
Abstract
Objective:
Bipolar disorder (BD) often goes unrecognized and untreated for several years leading to serious consequences. We have recently developed a manualized telehealth-based group psychoeducational and resilience enhancement program for individuals at high risk for bipolar disorder (PREP-BD). The primary objective of this study was to assess the feasibility of implementing PREP-BD to enhance help-seeking intentions among high-risk individuals.
Method:
The intervention consisted of eight weekly, 60-minute group psychoeducation sessions conducted via Zoom. Participants (N = 21), aged 17 to 24 years, who met the bipolar at-risk criteria, were assigned to one of four cohorts. Primary outcomes for this feasibility trial included sign-up rate, completion rate, and acceptability as measured by the Client Satisfaction Questionnaire (CSQ-8). Preliminary efficacy was assessed using validated measures of help-seeking intentions, resilience, quality of life, and stigma, with pre- and post-intervention comparisons.
Results:
Our findings indicate excellent feasibility as evidenced by timely recruitment, 100% sign-up rate, and 76.19% completion rate (defined as attending at least 75% of group sessions). The intervention showed preliminary improvements in help-seeking intentions, particularly for a hypomanic scenario. Quality of life also demonstrated significant improvement, while resilience and self-stigma showed non-significant trends toward improvement.
Conclusion:
Our findings suggest the feasibility of implementing psychoeducation as an early identification strategy in individuals at risk for BD. Future randomized controlled trials are needed to investigate the effectiveness of PREP-BD.
Introduction
Bipolar disorder (BD) is a potentially debilitating and highly heritable psychiatric condition that typically emerges during adolescence and early adulthood 1 and is associated with significant cognitive impairment, 2 brain tissue loss,3,4 and functional disability, 5 which are manifested even during the early stages of the illness. Despite availability of effective treatments, it is now well-recognized that BD tends to go undiagnosed and therefore untreated for several years.6,7 For instance, in a multicenter Canadian study, the median delay between the first mood episode and the accurate diagnosis of BD was found to be 5 years for the adult-onset and 15 years for the pediatric-onset group. 7 These findings align with a published meta-analysis that found the median delay in diagnosis of BD across 20 different studies to be 6.7 years. 8 Such prolonged delay in diagnosis and treatment is associated with a range of negative outcomes 9 including greater severity and frequency of mood episodes, 10 higher number of hospitalizations, 11 higher number of comorbidities including substance use disorders,12,13 and elevated risk of suicide12,14,15 as well as significantly higher healthcare costs. 16
The underlying factors leading to delays in diagnosing BD are intricate and can include a multitude of illness-, patient- and provider/healthcare system-factors. 17 Among these factors are limited awareness of early symptoms of BD among affected individuals and their families, along with challenges in symptom appraisal such as misattribution of those symptoms to normative developmental changes or personality traits, or external influences such as life stressors or substance use. 18 In addition, internalized negative beliefs about mental illness (i.e., self-stigmatization) can discourage individuals from seeking help, even when they recognize the need for intervention. 19 These challenges underscore the need for targeted interventions for individuals at high risk for developing BD aimed at raising awareness, resiliency building including development of coping strategies, emphasizing the importance of biorhythms, providing accurate information about BD, and reducing stigma in order to facilitate early help-seeking. Additionally, young people with BD have expressed interest in learning about self-management and receiving credible, stigma-free information, 20 highlighting the importance of integrating these elements into early intervention strategies.
Psychoeducation has shown promise as an intervention to enhance mental health literacy and promote early help-seeking among adolescents and young adults.21,22 By focusing on increasing awareness of mental health signs and symptoms and addressing stigma, psychoeducational interventions can empower individuals to seek help when needed. Psychoeducation is also among the most well-studied psychosocial interventions for BD 23 and has been shown to reduce recurrence rates, potentially by increasing knowledge and acceptance of a BD diagnosis and its treatment, enhancing the ability to detect and respond to potentially problematic mood changes, and fostering proactive management of the disorder. 24 Psychoeducation has also been shown to reduce internalized stigmatization in individuals with BD. 25
While psychoeducational programs exist for various mental health conditions, none specifically address the unique needs of individuals at high risk for developing BD, despite evidence of their potential benefits and favorable benefit–risk ratio in this population.26,27 A tailored psychoeducational program could be highly beneficial for individuals at high risk for BD since general mental health programs do not necessarily address critical issues unique to this population. For instance, antidepressant monotherapy, which is often recommended as first-line pharmacotherapy in adolescents and adults with moderate to severe depressive28,29 and anxiety disorders30,31 can trigger hypomania or mania in those at risk for BD. Furthermore, hypomanic symptoms tend to be underreported or misrecognized,17,32 making early identification of BD particularly challenging. A psychoeducational program tailored to this population can provide accurate information on risk factors and the early warning signs of BD while offering strategies for symptom management and building resilience. In addition, through emphasizing the importance of early access to care, reducing stigma, and fostering help-seeking behaviors, such specialized psychoeducational program can potentially lead to earlier identification of BD and enhanced long-term outcomes. To fill this gap, we have developed a manualized telehealth-based group psychoeducational and resilience enhancement program for individuals at high risk for BD (PREP-BD), based on the “Psychoeducation Manual for Bipolar Disorder” by Colom and Vieta. 33 To identify individuals at heightened risk for incidence of BD, we recruited youth that met the validated bipolar at-risk (BAR) criteria. 34 These criteria are based on the presence of subsyndromal symptoms with or without family history of BD. Prospective cohort studies using BAR criteria have shown a 10% to 23% incidence rate of conversion to BD in the first 1 to 2 years34,35 and a 29% incidence rate over 11 years of follow-up. 36 This article describes the development of PREP-BD and evaluation of its feasibility, acceptability, and preliminary efficacy in improving help-seeking intentions, enhancing resilience and quality of life, and reducing self-stigmatization among adolescents and young adults at risk for BD.
Methods
Study Design
This prospective single-arm trial was conducted at the University of British Columbia (UBC) Mood Disorders Center. The trial was approved by the UBC Clinical Research Ethics Board (H22-01060).
Participants
Participant recruitment began on June 11, 2023, and was completed on February 2, 2024. Individuals at risk for BD were recruited through online advertisements placed on social media including Reddit and Twitter (now called X), a health research study platform (REACH BC), the Collaborative RESearch Team to study psychosocial issues in Bipolar Disorder (CREST.BD) and the Vancouver Coastal Health Research Institute (VCHRI) websites. Study advertisements were also displayed in the UBC Mood Disorders Clinic and a local youth and young adult clinic (Foundry Centre). The advertisements included a brief description of the intervention as well as the inclusion and exclusion criteria for participation in the study. Interested individuals completed a phone screen by a research assistant to assess basic eligibility and those who were deemed suitable underwent a structured diagnostic interview using either the Mini-International Neuropsychiatric Interview (MINI) 37 or the Mini-International Neuropsychiatric Interview for Children and Adolescents (MINI-KID), 38 the Montgomery–Åsberg Depression Rating Scale (MADRS), the Young Mania Rating Scale (YMRS), as well as an unstructured clinical interview. All interviews were performed by a psychiatrist specialized in assessment and treatment of youth with BD (KK). Participants were compensated approximately 20 CAD per hour for their participation.
Participants were required to reside in the Metro Vancouver area, be able to understand and communicate in English and fulfill the BAR criteria, a BD risk prediction tool developed and validated by Bechdolf et al. 34 To meet the BAR criteria, the individual must be between 15 and 24 years old and fulfill the criteria for at least one of the following three groups within the last 12 months: Group 1, Subthreshold Mania; Group 2, Depression plus Cyclothymic Features: Depression; Group 3. Depression plus Genetic Risk (see Supplemental Table S1 for definitions). Exclusion criteria included: (a) participants with a history of treated or untreated manic/hypomanic episodes of 4 days or longer; (b) participants with a YMRS score of ≥12; (c) those with a history of treated or untreated psychosis of 7 days or longer; (d) participants with an active alcohol or substance use related disorder within the past 3 months; (e) participants with severe depression as measured by MADRS score of ≥35.
Intervention
We prepared the first draft of the PREP-BD manual based on the “Psychoeducation Manual for Bipolar Disorder” by Colom and Vieta which is a well-researched program for individuals with established BD. 39 The adaptability of this manual to the new target population (i.e., young individuals who are at high risk of developing BD) was discussed with one of the co-authors of the original psychoeducation manual (EV) who supported the adaptation and provided guidance throughout the process. The first draft of the manual was prepared by the first author (KK) and was reviewed and edited by another member of the research team (EM). For each session, both the content and procedures were examined for suitability. Modifications made to the original manual included a) incorporating materials tailored towards high-risk individuals; (b) updating the content based on recent research findings; and (c) adapting the manual for telehealth delivery. The manual was also reviewed by the CREST.BD Community Advisory Group, a 14-member group of individuals with BD, and their suggestions were incorporated into the current version of the manual.
The final intervention comprises of 8 weekly, 60-minute group sessions conducted via Zoom. Family members of BAR youth were also invited to join for the screening session and final psychoeducation session. All participants joined the sessions by entering the webinar ID and password. To ensure participants’ anonymity and privacy, they were provided with an option to join the sessions using an alias user ID. Intervention material was presented through PowerPoint slides through Zoom's Share Screen function and participants were able to ask questions and share their experiences during the sessions.
The treatment outline is as follows: Session 1: Group formation; Session 2: What is bipolar disorder?; Session 3: Mania and hypomania; Session 4: Depression and suicide; Session 5: Resilience building and stress management; Session 6: Treatment of bipolar disorder; Session 7: Substance use; Session 8: Closure. Each session of the treatment manual contains specific tasks and step-by-step procedures for the facilitators, as well as a handout for participants. Session 8 contains an additional information handout for families (see Supplemental Table S2 for details).
Participants were assigned to one of four cohorts consisting of 4 to 6 participants. The program was delivered by 4 facilitators (one facilitator for each cohort). Two facilitators were licensed psychiatrists (JJN and CWR), one was a senior psychiatry resident (AL) and one was a registered social worker (AF). All facilitators had experience in working with adolescents and young adults with mood disorders and conducting psychoeducation groups. All facilitators met with the study's Primary Investigator (KK) for a training session prior to the intervention. They were also provided with the lesson plans and PowerPoint slides prior to each session. During the intervention, facilitators had access to the study's Primary Investigator for ongoing support, including the ability to ask questions and engage in problem-solving as needed. The first psychoeducation session for the first cohort took place on September 3rd, 2023, and the final session for the fourth and final cohort took place on April 30th, 2024.
Measures
Primary outcomes for this feasibility trial included sign-up rate, completion rate (defined as the proportion of participants who attended at least 75% of group sessions), and acceptability as measured by the Client Satisfaction Questionnaire (CSQ-8) 40 completed by participants at the end of the intervention. The CSQ-8 is a validated tool consisting of 8 items designed to measure overall satisfaction with services or interventions. Each item is rated on a 4-point scale, with scores ranging from 1 to 4. To determine acceptability, we established an a priori threshold score of 20, which corresponds to the median score on the CSQ-8.41,42
Preliminary efficacy was assessed using the following questionnaires completed by participants pre- and post-intervention. (a) Help-seeking intentions were measured by a modified version of the General Help-Seeking Questionnaire-vignette (GHSQ-V) 43 that provided participants with two hypothetical vignettes, one describing a hypomanic episode and the other describing a depressive episode (see Supplementary Materials, Appendix A), and asked them to rate on a 7-point Likert Scale the likelihood they would seek help from a variety of sources (including a friend, a family member, their family doctor, and a mental healthcare professional) or the likelihood that they would not seek help from anyone. A total help-seeking intention (HSI) score ranging from 5 to 35 was calculated as the sum of likelihood to seek help from the 4 different sources and a reverse coding of responses to the item “I would not seek help from anyone”, similar to previous scoring of this scale.44,45 (b) Self-stigmatization was measured by the Self-Stigma of Mental Illness Scale-Short Form (SSMIS-SF), a 20-item self-report Likert scale that has been designed and validated to measure internalized stigma in individuals living with mental illnesses including BD. 46 (c) Self-perceived resilience was evaluated by the Connor-Davidson Resilience scale (CD-RISC), a 25-item self-report Likert scale designed to evaluate various aspects of resilience including the ability of an individual to cope with stress and adversity. 47 (d) Quality of life was assessed using the Quality of Life in Bipolar Disorder (QoL.BD), a 56-item scale validated tool to measure subjective quality of life in individuals living with BD. 48
Statistical Analyses
Baseline characteristics and feasibility metrics were calculated through means with standard deviations and percentages. Primary outcomes and efficacy measures were evaluated primarily using intention-to-treat analyses, though completer-only analyses are also reported. Significance was set at α = 0.05 for paired two-tailed t-tests with Holm–Sidak correction for multiple comparisons of similar constructs (i.e., responses to the individual GHSQ-V questions). Our sample size was insufficient to provide well-powered covariate analysis. A priori power calculations could not be completed for this proof-of-concept feasibility study, though Cohen's d effect sizes are reported to inform future studies and power calculations.
Results
Participants Characteristics and Feasibility Metrics
A total of 85 individuals expressed interest and completed a phone screening over an 8-month recruitment period. Of those, 39 completed the screening session by a psychiatrist, and 21 (15 female, 4 male, and 2 non-binary, mean age: 19.95 years, SD: 2.04) were deemed eligible based on the study's inclusion and exclusion criteria. The recruitment flowchart is outlined in Figure 1, and demographic and clinical characteristics of study participants are presented in Table 1. All 21 eligible participants consented to participate in the study (100% sign-up rate). Six participants invited their family members to attend the final intervention session, in accordance with the study protocol. The recruitment happened in less than 8 months with a recruitment rate of over 2.6 participant per month. Sixteen participants (76.19%) were completers, defined as those who participated in at least 75% of the program (6 out of 8 sessions) while 5 participants (23.81%) were non-completers. All 21 participants completed the post-intervention questionnaires. The mean score for CSQ-8 stands at 22.2 (scores above 20 are considered acceptable).
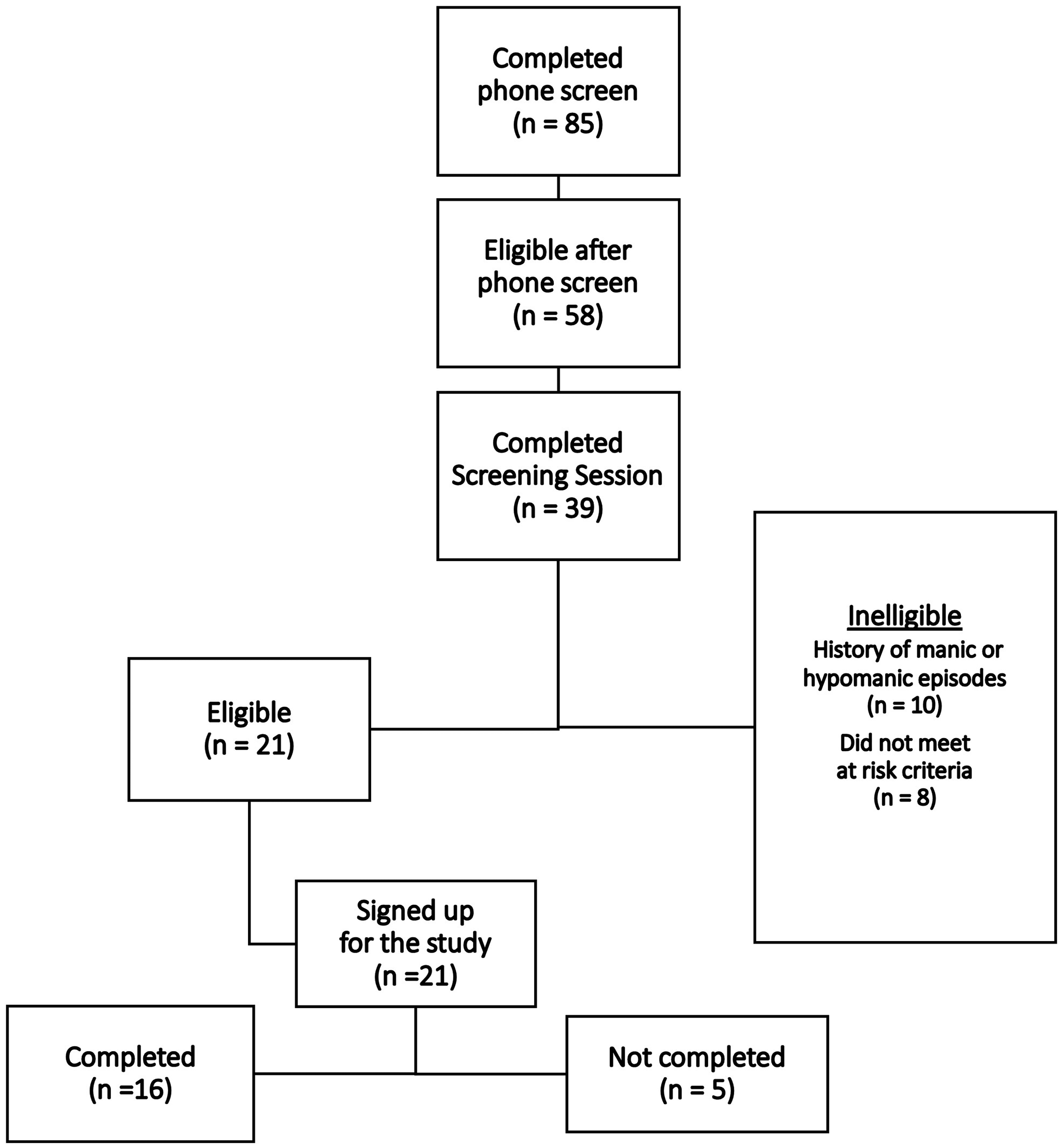
Study recruitment flowchart.
Demographic and Clinical Characteristics of Study Participants.
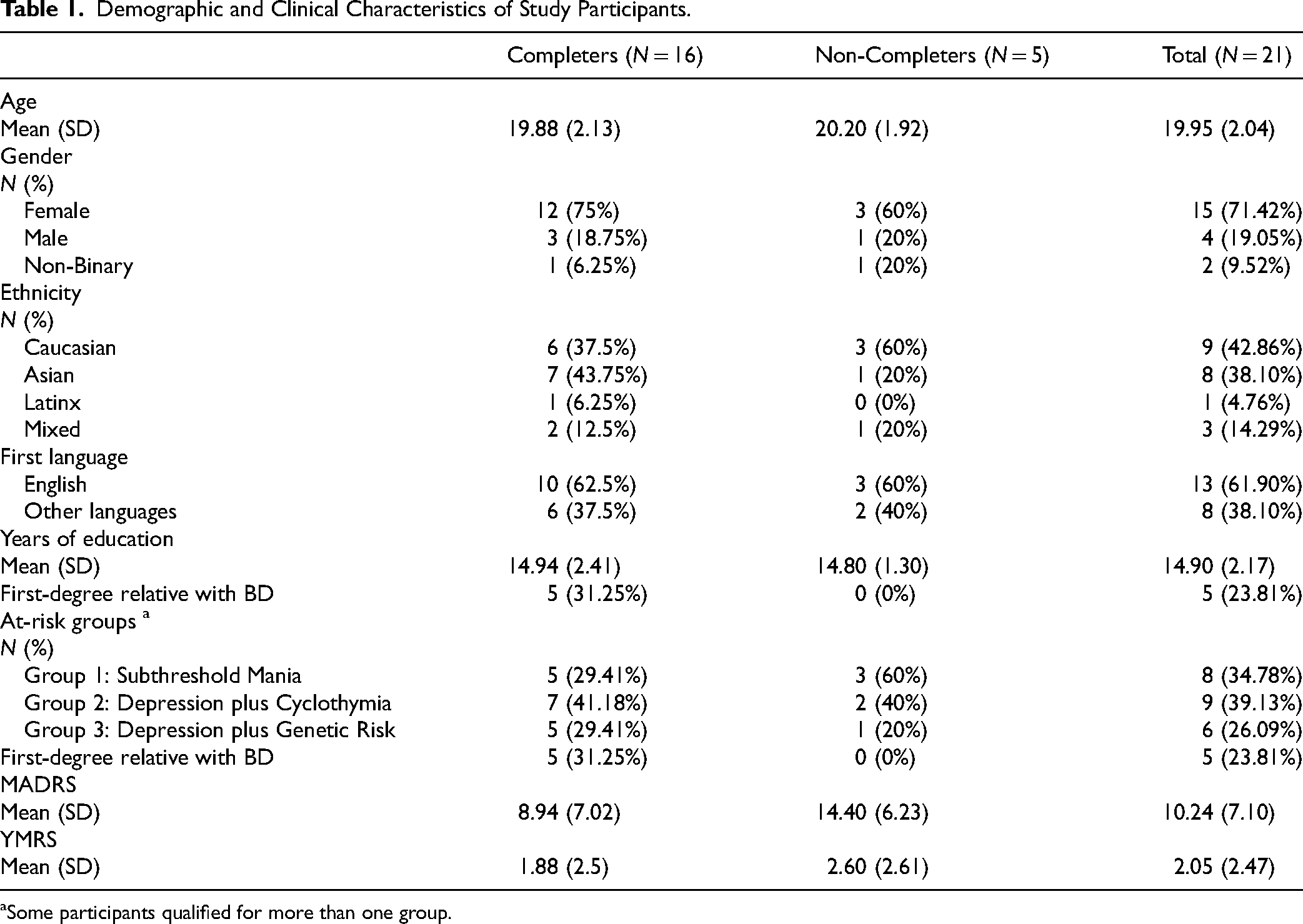
Some participants qualified for more than one group.
Preliminary Efficacy
The psychoeducation group improved HSI scores, predominantly in response to a vignette describing hypomania. HSIs for a scenario describing a depressive episode did not change significantly per intention-to-treat analysis (Figure 2), though the total score did increase significantly for completers-only (p = 0.02, t = 2.686, df = 15, d = 0.67; Supplementary Figure S1). There was no significant change in any of the individual help-seeking items with either intention-to-treat or completers-only analysis. Total HSIs for a scenario describing a hypomanic episode did increase both in the intention-to-treat analysis (p = 0.003, t = 3.449, df = 20, d = 0.75; Figure 3A) and for completers-only (p = 0.0003, t = 4.621, df = 15, d = 1.15; Supplemental Figure S2A). There was improvement in response to 4 of the 5 individual help-seeking items per intention-to-treat analysis (p < 0.03; Figure S3B), while there was improvement with each of the individual help-seeking items for completers-only (p < 0.02; Supplemental Figure S2B).
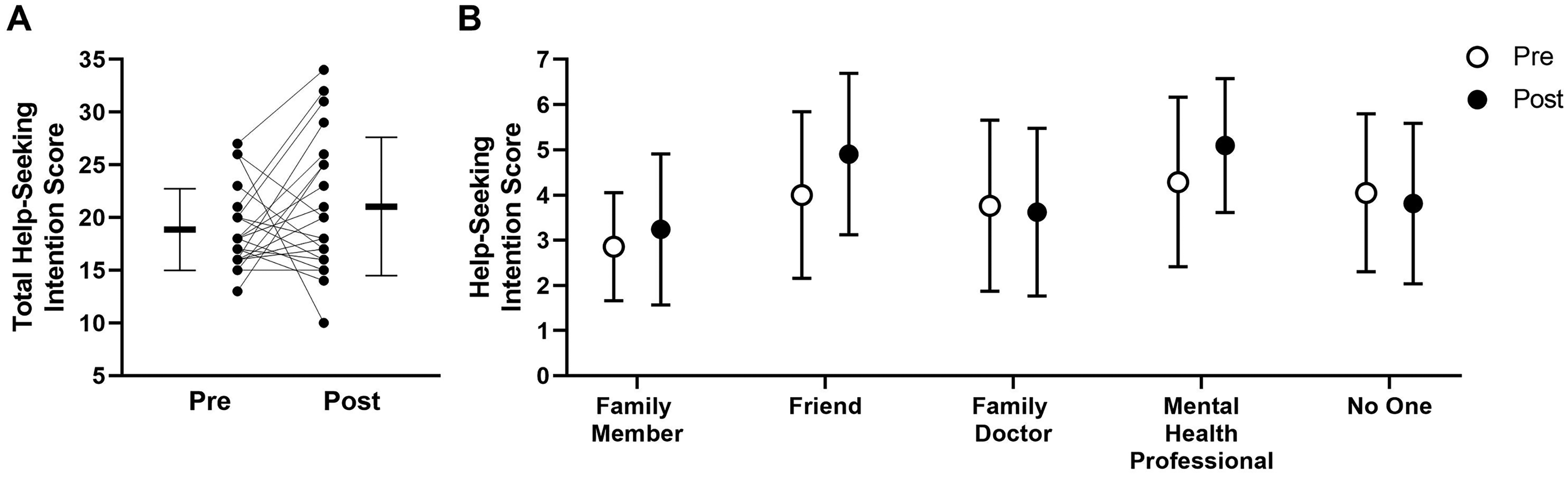
Impact of group psychoeducation on measures of help-seeking intention for a depressed scenario. (A) Total help-seeking intention score shown both as group mean (horizontal line) and individual scores (black circles) pre-group psychoeducation and post-group psychoeducation. (B) Mean help-seeking intention scores for the 5 specific sources where participants would seek help pre-group psychoeducation and post-group psychoeducation. All error bars represent standard deviation; n = 21 (intention-to-treat analysis).
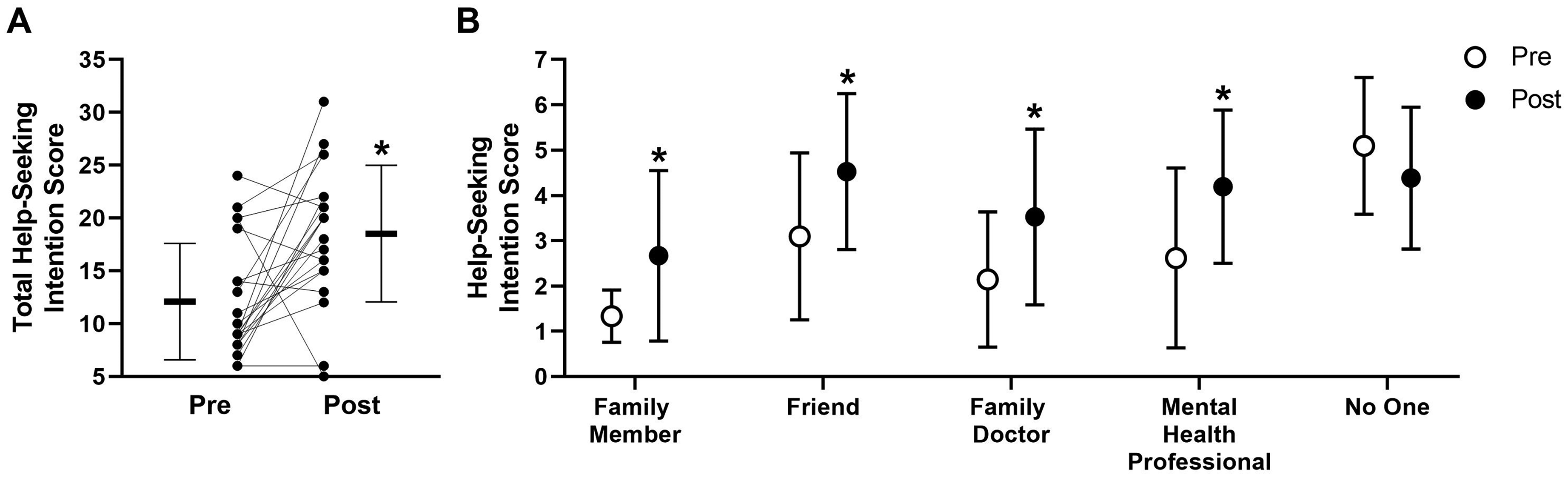
Impact of group psychoeducation on measures of help-seeking intention for a hypomanic scenario. (A) Total help-seeking intention score shown both as group mean (horizontal line) and individual scores (black circles) pre-group psychoeducation and post-group psychoeducation; *score increase was significant (p = 0.003). (B) Mean help-seeking intention scores for the 5 specific sources where participants would seek help pre-group psychoeducation and post-group psychoeducation; *score increase was signifcant (with Holm–Sidak correction for repeated measures; p < 0.03). All error bars represent standard deviation; n = 21 (intention-to-treat analysis).
Measures of resilience and self-stigma showed non-significant trends for improvement following the psychoeducation group, while quality of life scores did increase significantly (p = 0.02, t = 2.592, df = 20, d = 0.57; Figure 4). Similar trends were seen in the completers-only subgroup, though none were significant; this was attributed to inadequate statistical power in the completers-only group (estimated β = 0.44 based on significant effect size seen in intention-to-treat analysis).
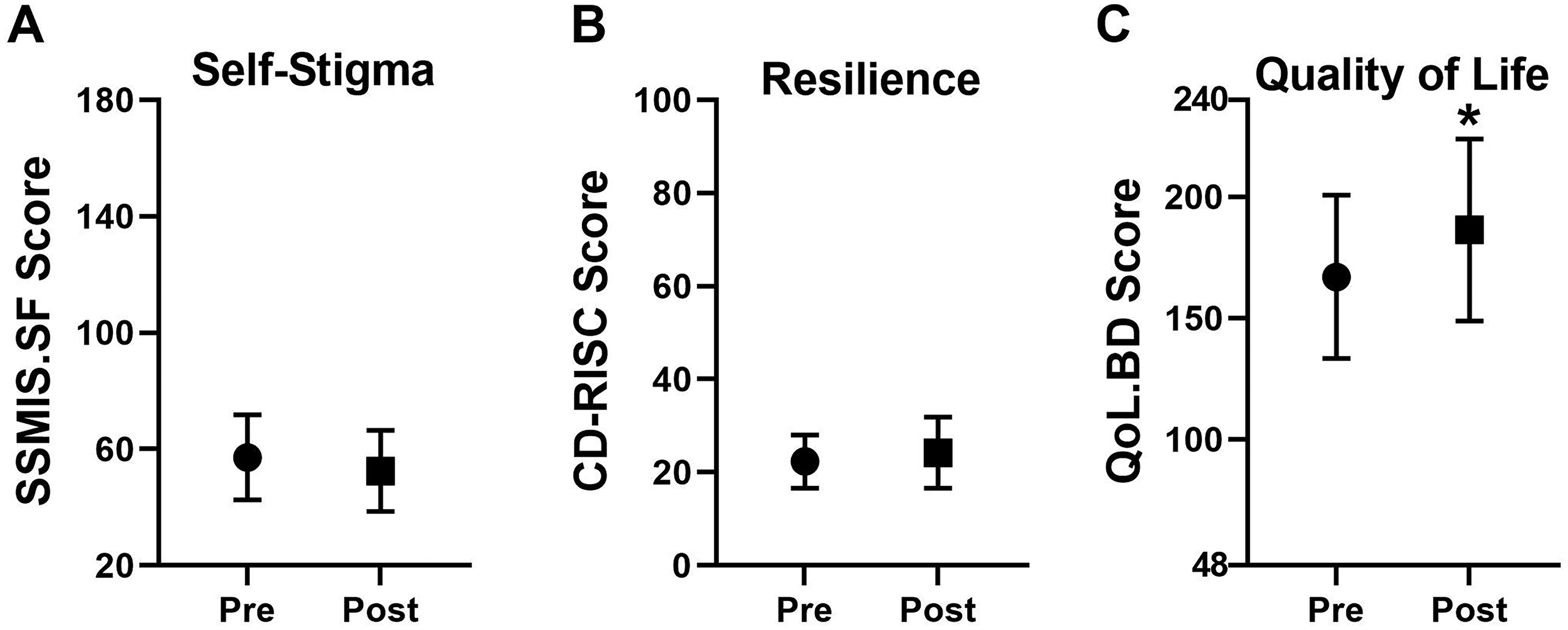
Impact of group psychoeducation on measures of self-stigma, resilience, and quality of life. Group mean changes in measures of (A) self-stigma, (B) resilience, and (C) Quality of Life pre-group psychoeducation and post-group psychoeducation; *score increase was signifcant (p = 0.02). All error bars represent standard deviation; n = 21 (intention-to-treat analysis).
Discussion
Psychoeducation is a key component of interventions, such as family-focused therapy and interpersonal and social rhythm therapy, both of which have been previously studied in at-risk populations.49,50 However, our study is the first study to assess the feasibility of a psychoeducational program tailored specifically for individuals at high risk of developing BD, with a focus on recognizing early signs of BD and improving HSIs. This feasibility study attempted to address a key gap in early intervention approaches by providing individuals at high risk of developing BD with foundational knowledge and strategies to recognize and respond to early symptoms of BD.
Our findings support the feasibility of PREP-BD, as indicated by our timely recruitment, and 100% sign-up rate. The high sign-up rate can be attributed to several factors, including the virtual modality of the program, which enhanced accessibility and convenience for participants. Additionally, the focus on relevant and practical information tailored to the needs of high-risk individuals may have contributed to participants’ motivation to enroll. The completion rate was 76.19%, further supporting the program's acceptability. For comparison, a real-world evaluation of group psychoeducation for BD reported a completion rate of approximately 60%. 51 This relatively high completion rate suggests that participants found the program engaging and beneficial, reinforcing the value of its design and delivery methods. It should be noted that the majority of non-completers (4 out of 5) were part of a single cohort, likely influenced by timing conflicts related to university examination schedules and potential group dynamics that may have impacted engagement and participation. All participants—both completers and non-completers—successfully completed the post-intervention questionnaires, with the mean CSQ-8 score of above 20, further supporting the relative acceptability of PREP-BD.41,42
Preliminary efficacy outcomes suggest that PREP-BD shows promise in enhancing HSIs in response to early BD symptoms, particularly regarding help-seeking for early signs of hypomanic symptoms. The educational intervention may have had a clearer impact on help-seeking for hypomania than depression as the majority of our group had already personally experienced depression. The intervention was also associated with an improvement in quality-of-life scores, as well as non-significant trends for improvements in measures of resilience and self-stigma. The mechanisms underlying these improvements, however, remain to be fully understood. Targeted information provided in the educational sessions might have facilitated participants’ understanding of early BD signs and available treatment options, potentially leading to enhanced HSIs. In addition, the emphasis of the program on self-management strategies could have contributed to the improvement in quality of life, as participants may have felt more informed and empowered to manage challenges related to their mental health and well-being. Alternatively, the relational dynamics between participants and facilitators could have played a role in enhancing the potential effectiveness of PREP-BD. Engaging with clinicians in a supportive, educational environment may have helped participants feel more confident in their ability to engage with the healthcare system and contributed to reduction in self-stigma. Overall, our preliminary efficacy signals warrant further investigation in an adequately powered randomized controlled trial designed specifically to address the effectiveness of PREP-BD and to identify the mechanisms through which the program can influence HSIs and other key outcomes.
An interesting observation was that, during the screening, 10 out of the 39 individuals who underwent a diagnostic assessment in our study reported a history of a full manic or hypomanic episode and were excluded from the study as a result. Notably, none of these individuals had ever received a diagnosis of BD. This observation aligns with existing concerns regarding the high prevalence of undiagnosed BD and with findings from the literature suggesting that the use of structured diagnostic interviews and screening tools tends to improve the detection rates of BD.52–54 However, despite their proven efficacy, these tools remain underutilized in routine clinical practice, contributing to the lengthy diagnostic delays. 17
The concept of an at-risk state for BD is still in its early stages and has not been as thoroughly validated as the ultra-high-risk (UHR) criteria for psychosis. 55 While a confirmed family history in a first-degree relative is a strong predictor of BD, a systematic review of high-risk studies suggests that predictive accuracy can be improved when combined with clinical risk factors such as depressive episodes and subthreshold manic symptoms. 56 In defining the high-risk state for this study, we selected the BAR criteria, a validated tool that incorporate both clinical features and family history rather than relying solely on familial risk. A potential limitation of this approach is the heterogeneity within the high-risk population identified by the BAR criteria, which may impact the magnitude of observed effects. Although more narrowly defined subgroups could allow for more tailored interventions, our study aims to develop and evaluate an intervention that can be applied to a broad high-risk population.
The findings from this feasibility study highlight the potential value of increasing awareness among individuals at high risk for developing BD, as demonstrated by the PREP-BD program. Enhancing knowledge about early symptoms and addressing self-stigmatization can improve help-seeking behaviors, potentially reducing the duration of undiagnosed BD and improving outcomes. Healthcare providers play a crucial role in delivering this education, empowering at-risk individuals to recognize warning signs and engage proactively with mental health services.
Limitations and Strengths
There are a number of important methodological considerations and limitations that warrant further discussion. First, since the primary objectives of this study were to evaluate the feasibility and acceptability of PREP-BD, it was conducted as an open trial without a control group. This limits any inference of improvement owing solely to the intervention. Future efficacy trials incorporating controlled comparisons are essential to assess the intervention's impact on help-seeking behaviors. Another important limitation of this feasibility trial is the small sample size which, while appropriate for feasibility testing, may not provide sufficient power to detect meaningful differences in outcomes despite being appropriate for feasibility assessment.
57
Another limitation of this study is that most participants were recruited through online advertisements, as opposed to patients who are engaged in mental health services. This may have introduced selection bias favoring motivated individuals and limit the generalizability of our findings. Additionally, the reliance on “soft” and mostly subjective outcome measure, such as HSIs, without incorporating objective outcome measures including help-seeking behaviors may limit the ability to draw robust conclusions about the intervention's effectiveness. One further limitation of this study is the limited training provided to facilitators and the lack of comprehensive evaluation of the fidelity of the intervention's delivery. Without assessing fidelity, it is difficult to ensure that the intervention was consistently implemented as intended, which may affect the reliability of the observed outcomes. Nevertheless, a key objective of this work was to develop a psychoeducational tool with minimal barriers to deployment on a larger scale. Future studies with larger sample sizes could investigate whether facilitators have variable impact in terms of efficacy and participant satisfaction, providing insight into the need for additional facilitator training
Despite these limitations, our study provides valuable insight on the feasibility of using psychoeducational interventions for individuals at risk of developing BD. One notable strength of this study lies in the use of multiple facilitators from diverse professional backgrounds and varying levels of experience. This diversity not only enriched the delivery of the intervention but also provides support for the scalability of the intervention by demonstrating that PREP-BD can be potentially implemented by a wide range of professionals with various levels of clinical experience. Further, the video-based delivery would allow for the widespread adoption of the intervention by overcoming practical challenges (such as the need for travel, time constraints, and geographic limitations) making the intervention more accessible to individuals who might otherwise face difficulties participating.
Conclusion and Future Directions
Undiagnosed BD is associated with serious consequences including prolonged suffering, delayed treatment, and poor outcomes, highlighting the urgent need for early identification strategies. The findings from this feasibility study highlight the potential of psychoeducation, as demonstrated by PREP-BD, to improve HSIs, particularly in response to hypomanic symptoms, and reducing self-stigmatization among individuals at risk for BD. Additionally, improvements in quality of life indicate the broader potential benefits of early psychoeducational interventions in this population.
Building on the promising results of this feasibility study, future research could focus on expanding to a larger, well-characterized high-risk group to evaluate the intervention's impact on additional outcomes including symptom improvement, adoption of healthy behaviors, and overall well-being. Stratifying participants based on their high-risk profiles, such as family history and clinical factors, would provide a better understanding of how the intervention works for different high-risk subgroups. Additionally, an exploratory analysis of the effectiveness of individual modules would help refine the program, ensuring that the most impactful components are emphasized. Finally, long-term follow-up in a controlled study design is critical to evaluate sustained outcomes beyond the immediate post-intervention period, allowing for a better understanding of the intervention's lasting effects.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437251342278 - Supplemental material for Early Psychoeducational Intervention for Youth and Young Adults at Risk for Bipolar Disorder: A Feasibility Study: Intervention psychoéducative précoce pour les adolescents et les jeunes adultes à risque de trouble bipolaire : Une étude de faisabilité
Supplemental material, sj-docx-1-cpa-10.1177_07067437251342278 for Early Psychoeducational Intervention for Youth and Young Adults at Risk for Bipolar Disorder: A Feasibility Study: Intervention psychoéducative précoce pour les adolescents et les jeunes adultes à risque de trouble bipolaire : Une étude de faisabilité by Kamyar Keramatian, Alexander Levit, Heeva Chavoshi-Nejad, Clara Westwell-Roper, John-Jose Nunez, Ashley Forbes, Emma Morton and Erin E. Michalak, Eduard Vieta, Lakshmi N. Yatham in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
KK holds a Tier 2 Canada Research Chair in Early Interventions in Psychosis/Bipolar Disorder and is supported by the Michael Smith Health Research Foundation of BC, Vancouver Coastal Health Research Institute and VGH & UBC Hospital.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KK has previously served on an advisory board of AbbVie.
EM has received honorarium for advising on the development of educational materials for Neurotorium, an online educational platform supported by the Lundbeck Foundation.
EEM has received funding to support unrelated patient education initiatives from Otsuka-Lundbeck.
JJN has received funding from the BC Cancer Foundation, as well as an unrestricted research grant from Pfizer Canada.
EV has received grants and served as consultant, advisor or CME speaker for the following entities: AB-Biotics, AbbVie, Adamed, Alcediag, Angelini, Biogen, Beckley-Psytech, Biohaven, Boehringer-Ingelheim, Celon Pharma, Compass, Dainippon Sumitomo Pharma, Ethypharm, Ferrer, Gedeon Richter, GH Research, Glaxo-Smith Kline, HMNC, Idorsia, Johnson & Johnson, Lundbeck, Luye Pharma, Medincell, Merck, Newron, Novartis, Orion Corporation, Organon, Otsuka, Roche, Rovi, Sage, Sanofi-Aventis, Sunovion, Takeda, Teva, and Viatris, outside the submitted work.
LNY reports consultant/speaker fees from Alkermes, Allergan (currently Abbvie), Intracellular Therapies, LivaNova, Merck, Newron, Sumitomo Pharma, and grants from Allergan (now AbbVie), CIHR, and Sumitomo Pharma, outside the submitted work, over the last 3 years.
AF, AL, CWR and HC have no conflict of interest to disclose.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the University of British Columbia Djavad Mowafaghian Centre for Brain Health Kickstart Grant (#F21-02746) awarded to KK.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.