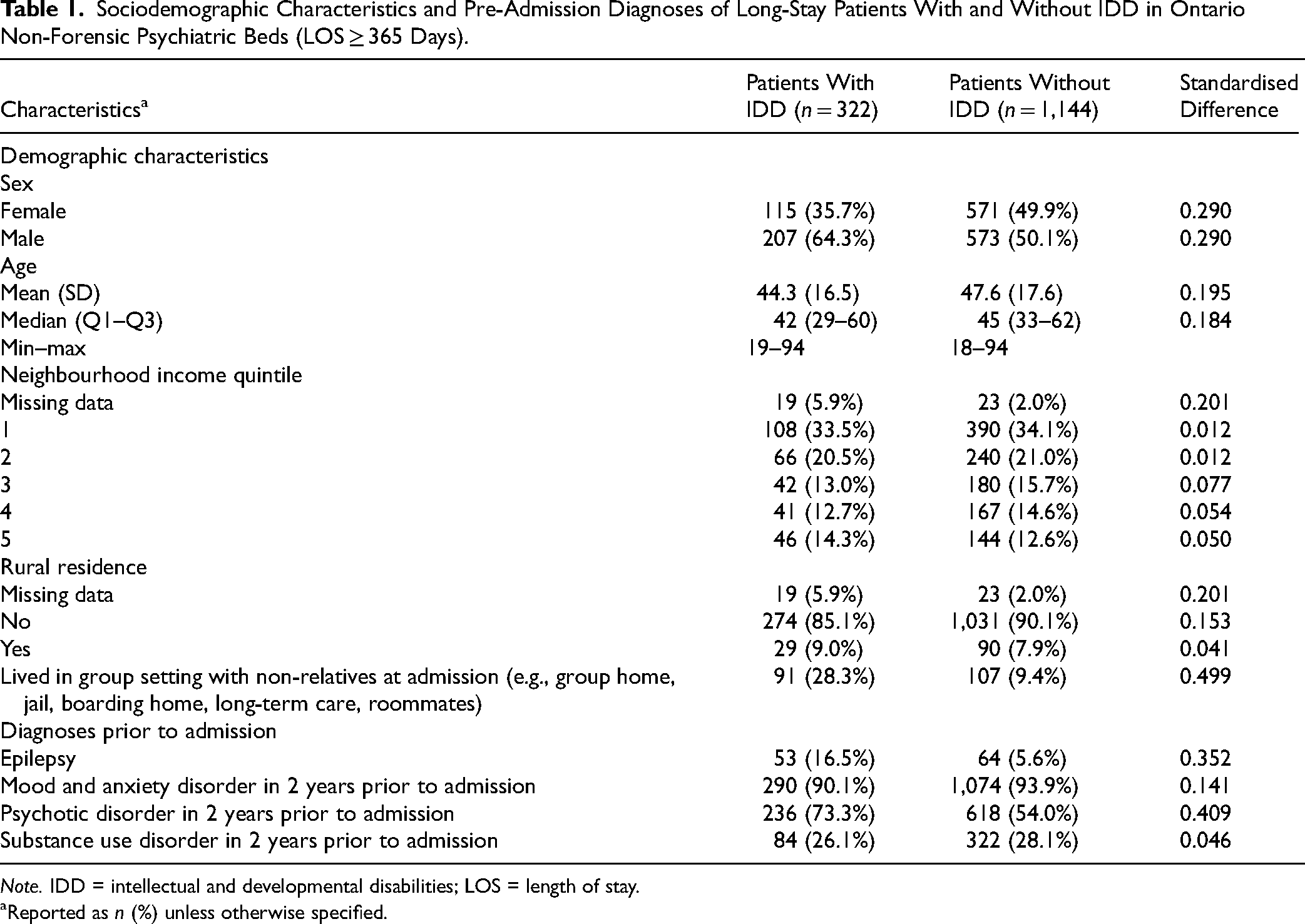
Note. IDD = intellectual and developmental disabilities; LOS = length of stay.
Reported as n (%) unless otherwise specified.
Both long-stay patients with and without IDD were likely to have utilised health care services in the two years prior to admission (see Table 2). Patients with IDD had a higher median number of outpatient psychiatry visits (3 vs. 1; StdDiff = 0.208) as well as a higher median number of ED visits (5 vs. 3; StdDiff = 0.226).
Health-Care Use During 2-Year Period Prior to Admission (LOS ≥ 365 Days).
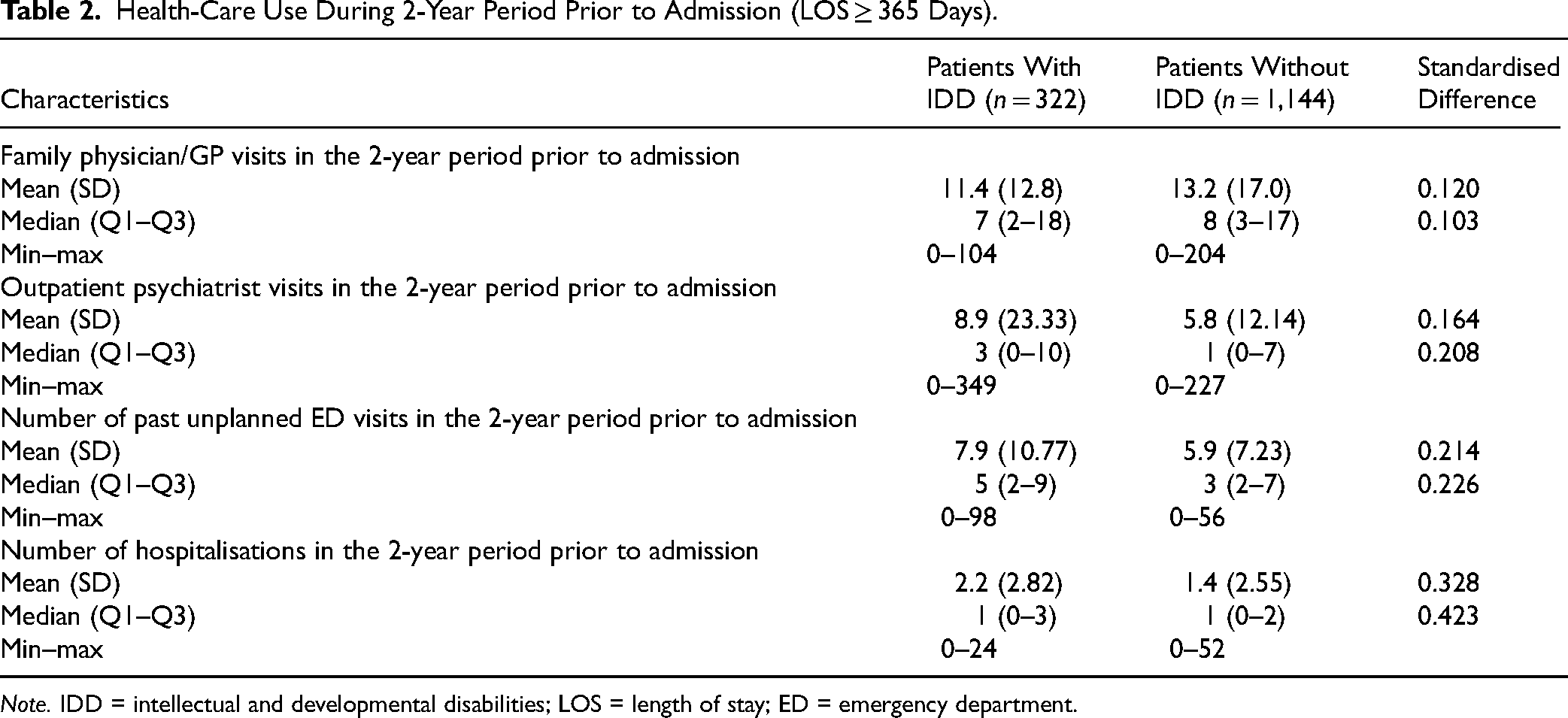
Note. IDD = intellectual and developmental disabilities; LOS = length of stay; ED = emergency department.
Both patients with and without an IDD had a median LOS of 3 years and a mean LOS over 4 years (see Table 3). Inpatients with IDD were more likely to be admitted due to threat to others or inability to care for self, whereas those without IDD were more likely to be admitted due to threat to self. Only 5.3% of patients with IDD were in specialised units for people with IDD, with the remainder in a range of different psychiatric units including acute units (41.0%), longer term units (32.3%), and geriatric units (6.5%) (not shown). While in hospital, a greater proportion of patients with IDD were subject to restraint use (12.4% vs. 8.0%; StdDiff = 0.148) and seclusion (20.2% vs. 11.2%; StdDiff = 0.249). Patients with IDD were also more likely to have difficulty with activities of daily living (39.8% vs. 15.0%; StdDiff = 0.577), severe cognitive impairment (29.5% vs. 9.6%; StdDiff = 0.518) and fewer social contacts in place to support discharge (59.3% vs. 48.6%; StdDiff = 0.216).
Clinical and Functional Characteristics During Hospital Admission (LOS ≥ 365 Days).
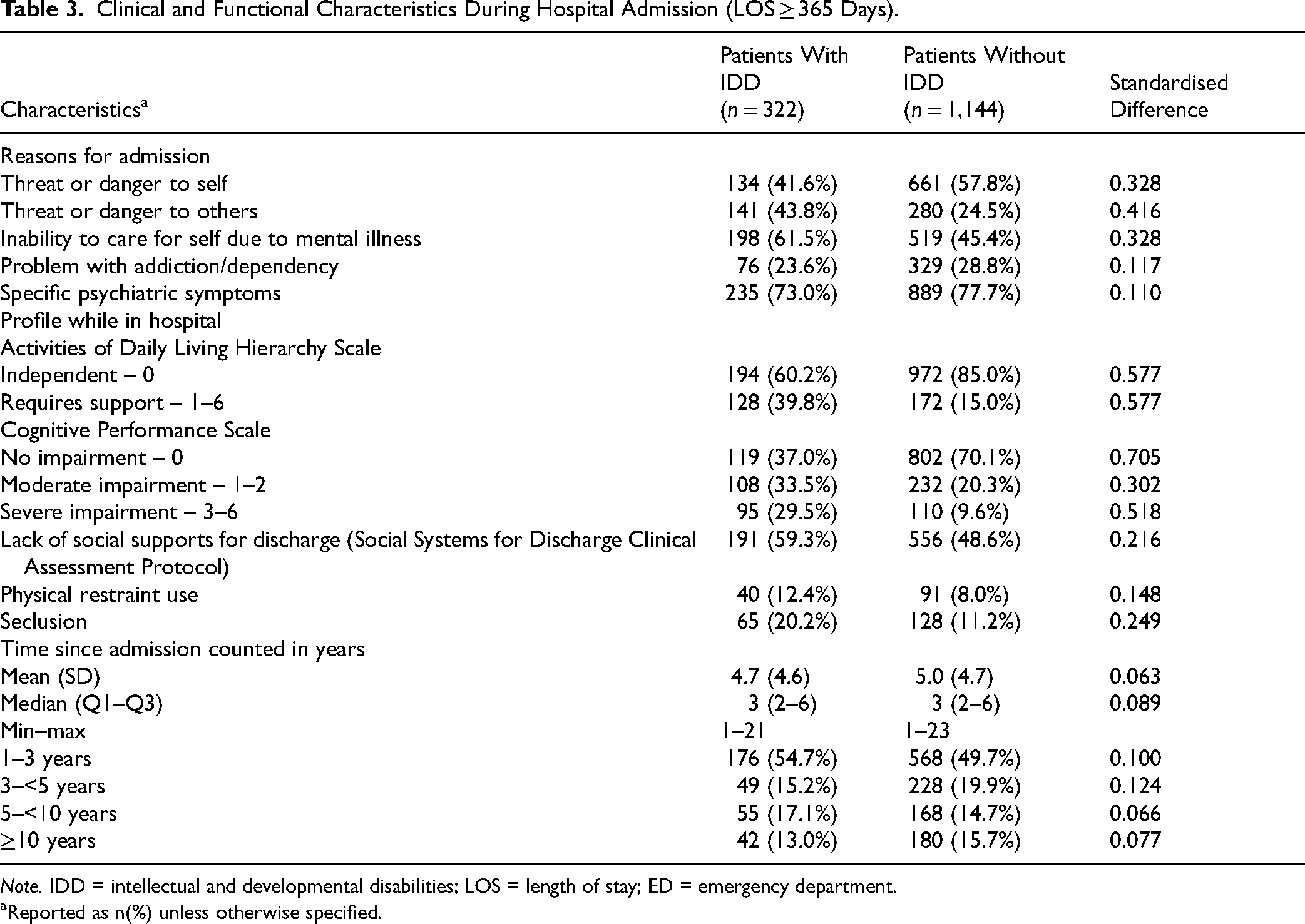
Note. IDD = intellectual and developmental disabilities; LOS = length of stay; ED = emergency department.
Reported as n(%) unless otherwise specified.
Discussion
This study found that more than one in five patients in Ontario who had been in a non-forensic psychiatric bed for over a year had an IDD, yet policies and practices to support long-stay patients are typically not designed considering this group. When we compared long-stay patients with and without IDD we found some similarities but also several differences. Almost three-quarters of long-stay patients with IDD in this study had a psychotic disorder, compared with just over half of long-stay patients without IDD. This aligns with other studies which have found a disproportionately high prevalence of psychosis diagnoses among people with IDD.22–25 Long-stay patients with IDD were more likely to be admitted due to threat to others or inability to care for self. They were also more likely to have moderate or severe cognitive impairment, epilepsy, difficulty with activities of daily living, and limited social support systems compared with other long-stay patients.
Given this complex needs profile, it is likely long-stay patients with IDD require support from both the community health and social services sectors to facilitate successful transitions out of hospital. Securing the community healthcare necessary for a successful discharge can be challenging for patients with IDD. There are limited specialised outpatient mental health programmes for adults with IDD26,27 and they may have less expertise in certain treatment areas, such as substance use.28,29 Non-specialised outpatient mental health providers often have limited training and confidence caring for patients with IDD, with the result that they may be reluctant to accept them into care.30–32 In the absence of specialised mental health services, primary care providers can also be reluctant to accept these patients and even if primary care can be secured, they are often inadequately resourced to be the sole health care provider.33–35 Additionally, it is challenging to secure appropriate developmental services housing and community-based programmes, further complicated by the limited established partnerships or pathways between the hospital and developmental services sectors.33,36
Though we do not know what proportion of the 322 long-stay patients with IDD in this study were designated as ALC, it is reasonable to assume many of these patients no longer required hospital-level care and remain in hospital due to a lack of appropriate community health and social services. We also know that many patients are designated ALC with far shorter lengths of stay 3 and it is likely the total number of patients with IDD who were ALC in hospital at the time of the study was much higher.
Another potential reason for long hospital stays may be lack of appropriate care while in hospital.37,38 There are few specialised psychiatric inpatient units for people with IDD in Ontario and the vast majority of patients with IDD in this study were located in non-specialised units. Non-specialised hospital providers often lack sufficient training on how to care for patients with IDD.30,39–42 Among other challenges, this can lead to mental health conditions being misattributed to the person's disability, or for people with a mild intellectual disability or autism with no intellectual disability, the disability may be overlooked. This is referred to as ‘diagnostic overshadowing’ and prevents people from getting the care they need.43,44 Additionally, non-specialised inpatient psychiatry units may not have the range of staff disciplines required to provide comprehensive care for patients with IDD, including psychology, occupational therapy, speech and language therapy, and behaviour analysis.26,39
Nonspecialized psychiatric units also often lack the built environment necessary to provide the structured, calm sensory-friendly setting required by many patients with IDD.37,45 This is a particular challenge for autistic patients who comprised almost 40% of long-stay patients with IDD in this study. For example, while bright florescent lights, disruptive code announcements, pungent cleaning products and loud roommates can be unpleasant for any patient, for patients with sensory sensitivities and reliance on specific routines, these common features of inpatient units can be intolerable. Sensory distress can impair communication ability and lead to distressed behaviours which may be met with medications, restraints and seclusion, which in turn lead to further decompensation and increased difficulty transitioning out of hospital.37,38,46–48 In the present study, long-stay patients with IDD were more likely to be subject to restraints and seclusion than patients without IDD.
Strategies to Address Prolonged Hospitalisations in the IDD Population
The Supporting Alternate Level of Care Patients with a Dual Diagnosis to Transition from Hospital to Home Practice Guidance (2023) 33 outlines 10 core components necessary to support successful transitions for this population. Critical elements include community healthcare, appropriate housing, comprehensive transition plans, patient and family involvement in transition planning, and coordinated transitions with overlapping support from the hospital and community. A central tenet of the guidance is the need for health and social services providers to work together to support successful transitions and appropriate follow-up care in the community. Implementing this guidance requires system-level infrastructure including clear system pathways, funding for housing and intensive community supports, and data systems which can identify ALC patients with IDD and communicate that data in real time to relevant health and social services providers to facilitate proactive response.
Increased capacity is needed within inpatient and outpatient mental health settings to provide appropriate care for patients with IDD. One strategy to achieve this is to hire or train staff to have the necessary IDD expertise. There are existing education programmes which can be leveraged such as the Extension for Community Healthcare Outcomes programme (Project ECHO), a virtual education programme which brings together health and social care providers to learn with and from each other. 49 Another strategy is to utilise consultation models to access IDD expertise as needed. For example, in the United Kingdom, acute care hospitals often have dedicated learning disability liaison nurses who provide consultation and support across the hospital as needed.50,51 Typically liaison nurses provide support in acute medical settings but the model may also have value for psychiatric settings. Currently IDD consultation models are not routinely available in Canada though some successful specialist consultation models exist. 52 For example, the Adult Neurodevelopmental Consult-Liaison Service at the Centre for Addiction and Mental Health, a large psychiatric hospital in Toronto, is an interprofessional team including psychiatrists and allied health professionals who provide consultation to inpatient units and the ED to support patients with IDD.
A third strategy is to increase access to specialised services. For example, specialised IDD Flexible Assertive Community Treatment teams have been implemented in a number of countries to support high need patients with IDD and psychiatric disorders in the community with emerging evidence of positive outcomes, including reduced hospitalisations.53–55 Finally, hospitals also require physical spaces, policies and procedures that make it possible to provide optimal care. 46 The Autistic SPACE Framework 45 identifies five elements necessary to meet the needs of autistic patients in healthcare settings: sensory needs, predictability, acceptance, communication, and empathy.
In addition to considering how to reduce LOS and transition patients out of hospital, it is also important to focus on upstream prevention. Long-stay patients with and without IDD both had high levels of healthcare utilisation prior to admission. This suggests that many of these individuals are known within the health system and there may be opportunities to enhance community supports and avoid long stay admissions. Work in Canada and elsewhere has shown that individuals with IDD can end up hospitalised when they have inadequate supports to meet their needs outside of hospital.56–58 Adequate appropriate outpatient mental health services, primary care, developmental services housing, community programmes, and family supports may circumvent admissions in some cases.
Limitations
There are several study limitations that should be acknowledged. We know from previous work 59 that not all patients with IDD are identified in the health data and it is possible that this study has undercounted the proportion of patients with IDD. Additionally, it can be difficult to accurately diagnose psychiatric disorders in people with IDD43,44 so some of the psychiatric diagnoses recorded may not be accurate. This project only included patients in designated psychiatric beds. There are also patients with psychiatric disorders with long-stay admissions in non-psychiatric beds who were not included in these data. It was not possible within our dataset to accurately identify what proportion of long-stay inpatients were designated as ALC as that information is held in a separate and unlinked dataset. This study focused on describing long-stay patients on one day, in one province; it is possible the profile of long-stay patients may differ at different points in time or in different jurisdictions.
Conclusion
This study found that people with IDD accounted for more than one in five patients who had been in a psychiatric inpatient bed in Ontario for over a year. They had unique characteristics, including higher rates of cognitive impairment, difficulty with activities of daily living, limited social support networks, difficulty caring for themselves and difficulty self-managing their aggression. Specialised supports within hospitals and in the community are required to reduce LOS and facilitate successful transitions out of hospital for this patient population. There is an urgent need to build this capacity within the inpatient and outpatient mental health sectors.
Supplemental Material
sj-pdf-1-cpa-10.1177_07067437251380731 - Supplemental material for Long-Stay Psychiatric Inpatients With and Without Intellectual and Developmental Disabilities: An Ontario Population-Based Study: Patients hospitalisés pour de longs séjours en psychiatrie avec ou sans déficiences intellectuelles et développementales,: Une étude fondée sur la population de l’Ontario
Supplemental material, sj-pdf-1-cpa-10.1177_07067437251380731 for Long-Stay Psychiatric Inpatients With and Without Intellectual and Developmental Disabilities: An Ontario Population-Based Study: Patients hospitalisés pour de longs séjours en psychiatrie avec ou sans déficiences intellectuelles et développementales,: Une étude fondée sur la population de l’Ontario by Avra Selick, Michael A. Campitelli, Anjie Huang, Robert Balogh, Paul Kurdyak and Yona Lunsky in The Canadian Journal of Psychiatry
Supplemental Material
sj-docx-2-cpa-10.1177_07067437251380731 - Supplemental material for Long-Stay Psychiatric Inpatients With and Without Intellectual and Developmental Disabilities: An Ontario Population-Based Study: Patients hospitalisés pour de longs séjours en psychiatrie avec ou sans déficiences intellectuelles et développementales,: Une étude fondée sur la population de l’Ontario
Supplemental material, sj-docx-2-cpa-10.1177_07067437251380731 for Long-Stay Psychiatric Inpatients With and Without Intellectual and Developmental Disabilities: An Ontario Population-Based Study: Patients hospitalisés pour de longs séjours en psychiatrie avec ou sans déficiences intellectuelles et développementales,: Une étude fondée sur la population de l’Ontario by Avra Selick, Michael A. Campitelli, Anjie Huang, Robert Balogh, Paul Kurdyak and Yona Lunsky in The Canadian Journal of Psychiatry
Supplemental Material
sj-docx-3-cpa-10.1177_07067437251380731 - Supplemental material for Long-Stay Psychiatric Inpatients With and Without Intellectual and Developmental Disabilities: An Ontario Population-Based Study: Patients hospitalisés pour de longs séjours en psychiatrie avec ou sans déficiences intellectuelles et développementales,: Une étude fondée sur la population de l’Ontario
Supplemental material, sj-docx-3-cpa-10.1177_07067437251380731 for Long-Stay Psychiatric Inpatients With and Without Intellectual and Developmental Disabilities: An Ontario Population-Based Study: Patients hospitalisés pour de longs séjours en psychiatrie avec ou sans déficiences intellectuelles et développementales,: Une étude fondée sur la population de l’Ontario by Avra Selick, Michael A. Campitelli, Anjie Huang, Robert Balogh, Paul Kurdyak and Yona Lunsky in The Canadian Journal of Psychiatry
Footnotes
Acknowledgements
This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health (MOH) Postal Code Conversion File, which contains data copied under licence from ©Canada Post Corporation and Statistics Canada. Parts of this material are based on data and/or information compiled and provided by CIHI and the Ontario MOH. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
Data Access Statement
The dataset from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (e.g., healthcare organisations and government) prohibit ICES from making the dataset publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at ![]() (email: das@ices.on.ca). The full dataset creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programmes may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
(email: das@ices.on.ca). The full dataset creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programmes may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Declaration of Conflicting Interests
The authors do not have any conflicts of interest to declare.
Funding
This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.