
Abstract
Objective:
Antipsychotic use is controversial in the management of adults with intellectual and developmental disabilities (IDD) because of inconclusive evidence for efficacy in the absence of a comorbid psychiatric condition, and substantial concerns about adverse effects. We aimed to characterize antipsychotic use among Ontario adults with IDD and compare profiles of those with and without a documented psychiatric diagnosis.
Method:
This population-based study included 51,881 adults with IDD under 65 y as of April 2010 receiving provincial drug benefits in Ontario who were followed until March 2016 to identify those dispensed at least one antipsychotic medication. Profiles of those with and without a psychiatric diagnosis were compared.
Results:
Overall, 39.2% of adults (n = 20,316) were dispensed an antipsychotic medication, which increased to 56.4% in a subcohort residing in group homes. Almost one-third (28.91%) of people prescribed an antipsychotic medication did not have a documented psychiatric diagnosis. Those without a psychiatric diagnosis differed considerably from those with a diagnosis. In particular, those without a psychiatric diagnosis were older, less likely to have used antidepressants or benzodiazepines in the year before, and less likely to have used ambulatory and acute care.
Conclusions:
Antipsychotic use in IDD is common, and occurs frequently without a psychiatric diagnosis. Attention toward how antipsychotics are prescribed and monitored for people with IDD in Canada is warranted to ensure appropriate prescribing.
The increased and sometimes inappropriate use of antipsychotic medication has been identified as problematic in children, youth, and older adults in Canada, 1 –3 and internationally. 4 Here and elsewhere, policies, monitoring, and education efforts have mainly targeted the use of antipsychotics to manage behavioural and psychological symptoms of dementia in older adults, with good results. 5 –9 In contrast, less attention has been paid to an equally vulnerable group of individuals: adults with intellectual and developmental disabilities (IDD). Both psychiatric disorders 10 and challenging behaviours 11 are common in this population. Data, mostly from the UK 12 –15 but also population-based evidence from The Netherlands, 16 Australia, 17 Norway, 18 and the US, 19 show that antipsychotics are frequently prescribed to treat either or both of these presentations together in adults with IDD. 20 Unfortunately, as it pertains to challenging behaviours in particular, studies on long-term effectiveness are absent, and evidence for their use in the short term remains inconclusive. 21 –25 In addition, antipsychotics are associated with a very high burden of adverse effects, particularly an increased risk for metabolic complications. 15,26 Adults with IDD have difficulties in providing informed consent to medication treatment and in reporting adverse effects, which are compounded by impairments in communication, cognition and memory, and frequent medical comorbidities. 20 As such, careful attention to appropriate use of antipsychotic medications in this population is warranted.
Several practice guidelines have been published 20,27 –30 to guide clinicians regarding the use of antipsychotic medications for adults with IDD for psychiatric and/or significant behaviour concerns. The recently published National Institutes for Clinical Excellence (NICE) guidance specifies that antipsychotic medication for behaviour should only be considered if psychological or other interventions alone do not produce change within an agreed amount of time, or treatment for any coexisting mental or physical health problem has not led to a reduction in the behaviour, or the risk to the person or others is very severe. Furthermore, antipsychotic medication should only be offered in combination with psychological or other interventions. 27
In 2015, in response to mounting evidence on the overuse of psychotropic medications in the IDD population in the UK, particularly antipsychotics, the National Health Service (NHS) issued a ‘call to action’ to improve its prescribing practices. This was followed by a pledge by the Royal College of Psychiatrists, together with 4 other professional bodies, to ‘stop over prescribing of medications for persons with learning disability [IDD]’ - StompLD. 31 In contrast, there has been limited dialogue on how to tackle this issue within the psychiatry community in Canada. One reason for this silence may be the absence of population data on the extent of antipsychotic use by those with IDD here. As suggested by Glover et al. 32 in their British Journal of Psychiatry commentary in 2014, the first step toward changing this practice is documentation of the extent of the problem.
This study aimed to describe rates of antipsychotics use in a Canadian cohort of adults with IDD, and to explore the demographic and clinical profiles of these individuals. We were additionally interested in demographic and clinical differences between those dispensed antipsychotic medication with and without a documented psychiatric diagnosis.
Methods
We conducted a population-based cohort study as part of the Health Care Access Research and Developmental Disabilities (H-CARDD) Program. Through the H-CARDD Program, we worked jointly with the government to assemble a cohort of 66,484 Ontario adults aged 18 to 64 y as of April 1, 2009 with a diagnosis of IDD. This was created by linking diagnostic information from provincial health and social services data. 33,34 IDD was identified based on the presence of IDD diagnostic codes in 2 or more physician claims, or one hospital claim since database inception (1991 for physician billing and 1988 for hospital claims), or based on IDD being recorded as a diagnosis relevant to eligibility for disability benefits from a social services database. IDD diagnostic codes were consistent with recent Ontario legislation, and include terms such as mental retardation / intellectual disability, as well as autism and other pervasive developmental disorders, foetal alcohol syndrome, and various chromosomal disorders. All individuals who were eligible for public drug benefits and alive on April 1, 2010 (N = 51,881), were followed for 6 y from April 1, 2010 to March 31, 2016 to determine antipsychotic medication exposure. A subcohort of 7,219 adults living in group-home settings was also identified, based on information from the social service records about current residential setting in 2009. The index date for each individual was defined as the date of first antipsychotic prescription over our study period.
Data Sources
We used the Ontario Drug Benefit (ODB) claims database to identify all current and previous prescription medications dispensed from pharmacies, and the medication costs. We used the Canadian Institute for Health Information’s (CIHI) Discharge Abstract Database (DAD), Same Day Surgery (SDS), National Ambulatory Care Reporting System (NACRS), and Ontario Mental Health Reporting System (OMHRS) to identify all psychiatric diagnoses and procedures from inpatient hospitalisations, emergency department visits, and mental health hospitalisations, respectively. We used the Ontario Diabetes Database and the Ontario Hypertension Database—2 validated databases constructed at the Institute for Clinical Evaluative Sciences (ICES) 35,36 —to determine previous diagnoses with diabetes and hypertension, respectively. We used the Ontario Health Insurance Program (OHIP) claims database to identify all psychiatric diagnoses from visits to primary care physicians and all specialist visits, and the Registered Persons Database to determine patient demographic and vital statistics. These datasets were linked using unique, encoded identifiers, were analysed at ICES (www.ices.on.ca), and are used regularly to assess the impact of policies in the Ontario healthcare system. ICES is a prescribed entity under Ontario’s Personal Health Information Protection Act and, as such, is authorised to collect and use personal health information from health care organisations without consent. This study was approved by the research ethics board of Sunnybrook Health Sciences Centre, Toronto.
Psychiatric Diagnosis Exposure
Psychiatric diagnosis was defined as having either a major mental illness (schizophrenia, non-schizophrenia psychotic disorder, bipolar disorder or major depressive disorder) or other psychiatric diagnosis (other depressive disorders, anxiety, somatoform, dissociative, psychosomatic, personality disorders, adjustment disorders, disorders of conduct or impulsivity) recorded in the OHIP claims, DAD, SDS, or OHMRS databases in the 2 years before the index date. Validation has been conducted in Ontario to support categorising psychiatric disorders in this way. 37 –39 This allowed us to consider antipsychotic prescriptions for those with a psychiatric indication for the drug (i.e., major mental illness), those with another type of psychiatric diagnosis where there may have been a psychiatric indication for the drug (i.e., other mental illness) and those with no psychiatric diagnosis. This classification aligns with that of the NICE guidance on antipsychotic medication prescribing for adults with IDD. 20
Sociodemographic and Clinical Characteristics
Among those treated with an antipsychotic, we measured demographic characteristics (sex, age, urban residence, neighbourhood income) at the time of antipsychotic prescription (i.e., index date). To further describe the cohort, we measured previous medication use (1 year before index date), comorbidity (Charlson comorbidity index 40 using hospitalisation data from the 3 y before index date), physician services (total number of visits in the previous year and visits to primary care physicians or psychiatrists in the past 90 days before index date), and health service utilisation, including emergency department (ED) visits and hospitalisations (2 years before index date).
Analysis
We determined the prevalence of antipsychotic prescribing among the entire cohort of adults with IDD. Prevalence rates were calculated overall, and within each year of follow-up separately. All analyses were conducted for the entire cohort and among a subcohort of individuals living in group homes. Cohort characteristics were compared between those with and without psychiatric diagnoses using standardised differences. Standardised differences are frequently used in large, population-based studies where P values can be influenced by the large size of the study population. 41,42 In general, standardised differences greater than 0.1 are considered to be meaningful. 41 All analyses were conducted for the entire cohort and among a subcohort of individuals living in group homes. Analyses were conducted using SAS version 9.4 (SAS Institute, Cary, North Carolina).
Results
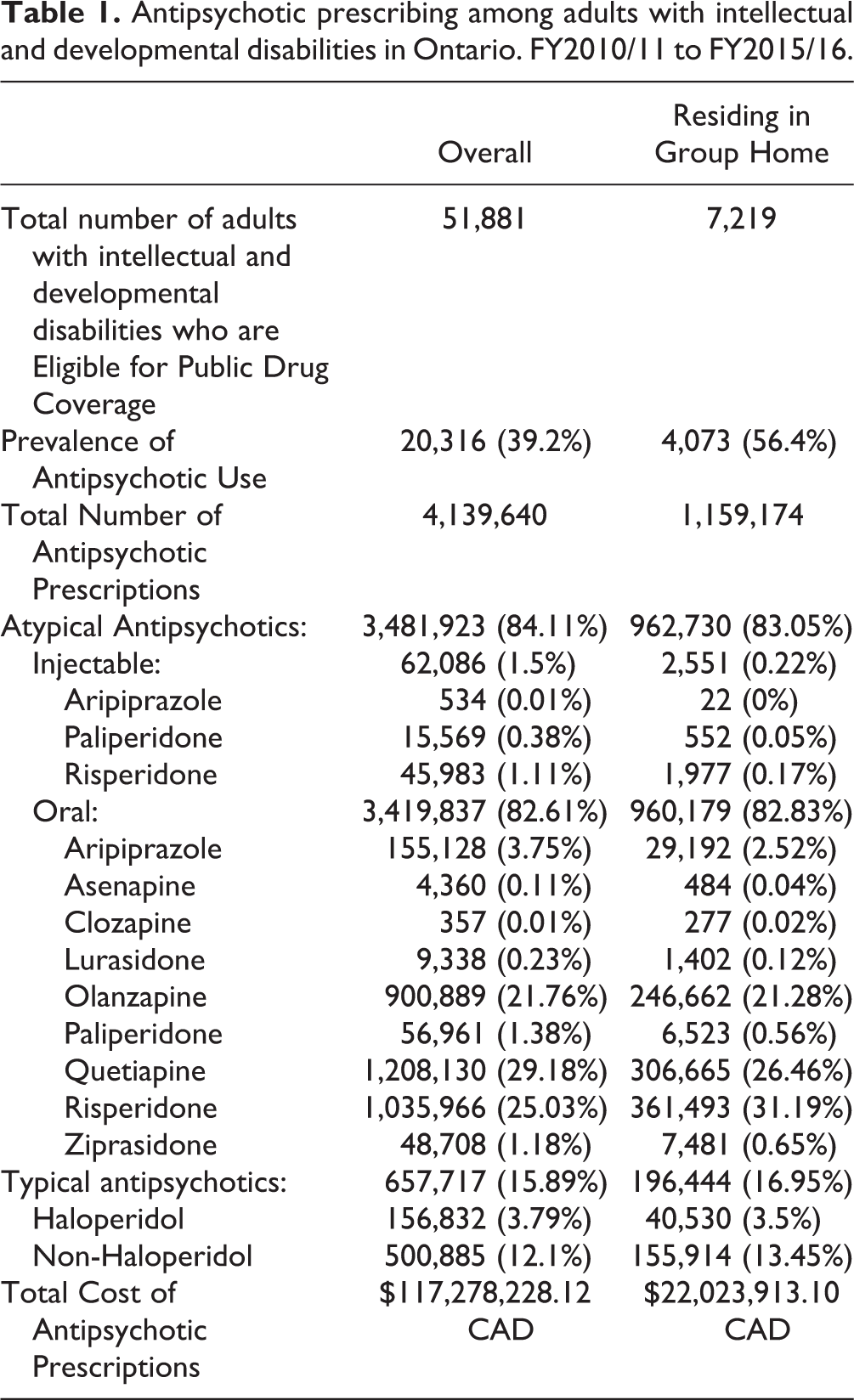
Among the 51,881 adults with IDD eligible for our study, 20,316 (39.2%) were dispensed at least one publicly funded antipsychotic between April 1, 2010 and March 31, 2016. This corresponded to a total cost of more than 117 million Canadian dollars (Table 1). Among adults with IDD residing in a group home, 56.4% (N = 4,073 of 7,219) were dispensed an antipsychotic. Annual prevalence estimates between fiscal year 2010 and 2015 were similar, increasing slightly from 29.1% to 31.2% in the overall population and 48.6% to 51.3% in the group-home residents. Most prescriptions were for atypical antipsychotics (84.1%), with the most commonly dispensed medications being oral quetiapine (29.2%), risperidone (25.0%), and olanzapine (21.8%). This pattern of results was similar for group-home residents, except that risperidone was the medication most commonly dispensed (31.2%) followed by quetiapine (26.5%).
Antipsychotic prescribing among adults with intellectual and developmental disabilities in Ontario. FY2010/11 to FY2015/16.
Antipsychotic users were 42 y of age on average, mostly male (58.8%), and living in an urban location (85.0%; Table 2). These individuals were dispensed a median of 7 drugs (both psychotropic and non-psychotropic) over the preceding year, with antidepressants (48.4%) and benzodiazepines (40.6%) being most common. Almost two-thirds (62.3%) had at least one ED visit in the previous 2 years, and 76.4% had at least one visit with a family physician or psychiatrist in the past 90 days.
Characteristics of adults with intellectual and developmental disabilities who were prescribed antipsychotics between April 2010 and March 2016 by psychiatric diagnosis.*
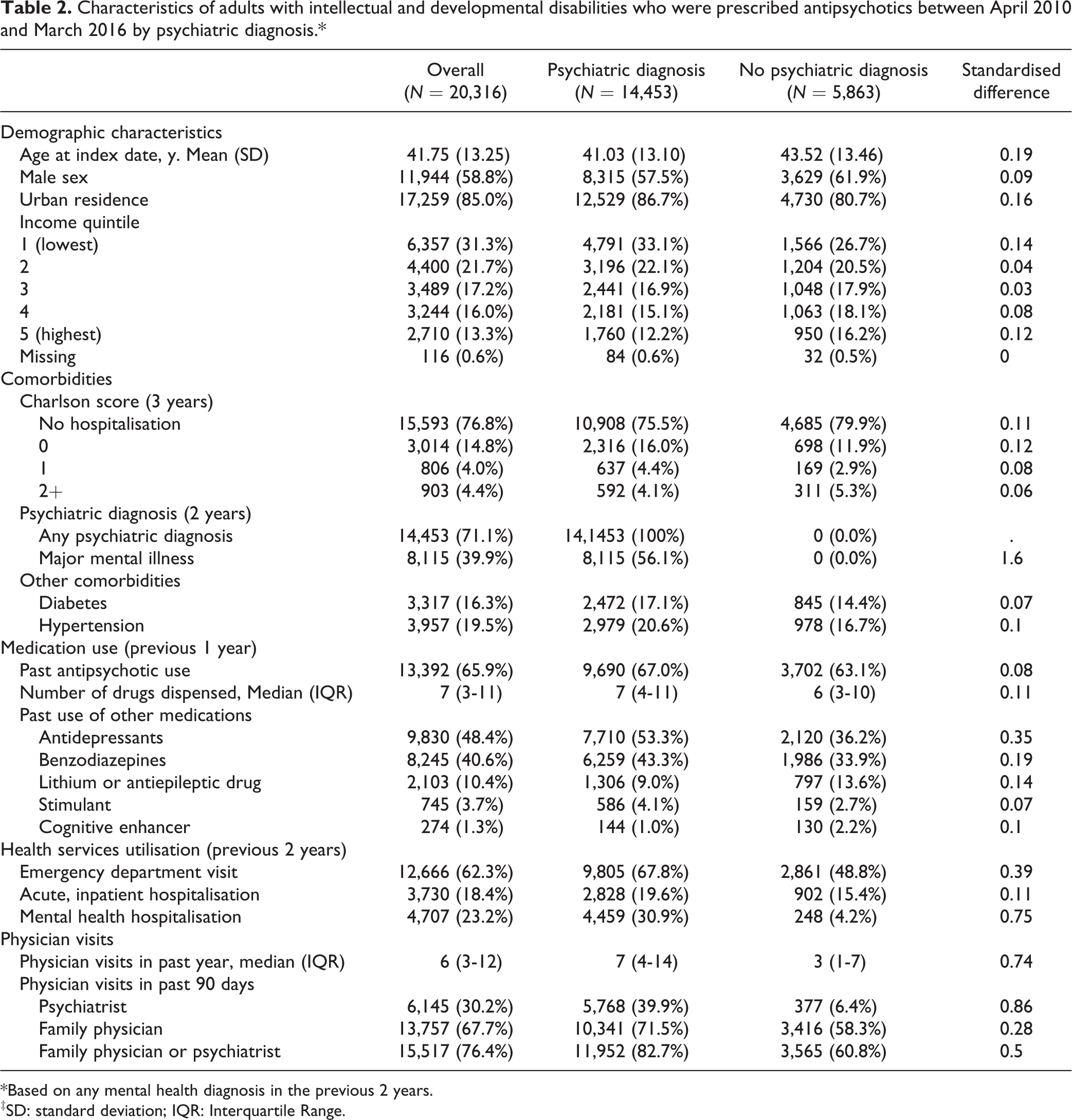
*Based on any mental health diagnosis in the previous 2 years.
‡SD: standard deviation; IQR: Interquartile Range.
Just over two-thirds (71.1%; N = 14,453) of antipsychotic users had a documented psychiatric diagnosis in the 2 years preceding the prescription date; only 39.9% (N = 8,115) had a major mental illness; namely, schizophrenia, bipolar disorder, or major depressive disorder. Compared with those with a psychiatric diagnosis, antipsychotic users without a psychiatric diagnosis tended to be slightly older, of higher socioeconomic status, and were less likely to reside in urban locations. They were less likely to have been prescribed antidepressants or benzodiazepines in the year preceding the antipsychotic prescription but more likely to have been prescribed lithium or an anti-epileptic drug (Table 2). Health service use was more common among those with v. without psychiatric diagnoses (also in Table 2). Specifically, a larger proportion of those with a psychiatric diagnosis had a physician visit within 90 days (82.7%) compared with 60.8% of those without a psychiatric diagnosis.
Sub-Analysis Among Group-Home Residents
The subgroup of 4,073 individuals residing in group homes who were treated with antipsychotics were 45 y of age, and most were men (63.1%; Table 3). Only 57.1% of antipsychotic users in group homes had a psychiatric diagnosis, and only 21.9% had a major mental illness recorded by a physician in the previous 2 years. Differences in medication use, health service utilisation, and comorbidity between antipsychotic users with and without psychiatric diagnoses align with what was reported for the larger group.
Characteristics of adults with intellectual and developmental disabilities residing in Group Homes who were prescribed antipsychotics between April 2010 and March 2016 by psychiatric diagnosis.*
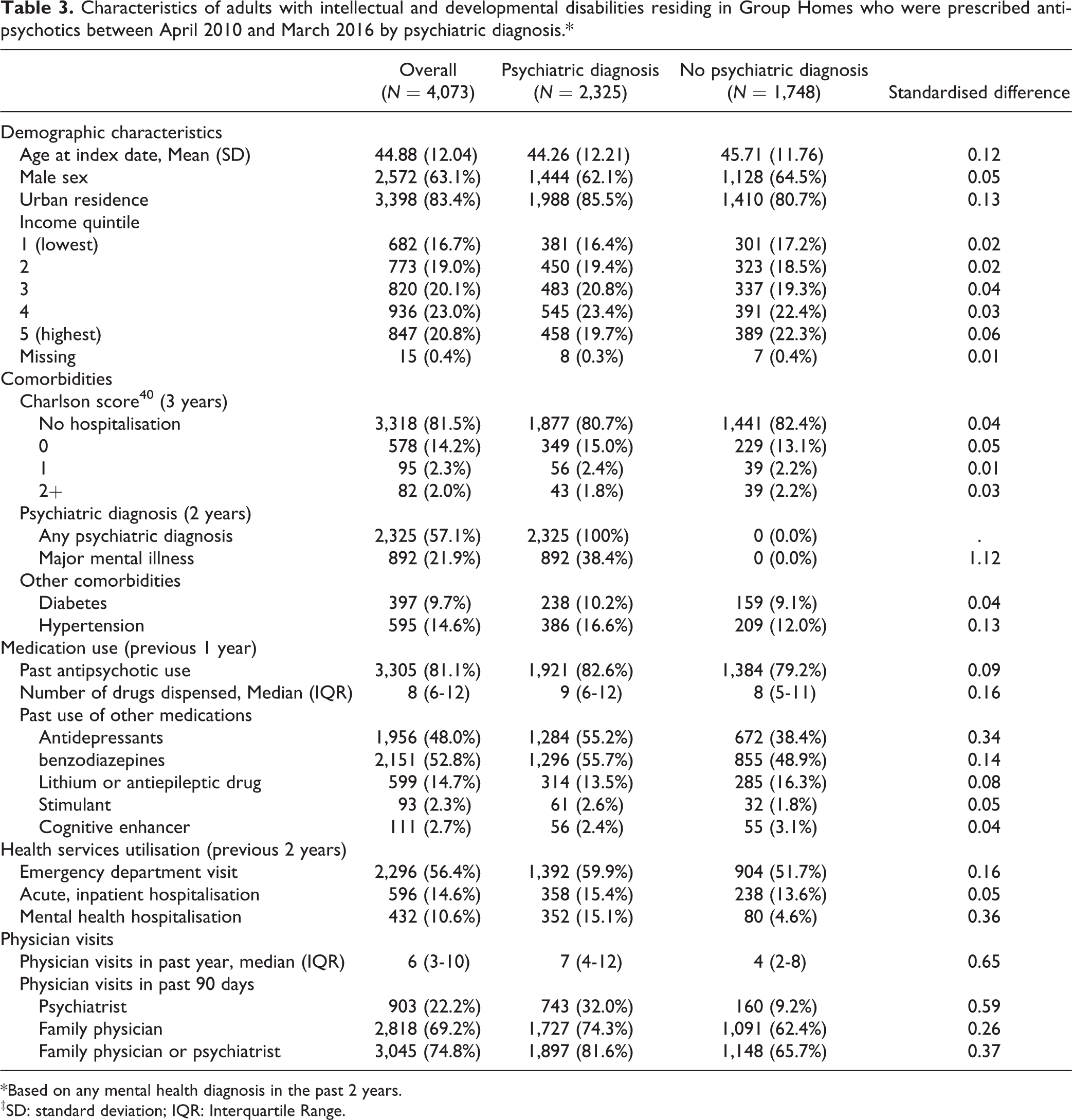
*Based on any mental health diagnosis in the past 2 years.
‡SD: standard deviation; IQR: Interquartile Range.
Discussion
In this large, population-based study, we found that over a 6-y window, 2 in 5 adults with IDD were dispensed an antipsychotic medication. In group homes, the rate was much higher, with more than half of the residents with IDD prescribed an antipsychotic. The costs of this prescribing pattern were significant, with the provincial government spending over 117 million dollars on antipsychotic drugs dispensed to adults with IDD over this 6-year period, equivalent to approximately $19.5 million, annually. Individuals prescribed antipsychotics had a host of medical concerns and were frequent health service users. Many users of these medications did not have a documented psychiatric diagnosis and this subgroup differed from those with a diagnosis both demographically and clinically. Taken together, these findings suggest that future attention to the appropriateness of antipsychotic prescribing for adults with IDD in Ontario is warranted.
The pattern of antipsychotic prescribing reported herein is consistent with what has been described in other jurisdictions where rates of antipsychotic prescribing among adults with IDD can range from 21% to 45%. Several studies have identified that a substantial subgroup of individuals are prescribed these medications without a recent psychiatric diagnosis. 12–13,16 –19 The largest, most comparable study to ours, drawn from The Health Improvement Network (THIN) clinical database of primary care practices across the UK, followed 33,016 adults with IDD. 12 They found that only 29% of those treated with antipsychotics in primary care had a serious mental illness diagnosis recorded in their primary care file, even with an incentive program in place there to encourage the recording of psychiatric diagnoses. This was slightly lower than our study, where closer to 40% of adults had a major mental illness diagnosis; although, our definition of major mental illness also included major depressive disorder (as antipsychotics are also now indicated for this condition), 43 whereas theirs did not. Interestingly, whereas our study reported that 39% of adults were prescribed at least one antipsychotic over 6 y, only 28% of adults in their study were prescribed at least one antipsychotic over 15 y. Furthermore, in contrast to the steady prevalence rate over 6 y described in our study (a total increase of 2%), they noted a 4% decrease in antipsychotics prescriptions each year of their study. The authors suggest that this decrease might illustrate the gradual impact of ongoing research, policy, and practice efforts in the UK to reduce harmful prescribing. 12 In addition to targeted efforts aimed at improving prescribing practices, it is important to recognize that ID psychiatry is a recognised subspecialty in the UK, with 6 months of training as part of the psychiatry residency. In addition, local community-based IDD teams in each region of the UK can deliver non-pharmacological interventions; similar services to those delivered by the NHS are not widely available in Ontario. 44 These findings highlight the benefit of comparing population results across jurisdictions to understand how different policy and practice approaches, including training opportunities, may lead to different patterns of use.
In the current study, over half of the adults known to be living in group homes were dispensed at least one antipsychotic medication in the period studied. Several studies have documented a higher use of antipsychotics by those in residential care settings than those living alone or with family; 19,45,46 although, such studies have generally been based on smaller samples than what is reported here. Rates of diabetes and hypertension were somewhat lower in this subgroup than the entire cohort, suggesting that the formal supports available may assist with chronic disease prevention. Notably, 42.9% of those living in group homes dispensed antipsychotics did not have a recently recorded psychiatric diagnosis, suggesting off-label use in close to half of those dispensed these medications. More research is needed to understand antipsychotic use in residential care. Current practices in group homes may be influenced by system challenges, such as staffing and environmental characteristics, in addition to clinical needs. 47,48 In addition to guidelines and training around antipsychotic prescribing and monitoring for prescribers and pharmacists, targeted efforts on the monitoring of antipsychotic medication use within residential care would be beneficial, especially given the staff knowledge gaps about these medications 49 and the considerable harms associated with this class of drug. 27
With nearly 40% of adults with IDD prescribed antipsychotics, it is important for psychiatrists to consider what is driving this use, and what can be done to ensure that these medications are being prescribed appropriately and safely in this population. One potential driver is the funding mechanism for pharmacologic and non-pharmacologic therapies in Ontario. Adults with IDD can receive medications as part of the Ontario Disability Support Program at no cost to them but not psychological interventions or behaviour therapy. Adults with IDD also experience challenges accessing psychiatric support beyond a single consultation, with very few adult psychiatrists with expertise in IDD in Ontario, and other parts of Canada, 44,50 and limited training in IDD psychiatry in Canadian residency programs. 44,51 Other research from Ontario has demonstrated that the mean annual number of psychiatrist visits is notably lower for those with IDD than the general population. 52 Without expertise in IDD, prescribers can misdiagnose distress due to physical pain or adjustment disorder as a more severe psychiatric diagnosis and prescribe antipsychotics. 44 Further research is required to fully understand the multiple factors contributing to antipsychotic prescribing in our country, which could inform proposed interventions.
This study has several strengths, including its use of linked population-based databases that allow us to study prescribing practices in a large cohort of adults with IDD that is not limited to those individuals receiving IDD services or to individuals accessing health services through a primary care setting. There are, however, several key limitations that merit emphasis. First, we could not measure the effectiveness of the antipsychotics prescribed or the degree of medication monitoring by physicians. Further, although the high number of medications dispensed to patients in our cohort is suggestive of significant polypharmacy, we do not know which medications were continued with the antipsychotic and for what duration. Second, we are unable to determine whether the individuals without a psychiatric diagnosis were prescribed antipsychotics to treat challenging behaviour, as was done through chart audit by Sheehan et al. 12 Although our definition of psychiatric diagnoses is broad, requiring a single diagnosis in a 2-y period, and has been used in similar studies in the past, 26,33 it is possible that we misclassified some individuals whose psychiatric diagnosis was not captured in billing data during the time period studied. However, given that most individuals with a psychiatric diagnosis should have had some physician contact over 2 y, it is unlikely that this is greatly influencing our study. Although the psychiatric diagnosis definitions have not been specifically validated in IDD, we believe that the administrative health information is a reasonable diagnostic proxy. Third, our study focused on a cohort aged 18 to 64 y in 2009, and so findings may not be generalizable to older adults or to youth with IDD. Furthermore, residential placement in group homes was determined in 2009, and we were unable to identify whether people’s living arrangements changed over the course of our study period. However, residence in group homes in Ontario is relatively stable, and therefore we believe that this would have little impact on our findings. Fourth, the specificity of diagnostic coding in our cohort did not allow us to further subcategorize our cohort into those with different types of developmental disabilities, or by disability severity. Finally, our data sources did not allow us to examine the role of non-pharmacological interventions within this population, either before antipsychotic prescribing or concurrently.
Conclusions
The high use of antipsychotics reported in the current study, particularly the large proportion that are being prescribed in the absence of a psychiatric diagnosis, raises some concern about the potential for inappropriate antipsychotic prescribing for adults with IDD in Canada. Future research and policy in Canada should focus on the extent to which antipsychotics are being appropriately prescribed in this highly vulnerable population, including using chart audits and other feedback mechanisms. There is also a need for more thorough research on the risks and benefits of the use of antipsychotics over the long term. Experts within psychiatry, pharmacy, and policy from across jurisdictions can work together to ensure that the use of antipsychotics aligns with clinical guidelines and adults with intellectual and developmental disabilities receive optimal health care.
Footnotes
Acknowledgments
We gratefully acknowledge the Province of Ontario for their support of this study through their research grants program. We thank IMS Brogan Inc for use of their Drug Information Database. Parts of this material are based on data and information compiled and provided by CIHI. However, the analyses, conclusions, opinions and statements expressed herein are those of the author, and not necessarily those of CIHI.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was also supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario MOHLTC. The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or the province is intended or should be inferred.